
Submitted:
18 September 2023
Posted:
20 September 2023
You are already at the latest version
Abstract
Zoon balanitis (ZB) is a mild and chronic inflammatory dermatosis that mostly affects uncircumcised men of middle and old age. The etiology of this disease remains unknown. Moreover, some authors have questioned the presence of this type of balanitis.
Our study aimed to assess the expression of proinflammatory cytokines in ZB and demonstrate the presence of a characteristic expression pattern, different from that reported in the literature for penile lichen sclerosus(LS) and penile cancer.
Skin biopsies from four foreskins affected by Zoon’s balanitis with surrounding morphologically unchanged skin and 13 from nonlesional foreskins (healthy control adult males undergoing circumcision) were obtained. RNA was extracted from each biopsy, followed by quantitative assessment of the gene expression of interleukin 1-A(IL-1A), interleukin 1-B(IL-1B),interleukin 1 receptor antagonist(IL-1RN),interleukin 6(IL-6), transforming growth factor β1(TGF-β1), and interferon-gamma(INF-γ).
The decreased level of IL-1A mRNA was observed in Zoon’s balanitis in both inflamed and healthy skin compared to control samples. There were no statistically significant differences in other investigated cytokines gene expression between Zoon’s balanitis and the control group. In conclusion, the expression of proinflammatory cytokines was not related to the course of zoon balanitis. Moreover, in the case of IL-1A, we observed the suppression of the immune response.
Keywords:
zoon balanitis
; IL‑1
; IL‑1RN
; IL‑6
; IFN‑γ
; TGF‑β1
1. Introduction
Zoon balanitis (ZB), also known as plasma cell balanitis (PCB) is a mild and chronic inflammatory dermatosis. This kind of balanitis affects mostly uncircumcised men in middle and old age, although its occurrence have also been described in the younger age group [1]. The etiology is unknown. However, some authors suggest poor hygiene and smoking could be associated with Zoon balanitis development [2]. Characteristic clinical picture consists of a well-circumcised orange-red glittering area on the glans penis or the prepuce [3].
Differential diagnosis comprises erythroplasia of Queyrat and chronic forms of balanitis such as psoriasis, lichen planus, bacterial or candida infection. Dermoscopy is an useful diagnostic tool [4]. Histologically, ZB is characterized by diamond- or lozenge-shaped flattened keratinocytes, while number and location of plasma cells may vary [5]. Topical treatment is based mostly on the use of corticosteroids, calcineurin inhibitors, antibiotics (such as mupirocin or fusidic acid), and recently topical tacrolimus [5,20], however the most effective treatment is circumcision, probably because of removing the cause of the irritation [6,7,8,9].
Although in the treatment of ZB immunosuppressive topical agents are widely used, in the literature there is lack information about the expression of the pro-inflammatory cytokines which could be potentially involved in ZB etiopathogenesis. There is only one study which indicates the lower mRNA expression of NF-κB1 and NF-κB2 (nuclear factor of kappa light polypeptide gene enhancer in B-cells 1 and 2) in ZB than in the control group [10].
Our study aimed to assess the mRNA expression of cytokines such as interleukin 1-A (encoded by IL1A gene, alias IL-1A), interleukin 1-B (IL1B, IL-1B), interleukin 1 Receptor Antagonist (IL1RN, IL-1RN, IL-1Ra) interleukin 6 (IL6, IL-6), transforming growth factor β1 (TGFB1, TGFβ-1), and Interferon-gamma (INFG, INF-γ) in the foreskin samples of Zoon balanitis in comparison with the healthy penile skin.
2. Materials and Methods
Patients and skin biopsies
The biopsies from Zoon balanitis affected an healthy (morphologically unchanged) foreskins were obtained from 4 patients who underwent circumcision at the Department of Urology, between January 2017 and December 2019. The control group consist of foreskin specimens obtained during complete circumcision and histopathological examination of the whole prepuce confirmed healthy skin. Moreover, C-reactive protein (CRP) levels were measured before surgery. An independent Bioethics Committee has approved the present study (decision No. NKBBN/369/2017), and all patients had signed written informed consent before circumcision. The follow-up data of ZB patients was collected till Dec 2021.
Skin biopsies acquisition
The biopsies were collected during complete circumcision due different reasons such as Zoon balanitis (n=4; 23.5%) and short frenulum (n=13; 76.5%). Before surgery patients have not received any topical treatment, especially corticosteroids. After circumcision, tissue fragments of inflamed and healthy fragments were cut into two similar fragments, separately; one was immediately placed in 5 volumes of RNA-Later (Ambion Inc., a brand of Thermo Fisher Scientific, Inc.), and stored in a fridge for 6 to 24 hours, than storage in -80°C until further processing (RNA extraction). The remaining tissue fragment underwent fixation in ~10 volumes of buffered 4% formaldehyde (pH=7.4, POCH, Poland), and stored at 4°C. Formalin-stored tissues were further processed for histopathological assessment.
RNA extraction and transcription assessment
Assessment of the mRNA expression of IL-1A, IL-1B, IL-1RN, IL-6, TGF-β1 and IFN-γ genes
RNA isolation was optimized by adapting a modified method of Chomczynski and Sacchi [11] using a Total RNA Mini protocol isolation kit (A&A Biotechnology, Gdańsk, Poland). Briefly, RNA-Later samples were defrosted, drained of liquid with a sterile paper towel; from each sample two 3×3×3 mm tissue fragments were cut out for RNA extraction. The remaining tissue sample of similar size was placed in a sterile vial and immediately placed in liquid nitrogen, and then was stored at -80°C for different analyzes. The processed biopsy tissue was cut with sterile scissors to as small as possible fragments and placed in a 1.5 ml Eppendorf tube with 800 µl Fenozol. The tube was incubated in TS-100C (BioSan, Riga, Latvia) thermoblock at 50°C for 45 min. After adding 200 µl chloroform (POCH, Gliwice, Poland), samples were gently mixed, and incubated at room temperature (RT) for 5 min, followed by centrifugation at 12000 rpm for 15 min at 4°C. The next steps of RNA extraction were carried out by the manufacturer’s protocol with the final elution volume of 100 µl RNAse-free water. After RNA quantity and purity assessment (Epoch 800 plate reader), RNA was stored at -80°C for further analyses. cDNA synthesis was performed as previously described [12]. Total RNA samples (2 µg) were reverse transcribed with RevertAid Reverse Transcriptase (Fermentas; Thermo Fischer Scientific, Inc.). Details concerning the qPCR methodology are provided in Table 1. One µl of four-times diluted cDNA was used in 10 µl total volume of qPCR reaction. All reactions were run in duplicate; each sample was represented by two independent results, which have been statistically processed. The measurement of glucuronidase beta (GUSB) gene expression was used for the normalization of qPCR results with Livak and Schmittgen’s 2ΔΔCq method [13,14].
Statistical analysis
Statistical analysis was performed using GraphPad Prism version 6.07 (GraphPad Software) software. The following statistical tests were used: Shapiro-Wilk normality; Spearman’s correlation and parametric Student t- test. A two-sided p<0.05 was considered to indicate a statistically significant difference, with a 95% confidence interval in all analyses.
3. Results
Patient characteristics
According to histopathological examination, patients enrolled on the study were divided into two groups: Zoon balanitis (n=4; 23.5%); healthy skin (n=13; 76.5%).
The patient's demographic and clinical data were collected in the database and shown in the Table 2.
The average follow-up period was 55 months (range: 48 – 58 months). There are no recurrence of Zoon balanitis in the follow-up period.
Expression of the cytokines’ gene in all groups of patients
The decreased IL-1A expression levels were observed in Zoon balanitis in inflamed biopsies (mean ± SD: 0.028 ± 0.006) and in healthy fragments of foreskin (mean ± SD: 0.019 ± 0.007) comparison with the control group (mean ± SD: 1 ± 0.091, p = 0.039 and p=0.023, separately), Figure 1. Levels of other analyzed cytokines were also decreased (except for IL-6 in healthy foreskins of ZB patients), however with no statistical significance.
Association between cytokines’ mRNA levels and clinical data
Further we checked all possible relationships between molecular and clinical data, with the use of Spearman’s correlation test. No relationship between the mRNA levels of the tested cytokines and age, BMI or CRP values, neither in inflamed or morphologically unchanged ZB samples or control biopsies. In turn, the comparison between the mRNA levels of individual cytokines in the samples showed a very strong positive correlation (rs=0.9524, p = 0.0011) between mRNA expression for IL-1A and IL-1RN genes in inflamed tissues (Figure 2A), but not in healthy ZB samples (Figure 2C). The opposite observation was noted to IL1A/IL-6 mRNA levels, which positive relationship has been revealed in ZB margin foreskin, but not in active ZB samples (Figure 2D and B, respectively). No other relationships between the molecular data were observed.
4. Discussion
The pro-inflammatory cytokines such as interleukin 1A, 1B and IL-6 are produced mostly by macrophages and participate in the inflammatory or fibrogenic processes [15,16]. The macrophages are recruited among others by INF-γ which is antiviral and pro-inflammatory cytokine [17]. The anti-inflammatory effect depends on blocking the IL-1 receptor, which was observed in case of IL-1RN molecule [18]. Another pro-fibrotic cytokine, which takes part in wound healing is TGF-β [19]. The altered expression of cytokines leads to the imbalance in the organism and the formation of various diseases.
Zoon balanitis is a mild, chronic inflammatory dermatosis of unknown aetiology that affects mostly uncircumcised men in middle and old age. Histologically it is characterized by numerous presence of B cells (>50% of all immune cells) in the dermis [1]. In later stages of ZB, atrophy of the epidermis, superficial erosions, scant neutrophils in the upper epidermis, slight spongiosis, extravasation of erythrocytes, and a much denser infiltrate with many plasma cells are seen. Additional findings at even later stages consist of subepidermal clefts, sometimes with loss of the entire epidermis, marked fibrosis of the superficial dermis and many siderophages. Moreover, in ZB there is a nonspecific polyclonal stimulation of B cells secondary to chronic inflammation. IgG-, IgA- and IgD-positive plasma cells predominate in the infiltrate; however, IgM-producing plasma cells may also be found [20]. Despite the fact that there are numerous case series about the successful treatment of ZB, some authors questions its existence as a separate kind of balanitis [21]. They claim that ZB does not exist separately but often accompanies other dermatoses such as lichen sclerosus (LS) or penile intraepithelial neoplasia (PeIN) and squamous cell carcinoma (SCC). Additionally, in their opinion biopsy could be taken from “Zoon-like lesions” and missed another dermatosis [21]. Although ZB is a disease related to accumulation of B cells/plasma cells in the dermis [5,22], it is not related to possible neoplastic transformation, due to absence of B-cell predominant infiltrations that lack a reactive etiology [22].
In our study we have enrolled patients after histopathological examination of whole foreskin specimens with ZB confirmation. Although our project comprised only on 4 patients from one clinic collected within 2 years, which can be compared to case study by Moreno-Arias et al. who analyzed samples from two patients [20], while Jormanainen et al. collected samples from 129 ZB patients for several years [5]. Additionally, other dermatoses or penile cancer were excluded. After assessment of mRNA expression of proinflammatory cytokines, we have detected the 36 times decreased level of IL-1A and ca. 20% decrease of IL-6 and INF-γ in Zoon balanitis at the mRNA levels in comparison to the healthy controls. Contrary, in lichen sclerosus the mRNA expression of IL-1A, INF-γ, and IL-6 was increased, as observed in our previous report [23]. We suppose, that if ZB was accompanied by LS or a penile cancer in studied 4 cases, the level of the analyzed proinflammatory cytokines should be increased. The same mRNA expression levels of NF-κB1 and NF-κB2 were elevated in LS and penile cancer. Interestingly, in ZB there were no differences in expression levels of such nuclear factors [10]. Those molecular findings partially indicated that ZB remains different disease apart from dermatosis and does not represent pre-cancerous lesion, at least for the formation of penile SCC.
We observed very strong positive relationship between IL-1A and IL-1RN expression rates in inflamed ZB samples. Although IL-1A is secreted by epithelial, endothelial and stromal cells [15] and trigger neutrophils, macrophages and lymphocytes, which can also secrete IL-1A [24]. Driving inflammation is the primary role of IL-1A via activation and control of immune cells, but also in maintenance of epithelial barriers. Keratinocytes secrete pro-IL-1α that can be processed by thrombin activated during hemostasis after wounding. This connection between the coagulation and immune systems allows rapid IL-1α activation and immune cell recruitment that can safeguard against potential infection after breach of the epidermal barrier [25]. Although it was noted that high levels of IL-1A may be connected to autoimmunological dermatoses, especially neutrophilic dermatoses [26]. On the contrary, IL-1RN (IL-1Ra), IL-1ra is the first endogenous receptor antagonist described for a cytokine signalling system and has been shown to specifically block the effects of both IL-1A and B [27]. Inhibition of IL-1A by IL-1RN was proven to play a vital role in immune balance. DIRA (deficiency of IL-1Ra) is a rare, neonatal-onset characterized by constitutive lack of IL-1Ra. Newborns with DIRA develop severe, multisystem inflammation. A striking clinical manifestation of DIRA is severe, widespread neutrophilc dermatosis, which resembles pustular psoriasis as a result of overexpression of IL-1A [26]. IL-1A and IL-1RN cross-talk was observed in central nervous system development and diseases [27]. Moreover, IL-1RN mesenchymal producing cells function as modulator of diabetogenesis via silencing response of pancreatic β-cells to IL-1A [28]. Our observation suggest, that in active ZB, a moderate level of IL-1RN expression (in comparison to control samples) can effectively suppress IL-1A expression by inflammatory cells. Such association was not observed in non-inflamed ZB skin samples, contributing unique immunological pattern of zoon balanitis. However, larger study needs to be conducted in order to verify this observation.
Interleukin-6 is a pleiotropic cytokine that plays a crucial role in immune and inflammatory responses. Among its functions, IL-6 is involved in induction of the hepatic acute phase response, bone metabolism, reproduction, neoplasia and aging [29]. Canonical activation of IL-6 expression is triggered by bacterial molecules (i.e. LPS) via activation PI3K followed by AKT pathway [29]. However, proinflammatory cytokines: IL-1 and TNF and TGFβ also induce IL-6 expression; IL-1A induce IL-6 biosynthesis via activation of IKK (NFKB) pathway [30]. Such association was observed in our ZB samples from the margin foreskin. Both cytokines, IL-6 and IL-1A are strongly associated, however, IL-1A is decrease while IL-6 level is almost unchanged in comparison to healthy controls samples. IL-6 levels in ZB margin may be affected by presence of bacterial environment. The observed IL-1A/IL-6 relationship in unchanged ZB samples was no longer visible in active ZB, despite of similar decreased IL-1A expression in both types of ZB biopsies. It seems that expression of IL-1A in ZB depends on inhibitory relation with IL-1RN during ZB active inflammation, which results in deregulation an partial inhibition of IL-6 in inflamed foreskin.
Patients suffering from ZB in our study underwent surgical circumcision. As data from several years of follow-up showed, there was no recurrence of the disease, which confirms the effectiveness of the selected treatment method, which is consistent with the results of other clinical trials [6,7,8,9]. On the other hand, circumcision is an invasive method, and pharmacological treatment methods can replace surgical techniques. According to the review by Dayal and Sahu, the best treatment results in the absence of recurrence were observed with the use of tacrolimus 0.1% [1], which was confirmed in a large study by Jormanainen et al . on 129 patients with ZB, none of whom had undergone circumcision [5]. The effect of tacrolimus is the inhibition of the formation of cytotoxic T cells, but the most important thing is the inhibition of the proliferation of T helper-dependent B lymphocytes. On the other hand, tacrolimus is an immunosuppressive drug, not indifferent to the body even in the form of an ointment. Therefore, there is a need to implement a treatment other than the above surgical or immunosuppressive ones, and the results of our work may support this choice.
Currently, there is no data regarding the measurement of any cytokine in the ZB, therefore, our results are the first to be published in this field. Moreover, the IL-1RN vs. IL-1A balance in any disease related to B cell or plasmocyte has not been checked yet. Our results may be evidence of non-participation of analyzed cytokines in the etiopathology of Zoon balanitis or, the specific relationship between IL-1RN and IL-1A which results in partial IL-1A expression silencing. Moreover, our study shows a specific pattern of proinflammatory cytokines expression in ZB, both in active inflammation and healthy margin foreskin samples which was different from LS or penile cancer. These results could confirm the existence of ZB as a separate disease. However, the small number of cases does not allow us to make any decisive statement.
5. Conclusions
Expressions of proinflammatory cytokines mRNA are not increased in Zoon’s balanitis. Moreover, in case of IL-1A, we observed the suppression of the immune response, which may be associated with strong expression of IL-1RN in particular samples.
Author Contributions
Conceptualization: M.Cz., K.Cz., methodology: P.W, A. K-C., formal analysis: M.Cz, P.W., investigation: M.Cz, K.Cz., resources: M.Cz., data curation: M.Cz, K.Cz., writing—original draft preparation: M.Cz, K.Cz., writing—review and editing: M. S-W, Z.K., M.M. M. K-W., supervision: M. S-W, Z.K, M.M. All authors have read and agreed to the published version of the manuscript.
Funding
The study was founded by the 01-02-10022/0000651 and 02-10022/0000672 funds of the Medical University of Gdańsk.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional independent Ethics Committee of Medical University of Gdansk (decision No. NKBBN/369/2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dayal S, Sahu P. Zoon balanitis: A comprehensive review. Indian J Sex Transm Dis AIDS. 2016, 37, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Piaserico S, Orlando G, Linder MD, Cappozzo P, Zarian H, Iafrate M. A case-control study of risk factors associated with Zoon balanitis in men. J Eur Acad Dermatol Venereol. 2019, 33, 1591–1594. [Google Scholar] [CrossRef] [PubMed]
- Edwards SK, Bunker CB, Ziller F, van der Meijden WI. 2013 European guideline for the management of balanoposthitis. Int J STD AIDS. 2014, 25, 615–626. [Google Scholar] [CrossRef]
- Errichetti E, Lallas A, Di Stefani A, Apalla Z, Kyrgidis A, Lacarrubba F, et al. Accuracy of dermoscopy in distinguishing erythroplasia of Queyrat from common forms of chronic balanitis: results from a multicentric observational study. J Eur Acad Dermatol Venereol. 2019, 33, 966–972. [Google Scholar] [CrossRef]
- Jormanainen, A, Pasternack, C, Pasternack, R. A retrospective study of 129 patients with plasma cell balanitis. JEADV Clin Pract. 2023, 2, 293–299. [Google Scholar] [CrossRef]
- Niu X, Yang X, Wang F, Hou R, Yao L, Han Q, et al. A novel and effective therapy for Zoon balanitis: Topical crisaborole 2% ointment. J Eur Acad Dermatol Venereol. 2023, 37, e212–e214. [Google Scholar]
- Lee MA, Cohen PR. Zoon Balanitis Revisited: Report of Balanitis Circumscripta Plasmacellularis Resolving With Topical Mupirocin Ointment Monotherapy. J Drugs Dermatol. 2017, 16, 285–287. [Google Scholar]
- Roé E, Dalmau J, Peramiquel L, Pérez M, López-Lozano HE, Alomar A. Plasma cell balanitis of zoon treated with topical tacrolimus 0.1%: report of three cases. J Eur Acad Dermatol Venereol. 2007, 21, 284–285. [Google Scholar] [CrossRef]
- Kumar B, Narang T, Dass Radotra B, Gupta S. Plasma cell balanitis: clinicopathologic study of 112 cases and treatment modalities. J Cutan Med Surg. 2006, 10, 11–15. [Google Scholar] [CrossRef]
- Wierzbicki PM, Czajkowski M, Kotulak-Chrząszcz A, Bukowicz J, Dzieciuch K, Sokołowska-Wojdyło M, et al. Altered mRNA Expression of NFKB1 and NFKB2 Genes in Penile Lichen Sclerosus, Penile Cancer and Zoon Balanitis. J Clin Med. 2022, 11, 7254. [Google Scholar] [CrossRef]
- Chomczynski P, Sacchi N. The single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction: twenty-something years on. Nat Protoc. 2006, 1, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicki PM, Klacz J, Kotulak-Chrzaszcz A, Wronska A, Stanislawowski M, Rybarczyk A, et al. Prognostic significance of VHL, HIF1A, HIF2A, VEGFA and p53 expression in patients with clear-cell renal cell carcinoma treated with sunitinib as first-line treatment. Int J Oncol. 2019, 55, 371–390. [Google Scholar]
- Schlotter YM, Veenhof EZ, Brinkhof B, Rutten VP, Spee B, Willemse T, et al. A GeNorm algorithm-based selection of reference genes for quantitative real-time PCR in skin biopsies of healthy dogs and dogs with atopic dermatitis. Vet Immunol Immunopathol. 2009, 129, 115–118. [Google Scholar] [CrossRef]
- Schmittgen TD, Livak KJ. Analyzing real-time PCR data by the comparative C(T) method. Nat Protoc. 2008, 3, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Malik A, Kanneganti TD. Function and regulation of IL-1α in inflammatory diseases and cancer. Immunol Rev. 2018, 281, 124–137. [Google Scholar] [CrossRef] [PubMed]
- Kumari N, Dwarakanath BS, Das A, Bhatt AN. Role of interleukin-6 in cancer progression and therapeutic resistance. Tumour Biol. 2016, 37, 11553–11572. [Google Scholar] [CrossRef] [PubMed]
- Mojic M, Takeda K, Hayakawa Y. The Dark Side of IFN-γ: Its Role in Promoting Cancer Immunoevasion. Int J Mol Sci. 2017, 19, E89. [Google Scholar] [CrossRef]
- Cauci S, Buligan C, Rocchi F, Salvador I, Xodo L, Stinco G. Interleukin 1 receptor antagonist gene variable number of tandem repeats polymorphism and cutaneous melanoma. Oncol Lett. 2019, 18, 5759–5768. [Google Scholar]
- Lichtman MK, Otero-Vinas M, Falanga V. Transforming growth factor beta (TGF-β) isoforms in wound healing and fibrosis. Wound Repair Regen. 2016, 24, 215–222. [Google Scholar] [CrossRef]
- Moreno-Arias GA, Camps-Fresneda A, Llaberia C, Palou-Almerich J. Plasma cell balanitis treated with tacrolimus 0.1%. Br J Dermatol. 2005, 153, 1204–1206. [Google Scholar] [CrossRef]
- Bunker, CB. Zoon balanitis-does it exist. J Eur Acad Dermatol Venereol. 2020, 34, e116–e117. [Google Scholar] [CrossRef] [PubMed]
- Khalil S, Donthi D, Gru AA. Cutaneous reactive B-cell lymphoid proliferations. J Cutan Pathol. 2022, 49, 898–916. [Google Scholar] [CrossRef] [PubMed]
- Czajkowski M, Wierzbicki P, Kotulak-Chrząszcz A, Czajkowska K, Bolcewicz M, Kłącz J, et al. The role of occlusion and micro-incontinence in the pathogenesis of penile lichen sclerosus: an observational study of pro-inflammatory cytokines' gene expression. Int Urol Nephrol. 2022, 54, 763–772. [Google Scholar] [CrossRef]
- Pyrillou K, Burzynski LC, Clarke MCH. Alternative Pathways of IL-1 Activation, and Its Role in Health and Disease. Front Immunol. 2020, 11, 613170. [Google Scholar] [CrossRef]
- Burzynski LC, Humphry M, Pyrillou K, Wiggins KA, Chan JNE, Figg N, et al. The Coagulation and Immune Systems Are Directly Linked through the Activation of Interleukin-1α by Thrombin. Immunity 2019, 50, 1033–1042. [Google Scholar] [CrossRef]
- Cavalli G, Colafrancesco S, Emmi G, Imazio M, Lopalco G, Maggio MC, et al. Interleukin 1α: a comprehensive review on the role of IL-1α in the pathogenesis and treatment of autoimmune and inflammatory diseases. Autoimmun Rev. 2021, 20, 102763. [Google Scholar] [CrossRef]
- Spulber S, Bartfai T, Schultzberg M. IL-1/IL-1ra balance in the brain revisited - evidence from transgenic mouse models. Brain Behav Immun. 2009, 23, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Volarevic V, Al-Qahtani A, Arsenijevic N, Pajovic S, Lukic ML. Interleukin-1 receptor antagonist (IL-1Ra) and IL-1Ra producing mesenchymal stem cells as modulators of diabetogenesis. Autoimmunity 2010, 43, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Cahill CM, Rogers JT. Interleukin (IL) 1beta induction of IL-6 is mediated by a novel phosphatidylinositol 3-kinase-dependent AKT/IkappaB kinase alpha pathway targeting activator protein-1. J Biol Chem. 2008, 283, 25900–25912. [Google Scholar] [CrossRef]
- Kwan Tat S, Padrines M, Théoleyre S, Heymann D, Fortun Y. IL-6, RANKL, TNF-alpha/IL-1: interrelations in bone resorption pathophysiology. Cytokine Growth Factor Rev. 2004, 15, 49–60. [Google Scholar] [CrossRef]
Figure 1.
Cytokines’ gene expression at the mRNA level in penile tissue. Gene expression was assessed as described in Methods. The ordinate axis is shown on a logarithmic scale. Bars and whiskers represent the mean ± standard deviation of the mean (SEM) normalized to control foreskin samples (presented as 1, dotted horizontal line); light grey bars for control, dark grey bars for inflammed samples while checkerboard motif for non-inflamed ZB samples. * P < 0.05 (Shapiro-Wilk normality; and parametric Student t- test).
Figure 1.
Cytokines’ gene expression at the mRNA level in penile tissue. Gene expression was assessed as described in Methods. The ordinate axis is shown on a logarithmic scale. Bars and whiskers represent the mean ± standard deviation of the mean (SEM) normalized to control foreskin samples (presented as 1, dotted horizontal line); light grey bars for control, dark grey bars for inflammed samples while checkerboard motif for non-inflamed ZB samples. * P < 0.05 (Shapiro-Wilk normality; and parametric Student t- test).
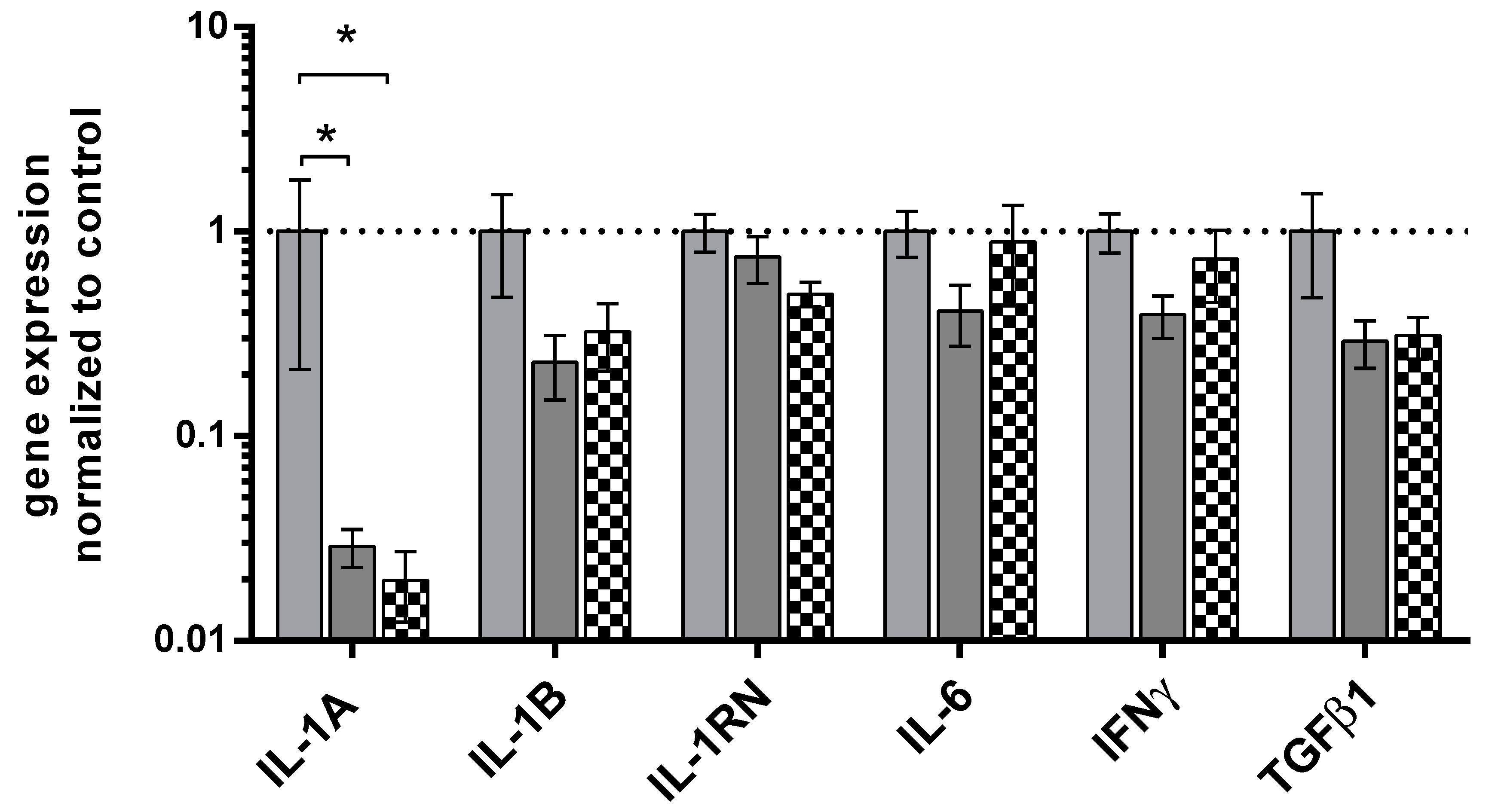
Figure 2.
Correlation plot of selected cytokines levels in ZB samples. Selected dots represent expression data normalized to control tissues (n=1). Solid line represents linear regression curve with 95% confidence band (dotted lines). (A,B) – expression pattern in active ZB samples; (C,D) – morphologically healthy ZB samples. Boxed values represent statistically significant correlations., Spearman's test. Abreviations: IL-1A; interleukin 1A, IL-1RN; interleukin 1 receptor antagonist, IL-6; interleukin 6.
Figure 2.
Correlation plot of selected cytokines levels in ZB samples. Selected dots represent expression data normalized to control tissues (n=1). Solid line represents linear regression curve with 95% confidence band (dotted lines). (A,B) – expression pattern in active ZB samples; (C,D) – morphologically healthy ZB samples. Boxed values represent statistically significant correlations., Spearman's test. Abreviations: IL-1A; interleukin 1A, IL-1RN; interleukin 1 receptor antagonist, IL-6; interleukin 6.
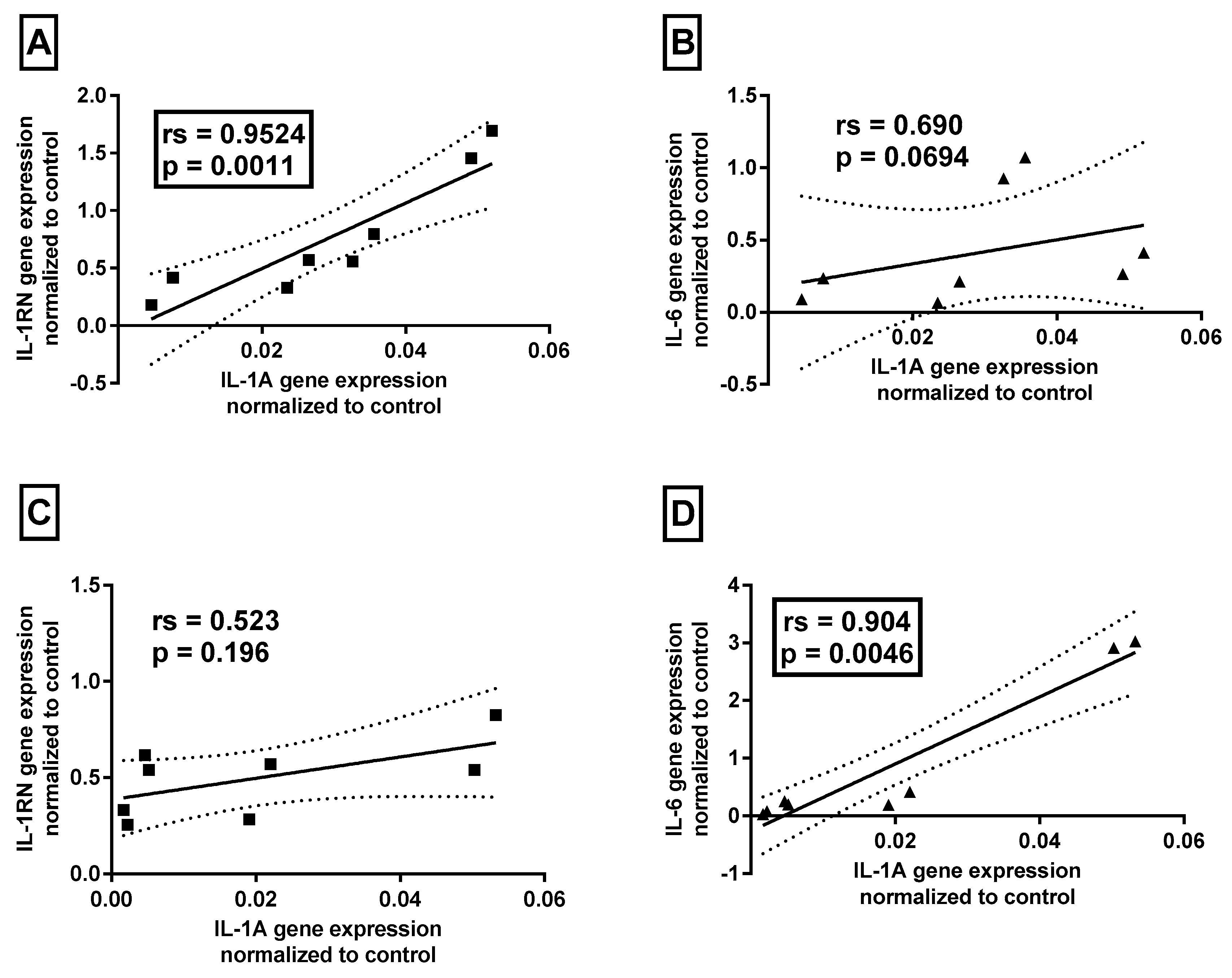

Table 1.
Details of qPCR assays.
| Gene name | Primers’ sequences | qPCR reaction conditions | qPCR reaction content |
|---|---|---|---|
| IL-1α | 5’-TAGGTCAGCACCTTTTAGCTTC 5’-GTATCTCAGGCATCTCCTTCAG |
95°C, 3 min; 45x (95°C, 5 sec; 59°C, 10 sec; 72°C, 10 sec; 75 °C, 10 sec – sample reading) Melting curve: 95°C, 15 sec; 60°C, 1 min; 60°C → 95°C reading every 0.3°C |
5 µl AmplifyMe NoRox SybrGreen (with SybrGreen fluorophore) ( Blirt, Poland), 200 nM each primer, Σ 10 µl |
| IL-1β | 5’- CCTTAGGGTAGTGCTAAGAGGA 5’- TACAGACACTGCTACTTCTTGC |
||
| IL-1RN | 5’- GGCACTTGGAGACTTGTATGAA 5’- GAGCTGAAGTCACAGGAAGTAG |
||
| IL-6 | 5’- CACTCACCTCTTCAGAACGAAT 5’- AGGCAAGTCTCCTCATTGAATC |
||
| INF- γ | 5’- TGGAAAGAGGAGAGTGACAGAA 5’- TATTGCTTTGCGTTGGACATTC |
||
| TNF-β | 5’- GAGCTGTACCAGAAATACAGCA 5’- AACTCCGGTGACATCAAAAGAT |
||
| GUSB | 5’ – ATGCAGGTGATGGAAGAAGTGGTG 5’ - AGAGTTGCTCACAAAGGTCACAGG |
Table 2.
Demographic characteristic and histopathological diagnosis of patients.
| Group | N | Age [y]: mean ± SD; median (range) | P (all groups) | BMI: mean ± SD | P* (all groups) | CRP [mg/dL]: mean ± SD | P *(all groups) |
|---|---|---|---|---|---|---|---|
| Zoon Balanitis | 4 | 59.25 ± 25.00; 65.0 (24-83) | 25.75 ± 3.13 | 1.83 ± 0.79 | |||
| Control | 13 | 31.38 ± 14.80; 24.0 (21-65) | 0.0011 | 28.21 ± 6.96 | Ns (0.86) | 1.76 ± 2.85 | Ns (0.11) |
| *Student t test used since Shapiro-Wilk normality test was passed, otherwise Mann-Whitney U test. | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



