
Submitted:
18 September 2023
Posted:
20 September 2023
You are already at the latest version
Abstract
The anterior cruciate ligament (ACL) injury is the most serious injury in judo. Therefore, its prevention is of great importance. The main mechanism of injury is the collapse of the knee in valgus, which usually occurs when there are deficits of strength and neuromuscular control of the core, external rotators and hip abductors, as well as limitations of ankle and hip mobility. In most sports there is a difference in the prevalence of this injury between both sexes, being more common in women. Therefore, in the present study we observed this possible intersexual disparity in the difference of movement patterns among elite judokas according to their sex, in order to identify those athletes with a higher risk of ACL injury. In addition, it was not observed differences between sexes in the performance of the Single Leg Squat test (SLS test); There was worse neuromuscular control of the non-dominant leg in men and women; No differences were observed in in the range of motion of ankle dorsiflexion and hip external rotation between men and women, but there were differences in internal rotation, a movement whose restriction may be related to an increased risk of ACL injury.
Keywords:
anterior cruciate ligament
; judo
; biomechanics
; knee injury
; gender differences
1. Introduction
Judo is a very popular and commonly practiced martial art and Olympic sport of Japanese origin [1] with more than 20 million judokas worldwide [2]. It is observed that 79% of judokas suffer or have suffered an injury lasting more than 3 weeks[3]. Of all the injuries recorded, the most serious is the anterior cruciate ligament (ACL) rupture[2]. The ACL rupture affects with a time loss of 3-12 weeks in 10%, 3-6 months in 26%, 6-9 months in 32%, 9-12 months in 18% and more than 12 months in 14% of the injured judokas. Regarding the post-injury sport level, 32% reached the same level, 39% slightly reduced, 24% quite reduced and 5% gave up judo [2]. It is especially important to note that ACL injuries can lead to the development of osteoarthritis and/or joint instability, which can affect sports practice as well as work or daily life [4].
According to multiple literature sources, the mechanism of ACL injury is knee collapse in knee valgus [5,6,7,8,9,10,11,12,13]. Dynamic knee valgus is a multiplanar movement pattern of the lower extremity, potentially composed of a combination of femoral adduction and internal rotation, knee abduction, anterior tibial translation, external tibial rotation and ankle eversion [7,9].
The origin of ACL injury is multifactorial and is largely caused by neuromuscular deficits in structures such as the core, hamstring and quadriceps muscles, hip abductors and external rotators, decreased ankle dorsiflexion and hip mobility [7,8]. Of all these there are differences between men and women, which can lead to a dynamic valgus of the knee and, consequently, to the risk of ACL injury [7,8,10,11,12,13,14,15,16,17,18,19,20,21,22,23]. A study developed by Hewett et al. [7] demonstrate that men and women exhibit different activation and muscle recruitment strategies at the hip and knee joints.
In judo, the most common mechanism of suffering an ACL tear is through direct contact (70.1%), or indirect contact (20.1%), unlike other sports such as basketball, where the injury usually occurs without contact, in movements such as braking, jumping or pivoting [5]. It has also been seen that most cases occur when the injured judoka is attacked (67.4%), especially in those techniques in which the leg is used as a fulcrum to knock the opponent down, such as osoto-gari (18,6%) (Figure 1), harai-goshi (11.6%) (Figure 2), kosoto-gari/gake (14%) (Figure 3) or kouchi-gari/gake (9.3%) (Figure 4) although also when counterattacking (18.6%) (Figure 5) or when attacking (14%), with the tai-otoshi technique (11.6%) (Figure 6) being of note [5,24].
It has been observed that more injuries occur when judokas fight between judokas of different laterality (kenka-yotsu), i.e. right-handed vs left-handed, than when they are of the same laterality (ai-yotsu), right-handed vs right-handed or left-handed vs left-handed (Figure 7) [1,2]. It is speculated that the higher risk of injury in kenka-yotsu is due to a greater likelihood of being counter-attacked, a common situation of suffering an ACL tear [3,24].
In a study of ACL injuries in soccer [25], researchers examined 107 case videos of 134 Italian men's professional soccer matches over 10 years. They found that 44% of injuries were non-contact, 44% were indirect contact, and 12% were direct contact. Four main injury situations were identified: pressing and tackling, tackling, regaining balance after a kick, and landing from a jump. Knee valgus loading was the primary injury pattern in all situations (81%). Most injuries (62%) occurred in the first half of matches, with peaks at the start and end of the season.
Under a physiologic load in a position commonly assumed in sports, women tend to position their entire lower extremity and activate muscles in a manner that could increase strain on the anterior cruciate ligament [26].
Therefore, the main objective of the present study was to detect the possible existence of a differences in movement patterns among elite judokas according to their sex, in order to identify those athletes with a higher risk of ACL injury.
2. Materials and Methods
2.1. Study Design
We conducted an observational cross-sectional study on 14 male (61%) and 9 female (39%) professional judokas worldwide (n=23) performed between November 2022 and March 2023. Procedures were conducted following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement and checklist [27]. The study protocol was approved by the Human Research Ethics Committee from the Universitat de Valencia by number 1675151998994, Valencia, Spain (February 09, 2023). Informed consent was obtained from all participants, and all procedures were conducted according to the Declaration of Helsinki.
2.2. Participants
In order to reach an approximation to this athlete profile, the sample was composed of a group of elite judokas from the Specialized High-Performance Center (C.e.A.R.) of Judo from Valencia (Figure 8). The selected athletes had to meet a series of requirements to be included in the study: be judoka from the Valencia Judo C.e.A.R. and be competing at the time of the measurements in national and international championships; be over 18 years of age, not suffer any injury, not have undergone recent surgery or be in a period of readaptation.
2.3. Clinical Measurements
For the present study, the test chosen to assess the risk of ACL injury was the Single Leg Squat test (SLS). The reason for choosing this test is that, as noted above, the mechanism of ACL injury production in judo is through a displacement of the centre of mass towards one leg together with direct contact on that leg, which makes it similar to a monopodal squat. According to the study developed by Zeller et al. [26], the SLS test can be considered a promising candidate for the assessment of risk of ACL injury. Based on Baldazzi et al. [28], the SLS test includes single-leg closed-chain movements, which are typical of open-skill sports, and is also used for knee stability and on the likelihood of ACL injury.
The test was performed by asking the athletes, who had to be barefoot, to place their hands on their hips and stand on one limb and flex the opposite limb to 90° of knee flexion. They were then instructed to perform a single-leg squat to 30° of flexion of the supported knee [29] (Figure 9). Subsequently, they were required to perform a knee extension to full extension, i.e. 0° of flexion [29]. While the athletes performed the test, a visual inspection was carried out to estimate whether the participant reached 30° knee flexion, giving verbal feedback to ensure that the knee flexion was neither greater nor less than 30°. The monopodal squat was performed 3 times in a row on each leg while the investigator noted any abnormal response consisting of arm flailing, Trendelenberg or valgus knee collapse. The SLS test is positive if more than 2 of the 3 possible abnormal movements appeared in any of the legs out of the total of 6 attempts (3 SLS attempts on each leg). A positive SLS test may suggest poor lower extremity mechanics, decreased core strength or weakness of the hip abductors [26]. In a recent study published by Ressman et al, they found "moderate" interrater reliability and " almost perfect" intrarater reliability, regardless of rater experience[30].
Assessment of ankle dorsiflexion was performed using the Lunge test method described in the article by Simondson et al. [31] (Figure 10). The patient placed the foot of the ankle to be measured along the tape measure, with the big toe against the wall and the toe and heel on the centre line of the tape. The patient was instructed to bring his knee as close to the wall as stiffness or pain would allow. Pronation was not controlled. The patient was allowed to lean against the wall if necessary. The therapist firmly held the patient's heel to the floor. Progressively, they were asked to move their toe backwards away from the wall on the treadmill, repeating the lunging motion until the maximum distance the knee could be brought towards the wall without the heel being lifted. The point at which the patient's heel was felt to lift indicated the limit of motion, at which the measurement was taken [31]. Lunge test demonstrated good to excellent reliability, with ICCs between 0.8 and 0.96 for the asymptomatic side. On the symptomatic side, Lunge test showed excellent reliability, with ICCs above 0.90 [32].
Passive hip mobility was assessed bilaterally by Hip mobility test. For this purpose, the participant was placed in the supine position with the hip to be assessed in 90° flexion. The contralateral limb was placed in full extension. While performing internal and external rotations of the hip to be measured, the pelvis was stabilized so that the head and neck of the femur contacted the acetabular rim (Figure 11).
These measurements were performed 3 times with each hip and measured with a universal goniometer and the average value was calculated [21].
In order to perform the tests, it was necessary to use a tape measure with an accuracy of 1 mm for the Lunge test and a goniometer for the hip mobility test. The application of a goniometer in these circumstances provides good reliability for the symptomatic side [30].
2.4. Statistical Analysis
For statistical analysis, the program R Ver. 4.1.3 (R Foundation for Statistical Computing, Institute for Statistics and Mathematics, Welthandelsplatz 1, 1020 Vienna, Austria) was used. The level of significance was established at p<0.05. The Shapiro-Wilk test was used to test the distribution of the quantitative variables. Quantitative variables were described with mean ± standard deviation and qualitative variables with absolute and relative values (%). The presence of significant differences in the quantitative outcome variables based on gender was analyzed using the student’s T test (after verification of the assumption of homogeneity of variances with the Levene test) or with the Mann-Whitney U test depending on gender. its distribution, while Fisher’s exact test was applied to the qualitative variables. The effect size was calculated using Cohen’s D in the quantitative variables with a normal distribution, defined as small (<0.5), medium (0.5-0.8) and large (0.8), or with the non-parametric estimator r in the variables with a non-normal distribution defined as small (<0.4), medium (0.4-0.6) and large (>0.6). In the case of qualitative variables, Cramer’s V was used, defining it as small (<0.1), medium (0.1-0.2) and large (>0.2). Linear regression models were applied with the quantitative outcome variables as dependent and gender and dominance as explanatory variables; in the case of the SLS, it was dichotomized as negative (absence of response) and positive (presence of any response) to apply similar binary logistic regression models. In both cases the objective was to evaluate the effect of the dominant leg on the results depending on gender.
3. Results
The study involved 23 players with a majority of men (60.9%) and right dominant leg (69.6%) (Table 1).
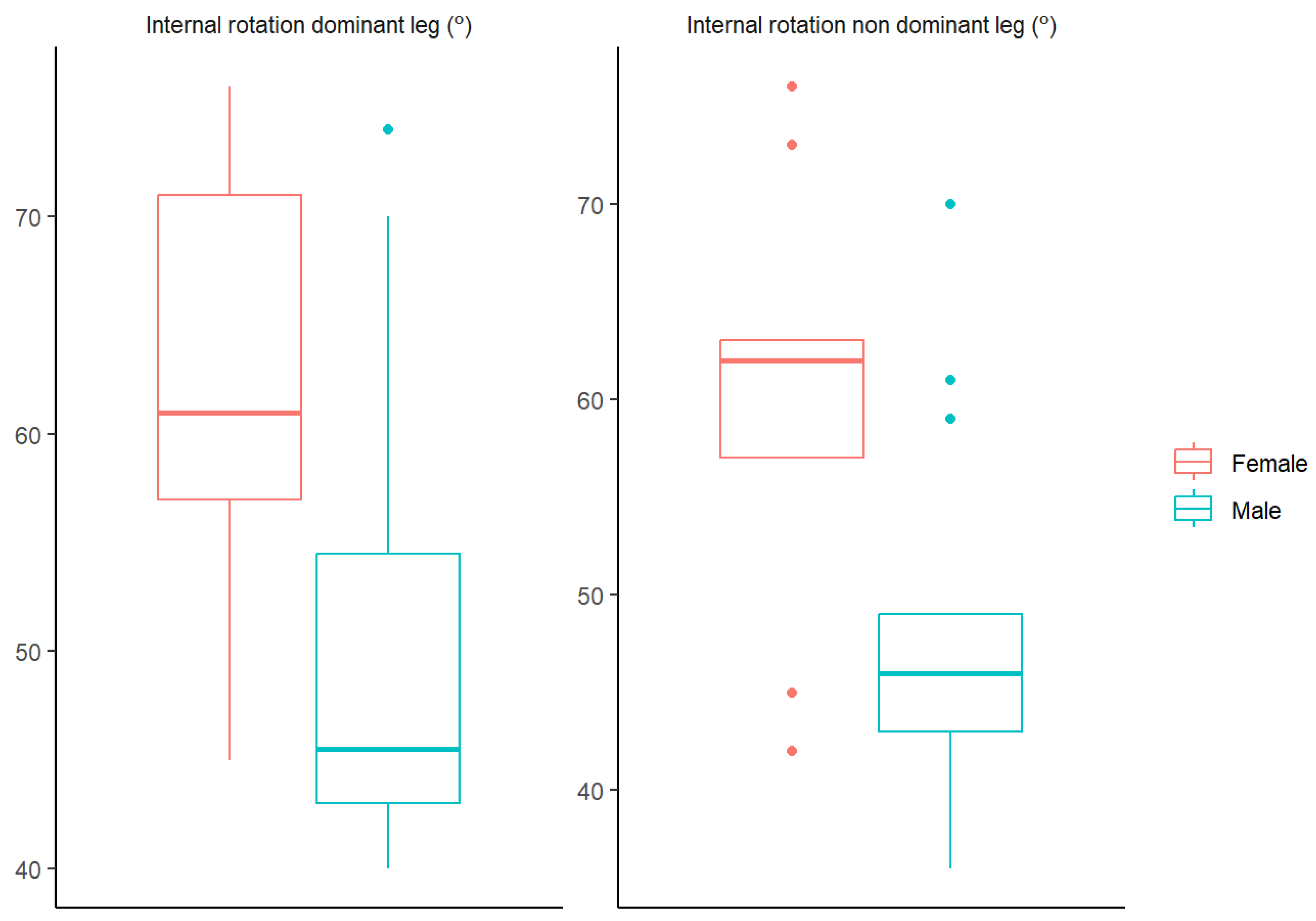
The presence of significant differences is verified in the variable Internal rotation dominant leg (º) (Z=2.588, p=0.01) with a medium and significant effect size and higher values in women in 12.389 (2.651, 22.127) degrees compared to men. Significant differences are also shown in the variable Internal rotation non-dominant leg (º) (t(15.614)=2.615, p=0.014) with a large and significant effect size and values also higher in women in 12 (2.253, 21.747) degrees. compared to men (Table 2 and Figure 1).
Figure 1.
Significant variables boxplots.
The anova table shows how neither the Dominant leg nor the interaction Gender:Dominant leg are significant, which indicates that dominance does not influence the results (Table 3).
4. Discussion
The main objective of the present study was to detect the possible existence of a differences in movement patterns among elite judokas according to their sex, in order to identify those athletes with a higher risk of ACL injury.
Firstly, no differences were observed between sexes in the Single Leg Squat test, neither in the dominant nor in the non-dominant leg. Furthermore, no differences were observed between men and women in the different hip external rotation tests of both lower limbs and in the Lunge test bilaterally. On the other hand, in the hip internal rotation tests, differences were observed between men and women, both in the dominant and non-dominant leg.
With regard to the SLS test, no differences were observed between men and women in either the dominant or non-dominant lower limb. It should also be noted that the prevalence of obtaining a positive test in this test is quite low, 8.7% for the dominant and 26.1% for the non-dominant. If the data is analyzed in more depth, it can be observed that of all the judokas, a large number obtained at least 1 positive in one of the items assessed in the SLS test (in the dominant leg 60.9% and in the non-dominant leg 82.6%). If only 1 positive in these items, the overall test result is negative, so it is of great importance to note the high rate of positives in these aspects in isolation. This data is of great interest as it may support the high prevalence of ACL injury in judo.
If we analyze the positivity of the test between both legs, we observe a higher positivity of some of the items and of the SLS test in the non-dominant leg, which is of great importance since this is the support leg in monopodal support techniques. In addition, more ACL injuries occur in bouts between judokas with opposite laterality and with techniques such as osoto-gari or harai-goshi in which the attacked judoka receives the attack on the non-dominant leg [5].
Of all the possible abnormal movement patterns that can be observed and assessed in the SLS test, such as arm flailing, knee valgus and Trendelenberg, the one that can be seen the least in both legs is pelvic instability or Trendelenberg sign (8.7% in the dominant lower limb and 21.7% in the non-dominant). This indicates that there is good control of the core musculature. However, there is a high percentage of judokas with uncontrolled arm movements (17.4 and 34.8% respectively) and dynamic knee valgus (34.8 and 26.1% respectively). From these data it can be assumed that the judoka's stability cannot depend on the arms, since in the usual combat situations in which the ACL injuries usually occur, it is the opponent who attacks, being unlikely to be able to maintain the balance and stability of the attacked knee with a support of the hands on the opponent. On the other hand, it is of utmost importance to highlight the role of knee valgus observed in the SLS test, a movement previously mentioned as being mainly responsible for the ACL injury [5,6,7,8,9,10,11,12,13]. Therefore, it would be of great interest to perform neuromuscular control exercises to stabilize dynamic knee valgus without the intervention of the arms.
The study by Della Villa et al. [25] found that 90% of ACL injuries involved loading the injured leg, often with a limb on the ground (70%). They stated that proper biomechanics, aligning force vectors for joint stability, were crucial. ACL injuries were the result of mechanical perturbations to the upper or lower body during interactions with opponents, without direct contact with the knee. Hip abduction motion was frequent, resulting in increased hip internal rotation and adduction in most cases, possibly due to an externally oriented knee abduction moment from hip abduction. Injuries were more frequent in the first half of the matches, suggesting that factors other than fatigue played a role, possibly related to hip rotation and myotatic reflexes.
In terms of physical preparation for competition, von Gerhardt et al. [33] evaluated the efficacy of a specific judo injury prevention warm-up program supervised by a coach on overall injury prevalence, and concluded that the intervention did not significantly reduce the prevalence of overall and severe injuries.
Lambert et al. [34] found that the type of injury, sport level, treatment method and gender seemed to influence the judoka's psychological preparation and ability to return to sport after injury. However, in the present study no differences were observed between sexes in the external rotation of the athletes participating in the study, neither in the dominant nor in the non-dominant leg. On the other hand, statistically significant differences were observed in the internal rotation of both legs, with the mean range of this movement being lower in men than in women. This difference may be related to the dynamic knee valgus observed as the main mechanism of injury [5,6,7,8,9,10,11,12,13]. As for the hip, this movement involves adduction and internal rotation of this joint [7,9].
On the other hand, it is of great relevance to highlight that restrictions in hip mobility may be a risk factor for ACL injury [21,22,31]. Clinical and radiological studies assessing this injury risk have shown an association between decreased hip rotations and the likelihood of previous ACL injury [22]. In addition, in silico biomechanical simulations and cadaver studies have provided evidence of a mechanism of hip restriction at the ACL, highlighting the importance of internal rotation restrictions. Indeed, the article by VandenBerg et al. [22] discusses the association of ACL injury risk with hip internal rotation limitation. As hip IR increases, the likelihood of ACL rupture decreases. However, prospective cohort studies are needed to establish that decreased hip mobility is a risk factor for ACL injury, so this may not be sufficient reason to determine that men are at greater risk of ACL injury. However, as mentioned above, it is of great importance to work on the neuromuscular control of the external rotators and hip abductors, which are responsible for braking and stabilizing the knee towards valgus collapse. If they do not exercise their function, they could lead to increased ligamentous tension and thus an increased risk of ACL injury [7,9,10,15].
Finally, the data obtained in the Lunge test was analyzed. This test also does not show different results between men and women in both dominant and non-dominant lower limbs. Although the averages of both legs were higher in the male gender, these differences were not statistically significant, so neither can we show a disparity in the risk of ACL injury between the sexes due to ankle dorsiflexion restriction.
As already noted, there is no biomechanical factor that is really a demonstrable cause to conclude that, as in other sports such as basketball, handball, volleyball or football, the risk of ACL injury is higher in women than in men [5,6,7,35]. This is probably due to the way in which they occur. In all the sports mentioned above, the majority of ACL injuries occur in non-contact actions such as changes of direction, braking and jumping. Based on these results, neuromuscular training methods were developed to reduce the risk of non-contact ACL injuries. Due to the characteristics of judo as a martial art, a non-contact mechanism is not the main cause of ACL injuries and a neuromuscular training approach may not be suitable for prevention [5]. As developed by Koshida et al., the occurrence of ACL injury is more common in movements where the leg is used as a fulcrum, when the injured judoka is attacked and when the judoka is on the opposite side of the body [5]. Therefore, the difference observed between both sexes in other sports may not be extrapolated to judo [36]. Deficits in postural control and neuromuscular function of the knee and hip are highly predictive of the risk of a second ACL injury after return to sport following ACL reconstruction [7,37]. Rehabilitation programs aimed at reducing functional asymmetries prior to return to sport after ACL reconstruction may be necessary to more safely reintegrate these patients into sport [7,37].
In our study we have assessed mobility and activation of the lower limb joints, observing limitation in hip internal rotation that could modify the force vectors in the entire lower limb, increasing the risk of injury. Impaired hip rotation ROM is commonly associated to lower extremity pathology [38]. The influence of central descending reflexes in improving hip mobility has been demonstrate [39]. Due to the contribution of the sensorimotor cortex in joint flexibility [40].
It would be necessary to find and modulate the mobility dysfunctions produced by the central descending reflexes in order to improve neuromuscular activation and therefore joint stability. In this way, the judoka would be as well repaired as possible to respond and protect himself from the opponent's impacts.
4.1. Limitations and Strengths
This study also presents a series of limitations, such as the proportion between both sexes and the number of participants because they are elite athletes.
In addition, no data was collected on previous injuries because they were competing at a high level and thus be able to assess the possible dysfunctions that they could create.
This would have been of great interest as a previous ACL injury significantly increases the likelihood of sustaining another ACL injury. Even so, significant differences were only found in hip internal rotation.
5. Conclusions
Although in other sports there is a difference between men and women in the prevalence of ACL injury, there is no gender disparity in judo. This may be due to the fact that the most common mechanism of injury in judo is contact, unlike in other sports where it is non-contact. There is worse neuromuscular control of the non-dominant leg in men and women. No differences are observed in hip external rotation between men and women, but there are differences in internal rotation possibly produced by central descending reflexes, a movement whose restriction may be related to an increased risk of ACL injury.
Author Contributions
Conceptualization, F.J.P.B. and F.S.S.; methodology, F.J.P.B., J.N.C.Z. and F.S.S.; software, F.J.P.B.; validation, all authors; formal analysis, J.N.C.Z., F.S.S. and E.A.S.R.; investigation, F.J.P.B.; resources, F.J.P.B.; data curation, J.N.C.Z. and F.J.P.B.; writing—original draft preparation, F.J.P.B. and F.S.S.; writing—review and editing, F.S.S., J.N.C.Z. and E.A.S.R.; visualization, F.J.P.B.; supervision, F.S.S.,J.N.C.Z. and E.A.S.R.; project administration, F.S.S.; funding acquisition, No funding. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Human Research Ethics Committee from the Universitat de Valencia by number 1675151998994, Valencia, Spain (February 09, 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data presented in this study are available upon request from the corresponding authors. The data are not publicly available due to ethical restrictions.
Acknowledgments
Thanks to the Specialized High-Performance Center (C.e.A.R.) and the Valencia Judo Federation for allowing us to use their facilities to carry out thes test and photographs. Special thanks to all judo trainers and judo athletes from the C.e.A.R. Judo Valencia and the Valencia Judo Federation for their participation in the study. Also thanks to all experts involved in the development of the intervention.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pocecco, E.; Ruedl, G.; Stankovic, N.; Sterkowicz, S.; Del Vecchio, F.B.; Gutiérrez-García, C.; Rousseau, R.; Wolf, M.; Kopp, M.; Miarka, B.; et al. Injuries in judo: a systematic literature review including suggestions for prevention. Br. J. Sports Med. 2013, 47, 1139–1143. [Google Scholar] [CrossRef] [PubMed]
- Akoto, R.; Lambert, C.; Balke, M.; Bouillon, B.; Frosch, K.-H.; Höher, J. Epidemiology of injuries in judo: a cross-sectional survey of severe injuries based on time loss and reduction in sporting level. Br. J. Sports Med. 2017, 52, 1109–1115. [Google Scholar] [CrossRef]
- von Gerhardt, A.L.; Vriend, I.; Verhagen, E.; Tol, J.L.; Kerkhoffs, G.M.M.J.; Reurink, G. Systematic development of an injury prevention programme for judo athletes: the IPPON intervention. BMJ Open Sport Exerc. Med. 2020, 6, e000791. [Google Scholar] [CrossRef] [PubMed]
- Sánchez Romero EA, Lim T, Alonso Pérez JL, Castaldo M, Martínez Lozano P, Villafañe JH. Identifying Clinical and MRI Characteristics Associated with Quality of Life in Patients with Anterior Cruciate Ligament Injury: Prognostic Factors for Long-Term. Int J Environ Res Public Health. 2021 Dec 6;18(23):12845. [CrossRef]
- Koshida, S.; Deguchi, T.; Miyashita, K.; Iwai, K.; Urabe, Y. The common mechanisms of anterior cruciate ligament injuries in judo: a retrospective analysis. Br. J. Sports Med. 2008, 44, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Larwa, J.; Stoy, C.; Chafetz, R.S.; Boniello, M.; Franklin, C. Stiff Landings, Core Stability, and Dynamic Knee Valgus: A Systematic Review on Documented Anterior Cruciate Ligament Ruptures in Male and Female Athletes. Int. J. Environ. Res. Public Heal. 2021, 18, 3826. [Google Scholar] [CrossRef]
- Hewett TE, Myer GD, Ford KR, Paterno MV, Quatman CE. Mechanisms, prediction, and prevention of ACL injuries: Cut risk with three sharpened and validated tools: ACL INJURY PREVENTION. J Orthop Res. noviembre de 2016;34(11):1843-55. [CrossRef]
- Mehl, J.; Diermeier, T.; Herbst, E.; Imhoff, A.B.; Stoffels, T.; Zantop, T.; Petersen, W.; Achtnich, A. Evidence-based concepts for prevention of knee and ACL injuries. 2017 guidelines of the ligament committee of the German Knee Society (DKG). Arch. Orthop. Trauma Surg. 2017, 138, 51–61. [Google Scholar] [CrossRef]
- Wilczyński, B.; Zorena, K.; Ślęzak, D. Dynamic Knee Valgus in Single-Leg Movement Tasks. Potentially Modifiable Factors and Exercise Training Options. A Literature Review. Int. J. Environ. Res. Public Heal. 2020, 17, 8208. [Google Scholar] [CrossRef]
- Jeong, J.; Choi, D.-H.; Shin, C.S. Core Strength Training Can Alter Neuromuscular and Biomechanical Risk Factors for Anterior Cruciate Ligament Injury. Am. J. Sports Med. 2020, 49, 183–192. [Google Scholar] [CrossRef]
- LaBella, C.R.; Hennrikus, W.; Hewett, T.E.; Brenner, J.S.; Brookes, M.A.; Demorest, R.A.; Halstead, M.E.; Kelly, A.K.W.; Koutures, C.G.; LaBotz, M.; et al. Anterior Cruciate Ligament Injuries: Diagnosis, Treatment, and Prevention. PEDIATRICS 2014, 133, e1437–e1450. [Google Scholar] [CrossRef]
- Hewett TE, Ford KR, Hoogenboom BJ, Myer GD. UNDERSTANDING AND PREVENTING ACL INJURIES: CURRENT BIOMECHANICAL AND EPIDEMIOLOGIC CONSIDERATIONS - UPDATE 2010. :18.
- Hewett, T.E.; Ford, K.R.; Xu, Y.Y.; Khoury, J.; Myer, G.D. Utilization of ACL Injury Biomechanical and Neuromuscular Risk Profile Analysis to Determine the Effectiveness of Neuromuscular Training. Am. J. Sports Med. 2016, 44, 3146–3151. [Google Scholar] [CrossRef]
- Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. The Effects of Core Proprioception on Knee Injury: A Prospective Biomechanical-Epidemiological Study. Am J Sports Med. marzo de 2007;35(3):368-73. [CrossRef]
- Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in Neuromuscular Control of the Trunk Predict Knee Injury Risk: Prospective Biomechanical-Epidemiologic Study. Am J Sports Med. julio de 2007;35(7):1123-30. [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S., Jr.; Colosimo, A.J.; McLean, S.G.; Van Den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical Measures of Neuromuscular Control and Valgus Loading of the Knee Predict Anterior Cruciate Ligament Injury Risk in Female Athletes: A Prospective Study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef]
- Wahlstedt, C.; Rasmussen-Barr, E. Anterior cruciate ligament injury and ankle dorsiflexion. Knee Surgery, Sports Traumatol. Arthrosc. 2014, 23, 3202–3207. [Google Scholar] [CrossRef]
- Hewett, T.E.; Lindenfeld, T.N.; Riccobene, J.V.; Noyes, F.R. The Effect of Neuromuscular Training on the Incidence of Knee Injury in Female Athletes. Am. J. Sports Med. 1999, 27, 699–706. [Google Scholar] [CrossRef]
- Sasaki, S.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Kimura, Y.; Fujita, Y.; Ishibashi, Y. Core-Muscle Training and Neuromuscular Control of the Lower Limb and Trunk. J. Athl. Train. 2019, 54, 959–969. [Google Scholar] [CrossRef]
- Dargo, L.; Robinson, K.J.; Games, K.E.; Dargo Lucas Dargo, MS, ATC; Kelsey J. Robinson, MS, AT, ATC; Kenneth E. Games, PhD, LAT, ATCDepartment of Applied Medicine and Rehabilitation, Indiana State University, Terre Haute; Atc; At, A.; Lat, A. Prevention of Knee and Anterior Cruciate Ligament Injuries Through the Use of Neuromuscular and Proprioceptive Training: An Evidence-Based Review. J. Athl. Train. 2017, 52, 1171–1172. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.L.E.; de Castro, J.V.; Becker, R. Decreased Hip Range of Motion and Noncontact Injuries of the Anterior Cruciate Ligament. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 1034–1037. [Google Scholar] [CrossRef]
- VandenBerg, C.; Crawford, E.A.; Enselman, E.S.; Robbins, C.B.; Wojtys, E.M.; Bedi, A. Restricted Hip Rotation Is Correlated With an Increased Risk for Anterior Cruciate Ligament Injury. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 33, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Powden, C.J.; Hoch, J.M.; Hoch, M.C. Reliability and minimal detectable change of the weight-bearing lunge test: A systematic review. Man. Ther. 2015, 20, 524–532. [Google Scholar] [CrossRef] [PubMed]
- von Gerhardt, A.L.; Reurink, G.; Kerkhoffs, G.M.M.J.; Verhagen, E.; Krabben, K.; Mooren, J.; I Gal, J.S.; Brons, A.; Joorse, R.; Broek, B.v.D.; et al. Effectiveness of a judo-specific injury prevention programme: a randomised controlled trial in recreational judo athletes. Br. J. Sports Med. 2023, 57, 450–456. [Google Scholar] [CrossRef]
- Della Villa, F.; Buckthorpe, M.; Grassi, A.; Nabiuzzi, A.; Tosarelli, F.; Zaffagnini, S.; Della Villa, S. Systematic video analysis of ACL injuries in professional male football (soccer): injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br. J. Sports Med. 2020, 54, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Zeller, B.L.; McCrory, J.L.; Ben Kibler, W.; Uhl, T.L. Differences in Kinematics and Electromyographic Activity between Men and Women during the Single-Legged Squat. Am. J. Sports Med. 2003, 31, 449–456. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 11, 260–265. [Google Scholar] [CrossRef]
- Baldazzi A, Molinaro L, Taborri J, Margheritini F, Rossi S, Bergamini E (2022) Reliability of wearable sensors-based parameters for the assessment of knee stability. PLoS ONE 17(9): e0274817. [CrossRef]
- Ugalde, V.; Brockman, C.; Bailowitz, Z.; Pollard, C.D. Single Leg Squat Test and Its Relationship to Dynamic Knee Valgus and Injury Risk Screening. PM&R 2014, 7, 229–235. [Google Scholar] [CrossRef]
- Ressman J, Grooten WJA, Rasmussen-Barr E. Visual assessment of movement quality: a study on intra- and interrater reliability of a multi-segmental single leg squat test. BMC Sports Sci Med Rehabil. 2021 Jun 8;13(1):66. [CrossRef]
- Simondson, D.; Brock, K.; Cotton, S. Reliability and smallest real difference of the ankle lunge test post ankle fracture. Man. Ther. 2012, 17, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Ganderton, C.; Tirosh, O.; Adams, R.; Ei-Ansary, D.; Han, J. Test-retest reliability of ankle range of motion, proprioception, and balance for symptom and gender effects in individuals with chronic ankle instability. Musculoskelet. Sci. Pr. 2023, 66, 102809. [Google Scholar] [CrossRef]
- von Gerhardt, A.L.; Reurink, G.; Kerkhoffs, G.M.M.J.; Verhagen, E.; Krabben, K.; Mooren, J.; I Gal, J.S.; Brons, A.; Joorse, R.; Broek, B.v.D.; et al. Effectiveness of a judo-specific injury prevention programme: a randomised controlled trial in recreational judo athletes. Br. J. Sports Med. 2023, 57, 450–456. [Google Scholar] [CrossRef]
- et al. encontraron que el tipo de lesión, el Lambert C, Guenther D, Schütz LM, Kern N, Ritzmann R, Reinert N, Walz M, Wafaisade A, Nagy K, Reuter S. Psychological readiness is related to return to sport in judo injuries: a cross-sectional study. BMC Sports Sci Med Rehabil. 2023 Feb 16;15(1):20. [CrossRef]
- Nakano N, Bartlett J, Khanduja V. Is restricted hip movement a risk factor for anterior cruciate ligament injury? J Orthop Surg (Hong Kong). 1 de septiembre de 2018;26(3):230949901879952. [CrossRef]
- Pappas, E.; Shiyko, M.P.; Ford, K.R.; Myer, G.D.; Hewett, T.E. Biomechanical Deficit Profiles Associated with ACL Injury Risk in Female Athletes. Med. Sci. Sports Exerc. 2016, 48, 107–113. [Google Scholar] [CrossRef]
- Prill, R.; Michel, S.; Schulz, R.; Coriolano, H.-J.A. Body Composition and Strength Parameters in Elite Judo Athletes 5 Years after Anterior Cruciate Ligament Reconstruction. Int. J. Sports Med. 2018, 40, 38–42. [Google Scholar] [CrossRef]
- Martin, R.L.; Enseki, K.R.; Draovitch, P.; Trapuzzano, T.; Philippon, M.J. Acetabular Labral Tears of the Hip: Examination and Diagnostic Challenges. J. Orthop. Sports Phys. Ther. 2006, 36, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Henriques, I.A.D.; Lattari, E.; Torres, G.; Rodrigues, G.M.; Oliveira, B.R.R.; Neto, G.A.M.; Neto, S.R.M.; Machado, S. Can transcranial direct current stimulation improve range of motion and modulate pain perception in healthy individuals? Neurosci. Lett. 2019, 707, 134311. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, T.; Aramaki, Y. Cathodal transcranial direct current stimulation over the Cz increases joint flexibility. Neurosci. Res. 2017, 114, 55–61. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Osoto-gari.

Figure 2.
Harai-goshi.

Figure 3.
Kosoto-gari/gake.

Figure 4.
Kouchi-gari/gake counterattack.

Figure 5.
Counterattack.

Figure 6.
Tai-otoshi.

Figure 7.
Grip styles. (a) kenka-yotsu grip style: a judoka and the opponent have different grip sides; (b) Ai-yotsu grip style: a judoka and the opponent have the same grip side. Informed consent was obtained for publication of this figure.
Figure 7.
Grip styles. (a) kenka-yotsu grip style: a judoka and the opponent have different grip sides; (b) Ai-yotsu grip style: a judoka and the opponent have the same grip side. Informed consent was obtained for publication of this figure.

Figure 8.
(a) C.e.A.R. sport facilities; (b) C.e.A.R. judo mat in a judo training.

Figure 9.
Single Leg Squat test. a) First stage of the test, b) Second stage of the test.
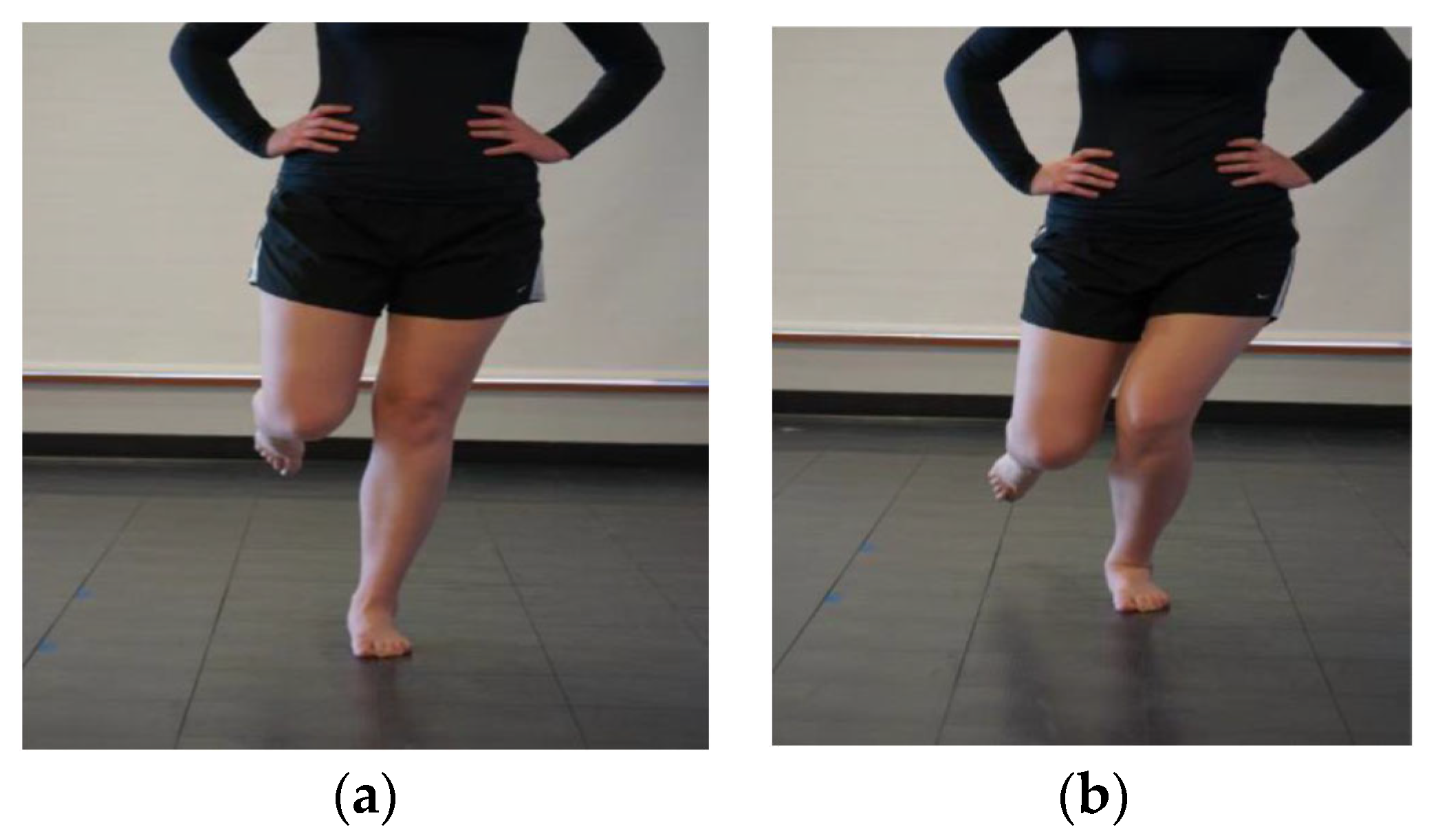
Figure 10.
Lunge test.

Figure 11.
Passive hip internal rotation.
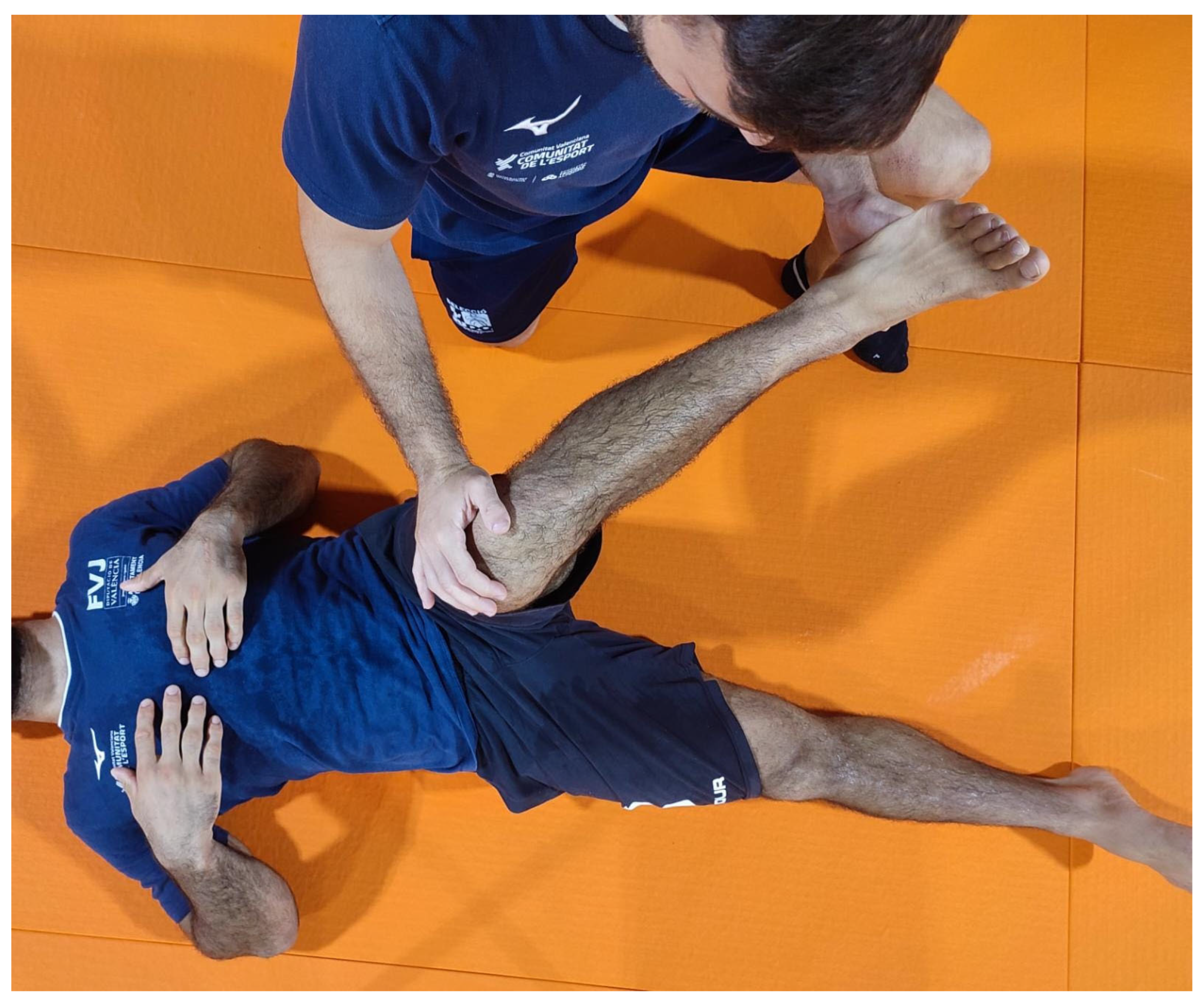

Table 1.
Demographic characteristics of the participants and overall outcomes.
| n. | 23 | |
| Gender, n(%) | Female | 9 (39.1) |
| Male | 14 (60.9) | |
| Dominant leg, n(%) | Left | 7 (30.4) |
| Right | 16 (69.6) | |
| SLS dominant leg, n(%) | Arms | 2 (8.7) |
| Nothing | 12 (52.2) | |
| Pelvis | 1 (4.3) | |
| Valgus | 6 (26.1) | |
| Valgus and arms | 1 (4.3) | |
| Valgus, arms and pelvis | 1 (4.3) | |
| SLS non-dominant leg, n(%) | Arms | 5 (21.7) |
| Arms and pelvis | 2 (8.7) | |
| Nothing | 10 (43.5) | |
| Pelvis and valgus | 2 (8.7) | |
| Valgus | 2 (8.7) | |
| Valgus and arms | 1 (4.3) | |
| Valgus and pelvis | 1 (4.3) | |
| Lunge test dominant leg | 13.04±3.47 | |
| Lunge test non-dominant leg | 13.17±3.02 | |
| External rotation dominant leg (º) | 90.52±8.70 | |
| Internal rotation dominant leg (º) | 54.35±12.32 | |
| External rotation non-dominant leg (º) | 87.91±10.25 | |
| Internal rotation non-dominant leg (º) | 52.91±11.72 | |
| Data expressed as mean±standard deviation or with absolute and relative values (%); SLS: Single Leg Squat test. |
Table 2.
Outcomes by gender.
| Female | Male | Levene test p valuea | ap value | Average difference (95%CI) | Effect size (95%CI) | ||
|---|---|---|---|---|---|---|---|
| n | 9 | 14 | NA | NA | |||
| SLS dominant leg, n(%) | Arms | 0 (0.0) | 2 (14.3) | NA | 0.486 | 0.44 (0.466, 1)✣ | |
| Nothing | 5 (55.6) | 7 (50.0) | NA | NA | |||
| Pelvis | 0 (0.0) | 1 (7.1) | NA | NA | |||
| Valgus | 3 (33.3) | 3 (21.4) | NA | NA | |||
| Valgus and arms | 0 (0.0) | 1 (7.1) | NA | NA | |||
| Valgus, arms and pelvis | 1 (11.1) | 0 (0.0) | NA | NA | |||
| SLS non-dominant leg, n(%) | Arms | 2 (22.2) | 3 (21.4) | NA | 0.719 | 0.4 (0.511, 1)✣ | |
| Arms and pelvis | 1 (11.1) | 1 (7.1) | NA | NA | |||
| Nothing | 4 (44.4) | 6 (42.9) | NA | NA | |||
| Pelvis and valgus | 0 (0.0) | 2 (14.3) | NA | NA | |||
| Valgus | 1 (11.1) | 1 (7.1) | NA | NA | |||
| Valgus and arms | 0 (0.0) | 1 (7.1) | NA | NA | |||
| Valgus and pelvis | 1 (11.1) | 0 (0.0) | NA | NA | |||
| Lunge test dominant leg | 12.11±2.98 | 13.64±3.73 | 0.354 | 0.313 | -1.532 (-4.468, 1.405) | -0.442 (-1.341, 0.457)* | |
| Lunge test non-dominant leg | 12.33±2.65 | 13.71±3.22 | 0.451 | 0.296 | -1.381 (-3.955, 1.193) | -0.458 (-1.358, 0.441)* | |
| External rotation dominant leg (º) | 93.11±8.88 | 88.86±8.47 | 0.698 | 0.262 | 4.254 (-3.624, 12.132) | 0.493 (-0.408, 1.394)* | |
| Internal rotation dominant leg (º) | 61.89±10.69 | 49.50±11.04 | 0.884 | 0.01 | 12.389 (2.651, 22.127) | 0.54 (0.16, 0.798)☨ | |
| External rotation non-dominant leg (º) | 92.56±12.95 | 84.93±7.08 | 0.017 | 0.134 | 7.627 (-2.735, 17.989) | 0.783 (-0.137, 1.703)* | |
| Internal rotation non-dominant leg (º) | 60.00±11.18 | 48.00±9.65 | 0.79 | 0.014 | 12 (2.253, 21.747) | 1.166 (0.19, 2.142)* |
Data expressed as mean±standard deviation or with absolute and relative values (%); SLS: Single Leg Squat test; *: Cohen´s D effect size; ☨: non-parametric r effect size; ✣: Cramer´s V effect size.asignificant if p<0.05 (shown in red).
Table 3.
Dominant leg covariable effect over gender.
| Gender | Lunge test dominant leg | F(1)=1.154, p=0.296 | External rotation dominant leg (º) | F(1)=1.23, p=0.281 | External rotation non-dominant leg (º) | F(1)=3.793, p=0.066 | SLS dominant leg | Z=0.438, p=0.661 |
| Dominant leg | F(1)=3.642, p=0.072 | F(1)=0.27, p=0.609 | F(1)=4.157, p=0.056 | Z=-0.299, p=0.765 | ||||
| Gender:Dominant leg | F(1)=0, p=0.987 | F(1)=0.149, p=0.703 | F(1)=0.565, p=0.461 | Z=-0.244, p=0.807 | ||||
| Gender | Lunge test non-dominant leg | F(1)=1.269, p=0.274 | Internal rotation dominant leg (º) | F(1)=7.36, p=0.014 | Internal rotation non-dominant leg (º) | F(1)=7.616, p=0.013 | SLS non-dominant leg | Z=0.008, p=0.993 |
| Dominant leg | F(1)=4.159, p=0.056 | F(1)=2.334, p=0.143 | F(1)=1.161, p=0.295 | Z=1.546, p=0.122 | ||||
| Gender:Dominant leg | F(1)=0.018, p=0.895 | F(1)=0.551, p=0.467 | F(1)=1.903, p=0.185 | Z=-0.009, p=0.993 |
SLS: Single Leg Squat test.asignificant if p<0.05 (shown in red).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



