
Submitted:
19 September 2023
Posted:
21 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The global pandemic of coronavirus disease 2019 (COVID-19) resulted to many deaths from fulminant respiratory failure. Chronic obstructive pulmonary disease (COPD) is the leading cause of morbidity and mortality worldwide. There has been great concern regarding the impact of COPD on COVID-19 illness. Methods: Data from the Philippine CORONA Study were analyzed to determine the association of COPD and COVID-19 in terms of mortality, disease severity, respiratory failure, mechanical ventilation, and lengths of stay in the intensive care unit (ICU) and hospital. The influence of smoking on COVID-19 disease severity and mortality were also reviewed. Results: A total of 10,881 patients were included in the study and 156 (1.4%) patients had been diagnosed with COPD. Majority of COVID-19 patients with COPD had other existing comorbidities: hypertension, diabetes mellitus, chronic cardiac disease, and chronic kidney disease. COPD patients more commonly present with severe or critical COVID-19. COPD patients with COVID-19 were at higher risk to experience in-hospital mortality, respiratory failure, and to be admitted in the ICU. Smokers were more likely to present with higher COVID-19 severity and experience in-hospital mortality. Conclusion: Our study supports that the growing evidence that COPD among COVID-19 patients is a risk for higher mortality, more severe form of COVID-19, higher ICU admission, and higher respiratory failure needing ventilatory support. Smoking increases risk for developing severe COVID-19 and mortality.
Keywords:
COVID-19
; COPD
; smoking
; mortality
; respiratory failure
1. Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been responsible for the global pandemic of coronavirus disease 2019 (COVID-19). This highly transmissible disease can cause a wide range of symptoms from mild viral illness to fulminant respiratory failure and death [1]. As of September 2023, there has been 695,358,466 cases worldwide and 6,915,923 deaths [2].
Multiple descriptive studies have been made regarding the effect of co-morbidities on the severity of COVID 19 disease. At least one co-morbidity is present in 20-51% of COVID-19 patients, including hypertension and diabetes [3]. In the Philippines, the presence of hypertension, diabetes, cancer, higher body mass index, stroke, and dementia all conferred poorer clinical outcomes (increased risk of mortality, respiratory failure, and need for ICU admission) among Filipino COVID-19 patients [4,5,6,7,8,9]. On the other hand, outcome was the same for pregnant and non-pregnant women with COVID-19 [10].
The Global Initiative for Chronic Obstructive Lung Disease in its 2023 document defines chronic obstructive pulmonary disease (COPD) as a heterogeneous lung condition presenting with chronic respiratory symptoms as a result of abnormalities in the airways/or alveoli that lead to persistent, often progressive, airflow limitation [11]. To date, smoking tobacco remains to be the main environmental exposure that leads to the pathology of COPD. COPD is the leading cause of morbidity and mortality worldwide [11].
As COVID-19 is a predominantly respiratory infection, there has been great concern regarding patients with COPD and their susceptibility in acquiring the SARS-CoV-2 virus and risk for developing severe disease. It is an established fact that viral infections can cause COPD exacerbations that can lead to poor clinical outcomes.
Evidence regarding the impact of having COPD as a comorbidity in COVID-19 infection is limited and to date there has been no studies published regarding data on the Philippine population. This study aimed to determine and compare the outcomes of COVID-19 patients with COPD versus those without COPD history in terms of COVID-19 severity, respiratory failure, ICU admission, and length of ICU stay. We also explored the potential influence of smoking among COVID-19 patients in terms of disease severity and mortality.
2. Materials and Methods
Study design, data collection, sampling and definition of cohorts.
We performed an analysis of data of patient with and without physician diagnosis of COPD from a nationwide, multicenter, comparative, retrospective, cohort study involving patients with COVID-19 who were admitted to the hospitals/ major study sites of the Philippine CORONA (COVID-19 Outcomes: a Retrospective study Of Neurological manifestations and Associated symptoms) Study from February 2020 until December 2020 [12]. This was the largest Philippine study of COVID-19 to date involving 10,881 patients. COVID-19 cases were identified from the census of all participating institutions. Pertinent data were obtained through review of the medical records and encoded using electronic data collection form using Epi Info Software (V.7.2.2.16). The data collection process and details of the protocol have been published in 2020 [13]. The original cohort was approved by the individual institutional review and research boards of the hospital sites and the Single Joint Research Ethics Board of the Department of Health of the Philippines (see complete list below).
Outcome variables
In this study, the following effect of COPD on the following outcomes were measured: (a) mortality, (b) severity of COVID-19 (defined as the worst COVID classification of severity throughout the admission: mild-moderate – presence of mild pneumonia or absence of pneumonia; severe – presence of dyspnea, respiratory rate above 30 breaths per minute, oxygen saturations < 93% or more than 50% lung involvement on radiologic imaging within 24-48 hours; critical – presence of respiratory failure, shock or multiorgan dysfunction), (c) respiratory failure defined as use of ventilatory support, (d) intensive care unit (ICU) admission, (e) length of ICU stay, (f) length of hospital stay, and (g) ventilator days for those placed on mechanical ventilation. In this analysis, we also explored the association of smoking with COVID-19 severity and mortality.
Statistical analysis
Baseline characteristics and clinical outcomes of the participants were summarized by descriptive statistics. Numerical variables were described as mean and standard deviation, if the data was normally distributed as assessed by Shapiro-Wilk test for normality, and as median and interquartile range (IQR), if otherwise. Categorical variables were described as count and proportion. These different baseline characteristics and clinical outcomes were compared between the two groups: with COPD and without COPD. Significant difference in the mean/median/mean-rank of the different numerical variables between the two groups were determined by Student’s t test for the variables with normally distributed data, while Mann-Whitney U test was done for non-normally distributed variables. Heterogeneity of the proportions of the different categorical variables between the two groups were determined by chi-square test or Fisher exact test.
The associations between COPD and the different individual ordered, and dichotomous outcome variables of interest were determined by ordinal, and binary logistic regression, respectively. Survival analysis was also done for time-to-event data of mortality, respiratory failure, and admission to the intensive care unit (ICU). The time-to-event were right-censored on time-to-discharge as the exit from the time-at-risk among those who have not experienced the event, i.e., mortality, respiratory failure, or admission to ICU during the hospital stay. The associations between having COPD and the different time-to-event outcome variables of interest were determined by multivariable Cox proportional hazards regression. On the other hand, Poisson regression was done to determine the association between COPD and the lengths of hospital stay, ICU admission, and invasive mechanical ventilation. The Poisson regression model was adjusted for the effect-measure modifier COVID-19 severity at nadir for lengths of hospital, and ICU stay. Association between smoking status and COVID-19 severity at nadir and in-hospital mortality were also determined by binary logistic regression analysis. A cutoff of p-value < 0.05 identifies COPD, and smoking status as significant predictor of the different outcomes of interest. Kaplan-Meier curves were constructed to visualize the survival curves of COPD versus non-COPD patients for the different time-to-event outcome variables.
3. Results
A total of 10,881 patients were included in the study and 156 (1.4%) patients had been diagnosed with COPD. Table 1 presents the clinicodemographic characteristics of patients included in the study. COVID-19 patients with COPD were from the older age group 60 years old and above (78.8%, p < 0.001), predominantly male (84.0%, p < 0.001) and had a significant smoking history (52.5%, p < 0.001). Majority of COVID-19 patients with COPD had other existing co-morbidities. The most common of which are hypertension (66.7%, p < 0.001), diabetes mellitus (39.1%, p < 0.001), chronic cardiac disease (18.6%, p < 0.001) and chronic kidney disease (10.9%, p = 0.004). Many of COVID-19 patient with COPD reported a history of a previous stroke (6.4% p = 0.026) and of neurodegenerative disorders (1.9%, p = 0.025).
COVID-19 patients with COPD presented more often with fever, cough, dyspnea, and sputum production as compared to those without COPD diagnosis. They also tend to present with new onset neurologic symptoms manifesting as altered mental state (8.3%, p = 0.035) or encephalopathy (12.1%, p = 0.001).
The COVID-19 patients with COPD in our study received a higher proportion of COVID-19 treatments namely glucocorticoids (55.8%, p < 0.001), tocilizumab (15.4%, p = 0.011), anti-virals (29.5%, p < 0.001), anti-bacterials (96.2%, p < 0.001), and other therapies (48.1%, p = 0.001) as compared to those without COPD.
Table 2 summarizes the clinical outcomes of COVID-19 patients stratified according to presence of COPD diagnosis. COPD patients more commonly present with severe (38.1%, p < 0.001) or critical (33.6%, p < 0.001) COVID-19 compared to those without COPD. Figure 1 shows the Kaplan-Meier Curves on mortality, development of respiratory failure and ICU admission. Our study showed that COVID-19 patients with COPD have higher rates of in-hospital mortality (Hazard ratio [HR] = 1.52, 95% CI (1.17, 1.97), p = 0.02), increased risk for developing respiratory failure predominantly from acute respiratory distress syndrome (HR = 2.90, 95% CI (2.24, 3.76), p < 0.001), and greater ICU admission rates (HR = 2.56, 95% CI (3.56, 4.17), p < 0.001), These suggests that COPD is a significant risk factor for mortality, development of respiratory failure and ICU admission for COVID-19 patients.
On further analysis however, there was no sufficient evidence to conclude any significant difference in time to development of respiratory failure, duration of mechanical ventilation, time to ICU admission, and length of ICU stay between COPD and non-COPD patients.
The association of having COPD diagnosis with different outcomes of interest in COVID-19 is shown in Table 3. Our COPD patients with COVID-19 were 4.36 times more likely to present as severe to critical COVID. They were also 3.4 times more likely to experience in-hospital mortality, 3.6 times more likely to have respiratory failure during the course of their admission and have 4.4 times more likely to be admitted in the ICU. COPD COVID-19 patients have been found to also have 19% decreased odds of full/partial neurological improvement as compared to patients without COPD.
The association of smoking history to different outcomes of treatment is shown in Table 4. COVID-19 patient who are smokers are 1.8 times more likely to present with higher COVID-19 severity and 1.9 times more likely to experience in-hospital mortality than those who are never smokers.
4. Discussion
Our study showed a small proportion of admitted COVID-19 patients had COPD diagnosis (1.4%). This however does not mean that COPD patients are at lower risk for contracting the disease. The cases in this study were during the early part of the pandemic when COVID-19 restrictions on mobility were heightened. Many of the COPD patients have been shielded from potential COVID-19 exposures because of these measures. The propensity to acquire COVID-19 among COPD patients in various studies have been confounded by these as well.
The manifestations of COPD exacerbation and COVID-19 among COPD patients may be difficult to distinguish. A high index of suspicion and vigilance is recommended to ensure early diagnosis and access to life saving COVID-19 treatment modalities.
Our study highlighted that COPD patients who get admitted for COVID-19 have 3.4 times increased mortality and are 4.3 times likely to experience a severe or critical form of the disease ventilatory support. Our study also showed increased health care utilization among COPD patients with COVID-19: 4.4 times likelihood of ICU admission, anti-inflammatory therapy (steroids and tocilizumab), antiviral, and antibacterial use. Furthermore, our study showed that COPD patients with COVID-19 have a higher incidence of neurologic symptoms and poor neurologic recovery. Smoking also increased the likelihood of a more severe COVID-19 disease and higher in-patient mortality. These associations of COPD and smoking among COVID-19 patients are similar to all other meta-analysis and cohorts from various countries [14,15,16].
The reason behind the poor outcomes of COVID-19 among COPD patients continues to be investigated. Multiple factors have been postulated. First, COPD patients and smokers may have the predisposition for acquiring SARS-CoV-2 infection. Studies have demonstrated that the gene expression for ACE-2 in bronchial epithelial cells from COPD patients is significantly elevated compared to control subjects [17]. The overexpression of the virus receptor could allow faster spread of the virus into the distal airways and alveoli, facilitating progression from to a more severe COVID-19 pneumonia [18].
Another potential reason is that COPD patients have poor lung function due to small airway disease and emphysema and thus have poor respiratory functional reserve to cope with intrapulmonary shunting during superimposed COVID-19 pneumonia or pulmonary vascular thromboembolic events observed in COVID-19 [15]. This increased intrapulmonary shunting was associated with worse outcome, including mortality [19].
There are impaired innate immune responses to viruses in COPD as well. An example is the finding of defective interferon responses to SARS-CoV-2 being linked to increased risk of severe COVID-19 [16]. It has been established that COPD patients have colonizing pathogenic bacteria in the airways during the stable state, which cause secondary bacterial infections following respiratory viral infections. Secondary bacterial infection is common among COVID-19 patients, causing worse outcomes. This may be due to dampened antimicrobial responses during viral infections including reduced bacterial phagocytosis by alveolar macrophages and reduces antimicrobial peptide release [20].
One other explanation for the poor outcomes was the presence of metabolic comorbidities, which was associated with more severe COVID-19 [4,5,6,7,8,9,16]. This was also seen in our patients.
Our study had several limitations. Our data collection did not differentiate different types of ventilatory support like invasive ventilation, high flow nasal oxygen therapy, and non-invasive ventilation. As the diagnosis of COPD was based on history, there was no data on COPD severity, use of maintenance medication and adherence as well as lung function. These details may provide further insight into which subset or phenotype of COPD may have a poorer prognosis for COVID-19. Furthermore, our data on smoking did not differentiate current from previous smokers. It is interesting to know if smoking cessation have impact on COVID-19 severity as well. We therefore recommend to interested researchers to include these data on future research endeavors.
5. Conclusions
This study on Filipino patients with COVID-19 supports that the growing evidence that COPD patients developing COVID-19 are at higher risk mortality, at having severe and critical forms of COVID-19, at higher likelihood of needing ICU admission and higher chances of developing respiratory failure needing ventilatory support. Smoking increases risk for developing severe COVID-19 and mortality.
Author Contributions
Conceptualization, R.D.G.J, M.C.C.S, A.I.E. and V.M.M.A.; data curation M.C.C.S.; formal analysis, E.Q.V.; interpretation of data, E.Q.V.; writing-original draft, A.B.A., M.B.D.F.D.; writing-review, R.D.G.J., A.B.A., M.B.D.F.D.; editing, R.D.G.J., A.I.E., V.M.M.A.; study supervision, R.D.G.J., M.C.C.S., A.I.E., V.M.M.A and final approval of the version to be published, R.D.G.J, A.B.A., M.B.D.F.D., M.C.C.S, E.Q.V., A.I.E. and V.M.M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Our protocol was approved and endorsed by the local institutional review boards (code): Asian Hospital and Medical Center, Muntinlupa City (2020-010-A); Baguio General Hospital and Medical Center, Baguio City (BGHMC-ERC-2020–13); Cagayan Valley Medical Center, Tuguegarao City (2020–314-01 SJREB); Capitol Medical Center, Quezon City; Cardinal Santos Medical Center, San Juan City (CSMC REC 2020–020); Chong Hua Hospital, Cebu City (IRB 2420–04); De La Salle Medical and Health Sciences Institute, Cavite (2020–23-02-A); Dr. Jose N. Rodriguez Memorial and Sanitarium Hospital, Caloocan City (2020–314-01 SJREB); East Avenue Medical Center, Quezon City (EAMC IERB 2020-38); Jose B. Lingad Memorial Regional Hospital, City of San Fernando, Pampanga (2020–314-01 SJREB); Jose R. Reyes Memorial Medical Center, Manila (2020–314-01 SJREB); Lung Center of the Philippines, Quezon City (LCP-CT-010–2020); Makati Medical Center, Makati City (MMC IRB 2020–054); Manila Doctors Hospital, Manila (MDH IRB 2020–006); Medical Center Manila, Manila (MMERC 2020–09); Northern Mindanao Medical Center, Cagayan de Oro City (025–2020); Quirino Memorial Medical Center, Quezon City (QMMC REB GCS 2020–28); Ospital ng Makati, Makati City (2020–314-01 SJREB); Philippine General Hospital, Manila (2020–314-01 SJREB); Philippine Heart Center, Quezon City (2020–314-01 SJREB); Research Institute for Tropical Medicine, Muntinlupa City (RITM IRB 2020–16); San Lazaro Hospital, Manila (2020–314-01 SJREB); San Juan De Dios Educational Foundation Inc. Hospital, Pasay City (SJRIB 2020–0006); Single Joint Research Ethics Board of the DOH, Philippines (SJREB-2020–24); Southern Isabela Medical Center, Santiago City (2020–03); Southern Philippines Medical Center, Davao City (P20062001); St. Luke’s Medical Center, Quezon City (SL-20116); St. Luke’s Medical Center, Bonifacio Global City, Taguig City (SL-20116); The Medical City, Pasig City; University of Santo Tomas Hospital, Manila (UST-REC-2020–04-071-MD); University of the East Ramon Magsaysay Memorial Medical Center, Inc., Quezon City (0835/E/2020/063); Veterans Memorial Medical Center, Quezon City (VMMC-2020–025), and Vicente Sotto Memorial Medical Center, Cebu City (VSMMC-REC-O-2020–048).
Informed Consent Statement
Acquiring informed consent was not needed for this study since the design was a retrospective cohort study employing medical chart review and the data obtained for this study were completely anonymized.
Data Availability Statement
Anonymized data not published within this article will be made available by request from any qualified investigator.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID 19) Dashboard. Available online: https://www.worldometers.info/coronavirus/. (Accessed on 16 September 2023).
- Song, J.; Zeng, M.; Wang, H.; Qin, C.; Hou, H.Y.; Sun, Z.Y.; Xu, S.P.; Wang, G.P.; Guo, C.L.; Deng, Y.K.; Wang, Z.C.; Ma, J.; Pan, L.; Liao, B.; Du, Z.H.; Feng, Q.M.; Liu, Y.; Xie, J.G.; Liu, Z. Distinct effects of asthma and COPD comorbidity on disease expression and outcome in patients with COVID-19. Allergy. 2021, 76, 483–496. [Google Scholar] [CrossRef]
- Espiritu, A.I.; Sucaldito, M.S.F.P.; Ona, D.I.D.; Apor, A.D.A.O.; Sy, M.C.C.; Anlacan, V.M.M.; Jamora, R.D.G. Clinical outcomes in COVID-19 among patients with hypertension in the Philippine CORONA Study. Eur J Med Res 2023, 28, 62. [Google Scholar] [CrossRef]
- Anlacan, V.M.M.; Piamonte, B.L.C.; Sy, M.C.C.; Villanueva, E.Q.; Jamora, R.D.G.; Espiritu, A.I. Clinical outcomes of older persons and persons with dementia admitted for coronavirus disease 2019: findings from the Philippine CORONA Study. Dement Geriatr Cogn Disord 2022, 51, 485–498. [Google Scholar] [CrossRef] [PubMed]
- Jamora, R.D.G.; Prado, M.B.; Anlacan, V.M.M.; Sy, M.C.C.; Espiritu, A.I. Incidence and risk factors for stroke in patients with COVID-19 in the Philippines: an analysis of 10,881 cases. J Stroke Cerebrovasc Dis. 2022, 31, 106776. [Google Scholar] [CrossRef] [PubMed]
- Espiritu, A.I.; Reyes, N.G.D.; Leochico, C.F.D.; Villanueva, E.Q.; Anlacan, V.M.M.; Jamora, R.D.G. Body mass index and its association with COVID-19 clinical outcomes: findings from the Philippine CORONA Study. Clin Nutr ESPEN. 2022, 49, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Espiritu, A.I.; Larrazabal, R.B.; Sy, M.C.C.; Villanueva, E.Q.; Anlacan, V.M.M.; Jamora, R.D. Outcomes and risk factors of patients with COVID-19 and cancer (ONCORONA): findings from the Philippine CORONA Study. Front Oncol. 2022, 12, 857076. [Google Scholar] [CrossRef] [PubMed]
- Espiritu, A.I.; Chiu, H.H.C.; Sy, M.C.C.; Anlacan, V.M.M.; The Philippine CORONA Study Group, Jamora, R. D.G. The outcomes of patients with diabetes mellitus in The Philippine CORONA Study. Sci Rep. 2021, 11, 24436. [Google Scholar] [CrossRef] [PubMed]
- Espiritu, A.I.; Bravo, S.L.R.; Sombilla, H.A.A.; Tantengco, O.A.G.; Sy, M.C.C.; Sy, A.D.R.; Anlacan, V.M.M.; Jamora, R.D.G. Clinical outcomes of COVID-19 infection in pregnant and non-pregnant women: results from The Philippine CORONA Study. Vaccines 2023, 11, 226. [Google Scholar] [CrossRef] [PubMed]
- Global initiative for chronic obstructive lung disease. Global strategy for prevention, diagnosis and management of COPD: 2023 report. Available online: https://goldcopd.org. (Accessed on 1 May 2023).
- Espiritu, A.I.; Sy, M.C.C.; Anlacan, V.M.M.; Jamora, R.D.G.; Philippine CORONA Study Group, Investigators. COVID-19 Outcomes of 10,881 patients: Retrospective study Of Neurological symptoms and Associated manifestations (Philippine CORONA Study). J Neural Trans (Vienna) 2021, 128, 1687–1703. [Google Scholar] [CrossRef] [PubMed]
- Espiritu, A.I.; Sy, M.C.C.; Anlacan, V.M.M.; Jamora, R.D.G. The Philippine COVID-19 Outcomes: a Retrospective study Of Neurological manifestations and Associated symptoms (The Philippine CORONA Study): a protocol study. BMJ Open. 2020, 10, e040944. [Google Scholar] [CrossRef] [PubMed]
- Uruma, Y.; Manabe, T.; Fujikura, Y.; Iikura, M.; Hojo, M.; Kudo, K. Effect of asthma, COPD, and ACO on COVID-19: a systematic review and meta-analysis. PloS One. 2022, 17, e0276774. [Google Scholar] [CrossRef] [PubMed]
- Gerayeli, F.V.; Milne, S.; Cheung, C.; Li, X.; Yang, C.W.T.; Tam, A.; Choi, L.H. ; Bae A; Sin D.D. COPD and the risk of poor outcomes in COVID-19: a systematic review and meta-analysis. EClinicalMedicine. 2021, 33, 100789. [Google Scholar]
- Bonato, M.; Semenzato, U.; Tinè, M.; Bazzan, M.; Damin, M.; Biondini, D.; Casara, A.; Romagnoli, M.; Turato, G.; Cosio, M.G.; Saetta M., Baraldo, S. Risk factors for development and severity of COVID-19 in COPD patients. Front Med (Lausanne) 2021, 8, 714570. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.M.; Niikura, M.; Yang, C.W.; Sin, D.D. COVID-19 and COPD. Eur Respir J. 2020, 56, 2002108. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.M.; Yang, C.X.; Tam, A.; Shaipanich, T.; Hackett, T.L.; Singhera, G.K.; Dorscheid, D.R.; Sin, D.D. ACE-2 expression in the small airway epithelia of smokers and COPD patients: implications for COVID-19. Eur Respir J. 2020, 55, 2000688. [Google Scholar] [CrossRef] [PubMed]
- Kotwica, A.; Knights, H.; Mayor, N.; Russell-Jones, E.; Dassios, T.; Russell-Jones, D. Intrapulmonary shunt measured by bedside pulse oximetry predicts worse outcomes in severe COVID-19. Eur Respir J 2021, 57, 2003841. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Mathioudakis, A.G.; Higham, A. Chronic obstructive pulmonary disease and COVID-19: interrelationships. Curr Opin Pulm Med. 2022, 28, 76–83. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Comparison of Kaplan-Meier curves of (A) in-hospital mortality, (B) respiratory failure, and (C) ICU admission, between COPD and non-COPD COVID-19 patients.
Figure 1.
Comparison of Kaplan-Meier curves of (A) in-hospital mortality, (B) respiratory failure, and (C) ICU admission, between COPD and non-COPD COVID-19 patients.
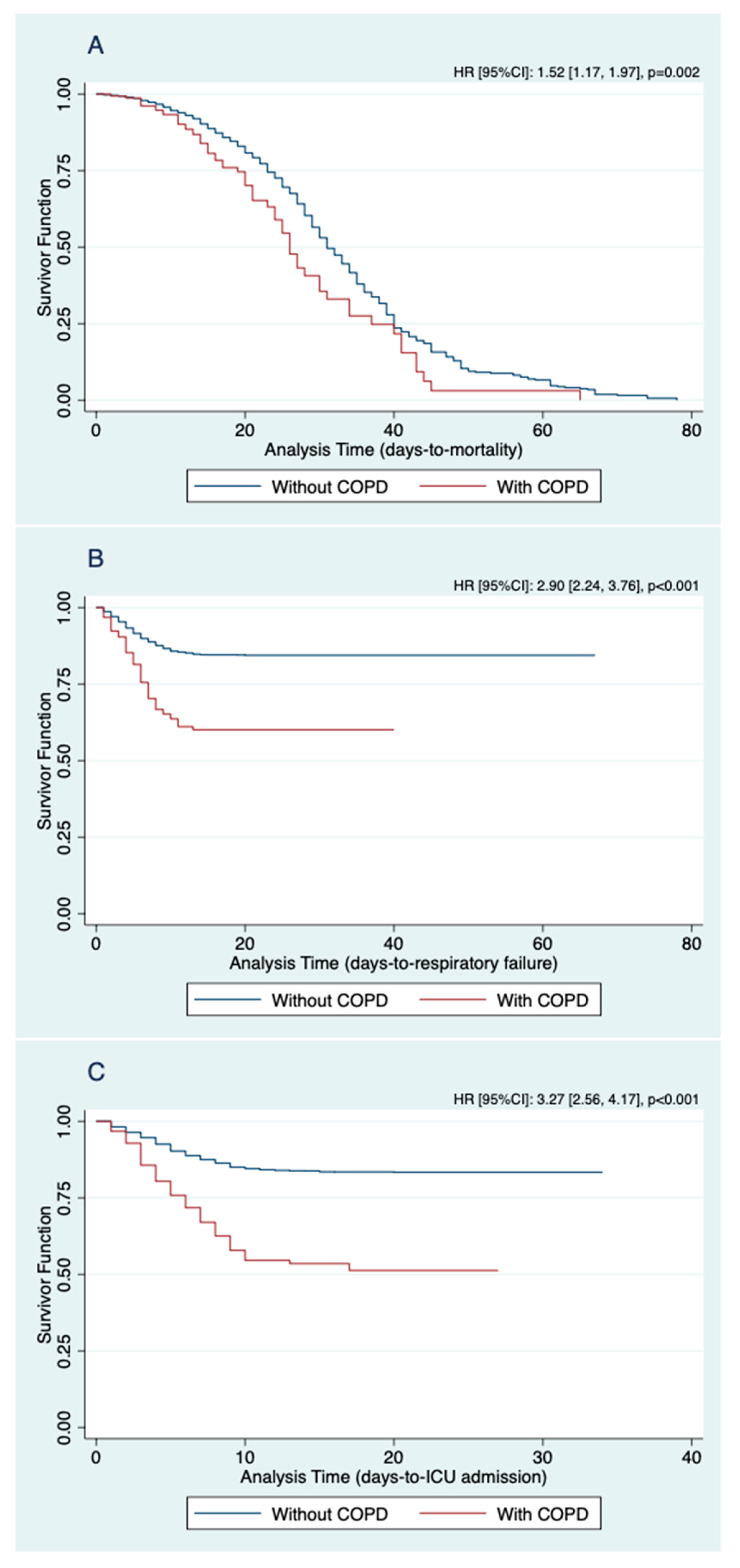

Table 1.
Clinicodemographic characteristics of the stratified according to having COPD.
| Features | All patients | With COPD | Without COPD |
p value |
|---|---|---|---|---|
| (n = 10,881) | (n = 156) | (n = 10,725) | ||
| Socio-demographic data | ||||
| Age group | <0.001 | |||
| 19 – 59 y, n (%) | 7047 (64.7) | 33 (21.2%) | 7014 (65.4%) | |
| ≥ 60 y, n (%) | 3834 (35.2%) | 123 (78.8%) | 3711 (34.6%) | |
| Female, n (%) | 5099 (46.9%) | 25 (16.0%) | 5074 (47.3%) | <0.001 |
| Ever-smoker (past/ current), n (%) | 1026 (9.4%) | 82 (52.5%) | 944 (8.8%) | <0.001 |
| Non-neurologic comorbidities, n (%) | ||||
| Hypertension | 3647 (33.5%) | 104 (66.7%) | 3543 (33.0%) | <0.001 |
| Diabetes mellitus | 2191 (20.1%) | 61 (39.1%) | 2130 (19.8%) | <0.001 |
| Chronic cardiac diseasea | 512 (4.7%) | 29 (18.6%) | 483 (4.5%) | <0.001 |
| Chronic kidney disease | 611 (5.6%) | 17 (10.9%) | 594 (5.5%) | 0.004 |
| Chronic liver disease | 60 (0.6%) | 2 (1.2%) | 58 (0.5%) | 0.212 |
| Malignancy | 244 (2.2%) | 4 (2.5%) | 240 (2.2%) | 0.781 |
| HIV/ AIDS | 37 (0.3%) | - | 37 (0.3%) | 1.000 |
| Past neurologic history, n (%) | ||||
| Stroke/ cerebrovascular | 321 (3.0%) | 10 (6.4%) | 311 (2.9%) | 0.026 |
| Epilepsy | 27 (0.3%) | - | 27 (0.3%) | 1.000 |
| Neurodegenerativeb | 44 (0.4%) | 3 (1.9%) | 41 (0.4%) | 0.025 |
| Headache syndrome | 5 (0.1%) | - | 5 (0.1%) | 1.000 |
| Demyelinating disorder | 2 (0.0%) | - | 2 (0.0%) | 1.000 |
| Central nervous system infection | 5 (0.1%) | - | 5 (0.1%) | 1.000 |
| Peripheral nervous system disordersc | 15 (0.1%) | - | 15 (0.1%) | 1.000 |
| Respiratory and constitutional symptoms, n (%) | ||||
| Fever | 3927 (36.1%) | 80 (51.2%) | 3847 (35.9%) | <0.001 |
| Cough | 4411 (40.5%) | 114 (73.1%) | 4297 (40.1%) | <0.001 |
| Dyspnea | 2703 (24.8%) | 106 (67.9%) | 2597 (24.2%) | <0.001 |
| Rhinorrhea | 607 (5.6%) | 6 (3.9%) | 601 (5.6%) | 0.342 |
| Sputum production | 637 (5.9%) | 23 (14.7%) | 614 (5.7%) | <0.001 |
| Sore throat | 751 (6.9%) | 9 (5.8%) | 742 (6.9%) | 0.574 |
| Diarrhea | 597 (5.5%) | 5 (3.2%) | 592 (5.5%) | 0.208 |
| Fatigue | 713 (6.6%) | 15 (9.6%) | 698 (6.5%) | 0.119 |
| Others | 1674 (15.3%) | 16 (10.2%) | 1658 (15.4%) | 0.074 |
| New onset neurological symptoms, n (%) | ||||
| Headache | 607 (5.6%) | 5 (3.2%) | 602 (5.6%) | 0.193 |
| Nausea or vomiting | 158 (1.5%) | 2 (1.3%) | 156 (1.5%) | 1.000 |
| Seizure | 96 (0.9%) | 1 (0.6%) | 95 (0.9%) | 1.000 |
| Altered mental stated | 518 (4.7%) | 13 (8.3%) | 505 (4.7%) | 0.035 |
| Olfactory or taste dysfunction | 663 (6.1%) | 6 (3.9%) | 657 (6.1%) | 0.237 |
| Dysfunctions of other sensese | 166 (1.5%) | 1 (0.6%) | 165 (1.5%) | 0.735 |
| Bulbar symptomsf | 122 (1.1%) | 2 (1.3%) | 120 (1.1%) | 0.695 |
| Motor symptoms | 246 (2.2%) | 5 (3.2%) | 241 (2.3%) | 0.406 |
| Sensory symptoms | 53 (0.5%) | 1 (0.6%) | 52 (0.4%) | 0.536 |
| Myalgia | 256 (2.4%) | 6 (3.9%) | 250 (2.3%) | 0.186 |
| Othersg | 33 (0.3%) | 1 (0.6%) | 32 (0.3%) | 0.380 |
| New-onset neurological disorders/ complications, n (%) | ||||
| Encephalopathyh | 644 (5.9%) | 19 (12.1%) | 625 (5.8%) | 0.001 |
| Symptomatic seizure/ status epilepticus | 125 (1.2%) | 1 (0.6%) | 124 (1.1%) | 1.000 |
| Stroke/ cerebrovasculari | 367 (3.4%) | 9 (5.8%) | 358 (3.3%) | 0.095 |
| Central nervous system infectionj | 7 (0.07%) | - | 7 (0.07%) | 1.000 |
| Othersk | 14 (0.1%) | - | 14 (0.1%) | 1.000 |
| Treatment/s received, n (%) | ||||
| Glucocorticoids | 2844 (26.1%) | 87 (55.8%) | 2757 (25.7%) | <0.001 |
| Tocilizumab | 1029 (9.5%) | 24 (15.3%) | 1005 (9.4%) | 0.011 |
| Antivirall | 1902 (17.4%) | 46 (29.5%) | 1856 (17.3%) | <0.001 |
| Antibacterial | 9014 (82.8%) | 150 (96.2%) | 8864 (82.7%) | <0.001 |
| Othersm | 3905 (35.9%) | 75 (48.1%) | 3830 (35.7%) | 0.001 |
| aIncludes heart failure, coronary artery disease, prior history of myocardial infarction, and other cardiac conditions | ||||
| bIncludes dementia, and movement disorders | ||||
| cIncludes peripheral nerve disease, neuromuscular junction disorder, and muscle disorder | ||||
| dIncludes altered sensorium, and confusion | ||||
| eIncludes visual, hearing, and vestibular dysfunctions | ||||
| fIncludes facial paresthesia, facial weakness, dysarthria, dysphonia, dysphagia, tongue weakness, and neck weakness | ||||
| gIncludes tremor, dystonia, choreoathetosis, bradykinesia, ataxia, and meningisimus | ||||
| hIncludes encephalopathy and anoxic brain injury | ||||
| iAny acute cerebrovascular disease (no need to distinguish between infarction, hemorrhagic) | ||||
| jIncludes encephalitis, meningitis, and meningoencephalitis | ||||
| kIncludes acute disseminated encephalomyelitis, optic neuritis, sensory ganglionitis, radiculitis, anterior horn syndrome, peripheral neuritis (Guillain Barre Syndrome, other than Guillain Barre Syndrome), neuromuscular disorder, and myositis | ||||
| lIncludes remdesivir, lopinavir, and ritonavir | ||||
| mIncludes chloroquine, hydroxychloroquine, convalescent plasma, and other therapies | ||||
| COPD – Chronic obstructive pulmonary disease; HIV/ AIDS – Human immunodeficiency virus/ Acquired immunodeficiency syndrome | ||||
Table 2.
Clinical outcomes of COVID-19 patients stratified according to COPD.
| Outcomes | All patients | With COPD | Without COPD | p value |
|---|---|---|---|---|
| (n = 10,881) | (n = 156) | (n = 10,725) | ||
| COVID-19 severity at nadir | <0.001 | |||
| Mild/ moderate, n (%) | 6690 (62.2%) | 43 (28.3%) | 6647 (62.7%) | |
| Severe, n (%) | 2354 (21.9%) | 58 (38.1%) | 2296 (21.7%) | |
| Critical, n (%) | 1707 (15.9%) | 51 (33.6%) | 1656 (15.6%) | |
| In-hospital mortality | 1702 (15.6%) | 60 (38.4%) | 1642 (15.3%) | <0.001 |
| Time to in-hospital mortality in days, median (IQR; range) | 15 (13; 1 to 78) | 20 (15.5; 2 to 65) | 15 (13; 1 to 78) | 0.004 |
| Respiratory failure, n (%) | 1608 (14.7%) | 59 (37.8%) | 1549 (14.4%) | <0.001 |
| Cause/sa | ||||
| Pneumonia | 891 (55.4%) | 30 (50.9%) | 861 (55.6%) | 0.472 |
| Acute respiratory distress syndrome | 845 (52.6%) | 43 (72.8%) | 802 (51.7%) | 0.001 |
| Shock | 140 (8.7%) | 3 (5.1%) | 137 (8.8%) | 0.315 |
| Central neurologic cause | 86 (5.4%) | 1 (1.7%) | 85 (5.5%) | 0.368 |
| Pulmonary edema | 32 (2.0%) | 1 (1.7%) | 31 (2.0%) | 1.000 |
| Pulmonary embolism | 19 (1.1%) | 2 (3.4%) | 17 (1.1%) | 0.152 |
| Time to respiratory failure in days, median (IQR; range) | 5 (4; 0 to 20) | 6 (4; 1 to 13) | 5 (4; 0 to 20) | 0.342 |
| Duration of invasive mechanical venticlation in days, median (IQR; range) | 13 (12; 0 to 75) | 15 (14; 1 to 62) | 13 (12; 0 to 75) | 0.150 |
| Admitted to ICU, n (%) | 1740 (15.99%) | 70 (44.87%) | 1670 (15.57%) | <0.001 |
| Time to ICU admission in days, median (IQR; range) | 5 (4; 0 to 20) | 5 (5; 0 to 17) | 5 (4; 0 to 20) | 0.290 |
| Length of ICU stay in days, median (IQR; range) | 15 (11; 0 to 77) | 15 (14; 1 to 64) | 15 (11; 0 to 77) | 0.923 |
| Length of hospital stayb in days, median (IQR; range) | 13 (9; 1 to 78) | 14 (10; 2 to 65) | 13 (9; 1 to 78) | 0.003 |
| Neurologic deficits, n (%) | 2291 (21.0%) | 35 (22.4%) | 2256 (21.0%) | 0.670 |
| Neurologic outcomec | <0.001 | |||
| Full/ partial improvement of neurologic deficits, n (%) | 1639 (88.0%) | 12 (57.1%) | 1627 (86.3%) | |
| No improvement of neurologic deficits, n (%) | 266 (13.9%) | 9 (42.8%) | 257 (13.6%) | |
| aNon-mutually exclusive | ||||
| bDerived from overall length of stay for patients who were never admitted to the ICU; excludes length of ICU stay for those who were admitted in the ICU | ||||
| cPatients with recorded data for neurologic outcome (n = 1905) | ||||
| COPD – Chronic obstructive pulmonary disease; COVID-19 – Coronavirus disease 2019; IQR – Interquartile range; ICU – intensive care unit | ||||
Table 3.
Association of having a COPD with the different outcomes of interest.
| Outcomes | Estimatea | 95% Confidence Interval | p value |
|---|---|---|---|
| Dichotomous outcomes | |||
| Severe/ critical COVID-19 at nadirb | 4.26 | 2.99, 6.08 | <0.001 |
| Neurologic deficit/s | 1.09 | 0.74, 1.59 | 0.670 |
| Full/ partial improvement of neurologic deficit/s | 0.21 | 0.09, 0.50 | <0.001 |
| In-hospital mortality | 3.46 | 2.49, 4.79 | <0.001 |
| Respiratory failure | 3.60 | 2.60, 5.00 | <0.001 |
| ICU admission | 4.41 | 3.21, 6.08 | <0.001 |
| Time-to-event outcomes | |||
| In-hospital mortality | 1.52 | 1.17, 1.97 | 0.002 |
| Respiratory failure | 2.90 | 2.24, 3.76 | <0.001 |
| ICU admission | 3.27 | 2.56, 4.17 | <0.001 |
| Count outcomes | |||
| Days of invasive mechanical ventilation | 1.15 | 1.08, 1.22 | <0.001 |
| Days of ICU stay | |||
| Among mild/ moderate COVID-19 | 0.88 | 0.65, 1.21 | 0.435 |
| Among severe COVID-19 | 1.02 | 0.92, 1.13 | 0.688 |
| Among critical COVID-19 | 1.04 | 0.97, 1.12 | 0.273 |
| Days of hospital stay | |||
| Among mild/ moderate COVID-19 | 0.98 | 0.91, 1.06 | 0.656 |
| Among severe COVID-19 | 1.17 | 1.10, 1.23 | <0.001 |
| Among critical COVID-19 | 1.15 | 1.08, 1.22 | <0.001 |
| a Odds ratio for ordered and dichotomous outcomes, hazard ratio for time-to-event outcomes, and incidence rate ratio for count outcomes | |||
| b Dichotomized to mild/moderate, and severe/critical, due to violation of the proportional odds assumption of ordinal logistic regression for the three-level severity, i.e., mild/moderate, severe, and critical | |||
| COPD – Chronic obstructive pulmonary disease; COVID-19 – Coronavirus disease 2019; ICU – Intensive care unit | |||
Table 4.
Association of being an ever-smoker with the different outcomes of interest.
| Outcomes | Odds Ratio | 95% Confidence Interval | p value |
|---|---|---|---|
| COVID-19 severity at nadira | 1.78 | 1.58, 2.01 | <0.001 |
| In-hospital mortalityb | 1.90 | 1.63, 2.21 | <0.001 |
| a Ordered outcomes: mild/ moderate, severe, and critical | |||
| b Dichotomous outcomes: in-hospital mortality and discharged | |||
| COVID-19 – Coronavirus disease 2019; IQR – Interquartile range | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



