
Submitted:
20 September 2023
Posted:
21 September 2023
You are already at the latest version
Abstract
The association between depressive symptomatology and cognitive decline has been examined using the Centre for Epidemiologic Studies-Depression Scale (CES-D), however, concerns have been raised about this self-report measure. Here, we examined how the CES-D total score from the 14- and 10-item versions compared to the 20-item version in predicting progression to cognitive decline from a cognitively unimpaired baseline. Data from 1,054 participants were analysed using ordinal logistic regression, alongside moderator and receiver-operating characteristics curve analyses. All baseline total scores significantly predicted progression to cognitive decline. The 14-item version was better than the 20-item version in predicting consensus diagnosis, as shown by their AICs, while also showing the highest accuracy when discriminating between participants by diagnosis at last visit. We did not find sex to moderate the relationship between CES-D score and cognitive decline. Current findings suggest the 10- and 14-item versions of the CES-D are comparable to the 20-item version, and that the 14-item version may be better at predicting longitudinal consensus diagnosis compared to the 20-item version.
Keywords:
depression
; CES-D
; cognitive decline
; MCI
; aging
1. Introduction
Depression is one of the most frequently reported psychiatric disorders in older adults (American Psychological Association, 2013), and has been found to affect up to 50% of people living with Alzheimer’s disease (AD) dementia (Diniz et al., 2013; Lyketsos et al., 2002). Depressive symptomatology has been found to be associated with cognitive decline in elderly individuals (e.g., Chodosh et al., 2007; Fuhrer et al., 1992; Gonzalez et al., 2008; Kim et al., 2019; Raji et al., 2007; Wilson et al., 2002; 2004; Yaffe et al., 1999; Zahodne et al., 2014). Depressive symptoms have also been shown to be associated with greater risk of developing mild cognitive impairment (MCI; e.g., Barnes et al., 2006; Geda et al., 2006), AD, or dementia in older adults (e.g., Devanand et al., 1996; Gatz et al., 2005; Jorm et al., 1991; 2001; Kim et al., 2021a; Saczynsk et al., 2010; Wilson et al., 2002). However, contradictory findings indicating these symptoms do not significantly increase risk of cognitive decline (e.g., Chodosh et al., 2010; Dufouil et al., 1996; Ganguli et al., 2006; Henderson et al., 1997) or dementia (e.g., Chen et al., 1999; Becker et al., 2009) have also been reported. Various factors might contribute to the disparity in results, including participants’ age, duration of follow-up, and methods used to diagnose AD or to assess depressive symptoms (Saczynsk et al., 2010). Overall, most studies support this association (for a review, see Byers & Yaffe, 2011), although the nature of the relationship remains unclear (Kim et al., 2021b).
One of the most popular screening tools for depressive symptomatology is the Centre for Epidemiologic Studies-Depression Scale (CES-D; Radloff, 1977). Although the CES-D is comparable to the Beck Depression Inventories (Beck et al., 1961; 1996), and it is widely used in clinical and research studies (Carleton et al., 2013), it has been described as too long (Kohout et al., 1993) or challenging (Cheng & Chan, 2008) when used in certain populations (Gonzalez et al., 2017), such as in people with cognitive impairment or with poorer literacy. The item content of the original 20-item CES-D has also been questioned, as certain items have been found to perform differently depending on sex, age, health, cultural and/or social differences (Carleton et al., 2013; Carter et al., 2016). Items related to social issues, such as, ‘People were unfriendly’’ and ‘‘I felt that people disliked me’’, could be measuring other constructs, such as perceived social skills, and symptoms of interpersonal disorders (Carleton et al., 2013; Kohout et al., 1993; Shafer, 2006; Stansbury et al., 2006; Williams et al., 2007). Items referring to somatic physical symptoms, “I felt that everything I did was an effort”, could misrepresent depressive symptoms in older individuals (Carleton et al., 2013; Snarski & Scogin, 2006) or in those with chronic pain (Carleton et al., 2013; Ohayon & Schatzberg, 2003). Moreover, responses to item number 17, ‘‘I had crying spells’’, have been shown to vary with sex, resulting in an increase in total score in women (Cole et al., 2000; Rivera-Medina et al., 2010), causing an overestimation of depressive symptoms in women and an underestimation in men (Carleton et al., 2013). In a study by Carleton et al. (2013), confirmatory factor analyses were conducted to compare previous and new models of the CES-D and results supported a 14-item, 3-factor model, comprising somatic symptoms, negative affect, and anhedonia; the authors argue the 14-item version (CESD-14) is more consistent with current diagnostic criteria for depression. Also, a 10-item version (CESD-10) is used in clinical and research settings, in which redundant items are removed (Andresen et al., 1994), and the focus is on affective symptoms by reducing somatic items (Cheng & Chan, 2005).
Although CESD-10 and CESD-14 have been used and validated in previous studies (e.g., Carleton et al., 2017; Harenberg et al., 2015; Irwin et al., 1999; Mason et al., 2019), to our knowledge, it is yet unclear how the 10-item and 14-item versions compare to the 20-item version in predicting progression from a cognitively unimpaired baseline to a clinically-diagnosed impaired status in older adults.
The aims of this study were to determine if baseline total CES-D scores were associated with progression to cognitive decline from a cognitively unimpaired baseline, and to examine how the CES-D total score from the 14- and 10-item versions compared to the 20-item version in predicting progression. We tested if the risk of progression differed by sex by conducting a moderator analysis, while also comparing the three CES-D versions. Finally, we examined how the CES-D total score from the 14- and 10-item versions compared to the 20-item version in differentiating between participants who remained cognitively unimpaired stable and those who had cognitively declined at last follow-up visit. We predicted that baseline total CES-D scores would be associated with progression to cognitive decline, that the 14- and 10-item total scores would be better predictors and discriminators than the original 20-item version, and that the risk of progression would differ between males and females.
2. Methods
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study. This study was not preregistered.
2.1. Participants
The Wisconsin Registry for Alzheimer’s Prevention (WRAP) study is an ongoing longitudinal cohort study based at the University of Wisconsin–Madison, USA, of older adults who attend regular visits, the first follow-up occurs at least after 4 years and then every 2 years (for details, see Johnson et al., 2017; Sager et al., 2005). Participants were classified after each study visit as cognitively unimpaired—stable (CUS), cognitively unimpaired—declining (CUD), MCI, or Dementia, via a consensus conference diagnosis (as described in Langhough Koscik et al., 2021 and in Procedure). For the present study, participants were selected based on having completed at least two visits with item-level CES-D data, being classified as CUS at CES-D baseline, and either being classified as still cognitively unimpaired (stable or declining), with MCI, or Dementia at their last visit. From the total pool of 1,670 participants, 1,054 participants fulfilled the above inclusion criteria: 1,019 were native English speakers, eight Spanish native speakers, nine other languages (unspecified) and 18 did not report their native language; seven participants reported their race as American Indian or Native American, two as Asian, 26 as Black or African American, 10 as Spanish or Hispanic, 1,008 as White and one as unknown. Item-level data availability for the CES-D began at visit 2, which was considered baseline for these analyses. At their last visit, from the same participants, 952 individuals were classified as CUS, 79 as CUD, 19 as MCI and four as dementia. All activities for this study were approved by the institutional review board of the University of Wisconsin–Madison and completed in accordance with the Helsinki Declaration. All participants provided informed consent prior to testing.
2.2. Procedure
At each study visit, participants completed self-report questionnaires on demographics, health history and lifestyle, in addition to clinical assessments, and a neuropsychological test battery (for a full list of procedures and tests, see Johnson et al., 2017). To classify individuals based on their cognitive status, WRAP uses a two-tiered consensus conference approach (see Langhough Koscik et al., 2021 for details). Briefly, in the first step, an algorithm that identifies cases where impairment may exist is applied, based on whether or not they meet one or more of the following criteria: (1) the participant obtains 1.5 SDs below the mean on factor scores or individual measures of memory, executive function, language, working memory, or attention (Clark et al., 2016; Koscik et al., 2014); (2) cognitive performance on one or more tests fell below values used in other studies as cut-points for clinical MCI diagnoses (e.g. WMS-R Logical Memory II, Wechsler, 1987: story A score <9: AD Neuroimaging Initiative, Petersen et al., 2010); or (3) an abnormal informant report indicating subjective cognitive or functional decline. Second, consensus diagnosis of cognitively unimpaired, MCI and dementia, are then determined by a team that includes physicians, clinical neuropsychologists, and clinical nurse practitioners, based on cognitive, medical history, lifestyle, subjective cognitive complaints, and informant data, for each visit. The MCI diagnosis follows the core clinical criteria (excluding biomarkers) from Albert et al. (2011; but see also Winblad et al., 2004), adopted by the National Institute on Aging (NIA)–Alzheimer’s Association, while dementia diagnosis follows the recommendations from McKhann et al. (2011). If the consensus review committee determines MCI and dementia are absent, the CUD label is assigned when the consensus review team interprets the low performance as indicative of concerning subclinical decline from premorbid levels.
2.3. Assessment of depressive symptoms
The Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) measures levels of depression symptoms experienced in the past week with items expressed as self-statements (e.g., ‘‘I talked less than usual’’); see Table 1 for a list of items. The original CES-D version contains 20 items, in which participants are asked to indicate the frequency of the symptoms using a scale of 0 (rarely or none of the time, less than 1 day), 1 (some or a little of the time, 1–2 days), 2 (occasionally or a moderate amount of time, 3–4 days), or 3 (most or all of the time, 5–7 days), against a time frame of the past week. Total score is computed by adding the points from each item, except positive items 4, 8, 12, and 16, for which the scoring is reversed. The 14-item version (CESD-14, Carleton et al., 2013) excludes items 9, 10, 13, 15, 17 and 19, whereas the 10-item version (CESD-10, Andresen et al., 1994) excludes items 2, 3, 4, 9, 13, 15, 16, 17, 18, and 19; in both versions, total score is calculated in the same way as the 20-item version. In the current study, recording of item-level CES-D data began at visit 2, which was considered as baseline for the statistical analyses. Internal consistency for the 10-item CES-D (Cronbach’s α = .80), 14-item CES-D (Cronbach’s α = .85), and 20-item CES-D (Cronbach’s α = .87) in the current sample was acceptable.
2.4. Assessment of control variables
Included demographic factors were age at last follow-up visit, sex, and education, while also accounting for the elapsed time between baseline and last follow-up assessment. An APOE risk score was calculated based on the odds ratios of the presence of apolipoprotein E genotype (e2/e3/e4 genotype), as previously reported (Darst et al., 2017), which was included as a covariate. Because vascular factors have been suggested to be linked to late-life depression, cognitive decline, and risk for AD (Alexopoulos et al., 1997; Flicker et al., 2008; O’Brien et al., 2003; Richard et al., 2013; Teper et al., 2008), the following vascular risk factors were included as covariates: waist-hip ratio (calculated from measurements taken at baseline visit), current smoking, history of diabetes, hypertension, heart disease, and high cholesterol (all dichotomised into yes or no, and assessed via questionnaire). For more details on vascular risk factors and prediction of AD, see Reitz et al. (2010).
2.5. Statistical analysis
We ran Mann–Whitney tests or t-tests where appropriate, to determine if there were differences between participants classified by last cognitive status on the sample characteristics, APOE risk score, vascular risk factors, and in the baseline 10-item, 14-item, and 20-item total CES-D scores. See Table 2 for sample details, reported for the whole sample and by last cognitive status. To understand how correlated the total scores from the three CES-D versions were, we ran bivariate Spearman’s rank-order correlations between the scores from the 10-, 14-, and 20-item versions of the CES-D. Bivariate correlations were also conducted between the total CES-D scores and the control variables to check for multicollinearity.
To test if baseline total CES-D scores are associated with progression to cognitive decline at last follow-up visit (see Table 3 for sample details at last visit), we conducted three separate ordinal logistic regression analyses (one each for the three CES-D versions). We used either baseline total 10-, 14-, or 20-item score as predictor in each model, follow-up consensus diagnosis as outcome (cognitively unimpaired stable, cognitively unimpaired declining, or clinically-diagnosed impaired, by combining MCI and dementia), age at last follow-up assessment, sex, elapsed time between baseline and last follow-up assessment, years of education, APOE risk score, current smoking status, history of diabetes mellitus, hypertension, heart disease, high cholesterol and waist-hip ratio, as covariates. To determine if the 10- and 14-item CES-D scores are better predictors of risk of progression to cognitive decline than the 20-item scores, we compared AIC fit statistics (Aiken at al., 1991) across otherwise parallel models, lower AIC values indicate a better fit, and a model with a delta-AIC (i.e., the difference between the two AIC values being compared) greater than 2 is considered significantly better than the model it is being compared to (Burnham & Anderson, 2004).
To test our hypothesis that the risk of progression to CUD or worse impairment at last visit that is associated with baseline CES-D differs between males and females, we examined baseline total CES-D score by sex interactions in ordinal logistic regression models (one each for the 10-, 14- and 20-item version). Predictors included were sex, total CES-D scores (10-, 14- and 20-item in separate models), and the sex * total CES-D scores interaction term, while the outcome and covariates remained the same. If the interaction terms were found to be significantly associated with progression to CUD or worse impairment at last visit, the models were then assessed using a likelihood ratio chi-square test to examine if the full models with the interaction term decreased the deviance over the full models with no interaction term.
We generated receiver-operating characteristic (ROC) curves to check for the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), of the 10-item, 14-item, and 20-item total CES-D scores. The Area Under the ROC curve (AUC) of each total score was also computed to measure how well the total score of each version can distinguish between cognitively declined participants from those who were CUS at both CES-D baseline and last follow-up visit, where a larger area indicates better performance (Hanley and McNeil, 1982). The AUCs of the 10-item, 14-item and 20-item total CES-D scores were compared using the Z statistic, and because the ROC curves are expected to be correlated, a nonparametric approach proposed by DeLong et al. (1988) was used. A two-sided p-value < 0.05 was considered statistically significant and the optimal cut-off point was identified based on the maximum Youden’s index (Youden, 1950). ROC analyses were performed using MedCalc, version 20.114 (MedCalc Software, Ostend, Belgium).
3. Results
After a mean of 7 years (range = 0−12 years), of the 1,054 participants included in the current study one hundred and two (9.7%) progressed to CUD (79), MCI (19), or dementia (4), whereas 952 (90.3%) remained cognitively unimpaired and stable at last follow-up. Table 2 describes the sample demographic characteristics, APOE risk score, vascular risk factors, and baseline total 10-, 14-, and 20-item CES-D scores, for the whole sample and by cognitive status at last follow-up assessment; the table also reports how participants classified by last cognitive status differ on these variables. Figure 1 reports baseline total 10-, 14-, and 20-item CES-D scores by each of the four cognitive statuses at last follow-up visit.
We ran bivariate Spearman’s rank-order correlations between the total scores from the three CES-D versions to understand how they are associated with each other, and between all the variables included in the analyses to check for multicollinearity. The scores from 10-item version were significantly correlated with those from 14-item version (rs = 0.955, p < .001) and with the scores from the 20-item version (rs = 0.943, p < .001), which were in turn mutually correlated (rs = 0.979, p < .001). Although significant associations were found between the rest of the variables, these were either very weak (rs = 0.00 – 0.19) or weak (rs = 0.20 – 0.39), see Table 3 for details.
To test if baseline total CES-D scores were associated with progression to cognitive decline (CUD, MCI and Dementia) from a cognitively unimpaired and stable status, ordinal logistic regression analyses were conducted for each of the three total CES-D scores. The three logistic regression models with either 10-item, 14-item or 20-item total CES-D scores were statistically significant, as were the coefficients of each total CES-D score, see Table 4 for details. Specifically, a one-point increase in baseline total CES-D score from the 10-item version was significantly associated with an increase in the odds of future cognitive decline (b = .088; SE = .022; p < .001; OR = 1.092; 95% CI, 1.046−1.141), as was a one-point increase in baseline total CES-D score from the 14-item version (b = .067; SE = .016; p < .001; OR = 1.070; 95% CI, 1.036−1.104), and one-point increase in baseline total CES-D score from the 20-item version (b = .051; SE = .013; p < .001; OR = 1.052; 95% CI, 1.025−1.080).
To test the hypothesis that the 10- and 14-item CES-D scores are better predictors of risk of progression to cognitive decline than the 20-item scores, we then compared AIC fit statistics across otherwise parallel models. The model with lowest AIC was the baseline total CES-D scores from the 14-item version (AIC = 733.00), closely followed by the model with baseline total scores from the 10-item version (AIC = 733.77) and finally, the model with baseline total scores from the 20-item version (AIC = 735.07); delta-AIC between the 20-item model and the 14-item model was greater than 2, indicating there was a significant difference between them, but not between the 10- and 20-item models nor the 10- and 14-item models
To test our hypothesis that the risk of progression to CUD or worse impairment at last visit that is associated with baseline CES-D differs between males and females, we computed an interaction term with baseline total CES-D score and sex (one each for the 10-, 14- and 20-item version), and compared the interaction models to the non-interaction models using a likelihood ratio test. The three regression models with the interaction term were statistically significant, but their interaction terms were not (total 10-item score by sex, b = -.004; SE = .049; p = .934; total 14-item score by sex, b = -.016; SE = .036; p = .660; total 20-item score by sex, b = -.011; SE = .030; p = .701); thus, changes in model deviance were not tested further.
To investigate how the CES-D total score from the 14- and 10-item versions compared to the 20-item version in differentiating between cognitive declined and cognitively unimpaired and stable participants at last follow-up visit, ROC analyses were conducted. The ROC curve analyses showed that the 10-item (Z = 3.217; p = .001), 14-item (Z = 3.593; p = .000), and 20-item (Z = 3.219; p = .001) total scores of the CES-D significantly discriminated between cognitively declined participants and those who were cognitively unimpaired and stable at last follow-up visit, see Figure 2 for ROC curves. The AUCs showed that the 14-item total score had the highest accuracy (60.8%; SE = 0.03; 95% CI, 57.8%−63.8%), followed by the 10-item score (59.6%; SE = 0.03; 95% CI, 56.6%−62.6%), and the 20-item score (59.6%; SE = 0.03; 95% CI, 56.6%-62.6%). Z tests indicated that the 14-item and 20-item AUCs were significantly different (Z = 2.123; p = .034), whereas the 10-item and 20-item AUCs were not (Z = 0.014; p = .989), nor the 10-item and 14-item AUCs (Z = 1.182 p = .237).
As the three versions of total CES-D scores significantly differentiated between the two groups, diagnostic concordance was assessed using positive predictive values (PPV) and negative predictive values (NPV). For the 10-item total score, with a cut-off of 4 based on the Youden index, the PPV was 13.9% and the NPV was 92.7% (sensitivity 53.40%, specificity 64.08%). For the 14-item total score, a cut-off of 4 produced a PPV of 14.1% and a NPV of 94.0% (sensitivity 66.99%, specificity 55.67%). Finally, for the 20-item total score, a cut-off of 5 produced a PPV of 13.1% and a NPV of 93.9% (sensitivity 69.90%, specificity 49.79%).
4. Discussion
In the current study, we investigated if baseline total CES-D scores were associated with progression to cognitive decline from a cognitively unimpaired baseline and assessed how the CES-D total score from the 14- and 10-item versions compared to the 20-item version in predicting progression. We also tested if the risk of progression differed by sex by conducting a moderator analysis, while comparing the three CES-D versions. Lastly, we compared the CES-D total score from the 14- and 10-item versions to the 20-item version, in their ability to differentiate between participants who had progressed to cognitive decline from those who did not at last follow-up visit.
In contrast to the few studies reporting that depressive symptoms are not associated with future cognitive decline (e.g., Chodosh et al., 2010; Dufouil et al., 1996; Ganguli et al., 2006; Henderson et al., 1997), our ordinal logistic regression analyses showed that separate models with baseline total CES-D scores from either the 10-item, 14-item, or 20-item version, significantly predicted follow-up consensus diagnosis (cognitively unimpaired—stable vs. cognitive unimpaired—declining, MCI, or dementia) after approximately 7 years; whilst controlling for age at last follow-up assessment, elapsed time between baseline and last follow-up assessment, years of education, APOE risk score, and vascular factors. These findings are in line with most studies that reported an association between depressive symptoms and subsequent cognitive decline (e.g., Chodosh et al., 2007; Fuhrer et al., 1992; Gonzalez et al., 2008; Kim et al., 2019; Raji et al., 2007; Wilson et al., 2002; 2004; Yaffe et al., 1999; Zahodne et al., 2014), even though the nature of the relationship remains unclear (Kim et al., 2021b) and requires further investigation.
Revised versions of the CES-D, such as the 14-item (Carleton et al., 2013) or the 10-item version (Andresen et al., 1994), have been proposed to address concerns regarding item content (e.g., gender bias), latent factor structure, or length of the original 20-item scale (Carleton et al., 2013; Gonzalez et al., 2017). However, it is not known how the 10-item and 14-item versions compare to the original 20-item scale in predicting progression to cognitive decline in older adults. Current results showed that the variance explained by the models with the 10-item or 14-item total CES-D scores was comparable to the variance explained by the 20-item model in predicting progression to cognitive decline. The AICs from the models with the 10-item and 14-item version scores were similar, indicating a difference between them of 0.77 AIC units, while the model with the 20-item version showed the highest AIC of the three, the difference being greater than 2 AIC units when compared to the 14-item version, but not between the 20- and 10-item versions, for which the difference between them was of 1.30 AIC units. Following the rule-of-thumb requiring a difference of at least 2 AIC units to conclude that model fit is better, we suggest the 14-item version may be better at predicting longitudinal consensus diagnosis compared to the 20-item version. These findings leave the 10-item version in apparent limbo, as that version is not significantly better than the 20-item version, nor significantly worse than the 14-item version. This apparent contradiction suggests that, while the 10-item version is numerically a test to predict diagnosis than the 20-item version, we do not have firm enough evidence to draw that conclusion.
As rates of dementia and depression, along with depressive symptoms profiles and clinical course, are known to differ between the sexes (Letenneur et al., 1999; Smith et al., 2008), it could be argued that sex should be considered when assessing risk factors that can be modified (Kim 2021b), as it is the case with depressive symptomatology. To better understand if sex moderates the relationship between depressive symptoms and risk of progression to CUD or worse impairment, we also examined baseline total CES-D score by sex interactions. Our results did not show the interaction term to be a significant predictor of progression to cognitive decline.
We also examined if the total CES-D scores differentiated between cognitively unimpaired participants who remained stable and those who had cognitively declined at last follow-up visit, and ROC curve analyses indicated that total scores of the CES-D from the three versions significantly discriminated between them. When comparing the accuracy of each of three CES-D versions, we found that the total score from the 14-item version showed the highest accuracy, while the 10- and 20-item tests AUCs were identical. This latter finding, is in line with Chen and Chan (2008), who reported that the 10-item version was comparable to the original version in screening for depressive symptoms in elderly participants with mild dementia. Although these results show that the three CES-D versions perform better than chance in differentiating the two groups (i.e., 50%), the AUC values of the 10-item (59.6%), 14-item (60.8%), and 20-item (59.6%) models observed here are very similar between them and considered “poor”; generally, AUC values between 0.9-1 are considered “outstanding”, between 0.8-0.9 are considered “excellent”, and “acceptable” between 0.7-0.8. It is possible that within the cognitively declined group, the difference in the number of participants who were cognitively unimpaired but declining (N=80) and those who were with MCI (N=19) or dementia (N=4) was too large. As a result, the ability of the three CES-D versions to discriminate between cognitively unimpaired and stable, and a group largely comprised of participants who were unimpaired but declining, might have been affected.
This study has several strengths, such as the length of the follow-up, with an average of approximately 7 years between baseline visit and last follow-up visit, and that participants were classified via consensus conference diagnosis, based on cognitive, medical history, lifestyle, subjective cognitive complaints, and informant data, for each visit (see Procedure section for details and Langhough Koscik et al., 2021). Yet, this study also has some limitations, the sample size of the cognitively declined group at last follow-up visit was far from ideal; this, however, is not surprising considering the progression rates of cognitively unimpaired individuals observed in previous studies (progression to CU-D (formerly referred to as early MCI) was 14% in Bruno et al., 2018; and 15.2% in Johnson et al., 2017). The sample also consisted mostly of White participants, restricting the generalizability of current findings. Finally, it should be noted that current analyses and results were extrapolated from the 20-item version of the CES-D rather than from testing the three versions separately.
In summary, this study investigated if baseline total CES-D scores were associated with progression to cognitive decline from a cognitively unimpaired baseline, assessed how the CES-D total score from the 14- and 10-item versions compared to the 20-item version in predicting progression, CES-D by sex interaction, and the accuracy of baseline CES-D scores to discriminate between participants who had cognitively declined from those who remained unimpaired and stable at last visit. Results showed that baseline total scores from the three CES-D versions significantly predicted progression and that the model with total scores from the 14-item version was better than the model with scores from 20-item version in predicting progression to cognitive decline, as shown by their AICs. We did not find sex to moderate the relationship between CES-D score and cognitive decline. The 14-item baseline total CES-D score also showed the highest accuracy when discriminating between those who were cognitively unimpaired and stable and those who had cognitively declined at last follow-up visit. We believe that the 14-item version of the CES-D, could be a good alternative to the original 20-item version for studies investigating depressive symptoms and cognitive decline.
Funding
WRAP is funded by NIH grants AG027161. This secondary analysis of WRAP data was funded by a NIH-NIA (R01 144 AAI8612) grant to KDM, in which DB and RL are co-investigators.
Acknowledgments
We would like to thank the participants, the staff, and researchers at the University of Wisconsin, it is because of them that this work is possible.
Data availability
Data can be requested here: https://wrap.wisc.edu/data-requests/.
References
- Multiple Regression: Testing and Interpreting Interactions; Sage: New York.
- Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., Gamst, A., Holtzman, D. M., Jagust, W. J., Petersen, R. C., Snyder, P. J., Carrillo. M. C., Thies, B., & Phelps, C. H. (2011). The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & dementia, 7(3), 270-279. [CrossRef]
- Alexopoulos, G. S., Meyers, B. S., Young, R. C., Campbell, S., Silbersweig, D., & Charlson, M. (1997). 'Vascular depression' hypothesis. Archives of general psychiatry, 54(10), 915-922. [CrossRef]
- American Psychological Association, 2013; in Kim et al., 2019.
- Andresen, E. M., Malmgren, J. A., Carter, W. B., & Patrick, D. L. (1994). Screening for depression in well older adults: Evaluation of a short form of the CES-D. American journal of preventive medicine, 10(2), 77-84. [CrossRef]
- Barnes, D. E., Alexopoulos, G. S., Lopez, O. L., Williamson, J. D., & Yaffe, K. (2006). Depressive symptoms, vascular disease, and mild cognitive impairment: findings from the Cardiovascular Health Study. Archives of general psychiatry, 63(3), 273-279. [CrossRef]
- Bartolini, M., Coccia, M., Luzzi, S., Provinciali, L., & Ceravolo, M. G. (2005). Motivational symptoms of depression mask preclinical Alzheimer’s disease in elderly subjects. Dementia and geriatric cognitive disorders, 19(1), 31-36. [CrossRef]
- Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory for measuring depression. Archives of general psychiatry, 4(6), 561-571. [CrossRef]
- Beck, A. T., Steer, R. A., Ball, R., & Ranieri, W. F. (1996). Comparison of Beck Depression Inventories-IA and-II in psychiatric outpatients. Journal of personality assessment, 67(3), 588-597. [CrossRef]
- Becker, J. T., Chang, Y. F., Lopez, O. L., Dew, M. A., Sweet, R. A., Barnes, D., Yaffe, K., Young, J., Kuller, L., & Reynolds III, C. F. (2009). Depressed mood is not a risk factor for incident dementia in a community-based cohort. The American Journal of Geriatric Psychiatry, 17(8), 653-663. [CrossRef]
- Bruno, D., Koscik, R. L., Woodard, J. L., Pomara, N., & Johnson, S. C. (2018). The recency ratio as predictor of early MCI. International psychogeriatrics, 30(12), 1883-1888. [CrossRef]
- Burnham, K. P., & Anderson, D. R. (2004). Multimodel inference: understanding AIC and BIC in model selection. Sociological methods & research, 33(2), 261-304. [CrossRef]
- Byers, A. L., & Yaffe, K. (2011). Depression and risk of developing dementia. Nature Reviews Neurology, 7(6), 323-331. [CrossRef]
- Carleton, R. N., Thibodeau, M. A., Teale, M. J., Welch, P. G., Abrams, M. P., Robinson, T., & Asmundson, G. J. (2013). The center for epidemiologic studies depression scale: a review with a theoretical and empirical examination of item content and factor structure. PloS one, 8(3), e58067. [CrossRef]
- Carleton, R. N., Teale Sapach, M. J., Oriet, C., & LeBouthillier, D. M. (2017). Online attention modification for social anxiety disorder: replication of a randomized controlled trial. Cognitive Behaviour Therapy, 46(1), 44-59. [CrossRef]
- Carter, J., Cogo-Moreira, H., Herrmann, N., Merino, D., Yang, P., Shah, B. R., Kiss, A., Reitav, J., Oh, P. I., & Swardfager, W. (2016). Validity of the center for epidemiological studies Depression Scale in type 2 diabetes. Journal of Psychosomatic Research, 90, 91-97. [CrossRef]
- Chen, P., Ganguli, M., Mulsant, B. H., & DeKosky, S. T. (1999). The temporal relationship between depressive symptoms and dementia: a community-based prospective study. Archives of general psychiatry, 56(3), 261-266. [CrossRef]
- Cheng, S. T., & Chan, A. C. (2005). The center for epidemiologic studies depression scale in older Chinese: thresholds for long and short forms. International Journal of Geriatric Psychiatry: A journal of the psychiatry of late life and allied sciences, 20(5), 465-470. [CrossRef]
- Cheng, S. T., & Chan, A. C. (2008). Detecting depression in Chinese adults with mild dementia: findings with two versions of the Center for Epidemiologic Studies Depression Scale. Psychiatry Research, 159(1-2), 44-49. [CrossRef]
- Chodosh, J., Kado, D. M., Seeman, T. E., & Karlamangla, A. S. (2007). Depressive symptoms as a predictor of cognitive decline: MacArthur Studies of Successful Aging. The American journal of geriatric psychiatry, 15(5), 406-415. [CrossRef]
- Chodosh, J., Miller-Martinez, D., Aneshensel, C. S., Wight, R. G., & Karlamangla, A. S. (2010). Depressive symptoms, chronic diseases, and physical disabilities as predictors of cognitive functioning trajectories in older Americans. Journal of the American Geriatrics Society, 58(12), 2350-2357. [CrossRef]
- Clark, L. R., Koscik, R. L., Nicholas, C. R., Okonkwo, O. C., Engelman, C. D., Bratzke, L. C., Hogan, K. J., Mueller, K. D., Bendlin, B. B., Carlsson, C. M., Asthana, S., Sager, M. A., Hermann, B. P., & Johnson, S. C. (2016). Mild cognitive impairment in late middle age in the Wisconsin registry for Alzheimer's prevention study: prevalence and characteristics using robust and standard neuropsychological normative data. Archives of Clinical Neuropsychology, 31(7), 675-688. [CrossRef]
- Cole, S. R., Kawachi, I., Maller, S. J., & Berkman, L. F. (2000). Test of item-response bias in the CES-D scale: experience from the New Haven EPESE study. Journal of clinical epidemiology, 53(3), 285-289. [CrossRef]
- Dal Forno, G., Palermo, M. T., Donohue, J. E., Karagiozis, H., Zonderman, A. B., & Kawas, C. H. (2005). Depressive symptoms, sex, and risk for Alzheimer's disease. Annals of neurology, 57(3), 381-387. [CrossRef]
- Darst, B. F., Koscik, R. L., Racine, A. M., Oh, J. M., Krause, R. A., Carlsson, C. M., Zetterberg, H., Blennow, K., Christian, B. T., Bendlin, B. B., Okonkwo, O. C., Hogan, K. J., Hermann, B. P., Sager, M. A., Asthana, S., Johnson, S. C., & Engelman, C. D. (2017). Pathway-specific polygenic risk scores as predictors of amyloid-β deposition and cognitive function in a sample at increased risk for Alzheimer’s disease. Journal of Alzheimer's Disease, 55(2), 473-484. [CrossRef]
- DeLong, E. R., DeLong, D. M., & Clarke-Pearson, D. L. (1988). Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics, 837-845. [CrossRef]
- Devanand, D. P., Sano, M., Tang, M. X., Taylor, S., Gurland, B. J., Wilder, D., Stern, Y., & Mayeux, R. (1996). Depressed mood and the incidence of Alzheimer's disease in the elderly living in the community. Archives of general psychiatry, 53(2), 175-182. [CrossRef]
- Diniz, B. S., Butters, M. A., Albert, S. M., Dew, M. A., & Reynolds, C. F. (2013). Late-life depression and risk of vascular dementia and Alzheimer's disease: systematic review and meta-analysis of community-based cohort studies. The British Journal of Psychiatry, 202(5), 329-335. [CrossRef]
- Dufouil, C., Fuhrer, R., Dartigues, J. F., & Alpérovitch, A. (1996). Longitudinal analysis of the association between depressive symptomatology and cognitive deterioration. American Journal of Epidemiology, 144(7), 634-641. [CrossRef]
- Flicker, L. (2008). Vascular factors in geriatric psychiatry: time to take a serious look. Current Opinion in Psychiatry, 21(6), 551-554. [CrossRef]
- Fuhrer, R., Antonucci, T. C., Gagnon, M., Dartigues, J. F., Barberger-Gateau, P., & Alperovitch, A. (1992). Depressive symptomatology and cognitive functioning: an epidemiological survey in an elderly community sample in France. Psychological medicine, 22(1), 159-172. [CrossRef]
- Fuhrer, R., Dufouil, C., & Dartigues, J. F. (2003). Exploring sex differences in the relationship between depressive symptoms and dementia incidence: prospective results from the PAQUID Study. Journal of the American Geriatrics Society, 51(8), 1055-1063. [CrossRef]
- Ganguli, M., Du, Y., Dodge, H. H., Ratcliff, G. G., & Chang, C. C. H. (2006). Depressive symptoms and cognitive decline in late life: a prospective epidemiological study. Archives of general psychiatry, 63(2), 153-160. [CrossRef]
- Gatz, J. L., Tyas, S. L., St. John, P., & Montgomery, P. (2005). Do depressive symptoms predict Alzheimer's disease and dementia? The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 60(6), 744-747. [CrossRef]
- Geda, Y. E., Knopman, D. S., Mrazek, D. A., Jicha, G. A., Smith, G. E., Negash, S.,... & Rocca, W. A. (2006). Depression, apolipoprotein E genotype, and the incidence of mild cognitive impairment: a prospective cohort study. Archives of neurology, 63(3), 435-440. [CrossRef]
- González, H. M., Bowen, M. E., & Fisher, G. G. (2008). Memory decline and depressive symptoms in a nationally representative sample of older adults: The Health and Retirement Study (1998–2004). Dementia and Geriatric Cognitive Disorders, 25(3), 266-271. [CrossRef]
- González, P., Nuñez, A., Merz, E., Brintz, C., Weitzman, O., Navas, E. L., Camacho, A., Buelna, C., Penedo, F. J., Wassertheil-Smoller, S., Perreira, K., Isasi, C. R., Choca, J., Talavera, G. A., & Gallo, L. C. (2017). Measurement properties of the Center for Epidemiologic Studies Depression Scale (CES-D 10): findings from HCHS/SOL. Psychological assessment, 29(4), 372. [CrossRef]
- Hanley, J. A., & McNeil, B. J. (1982). The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology, 143(1), 29-36. [CrossRef]
- Harenberg, S., Marshall-Prain, N., Dorsch, K. D., & Riemer, H. A. (2015). Factorial validity and gender invariance of the center for epidemiological studies depression in cardiac rehabilitation patients. Journal of Cardiopulmonary Rehabilitation and Prevention, 35(5), 320-327. [CrossRef]
- Henderson, A. S., Korten, A. E., Jacomb, P. A., Mackinnon, A. J., Jorm, A. F., Christensen, H., & Rodgers, B. (1997). The course of depression in the elderly: a longitudinal community-based study in Australia. Psychological medicine, 27(1), 119-129. [CrossRef]
- Irwin, M., Artin, K. H., & Oxman, M. N. (1999). Screening for depression in the older adult: criterion validity of the 10-item Center for Epidemiological Studies Depression Scale (CES-D). Archives of internal medicine, 159(15), 1701-1704. [CrossRef]
- Johnson, S. C., Koscik, R. L., Jonaitis, E. M., Clark, L. R., Mueller, K. D., Berman, S. E., Bendlin, B. B., Engelman, C. D., Okonkwo, O. C., Hogan, K. J., Asthana, S., Carlsson, C. M., Hermann, B. P., & Sager, M. A. (2017). The Wisconsin Registry for Alzheimer's Prevention: a review of findings and current directions. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring, 10, 130-142. [CrossRef]
- Jorm, A. F., Van Duijn, C. M., Chandra, V., Fratiglioni, L., Graves, A. B., Heyman, A., Kokmen, E., Kondo, K., Mortimer, J. A., Rocca, W. A., Shalat, S. L., & Soininen, H. (1991). Psychiatric history and related exposures as risk factors for Alzheimer's disease: a collaborative re-analysis of case-control studies. International journal of epidemiology, 20(Supplement_2), S43-S47. [CrossRef]
- Jorm, A. F. (2001). History of depression as a risk factor for dementia: an updated review. Australian & New Zealand Journal of Psychiatry, 35(6), 776-781. [CrossRef]
- Kim, S., Kim, M. J., Kim, S., Kang, H. S., Lim, S. W., Myung, W., Lee, Y., Hong, C. H., Choi, S. H., Na, D. L., Seo, S. W., Ku, B. D., Kim, S. Y., Kim, S. Y., Jeong, J. H., Park, S. A., Carroll, B. J., & Kim, D. K. (2015). Gender differences in risk factors for transition from mild cognitive impairment to Alzheimer’s disease: A CREDOS study. Comprehensive Psychiatry, 62, 114-122. [CrossRef]
- Kim, J. H. (2019). Effect of depressive disorder on cognitive decline. Archives of Gerontology and Geriatrics, 83, 211-216. [CrossRef]
- Kim, H., Jeong, W., Kwon, J., Kim, Y., Park, E. C., & Jang, S. I. (2021a). Association between depression and the risk of Alzheimer’s disease using the Korean national health insurance service-elderly cohort. Scientific Reports, 11(1), 1-8. [CrossRef]
- Kim, D., Wang, R., Kiss, A., Bronskill, S. E., Lanctot, K. L., Herrmann, N., & Gallagher, D. (2021b). Depression and increased risk of Alzheimer's dementia: longitudinal analyses of modifiable risk and sex-related factors. The American Journal of Geriatric Psychiatry, 29(9), 917-926. [CrossRef]
- Kohout, F. J., Berkman, L. F., Evans, D. A., & Cornoni-Huntley, J. (1993). Two shorter forms of the CES-D depression symptoms index. Journal of aging and health, 5(2), 179-193. [CrossRef]
- Koscik, R. L., La Rue, A., Jonaitis, E. M., Okonkwo, O. C., Johnson, S. C., Bendlin, B. B., Hermann, B. P., & Sager, M. A. (2014). Emergence of mild cognitive impairment in late middle-aged adults in the wisconsin registry for Alzheimer's prevention. Dementia and geriatric cognitive disorders, 38(1-2), 16-30. [CrossRef]
- Langhough Koscik, R., Hermann, B. P., Allison, S., Clark, L. R., Jonaitis, E. M., Mueller, K. D., Betthauser, T. J., Christian, B. T., Du, L., Okonkwo, O., Birdsill, A., Chin, N., Gleason, C., & Johnson, S. C. (2021). Validity evidence for the research category, “cognitively unimpaired–declining,” as a risk marker for mild cognitive impairment and Alzheimer’s disease. Frontiers in Aging Neuroscience, 13, 688478. [CrossRef]
- Lara, E., Haro, J. M., Tang, M. X., Manly, J., & Stern, Y. (2016). Exploring the excess mortality due to depressive symptoms in a community-based sample: The role of Alzheimer's Disease. Journal of Affective Disorders, 202, 163-170. [CrossRef]
- Letenneur, L., Gilleron, V., Commenges, D., Helmer, C., Orgogozo, J. M., & Dartigues, J. F. (1999). Are sex and educational level independent predictors of dementia and Alzheimer’s disease? Incidence data from the PAQUID project. Journal of Neurology, Neurosurgery & Psychiatry, 66(2), 177-183. [CrossRef]
- Lyketsos, C. G., & Olin, J. (2002). Depression in Alzheimer’s disease: overview and treatment. Biological psychiatry, 52(3), 243-252. [CrossRef]
- McKhann, G. M., Knopman, D. S., Chertkow, H., Hyman, B. T., Jack Jr, C. R., Kawas, C. H., Klunk, W. E., Koroshetz, W. J., Manly, J. J., Mayeux, R., Mohs, R. C., Morris, J. C., Rossor, M. N., Scheltens, P., Carrillo, M. C., Thies, B., Weintraub, S., & Phelps, C. H. (2011). The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & dementia, 7(3), 263-269. [CrossRef]
- Mason, J. E., LeBouthillier, D. M., & Asmundson, G. J. (2019). Relationships between health behaviors, posttraumatic stress disorder, and comorbid general anxiety and depression. Cognitive behaviour therapy, 48(3), 184-199. [CrossRef]
- Norton, J., Carrière, I., Pérès, K., Gabelle, A., Berr, C., Ritchie, K., & Ancelin, M. L. (2019). Sex-specific depressive symptoms as markers of pre-Alzheimer dementia: findings from the Three-City cohort study. Translational psychiatry, 9(1), 1-10. [CrossRef]
- O'Brien, J. T., Erkinjuntti, T., Reisberg, B., Roman, G., Sawada, T., Pantoni, L., Bowler, J. V., Ballard, C., DeCarli, C., Gorelick, P. B., & DeKosky, S. T. (2003). Vascular cognitive impairment. The Lancet Neurology, 2(2), 89-98. [CrossRef]
- Ohayon, M. M., & Schatzberg, A. F. (2003). Using chronic pain to predict depressive morbidity in the general population. Archives of general psychiatry, 60(1), 39-47. [CrossRef]
- Petersen, R. C., Aisen, P. S., Beckett, L. A., Donohue, M. C., Gamst, A. C., Harvey, D. J., Jack, C. R., Jagust, W. J., Shaw, L. M., Toga, A. W., Trojanowski, J. Q., & Weiner, M. W. (2010). Alzheimer's disease neuroimaging initiative (ADNI): clinical characterization. Neurology, 74(3), 201-209. [CrossRef]
- Radloff, L. S. (1977). The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement, 1(3), 385–401. [CrossRef]
- Raji, M. A., Reyes-Ortiz, C. A., Kuo, Y. F., Markides, K. S., & Ottenbacher, K. J. (2007). Depressive symptoms and cognitive change in older Mexican Americans. Journal of geriatric psychiatry and neurology, 20(3), 145-152. [CrossRef]
- Reitz, C., Tang, M. X., Schupf, N., Manly, J. J., Mayeux, R., & Luchsinger, J. A. (2010). A summary risk score for the prediction of Alzheimer disease in elderly persons. Archives of neurology, 67(7), 835-841. [CrossRef]
- Richard, E., Reitz, C., Honig, L. H., Schupf, N., Tang, M. X., Manly, J. J., Mayeux, R., Devanand, D., & Luchsinger, J. A. (2013). Late-life depression, mild cognitive impairment, and dementia. JAMA neurology, 70(3), 383-389. [CrossRef]
- Rivera-Medina, C. L., Caraballo, J. N., Rodríguez-Cordero, E. R., Bernal, G., & Dávila-Marrero, E. (2010). Factor structure of the CES-D and measurement invariance across gender for low-income Puerto Ricans in a probability sample. Journal of Consulting and Clinical Psychology, 78(3), 398. [CrossRef]
- Saczynski, J. S., Beiser, A., Seshadri, S., Auerbach, S., Wolf, P. A., & Au, R. (2010). Depressive symptoms and risk of dementia: the Framingham Heart Study. Neurology, 75(1), 35-41. [CrossRef]
- Sager, M. A., Hermann, B., & La Rue, A. (2005). Middle-aged children of persons with Alzheimer’s disease: APOE genotypes and cognitive function in the Wisconsin Registry for Alzheimer’s Prevention. Journal of geriatric psychiatry and neurology, 18(4), 245-249. [CrossRef]
- Shafer, A. B. (2006). Meta-analysis of the factor structures of four depression questionnaires: Beck, CES-D, Hamilton, and Zung. Journal of clinical psychology, 62(1), 123-146. [CrossRef]
- Smith, D. J., Kyle, S., Forty, L., Cooper, C., Walters, J., Russell, E., Caesar, S., Farmer, A., McGuffin, P., Jones, I., Jones, L., & Craddock, N. (2008). Differences in depressive symptom profile between males and females. Journal of Affective Disorders, 108(3), 279-284. [CrossRef]
- Snarski, M., & Scogin, F. (2006). Assessing depression in older adults. In: Qualls SH, Knight BG, editors. Psychotherapy for depression in older adults. Hoboken: John Wiley and Sons. 45–77.
- Stansbury, J. P., Ried, L. D., & Velozo, C. A. (2006). Unidimensionality and bandwidth in the Center for Epidemiologic Studies Depression (CES–D) scale. Journal of personality assessment, 86(1), 10-22. [CrossRef]
- Teper, E., & O'Brien, J. T. (2008). Vascular factors and depression. International Journal of Geriatric Psychiatry: A journal of the psychiatry of late life and allied sciences, 23(10), 993-1000. [CrossRef]
- Underwood, E. A., Davidson, H. P., Azam, A. B., & Tierney, M. C. (2019). Sex differences in depression as a risk factor for Alzheimer’s disease: a systematic review. Innovation in aging, 3(2). [CrossRef]
- Vilalta-Franch, J., López-Pousa, S., Llinàs-Reglà, J., Calvó-Perxas, L., Merino-Aguado, J., & Garre-Olmo, J. (2013). Depression subtypes and 5-year risk of dementia and Alzheimer disease in patients aged 70 years. International journal of geriatric psychiatry, 28(4), 341-350. [CrossRef]
- Wechsler, D. (1987). WMS-R: Wechsler memory scale-revised. Psychological Corporation.
- Williams, C. D., Taylor, T. R., Makambi, K., Harrell, J., Palmer, J. R., Rosenberg, L., & Adams-Campbell, L. L. (2007). CES-D four-factor structure is confirmed, but not invariant, in a large cohort of African American women. Psychiatry research, 150(2), 173-180. [CrossRef]
- Wilson, R. S., Barnes, L. L., De Leon, C. M., Aggarwal, N. T., Schneider, J. S., Bach, J., Pilat, J., Beckett, L. A., Arnold, S. E., Evans, D. A., & Bennett, D. A. (2002). Depressive symptoms, cognitive decline, and risk of AD in older persons. Neurology, 59(3), 364-370. [CrossRef]
- Wilson, R. S., De Leon, C. M., Bennett, D. A., Bienias, J. L., & Evans, D. A. (2004). Depressive symptoms and cognitive decline in a community population of older persons. Journal of Neurology, Neurosurgery & Psychiatry, 75(1), 126-129.
- Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L., Wahlund, L. O., Nordberg, A., Backman, L., Albert, M., Almkvist, O., Arai, H., Basun, H., Blennow, K., de Leon, M., DeCarli, C., Erkinjuntti, T., Giacobini, E., Graff, C., Hardy, J., & Petersen, R. C. (2004). Mild cognitive impairment–beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. Journal of internal medicine, 256(3), 240-246. [CrossRef]
- Yaffe, K., Blackwell, T., Gore, R., Sands, L., Reus, V., & Browner, W. S. (1999). Depressive symptoms and cognitive decline in nondemented elderly women: a prospective study. Archives of general psychiatry, 56(5), 425-430. [CrossRef]
- Youden, W. J. (1950). Index for rating diagnostic tests. Cancer, 3(1), 32-35. [CrossRef]
- Zahodne, L. B., Stern, Y., & Manly, J. J. (2014). Depressive symptoms precede memory decline, but not vice versa, in non-demented older adults. Journal of the American Geriatrics Society, 62(1), 130-134. [CrossRef]
Figure 1.
Boxplot: Baseline total 10-, 14-, and 20-item CES-D scores by each of the four cognitive statuses at last follow-up visit. CUS: cognitively unimpaired-stable; CUD: cognitively unimpaired-declining; MCI: mild cognitive impairment; Dem: dementia.
Figure 1.
Boxplot: Baseline total 10-, 14-, and 20-item CES-D scores by each of the four cognitive statuses at last follow-up visit. CUS: cognitively unimpaired-stable; CUD: cognitively unimpaired-declining; MCI: mild cognitive impairment; Dem: dementia.
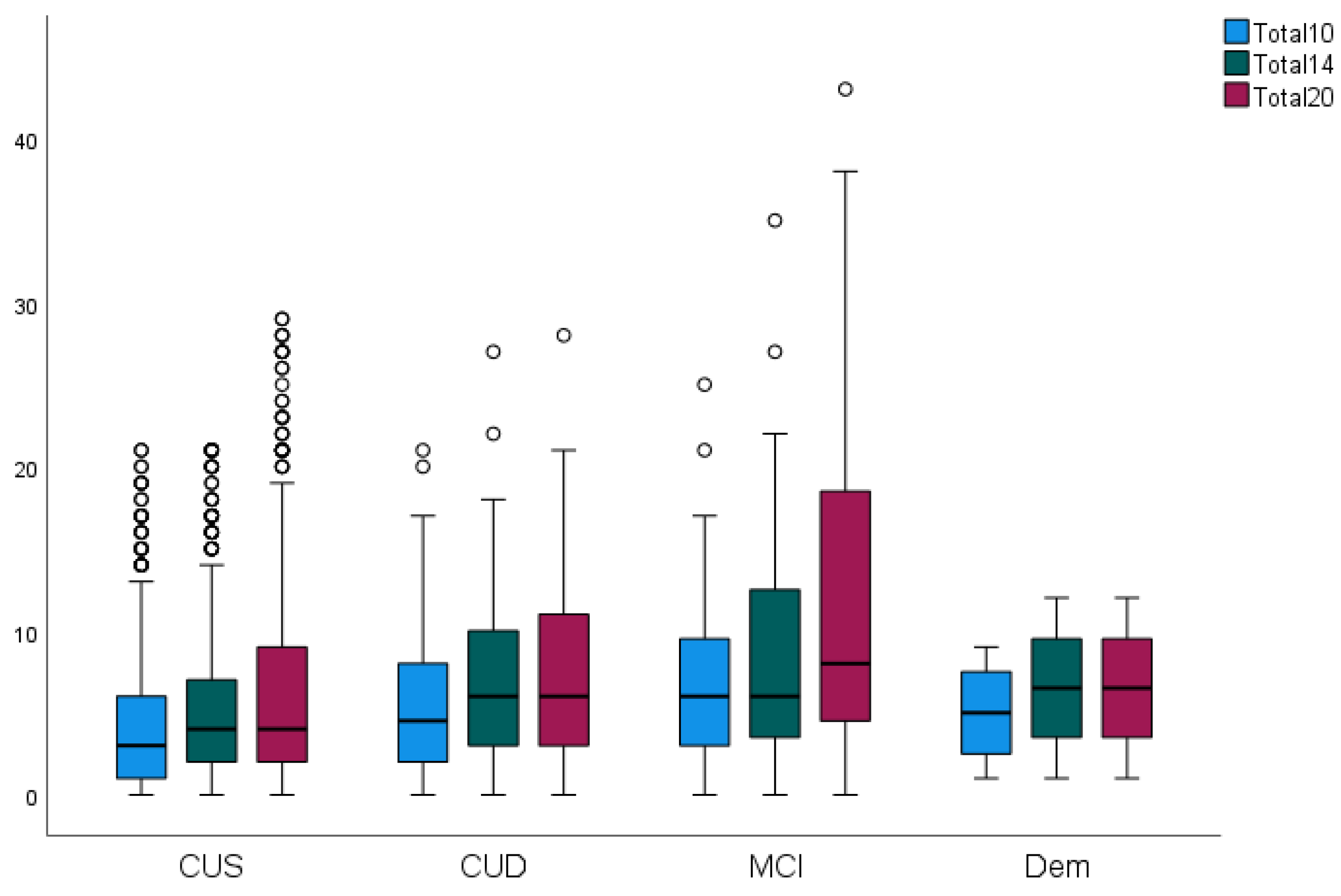
Figure 2.
Receiver Operating Characteristic (ROC) curve of the 10-item, 14-item, and 20-item total CES-D scores.
Figure 2.
Receiver Operating Characteristic (ROC) curve of the 10-item, 14-item, and 20-item total CES-D scores.
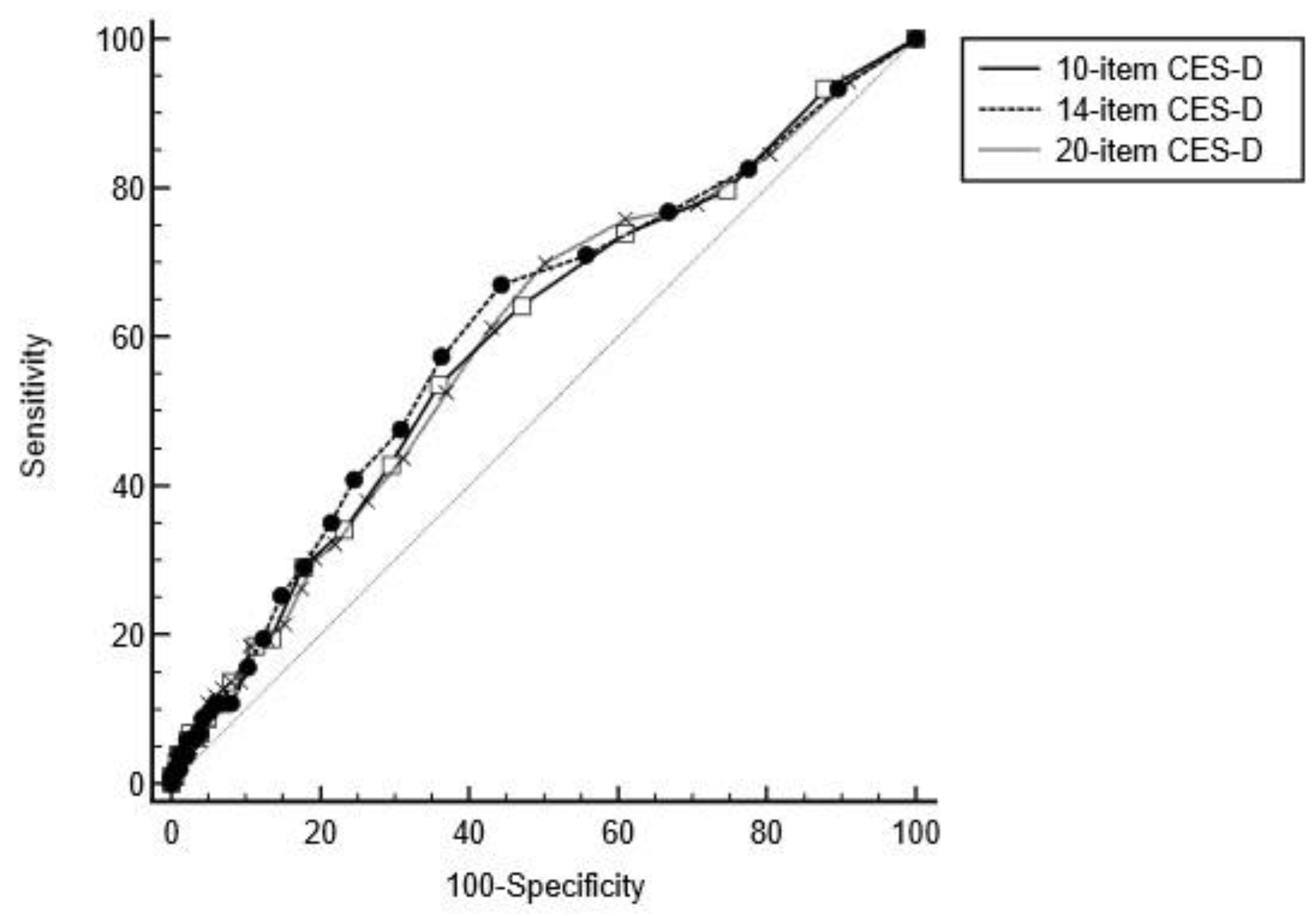

Table 1.
The 20 items from the original CES-D, items included in the CES-D 10 and CES-D 14 versions. X denotes item is included.
Table 1.
The 20 items from the original CES-D, items included in the CES-D 10 and CES-D 14 versions. X denotes item is included.
| 20-item CES-D | 10-item CES-D | 14-item CES-D |
|---|---|---|
| 1. I was bothered by things that usually don’t bother me. | X | X |
| 2. I did not feel like eating; my appetite was poor. | X | |
| 3. I felt that I could not shake off the blues, even with help from my family or friends. | X | |
| 4. I felt I was just as good as other people. | X | |
| 5. I had trouble keeping my mind on what I was doing. | X | X |
| 6. I felt depressed. | X | X |
| 7. I felt that everything I did was an effort. | X | X |
| 8. I felt hopeful about the future. | X | X |
| 9. I thought my life had been a failure. | ||
| 10. I felt fearful. | X | |
| 11. My sleep was restless. | X | X |
| 12. I was happy. | X | X |
| 13. I talked less than usual. | ||
| 14. I felt lonely. | X | X |
| 15. People were unfriendly. | ||
| 16. I enjoyed life. | X | |
| 17. I had crying spells. | ||
| 18. I felt sad. | X | |
| 19. I felt that people disliked me. | ||
| 20. I could not get “going”. | X | X |
Table 2.
Sample characteristics and comparison among participants by their last cognitive status. Means (standard deviations) or number of participants (percentages) are reported for the variables included in the regression analyses, by whole sample and consensus diagnosis at last follow-up assessment. For heart disease, diabetes mellitus, hypertension, and high cholesterol, yes refers to a previous or current history of the disease.
Table 2.
Sample characteristics and comparison among participants by their last cognitive status. Means (standard deviations) or number of participants (percentages) are reported for the variables included in the regression analyses, by whole sample and consensus diagnosis at last follow-up assessment. For heart disease, diabetes mellitus, hypertension, and high cholesterol, yes refers to a previous or current history of the disease.
| Characteristic | Total | Cognitively unimpaired stable | Cognitively unimpaired declining | MCI or Dementia | p |
|---|---|---|---|---|---|
| No. participants | 1,054 | 952 (90.3%) | 79 (7.5%) | 23 (2.2%) | |
| Age at last visit | 64.65 (6.9) | 64.32 (7.0) | 67.46 (5.7) | 68.65 (5.9) | .001 |
| Gender (females) | 766 (72.7%) | 697 (73.2%) | 52 (65.8%) | 17 (73.9%) | .364 |
| Education (years) | 16.27 (2.8) | 16.32 (2.8) | 16.20 (2.6) | 14.39 (2.2) | .004 |
| APOE risk score | 1.18 (0.7) | 1.14 (0.7) | 1.40 (0.8) | 1.67 (0.9) | .001 |
| Elapsed time | 6.86 (3.1) | 6.85 (3.1) | 7.16 (2.5) | 6.17 (2.6) | .375 |
| Heart disease (yes) | 47 (4.5%) | 40 (4.2%) | 3 (3.8%) | 4 (17.4%) | .010 |
| Diabetes mellitus (yes) | 63 (6.0%) | 52 (5.5%) | 8 (10.1%) | 3 (13.0%) | .086 |
| Hypertension (yes) | 261 (24.8%) | 221 (23.2%) | 29 (36.7%) | 11 (47.8%) | .001 |
| High cholesterol (yes) | 457 (43.4%) | 403 (42.3%) | 36 (45.6%) | 18 (78.3%) | .002 |
| Baseline smoking (yes) | 449 (42.6%) | 405 (42.5%) | 36 (45.6%) | 8 (34.8%) | .651 |
| Baseline WHR | 0.86 (0.1) | 0.86 (0.1) | 0.88 (0.8) | 0.88 (0.9) | .255 |
| Baseline CESD-10 | 4.53 (4.2) | 4.38 (4.1) | 5.46 (4.4) | 7.35 (6.6) | .001 |
| Baseline CESD-14 | 5.76 (5.7) | 5.55 (5.5) | 7.24 (6.1) | 9.13 (9.0) | .001 |
| Baseline CESD-20 | 6.82 (6.9) | 6.59 (6.7) | 8.24 (7.3) | 11.26 (11.5) | .001 |
Notes: *p-values from t-tests or Mann-Whitney tests where appropriate. WHR = waist-hip ratio.
Table 3.
Bivariate Spearman’s rank-order correlations. Correlation coefficients between the variables included in the regression analyses.
Table 3.
Bivariate Spearman’s rank-order correlations. Correlation coefficients between the variables included in the regression analyses.
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age at last visit | 1 | -.049 | .041 | -.092** | .101** | .023 | .187** | .046 | .138** | .074* | -.076* | -.089** | -.107** |
| 2. Gender | 1 | -.117** | .006 | -.094** | -.016 | .071* | .016 | -.052 | .102** | .115** | .093** | .101** | |
| 3. Education years | 1 | -.014 | -.043 | -.009 | -.078* | -.079* | -.066* | -.140** | -.063* | -.069* | -.073* | ||
| 4. APOE risk score | 1 | -.032 | .001 | -.046 | -.028 | .109** | -.038 | .011 | .007 | .013 | |||
| 5. Heart disease | 1 | .023 | .100** | .102** | .061* | .024 | .004 | -.015 | -.023 | ||||
| 6. Diabetes mellitus | 1 | .161** | -.031 | .151** | .141 | .006 | .015 | .013 | |||||
| 7. Hypertension | 1 | .013 | .217** | .160** | .062* | .048 | .051 | ||||||
| 8. Current smoking | 1 | .017 | .076* | .075* | .074* | .070* | |||||||
| 9. High cholesterol | 1 | .161** | .060 | .068* | .067* | ||||||||
| 10. Waist-hip ratio | 1 | .057 | .067* | .068* | |||||||||
| 11. CESD-10 | 1 | .955** | .943** | ||||||||||
| 12. CESD-14 | 1 | .979** | |||||||||||
| 13. CESD-20 | 1 |
Note: For heart disease, diabetes mellitus, hypertension, and high cholesterol, answers were dichotomised into yes/no, for previous or current history of the disease. CESD-10, CESD-14, and CESD-20, refer to baseline total scores from the 10-, 14-, and 20-item versions of the CES-D.
Table 4.
Ordinal logistic regression models predicting progression from CUS to CUD or clinically-diagnosed impaired status (MCI and Dementia combined) at last follow-up visit.
Table 4.
Ordinal logistic regression models predicting progression from CUS to CUD or clinically-diagnosed impaired status (MCI and Dementia combined) at last follow-up visit.
| Measures | 10-item Model1 | 14-item Model2 | 20-item Model3 | |||
|---|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | |
| Age last visit | 1.10 (1.06-1.14) | .000 | 1.10 (1.06-1.14) | .000 | 1.10 (1.06-1.14) | .000 |
| Gender | 0.63 (0.39-1.00) | .052 | 0.63 (0.39-1.01) | .054 | 0.63 (0.39-1.01) | .055 |
| Elapsed time | 0.97 (0.90-1.05) | .448 | 0.97 (0.90-1.05) | .457 | 0.97 (0.90-1.05) | .450 |
| Education | 0.93 (0.85-1.01) | .072 | 0.93 (0.85-1.01) | .076 | 0.93 (0.85-1.01) | .078 |
| APOE score | 1.92 (1.47-2.51) | .000 | 1.91 (1.47-2.50) | .000 | 1.91 (1.46-2.49) | .000 |
| Heart | 1.19 (0.50-2.82) | .692 | 1.18 (0.49-2.82) | .708 | 1.20 (0.51-2.86) | .675 |
| Diabetes | 1.57 (0.74-3.34) | .238 | 1.59 (0.75-3.38) | .225 | 1.57 (0.74-3.33) | .238 |
| Hypertension | 1.65 (1.03-2.64) | .037 | 1.66 (1.04-2.66) | .034 | 1.65 (1.03-2.64) | .036 |
| Smoking | 0.88 (0.57-1.36) | .579 | 0.87 (0.57-1.35) | .544 | 0.88 (0.57-1.35) | .551 |
| High cholest. | 0.97 (0.62-1.52) | .897 | 0.97 (0.62-1.53) | .907 | 0.97 (0.62-1.52) | .894 |
| WHR | 1.06 (0.82-1.38) | .639 | 1.06 (0.82-1.37) | .650 | 1.07 (0.82-1.38) | .631 |
| CESD score | 1.09 (1.05-1.14) | .000 | 1.07 (1.04-1.10) | .000 | 1.05 (1.03-1.08) | .000 |
| AIC | 733.77 | 733.00 | 735.07 | |||
Note: β (95%CI) = Odds ratio (95% confidence interval). AIC = Akaike Information Criterion. Heart = heart disease. High cholest. = high cholesterol. WHR = waist-hip ratio1 Model with 10-item Total CES-D score: χ2(12) = 76.026 p < .001, Nagelkerke R2 = 13.3%.,2 Model with 14-item Total CES-D score: χ2(12) = 77.305, p < .001, Nagelkerke R2 = 13.5%. 3 Model with 20-item Total CES-D score: χ2(12) = 74.900, p < .001. Nagelkerke R2 = 13.1%.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



