
Submitted:
23 November 2023
Posted:
24 November 2023
You are already at the latest version
Abstract
Background: Antibiotic-containing carrier systems are one option that offers the advantage of releasing active ingredients over a longer period of time. In vitro sustained drug release from a carrier system consisting of microporous β-TCP ceramic and alginate has been reported in previous works. Alginate dialdehyde (ADA) gelatin gel showed both better mechanical properties when loaded into a β-TCP ceramic and higher biodegradability than pure alginate. Methods: Dual release of daptomycin and BMP-2 was measured on days 1, 2, 3, 6, 9, 14, 21, and 28 by HPLC and ELISA. After release, the microbial efficacy of the daptomycin was verified and the biocompatibility of the composite was tested in cell culture. Results: Daptomycin and the model compound FITC protein A (n=30) were released from the composite over 28 days. A Daptomycin release above the minimum inhibitory concentration (MIC) by day 9 and a burst release of 71.7 ± 5.9 % were observed in the loaded ceramics. Low concentrations of BMP-2 were released from the loaded ceramics over 28 days.
Keywords:
dual release
; daptomycin
; BMP-2
; β-TCP scaffold
; ADA-gelatin gel
; bone infection
; bone regeneration
1. Introduction
Osteomyelitis is an inflammation of the bone that usually affects the bone (osteitis), the bone marrow (osteomyelitis), and the periosteum (periostitis) [1]. The adjacent soft tissue may also be impacted. This condition is instigated by various microorganisms, resulting in bone destruction [2]. Etiologically, osteomyelitis is categorized as hematogenous, locally transmitted (per continuitatem), exogenous, and specific [3]. In pediatric cases, hematogenous osteomyelitis predominantly affects long bones, while in adults, it often presents as spondylitis [4]. Infections can originate from sources such as common skin infections or contamination during intravenous drug administration, leading to hematogenous dissemination into the bone and subsequent osteomyelitis [5]. Staphylococcus aureus (S. aureus) is the primary causative agent for primary hematogenous and locally transmitted osteomyelitis [5]. Notably, in implant-associated infections, small colony variants (SCV) of Staphylococcus and coagulase-negative Staphylococcus should be considered [6]. Osteomyelitis can be initially classified into acute and chronic forms based on the infection duration or histological inflammation type [7]. Chronic osteomyelitis is identified when the causative agent persists for more than 6 weeks, although the distinction may be nuanced [3]. Conversely, the presence of sequestra on CT or MRI serves as a definitive criterion for chronic infection [4]. Sequestra refers to necrotic bone fragments rejected by healthy tissue, hindering infection resolution [8]. The usual therapy consists of debridement, i.e. surgical removal of the infected tissue, and systemic antibiotic therapy [9] tailored to the specific pathogen. Local antibiotic therapy is much more effective [10] and is sometimes already applied with the use of gentamicin-loaded PMMA chains (Septopal®)[11]. The disadvantage, however, is that they have to be removed again in a second surgical procedure and, in addition, a not inconsiderable proportion of the antibiotics remains in the PMMA [12] because it is biodegradable. A wide variety of processes have already been described for loading porous ceramics with additives such as antibiotics and pharmaceuticals. The manner in which these agents are loaded is especially critical for their release. One can spray the active substances onto the surface. In addition, regardless of the manufacturing process, it is possible to incubate the ceramics for a certain time in an aqueous solution containing antibiotics. [13,14,15,16,17,18]. Droplet loading, in which the ceramic is not immersed in a solution but the active ingredient solution is applied to the ceramic via a drip process, is another option [19]. These procedures have in common that a subsequent drying phase is necessary, this can include several procedures: in an oven with a temperature of max. 50°C to avoid the destruction of the antibiotics [15,16,20], both air and vacuum drying [21,22,23,24] are described in the literature. As the load is adhesive, these methods are usually applied for short-term drug release [25]. To prolong the release, the active ingredients can be encapsulated, as is done in the pharmaceutical industry in the production of tablets and capsules. For this purpose, a layer is applied as a diffusion barrier after the loading process. This can be done by dipping, dropping or spraying [26]. The literature has previously documented a delayed in vitro drug release from a carrier system [27], comprising microporous β-TCP ceramic and alginate [28,29,30,31]. Comparatively, ADA gelatin gel has exhibited superior mechanical properties when incorporated into β-TCP ceramic and demonstrated higher biodegradability than pure alginate [32]. Given its prior assessment for drug release [31,33], ADA gelatin gel emerges as a promising hydrogel for targeted and controlled drug delivery. Notably, the potential for dual drug release in this system remains unexplored, representing an avenue for enhancing patient outcomes by combining anti-infective treatment, bone growth promotion therapy, and improved bone stability facilitated by the β-TCP ceramic.
2. Materials and Methods
2.1. Preparing the microporous β-TCP ceramics
The described ceramics were manufactured according to the previously outlined procedure [34,35,36,37]. A mixture of 80 g α-tricalcium phosphate and 20 g tricalcium phosphate (Art. No. 102143, Merck, Darmstadt, Germany; a blend of apatite and calcium hydrogenphosphate) was combined with 60.0 ± 0.2 g of a solution containing 0.2M Na2HPO4 (Art. No. S9763, >99%, Sigma Aldrich, St. Louis, USA) and 1% polyacrylic acid (Art. No. 81132, Fluka, Hannover, Germany; Mw = 5.1 kDa). The mixture was stirred at 2000 rpm using a four-wing impeller for 45s (Eurostar Digital, IKA, Staufen, Germany), and the resulting paste was poured into plastic syringes after removing their tips (Ø = 23 mm). After 45 minutes of hardening, the paste was covered with 10 mL of PBS 7.4 solution (Art. No. P5368, Sigma, St. Louis, USA) and incubated at 60 °C for 3 days. The samples (Ø = 23 mm; L = 70 mm) were then dried at the same temperature and sintered at 1250 °C for 4 hours, with heating and cooling occurring at a rate of 1 °C per minute. The cylinders were subsequently trimmed to a length of 26 mm and a diameter of 7 mm. Finally, the ceramics were washed overnight in ethanol (Art. No. , 98%, Fluka, Hannover, Germany) to eliminate residual particles and calcined at 900 °C to eliminate all organic residues. Before usage, the ceramics were shortened to cylinders with a length of 6 mm and washed again. The samples underwent sterilization in a drying oven (Memmert UN55, Memmert, Schwabach, Germany) at 200 °C for 4 hours.
2.2. Characterization of the microporous β-TCP ceramics
The characterization procedures closely mirrored those detailed in prior publications [30,38]. The structural and pore size analyses were conducted using Environmental Scanning Electron Microscopy (ESEM) (FEI Quanta 250 FEG, Hillsboro, USA), Micro-computed Tomography (µCT) (Scanco Micro-CT 50, Brüttisellen, Switzerland), and porosimetry (Porotec Pascal 140/440, Hofheim, Germany). ESEM operated at an accelerating voltage of 10 kV, while µCT parameters were set at 90 kV, 4 W, 44 µA, with a resolution of 2 µm and an integration time of 5000 ms. Porosimetry, performed using the Pascal 140 instrument, covered pore sizes ranging from 1000 µm to 1.4 µm, with a pressure increase to 0.1 kPa. The Pascal 440 porosimeter addressed pore sizes from 1.4 µm to 1.8 nm, with a pressure increase to 400 MPa. To determine the composition of the ceramics, Energy-Dispersive X-ray Spectroscopy (EDX) was employed (Oxford Instruments, Abingdon, UK), with an accelerating voltage of 12 kV and a measurement time of 100 s (live time-corrected). X-ray Diffraction (XRD) analysis was carried out using Bragg-Brentano geometry equipped with a Cu anode, secondary graphite monochromator, scintillation counter, 40 kV/40 mA, 1°2-theta/min, and a step size of 0.02°2theta.
2.3. Preparation and Characterization of the ADA-gelatin hydrogels
Gelatin and alginate were sterilized by using low temperature hydrogen peroxide gas plasma sterilization (pressure 63.3 Pa; temperature 50°C; diffusion time 8 min; plasma time 4 min; H2O2 concentration 6 wt%; peroxyacetic acid 1 wt%)[39]. The fabrication of alginate di-aldehyde (ADA) was carried out as already described by us elsewhere [38]. Daptomycin hydrochloride (Cubicin 500mg Daptomycin i.v.; MSD Sharp&Dohme; PZN 06708869) was dissolved together with gelatin in a final concentration after mixing ADA and gelatin 1:1 together of 50 mg/mL. 1.5 g ADA from plasma-sterilized alginate were dissolved in 600 µl BMP stock solution (equivalent to 300 µg BMP-2) and 29.4 mL PBS.
2.3.1. Gel permeation chromatography (GPC)
GPC analysis was conducted to ascertain the molar mass distribution and mean molar masses of the employed alginate, ADA, and gelatin. A 20 mg sample was dissolved in 10 mL of the eluent over two days at room temperature. Prior to measurement, the solutions underwent filtration through a PTFE filter membrane with a porosity of 1 µm. Calibration involved the use of various pullulan standards in the separation area of the column combination (PSS Suprema 10 µm pre-column, ID 8.0 mm x 50 mm; PSS Suprema 10 µm, 100 Å, ID 8.0 mm x 300 mm; PSS Suprema 10 µm, 3000 Å, ID 8.0 mm x 300 mm; PSS Suprema 10 µm, 3000 Å, ID 8.0 mm x 300 mm (PSS, Mainz, Germany)). As eluent, 0.02 M phosphate buffer at pH of 6.6 and 0.5 M NaCl aq. was used.
2.3.2. Rheology
Rheological investigations were conducted using the Malvern Kinexus lab+ KNX2110 rheometer (Malvern, UK). The cone plate (CP1/40 SR3033 SS) employed had a diameter of 40 mm and an angle of 1°, with a distance to the fixed plate (PLS40 S2345 SS) set at 23 µm. The measurements, employing a frequency ramp, were carried out with a shear strain of 1% and at a temperature of 25 °C within the range of 0.02 Hz to 16 Hz. The measurements were performed for ADA and gelatin gels separately, as well as for ADA-gelatin (with/without daptomycin and BMP-2). 1 mL of gel was applied to the plate. After moving the plates together until the gap width was reached, any gel that escaped laterally was wiped off with cellulose.
2.4. Loading the microporous β-TCP ceramics
The loading principle developed by Seidenstuecker [28] using a flow chamber was used and 6 chambers were connected in parallel to the vacuum pump (KNF Neuberger SC920, Freiburg, Germany) so that several ceramics could be loaded at the same time. After the loading process, the ceramics were placed in 30 mM CaCl2 (Sigma Aldrich, St. Louis, USA) solution for crosslinking. The CaCl2 solutions also contained the same concentration of daptomycin and/or BMP-2 as in the gel. The distribution of the gel in the ceramic has already been measured in a previous work [30,38] using fluorescein and fluorescence microscopy. Therefore, we have not done so here.
2.5. Release experiments
The ceramics containing the load were reweighed and transferred to 5 mL vials following the same procedure as the unloaded negative controls. They were then covered with 3 mL of distilled water and positioned in a warming cabinet, shielded from light, at 37 °C for a duration of 28 days. On days 1, 2, 3, 6, 9, 14, 21, and 28 post-experiment, the ceramics were relocated to a new 5 mL vial containing fresh distilled water, while the previous vial was frozen at −20 °C.
2.6. Determination of the release kinetics of daptomycin and BMP-2
Each sample was thawed and subjected to sterile filtration using 0.2 µm disposable filters (Chromafil Xtra H-PTFE-20/25, Art. No. 729245, Macherey-Nagel, Düren, Germany). The antibiotic concentration in the samples was assessed through High-Performance Liquid Chromatography (HPLC), while the BMP2 content was determined using Enzyme-Linked Immunosorbent Assay (ELISA).
2.6.1. HPLC
Daptomycin determination using High-Performance Liquid Chromatography (HPLC) was performed with the Shimadzu CBM-20A, CTO-20AC, DGU-20A5R, LC-20ADXR, Reservoir Tray, RF-20A, SIL-30AC, SPD-M20A IVDD system from Kyoto, Japan. The Macherey-Nagel precolumn (EC 4/3 Nucleodur 300-5 C4ec) and column (EC 250/3 Nucleodur 300-5 C4 ec) from Düren, Germany, were employed. The analysis was conducted at a temperature of 25 °C with a running time of 15 minutes, 1 mL/min flow rate and λ = 221 nm. ACN and 25.08 mM Na2HPO4 (pH 5.5) in 30:70 ratio was used as mobile phase.
2.6.2. ELISA
ELISA was conducted utilizing Sino Biological's Human BMP-2 ELISA Kit (Art. No. KIT10426, Beijing, China) following the provided manufacturer's guidelines. The kit included a 96-well plate coated with the capture antibody. After three washes with 300 µl wash buffer, 100 µl of each release sample was carefully dispensed into the wells. Additionally, a BMP-2 standard (0–2500 pg/mL) was prepared and treated similarly to the samples. Both the samples and the standard were completely aspirated within 15 minutes and left to incubate for 2 hours at room temperature. Following three more washes, 100 μl of the detection antibody was added and allowed to incubate at room temperature for 1 hour. Subsequently, the wells were washed three times, and 200 µl of the substrate solution was dispensed into each well. After a 20-minute incubation at room temperature in the dark, the color reaction was halted by adding 50 µl of the stop solution.
2.7. Biocompatibility
All cell culture experiments were performed with MG-63 cells (ATCC-CRL 1429). In addition, the ceramics used for the cell culture experiments were sawn to a thickness of 2mm and filled with ADA-gelatin as described before. The Live-Dead assay (PromoCell Live/Dead Cell Staining Kit II, Art. No. PK-CA70730002, Heidelberg, Germany), WST-1 assay (Roche Cell Proliferation Reagent WST-1, Art. No. 11644807001, Basel, Switzerland), and LDH assay (Roche Cytotoxicity Detection Kit (LDH), Art. No. 11644793001, Basel, Switzerland) were conducted in accordance with the manufacturer's instructions. For the live-dead assay, 20,000 cells were used per sample, while 50,000 cells per sample were employed for both the WST-1 and LDH assays.
2.8. Anti-microbial activity
To demonstrate that the antibiotics used were still microbially effective after 28 days, their minimum inhibitory concentration was determined. For this purpose, ISO Standard 20776-1 and EUCAST [40] were followed. Samples from release days 1, 2, 3, 6, 9, 14, 21, and 28 of daptomycin BMP-2 release were tested. The exact procedure is already described elsewhere [30,38]. Defined dilutions of each concentration (original concentration as well as 4 above and 4 below the MIC) were prepared which were then tested for MIC in a microtiter experiment with S. aureus (ATCC 29213).
2.9. Statistics
The data was expressed as mean ± standard deviation and subjected to analysis using one-way analysis of variance (ANOVA). The comparison of means was conducted using Fisher LSD. The level of statistical significance was established at p < 0.05. All calculations were carried out using OriginPro 2022 SR1 from OriginLabs in Northampton, MA, USA.
3. Results
3.1. Characterization of the microporous β-TCP
The mean pore size of the ceramics was determined to be 4.9 ± 0.4 µm and a total porosity of 45 ± 4 % using scanning electron microscopy and porosimetry. The EDX shows a Ca/P ratio of 1.48, which identified the sample as β-TCP. The XRD measurement confirmed the result with the subsequent Rietveld refinement analysis (Profex 4.3., www.profex.org, Freeware). 99.5% β-TCP and traces of calciumpyprophpshate (CPP) from the manufacturing process could be detected. We came to similar conclusions in other studies of β-TCP [30,32,38] (pls. see Figure 1).
3.2. Characterization of the ADA-gelatin gel
Both alginate and gelatin show no changes in molecular weight before and after plasma sterilization. Unsterile ADA as well as ADA prepared from sterile alginate also show similar values Mn 52–55 kDa; Mw 298–320 kDa; Mz 1150–1300 kDa. The greatest differences can be observed in ADA that has been plasma sterilized after preparation. The values for Mn decrease from the range 50 kDa (before) to 7–13 kDa (after). PDI (Mw/Mn) halves from 5–6 to 2–3. The Table 1 below shows an overview of the plasma-sterilized gels. It becomes clear that the influence of the sterilization process on the gelatin and alginate is not as great as on ADA.
The complex viscosity of the ADA was found to be 0.2 ± 0.02 Pa∙s independent of the frequency. The shear viscosity of gelatin, on the other hand, was very strongly dependent on the frequency (3 Pa∙s at 1 Hz, 50 Pa∙s at 0.1 Hz and 0.3 Pa∙s at 10 Hz).
3.3. Release kinetics of dual release of daptomycin and BMP-2
The release of daptomycin and BMP-2 out of the composite showed a burst release of 71.7 ± 5.9% for daptomycin, but only 4.8 ± 7.1% for BMP-2, based on the amount of active agent released over the entire study period (see Table 2). According to Diederen et al. [41] this concentration lies within the MIC (0.125–1 mg/l) against S. aureus. Based on the initial weight during production, 105.13 ± 9.14% daptomycin was released, i.e. the entire initial weight, but only 0.72 ± 0.16% BMP-2.
3.4. Biocompatibility
In live/dead staining, living cells predominated with 65–78% on days 3, 7 and 10. The empty ceramic as control showed 89–96%, whereas ceramics with ADA/gelatin (control 2) showed 82–97% live cells. An overview of the results is shown in Table 3. We introduced the intermediate section because there were cells that were stained both green and red and were clearly not dead in the microscopy.
Cell proliferation of MG-63 cells on the composites of ADA-gelatin and daptomycin and BMP-2 was decreased compared to controls (empty TCP) and TCP with ADA/gelatin. In addition, proliferation was approximately constant over the study period, whereas it increased in both the empty ceramics and the ADA/gelatin-filled ceramics (see Figure 2a).
In terms of cytotoxicity, both controls (empty TCP, gel-filled TCP) showed similar values to the negative control (cells only) in the range of 0% (negative values also correspond to 0%) over the 3-day study period. The composite with daptomycin and BMP-2 showed almost constant values of 19–22% (see Figure 2b).
3.5. Antimicrobial activity
The MIC for daptomycin BMP-2 release ranged from 0.475 to 1 mg/l (see Table 4). For release days 14 to 28, no antimicrobial activity was detected. The inoculum control (GC) provided a bacterial concentration of 7 x 105 mL-1.
4. Discussion
Both EDX and XRD showed that the RMS ceramic consisted of β-TCP. Rietveld refinement analysis also confirmed this. In ESEM, µCT and porosimetry the pore structure could be verified (requirement ca 5µm pore diameter). These findings were in agreement with existing work on the ceramic. Rietveld refinement analysis also confirmed this [30,32,42]. Previous works have also successfully shown that the ceramic is very well integrated into the bone and degrades completely over time [34,43].
GPC measured a molar mass of 198 kDa for alginate and 52.4 kDa for ADA. Sarker et al. [44] determined the molar masses of alginate and ADA via their viscosities. This resulted in 422.3 ± 5.3 kDa for alginate and 185.5 ± 2.8 kDa for ADA, significantly lower molar masses than those determined via GPC in this work. This again showed the wide variation in the batches of alginate used, although the same alginate with the same order number from Sigma was used in both papers. In loading experiments by Seidenstücker et al. [30] performed with similar procedures, alginate with a molar mass Mn of 93 ± 18 kDa determined in GPC was used; before plasma sterilization, this value was 343 ± 45 kDa. Again, the molar mass of the alginate was higher than that of the alginate used in this work. It is worth noting that in the study by Seidenstuecker et al. [30], the molar mass of alginate underwent a significant reduction with plasma sterilization, whereas in our current investigation, plasma sterilization had minimal impact on the molar mass of alginate. This highlights that low-temperature hydrogen peroxide gas/plasma sterilization proves to be a gentler process. In a comparable loading procedure described in the literature, a 2.5% alginate gel required approximately 10 ± 3.1 minutes for complete loading of the ceramics [28]. Rheological analysis revealed a complex viscosity of 0.35 Pa∙s at a frequency of 10 rad/s (= 1.6 Hz). In our present work, the complex viscosity of the ADA gelatin gel at the same frequency increased from 0.09 Pa∙s to 0.16 Pa∙s after 10 minutes and reached 0.5 Pa∙s after 30 minutes during an exemplary crosslinking (measurement 1). Despite slight differences in measurement parameters, this resulted in a comparable expected loading time for the ADA gelatin gel. In comparison with another study [45], where both the gel preparation and rheological measurement parameters aligned, a significantly longer crosslinking time was observed. In Sarker et al. [45], this time was reported as 8.2 minutes, while in our current work, it was at least 43 minutes. The burst release of daptomycin at 71% is significantly greater than comparable results for vancomycin from alginate in a previous work [30]. There, the burst release was only 35.2 ± 1.5%. In contrast to the present work, however, alginate and not ADA gelatin was used. The BMP-2 release was significantly lower than in previous studies and was in the single-digit percentage range, whereas in Kissling’s [29] case 45.4% released within the first 48h.
The percentage of live cells on daptomycin and BMP-2-containing hydrogel was between 10–20% lower than on the blank ceramic. In comparison to this, the ADA-gelatin loaded ceramic showed a lower percentage of live cells of 5–20%. Nevertheless, the cytotoxicity measurements showed little difference from other work with CDHA [46]. The differences are due to the effects of BMP-2 concentration, as also seen in cell proliferation [29]. However, there is a habituation effect after 1 week with increasing numbers of living cells.
The concentrations of daptomycin released were effective against S. aureus for 9 days. Unfortunately, the concentration after 14 days, which was still in the range described by Diederen et al. [41], was no longer effective. EUCAST even demand a significantly higher classification of the MIC with 1 mg/mL [40]. Hall et al [47] described a similar release behavior of daptomycin. They were able to determine a release from PMMA beads over 86.7 ± 7.6 h depending on the initial concentration. However, the burst release also increased linearly with the higher initial concentration and a comparable burst release of 42% was determined as in the present work. Unfortunately, antimicrobial investigations were not carried out by Hall et al. [47]. In the work of Silva at al [48], a release from chitosan nanoparticles was described. However, the release was already completed within 3h. Nevertheless, they were able to determine a similar MIC between 0.5 – 1.0 mg/mL as we did.
However, no conformational changes were observed by us on the daptomycin by means of a shift in the mean transit time or by peak changes, which would indicate a degradation of the daptomycin and a less antimicrobial activity (in presence of BMP-2).
5. Conclusion
The dual release of daptomaycin and BMP-2 occurred over 28 days from the composite of microporous ceramic and ADA gelatin gel developed by us as the active carrier. The antimicrobial activity was also 9 days. Compared with previous release tests using nanoparticles (in the hour range) or PMMA (3 days), the new method is clearly superior despite the reduced antimicrobial activity. Nevertheless, further improvements are possible by using other gels, e.g. modified collagen gels, which would be completely biodegradable.
Author Contributions
Conceptualization, M.S.; methodology, M.S.; software, M.S., H.S.; validation, L.R., P.S. and M.S.; formal analysis, L.R.; investigation, L.R. and P.S.; resources, H.S.; data curation, L.R. and M.S..; writing—original draft preparation, M.S. and L.R..; writing—review and editing, M.S. and L.R..; visualization, L.R.; supervision, M.S.; project administration, M.S:; funding acquisition, M.S. All authors have read and agreed to the published version of the manuscript
Funding
This research was funded by German Research Foundation (DFG) grant number 388988890. The article processing charge was funded by the Baden-Württemberg Ministry of Science, Research and Art and the University of Freiburg in the funding program Open Access Publishing.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
The data presented in this article are available on request from the corresponding author.
Acknowledgments
The authors would like to thank the FILK Freiberg for plasma sterilizing our samples and Isabelle Caseley for proof-reading.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lee, Y.J.; Sadigh, S.; Mankad, K.; Kapse, N.; Rajeswaran, G.J.Q.I.i.M.; Surgery. The imaging of osteomyelitis. Quantitative Imaging in Medicine and Surgery 2016, 6, 184-198. [CrossRef]
- Oliveira, T.C.; Gomes, M.S.; Gomes, A.C. The crossroads between infection and bone loss. Microorganisms 2020, 8, 1765. [CrossRef]
- Zimmerli, W. Clinical presentation and treatment of orthopaedic implant-associated infection. Journal of Internal Medicine 2014, 276, 111-119. [CrossRef]
- Hatzenbuehler, J.; Pulling, T.J. Diagnosis and management of osteomyelitis. Am. Fam. Physician 2011, 84, 1027-1033.
- Sia, I.G.; Berbari, E.F. Infection and musculoskeletal conditions: Osteomyelitis. Best practice & research. Clinical rheumatology 2006, 20, 1065-1081. [CrossRef]
- Kapadia, B.H.; Berg, R.A.; Daley, J.A.; Fritz, J.; Bhave, A.; Mont, M.A. Periprosthetic joint infection. Lancet 2016, 387, 386-394. [CrossRef]
- Lew, D.P.; Waldvogel, F.A. Osteomyelitis. Lancet 2004, 364, 369-379. [CrossRef]
- Schmitt, S.K. Osteomyelitis. Infectious disease clinics of North America 2017, 31, 325-338. [CrossRef]
- Fraimow, H.S. Systemic antimicrobial therapy in osteomyelitis. Seminars in Plastic Surgery 2009, 23, 90-99. [CrossRef]
- Gogia, J.S.; Meehan, J.P.; Di Cesare, P.E.; Jamali, A.A. Local antibiotic therapy in osteomyelitis. Semin Plast Surg 2009, 23, 100-107. [CrossRef]
- Blaha, J.D.; Calhoun, J.H.; Nelson, C.L.; Henry, S.L.; Seligson, D.; Esterhai, J.L.J.; Heppenstall, R.B.; Mader, J.; Evans, R.P.; Wilkins, J., et al. Comparison of the clinical efficacy and tolerance of gentamicin pmma beads on surgical wire versus combined and systemic therapy for osteomyelitis. Clinical Orthopaedics and Related Research® 1993, 295,.
- Díez-Peña, E.; Frutos, G.; Frutos, P.; Barrales-Rienda, J.M. Gentamicin sulphate release from a modified commercial acrylic surgical radiopaque bone cement. I. Influence of the gentamicin concentration on the release process mechanism. Chem. Pharm. Bull. (Tokyo) 2002, 50, 1201-1208. [CrossRef]
- Alkhraisat, M.H.; Rueda, C.; Cabrejos-Azama, J.; Lucas-Aparicio, J.; Marino, F.T.; Torres Garcia-Denche, J.; Jerez, L.B.; Gbureck, U.; Cabarcos, E.L. Loading and release of doxycycline hyclate from strontium-substituted calcium phosphate cement. Acta Biomater 2010, 6, 1522-1528.S1742-7061(09)00478-4 . [CrossRef]
- Wisniewska, I.; Slosarczyk, A.; Mysliwiec, L.; Sporniak-Tutak, K. [lincomycin applied to the alveolus on tcp carrier and its effect on wound healing after surgical extraction of a third molar]. Ann Acad Med Stetin 2009, 55, 59-64.
- Silverman, L.D.; Lukashova, L.; Herman, O.T.; Lane, J.M.; Boskey, A.L. Release of gentamicin from a tricalcium phosphate bone implant. J Orthop Res 2007, 25, 23-29. [CrossRef]
- DiCicco, M.; Goldfinger, A.; Guirand, F.; Abdullah, A.; Jansen, S.A. In vitro tobramycin elution analysis from a novel beta-tricalcium phosphate-silicate-xerogel biodegradable drug-delivery system. J Biomed Mater Res B Appl Biomater 2004, 70, 1-20. [CrossRef]
- El-Ghannam, A.; Ahmed, K.; Omran, M. Nanoporous delivery system to treat osteomyelitis and regenerate bone: Gentamicin release kinetics and bactericidal effect. Journal of Biomedical Materials Research Part B: Applied Biomaterials 2005, 73B, 277-284. [CrossRef]
- El-Ghannam, A.; Jahed, K.; Govindaswami, M. Resorbable bioactive ceramic for treatment of bone infection. J Biomed Mater Res A 2010, 94, 308-316. [CrossRef]
- Baradari, H.; Damia, C.; Dutreih-Colas, M.; Laborde, E.; Pécout, N.; Champion, E.; Chulia, D.; Viana, M. Calcium phosphate porous pellets as drug delivery systems: Effect of drug carrier composition on drug loading and in vitro release. Journal of the European Ceramic Society 2012, 32, 2679-2690. [CrossRef]
- Laurent, F.; Bignon, A.; Goldnadel, J.; Chevalier, J.; Fantozzi, G.; Viguier, E.; Roger, T.; Boivin, G.; Hartmann, D. A new concept of gentamicin loaded hap/tcp bone substitute for prophylactic action: In vitro release validation. J Mater Sci Mater Med 2008, 19, 947-951. [CrossRef]
- Song, J.; Xu, J.; Filion, T.; Saiz, E.; Tomsia, A.P.; Lian, J.B.; Stein, G.S.; Ayers, D.C.; Bertozzi, C.R. Elastomeric high-mineral content hydrogel-hydroxyapatite composites for orthopedic applications. J. Biomed. Mater. Res. A 2009, 89, 1098-1107. [CrossRef]
- Sago, T.; Mori, Y.; Takagi, H.; Iwata, H.; Murase, K.; Kawamura, Y.; Hirose, H. Local treatment of dacron patch graft contaminated with staphylococcus aureus with antibiotic-releasing porous apatite ceramic: An experimental study in the rabbit. J Vasc Surg 2003, 37, 169-174. [CrossRef]
- Zhang, Y.; Zhang, M. Calcium phosphate/chitosan composite scaffolds for controlled in vitro antibiotic drug release. J Biomed Mater Res 2002, 62, 378-386. [CrossRef]
- Itokazu, M.; Yang, W.; Aoki, T.; Ohara, A.; Kato, N. Synthesis of antibiotic-loaded interporous hydroxyapatite blocks by vacuum method and in vitro drug release testing. Biomaterials 1998, 19, 817-. [CrossRef]
- Kundu, B.; Soundrapandian, C.; Nandi, S.K.; Mukherjee, P.; Dandapat, N.; Roy, S.; Datta, B.K.; Mandal, T.K.; Basu, D.; Bhattacharya, R.N. Development of new localized drug delivery system based on ceftriaxone-sulbactam composite drug impregnated porous hydroxyapatite: A systematic approach for in vitro and in vivo animal trial. Pharm Res 2010, 27, 1659-1676. [CrossRef]
- Fang, T.; Wen, J.; Zhou, J.; Shao, Z.; Dong, J. Poly (ε-caprolactone) coating delays vancomycin delivery from porous chitosan/β-tricalcium phosphate composites. Journal of Biomedical Materials Research Part B: Applied Biomaterials 2012, 100B, 1803-1811. [CrossRef]
- Kumar Giri, T.; Thakur, D.; Alexander, A.; Ajazuddin; Badwaik, H.; Krishna Tripathi, D. Alginate based hydrogel as a potential biopolymeric carrier for drug delivery and cell delivery systems: Present status and applications. Curr. Drug Del. 2012, 9, 539-555. [CrossRef]
- Seidenstuecker, M.; Kissling, S.; Ruehe, J.; Suedkamp, N.; Mayr, H.; Bernstein, A. Novel method for loading microporous ceramics bone grafts by using a directional flow. J Funct Biomater 2015, 6, 1085. [CrossRef]
- Kissling, S.; Seidenstuecker, M.; Pilz, I.H.; Suedkamp, N.P.; Mayr, H.O.; Bernstein, A. Sustained release of rhbmp-2 from microporous tricalciumphosphate using hydrogels as a carrier. BMC Biotechnol. 2016, 16, 44. [CrossRef]
- Seidenstuecker, M.; Ruehe, J.; Suedkamp, N.P.; Serr, A.; Wittmer, A.; Bohner, M.; Bernstein, A.; Mayr, H.O. Composite material consisting of microporous β-tcp ceramic and alginate for delayed release of antibiotics. Acta Biomater. 2017, 433–446. [CrossRef]
- Schrade, S.; Ritschl, L.; Süss, R.; Schilling, P.; Seidenstuecker, M. Gelatin nanoparticles for targeted dual drug release out of alginate-di-aldehyde-gelatin gels. Gels 2022, 8, 365. [CrossRef]
- Seidenstuecker, M.; Schmeichel, T.; Ritschl, L.; Vinke, J.; Schilling, P.; Schmal, H.; Bernstein, A. Mechanical properties of the composite material consisting of β-tcp and alginate-di-aldehyde-gelatin hydrogel and its degradation behavior. Materials 2021, 14, 1303. [CrossRef]
- Balakrishnan, B.; Jayakrishnan, A.; Kumar, S.S.P.; Nandkumar, A.M. Anti-bacterial properties of an in situ forming hydrogel based on oxidized alginate and gelatin loaded with gentamycin. . Trends Biomater Artificial Organs 2012, 26, 139-145.
- Mayr, H.O.; Klehm, J.; Schwan, S.; Hube, R.; Sudkamp, N.P.; Niemeyer, P.; Salzmann, G.; von Eisenhardt-Rothe, R.; Heilmann, A.; Bohner, M., et al. Microporous calcium phosphate ceramics as tissue engineering scaffolds for the repair of osteochondral defects: Biomechanical results. Acta Biomater. 2013, 9, 4845-4855. [CrossRef]
- Stahli, C.; Bohner, M.; Bashoor-Zadeh, M.; Doebelin, N.; Baroud, G. Aqueous impregnation of porous beta-tricalcium phosphate scaffolds. Acta Biomater. 2010, 6, 2760-2772. [CrossRef]
- Bohner, M.; van Lenthe, G.H.; Grünenfelder, S.; Hirsiger, W.; Evison, R.; Müller, R. Synthesis and characterization of porous -tricalcium phosphate blocks. Biomaterials 2005, 26, 6099-6105. [CrossRef]
- Mayr, H.O.; Hube, R.; Bernstein, A.; Seibt, A.B.; Hein, W.; von Eisenhart-Rothe, R. Beta-tricalcium phosphate plugs for press-fit fixation in acl reconstruction--a mechanical analysis in bovine bone. Knee 2007, 14, 239-244. [CrossRef]
- Ritschl, L.; Schilling, P.; Wittmer, A.; Bohner, M.; Bernstein, A.; Schmal, H.; Seidenstuecker, M. Composite material consisting of microporous beta-tcp ceramic and alginate-dialdehyde-gelatin for controlled dual release of clindamycin and bone morphogenetic protein 2. J. Mater. Sci. Mater. Med. 2023, 34, 39. [CrossRef]
- Voigt, D. Development of a low - temperature sterilization process for thermally unstable medical implants using collagen as example https://www.filkfreiberg.de/forschung-entwicklung/projekte-und-publikationen/projektbibliothek/entwicklung-eines-niedertemperatur-sterilisationsverfahrens-fuer-thermisch-instabile-medizinische-implantate-am-beispiel-von-kollagen (2023-10-23),.
- EUCAST. Breakpoint tables for interpretation of mics and zone diameters. The European Committee on Antimicrobial Susceptibility Testing - EUCAST: Växjö, 2023;
- Diederen, B.M.; van Duijn, I.; Willemse, P.; Kluytmans, J.A. In vitro activity of daptomycin against methicillin-resistant staphylococcus aureus, including heterogeneously glycopeptide-resistant strains. Antimicrob. Agents Chemother. 2006, 50, 3189-3191. [CrossRef]
- Kuehling, T.; Schilling, P.; Bernstein, A.; Mayr, H.O.; Serr, A.; Wittmer, A.; Bohner, M.; Seidenstuecker, M. A human bone infection organ model for biomaterial research. Acta Biomater. 2022, 230-241. [CrossRef]
- Bernstein, A.; Niemeyer, P.; Salzmann, G.; Südkamp, N.P.; Hube, R.; Klehm, J.; Menzel, M.; von Eisenhart-Rothe, R.; Bohner, M.; Görz, L., et al. Microporous calcium phosphate ceramics as tissue engineering scaffolds for the repair of osteochondral defects: Histological results. Acta Biomater. 2013, 9, 7490-7505. [CrossRef]
- Sarker, B.; Rompf, J.; Silva, R.; Lang, N.; Detsch, R.; Kaschta, J.; Fabry, B.; Boccaccini, A.R. Alginate-based hydrogels with improved adhesive properties for cell encapsulation. International Journal of Biological Macromolecules 2015, 78, 72-78. [CrossRef]
- Sarker, B.; Papageorgiou, D.G.; Silva, R.; Zehnder, T.; Gul-E-Noor, F.; Bertmer, M.; Kaschta, J.; Chrissafis, K.; Detsch, R.; Boccaccini, A.R. Fabrication of alginate-gelatin crosslinked hydrogel microcapsules and evaluation of the microstructure and physico-chemical properties. Journal of Materials Chemistry B 2014, 2, 1470-1482. [CrossRef]
- Blankenburg, J.; Vinke, J.; Riedel, B.; Zankovic, S.; Schmal, H.; Seidenstuecker, M. Alternative geometries for 3d bioprinting of calcium phosphate cement as bone substitute. Biomedicines 2022, 10, 3242. [CrossRef]
- Hall, E.W.; Rouse, M.S.; Jacofsky, D.J.; Osmon, D.R.; Hanssen, A.D.; Steckelberg, J.M.; Patel, R. Release of daptomycin from polymethylmethacrylate beads in a continuous flow chamber. Diagn. Microbiol. Infect. Dis. 2004, 50, 261-265. [CrossRef]
- Silva, N.C.; Silva, S.; Sarmento, B.; Pintado, M. Chitosan nanoparticles for daptomycin delivery in ocular treatment of bacterial endophthalmitis. Drug Deliv. 2015, 22, 885-893. [CrossRef]
Figure 1.
Overview of β-TCP characteristics: (a): ESEM Image HFW 46.6 µm (fracture surface); HV: 10 kV; LFD detector @ 100 Pa; (b): µCT of porosity of the β-TCP taken by Scanco Micro-CT 50 at 90 kV, 4 W, 44 µA at a resolution of 2 µm and an integration time of 5000 ms ; (c): Pore size distribution; measurements of the Pascal-140 porosimeter (1000 µm–1.4 µm; pressure increase to 0.1 kPa) in blue and the Pascal-440 porosimeter (1.4 µm–1.8 nm; pressure increase to 400 MPa) in purple (Porotec Pascal 140/440, Hofheim, Germany); (d): XRD pattern of the TCP (Bruker D8 Advance, Billerica, USA; Bragg-Brentano geometry; Cu anode; secondary graphite monochromator; scintillation counter; 40 kV/40 mA; 1°2-theta/ min; step size 0.02°2theta) and Rietveld Refinement with Profex 4.3.
Figure 1.
Overview of β-TCP characteristics: (a): ESEM Image HFW 46.6 µm (fracture surface); HV: 10 kV; LFD detector @ 100 Pa; (b): µCT of porosity of the β-TCP taken by Scanco Micro-CT 50 at 90 kV, 4 W, 44 µA at a resolution of 2 µm and an integration time of 5000 ms ; (c): Pore size distribution; measurements of the Pascal-140 porosimeter (1000 µm–1.4 µm; pressure increase to 0.1 kPa) in blue and the Pascal-440 porosimeter (1.4 µm–1.8 nm; pressure increase to 400 MPa) in purple (Porotec Pascal 140/440, Hofheim, Germany); (d): XRD pattern of the TCP (Bruker D8 Advance, Billerica, USA; Bragg-Brentano geometry; Cu anode; secondary graphite monochromator; scintillation counter; 40 kV/40 mA; 1°2-theta/ min; step size 0.02°2theta) and Rietveld Refinement with Profex 4.3.
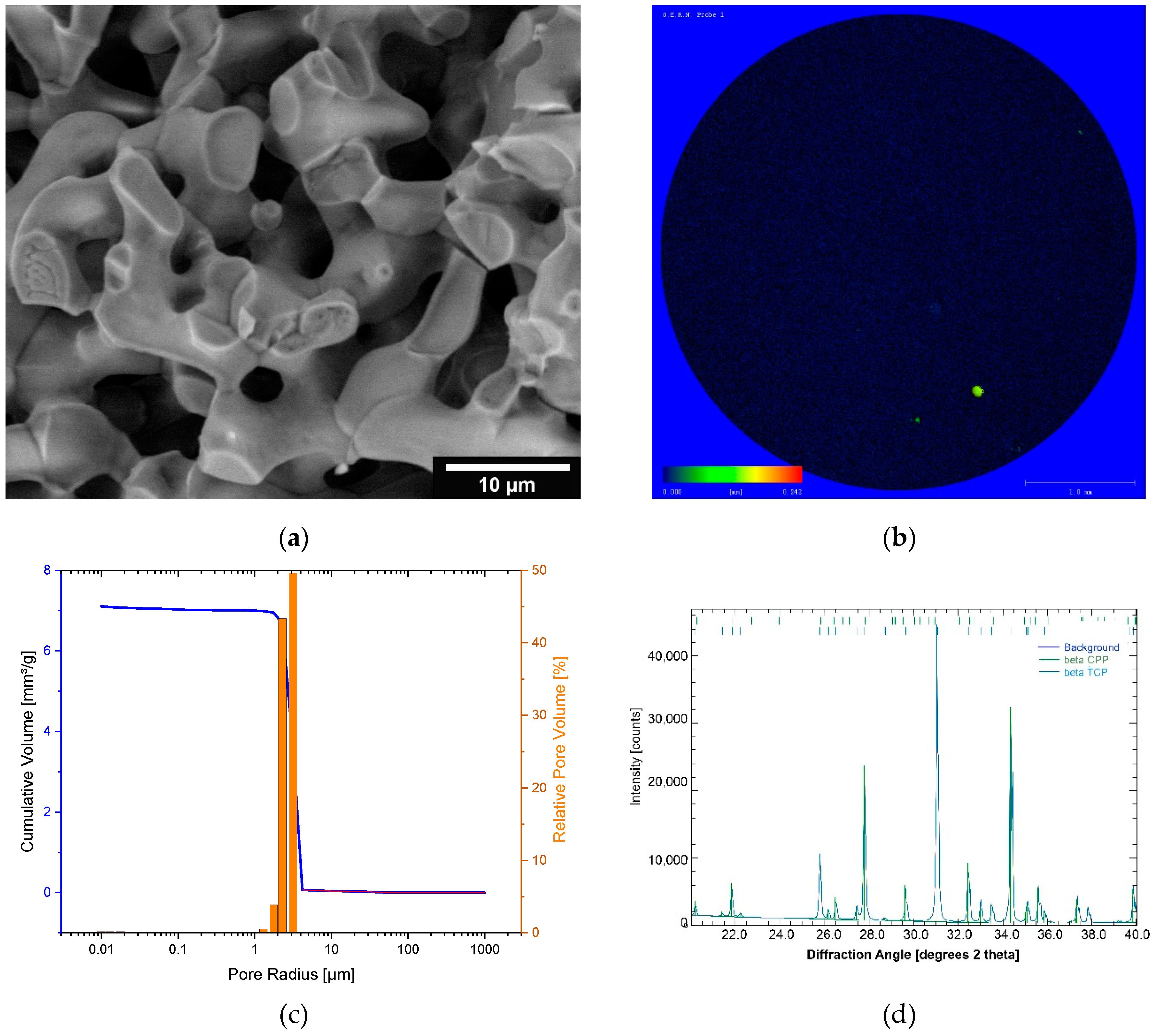
Figure 2.
Overview cell viability (a) and cytotoxicity (b).
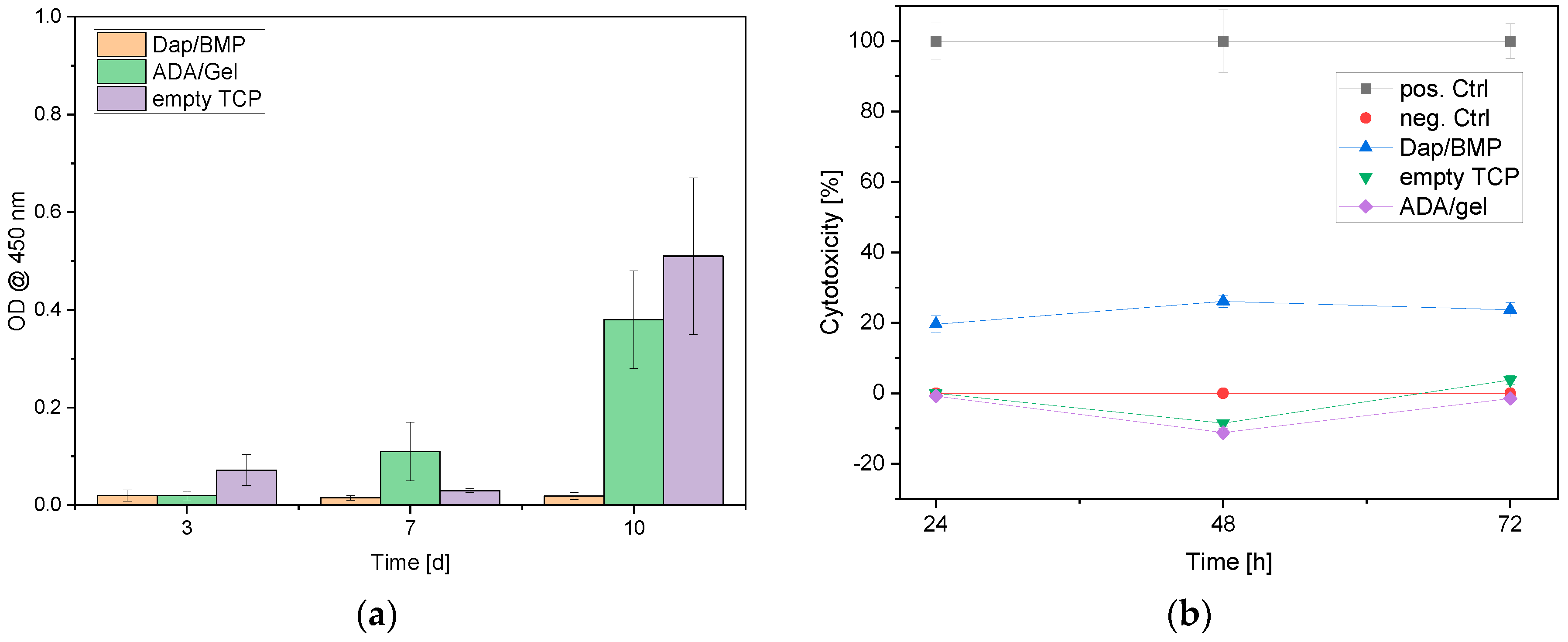

Table 1.
Molecular weights of alginate, ADA and gelatin at different times in the sterilization process; [n=3].
Table 1.
Molecular weights of alginate, ADA and gelatin at different times in the sterilization process; [n=3].
| Sample | Mn [kDa] | Mw [kDa] | Mz [kDa] | PDI (= Mw/Mn) |
|---|---|---|---|---|
| Alginate before plasma sterilization | 198 ± 23 | 729 ± 89 | 1440 ± 99 | 3.68 |
| Alginate after plasma sterilization | 201 ± 18 | 767 ± 57 | 1530 ± 187 | 3.81 |
| ADA unsterile | 52.4 ± 6,8 | 316 ± 26 | 1280 ± 111 | 6.03 |
| ADA out of plasma-sterile alginate | 55.3 ± 5.3 | 298 ± 17 | 1160 ± 53 | 5.38 |
| ADA out of unsterile alginate, plasma sterilized after manufacturing | 6.91 ± 0.87 | 17.8 ± 2.1 | 39.8 ± 2.5 | 2.57 |
| ADA out of plasma-sterile alginate and plasma sterilized again after manufacturing | 13.1 ± 1.4 | 41 ± 9 | 116 ± 12 | 3.13 |
| Gelatin before plasma sterilization | 16.3 ± 2.7 | 114 ± 9 | 254 ± 22 | 6.99 |
| Gelatine after plasma sterilization | 15.9 ± 3.3 | 105 ± 8 | 231 ± 16 | 6.61 |
Table 2.
Overview of released daptomycin and BMP-2 concentrations.
| Release period [d] | Daptomycin-Release [µg/mL] | BMP-2 Release [ng/mL] |
|---|---|---|
| 1 | 1026.05 ± 84.28 | 59.80 ± 90.0 |
| 2 | 318.01 ± 34.85 | 101.86 ± 92.04 |
| 3 | 72.43 ± 48.64 | 669.00 ± 148.40 |
| 6 | 8.62 ± 2.65 | 208.96 ± 43.20 |
| 9 | 2.76 ± 0.18 | 71.54 ± 47.63 |
| 14 | 1.45 ± 1.30 | 148.31 ± 100.86 |
| 21 | 0.37 ± 0.98 | 1.75 ± 6.14 |
| 28 | 0.18 ± 0.67 | 2.63 ± 9.15 |
| Recovery [%]: | 105.13 ± 9.14 | 0.72 ± 0.16 |
Table 3.
Relative cell counts MG-63 cells on composite vs empty ceramics.
| Sample | Relative cell count [%] | ||
| Alive | Intermediate | Dead | |
| Day3 | |||
| Dap/BMP-2 | 74.85 ± 48.16 | 5.56 ± 2.82 | 19.59 ± 9.08 |
| Control (empty ceramics) | 95.93 ± 14.21 | 0 ± 0 | 4.07 ± 1.20 |
| Control 2 (ADA/Gel no drugs) | 96.48 ± 31,22 | 0 ± 0 | 3.52 ± 1.93 |
| Day 7 | |||
| Dap/BMP-2 | 65.83 ± 27.14 | 0 ± 0 | 34.17 ± 23.41 |
| Control (empty ceramics) | 93.53 ± 11.33 | 0 ± 0 | 6.47 ± 1.48 |
| Control 2 (ADA/Gel no drugs) | 82.95 ± 31.48 | 0 ± 0 | 17.05 ± 4.80 |
| Day 10 | |||
| Dap/BMP-2 | 77.41 ± 63.13 | 0 ± 0 | 22.59 ± 22.97 |
| Control (empty ceramics) | 89.07 ± 53.61 | 0 ± 0 | 10.93 ± 3.84 |
| Control 2 (ADA/Gel no drugs) | 82.79 ± 27.79 | 0 ± 0 | 17.21 ± 10.67 |
intermediate = cells that were stained both green and red and were clearly not dead in the microscopy.
Table 4.
Overview of the antimicrobial activity of the released Daptomycin exemplary on one sample.
| Sample | Dilution levels of the original concentration [mg/l] | ||||||||||||
| 16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | 0.031 | GC | EW | MIC | |
| Control | - | - | - | - | - | - | +++ | +++ | +++ | +++ | +++ | - | 0.5 |
| 1291 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | 0.031 | GC | EW | MIC | |
| D1P1 | - | - | - | - | - | - | +++ | +++ | +++ | +++ | +++ | - | 0.5 |
| 308 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | 0.031 | GC | EW | MIC | |
| D2P1 | - | - | - | - | - | - | +++ | +++ | +++ | +++ | +++ | - | 0.5 |
| 110.5 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | 0.031 | GC | EW | MIC | |
| DT3P1 | - | - | - | - | - | +++ | +++ | +++ | +++ | +++ | +++ | - | 1 |
| 18.59 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.063 | 0.031 | GC | EW | MIC | |
| D6P1 | - | - | - | - | - | - | +++ | +++ | +++ | +++ | +++ | - | 0.5 |
| - | 0.95 | 0.475 | 0.238 | 0.119 | 0.059 | 0.03 | 0.015 | 0.007 | 0.004 | GC | EW | MIC | |
| D9P1 | / | - | - | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | - | 0.475 |
| - | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | GC | EW | MIC | |
| D14P1 | / | ++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | - | > 0 |
| - | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | GC | EW | MIC | |
| D21P1 | / | ++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | - | > 0 |
| - | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | GC | EW | MIC | |
| D28P1 | / | ++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | - | > 0 |
D1…D28 = day 1 …28; GC = growth control, only bacteria; EW = empty well; (-) no growth; (+) growth; (++) strong growth; (+++) very strong growth.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



