
Submitted:
21 September 2023
Posted:
22 September 2023
You are already at the latest version
Abstract
Instrumental activities of daily living (IADL) training is critical in clinical practice of occupational therapy (OT) for stroke patients. In the conventional approaches, the therapists simulate various occupational tasks in their healthcare settings or reach their nearby real circumstances for the training. As an alternative technology, immersive virtual reality (IVR) has been used widely in stroke rehabilitation for years; however, limited research has compared occupational performances between virtual and real environments. Our team has established a novel IVR shopping training system for stroke rehabilitation. We recruited 10 stroke patients from our department to test the system. All patients attempted to implement shopping tasks in the virtual and real environments respectively. The Wilcoxon test showed no significant differences between virtual and real environments in memory capacity and time-consuming for implementing tasks, and memory capacities in virtual and real environments presented excellent correlations with the IADL assessment. This study suggests that IVR shopping tasks can be used as an alternative approach in rehabilitation when there is limited resource for implementing shopping training in a real environment, while the psychometric property, clinical effect and the effect transferred to the real environment induced by virtual training require further study.
Keywords:
Instrumental activities of daily living
; immersive virtual reality
; Occupational performance
1. Introduction
Stroke rehabilitation concerns body function, activities, participation, and environmental and personal factors based on the framework of the International Classification of Functioning, Disability and Health (ICF) [1]. The occupational performances in the instrumental activities of daily living (IADL) are critical areas in the activities of ICF domains [2]. Occupational therapists assess and promote the performances of IADL through questionnaires or observation in real environments, such as the Functional Activities Questionnaire (FAQ) [3] and Lawton Index (LI) [4]. The consistency between the subjective questionnaire and observation is challenging, furthermore, some training contents of IADL are difficult to implement in general hospitals and rehabilitation settings because of limited human resources and instruments, for instance, shopping, public transportation, and spatial orientation in the community. Occasionally, the patients could reach nearby real environments for assessment and training under the supervision of occupational therapists.
Virtual reality (VR) technology has been used widely in stroke rehabilitation for some years [5]. Previous studies demonstrated that VR was popular in the rehabilitation of upper extremity [6], lower extremity [7], cognition [8], psychology[9], et al. Most of these studies employed commercial VR games or trained body function through intensive and repetitive practice. IADL assessment and training are full of challenges in real environments, and VR could be an alternative technology for overcoming these limitations. Son and Park presented that cognitive training based on VR could benefit mild cognitive impairment (MCI) and Alzheimer’s disease patients in IADL [10]. Moreover, these studies separated the results of neither immersive and non-immersive VR, nor commercial and serious games, the evidence could be influenced negatively. Since these technologies tend to use varied manners of human-computer interactions (HCI), immersive VR (IVR) and serious games showed more benefit for stroke patients in upper extremity recovery [6,11].
IVR has more freedom in HCI for system design compared with non-immersive VR. Such as movement patterns during the implementation of IADL could be simulated more naturally in the IVR, the head could be turned to the lateral or rear target, and the user could move in a larger space as usual, while the non-immersive VR requires the user to watch the screen continuously during the interaction [11]. Palacios-Navarro and Hogan found the advantages of IVR in gait, balance and upper extremity rehabilitation, but the interventions were not IADL-related [12]. Compared with the intensive and repetitive training, the distributed and IADL-related training showed significant differences in user experiences, and the occupational performances in IVR could be different from previous studies.
Activities initiated by the patients could be induced by well-designed HCI, however, the feedback in the virtual environments is considerably deficient (most of the VR systems simulate auditory, visual and vibration), and somatosensory simulation is a challenge [5]. Exploring the value of activity in IVR, compared with that in a real environment, is meaningful for this technology used as an alternative approach [13]. Brock and colleagues investigated the movement kinematic and postural control differences by virtual and real golf putting in undergraduate students, the results presented that compared with pure VR, haptic condition promoted the swing kinematics, and the movement pattern in the virtual environment was closer to the performance in the real environment [14]. The findings might be partially supported by the study conducted by Ferroni and colleagues. Remapping of Peripersonal Space could be presented in the real world with somatosensory input, but not in a virtual environment without somatosensory feedback [15]. Nevertheless, the review conducted by Tuena and colleagues concluded that the non-immersive virtual environment showed good suitability for spatial memory in the mild cognitive impairment population, and there was limited study that explored occupational performance in IVR [16]. Implementation of IADL requires multidimensional functions, e.g. cognition, motor, and interaction with the environment, the performances of IADL could be different.
Currently, there is little study comparing occupational performances between IVR and real environments when stroke patients implement IADL. So, this study aimed to compare the occupational performances in virtual and real shopping tasks in stroke patients. We hypothesize that the patients present similar performances in IVR and real environments.
2. Materials and Methods
2.1. Study Design
This preliminary study was based on the cross-sectional study of the clinical flexibility research for our IVR shopping training system. All the patients were recruited from the Department of Rehabilitation Medicine of Shenzhen Hospital, Southern Medical University. We followed the Declaration of Helsinki, and this pilot study was a part of the approved study by the Ethical Committee of the hospital (No. AF/SC-09/01.0). The registration number of this study on the Chinese Clinical Trial Registry is ChiCTR2000041058 (www.chictr.org.cn).
2.2. Inclusion Criteria and Participants
All the patients should meet the criteria as follows, a) completed primary education; b) stable stroke; c) Brunnstrom stages ranged from 3 to 6; d) independent ambulation at least by walk aid; e) MMSE reached 24 or above; and f) can understand the instructions of this study. These patients who met the following items were excluded, a) any discomfort caused by this study; b) cannot sign the information consent form; and c) participating in other studies.
2.3. Outcome measures
In addition to the occupational performances recorded in the virtual and real environments (memory capacity and time-consuming), the following conventional assessments were used as well, including the Mini-mental Status Examination (MMSE), Timed Up and Go Test (TUGT), Modified Barthel Index (MBI), and Lawton Index (LI).
The data related to the virtual environments was recorded by the IVR system, but the performance in real environments was recorded manually. We followed the instructions described in the following studies, the Chinese version of MMSE investigated by Katzman and colleagues [17], the TUGT reported by Mathias and Nayak [18], the Chinese version of the MBI translated by Leung and colleagues [19], and the Chinese version of the LI explored by Tong and colleagues [20].
2.4. Implementation of the shopping tasks
All the patients implemented the shopping tasks in virtual and real environments respectively, and they had enough time to explore the virtual and real environments to eliminate the extra time-consuming for unfamiliar circumstances. Randomized sequence was used for virtual and real environments to reduce the learning effect on occupational performances.
Shopping tasks in virtual environments were delivered by a set of all-in-one immersive head-mounted display. The method to wear the display and the screenshots from virtual environments can be seen in Figure 1 and Figure 2. Several modules were integrated into the virtual shopping, including virtual home, lift, bus, and store (Figure 2). The tasks were arranged randomly in the virtual home after the patients entered the system and set the parameters. The patients had 1 minute to memorize the tasks, including the bus route, the locations of the home, bus station and store, and the goods the patients should buy (photo 1 and 2 of Figure 2). All the patients started by buying 4 goods, and the amount (memory capacity) would be increased or decreased automatically to the extreme number as many as the patients could complete the tasks. The virtual shopping could be implemented several times to figure out the accurate memory capacity. The patients were required to move to the bus station by walking and taking the lift (photo 3, 4 and 5 of Figure 2). The store could be reached by taking the right bus route and getting off at the right bus station (photo 6 and 7 of Figure 2). The patients could go home by the reverse route after they bought goods and settled payment (photo 8 and 9 of Figure 2). The performances throughout the shopping could be shown after the patients arrived home (photo 10 of Figure 2). One research student always stood beside the patients during virtual shopping for safety and fall prevention reasons.
Shopping in a real environment was simulated in our hospital. The patients initiated the shopping tasks from our rehabilitation lab of mix reality on the second floor, and then reached the nearby hospital store on the first floor by lift, just as they did in the IVR shopping training system. The distance between the lab and the store was around 120 meters. The time-consuming for a healthy adult to move in this distance was close to the time-consuming they moved in the virtual environment. There were many goods shelves in the real store, and we used two shelves for this study. The number of the goods and the strategies of increasing and decreasing were the same as the virtual shopping, but the types of the goods were different. Figure 3 shows the flowchart of this study
2.5. Data analysis
Comparisons between virtual and real environments were analyzed by the Wilcoxon test, and the correlations between the assessments and the shopping performances were analyzed by Spearman correlation coefficients.
3. Results
Twelve potential patients were invited to participate in this study. Ten of them completed all the tasks; two of them were excluded (one participant claimed sickness during virtual shopping and another one presented exhaustion during shopping in real environments).
The demographic characteristics of the recruited patients are listed in Table 1. The majority of the patients were male (70%) and had ischemic stroke (90%). Their ages ranged from 14 to 73, and the time since stroke ranged from 1 to 42 months (70% are chronic stages).
Memory capacity and time-consuming showed no significant differences between the performances in virtual and real environments (p=1.000 and p=0.959) according to the Wilcoxon test (Table 2). The same performances in memory capacity were observed with the median values (1st and 3rd quartiles) at 3.50 (3.00, 4.75) and the difference was 0. The medians of the time-consuming in virtual and real environments were 604.50 (549.00, 636.75) and 582.50 (515.50, 611.50) respectively, and the median of the differences was 21.00 (-98.50, 72.50).
The correlations between memory capacity and LI showed excellent relationships in virtual and real environments (ρ=0.806, p=0.005). The time-consuming presented a moderate relationship with the TUGT in the virtual environment (ρ=0.681, p=0.030) and presented a borderline negative correlation with MMSE in real environment (ρ=-0.58, p=0.077).
4. Discussion
The purpose of this study was to compare the occupational performances during implementing shopping tasks between IVR and real environments. The primary parameters focused on were memory capacity and time-consuming for shopping tasks. The preliminary results supported our hypothesis that the occupational performances in these two circumstances are similar.
Exploration of the consistency of occupational performances in IVR and real environments is critical for this new technology used in rehabilitation. Our preliminary data showed no significant difference between IVR and real environments in cognition (memory capacity) and movement (time-consuming) perspectives. Currently, there is limited evidence related to the comparison between IVR and real environments, but a systematic review conducted by Tuena and colleagues showed that spatial memory performances were similar between non-immersive virtual and real environments [16]. The latest review on IVR and real Radial Arm Maze (RAM) reported by Palombi and colleagues concluded that IVR is suitable for navigation training and promoting spatial memory [21]. These findings might indicate that the cognitive performance in IVR is comparable with real environments.
While the movement performance comparison between IVR and real environments requires further research. A study on obstacle avoidance distance conducted by Khenak and colleagues presented that the movement in a real environment was significantly different from IVR (a larger avoidance distance was presented in a real environment) [22]. This study was partially supported by the study done by Brock and colleagues found that motor control (movement kinematic and postural control) in golf putting could be influenced by somatosensory input, and better performance could be observed in real environments [14]. The findings in these two studies might be compared cautiously with our findings, because of the following reasons. Firstly, the patients recruited were varied. We recruited stroke patients, however, the two previous studies recruited healthy adults and undergraduate students. Impaired ambulation could be a critical factor that influences the movement performances and covers the contribution of the difference between different environments. Second, varied systems were employed and different parameters were extracted. We simulated a full route of community shopping and extracted time-consuming as the movement performance, but the two previous studies used indoor navigation and golf putting. Finally, the sample size could be an important element in reducing the power of this study. These findings might suggest that the consistency of movement performances in different virtual environments compared with real environments could present varied outcomes, and could further influence occupational performances.
IADL refers to the integration and performances of body function e.g. cognition and movement [1]. In our study, we found that the correlation between cognition (memory capacity) and IADL (LI) was positive and excellent (r=0.806), and consistent performances were shown in IVR and real environments. This result was partially supported by the study on the predictors of IADL (LI) performance in stroke patients conducted by Ghaffari and colleagues (memory assessed by the Wechsler memory scale correlated with LI moderately) [23]. However, there was no significant correlation between movement (time-consuming) and LI in this study, and a previous study presented that the movement performances assessed by the Motoricity index on the upper and lower extremities showed a moderate correlation with LI [23]. Varied movements observed might lead the conflict. The time-consuming in virtual community ambulation could be influenced by multiple tasks throughout the shopping in this study, while fewer confounders in the previous study affected muscle strength. Currently, there is little study exploring the relationship between the movement and IADL in the virtual environment. The findings might prompt that cognitive performances are comparable in virtual and real environments, and the consistency of movement performances could be varied because of the difference of confounders.
Interestingly, we found that the correlation between the time-consuming and the TUGT in the IVR was moderate and significant (r=0.681, p=0.030), but there was no significance in the real environment. However, a borderline moderate negative correlation was presented between the time-consuming and MMSE in the real environment (r=-0.58, p=-0.077), and no significance could be seen in IVR. The TUGT and MMSE are valid and reliable assessments in ambulation and cognition screening respectively [17,18]. The results might suggest that movement performance (time-consuming) in a virtual environment could be a predictor for the ability to ambulate (but not in the real environment), and cognition (MMSE) could be a critical element that influences movement performance in the real environment (but not in the virtual environment). These conflicts might be attributed to the varied experiences in virtual and real environments, such as less somatosensory input delivered in a virtual environment [14,15].
Limitations of this study include a) a small sample size could influence the power of this preliminary study; b) the public bus route was not used in the real environment, this was a prominent difference between IVR and real environments, and might influence the shopping performance; c) we recruited the stroke patients with better functioning, the wore functioning patients might present different results, so the representativeness of this study could be influenced.
Further research could be explored as follows, a) more findings could be revealed by increasing the sample size; b) different manners of human-computer interaction and data extraction could influence occupational performances and observe different dimensions of occupational performance respectively; c) extend the use of IVR in stroke patients with wore functioning; d) Training effect and the transfer of the gain in IVR to the real environment; e) The benefits IVR in different circumstances, such as home-based, community-based and tele rehabilitation.
5. Conclusions
The occupational performances of stroke patients in IVR and real shopping tasks are comparable in cognition, and IVR might be an alternative approach for assessment and training in IADL when there is limited resource, but the psychometric properties, effect and transfer to the real environment still need further investigation.
Author Contributions
XJW prepared the proposal of this study and drafted the manuscript; YXW revised the manuscript and appointed the patients; DSW implemented the study; PZ and PQ assessed the patients; YYZ and JZ analyzed the data and revised the manuscript; ZBR, HL and YMZ gave comments before analysis of data and revised the manuscript before submission. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Shenzhen Science and Technology Program (No. JCYJ20190814112607443, No. GJHZ20190823115412789, and No. JCYJ20210324134401004), the Medical Research Fund of Guangdong Province (No. A2021041), the Innovation and Entrepreneurship Intern Program for Undergraduate Students (No. 202112121039 and No. S202212121170).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the ethical committee of Shenzhen Hospital, Southern Medical University (No. AF/SC-09/01.0, date of approval: 26th November 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The preliminary data used in this study will be available when any reader requests the corresponding author.
Acknowledgments
The authors acknowledge all the patients who were recruited in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Leonardi, M.; Fheodoroff, K. Goal setting with ICF (International Classification of Functioning, Disability and Health) and multidisciplinary team approach in stroke rehabilitation. In Clinical Pathways in Stroke Rehabilitation: Evidence-based Clinical Practice Recommendations, Platz, T., Ed.; Cham (CH), 2021; pp. 35-56. [CrossRef]
- Kelbling, E.; Ferreira Prescott, D.; Shearer, M.; Quinn, T.J. An assessment of the content and properties of extended and instrumental activities of daily living scales: a systematic review. Disabil Rehabil 2023. [Google Scholar] [CrossRef]
- Pfeffer, R.I.; Kurosaki, T.T.; Harrah, C.H., Jr.; Chance, J.M.; Filos, S. Measurement of functional activities in older adults in the community. J Gerontol 1982, 37, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst Rev 2017, 11, CD008349. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Or, C.K.; Chen, T. Effectiveness of using virtual reality-supported exercise therapy for upper extremity motor rehabilitation in patients with stroke: systematic review and meta-analysis of randomized controlled trials. J Med Internet Res 2022, 24, e24111. [Google Scholar] [CrossRef]
- Kim, M.; Kaneko, F. Virtual reality-based gait rehabilitation intervention for stroke individuals: a scoping review. J Exerc Rehabil 2023, 19, 95–104. [Google Scholar] [CrossRef]
- Lin, C.; Ren, Y.; Lu, A. The effectiveness of virtual reality games in improving cognition, mobility, and emotion in elderly post-stroke patients: a systematic review and meta-analysis. Neurosurg Rev 2023, 46, 167. [Google Scholar] [CrossRef]
- Liu, H.; Cheng, Z.; Wang, S.; Jia, Y. Effects of virtual reality-based intervention on depression in stroke patients: a meta-analysis. Sci rep 2023, 13, 4381. [Google Scholar] [CrossRef]
- Son, C.; Park, J.H. Ecological effects of VR-based cognitive training on ADL and IADL in MCI and AD patients: a systematic review and meta-analysis. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Hao, J.; He, Z.; Yu, X.; Remis, A. Comparison of immersive and non-immersive virtual reality for upper extremity functional recovery in patients with stroke: a systematic review and network meta-analysis. Neurol Sci 2023, 44, 2679–2697. [Google Scholar] [CrossRef]
- Palacios-Navarro, G.; Hogan, N. Head-mounted display-based therapies for adults post-stroke: a systematic review and meta-analysis. Sensors (Basel) 2021, 21. [Google Scholar] [CrossRef]
- Iosa, M. Virtual reality in stroke rehabilitation: virtual results or real values? Arq Neuropsiquiatr 2019, 77, 679–680. [Google Scholar] [CrossRef] [PubMed]
- Brock, K.; Vine, S.J.; Ross, J.M.; Trevarthen, M.; Harris, D.J. Movement kinematic and postural control differences when performing a visuomotor skill in real and virtual environments. Exp Brain Res 2023, 241, 1797–1810. [Google Scholar] [CrossRef] [PubMed]
- Ferroni, F.; Gallese, V.; Soccini, A.M.; Langiulli, N.; Rastelli, F.; Ferri, D.; Bianchi, F.; Ardizzi, M. The remapping of peripersonal space in a real but not in a virtual environment. Brain sci 2022, 12. [Google Scholar] [CrossRef]
- Tuena, C.; Mancuso, V.; Stramba-Badiale, C.; Pedroli, E.; Stramba-Badiale, M.; Riva, G.; Repetto, C. Egocentric and allocentric spatial memory in mild cognitive impairment with real-world and virtual navigation tasks: a systematic review. J Alzheimers Dis 2021, 79, 95–116. [Google Scholar] [CrossRef]
- Katzman, R.; Zhang, M.Y.; Ouang Ya, Q.; Wang, Z.Y.; Liu, W.T.; Yu, E.; Wong, S.C.; Salmon, D.P.; Grant, I. A Chinese version of the Mini-Mental State Examination; impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol 1988, 41, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Mathias, S.; Nayak, U.S.; Isaacs, B. Balance in elderly patients: the "get-up and go" test. Arch Phys Med Rehabil 1986, 67, 387–389. [Google Scholar]
- Leung, S.O.; Chan, C.C.; Shah, S. Development of a Chinese version of the Modified Barthel Index-- validity and reliability. Clin Rehabil 2007, 21, 912–922. [Google Scholar] [CrossRef]
- Tong, A.Y.C.; Man, D.W.K. The validation of the Hong Kong Chinese version of the Lawton instrumental activities of daily living scale for institutionalized elderly persons. OTJR-Occup part heal 2002, 22, 132–142. [Google Scholar] [CrossRef]
- Palombi, T.; Mandolesi, L.; Alivernini, F.; Chirico, A.; Lucidi, F. Application of real and virtual radial arm maze task in human. Brain sci 2022, 12. [Google Scholar] [CrossRef]
- Khenak, N.; Vezien, J.; Bourdot, P. Spatial presence, performance, and behavior between real, remote, and virtual immersive environments. IEEE Trans Vis Comput Graph 2020, 26, 3467–3478. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, A.; Rostami, H.R.; Akbarfahimi, M. Predictors of instrumental activities of daily living performance in patients with stroke. Occup Ther Int 2021, 2021, 6675680. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
One of the authors demonstrates the all-in-one VR headset used in this study.
Figure 2.
One of the authors demonstrates the shopping tasks in the IVR shopping training system.
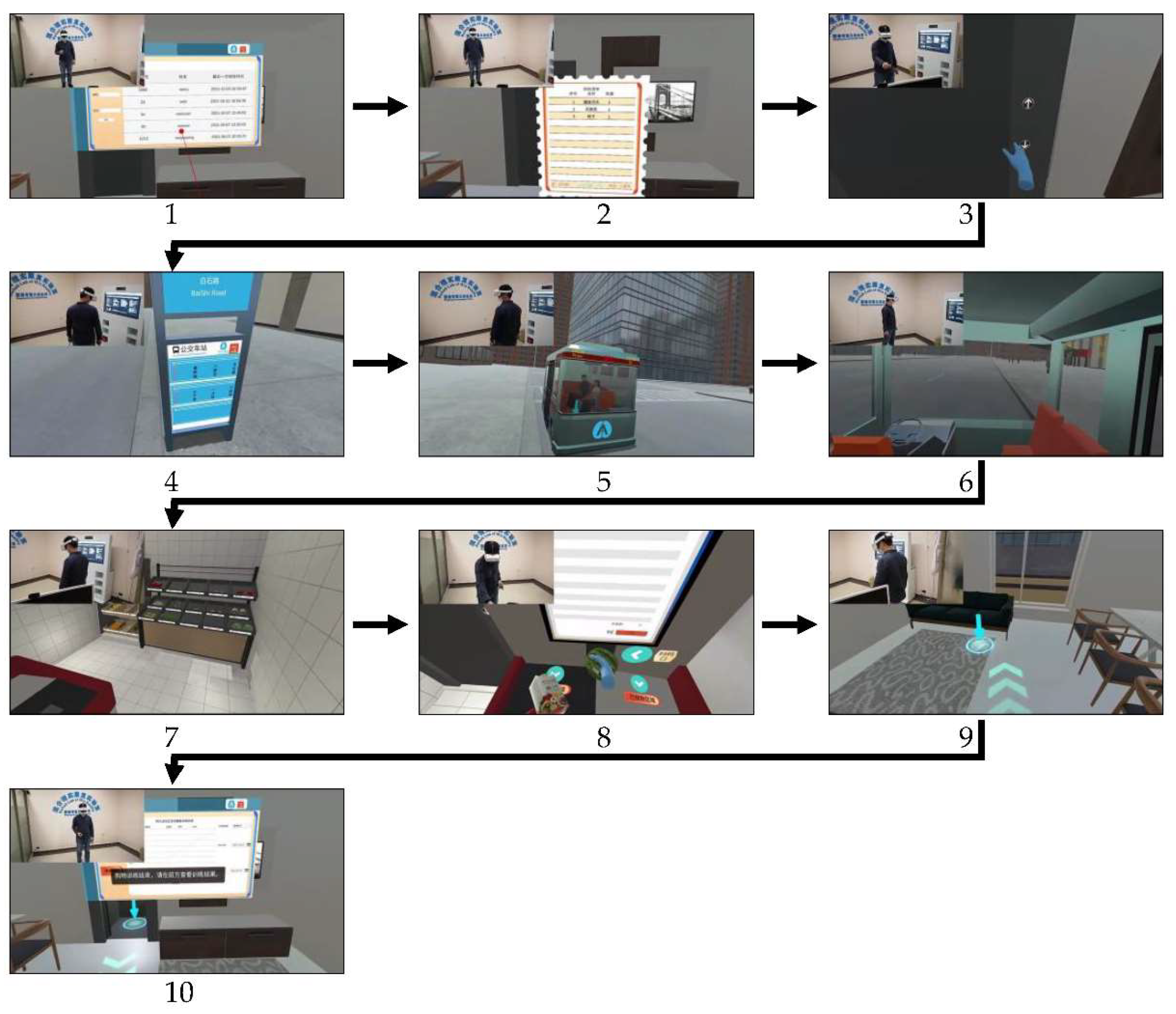
Figure 3.
Flowchart of this study.
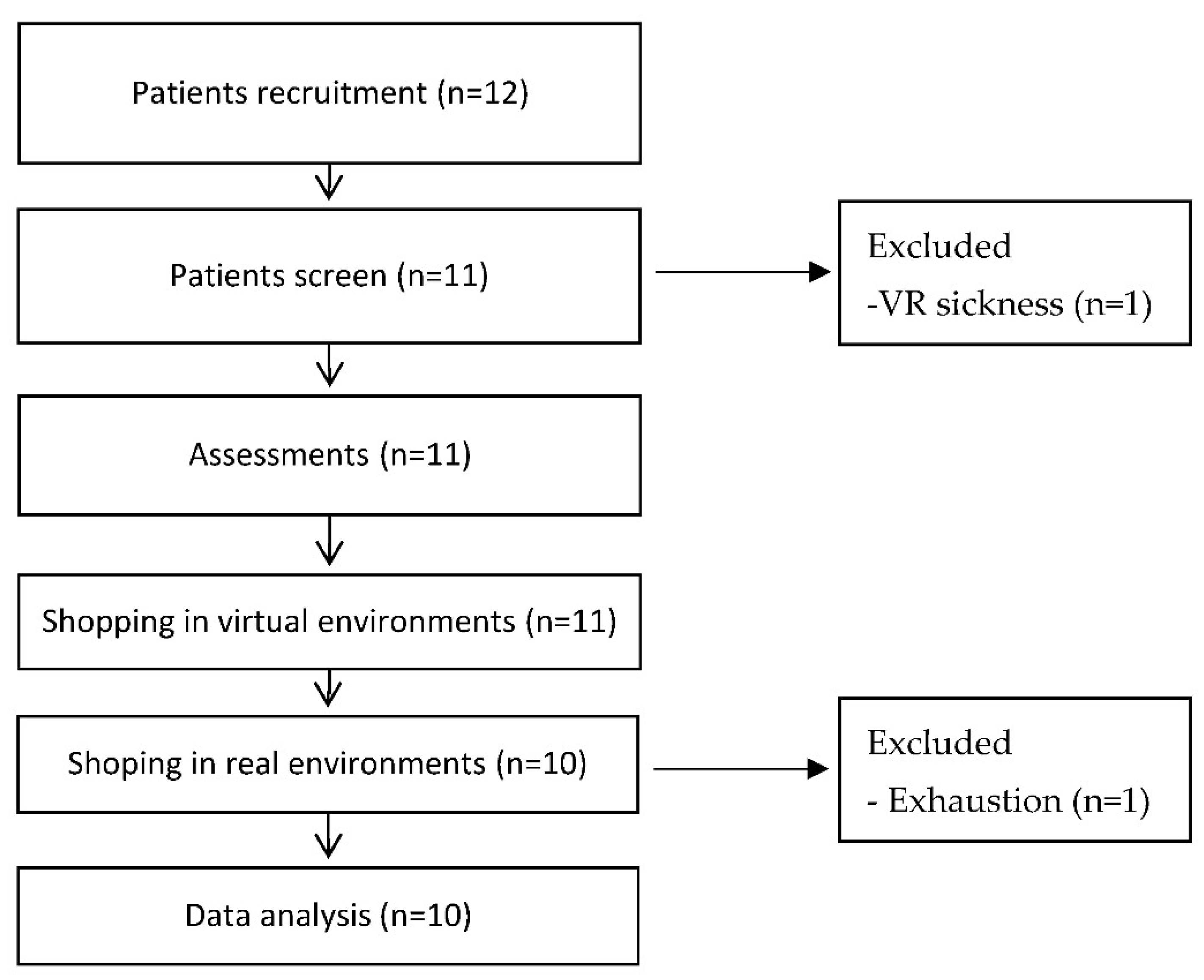

Table 1.
Demographic characteristics of the recruited patients.
| Patients | Gender | Age | Occupation | Education | Type of stroke | Time since stroke (months) | MMSE(max=30) | TUGT(seconds) | MBI(max=100) | LI(max=18) |
|---|---|---|---|---|---|---|---|---|---|---|
| Patient 1 | Male | 59 | Retired businessman | High school | Ischemic | 7 | 29 | 38 | 100 | 15 |
| Patient 2 | Male | 50 | Businessman | Middle school | Ischemic | 9 | 27 | 8 | 100 | 15 |
| Patient 3 | Male | 66 | Retired engineer | University | Hemorrhagic | 42 | 30 | 57 | 93 | 15 |
| Patient 4 | Female | 37 | Clerk | High school | Ischemic | 8 | 28 | 31 | 86 | 12 |
| Patient 5 | Male | 38 | Businessman | Primary school | Ischemic | 3 | 29 | 21 | 100 | 15 |
| Patient 6 | Male | 14 | Student | Middle school | Ischemic | 10 | 30 | 11 | 100 | 16 |
| Patient 7 | Male | 44 | Manager | Middle school | Ischemic | 4 | 29 | 19 | 100 | 17 |
| Patient 8 | Female | 73 | Farmer | Primary school | Ischemic | 1 | 30 | 14 | 100 | 15 |
| Patient 9 | Female | 30 | Unemployed | Middle school | Ischemic | 11 | 25 | 31 | 100 | 10 |
| Patient 10 | Male | 53 | Clerk | University | Ischemic | 11 | 29 | 23 | 100 | 18 |
| LI-Lawton Index, MBI-Modified Barthel Index, MMSE-Mini Mental Status Examination, TUGT-Timed Up and Go Test. | ||||||||||
Table 2.
Occupational performance comparison between virtual and real environments (n=10).
| Occupational performances | Virtual (1st,3rd quartile) | Real (1st,3rd quartile) | Wilcoxon test | Difference between virtual and real ((1st,3rd quartile) |
|---|---|---|---|---|
| Memory capacity | 3.50 (3.00, 4.75) | 3.50 (3.00, 4.75) | 1.000 | 0 (0,0) |
| Time-consuming | 604.50 (549.00, 636.75) | 582.50 (515.50, 611.50) | 0.959 | 21.00 (-98.50, 72.50) |
Table 3.
Correlations between occupational performances and demographic characteristics (Two-tailed Spearman correlation coefficients).
Table 3.
Correlations between occupational performances and demographic characteristics (Two-tailed Spearman correlation coefficients).
| Occupational performances | MMSE | TUGT | LI | |
|---|---|---|---|---|
| Virtual environments | Memory capacity | NS | NS | 0.806(p=0.005) |
| Time-consuming | NS | 0.681(p=0.030) | NS | |
| Real environments | Memory capacity | NS | NS | 0.806(p=0.005) |
| Time-consuming | -0.58 (p=0.077) | NS | NS |
LI-Lawton Index, MMSE-Mini Mental Status Examination, NS-Nonsignificance, TUGT-Timed Up and Go Test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



