
Submitted:
26 September 2023
Posted:
27 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Purpose: This study investigated the impact of the COVID-19 pandemic on mental health, quality of life, and family functioning in a sample of the general female population, exploring difficulties encountered in managing family and work responsibilities and burden of care when taking care of a loved one. The study was moreover aimed at investigating factors capable of influencing severe depressive symptomatology in the context of socio-demographics, traumatic events, individual vulnerability, and family functioning.
Method: During a weekend devoted to Mental Health initiatives (October 8-10, 2021), 211 women were interviewed (47% exposed to the 2009 L’Aquila earthquake).
Results: More than 50% of the sample reported a higher complexity in managing their lives during the COVID-19 pandemic compared to their previous routine, with no statistically significant differences between working women and non-workers, although the latter obtained higher scores for depressive symptomatology and poorer quality of life. Compared to non-caregivers, women caregivers (22.3%) in charge of the care of loved ones affected by physical (10.9%) or psychiatric disabilities (11.4%) complained of a poorer quality of life, with those caring for people affected by mental disorders seeming to experience a more significant worsening.
Approximately 20% of the total sample reported severe depressive symptomatology. Previous access to mental health services (O.R. 10.923), low level of education (O.R. 5.410) and difficulties in management of their everyday lives during the COVID-19 pandemic (O.R. 3.598) were found to be the main variables predictive of severe depressive psychopathology. Old age, good problem-solving skills and ability to pursue personal goals were identified as protective factors.
Conclusions: The COVID-19 pandemic underlined the need for support for emotionally vulnerable women with pre-existing mental health conditions, partly reflecting the cumulative effects of traumas.
Keywords:
Women
; depression
; family burden
; family functioning
; pandemic COVID-19
; collective traumas
1. Introduction
In the early waves, distancing and reduced social contacts proved to be the most effective means of slowing down the COVID-19 pandemic. However, measures applied to contain the spread of COVID-19 dramatically changed how people worked, lived, and studied, with numerous organizations switching to remote working and many planning to continue the practice long term. Changes in the nonwork domain have been equally dramatic; new responsibilities have emerged for many, while interpersonal resources have shrunk [1,2].
The feeling of loneliness and conditions of uncertainty constitute key risk factors for short and long-term consequences on mental health and affect how we interact with others [3,4,5]. Numerous international studies have highlighted how the COVID-19 pandemic has led to high levels of psychological distress [6,7], depression [8], and anxiety [9,10,11]. Studies have also confirmed how social distancing implemented in response to the first wave of COVID-19 coincided with a worsening of mental health across multiple countries [12,13,14].
Several studies conducted in Italy have investigated the negative psychological consequences produced by the pandemic on the general population, taking into account predictors including female gender, infection of an acquaintance, history of medical problems, having been subjected to stressful and traumatic situations, such as previous natural disasters [15,16], and availability of inadequate physical space during isolation [7,17,18]. Moreover, the severe impact on the population’s mental health coincided with a drastic reduction in levels of care [19].
With regard to the effect of COVID-19 on mental health, a large number of studies have highlighted in the female gender a significant association with higher self-reported levels of stress, anxiety, depression, and post-traumatic stress symptoms and a more severe overall psychological impact [8,20,21,22]. Compared to men, the increased prevalence of depressive disorders observed in women underlined the presence of a highly significant difference produced as a result of the social and economic consequences of the pandemic [23]. Indeed, the female sex is characterised by a higher prevalence of risk factors known to intensify during a pandemic, including chronic environmental strain [24], pre-existing depressive and anxiety disorders [25], and domestic violence [26,27,28].
COVID-19 seems to have amplified gender inequalities in the work domain [29,30]. Throughout the COVID-19 pandemic and compulsory lockdowns, working women undoubtedly fgoun d it challenging to cope with changes in the workplace and to adapt to remote home working routines [31,32,33]. Mothers who were suddenly expected to balance remote working with family life were affected by a series of physical, mental, and social issues including anxiety, stress, sleep deprivation, and relationship problems [30]. The results of a cross-sectional survey of European working women from five countries: France, Italy, Poland, Sweden and the United Kingdom revealed how women working from home displayed a higher prevalence of depressive symptoms compared to those who commuted to work, suggesting that networking with people face-to-face acted as a significant protective factor against experiencing symptoms of depression during a period of social distancing [34].
Moreover, in addition to having to work from home, women were often required to shoulder the burden of additional caring responsibilities, such as supporting children during online education or taking care of a family member with a physical or mental disability. As the majority of support services implemented virtual services, the family, in particular mothers, were relied on increasingly for support. Women assumed the role of caregiver more often than men and scored lower on the quality of life measure, reporting higher levels of anxiety [35,36,37]. Caregivers reported a limited ability to cope with life stressors and increased social isolation [38]. One year into the pandemic, female caregivers of dementia patients tended to display more stress-related symptoms compared to baseline, including depression, anxiety, irritability, and anguish [39]. Caregivers of people affected by schizophrenia reported a heavy burden of care and high levels of stress during the pandemic [40,41]. Indeed, even prior to onset of the COVID-19 pandemic, quality of life amongst caregivers of schizophrenic subjects had been particularly poor [42]. Throughout the COVID-19 pandemic, caregivers’ concerns were focused not only on their own health but also on the continuity of care and well-being of their family members affected by mental illnesses [43,44] and disabilities [45].
In Italy, the ONDA Foundation, a National Gender Observatory on Women’s Health established in Milan, has been working since 2005 to promote women’s health by carrying out a series of activities and projects (gender surveys, events, publications, digital campaigns, and thematic focuses). The Onda Foundation collaborates with the National Health Service and social-health structures. Every year, the Foundation recognizes the focus of Italian hospitals on gender-specific medicine by conferring the “Bollini rosa” award. With the support of this virtuous network of 354 hospitals in Italy, ONDA organizes (H) Open Days, (H) Open Weeks, and (H) Open Weekends, free initiatives aimed at facilitating diagnosis and access to appropriate treatment in the female population. One of the targets of these activities is to raise awareness of mental health issues, particularly depression, in the female population.
In the context of initiatives carried out by the ONDA network, our study aimed to: 1) evaluate depressive symptomatology, quality of life and family functioning, with particular focus on difficulties faced by women during the COVID-19 pandemic, in a general population sample comparing working and non-working women; 2) and women caring for a loved one affected by physical or psychiatric disabilities and non-caregivers, and 3) factors influencing the onset of severe depressive symptomatology in the context of socio-demographics, traumatic events, and individual vulnerability and family functioning skills.
In the conceptual framework of a psychosocial vulnerability model [46] including socio-demographic (age, educational level, civil status), clinical (pre-existing psychological problems), contextual (previous traumatic events and family functioning), and psychosocial (caregiver role) variables, we were interested in evaluating the factors impacting on higher depressive symptomatology during the COVID-19 pandemic.
We hypothesized that older, less educated women who were lacking a stable affective relationship, living in poor economic conditions, and had been distressed by both previous traumatic events (2009 L'Aquila earthquake) and by household and life management during the COVID-19 pandemic, either with pre-existing mental health conditions, who were taking care of a loved one, or with low family functioning might be at increased risk of developing severe depressive symptoms.
2. Methods
2.1. Context
In April 2009, an earthquake of magnitude 6.3 hit the province of L’Aquila, claiming the lives of 309 people, injuring thousands of citizens, causing tens of thousands of displaced people, and provoking severe material destruction [47,48,49]. Reconstruction of the city is still ongoing, as is the process of “remediation” of the psychosocial vulnerability of the exposed population [50,51,52]. In this study, we also focused on the variables of exposure to and impact produced by experiencing the April 2009 earthquake, considered a crucial collective life event for people living in the area.
2.2. Study Design and Population
The survey took place during the H)-Open Weekend (October 8-10, 2021) organized by the National Gender Observatory on Women’s Health “Fondazione Onda” on occasion of the World Mental Health Day.
The University Unit for Rehabilitation Treatment and Early Interventions in Mental Health, known as TRIP, located within the S. Salvatore Hospital and directed by Prof. Rita Roncone, took part in the initiative to raise awareness amongst women of the importance of defending their mental well-being and the right to “Re-start” from their own life goals, encouraging them, in case of distress, to seek early diagnosis and access to treatment, helping them overcome fears, prejudice, and stigma related to mental disorders.
The team included psychiatrists, researchers and Ph.D. students in clinical psychology, as well as undergraduate students in psychiatric rehabilitation techniques, who conducted the questionnaire-based ‘face-to-face’ street interviews and collected the data online. The team attended a short 4-hour training session based on interview techniques and early identification of emotional distress.
The entire team set up a station in the Centre of L’Aquila where women were able to voice their concerns and emotions and where interviewers could suggest strategies to help the women improve their quality of life.
Street interviews are one of the fastest and most accurate forms of real-time data collection. In this form of data collection, women who had been approached on the street and were agreeable, were asked targeted questions included in a survey “I start from myself” in the form of a structured interview. At the end of the interview, they were all encouraged to access the service for a free comprehensive psychiatric consultation if they thought it might be helpful.
The interview questions derived from the results of an online focus group on Microsoft Teams® (Microsoft Corporation, Redmond, WA, USA) set up to develop concepts and questions for the questionnaire design. The focus group meeting lasted two hours and included all the authors of this study.
2.3. Assessment tools
The assessment consisted of three parts:
- a)
- Section 1 included information on the study, privacy protection, and informed consent.
- b)
- Section 2 included the participants’ demographic backgrounds, including age, education, work, marital status, number of children, working activity, and socio-economic status. The history of life-events included: the impact of the COVID-19 pandemic, complex management of family life and work during the COVID-19 pandemic, and the impact produced by the 2009 L’Aquila earthquake measured on a 5-point Likert scale (0 = None; 1 = Only a little; 2 = To some extent; 3 = Considerably; 4 = Greatly). Previous contact with mental health services, mental health issues, and treatments were also assessed.
- c)
- Section 3 included standardized questionnaires investigating the quality of life, psychopathology, family functioning, and family burden.
The Patient Health Questionnaire (PHQ-9) [53] is a tool applied to evaluate depressive symptoms and levels of severity. It contains nine items rated on a four-point Likert scale (0 = not at all; 3 = nearly every day). The PHQ-9 total score for the nine items ranges from 0 to 27. The PHQ-9 A PHQ-9 score ≥10 had a sensitivity of 88% and a specificity of 88% for major depression. PHQ-9 scores of 5, 10, 15, and 20 represent mild, moderate, moderately severe, and severe depression, respectively [54]. For the purpose of this study, we used a cut-off score of 10. Internal reliability was excellent, with a Cronbach’s alpha of 0.89 (Kroenke et al., 2001). Our sample’s internal consistency for the PHQ-9 was high (Cronbach’s α = 0.87).
The 36-Item Short Form Survey (SF-36) [55,56] is a self-reported measure of the population’s health-related quality of life (QoL). The SF-36 Health Survey is a 36-item form that measures eight different dimensions of health: general health perception (GH), physical function (PF), role limitations related to physical problems (RF), bodily pain (BP), mental health (MH), role limitations due to emotional problems (RE), vitality (VT), and social functioning (SF). The raw scores are linearly transformed into 0–100 scales. Higher transformed scores indicate better health.
Family functioning was assessed using the Family Functioning Questionnaire, FFQ [57]. Developed to assess the family functioning pattern in the frame of psychoeducational family interventions, the questionnaire consists of 24 items. It measures the following three dimensions:
1) Problem solving (eight items), referred to the six steps of structured problem-solving: identify the problem or the objective, list possible alternative solutions, discuss the positive and negative aspects of each proposal, and choose the best (or better, a satisfying and realistic solution), plan the solution, check and review the implementation and planning;
2) Communication skills (eight items), concerning the expression of positive and negative feelings, the making of requests and active listening skills (probing questions, a summary of what has been understood) and
3) Personal Goals (eight items), defined as the ability of each family member to identify everyday personal goals (not linked to subject care). Responses range from 1 “never” to 4 “always”. Higher scores are indicative of healthier functioning.
Items are evaluated on a 4-point Likert scale; a higher score is associated with better family functioning (range 24-96). The scale was originally developed and standardized in the Italian population and has demonstrated good internal consistency (Cronbach’s alpha coefficient ranges from 0.75 to 0.84 for the three dimensions) and test-retest reliability (Pearson’s r correlation coefficient ranges from 0.75 to 0.60) [57]. Internal consistency for the FFQ in our sample was high (Cronbach’s a = 0.88).
The version of the Family Problem Questionnaire, FPQ [58] used in this study consisted in a shortened version of the 44-item instrument [59], recently utilized in an Italian multicentric family study [60]. In this study, we selected sections specifically aimed at assessing the objective and subjective burden of care and the dimension of support received (from professionals, relatives, and friends). We investigated: 1) objective burden (twelve items, range 13-52) related to impact on daily activities/social life; 2) subjective burden (six items, range 6-24) related to impact on caregiver well-being, distress over the condition of the affected family member, concern for the future; 3a) professional support received (four items, range 4-16); 3b) support from relatives and friends (three items, range 3-12).
Items were evaluated on a 4-point Likert scale. Higher scores were associated with a higher burden of care and scarce support from professionals, relatives, and friends.
2.4. Statistical analyses
Statistical analyses were conducted in four phases: (1) descriptive analysis of socio-demographics, clinical data and health-related quality of life, depression, family functioning, and burden of care in women caregivers. (2) Continuous variables were reported as means (standard deviations), and categorical variables were reported as frequencies (percentages). Baseline comparisons [chi-square, t-tests, and one-way analysis of variance (ANOVA)] were performed to assess differences between female caregivers and non-caregivers and between non-caregivers and caregivers of subjects affected by either physical or mental disabilities. The Bonferroni post-hoc correction was calculated.
A correlation analysis (r-Pearson) was conducted to verify relationships between caregivers’ age and years of education and five out of the eight dimensions of health-related quality of life as measured by the SF-36 (general health perception GH; mental health, MH; role limitations due to emotional problems, RE; vitality, VT; and social functioning, SF), the four-subscales (objective burden, subjective burden, professional support, support from relatives and friends) of burden of care as measured by FPQ, and the three-dimensions (problem-solving, communication, and personal goals) of family functioning (FFQ).
Multinominal logistic regression analyses were conducted to identify variables capable of influencing depressive symptomatology. The dependent variable, depression (based on PHQ-9 scores), was coded 1 = absent – mild depression (PHQ-9 scores 0-5); 2 = moderate depression (PHQ-9 scores 6-10); 3 = moderately severe depression (PHQ-9 scores 11-15); 4 = severe depression (PHQ-9 scores >15).
Independent variables in the model included women’s age; not having a stable affective partnership; low educational level; financial difficulties; having traumatically experienced the 2009 L’Aquila earthquake; having contracted COVID-19; complex life management during the COVID-19 pandemic; previous access to mental health services; caregiving for a loved one; and the three dimensions of the FFQ (problem-solving, communication, and personal goals).
Not having a stable affective partnership was coded into two categories (1 = single, separated/divorced, widows; 0 = married). Education was coded into two categories (1 = less than 13 years of education; 0 = 13 years or more of education, i.e., graduation or higher). Economic difficulties, having traumatically experienced the 2009 L’Aquila earthquake, having contracted COVID-19, complex life and household management during the COVID-19 pandemic, previous contact with mental health services and caregiving for a loved one were coded into two categories (1 = yes; 0 = no).
With regard to our model, the selection of independent variables was based prevalently on previous literature research. “Age”, as an independent variable, was included in estimating the ability of younger women to better manage disasters [61] and distress, particularly for psychiatric caregivers [62,63]. The inclusion of independent variables related to collective traumatic events and their consequences (severe long-term impact of the April 6, 2009 L’Aquila earthquake; having contracted COVID-19 virus infection; complex management of family life and work during the COVID-19 pandemic) was motivated by the vulnerability of women to collective traumatic events such as earthquakes [15,16,64], and the recent collective trauma of the COVID-19 pandemic [65,66,67]. In women, isolation, economic precarity, and previous mental health issues were predictors of traumatic conditions during COVID-19 [65,68], in view of the complexity of managing the household and their own lives during the COVID-19 pandemic, continuously juggling the work and family balance [30,69]. In our model, the three dimensions of family functioning were selected based on the assumption that low family functioning could be predictive of depression [70,71,72].
Our comprehensive model assumed that older, less educated women who were lacking a stable affective relationship, living in poor economic conditions, and had been distressed by previous traumatic events (2009 L'Aquila earthquake) and by the COVID-19 pandemic, might be at greater risk of developing severe depressive symptoms based on a psychopathological vulnerability or due to taking care of a loved one or low family functioning.
Statistical analyses were conducted using SPSS 27.0 (SPSS Inc., Chicago, IL, USA). All tests were two-tailed, and P < 0.05 was considered significant.
3. Results
3.1. Socio-demographic and characteristics of the sample, depression, health-related quality of life, and family functioning
Table 1 describes the main demographic and clinical characteristics of the 211 women who took part in the study.
The mean age in the total sample was 35.6 (SD = 18.5) (range: 18-82). The majority of women were Italian, with less than 5% (n=10) originating from Moldova, Ukraine, Albania, Iran, and Argentina. More than half the sample (53.1%, n=112) was comprised of women living alone without a stable affective realtionship.
Approximately 70% of this sample of young women (43% students) had no children and less than 35% were employed in a paid position, whilst more than 40% held a University degree. Slightly more than 15% complained of financial difficulties.
Statistically significant differences were detected between the two groups (workers and non-workers). Non-working women were characterised by a younger age than working women (t-test: -3.598; p = 0.000), were more likely to be married (chi-square: 27.970; f.d. 3; p = 0.000) have children (chi-square: 10.858; f.d. 3; p = 0.001), and possessed a lower level of education (chi-square: 26.201; f.d. 3; p = 0.000) (Table 1).

Table 1.
Comparison of socio-demographic and clinical characteristics of the sample (n= 211) between working and non-working women (n= 211).
Table 1.
Comparison of socio-demographic and clinical characteristics of the sample (n= 211) between working and non-working women (n= 211).
| Variables included | Workers (n=73) |
Non-workers (n=138) |
|---|---|---|
| Age, mean (SD)* | 41.8 (13.2) | 32.4 (20.1) |
| Working conditions (%) | ||
| Self-employed/freelancers | 23 (31.5) | |
| Full-time work | 35 (47.9) | |
| Part-time work | 15 (20.5) | |
| Student | - | 91 (65.9) |
| Housewife | - | 13 (9.4) |
| Unemployed | - | 12 (8.7) |
| Retired | - | 22 (15.9) |
| Nationality (%) | ||
| Non-EU citizens | 4 (5.5) | 4 (2.9) |
| Marital status (%)* | ||
| Single | 16 (21.9) | 77 (55.8) |
| Married/Partnership | 49 (67.1) | 50 (36.2) |
| Separated/ Divorced | 7 (9.6) | 4 (2.9) |
| Widowed | 1 (1.4) | 7 (5.1) |
| Parents of children (%)* | 33 (45.2) | 32 (23.2) |
| Level of education (%)* | ||
| >13 years (graduated) | 24 (32.9) | 96 (69.6) |
| Socio-economic status (%) | ||
| High- upper middle income | 39 (53.4) | 56 (40.6) |
| Middle - low income | 27 (40.2) | 57 (41.3) |
| Struggling financially | 7 (9.6) | 25 (18.1) |
More than 50% of the sample (N=108, 51.2%) reported complexities in managing their lives during the COVID-19 pandemic compared to pre-pandemic times (Table 2); no statistically significant differences were detected between workers (42.5%) and non-workers (55.8%). Ten percent of the sample had contracted COVID-19 infection, and 13.3% referred having lost loved ones due to COVID-19.
Only a small proportion of women (7.6%; n=16) had refused COVID-19 vaccination. These decisions were not found to be related in a statistically significant manner to socio-demographics, level of education (some held a university degree) or clinical variables.
Less than half of the sample (n=100, 47.4%) had been exposed to the 2009 L’Aquila earthquake; of these, 43% referred a severe impairment in at least two of the three dimensions investigated (family life, work, or social life), while 7.1% (n=15) confirmed having lost someone close. Compared to non-workers, a higher proportion of female workers had been exposed to the 2009 L'Aquila earthquake (chi-square: 9.091; f.d. 1; p = 0.003), with the catastrophic event producing a severe impact on their lives (chi-square: 6.550; f.d. 1; p = 0.010).
Almost 45% of the total sample (n = 94) reported having previously accessed mental health services, with no statistically significant differences between those who had contacted the mental health services and those who had not (Table 2). Psychopharmacological treatment had been prescribed to 18.5% of the total sample, with no statistically significant differences between the two groups with regard to subsequent integrated (psychopharmacological plus psychotherapeutic treatments) or psychotherapeutic therapies alone.
Forty percent of the sample obtained a PHQ-9 score superior to the cut-off score of 10, with approximately 20% being diagnosed as affected by severe depression based on PHQ-9 scores (Table 3). A statistically significant difference was found at PHQ-9 scores between the two groups of women, with non-workers obtaining higher scores (t-test: 2.936; p = 0.004). A higher proportion of non-workers (n = 63, 76.8%) had a PHQ-9 score exceeding the cut-off score of 10 compared to working women (58.9%) (chi-square = 7.157; f.d. = 1; p = 0.005).
Statistically significant differences were found between the two groups of women in family functioning dimensions, with working women showing higher scores in communication (t-test: -3.496; p = 0.001) and problem-solving (t-test: -4.118; p = 0.000) and lower scores in pursuing personal goals (t-test: 4.027; p = 0.000) compared to non-workers (Table 3).
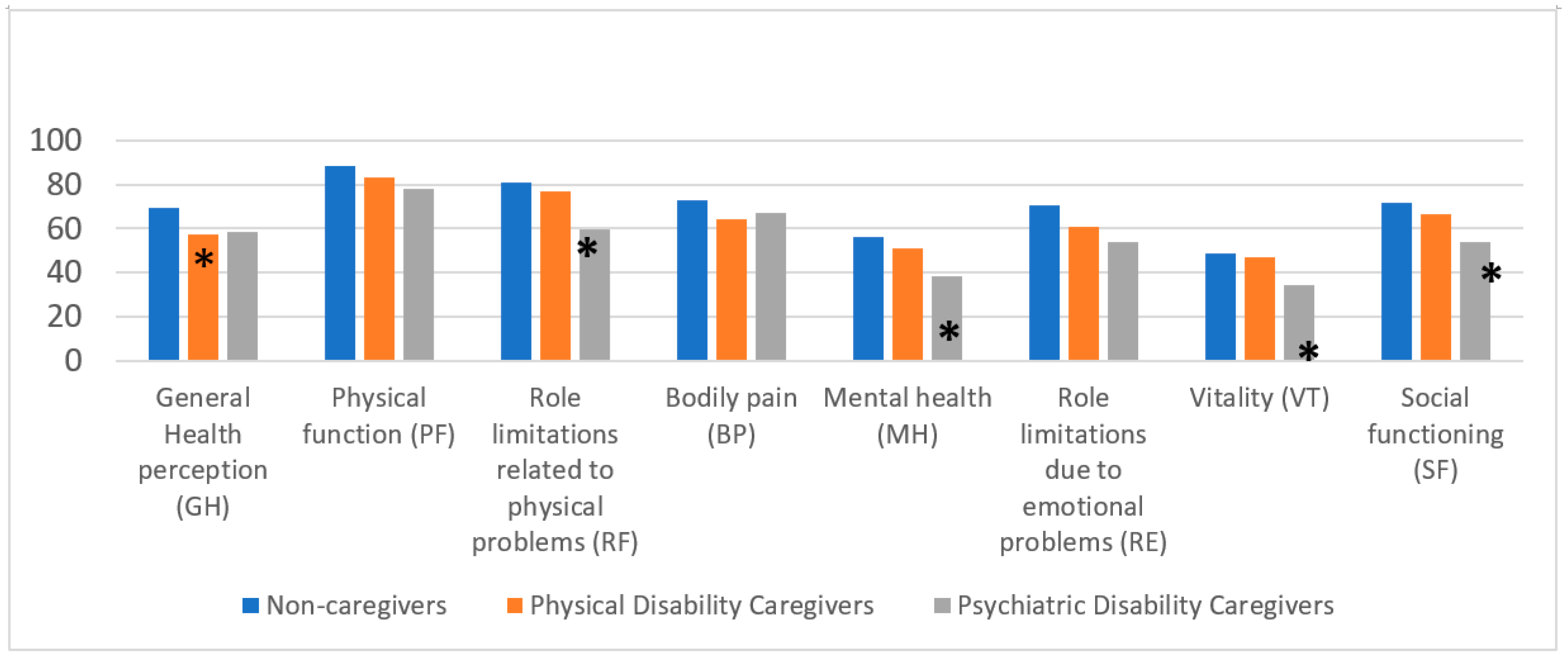
Compared to workers, non-workers obtained lower scores at all quality of life domains correlated to mental health, MH (t-test: -3.148; p = 0.002), RE (t-test: -3.585; p = 0.000), VT (t-test: -3.090; p = 0.002), SF (t-test: -2.843; p = 0.005) (Figure 1).
No statistically significant differences were revealed in the proportion of workers (n = 32) and non-workers (n = 15) who acted as caregivers (n = 47, 22.3%) or were taking care of loved ones with physical (n = 23, 10.9%) or psychiatric disabilities (n = 24, 11.4%) (Table 4).
Likewise, no statistically significant differences were detected between the two groups (caregivers and non-caregivers) with regard to socio-demographic variables such as age, nationality, marital status, having children, level of education, working conditions, and socio-economic status (Table 4).
Caregivers were characterised by a statistically significant higher proportion of loss of loved ones due to COVID-19 compared to non-caregivers (chi-square: 5.396; d.f. 1; p=0.020) (Table 5). No statistically significant differences were revealed between the two groups (caregivers and non-caregivers) with regard to other variables related to life events and clinical characteristics of the samples (Table 5). Working caregivers did not complain about the complexity of managing their lives any more than non-working caregivers.
No statistically significant differences were found between the two groups of women with regard to PHQ-9 scores and family functioning dimensions (Table 6).
Compared to non-caregivers, women who had a caregiving role obtained lower scores at 6 out of 8 health-related quality of life domains (with a preeminent impact on physical health), GH (t-test: 3.370; p = 0.002), PF (t-test: 2.556; p = 0.011), RF (t-test: 2.412; p = 0.017), BP (t-test: 2.464; p = 0.015), MH (t-test: 2.887; p = 0.004), SF (t-test: 2.720; p = 0.007), while RE (t-test: 1.922; p = 0.056), VT (t-test: 1.949; p = 0.053) scores approach statistical significance (Figure 2).
We subsequently better characterized the population of caregivers by specifying whether they cared for people with physical (n=23; mean age, years=39.0 SD=19.4) or mental disabilities (n=24; mean age, years=35.3 SD=18.3), six out of the eight SF-36 dimensions were statistically significant (Figure 3).
An ANOVA test and post hoc analysis provided evidence of differences between the mean of non-caregivers compared to the two groups of caregivers for GH (ANOVA: F = 5.668; p = 0.004), highlighting a greater impairment in women caring for people with physical (Bonferroni method: mean difference: 11.66278, p = 0.028) and psychiatric disabilities (Bonferroni method: mean difference: 10.59756, p = 0.048) (Figure 3).
In the PF dimension, we found evidence of differences between the mean of non-caregivers compared to caregivers of people with psychiatric disabilities ANOVA: F = 3.676; p = 0.027), with the latter displaying poorer physical function (Bonferroni method: mean difference: 10.68089; p = .037). Moreover, the RF dimension underlined a marked difference between the mean of female non-caregivers compared to those who cared for a person with psychiatric disabilities (ANOVA: F = 4.761; p = 0.001), highlighting the presence in caregivers of subjects with psychiatric issues of a role limitation related to physical problems (Bonferroni method: mean difference: 21.570; p = 0.007) (Figure 3).
With regard to MH, evidence of a significant difference between the mean of women caring for a person with psychiatric disabilities versus non-caregivers was revealed (ANOVA: F = 5.829; p = 0.003), highlighting the poorer mental health of those caring for someone with a psychiatric disability (Bonferroni method: mean difference: 17.50000; p = .003) (Figure 3).
Analysis of the SF-36 dimensions of VT and SF revealed a significant difference only for caregivers of people with mental disabilities versus those caring for a person with physical disabilities and non-caregivers (VT ANOVA: F = 3.488; p = 0.003; Bonferroni method 14.27846; p = 0.027; SF ANOVA F = 5.147; p = 0.007; Bonferroni method 17.84807; p = 0.005), thus demonstrating how these two specific dimensions were only impaired in this subpopulation (Figure 3).
Figure 3.
Health-related quality of life in its eight dimensions in the three groups of women. ANOVA test *p=<0.05.
Figure 3.
Health-related quality of life in its eight dimensions in the three groups of women. ANOVA test *p=<0.05.
No statistically significant differences in family functioning were found in the three dimensions identified by the FFQ between the two groups of caregivers (Table 7).
Caregivers of psychiatric subjects complained of a higher subjective burden (t-test for independent samples: t(45) = -3.461, p = 0.001), and less support from relatives and friends (t-test for independent samples: t(45) = -.2.256 p = 0.029) compared to caregivers of patients with an organic illness (Table 7).
3.2. Correlations between age, years of education, health-related quality of life, family functioning, and burden of care
Table 8 shows the correlations between the variables of health-related quality of life, family functioning, and burden of care with age and level of education. Age was positively and statistically significantly correlated with GH, MH, RE, VT, and SF, as measured by SF-36, suggesting that getting older allows greater adaptation, better perception of general health conditions, and improved social functioning. In the same way, level of education positively and significantly correlated with all quality of life dimensions measured by SF-36. It was, however, negatively and significantly associated with depressive symptoms, suggesting a protective role for a higher level of education on mental health and quality of life.
Depressive symptoms, as measured by PHQ 9, seemed to increase over time in caregivers with a lower level of education. Despite their satisfying functional adaptation and positive restructuring of difficulties, they displayed a persistently depressed mood. Correlation analyses revealed significant negative correlations between depressive symptoms and GH, MH, RE, VT, and SF.
Statistically significant negative correlations were found between objective and subjective burden of care, as measured by FPQ, and perceived quality of life and its related dimensions (GH, MH, ER, VT, SF), confirming the strong impact of a caregiving role on subjects' health-related quality of life. However, our data showed that objective burden of care tends to impair the perception of mental health conditions more than subjective burden. Correlation analyses showed negative and significant correlations between a lack of support from friends and MH. Indeed, a lack of support from both friends and relatives and of professional help negatively and significantly correlated with VT, whilst it positively and significantly correlated with depressive symptoms (PHQ 9), confirming the crucial role of social support on the mental health of patients and their caregivers.
With regard to family functioning, good problem-solving and communication skills and achieving personal goals in the family context were positively and significantly associated with age, level of education and all quality of life dimensions. In contrast, they were associated negatively and significantly with depressive symptoms (PHQ-9). In addition, these skills seemed to increase over time, along with a lower subjective burden of care and better perception of social and professional support (with the exception of problem-solving skills). Communication skills however seemed to increase in line with a better perception of both the objective and subjective burden of care. These latest results further confirm the potential of good problem-solving and communication skills, and achievement of personal goals acting as promoters of improved mental well-being, better quality of life, and social /professional support for family members and their caregivers.
3.3. Variables impacting severe depressive symptomatology
Table 9 illustrates the results of multinominal logistic regression for absent/mild depression symptoms (PHQ-9 = 1, score 0-5), as the dependent variable.
The first set of coefficients comparing women who obtained a score of 1 at PHQ-9 (absent/mild depression symptoms) and those scoring 2 (range 6-10, moderate depression) revealed two statistically significant predictors. Firstly, women who had lived through the highly traumatic 2009 L’Aquila earthquake were almost 4 times more likely to suffer from moderate depression. Secondly, older age appeared to exert a protective effect against manifestations of moderate depression compared to a mild presentation.
Compared to the first set of coefficients, in the second set, representing a comparison between women scoring 1 (PHQ-9 range 0-15, absent/mild depression symptoms) and women scoring 3 (PHQ-9 range 11-15, moderately severe depression), the highly traumatic experience of the 2009 L’Aquila earthquake displayed a 9-fold increased predictive probability of onset of moderately severe depression versus women displaying mild depressive symptoms. In the sample investigated, previous access to mental health services resulted in a significant 7-fold increase in the likelihood of manifesting moderately severe depression compared to women with mild depression. Life management difficulties perceived during the COVID-19 pandemic led to an almost 3-fold statistically significant increase in the probability of being affected by moderately severe depression. The protective role exerted by older age against manifesting a more severe depressive psychopathology was confirmed, and an adjunctive variable represented by problem-solving skills in the family context, was identified as a protective factor in this second set of coefficients.
In the third set of coefficients, illustrating the comparison between women scoring 1 (PHQ-9 range 0-15, absent/mild depression symptoms) and women scoring 4 (PHQ-9 > 15 severe depression), the more robust variable was previous access to mental health services, which significantly increased 10-fold the likelihood of exhibiting severe rather than mild depressive symptomatology. A low level of education was identified as a risk variable, accounting for a more than 5-fold probability of manifesting severe depression. The perceived difficulties in life and household management during the COVID-19 pandemic confirmed a more than 3-fold statistically significant increase.
In women, older age and good problem-solving strategies were confirmed as exerting a predictive protective role against severe depression versus the manifestation of mild symptoms. In this third set of coefficients, the pursuit of reaching individual goals reached statistical significance as a predictive protective factor in maintaining improved mood and not manifesting severe depressive symptoms.
4. Discussion
Previous access to mental health services, low level of education and difficulties in life management during the COVID-19 pandemic were confirmed as variables capable of influencing the onset of severe depressive psychopathology compared to presentation of a normal mood tone in our sample obtained from the general female population. Older age, good problem-solving skills, and ability to pursue personal goals were identified as protective factors. Having previously experienced natural catastrophic collective traumas (2009 L’Aquila earthquake) displayed the most robust predictive value related to the presentation of clinical pictures characterized by moderately severe depressive symptomatology, suggesting a role of past life events in psychopathological frailty alongside the vulnerability variable of stressful pre-existing mental health conditions.
In our general population sample, half of the women complained about the complexities of managing their lives during the COVID-19 pandemic compared to their previous routines. Surprisingly, working women, commonly assumed as being more distressed due to their work-family balance [30], manifested less depressive symptoms, a better quality of life, and more competent problem-solving and communication skills in a family context, alongside an understandable poorer ability to pursue their personal goals than non-working women.
Compared to European working women, in whom a higher prevalence of depressive symptoms was manifested by women working from home compared to those who commuted to their place of work [34], our findings seem to positively evaluate the role of “paid work”. Indeed, in our study, stay-at-home women who carried out no paid work displayed more depressive symptoms and worse health-related quality of life, despite better functioning in pursuing their personal goals. Limitation of social contact seemed to be a key factor involved in the presentation of higher levels of depression, with home-working resulting in a marked reduction of face-to-face social contacts with family, friends, and colleagues [33], whilst women who continued to work from the office were still able to network to some extent with people outside the house during lockdowns.
With regard to difficulties encountered in life and household management, the findings of our study only partially align with the national survey conducted by the ONDA Foundation in April 2021 in Italy [73]. The comparison is hampered by the diversity of characteristics of the samples recruited. The national ONDA online survey included 609 women (over 55% in central-southern Italy, age range 25-55 years) who, prior to the pandemic, had been in paid employment, many of whom with a university degree (40%), and had been in a stable affective relationship (almost 70%). In our study, although the level of higher education was comparable, more than half the women were living alone without a stable relationship, and around three-quarters were not in paid employment or financially independent. Moreover, in the present study, just over 15% of women reported struggling financially, whilst in the ONDA national survey, 39% of working women reported having experienced significant economic challenges following the COVID-19 outbreak, which had mainly affected workers who were contractually less protected or women who had lost/changed jobs, had their working hours reduced or had been furloughed, particularly in Central-Southern Italy [73].
On investigating mental health conditions, the ONDA 20121 survey reported how, since the start of the pandemic, 85% of women had been affected by at least one mental disorder over a prolonged period and had resorted to treatment. Our study, however, was aimed prevalently at assessing the presence of depressive symptoms, thus resulting in the detection of a lower 40% rate of other mental issues in our sample based on a PHQ-9 cut-off of 10 used to identify the presence of moderately severe/severe depression. The data obtained in our study were similar to those reported by Arpino & Pasqualini in Italy, reporting how 47% of the sample evaluated had felt depressed during the first COVID-19 lockdown [74].
Our study found how during the COVID-19 pandemic, when compared with non-caregivers, women in charge of the care of a family member with a physical or psychiatric disability complained of a worse health-related quality of life, as also reported in a German study [36]. Caregivers of subjects affected by mental disabilities showed a statistically significant impairment in vitality and social functioning compared to the other two subgroups of women studied. They complained of a higher subjective burden and less support from relatives and friends than caregivers of patients affected by organic diseases. With regard to objective burden of care, a lack of help from relatives, friends, and professionals was associated with lower family functioning. Our findings align with previous literature studies highlighting the stressful role of caregivers during the COVID-19 pandemic [39,41,43,44,61,75,76]. Our findings are consistent with those of recent studies demonstrating how female caregivers experienced mental health issues during the pandemic [75,77], with a multicentric Italian study reporting even higher values than those obtained by caregivers of schizophrenic family members prior to the pandemic [60]. Family distress was higher in households caring for a psychiatric patient, and the increasingly onerous burden for mental health caregivers compared to those with family members affected by physical disabilities confirmed the findings of both Fusar-Poli et al. [41,44] and previous literature data [78]. A limitation of our study related to the assessment of caregivers looking after people with intellectual disabilities, who seemed to experience more significant difficulties during the COVID-19 lockdowns than those who cared for the mentally ill [75].
Within our conceptual framework of a psychosocial vulnerability model, the deepening of depressive symptomatology during the COVID-19 pandemic was carefully investigated. In the sample investigated, we recorded 20% of women reporting severe depressive symptoms (PHQ-9 > 15), thus promoting our interest in exploring factors that might have contributed to the severity levels of its manifestation.
Compared to women displaying a normal mood tone, the likelihood of manifesting moderate depression was approximately four times higher in women exposed to the 2009 L’Aquila earthquake who reported this as a highly traumatic collective experience. This variable increased by more than double its predictive power when women reported moderately severe depression, highlighting a vulnerability to life-event stressors. Our results confirmed the finding that prior traumas seem to increase reactivity to and potential harm of new trauma [65].
Pre-existing mental health conditions increased more than 10-fold the likelihood of exhibiting severe depression, confirming this factor as a risk factor, in line with previous studies [65,68,79]., The finding concerning the predictive value of lower educational attainment, which led to a more than 5-fold increase in the likelihood of experiencing severe depression, provides further confirmation of previous literature data [68,79]. The identified risk factor for the manifestation of severe depression, represented by the variable “complex life management during the COVID-19 pandemic”, seemed to include numerous issues related not only to women’s household duties and responsibilities and their “work–life” balance [30], but also to the lack of a job and financial independence, the absence of an affective relationship, family lifestyle, and social isolation [69]. Older age, higher education, and better family functioning were identified as protective factors in contrasting severe depression and were associated with a reduced burden of care in caregivers. Problem-solving abilities, pursuing personal goals, and avoiding overinvolvement in family or other problems represented the life skills needed to cope more effectively with the consequence of a deepening depression caused by pandemic-related difficulties. This finding does not yet seem to have been addressed in literature.
Our initial hypothesis relating to variables capable of influencing severe depression in women was only partially confirmed by our estimated comprehensive psychosocial model. Pre-existing mental health conditions suggested an underlying vulnerability which heavily influenced the manifestation of severe depression. With regard to the role of traumas, our study did not take into consideration exposure to adverse childhood experiences (ACEs) known to act as pervasive risk factors for developing major mental and somatic disorders across the lifespan and for reduced longevity [80]. Nevertheless, the findings obtained in our study population suggest the impact of previous traumas, such as the collective traumatic experience of the earthquake, which seem less enduring and stable than ACEs, but nonetheless play a relevant “retraumatization” role, source of the presentation of psychopathological moderate depression.
4.1. Strengths and limitation
To the best of our knowledge, this is the first Italian study to evaluate depressive symptomatology during the COVID-19 pandemic in a general female population, taking into account the women's working roles, experience of caring for disabled people, and influence of previous catastrophic events.
Furthermore, this study represents a step towards verifying the need for identifying and preventing an escalation of mental health problems deriving from the pandemic, in line with the Sustainable Development Goals proposed by the United Nations Organization, namely Goals 3 and 5.
According to the United Nations, Goal 3 aspires to ensure health and well-being for all. Campaigns and events, such as the women's health events generally promoted by ONDA, which we took part in and reported on in this study, contribute to the early identification and destigmatization of mental disorders from a gender perspective. Our Goal 3 is closely related to Goal 5, pursuing gender equality and empowerment, identifying multiple areas of commitment towards women’s challenges, and topical issues for gender equality, including work-life balance and disabled caregiving, which strongly impact, not only during a pandemic, on their lives,.
Nevertheless, this study presents several limitations. Firstly, the present study shows a primary limit in sample recruitment. Street interviews are one of the fastest and most accurate forms of real-time data collection. In this data collection, respondents are approached on the street and asked targeted questions. Researchers registered their responses using an electronic device such as a tablet, iPad, or pen and paper. We estimate a potential bias in agreeing to the interview, reflecting that women with problematic symptoms will be more likely to accept the invitation in order to share their emotional distress.
Secondly, we were only able to involve a limited sample of women because of the time of the interview.
Thirdly, depression categorizations were based on a questionnaire, the PHQ-9. Although PHQ-9 is “an instrument for making criteria-based diagnoses of depressive and other mental disorders commonly encountered in primary care … reliable and valid measure of depression severity” [54], this type of measure cannot replace a more comprehensive clinical assessment.
Fourth, due to the selectivity of our sample, our findings are of limited generalizability, also in view of the territory and the consequences for residents of the catastrophic 2009 L’Aquila earthquake. The evacuation of the town, displacement, temporary accommodation - more than 10,000 people are still living in temporary housing, slow rebuilding [52], social and economic consequences on the community and the COVID-19 pandemic have led to a situation where, for the residents, life in the town has never truly “returned to normal”, as is the case of geographical areas experiencing “unique circumstances and challenges” [65].
5. Conclusions
The present study, conducted in a nonclinical sample of women, investigated the impact of the COVID-19 pandemic on working activities, caregiving responsibilities, and family functioning.
The results obtained suggest that the pandemic produced a more serious impact on the mental health of non-working women and caregivers of family members with pre-existing psychiatric conditions. Therefore, based on our findings, during the pandemic, difficulties in life management did not seem to be intended “tout-court” as a “work–life balance” distress but rather as a more comprehensive distress (“life is hard”), presumably due to the lack of a job and financial independence, the responsibilities of taking care of relatives, absence of an affective relationship, and social isolation.
A series of factors concurred to influence in women the onset of depression and severity of symptoms in response to the pandemic, almost as though the pandemic had partly reflected the cumulative effects of traumas. Interestingly, the value of women’s protective skills against depression, such as problem-solving abilities, pursuing individual goals, and taking care of themselves first without necessarily prioritizing the need of family and others came to the forefront. These characteristics are an antithesis to those commonly used to describe the stereotypical Italian “woman and mom”.
The findings of our study should be expanded to address further in-depth studies focused on the complexities of psychopathological frailties in women and their individual and psychosocial strengths following life stressors and “immersive” traumatic events such as the COVID-19 pandemic. The ultimate aim will be to translate the findings obtained into evidence-based, gender-specific, personalized clinical strategies for the purpose of improving the mental health of women in everyday life.
Author Contributions
Conceptualization, R.R., L.G. and M.C.; Methodology, L.G. and S.M.; Formal Analysis, S.M.; Investigation, S.M., S.D.V., A.S..; Data Curation, S.M.; Writing – Original Draft Preparation, R.R.; Writing – Review & Editing, R.R., L.G.; Visualization, S.M.; Supervision, M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of L’Aquila, Italy (n. 58-2021-2022), date of approval 26 October 2021).
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We would like to thank Dr. Giovanna Micolucci and Dr. Raffaella Anna Lepore, Hospital Management of San Salvatore Hospital, L’Aquila, Italy, for supporting our initiative as part of a broader health campaign promoted by the ONDA Foundation, Italy. We would like to thank Donatella Ussorio for her professional support in conducting the interviews and Luigia Marcocci for her technical support. The publication of this article was supported by the Department of Life, Health, and Environmental Sciences, University of L’Aquila, L’Aquila, Italy (Competitive Call for Internal Research Projects 2021, R.R., L.G.).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shockley, K.M.; Clark, M.A.; Dodd, H.; King, E.B. Work-family strategies during COVID-19: Examining gender dynamics among dual-earner couples with young children. J Appl Psychol 2021, 106, 15-28. [CrossRef]
- Wanberg, C.R.; Csillag, B.; Douglass, R.P.; Zhou, L.; Pollard, M.S. Socioeconomic status and well-being during COVID-19: A resource-based examination. J Appl Psychol 2020, 105, 1382-1396. [CrossRef]
- Pai, N.; Vella, S.L. COVID-19 and loneliness: A rapid systematic review. Aust N Z J Psychiatry 2021, 55, 1144-1156. [CrossRef]
- Lampraki, C.; Hoffman, A.; Roquet, A.; Jopp, D.S. Loneliness during COVID-19: Development and influencing factors. PLoS One 2022, 17, e0265900. [CrossRef]
- Currin, J.M.; Evans, A.E.; Miller, B.M.; Owens, C.; Giano, Z.; Hubach, R.D. The impact of initial social distancing measures on individuals' anxiety and loneliness depending on living with their romantic/sexual partners. Curr Psychol 2022, 1-9. [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr 2020, 33, e100213. [CrossRef]
- Giusti, L.; Salza, A.; Mammarella, S.; Bianco, D.; Ussorio, D.; Casacchia, M.; Roncone, R. #Everything Will Be Fine. Duration of Home Confinement and "All-or-Nothing" Cognitive Thinking Style as Predictors of Traumatic Distress in Young University Students on a Digital Platform During the COVID-19 Italian Lockdown. Front Psychiatry 2020, 11, 574812. [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int J Environ Res Public Health 2020, 17. [CrossRef]
- Horesh, D.; Brown, A.D. Traumatic stress in the age of COVID-19: A call to close critical gaps and adapt to new realities. Psychol Trauma 2020, 12, 331-335. [CrossRef]
- Lima, C.K.T.; Carvalho, P.M.M.; Lima, I.; Nunes, J.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res 2020, 287, 112915. [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J Psychiatr 2020, 52, 102066. [CrossRef]
- Alzueta, E.; Perrin, P.; Baker, F.C.; Caffarra, S.; Ramos-Usuga, D.; Yuksel, D.; Arango-Lasprilla, J.C. How the COVID-19 pandemic has changed our lives: A study of psychological correlates across 59 countries. J Clin Psychol 2021, 77, 556-570. [CrossRef]
- Zhao, S.Z.; Wong, J.Y.H.; Luk, T.T.; Wai, A.K.C.; Lam, T.H.; Wang, M.P. Mental health crisis under COVID-19 pandemic in Hong Kong, China. Int J Infect Dis 2020, 100, 431-433. [CrossRef]
- Cecchini, J.A.; Carriedo, A.; Fernandez-Rio, J.; Mendez-Gimenez, A.; Gonzalez, C.; Sanchez-Martinez, B.; Rodriguez-Gonzalez, P. A longitudinal study on depressive symptoms and physical activity during the Spanish lockdown. Int J Clin Health Psychol 2021, 21, 100200. [CrossRef]
- Bianchini, V.; Giusti, L.; Salza, A.; Cofini, V.; Cifone, M.G.; Casacchia, M.; Fabiani, L.; Roncone, R. Moderate Depression Promotes Posttraumatic Growth (Ptg): A Young Population Survey 2 Years after the 2009 L'Aquila Earthquake. Clin Pract Epidemiol Ment Health 2017, 13, 10-19. [CrossRef]
- Gao, X.; Leng, Y.; Guo, Y.; Yang, J.; Cui, Q.; Geng, B.; Hu, H.; Zhou, Y. Association between earthquake experience and depression 37 years after the Tangshan earthquake: a cross-sectional study. BMJ Open 2019, 9, e026110. [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int J Environ Res Public Health 2020, 17. [CrossRef]
- Pancani, L.; Marinucci, M.; Aureli, N.; Riva, P. Forced Social Isolation and Mental Health: A Study on 1,006 Italians Under COVID-19 Lockdown. Front Psychol 2021, 12, 663799. [CrossRef]
- Carpiniello, B.; Tusconi, M.; Zanalda, E.; Di Sciascio, G.; Di Giannantonio, M.; Executive Committee of The Italian Society of, P. Psychiatry during the Covid-19 pandemic: a survey on mental health departments in Italy. BMC Psychiatry 2020, 20, 593. [CrossRef]
- Almeida, M.; Shrestha, A.D.; Stojanac, D.; Miller, L.J. The impact of the COVID-19 pandemic on women's mental health. Arch Women Ment Hlth 2020, 23, 741-748. [CrossRef]
- Thibaut, F.; van Wijngaarden-Cremers, P.J.M. Women's Mental Health in the Time of Covid-19 Pandemic. Front Glob Womens Health 2020, 1, 588372. [CrossRef]
- Liu, H.; Wang, L.L.; Zhao, S.J.; Kwak-Kim, J.; Mor, G.; Liao, A.H. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. J Reprod Immunol 2020, 139, 103122. [CrossRef]
- Santomauro, D.F.; Mantilla Herrera, A.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. The Lancet 2021, 398, 1700-1712. [CrossRef]
- Street, A.E.; Dardis, C.M. Using a social construction of gender lens to understand gender differences in posttraumatic stress disorder. Clin Psychol Rev 2018, 66, 97-105. [CrossRef]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav Immun 2020, 87, 100-106. [CrossRef]
- Campbell, A.M. An increasing risk of family violence during the Covid-19 pandemic: Strengthening community collaborations to save lives. Forensic Science International: Reports 2020, 2. [CrossRef]
- Romito, P.; Pellegrini, M.; Saurel-Cubizolles, M.J. Intimate Partner Violence Against Women During the COVID-19 Lockdown in Italy: A Multicenter Survey Involving Anti-Violence Centers. Violence Against Women 2022, 28, 2186-2203. [CrossRef]
- Piquero, A.R.; Jennings, W.G.; Jemison, E.; Kaukinen, C.; Knaul, F.M. Domestic violence during the COVID-19 pandemic - Evidence from a systematic review and meta-analysis. Journal of Criminal Justice 2021, 74. [CrossRef]
- Leroy, S.; Schmidt, A.M.; Madjar, N. Working from home during COVID-19: A study of the interruption landscape. J Appl Psychol 2021, 106, 1448-1465. [CrossRef]
- Loezar-Hernandez, M.; Briones-Vozmediano, E.; Ronda-Perez, E.; Otero-Garcia, L. Juggling during Lockdown: Balancing Telework and Family Life in Pandemic Times and Its Perceived Consequences for the Health and Wellbeing of Working Women. Int J Environ Res Public Health 2023, 20. [CrossRef]
- Matthews, T.A.; Chen, L.; Omidakhsh, N.; Zhang, D.; Han, X.; Chen, Z.; Shi, L.; Li, Y.; Wen, M.; Li, H.; et al. Gender difference in working from home and psychological distress - A national survey of U.S. employees during the COVID-19 pandemic. Ind Health 2022, 60, 334-344. [CrossRef]
- Xiao, Y.; Becerik-Gerber, B.; Lucas, G.; Roll, S.C. Impacts of Working From Home During COVID-19 Pandemic on Physical and Mental Well-Being of Office Workstation Users. J Occup Environ Med 2021, 63, 181-190. [CrossRef]
- Möhring, K.; Naumann, E.; Reifenscheid, M.; Wenz, A.; Rettig, T.; Krieger, U.; Friedel, S.; Finkel, M.; Cornesse, C.; Blom, A.G. The COVID-19 pandemic and subjective well-being: longitudinal evidence on satisfaction with work and family. European Societies 2020, 23, S601-S617. [CrossRef]
- Burn, E.; Tattarini, G.; Williams, I.; Lombi, L.; Gale, N.K. Women's Experience of Depressive Symptoms While Working From Home During the COVID-19 Pandemic: Evidence From an International Web Survey. Front Sociol 2022, 7, 763088. [CrossRef]
- Damian, A.C.; Ciobanu, A.M.; Anghele, C.; Papacocea, I.R.; Manea, M.C.; Iliuta, F.P.; Ciobanu, C.A.; Papacocea, S. Caregiving for Dementia Patients during the Coronavirus Pandemic. J Clin Med 2023, 12. [CrossRef]
- Zwar, L.; Konig, H.H.; Hajek, A. Gender Differences in Mental Health, Quality of Life, and Caregiver Burden among Informal Caregivers during the Second Wave of the COVID-19 Pandemic in Germany: A Representative, Population-Based Study. Gerontology 2022, 1-14. [CrossRef]
- Maggio, M.G.; La Rosa, G.; Calatozzo, P.; Andaloro, A.; Foti Cuzzola, M.; Cannavo, A.; Militi, D.; Manuli, A.; Oddo, V.; Pioggia, G.; et al. How COVID-19 Has Affected Caregivers' Burden of Patients with Dementia: An Exploratory Study Focusing on Coping Strategies and Quality of Life during the Lockdown. J Clin Med 2021, 10. [CrossRef]
- Dhiman, S.; Sahu, P.K.; Reed, W.R.; Ganesh, G.S.; Goyal, R.K.; Jain, S. Impact of COVID-19 outbreak on mental health and perceived strain among caregivers tending children with special needs. Res Dev Disabil 2020, 107, 103790. [CrossRef]
- Busse, C.; Barnini, T.; Zucca, M.; Rainero, I.; Mozzetta, S.; Zangrossi, A.; Cagnin, A. Depression, Anxiety and Sleep Alterations in Caregivers of Persons With Dementia After 1-Year of COVID-19 Pandemic. Front Psychiatry 2022, 13, 826371. [CrossRef]
- Eckardt, J.P. Caregivers of people with severe mental illness in the COVID-19 pandemic. The Lancet Psychiatry 2020, 7. [CrossRef]
- Fusar-Poli, L.; Surace, T.; Meo, V.; Patania, F.; Avanzato, C.; Pulvirenti, A.; Aguglia, E.; Signorelli, M.S. Psychological well-being and family distress of Italian caregivers during the COVID-19 outbreak. J Community Psychol 2022, 50, 2243-2259. [CrossRef]
- Stanley, S.; Balakrishnan, S.; Ilangovan, S. Psychological distress, perceived burden and quality of life in caregivers of persons with schizophrenia. J Ment Health 2017, 26, 134-141. [CrossRef]
- Yasuma, N.; Yamaguchi, S.; Ogawa, M.; Shiozawa, T.; Abe, M.; Igarashi, M.; Kawaguchi, T.; Sato, S.; Nishi, D.; Kawakami, N.; et al. Care difficulties and burden during COVID-19 pandemic lockdowns among caregivers of people with schizophrenia: A cross-sectional study. Neuropsychopharmacol Rep 2021, 41, 242-247. [CrossRef]
- Mork, E.; Aminoff, S.R.; Barrett, E.A.; Simonsen, C.; Hegelstad, W.T.V.; Lagerberg, T.V.; Melle, I.; Romm, K.L. COVID-19 lockdown - who cares? The first lockdown from the perspective of relatives of people with severe mental illness. BMC Public Health 2022, 22, 1104. [CrossRef]
- Jesus, T.S.; Bhattacharjya, S.; Papadimitriou, C.; Bogdanova, Y.; Bentley, J.; Arango-Lasprilla, J.C.; Kamalakannan, S.; The Refugee Empowerment Task Force International Networking Group Of The American Congress Of Rehabilitation, M. Lockdown-Related Disparities Experienced by People with Disabilities during the First Wave of the COVID-19 Pandemic: Scoping Review with Thematic Analysis. Int J Environ Res Public Health 2021, 18. [CrossRef]
- Kinser, P.A.; Lyon, D.E. A conceptual framework of stress vulnerability, depression, and health outcomes in women: potential uses in research on complementary therapies for depression. Brain Behav 2014, 4, 665-674. [CrossRef]
- Roncone, R.; Giusti, L.; Mazza, M.; Bianchini, V.; Ussorio, D.; Pollice, R.; Casacchia, M. Persistent fear of aftershocks, impairment of working memory, and acute stress disorder predict post-traumatic stress disorder: 6-month follow-up of help seekers following the L'Aquila earthquake. Springerplus 2013, 2, 636. [CrossRef]
- Casacchia, M.; Bianchini, V.; Mazza, M.; Pollice, R.; Roncone, R. Acute stress reactions and associated factors in the help-seekers after the L'Aquila earthquake. Psychopathology 2013, 46, 120-130. [CrossRef]
- Casacchia, M.; Pollice, R.; Roncone, R. The narrative epidemiology of L'Aquila 2009 earthquake. Epidemiol Psychiatr Sci 2012, 21, 13-21. [CrossRef]
- Cofini, V.; Carbonelli, A.; Cecilia, M.R.; di Orio, F. Quality of life, psychological wellbeing and resilience: a survey on the Italian population living in a new lodging after the earthquake of April 2009. Ann Ig 2014, 26, 46-51. [CrossRef]
- Gigantesco, A.; Mirante, N.; Granchelli, C.; Diodati, G.; Cofini, V.; Mancini, C.; Carbonelli, A.; Tarolla, E.; Minardi, V.; Salmaso, S.; et al. Psychopathological chronic sequelae of the 2009 earthquake in L'Aquila, Italy. J Affect Disord 2013, 148, 265-271. [CrossRef]
- Imperiale, A.J.; Vanclay, F. The mechanism of disaster capitalism and the failure to build community resilience: learning from the 2009 earthquake in L'Aquila, Italy. Disasters 2021, 45, 555-576. [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737-1744. [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001, 16, 606-613. [CrossRef]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. . Med. Care 1992, 30, 473-483.
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey. Journal of Clinical Epidemiology 1998, 51, 1025-1036. [CrossRef]
- Roncone, R.; Mazza, M.; Ussorio, D.; Pollice, R.; Falloon, I.R.; Morosini, P.; Casacchia, M. The questionnaire of family functioning: a preliminary validation of a standardized instrument to evaluate psychoeducational family treatments. Community Ment Health J 2007, 43, 591-607. [CrossRef]
- Morosini, P.; Roncone, R.; Veltro, F.; Palomba, U.; Casacchia, M. Routine assessment tool in psychiatry: the case of questionnaire of family attitude and burden Italian Journal of Psychiatry and Behavioural Sciences 1991, 1, 95-101.
- Andrews, G.; Hunt, C.; Jarry, M.; Morosini, P.; Roncone, R.; Tibaldi, G. Disturbi mentali. Competenze di base, strumenti e tecniche per tutti gli operatori.; Centro Scientifico Editore: Torino, 2004.
- Roncone, R.; Giusti, L.; Bianchini, V.; Casacchia, M.; Carpiniello, B.; Aguglia, E.; Altamura, M.; Barlati, S.; Bellomo, A.; Bucci, P.; et al. Family functioning and personal growth in Italian caregivers living with a family member affected by schizophrenia: Results of an add-on study of the Italian network for research on psychoses. Front Psychiatry 2022, 13, 1042657. [CrossRef]
- Yazawa, A.; Aida, J.; Kondo, K.; Kawachi, I. Gender differences in risk of posttraumatic stress symptoms after disaster among older people: Differential exposure or differential vulnerability? J Affect Disord 2022, 297, 447-454. [CrossRef]
- Ribe, J.M.; Salamero, M.; Perez-Testor, C.; Mercadal, J.; Aguilera, C.; Cleris, M. Quality of life in family caregivers of schizophrenia patients in Spain: caregiver characteristics, caregiving burden, family functioning, and social and professional support. Int J Psychiatry Clin Pract 2018, 22, 25-33. [CrossRef]
- Barrowclough, C.; Gooding, P.; Hartley, S.; Lee, G.; Lobban, F. Factors associated with distress in relatives of a family member experiencing recent-onset psychosis. J Nerv Ment Dis 2014, 202, 40-46. [CrossRef]
- Ilhan, B.; Berikol, G.B.; Eroglu, O.; Deniz, T. Prevalence and associated risk factors of post-traumatic stress disorder among survivors of the 2023 Turkey earthquake. Am J Emerg Med 2023, 72, 39-43. [CrossRef]
- Pazderka, H.; Shalaby, R.; Eboreime, E.; Mao, W.; Obuobi-Donkor, G.; Agyapong, B.; Oluwasina, F.; Adu, M.K.; Owusu, E.; Sapara, A.; et al. Isolation, Economic Precarity, and Previous Mental Health Issues as Predictors of PTSD Status in Females Living in Fort McMurray During COVID-19. Front Psychiatry 2022, 13, 837713. [CrossRef]
- Wenham, C.; Smith, J.; Davies, S.E.; Feng, H.; Grepin, K.A.; Harman, S.; Herten-Crabb, A.; Morgan, R. Women are most affected by pandemics - lessons from past outbreaks. Nature 2020, 583, 194-198. [CrossRef]
- Wenham, C.; Smith, J.; Morgan, R.; Gender; Group, C.-W. COVID-19: the gendered impacts of the outbreak. Lancet 2020, 395, 846-848. [CrossRef]
- Bu, F.; Steptoe, A.; Fancourt, D. Loneliness during a strict lockdown: Trajectories and predictors during the COVID-19 pandemic in 38,217 United Kingdom adults. Soc Sci Med 2020, 265, 113521. [CrossRef]
- Purvis, R.S.; Ayers, B.L.; Rowland, B.; Moore, R.; Hallgren, E.; McElfish, P.A. "Life is hard": How the COVID-19 pandemic affected daily stressors of women. Dialogues Health 2022, 1, 100018. [CrossRef]
- Keitner, G.I.; Miller, I.W. Family functioning and major depression: an overview. Am J Psychiatry 1990, 147, 1128-1137. [CrossRef]
- Herr, N.R.; Hammen, C.; Brennan, P.A. Current and past depression as predictors of family functioning: a comparison of men and women in a community sample. J Fam Psychol 2007, 21, 694-702. [CrossRef]
- Febres, J.; Rossi, R.; Gaudiano, B.A.; Miller, I.W. Differential relationship between depression severity and patients' perceived family functioning in women versus in men. J Nerv Ment Dis 2011, 199, 449-453. [CrossRef]
- Fondazione ONDA Osservatorio nazionale sulla salute della donna e di genere. COVID-19 e salute di genere: da pandemia a sindemia. Esperienze, nuove consapevolezze, sfide future. Libro bianco 2021; Franco Angeli: Milano, 2021.
- Arpino, B.; Pasqualini, M. Effects of Pandemic on Feelings of Depression in Italy: The Role of Age, Gender, and Individual Experiences During the First Lockdown. Front Psychol 2021, 12, 660628. [CrossRef]
- Wormald, A.; McGlinchey, E.; D'Eath, M.; Leroi, I.; Lawlor, B.; McCallion, P.; McCarron, M.; O'Sullivan, R.; Chen, Y. Impact of COVID-19 Pandemic on Caregivers of People with an Intellectual Disability, in Comparison to Carers of Those with Other Disabilities and with Mental Health Issues: A Multicountry Study. Int J Environ Res Public Health 2023, 20. [CrossRef]
- Rainero, I.; Bruni, A.C.; Marra, C.; Cagnin, A.; Bonanni, L.; Cupidi, C.; Lagana, V.; Rubino, E.; Vacca, A.; Di Lorenzo, R.; et al. The Impact of COVID-19 Quarantine on Patients With Dementia and Family Caregivers: A Nation-Wide Survey. Front Aging Neurosci 2020, 12, 625781. [CrossRef]
- Boyd, K.; Winslow, V.; Borson, S.; Lindau, S.T.; Makelarski, J.A. Caregiving in a Pandemic: Health-Related Socioeconomic Vulnerabilities Among Women Caregivers Early in the COVID-19 Pandemic. Ann Fam Med 2022, 20, 406-413. [CrossRef]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family - caregivers of people with mental illnesses. World J Psychiatry 2016, 6, 7-17. [CrossRef]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry 2021, 8, 141-149. [CrossRef]
- Holz, N.E.; Berhe, O.; Sacu, S.; Schwarz, E.; Tesarz, J.; Heim, C.M.; Tost, H. Early Social Adversity, Altered Brain Functional Connectivity, and Mental Health. Biol Psychiatry 2023, 93, 430-441. [CrossRef]
Figure 1.
Comparison of health-related quality of life in its eight dimensions in female workers and non-workers. T-test *p=<0.05.
Figure 1.
Comparison of health-related quality of life in its eight dimensions in female workers and non-workers. T-test *p=<0.05.
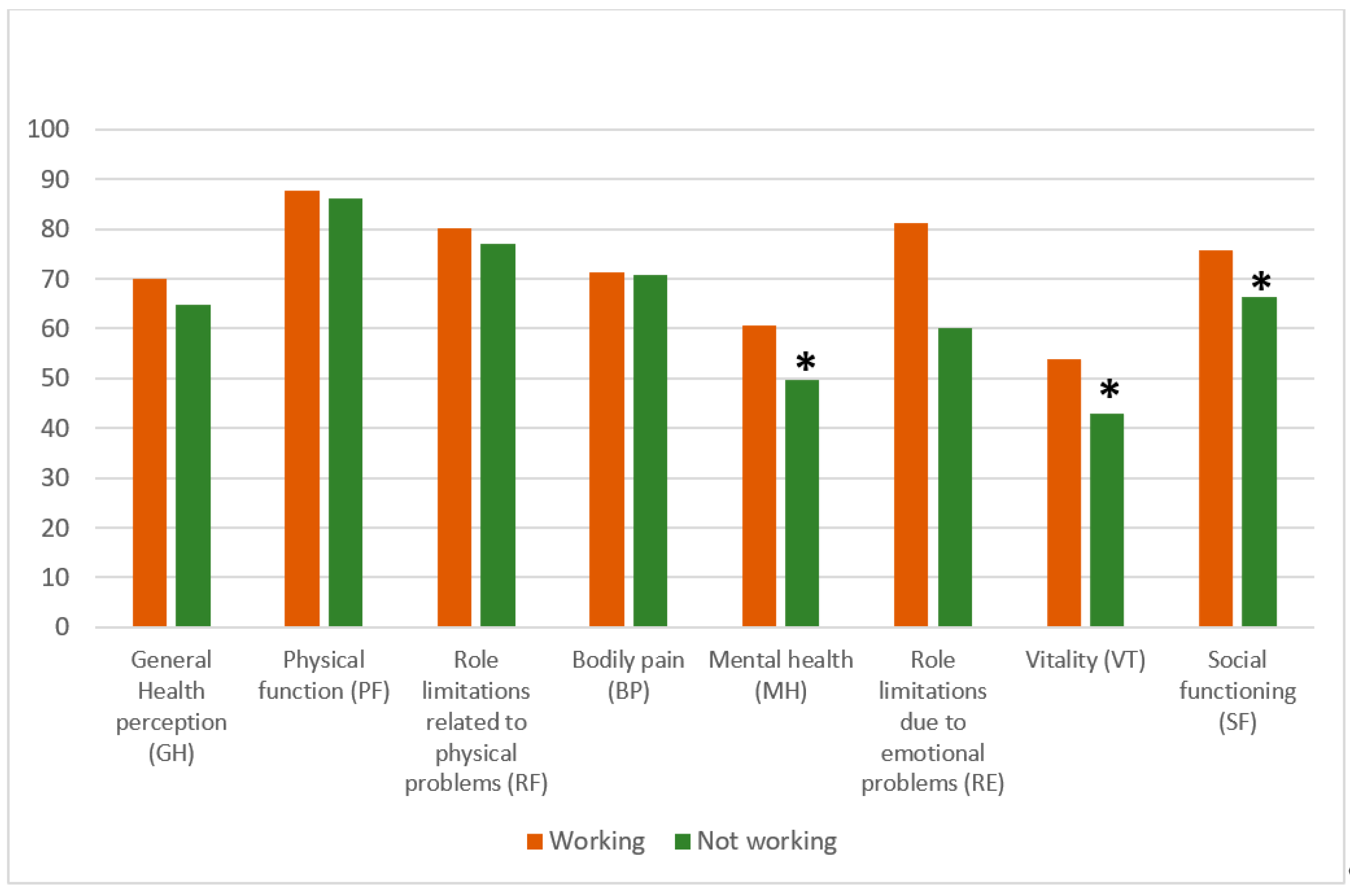
Figure 2.
Health-related quality of life in its eight dimensions in caregiving and non-caregiving women. T-test *p=<0.05.
Figure 2.
Health-related quality of life in its eight dimensions in caregiving and non-caregiving women. T-test *p=<0.05.
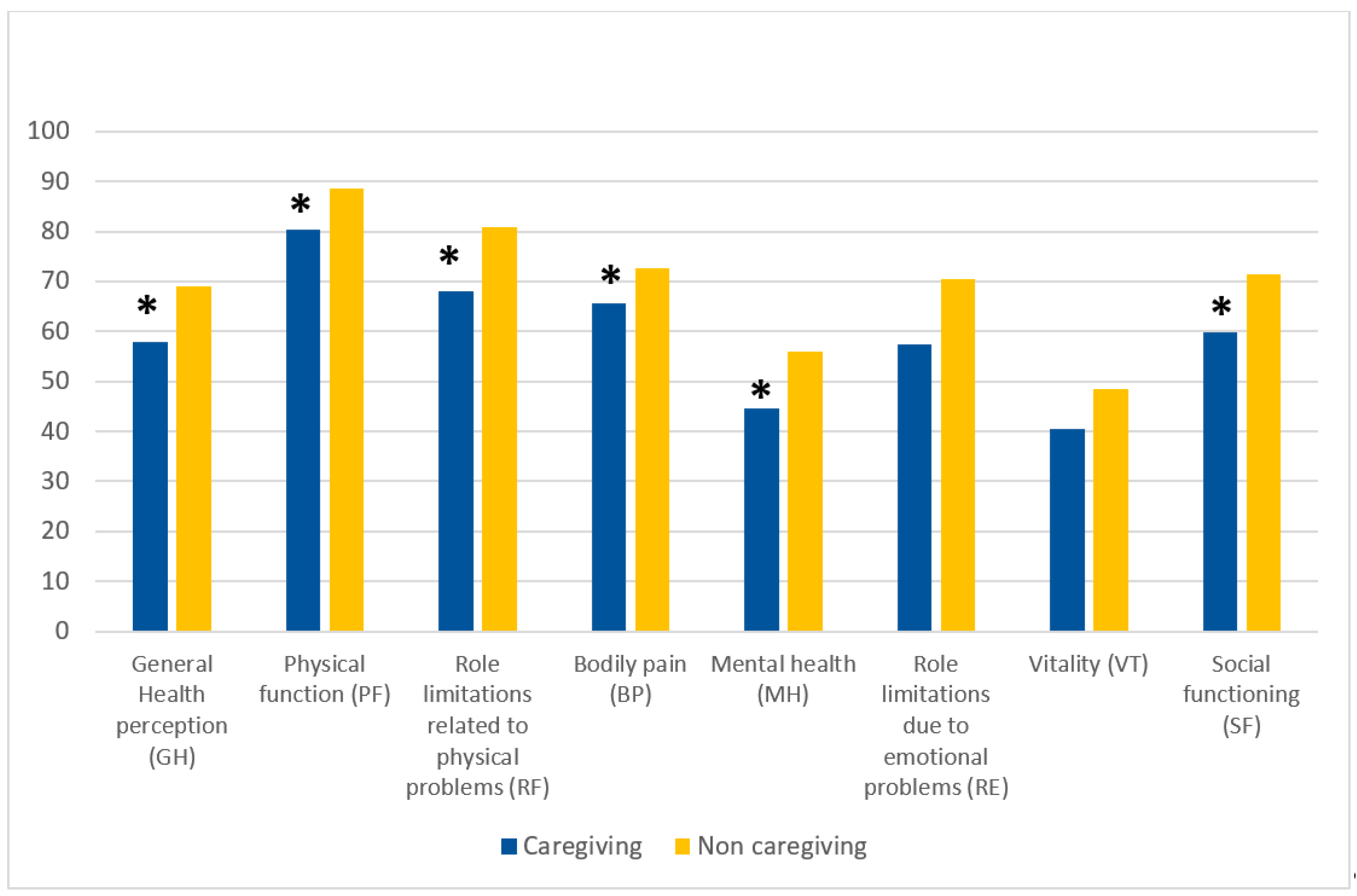
Table 2.
Comparison of life events and clinical characteristics of the sample of female workers and non-workers (n= 211).
Table 2.
Comparison of life events and clinical characteristics of the sample of female workers and non-workers (n= 211).
| Variables | Working (n=73) |
Not-working (n=138) |
|---|---|---|
| Complex management of family life and work during COVID-19 pandemic (%) |
31 (42.5) |
77 (55.8) |
| Infection with COVID-19 (%) | 9 (12.3) | 12 (8.7) |
| Refusal of COVID-19 vaccination (%) | 6 (8.2) | 10 (7.2) |
| Loss of someone close to COVID-19 (%)* | 7 (9.6) | 21 (15.2) |
| Subjected to the 2009 L'Aquila earthquake (%) (n = 100)* | 45 (61.6) | 55 (39.9) |
| Loss of someone close in the 2009 L'Aquila earthquake (%) (n= 100) | 5 (11.1) | 10 (18.2) |
|
Severe impact of 2009 L'Aquila earthquake on (%) (n = 100 women exposed) (intensity: severe; very severe) |
||
| Family life | 21 (46.7) | 27 (49.1) |
| Work | 18 (40) | 13 (23.6) |
| Social life | 21 (46.7) | 22 (40) |
| Severe impairment due to the L’Aquila 2009 earthquake in two out of the three domains investigated (%) (n=43)* |
22 (30.1) |
21 (15.2) |
| Previous contact due to mental health problems (%) (n = 94) | 38 (52.1) | 56 (40.6) |
| Mental health problems reported (%) | ||
| Anxiety | 20 (27.4) | 40 (29) |
| Family and interpersonal problems | 13 (17.8) | 26 (18.8) |
| Depression | 14 (19.2) | 23 (16.7) |
| Sleep disorders | 9 (12.3) | 15 (10.9) |
| Eating disorders | 10 (13.7) | 12 (8.7) |
| Substance abuse | -- | 3 (2.2) |
| Other problems | 5 (6.8) | 14 (10.1) |
| Treatments | ||
| Admission to a psychiatric ward | -- | 2 (3.5) |
| Psychopharmacological treatment (n=39) | 11 | 28 |
| Type of drug | ||
| Anxiolytic drugs | 4 (36.4) | 8 (28.6) |
| Antidepressant drugs | 6 (54.5) | 14 (50) |
| Antipsychotic drugs | 1 (9.1) | 6 (21.4) |
*p<0.05.
Table 3.
Depressive symptomatology measured by PHQ-9, and family functioning measured by FFQ, in the two groups of female workers and non-workers included in the sample.
Table 3.
Depressive symptomatology measured by PHQ-9, and family functioning measured by FFQ, in the two groups of female workers and non-workers included in the sample.
| Variables | Total Sample (n=211) |
Workers (n=73) |
Non workers (n=138) |
|---|---|---|---|
| PHQ-9 Total mean score (SD)* | 9.5 (6.17) | 7.82 (5.7) | 10.30 (6.2) |
| PHQ-9 Total scoring >10 (%)* | 82 (40.2) | 19 (26) | 63 (45.7) |
| PHQ-9 score 1 - 5 – absent - mild depression (%) | 64 (30.3) | 28 (38.4) | 36 (26.1) |
| PHQ-9 score 6 - 10 – moderate depression (%) | 65 (30.8) | 26 (35.6) | 39 (28.3) |
| PHQ-9 score 11 - 15 - moderately severe depression (%) | 44 (20.9) | 9 (20.5) | 35 (25.4) |
| PHQ-9 score >15 - severe depression (%) | 38 (18) | 10 (26.3) | 28 (20.3) |
| Family Functioning Questionnaire (SD) | |||
| Communication* | 23.3 (4.8) | 24.9 (4.7) | 22.5 (4.6) |
| Problem-Solving* | 21.0 (6.7) | 23.6 (6.0) | 19.7 (6.7) |
| Personal Goals* | 23.8 (3.9) | 22.3 (3.8) | 24.5 (3.8) |
*p<0.05.
Table 4.
A comparison of socio-demographic and clinical characteristics in a sample of female non-caregivers and caregivers (n= 211).
Table 4.
A comparison of socio-demographic and clinical characteristics in a sample of female non-caregivers and caregivers (n= 211).
| Variables included | Non-caregivers (n=164) | Caregivers (n=47) |
|---|---|---|
| Age, mean (SD) | 35.3 (18.5) | 37.0 (18.8) |
| Range age | ||
| Young adults (18 – 35 years) (%) | 100 (61) | 26 (55.3) |
| Adults (%) | 51 (31.1) | 18 (38.3) |
| Over 65 (%) | 13 (7.9) | 3 (6.4) |
| Nationality (%) | ||
| Non-EU citizens | 7 (4.3) | 1 (2.1) |
| Marital status (%) | ||
| Single | 72 (43.9) | 21 (44.7) |
| Married/Partnership | 76 (46.3) | 23 (48.9) |
| Separated/ Divorced | 8 (4.9) | 3 (6.4) |
| Widowed | 8 (4.9) | -- |
| Parents of children (%) | ||
| no | 118 (71.3) | 29 (61.7) |
| 1 child | 15 (9.2) | 8 (17.0) |
| 2 children | 23 (14.1) | 6 (12.7) |
| 3 children | 8 (4.2) | 4 (10.6) |
| Level of education (%) | ||
| >13 years (graduated) | 70 (42.3) | 21 (44.7) |
| Working conditions (%) | ||
| Self-employed/freelancers | 15 (9.1) | 8 (17.0) |
| Full-time work | 32 (19.5) | 3 (6.4) |
| Part-time work | 11 (6.7) | 4 (8.5) |
| Student | 72 (43.9) | 19 (40.4) |
| Housewife | 9 (5.5) | 4 (8.5) |
| Unemployed | 9 (5.5) | 3 (6.4) |
| Retired | 16 (9.8) | 6 (12.8) |
| Socio-economic status (%) | ||
| High-upper middle income | 75 (45.7) | 20 (42.6) |
| Middle-low income | 66 (40.2) | 18 (38.3) |
| Struggling financially | 23 (14.0) | 9 (19.1) |
Table 5.
Life events and clinical characteristics of the comparative sample of female non-caregivers and caregivers (n= 211).
Table 5.
Life events and clinical characteristics of the comparative sample of female non-caregivers and caregivers (n= 211).
| Variables | Non-caregivers (n=164) | Caregivers (n=47) |
|---|---|---|
| Complex management of family life and work during COVID-19 pandemic (%) | 86 (52.4) | 22 (46.8) |
| COVID-19 infection (%) | 16 (9.8) | 5 (10.6) |
| Refusal of COVID-19 vaccination (%) | 11 (6.7) | 5 (10.6) |
| Loss of someone close to COVID-19 (%)* | 17 (10.4) | 11 (23.4) |
| Subjected to 2009 L'Aquila earthquake (%) (n = 100) | 77 (47) | 23 (48.9) |
| Loss of someone close in the 2009 L’Aquila earthquake (%) | 12 (15.5) | 3 (13) |
|
Severe impact of 2009 L'Aquila earthquake on (%) (n = 100 women exposed) (intensity: severe; very severe) |
||
| Family life | 37 (48) | 11 (47.8) |
| Work | 25 (32.4) | 6 (26.1) |
| Social life | 32 (41.5) | 11 (47.8) |
| Severe impairment due to the 2009 L'Aquila earthquake in two out of the three domains investigated (%) (n=43) | 33 (42.9) | 10 (43.5) |
| Previous contact due to mental health problems (%) (n = 94) | 71 (43.3) | 23 (48.9) |
| Mental health problems reported (%) | ||
| Anxiety | 42 (25.6) | 18 (38.3) |
| Family and interpersonal problems | 28 (17.1) | 11 (23.4) |
| Depression | 27 (16.5) | 10 (21.3) |
| Sleep disorders | 16 (9.8) | 8 (17) |
| Eating disorders | 17 (10.4) | 5 (10.6) |
| Substance abuse | 1 (0.6) | 2 (4.3) |
| Other problems | 16 (9.8) | 3 (6.4) |
| Treatments | ||
| Admission to a psychiatric ward | 1 | 1 |
| Integrated treatment (drug prescription + psychotherapy) | 14 (8.5) | 7 (14.8) |
| Psychopharmacological treatment (n=39) | 29 | 10 |
| Type of drug | ||
| Anxiolytic drugs | 10 (34.5) | 2 (20) |
| Antidepressant drugs | 16 (55.2) | 4 (40) |
| Antipsychotic drugs | 3 (10.3) | 4 (40) |
Table 6.
Depressive symptomatology measured by PHQ-9, and family functioning measured by FFQ in the two groups of women included in the sample.
Table 6.
Depressive symptomatology measured by PHQ-9, and family functioning measured by FFQ in the two groups of women included in the sample.
| Variables | Non-caregivers (n=164) |
Caregivers (n=47) |
|---|---|---|
| PHQ-9 Total mean score (SD) | 9.07 (5.8) | 11 (7.1) |
| PHQ-9 Total scoring >10 (%) | 59 (37.1) | 23 (51.1) |
| PHQ-9 score 1 - 5 – absent - mild depression (%) | 51 (31.1) | 13 (27.7) |
| PHQ-9 score 6 - 10 – moderate depression (%) | 54 (32.9) | 11 (23.4) |
| PHQ-9 score 11 - 15 - moderately severe depression | 35 (21.3) | 9 (19.1) |
| PHQ-9 score >15 - severe depression (%) | 24 (14.6) | 14 (29.8) |
| Family Functioning Questionnaire (SD) | ||
| Communication | 23.5 (4.4) | 22.7 (5.7) |
| Problem-Solving | 21.4 (6.6) | 19.8 (7.1) |
| Personal Goals | 24.0 (3.8) | 23.0 (4.3) |
Table 7.
Family functioning measured by FFQ, and family burden of care measured by FPQ in the two groups of female caregivers included in the sample.
Table 7.
Family functioning measured by FFQ, and family burden of care measured by FPQ in the two groups of female caregivers included in the sample.
| Physical Disability Caregivers (n=23) |
Mental Disability Caregivers (n=24) |
|
|---|---|---|
| Family Functioning | ||
| Communication | 22.6 (6.5) | 22.8 (5.1) |
| Problem-Solving | 20.6 (4.3) | 19.0 (6.5) |
| Personal Goals | 22.9 (4.6) | 23.0 (4.1) |
| Burden of care | ||
| Objective burden | 1.79 (0.50) | 1.86 (0.41) |
| Subjective burden* | 2.00 (0.54) | 2.64 (0.70) |
| Support received from professionals | 2.43 (0.92) | 2.51 (0.68) |
| Support received from relatives and friends* | 2.24 (0.98) | 2.80 (0.69) |
Table 8.
Correlations between age, years of education, and the 5 dimensions of the SF-36 (n = 211 women), PHQ-9 total score (n = 211 women), the 4 dimensions of burden of care measured by FPQ (n = 47 women), and the 3 dimensions of family functioning (n = 211) measured by FFQ.
Table 8.
Correlations between age, years of education, and the 5 dimensions of the SF-36 (n = 211 women), PHQ-9 total score (n = 211 women), the 4 dimensions of burden of care measured by FPQ (n = 47 women), and the 3 dimensions of family functioning (n = 211) measured by FFQ.
| Measures | Age | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Pearson’s Correlation | .304** | -- | ||||||||||||
| 2-tailed p-value | .000 | ||||||||||||||
|
Pearson’s Correlation | .245** | .143* | -- | |||||||||||
| 2-tailed p-value | .010 | .038 | |||||||||||||
|
Pearson’s Correlation | .413** | .202** | .512** | -- | ||||||||||
| 2-tailed p-value | .000 | .003 | .000 | ||||||||||||
|
Pearson’s Correlation | .380** | .322** | .451** | .628** | -- | |||||||||
| 2-tailed p-value | .000 | .000 | .000 | .000 | |||||||||||
|
Pearson’s Correlation | .419** | .204** | .590** | .835** | .646** | -- | ||||||||
| 2-tailed p-value | .000 | .003 | .000 | .000 | .000 | ||||||||||
|
Pearson’s Correlation | .412** | .214** | .542** | .755** | .611** | .697** | -- | |||||||
| 2-tailed p-value | .001 | .002 | .000 | .000 | .000 | .000 | |||||||||
|
Pearson’s Correlation | -.452** | -.310** | -.560** | -.836** | -.681** | -.799** | -.738** | -- | ||||||
| 2-tailed p-value | .000 | .000 | .000 | .000 | .000 | .000 | .000 | ||||||||
|
Pearson’s Correlation | -.171 | -.151 | -.384** | -.207 | -.354* | -.337* | -.300* | .332* | -- | |||||
| 2-tailed p-value | .249 | .312 | .008 | .162 | .015 | .020 | .040 | .023 | |||||||
|
Pearson’s Correlation | -.076 | -.011 | -.292* | -.545** | -.391** | -.631** | -.550** | .501** | .563** | -- | ||||
| 2-tailed p-value | .612 | .940 | .047 | .000 | .007 | .000 | .000 | .000 | .000 | ||||||
|
Pearson’s Correlation | .020 | -.179 | -.207 | -.342* | -.155 | -.412** | -.231 | .303* | .232 | .304* | -- | |||
| 2-tailed p-value | .892 | .228 | .163 | .019 | .298 | .004 | .118 | .039 | .116 | .038 | |||||
|
Pearson’s Correlation | -.031 | -.186 | -.236 | -.200 | -.139 | -.336* | -.199 | .301* | .007 | .155 | .580** | -- | ||
| 2-tailed p-value | .836 | .211 | .111 | .178 | .352 | .021 | .179 | .040 | .962 | .299 | .000 | ||||
|
Pearson’s Correlation | .434** | .291** | .422** | .519** | .399* | .556** | .529** | -.569** | -.130 | -.110 | -.465** | -.453** | -- | |
| 2-tailed p-value | .000 | .000 | .000 | .000 | .010 | .000 | .000 | .000 | .385 | .462 | .001 | .001 | |||
|
Pearson’s Correlation | .382** | .214** | .404** | .442** | .324** | .460** | .433** | -.472** | -.290* | -.291* | -.373** | -.309* | .733** | -- |
| 2-tailed p-value | .000 | .002 | .000 | .000 | .002 | .000 | .000 | .000 | .048 | .047 | .010 | .034 | .000 | ||
|
Pearson’s Correlation | -.147* | -.167* | .350** | .208** | .131 | .233** | .277** | -.209** | -.261 | -.300* | -.403** | -.315* | .171* | .165* |
| 2-tailed p-value | .032 | .015 | .000 | .002 | .058 | .001 | .000 | .002 | .076 | .041 | .005 | .031 | .013 | .016 | |
Table 9.
Logistic multinominal regression for depression as dependent variable. PHQ-9=1 (absent/mild depression, score 0-5).
Table 9.
Logistic multinominal regression for depression as dependent variable. PHQ-9=1 (absent/mild depression, score 0-5).
| Variables | B | Standard error | Wald | df | p | Exp(B) | 95% confidence interval for Exp(B) | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||||||
| Moderate depression (PHQ-9 = scoring 2) |
Intercepts | 7.611 | 2.175 | 12.244 | 1 | .000 | |||
| Age | -.036 | .014 | 6.719 | 1 | .010 | .964 | .938 | .991 | |
| Lack of a stable romantic partnership | .124 | .454 | .075 | 1 | .784 | 1.132 | .465 | 2.756 | |
| Less than 13 years of education | .362 | .441 | .675 | 1 | .411 | 1.436 | .605 | 3.408 | |
| Struggling financially | -.427 | .770 | .307 | 1 | .579 | .652 | .144 | 2.952 | |
| Previous access to mental health services | .634 | .446 | 2.022 | 1 | .155 | 1.885 | .787 | 4.514 | |
| Traumatic experience with the 2009 L’Aquila earthquake | 1.369 | .552 | 6.142 | 1 | .013 | 3.932 | 1.332 | 11.612 | |
| COVID-19 infection | .239 | .724 | .109 | 1 | .742 | 1.270 | .307 | 5.248 | |
| Complex life management during the COVID-19 pandemic | .533 | .435 | 1.501 | 1 | .221 | 1.705 | .726 | 4.003 | |
| Caregiving for a loved one | -.129 | .571 | .051 | 1 | .821 | .879 | .287 | 2.693 | |
| Problem-solving | -.093 | .056 | 2.768 | 1 | .096 | .912 | .817 | 1.017 | |
| Communication | -.095 | .073 | 1.700 | 1 | .192 | .909 | .788 | 1.049 | |
| Personal goals | -.100 | .061 | 2.708 | 1 | .100 | .905 | .803 | 1.019 | |
| Moderately severe depression (PHQ-9 = scoring 3) |
Intercepts | 7.688 | 2.659 | 8.362 | 1 | .004 | |||
| Age | -.095 | .024 | 16.332 | 1 | .000 | .909 | .868 | .952 | |
| Lack of a stable romantic partnership | 1.101 | .568 | 3.759 | 1 | .053 | 3.006 | .988 | 9.148 | |
| Less than 13 years of education | .306 | .570 | .289 | 1 | .591 | 1.358 | .444 | 4.152 | |
| Struggling financially | .870 | .773 | 1.269 | 1 | .260 | 2.387 | .525 | 10.852 | |
| Previous access to mental health services | 1.956 | .576 | 11.548 | 1 | .001 | 7.070 | 2.288 | 21.842 | |
| Traumatic experience with the 2009 L’Aquila earthquake | 2.242 | .771 | 8.454 | 1 | .004 | 9.416 | 2.077 | 42.691 | |
| COVID-19 infection | -.073 | .955 | .006 | 1 | .939 | .930 | .143 | 6.039 | |
| Complex life management during the COVID-19 pandemic | 1.086 | .545 | 3.970 | 1 | .046 | 2.964 | 1.018 | 8.628 | |
| Caregiving for a loved one | .304 | .674 | .203 | 1 | .652 | 1.355 | .362 | 5.075 | |
| Problem-solving | -.164 | .063 | 6.666 | 1 | .010 | .849 | .750 | .961 | |
| Communication | -.029 | .084 | .123 | 1 | .726 | .971 | .824 | 1.145 | |
| Personal goals | -.127 | .078 | 2.628 | 1 | .105 | .881 | .756 | 1.027 | |
| Severe depression (PHQ-9 = scoring 4). |
Intercepts | 10.578 | 2.888 | 13.412 | 1 | .000 | |||
| Age | -.068 | .026 | 6.944 | 1 | .008 | .934 | .888 | .983 | |
| Lack of a stable romantic partnership | 1.113 | .674 | 2.730 | 1 | .098 | 3.044 | .813 | 11.399 | |
| Less than 13 years of education | 1.688 | .732 | 5.318 | 1 | .021 | 5.410 | 1.288 | 22.714 | |
| Struggling financially | 1.224 | .841 | 2.119 | 1 | .145 | 3.402 | .654 | 17.687 | |
| Previous access to mental health services | 2.391 | .675 | 12.541 | 1 | .000 | 10.923 | 2.908 | 41.020 | |
| Traumatic experience with the 2009 L’Aquila earthquake | 1.705 | .966 | 3.117 | 1 | .077 | 5.502 | .829 | 36.527 | |
| COVID-19 infection | -.483 | 1.068 | .204 | 1 | .651 | .617 | .076 | 5.008 | |
| Complex life management during the COVID-19 pandemic | 1.280 | .640 | 4.001 | 1 | .045 | 3.598 | 1.026 | 12.616 | |
| Caregiving for a loved one | 1.058 | .734 | 2.076 | 1 | .150 | 2.880 | .683 | 12.147 | |
| Problem-solving | -.234 | .073 | 10.438 | 1 | .001 | .791 | .686 | .912 | |
| Communication | -.124 | .095 | 1.725 | 1 | .189 | .883 | .734 | 1.063 | |
| Personal goals | -.222 | .088 | 6.368 | 1 | .012 | .801 | .674 | .952 | |
|
a. The reference category is 1. PHQ-9 absent / mild depression total score: 0-5 In bold: statistically significant values | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



