Submitted:
22 September 2023
Posted:
28 September 2023
You are already at the latest version
Abstract
The emergence of M. tuberculosis strains resistant to Isoniazid (INH) and Rifampicin (RIF), the two most potent drugs of first-line anti-TB therapy is termed multidrug drug-resistant TB (MDR-TB). Multidrug-resistant tuberculosis has been a serious medical and epidemic problem all over the world. We present here a series of clinical cases consist of two patients diagnosed with isoniazid resistant tuberculosis. Histopathological examination supports the diagnosis of tuberculous granulomas. And the pathology molecular examination revealed the presence of Isoniazid-resistant Mycobacterium tuberculosis1,2 via the following mutation c.947G>A; p.Gly316Asp. Isoniazid-resistance is associated with mutations in the furA-katG and fabG1-inhA operons, as well as mutations in the ahpC gene. 64% of the isoniazid-resistance phenotypes were associated with the katG315 mutation worldwide. The second most common mutation is inhA-15, and it has been reported in 19% of the Isoniazid-resistant isolates. The significant association between the two mutations, inhA c-15 and katG 315 respectively, and the high-level resistance is of interest in the interpretation of current and future molecular diagnostic testing, as an early prediction of the level of Isoniazid-resistance is essential to decide the benefit of high-dose Isoniazid use.
Keywords:
multidrug-resistant tuberculosis
; genetic mutations
; clinical cases.
Case no 1.
A 20-year-old non-smoking female patient, with no significant personal pathological history and no need for chronic treatment presents to the hospital for dry cough in the last 6 months and an episode of low-grade hemoptysis. No clinically significant findings at the physical examination, well preserved cardio-respiratory status. In the clinical and paraclinical context, the following preliminary investigations were requested: laboratory tests (complete blood count, electrolytes levels, coagulation tests, inflammatory markers), sputum microscopy for non-specific bacteria and Koch’s bacillus, GeneXpert, chest radiography, electrocardiogram. The chest X-ray revealed a heterogeneous left pulmonary basal consolidation process, and the following imaging investigations, such as chest CT scan, found a left pulmonary lower lobe consolidation process with a tendency to cavitation, raising the suspicion of bacillary foci (Figure 1). Sputum examination for Koch’s bacillus showed the presence of Mycobacterium tuberculosis (9 AFB per 100 HPF), with positive GenExpert genetic testing (low detected) and no resistance detected. Specific investigations were further carried out by performing bronchoscopy with bronchial biopsy, which revealed periorificial congestive infiltrative lesions at the apical level of the left lower lobe, with the histopathological examination supporting the diagnosis of endobronchial tuberculosis. Anti-tuberculosis treatment regimen I was initiated as follows HIN 300 mg per day, RMP 600 mg per day, EMB 800 mg per day, PZM 1500 mg per day. In dynamic at T2 (negative AFB at the microscopic examination and cultures), the patient has a good radiological outcome but with symptoms persistence, so the decision is to continue the intensive phase until T3. At T3, bronchoscopic and imaging reassessment is performed. The bronchoscopy showed mutilating bronchial statics changes in the LIL segments, with punctiform stenosis of one of the segments. And the imaging exam revealed the persistence of the left pulmonary lower lobe consolidations processes with air bronchogram and bilateral non-calcified pulmonary micronodular lesions. It is decided to move on to the continuation phase of the treatment with a customised regimen as follows: HIN 600 mg per day, RMP 600 mg per day, EMB 1200 mg per day.At T8, the patient is clinically asymptomatic, endoscopically unchanged, due to the presence of the punctiform stenosis of the LIL segment, and at the imaging exam, the retrostenotic changes are persistent. At this moment, it is not deemed necessary to continue the tuberculostatic treatment, and no surgical therapy is recommended for the remaining lesions. Over the next 12 months, multiple episodes of retrostenotic pneumonia occur from time to time. Imaging shows a clear lesional dynamics (Figure 2). Therefore, there is a suspicion of pulmonary malignancy including pulmonary sequestration syndrome, and further investigation by MR angiography of the thoracic aorta shows no aberrant arterial tracts from the thoracic aorta, left renal artery or the right atrium, specific to the pulmonary sequestration syndrome due to LIL consolidation (Figure 3). Subsequently, a surgical left lower lobectomy was performed, with a good outcome and complete recovery (Figure 4). Histopathological examination supports the diagnosis of tuberculous granulomas. And the pathology molecular examination revealed the presence of Isoniazid-resistant Mycobacterium tuberculosis 1,2 via the following mutation c.947G>A; p.Gly316Asp, a mutation that has not been yet described in medical literature (Figure 5). The patient’s outcome was good and it is not considered necessary to resume treatment. Drug resistance occurs when mutations or chromosomal replication errors occur in the genes encoding drug targeting or drug biotransformation mechanisms, and it has a significant impact on the efficacy of tuberculostatic therapy [1,2,3,4]. Isoniazid has potent bactericidal activity against Mycobacterium tuberculosis, primarily by inhibiting mycolic acid synthesis [5,6]. Isoniazid-resistance is associated with mutations in the furA-katG and fabG1-inhA operons, as well as mutations in the ahpC gene [5,7,8,9]. INH is a prodrug activated by the catalase-peroxidase enzyme encoded by the katG gene [8]. Mutations in the katG gene, reducing the gene activity related to INH, are among the main mechanisms of the INH-resistance [5,8]. Alternatively, INH-resistance may arise due to point mutations within the promoter region of the inhA operon or the inhA gene. Mutation within the promoter region of inhA can lead to an overexpression of inhA, resulting in a relative resistance to INH. InhA mutations can be the cause of cross-resistance to ethionamide [5,8,9]. 64% of the isoniazid-resistance phenotypes were associated with the katG315 mutation worldwide [10,11,12]. Although more than 300 different katG mutations have been identified, mutations within codon 315 are the most prevalent [11,12]. Moreover, a specific amino acid substitution (from serine to threonine) is responsible for 95% of the katG 315 mutations [12]. Mutations within the katG are associated with a wide range of moderate to high level Isoniazid-resistance [10]. The second most common mutation is inhA-15, and it has been reported in 19% of the Isoniazid-resistant isolates [12]. Mutations within the promoter region of inhA tend to result in a low-level phenotypic resistance. and they also confer resistance to second-line drugs, namely ethionamide and prothionamide [11,13]. The most prevalent mutation within the inhA promoter region is the c-15t mutation, which is present in a median of 19% of the clinically Isoniazid-resistant isolates worldwide [10,12].Mutations within the inhA promoter region were not associated with a poor outcome (treatment failure or death) of the first-line regimen I tuberculostatic treatment, although such mutations were associated with an increased risk of relapse. On the other hand, katG 315 mutations have been associated with a poor treatment outcome [10,14].These two mutations, katG315 and inhA-15, combined with ten of the most common mutations within the inhA promoter and ahpC-oxyR intergenic region explain 84% of the global Isoniazid-resistance phenotypes [10]. In conclusion, the significant association between the two mutations, inhA c-15 and katG 315 respectively, and the high-level resistance is of interest in the interpretation of current and future molecular diagnostic testing, as an early prediction of the level of Isoniazid-resistance is essential to decide the benefit of high-dose Isoniazid use [10]. LPA testing, such as MTBDRplus (Hain test), can reliably identify isolates containing these mutations and thus can predict the level of Isoniazid-resistance [15,16]. But an isolated katG or inhA mutation may suggest highly variable levels of minimum inhibitory concentration. Thus, inhA mutations do not always predict low resistance levels and katG mutations high resistance levels, so LPA testing may not be used to decide whether or not Isoniazid will be useful in a combination therapy regimen when only one of these mutations is detected [10]. Moreover, further research is necessary to investigate the real benefits of high-dose Isoniazid use in patients with low or moderate resistance caused by only one of the two mutations [10]. Local variability of the individual mutation frequency may limit the sensitivity of molecular diagnostic testing [12]. Therefore, well-designed systematic surveys and whole genome sequencing are needed in order to identify mutation frequencies across geographic regions where rapid molecular testing is currently implemented, providing a context for the interpretation of the results and the opportunity to improve the next generation of diagnostic tests [12].
Case no. 2
A 21-year-old male patient, smoker, with no occupational exposure to respiratory toxic substances and no significant personal pathological history, presents to the hospital with fever, chills, fatigability, posterior thoracic pain in the right hemithorax, poor appetite and slight weight loss, recurrent symptoms with onset 1 year ago. From the recent history, we note that the patient has been investigated multiple times in other medical services in the last 12 months and has had many chest CT scans showing bilateral upper lobe micronodular lesions, mediastinal micro-lymphadenopathy and recurrent left pleural effusion, and the last imaging examination also revealed minimal pelvic ascites. Patient with serial negative sputum examinations for Koch’s bacillus, at microscopy and cultures, diagnostic suspicion of Langerhans cell histiocytosis was raised. At that time, the investigations continued with a skull X-ray which revealed multiple osteolytic lesions and, following a haematological evaluation, a bone marrow biopsy was recommended in order to rule out a diagnosis of multiple myeloma. This hypothesis was later refuted by histopathological and immunohistochemical testing. The following investigations were requested and performed: laboratory tests (complete blood count, electrolytes levels, coagulation tests, inflammatory markers), sputum microscopy for non-specific bacteria and Koch’s bacillus, GeneXpert, contrast enhanced CT scans of the chest and brain, complex respiratory functional explorations, i.e., plethysmography + DLco-measurements, cardiology consultation and echocardiography, bronchoscopy with bronchoalveolar lavage and thoracentesis for diagnostic and therapeutic purposes. Laboratory tests revealed mild microcytic hypochromic anaemia and a significant inflammatory syndrome. Imaging examinations showed multiple bilateral diffuse pulmonary nodules and micronodules, in numerical progression from the previous assessments, as well as layered mediastinal adenopathy with slightly non-homogeneous iodophilia, progressive in size, and bilateral laterothoracic loculated pleural effusion. Brain CT refuted the previously detected osteolytic lesions (Figure 6). Pleural fluid analysis revealed an exudate (total proteins = 5.5 g/dL) with elevated ADA (adenosine deaminase) levels (77.7 U/L), and the cytological smear showed moderate lymphocytosis, with no tumour cells on the examined smear. Functionally, the patient has moderate restrictive ventilatory dysfunction, normal central flow resistance and severely decreased alveolar-capillary membrane gas transfer factor. At endoscopy, autofluorescence bronchoscopy did not detect actual or suspected proliferating lesions. Bronchial aspirate and bronchoalveolar lavage were non-specific. Diagnostic investigations continued with a right thoracotomy with lung biopsy and parietal pleura biopsy. Histopathological examination revealed pulmonary and pleural granulomatosis suggestive for a TB etiology (Figure 7a,b). Tuberculostatic treatment regimen I HRZE adjusted to patient’s weight was initated as follows HIN 300 mg per day, RMP 450 mg per day, EMB 800 mg per day, PZM 1500 mg per day. Since the beginning of the tuberculostatic treatment, the clinical outcomes have been less favourable, with the occurrence and persistence of gastrointestinal symptoms (postprandial abdominal pain, nausea, vomiting and loss of appetite), with intolerance to Isoniazid. At T2, the results of the liquid medium cultures for Koch’s bacillus from the lung fragment are positive, and the antibiogram showed resistance to Isoniazid, so it was decided to replace it with Levofloxacin 500 mg per day in the treatment regimen, with monthly ECG monitoring. The patient had a good drug tolerance, but mild gastrointestinal symptoms persisted. At T5, the patient required emergency admission to the General Surgery Department for diffuse abdominal pain, feculent vomiting and altered general condition. Surgical treatment was performed, intraoperatively the findings were inflammatory bowel disease, subocclusive syndrome, prevesical properitoneal abscess bilaterally fused in the paracolic gutters, for which viscerolysis, evacuation, lavage and drainage were performed. Following the investigations, the diagnosis of prevesical properitoneal TB bilaterally fused in the paracolic gutters was established. The patient’s postoperative outcome was good, with complete remission of the gastrointestinal symptoms. At T9, the patient is clinically asymptomatic, with a favourable outcome of the imaging changes described above, therefore there was no indication for continuing the tuberculostatic treatment.
Author Contributions
Conceptualization, T.B, F.D.M, A.C; methodology, T.B, F.D.M, A.C.; validation, F.D.M, A.C; form writing—T.B.; writing—review and editing, T.B, F.D.M, A.C.; visualization, T.B, F.D.M, A.C.; supervision, F.D.M, A.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from the subject involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila, through the institutional program Publish not Perish.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Seifert, M.; Catanzaro, D.; Catanzaro, A.; Rodwell, T.C. Genetic Mutations Associated with Isoniazid Resistance in Mycobacterium tuberculosis: A Systematic Review. PLOS ONE 2015, 10, e0119628. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Report. Geneva, Switzerland; WHO press; 2013.
- World Health Organization; Multidrug and Extensively Drug-Resistant TB 2010 Global Report of Surveillance and Response. Geneva, Switzerland; WHO press; 2010.
- Sougakoff, W. Molecular epidemiology of multidrug-resistant strains of Mycobacterium tuberculosis. Clin. Microbiol. Infect. 2011, 17, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Narmandakh, E.; Tumenbayar, O.; Borolzoi, T.; Erkhembayar, B.; Boldoo, T.; Dambaa, N.; Burneebaatar, B.; Nymadawa, N.; Mitarai, S.; Jav, S.; et al. Genetic Mutations Associated with Isoniazid Resistance in Mycobacterium tuberculosis in Mongolia. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef] [PubMed]
- Jindani, A.; Aber, V.R.; Edwards, E.A.; Mitchison, D.A. The early bactericidal activity of drugs in patients with pulmonary tuberculosis. Am Rev Respir Dis 1980, 121, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Heym, B.; Allen, B.; Young, D.; Cole, S. The catalase—peroxidase gene and isoniazid resistance of Mycobacterium tuberculosis. Nature 1992, 358, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Dubnau, E.; Quemard, A.; Balasubramanian, V.; Um, K.S.; Wilson, T.; Collins, D.; de Lisle, G.; Jacobs, W.R., Jr. inhA, a gene encoding a target for isoniazid and ethionamide in Mycobacterium tuberculosis. Science 1994, 263, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Vilchèze, C.; Jacobs, W.R. Resistance to isoniazid and ethionamide in Mycobacterium tuberculosis: genes, mutations, and causalities. Microbiol Spectr 2014, 2, MGM2. [Google Scholar] [CrossRef] [PubMed]
- Lempens, P.; Meehan, C.J.; Vandelannoote, K.; Fissette, K.; de Rijk, P.; Van Deun, A.; Rigouts, L.; de Jong, B.C. Isoniazid resistance levels of Mycobacterium tuberculosis can largely be predicted by high-confidence resistance-conferring mutations. Sci. Rep. 2018, 8, 3246. [Google Scholar] [CrossRef] [PubMed]
- Vilcheze, C.; Jacobs, W.R., Jr. Resistance to isoniazid and ethionamide in mycobacterium tuberculosis: genes, mutations, and causalities. Microbiology Spectrum. 2014, 2, MGM2-0014-2013. [Google Scholar] [CrossRef] [PubMed]
- Seifert, M.; Catanzaro, D.; Catanzaro, A.; Rodwell, T.C. Genetic Mutations Associated with Isoniazid Resistance in Mycobacterium tuberculosis: A Systematic Review. PLOS ONE 2015, 10, e0119628. [Google Scholar] [CrossRef] [PubMed]
- Böttger, E. C. In Antituberculosis Chemotherapy Vol. 40 (eds P. R. Donald & P. D. van Helden) Ch. 14, 128–144 (Karger, 2011).
- Huyen, M.N.T.; Cobelens, F.G.J.; Buu, T.N.; Lan, N.T.N.; Dung, N.H.; Kremer, K.; Tiemersma, E.W.; van Soolingen, D. Epidemiology of Isoniazid Resistance Mutations and Their Effect on Tuberculosis Treatment Outcomes. Antimicrob. Agents Chemother. 2013, 57, 3620–3627. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, S.V.; Reich, R.; Dou, S.-J.; Jasperse, L.; Pan, X.; Wanger, A.; Quitugua, T.; Graviss, E.A. Single Nucleotide Polymorphisms in Genes Associated with Isoniazid Resistance in Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 2003, 47, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Jagielski, T.; Grzeszczuk, M.; Kamiński, M.; Roeske, K.; Napiórkowska, A.; Stachowiak, R.; Augustynowicz-Kopeć, E.; Zwolska, Z.; Bielecki, J. Identification and Analysis of Mutations in the KatG Gene in Multidrug-Resistant Mycobacterium tuberculosis Clinical Isolates. Adv. Respir. Med. 2013, 81, 298–307. [Google Scholar] [CrossRef]
Figure 1.
Initial CT exam of the thorax with contrast substance reveales the following: heterogeneous consolidation process with a tendency to cavitation, moderate iodophillia and peripheral microcalcifications, associating tubular bronchiectasis occupied by mucoid impacts, designed LIL. Suspicious lesion is marked with blue arrows.
Figure 1.
Initial CT exam of the thorax with contrast substance reveales the following: heterogeneous consolidation process with a tendency to cavitation, moderate iodophillia and peripheral microcalcifications, associating tubular bronchiectasis occupied by mucoid impacts, designed LIL. Suspicious lesion is marked with blue arrows.
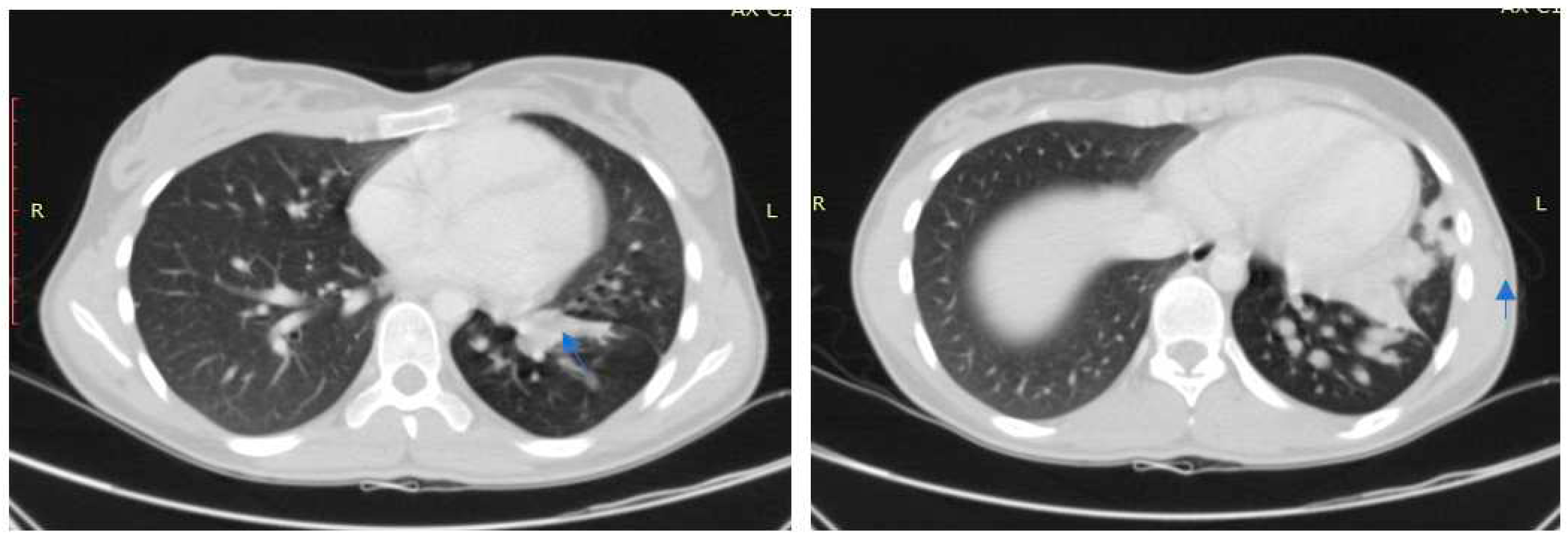
Figure 2.
CT exam of the thorax with contrast substance in contract with the previos CT exam reveales the following: Heterogeneous consolidation process with moderate iodophillia and peripheral microcalcifications, associating tubular bronchiectasis occupied by mucoid impacts, designed LIL. Multiple images of microcalcifications with centropulmonary and subpleural topography with dimensions between 3 and 6 mm bilaterallydispersed. No pleural or pericardial fluid accumulations. Without mediastinal adenopathy or hiatus with a pathological visa. Medium-sized media with opacified homogeneous size. Conclusions: dimensional progression of the retro-stenotic triangular condensation with sacral bronchiectasis and endo-luminal secretion retention.
Figure 2.
CT exam of the thorax with contrast substance in contract with the previos CT exam reveales the following: Heterogeneous consolidation process with moderate iodophillia and peripheral microcalcifications, associating tubular bronchiectasis occupied by mucoid impacts, designed LIL. Multiple images of microcalcifications with centropulmonary and subpleural topography with dimensions between 3 and 6 mm bilaterallydispersed. No pleural or pericardial fluid accumulations. Without mediastinal adenopathy or hiatus with a pathological visa. Medium-sized media with opacified homogeneous size. Conclusions: dimensional progression of the retro-stenotic triangular condensation with sacral bronchiectasis and endo-luminal secretion retention.
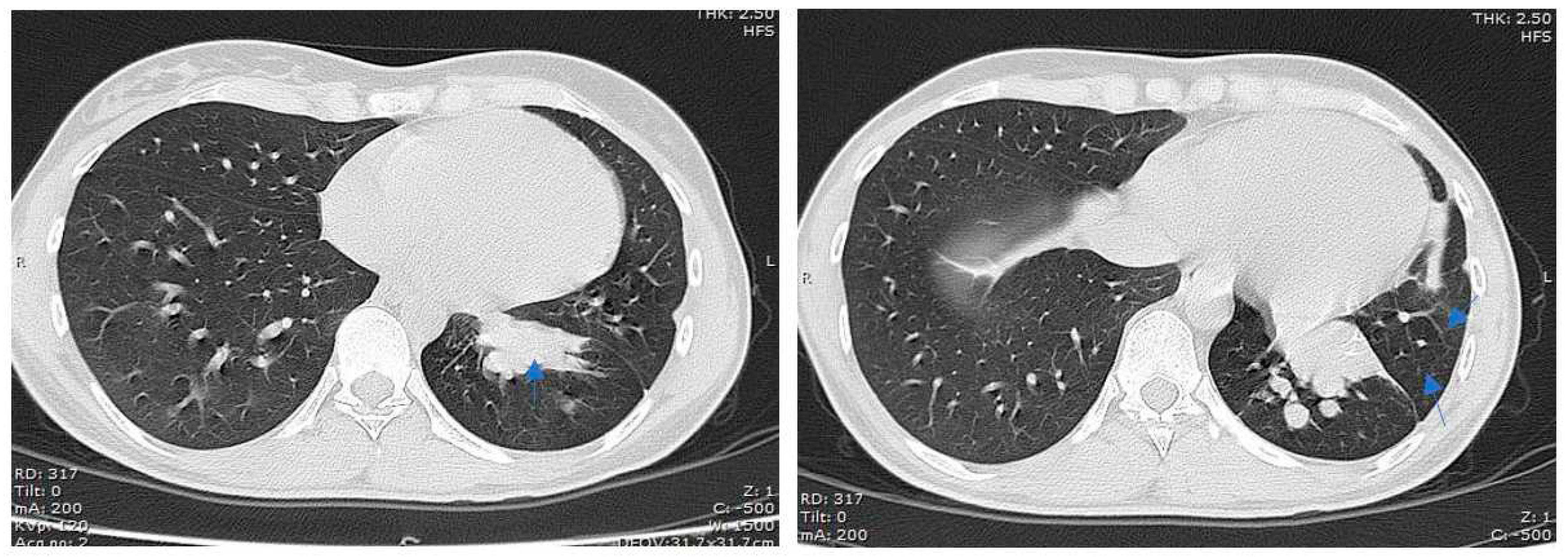
Figure 3.
The angio IRM exam with iv contrast enhancement, the toraco-abdominal aorta, highlights : Angiography of ECM 3D CE, of the dorsal-lumbar aorta, from infrarenal training to angiography TRICKS (12 acquisitions in the coronal plane) does not reveal aberrant tracts of thoracic aorta, right or right atrial renal artery with specificity for pulmonary seizure syndrome tributary to the condensation process in the basal medial segment of the lower left pulmonary lobe. Segmental pulmonary changes will be characterized as cystic bronsiectatic ystic cavities, panopacified by serum mucinous fluid.
Figure 3.
The angio IRM exam with iv contrast enhancement, the toraco-abdominal aorta, highlights : Angiography of ECM 3D CE, of the dorsal-lumbar aorta, from infrarenal training to angiography TRICKS (12 acquisitions in the coronal plane) does not reveal aberrant tracts of thoracic aorta, right or right atrial renal artery with specificity for pulmonary seizure syndrome tributary to the condensation process in the basal medial segment of the lower left pulmonary lobe. Segmental pulmonary changes will be characterized as cystic bronsiectatic ystic cavities, panopacified by serum mucinous fluid.

Figure 4.
Left lower lobe lobectomy. Macroscopy—Lobectomy specimen from the lower lobe. Centrally there is a 4.5 cm long staple line, directly adjacent to it is a polypoid of grey-green gel-like material protruding from the parenchyma. The pleural surface is partly coarse, dark red in color with scarred connective tissue. On the lamellar cut surface, the parenchyma is prominently solidified at all levels, there are multiple, smaller foci with a crumby consistent cut surface, in the area of the dark red colored pleura with the palpably solidified parenchyma the are numerous dilated alveoli, these filled with similar gel-like material surrounding parenchyma homogeneously hemorrhagically imbibed.—Histopathological examination revealed partial lung resection with chronic bronchitis and bronchiolitis as well as bronchiectasis and centrally necrotizing epithelioid cell granulomas encapsulated in connective tissue, some with calcifications, consistent with tuberculous granulomas.
Figure 4.
Left lower lobe lobectomy. Macroscopy—Lobectomy specimen from the lower lobe. Centrally there is a 4.5 cm long staple line, directly adjacent to it is a polypoid of grey-green gel-like material protruding from the parenchyma. The pleural surface is partly coarse, dark red in color with scarred connective tissue. On the lamellar cut surface, the parenchyma is prominently solidified at all levels, there are multiple, smaller foci with a crumby consistent cut surface, in the area of the dark red colored pleura with the palpably solidified parenchyma the are numerous dilated alveoli, these filled with similar gel-like material surrounding parenchyma homogeneously hemorrhagically imbibed.—Histopathological examination revealed partial lung resection with chronic bronchitis and bronchiolitis as well as bronchiectasis and centrally necrotizing epithelioid cell granulomas encapsulated in connective tissue, some with calcifications, consistent with tuberculous granulomas.
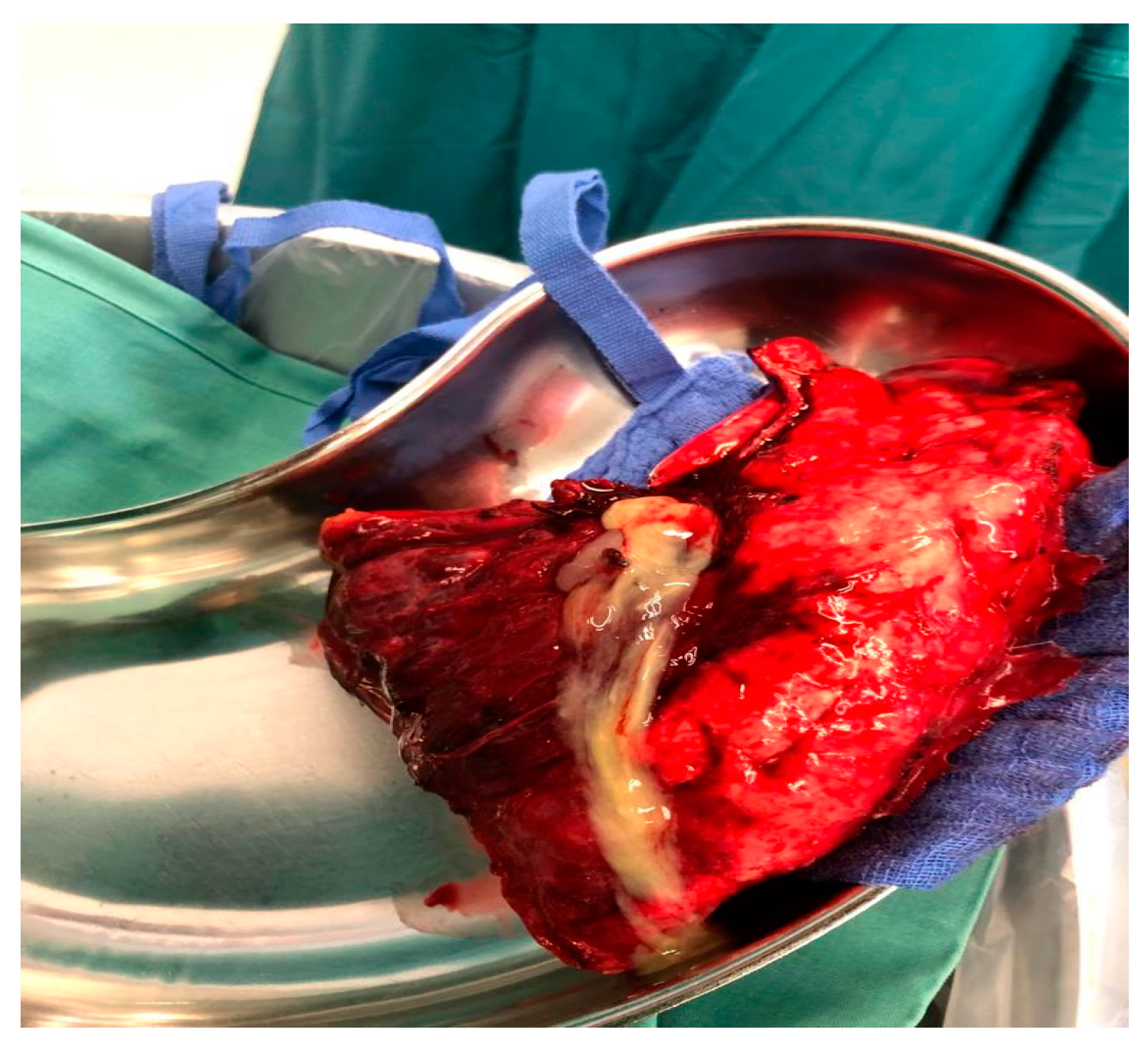
Figure 5.
Molecular pathological examination—Rifampicin (rpoB gene): no mutation was detected. Fluoroquinolones (gyrA gene): no mutation was detected. Isoniazid (kaC gene): the following mutation can be detected: c.947G>A; p.Gly316Asp. Final overall assessment: Mycobacterium tuberculosis has been proven by molecular biology and there is evidence of isoniazid resistance. There is no evidence of rifampicin or fluoroquinolone resistance. The rifampicin (525) and capreomycin (tlyA gene) resistance testing does not produce any usable results. The mutation c.947G>A; p.Gly316Asp in the katC gene has not yet been reported in the medical literature. This method covers the region 507 and 526-531 for rifampicin in the rpoB gene. Further resistance mechanism cannot be ruled out.
Figure 5.
Molecular pathological examination—Rifampicin (rpoB gene): no mutation was detected. Fluoroquinolones (gyrA gene): no mutation was detected. Isoniazid (kaC gene): the following mutation can be detected: c.947G>A; p.Gly316Asp. Final overall assessment: Mycobacterium tuberculosis has been proven by molecular biology and there is evidence of isoniazid resistance. There is no evidence of rifampicin or fluoroquinolone resistance. The rifampicin (525) and capreomycin (tlyA gene) resistance testing does not produce any usable results. The mutation c.947G>A; p.Gly316Asp in the katC gene has not yet been reported in the medical literature. This method covers the region 507 and 526-531 for rifampicin in the rpoB gene. Further resistance mechanism cannot be ruled out.
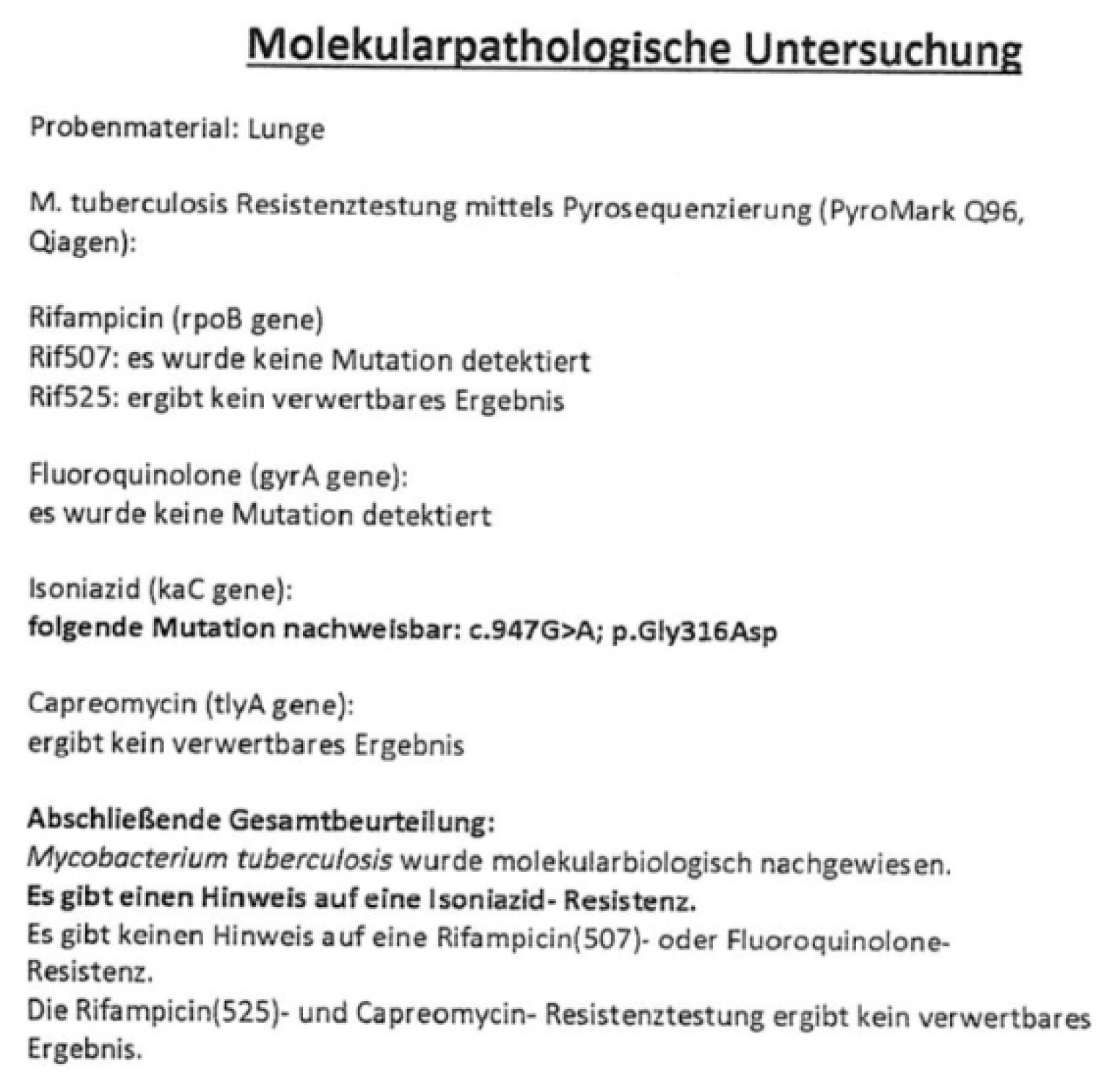
Figure 6.
CT exam of the thorax with contrast substance highlights multiple micronodules and small juxacentimeter pulmonary nodules distributed bilaterally, predominantly in the upper ½ apprently in slight numerical progression. Bilateral pleural effusion with a latero-thoracic constricted appearance, with a thickness of 19mm on the left side, respectively 30mm on the right side, which associates underlying pulmonary compression with a lamellar appearance in the lower lobes and medium lobe. Layered mediastinal adenopathies with slightly inhomogeneous iodophilia and sizes up to 17/12mm lower right paratracheal, in progression. Multiple adenopathies in the abdominal floor included in the examination, most found in the root of the mesentery, with sizes up to 19/15mm. Permeable pulmonary vascular axes. Suspicious lesion is marked with blue arrows.
Figure 6.
CT exam of the thorax with contrast substance highlights multiple micronodules and small juxacentimeter pulmonary nodules distributed bilaterally, predominantly in the upper ½ apprently in slight numerical progression. Bilateral pleural effusion with a latero-thoracic constricted appearance, with a thickness of 19mm on the left side, respectively 30mm on the right side, which associates underlying pulmonary compression with a lamellar appearance in the lower lobes and medium lobe. Layered mediastinal adenopathies with slightly inhomogeneous iodophilia and sizes up to 17/12mm lower right paratracheal, in progression. Multiple adenopathies in the abdominal floor included in the examination, most found in the root of the mesentery, with sizes up to 19/15mm. Permeable pulmonary vascular axes. Suspicious lesion is marked with blue arrows.
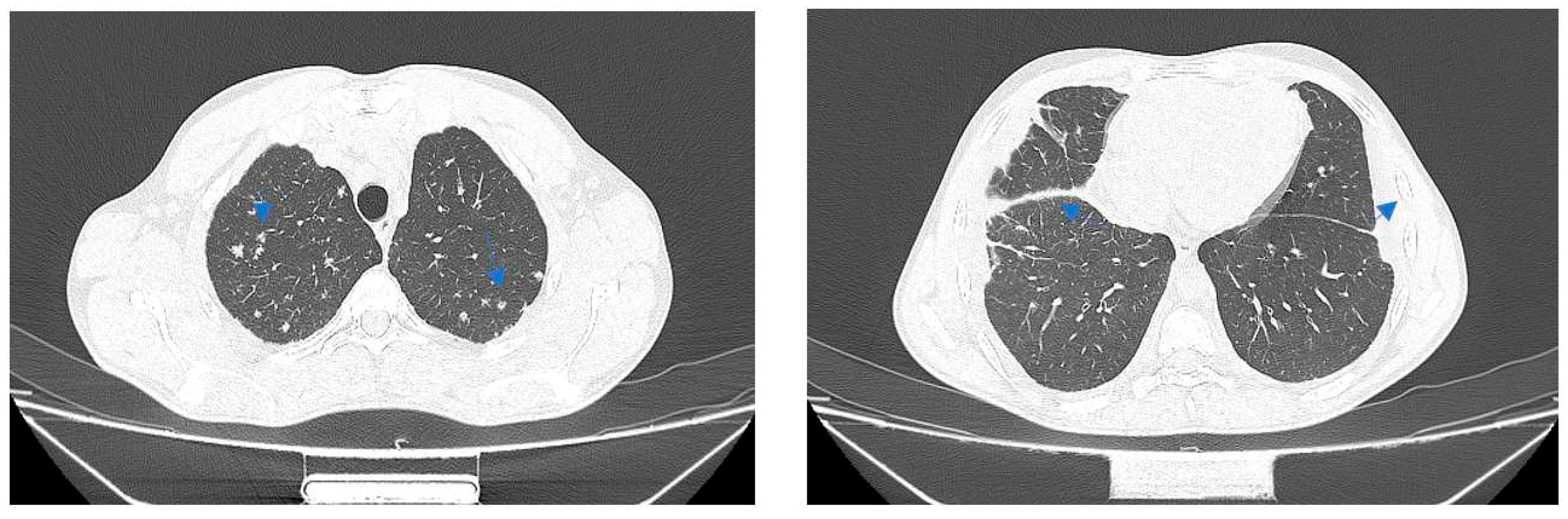
Figure 7.
(a). Conglomerate gigantocellular epithelioid granulomas (green arrow); towards the periphery of the granulomas multinucleated giant Langhans cells are observed. Figure 7(b). Confluent, necrotizing gigantocellular epithelioid granulomas. Arrow indicates caseous necrosis, necrosis is bordered by epithelioid histiocytes and giant Langhans cells.
Figure 7.
(a). Conglomerate gigantocellular epithelioid granulomas (green arrow); towards the periphery of the granulomas multinucleated giant Langhans cells are observed. Figure 7(b). Confluent, necrotizing gigantocellular epithelioid granulomas. Arrow indicates caseous necrosis, necrosis is bordered by epithelioid histiocytes and giant Langhans cells.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



