
Submitted:
27 September 2023
Posted:
28 September 2023
You are already at the latest version
Abstract
(1) Background: Psychological well-being (PWB) and female sexual health are two important areas for women’s quality of life and research, and they are closely related. The aim of this study was to conduct a systematic review of the existing literature to explore the association between PWB and sexual health in women. (2) Methods: This review was carried out following PRISMA. The inclusion criteria were studies with samples of adult women, that evaluated and associated sexual functioning and mental health. Scientific articles were identified on Web of Science, Scopus, EBSCO (PsycInfo, PsycArticles, and Psicodoc), ProQuest, and PubMed. The search was limited to years between 2010 and 2023. (3) Results: 14 selected articles were analyzed, in which population samples and variables related to mental and sexual health were examined. 42.9% of the studies included clinical samples, 71.4% focused on anxiety and depression as main mental health variables, and 50% examined female sexual functioning as a sexual health variable. (4) Conclusions: This review provides more up-to-date information about valuable insights into the possible determinants of female sexual health. The association between PWB and female sexual health has been demonstrated.
Keywords:
sexual health
; psychological well-being
; women
; systematic review
1. Introduction
Psychological well-being (PWB) and female sexual health are two important areas for women’s quality of life and research and is well-known that there is a close relationship between both aspects. PWB is commonly characterized as reaching one's full potential and is linked to meaningful (eudaimonic) wellness attitudes [1], and it embraces different aspects such as autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance [2,3]. Sexual health, as mentioned by the World Health Organization (WHO) [4], refers to "a state of physical, emotional, mental, and social well-being in relation to sexuality" (p. 5). It emphasizes the importance of a positive and respectful approach to ensure pleasurable and safe sexual experiences [4]. When it comes to women, female sexual health encompasses various physical, emotional, and social factors that influence their sexual experiences and overall quality of life. Research consistently shows associations between PWB and sexual health outcomes across diverse cultures [5]. Some examples of these associations have shown that positive PWB and better mental health, including high self-esteem, life satisfaction, and lower levels of depression and anxiety, are associated with improved sexual functioning and satisfaction in women [6-8]. Conversely, negative PWB and mental health issues, such as depression and anxiety, have been found to be associated with sexual dysfunction, decreased sexual desire, and difficulties with sexual arousal and orgasm [5,9-11].
Along the same line, it is important to acknowledge that female sexual dysfunction (FSD) is a complex issue influenced by various factors, including biological, psychological, and interpersonal aspects [12]. Psychological factors play a significant role in FSD, as evidenced by studies linking sexual dysfunction to depression in women with diabetes [13] and the association between sexual dysfunction and psychological distress in women with depression [14]. Furthermore, sexual dysfunction –in general– significantly impacts community health, particularly affecting women. Several international studies have provided compelling evidence regarding the prevalence of sexual dysfunction. For instance, in the United States, 43% of women reported experiencing sexual dysfunction, compared to 31% of men [15]; in Turkey, the prevalence of FSD was found to be 53.2% [16]; in China, it reached 60% [17]; Brazil exhibited a prevalence ranging from 13.3% to 79.3% among women [18]; and, lastly, in Latin America, a study involving 5,391 individuals found that 56.8% of sexually active women aged 40-59 experienced sexual dysfunction [19]. To promote comprehensive sexual well-being for women is crucial for researchers and healthcare professionals to acknowledge and address the intricate relationship between PWB and sexual health outcomes. By understanding the interplay between these factors, healthcare providers can develop more effective strategies to support women in achieving optimal sexual health and overall well-being.
Regarding a different matter, given the fact that systematic reviews are considered “one of the highest forms of research evidence” [20] (p. 199), and “answer an empirical question based on a minimally biased appraisal of all the relevant empirical studies” [21] ( p. 121), conducting a systematic review of PWB and female sexual health could provide a stronger and more reliable understanding by combining findings from multiple studies. Also, this review could identify gaps, inform future research, and promote overall well-being and quality of life for women. Despite the significance of this topic, more research is needed to identify risk factors for sexual dysfunction and better understand the interaction between PWB and female sexual health. Lastly, the examination of recent studies with certain populations, and informing the most used measures that assess women's sexual health and mental health are issues that need to be addressed in research.
In summary, it is known that human sexuality is an important part of peoples’ lives and well-being [22]. The link between psychological well-being and female sexual health is crucial to women's quality of life. As aware as we are, a systematic review of the scientific literature specifically focused on these two topics does not exist. Thus, the aim of this study is to conduct a comprehensive review of the existing literature to explore the association between PWB and sexual health in women.
2. Materials and Methods
Study design
This systematic review was carried out following the PRISMA statement [23]. Due to no human participants being involved, there were no requirements for an ethical review of this work.
Eligibility criteria
The inclusion criteria for the review were as follows:
- Studies with samples of adult women from both clinical and non-clinical contexts.
- Studies that evaluated sexual health and mental health or PWB variables.
- Studies that associated sexual health and mental health or PWB variables.
The exclusion criteria were other type of documents (systematic, narrative, bibliographic reviews, non-relational qualitative studies), studies with samples of women under 18 years of age such as adolescents or girls, and studies that did not include the analysis of sexual health or sexual functioning and mental health variables and their association. Studies in this review were grouped for the syntheses.
Information source
The studies were identified on Web of Science, Scopus, EBSCO (PsycInfo, PsycArticles, and Psicodoc), ProQuest, and PubMed. The date when each source was last searched was between 1 February 2023 and 30 April 2023.
Search strategies
The search strategy was [“Sexual health” AND “Psychological well-being” AND (“women” OR “female”)]. We used the filters and limits for years between 2010 and 2023, language in English or Spanish, and only scientific articles.
Data collection process
To guarantee the objectivity and rigour of the results, two reviewers collected data from each database by working independently. Then, they pooled and confirmed the data. Based on the inclusion criteria, a screening of the titles was conducted. Studies that clearly did not respond to the review objectives and duplicates were excluded. The two reviewers screed the abstracts separately. Finally, the most relevant studies were full-text read. No automation tools were used in the process.
Data items
Data from studies with samples of adult women (clinical and non-clinical) that evaluated sexual functioning and mental health or psychological well-being variables and associated them were considered.
Study risk of bias assessment
To assess the risk of bias in the included studies, we considered the psychometric properties of the measurement instruments used in each study. Two reviewers assessed each study by working independently. After reading the articles that met the inclusion criteria, their methodological quality was assessed using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (QATOCCS) [24]. This tool ensures scientific quality and methodological transparency by evaluating aspects such as the clarity of the research question and the definition of the study population through a checklist of requirements (e.g., "Was the research question or objective in this paper clearly stated?", "Was the study population clearly specified and defined?"). The rigorous evaluation ensured the studies' robustness and the results' reliability. For the current analysis, the two reviewers independently read and rated each of the selected studies across the QATOCCS criteria. Any discrepancies in ratings were discussed until a consensus was reached. This comprehensive quality assessment ensured that only methodologically robust studies with reliable psychometrics and minimal bias were included, strengthening the reliability of results. The QATOCCS provided a standardized and transparent framework for critically evaluating the scientific rigor of all studies under consideration.
Synthesis methods
Table S1 in the supplementary material displays the results of individual studies and syntheses. We tabulated for a better visualization the authors and year of publication, samples, list of mental health variables, list of sexual health variables, measurement instruments, and main results about how the observed variables were associated.
3. Results
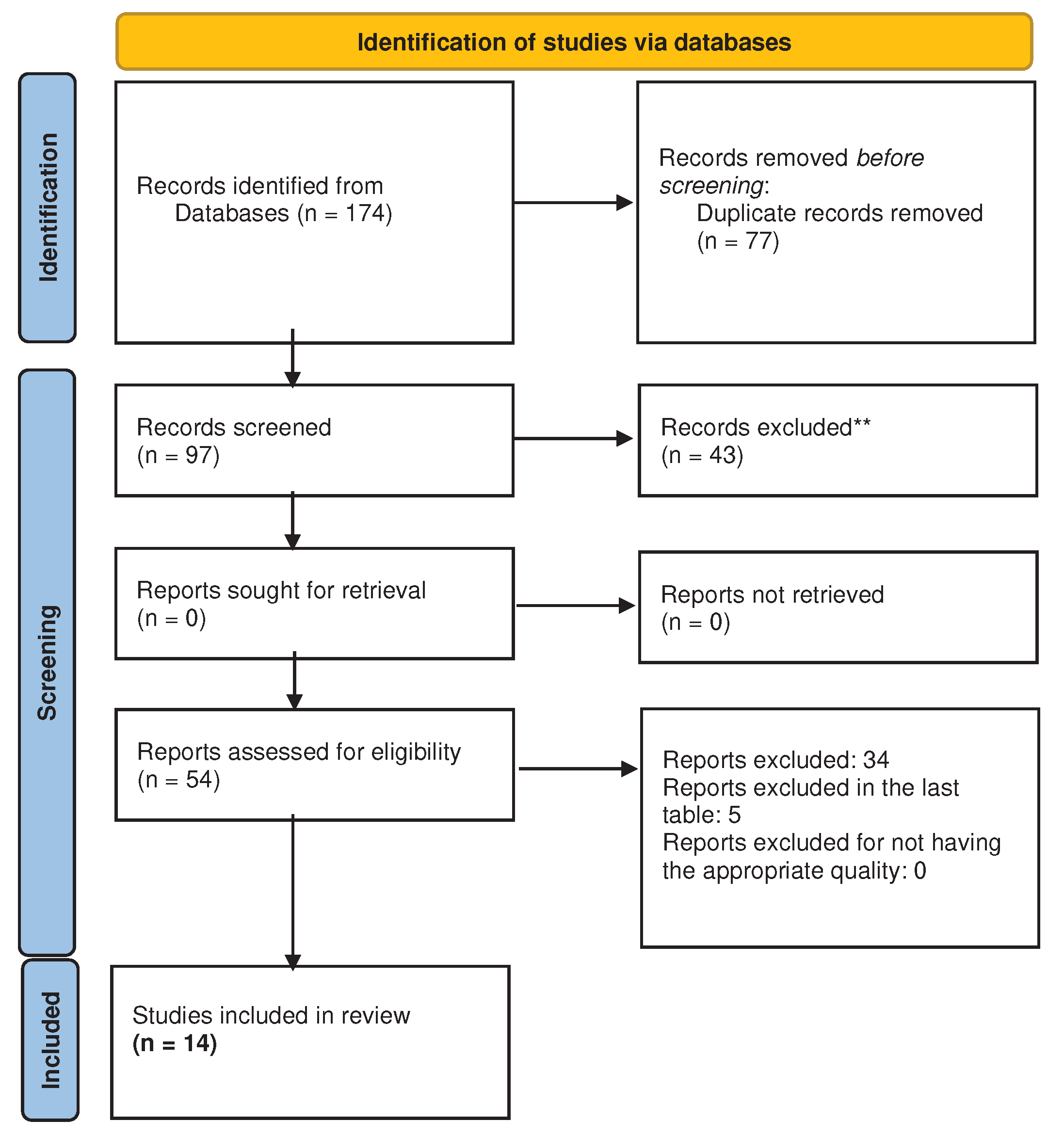
The search yielded a total of 174 articles. After analyzing them to determine their compliance with the inclusion criteria and assessing their quality, a final set of 14 articles remained for further analysis (see Figure 1). Thus, in the present systematic review study, 14 selected articles were analyzed, in which population samples and variables related to mental and sexual health were examined. Regarding the former, it was found that 42.9% of the studies used clinical samples as the study population [25-30], while 35.7% used representative samples of the general population [31-35]. Only three studies (21.4%) used both types of samples, clinical and general population [36-38].
Secondly, regarding variables related to mental health, it was observed that anxiety and depression were the most investigated constructs. 71.4% of the studies examined these constructs individually, in combination, or with other mental health constructs. Only four studies (28.6%) of the reviewed articles investigated other variables than anxiety or depression, such as sense of responsibility [31], attention deficit hyperactivity disorder [37], constructs related to objectification [33], and other aspects of mental health [30]. In relation to sexual health variables, 50% of the studies exclusively evaluated variables linked to sexual functioning, while two articles (14.3%) analyzed aspects other than sexual functioning but related to sexual health [28,33]. 5 articles (35.7%) examined variables associated with sexual functioning along with other variables related to sexual health [26,27,29,37,38].
Concerning the measures used to assess variables related to mental and sexual health, it was found that standardized scales were used in most of the reviewed studies. To measure anxiety exclusively, the Florida Shock Anxiety Scale (FSAS) by Ford et al. [39] and the Generalized Anxiety Disorder Scale (GAD-7) by Löwe et al. [40] were employed. As for depression, the Beck Depression Inventory (BDI) [41], the Beck Depression Inventory-II (BDI-II) [42], and the Beck Depression Inventory Primary Care (BDI-PC) [43] were used. Only three articles (21.4%) employed measures that assessed both anxiety and depression, such as the Hospital Anxiety and Depression Scale (HADS) by Zigmond and Snaith [44], the Brief Symptom Inventory (BSI) by Derogatis [45], and an ad hoc measure that evaluated general aspects of mental health. Considering the measures used to assess variables related to sexual health, the Female Sexual Function Index (FSFI) developed by Rosen et al. [46] was the most used in nine studies (64.3%), being the predominant scale in this review. Of the nine studies, four studies exclusively used the FSFI, while the other five studies used the FSFI along with other scales to assess various constructs related to sexual health. It is worth mentioning that in the study by Vedovo et al. [34], both the FSFI and the Operated Male to Female Sexual Function Index (OMtFSI) [47] were used, with the latter being the first scale designed to assess sexual functioning in trans women. Other scales used to assess sexual functioning or related aspects included the Female Sexual Function Questionnaire-2 (FSM-2; for its acronym in Spanish) designed by Sánchez-Sánchez et al. [48], the Global Measure of Sexual Satisfaction (GMSEX) by Lawrance et al. [49], an ad hoc questionnaire used by Dubin et al. [31] to assess desire and satisfaction, and a Female Orgasmometer, a single-item Likert scale derived from the Visual Analog Scale for Pain [50], which was used in the study by Mollaioli et al. [32]. Other scales that did not directly assess sexual functioning but rather other aspects of sexual health were used such as the Sexual Distress Scale (SDS) created by Santos-Iglesias et al. [51], the Sexual Complaint Screener-Women (SCS-W) developed by the International Society of Sexual Medicine (ISSM) [52], the Sexual Risk Survey (SRS) by Turchik and Garske [53], and the Interpersonal Sexual Objectification Scale (ISOS) by Kozee et al. [54], among others (see Table S1).
Finally, the results of the reviewed articles were categorized according to their focus, whether contextual, medical, or psychological. Seven articles (50%) presented results that combined two of these categories. Of these, five were categorized as contextual-psychological, with risk factors influencing mental and sexual health variables. They explored factors related to the COVID-19 pandemic, social stigmas towards women, and postponed fertility treatments [25,28,32,33,35]. The other two articles were categorized as medical-psychological, focusing on risk factors related to ADHD and hypoactive sexual desire diagnosis, respectively [30,37]. Additionally, other four articles (28.6%) centered only on medical outcomes, addressing factors related to cancer, menopause, and pelvic-genital pain [26,27,29,38]. Two articles (14.3%) presented exclusively psychological outcomes, with anxiety and depression as the risk factors [35, 36]. Finally, only one article (7.1%) addressed contextual outcomes, specifically the partner context, by examining couple´s problems caused by the partner’s erectile dysfunction [31]. This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
4. Discussion
The aim of this study was to carry out a systematic review of the association between PWB and female sexual health. In general, findings show that recent research focuses on women of clinical samples and considers anxiety and depression as the most important health variables, while general sexual functioning is the most relevant sexual variable.
This recent scientific literature, that examined the association between mental and sexual health, has shown great interest in women diagnosed with certain health problems. Therefore, the majority of the studies focused on women with specific medical diagnoses when evaluating the link between psychological and sexual health. These health topics include issues related to congenital heart disease with implantable cardioverter-defibrillators, and breast, anal, or rectal cancer. For example, results have shown that in women with congenital heart disease, depression, and anxiety are negatively associated with worse sexual functioning [36]. Some psychological disorders like Attention-Deficit/Hyperactivity Disorder (ADHD) and opioid use disorder are also considered, for example, women with ADHD reported more hypersexual behaviors [37]. Also, literature considers sexual and reproductive health problems such as Persistent Genital Arousal Disorder/Genito-pelvic Dysesthesia (PGAD/GPD), Hypoactive Sexual Desire Disorder (HSDD), and fertility. In this line, individuals with PGAD/GPD symptoms indicate lower relationship satisfaction and sexual satisfaction and greater sexual distress in comparison to a control group [38]. All this information could reveal a greater interest in medical aspects rather than psychological or sexual ones when assessing clinical samples.
Anxiety and depression are the most investigated variables in mental health when the objective is also examining sexual health in women in the reviewed studies. Philip et al. [29] have found that anxiety is negatively associated with desire, arousal, orgasm, and satisfaction while depression is negatively associated with arousal and sexual satisfaction in post-treatment anal or rectal cancer survivors. Mooney et al. [38] have demonstrated that women with PGAD/GPD report more symptoms of depression and anxiety. Building upon this finding, Mollaioli et al. [32] further established the beneficial impact of sexual activity in safeguarding against psychological distress, promoting relational well-being, and enhancing sexual health.
Moreover, research examining female sexual health has primarily focused on sexual functioning, often overlooking other critical aspects like sexual behaviors, attitudes, gender roles, and prevention of sexual and reproductive infections or diseases, unwanted pregnancies, or sexual violence. As a result of this focus, and in terms of assessment, the most used measurement instrument for evaluating sexual functioning in women is the FSFI [46]. In this line, quality assessment of women's sexuality requires standardized validated scales encompassing multidimensional constructs. Beyond the Female Sexual Function Index, other validated questionnaires can provide an assessment of sexual functioning across genders. Two examples of valid measurement instruments are the Massachusetts General Hospital Sexual Functioning Questionnaire (MGH-SFQ) [55] and the Arizona Sexual Experiences Scale (ASEX) [56]. These multifaceted instruments quantify the diverse elements of sexual functioning in both women and men. Broader implementation of the MGH-SFQ, ASEX, and other multidimensional tools is crucial for advancing scientific understanding of both female and male sexual well-being. Findings will inform the development of optimized, gender-inclusive models of care and interventions tailored to the complete spectrum of sexual issues and concerns and inform the provision of comprehensive patient-centered care.
Regarding the focus on contextual, medical, or psychological areas, most of the studies explore the relationship of mental and sexual health with a medical pathological origin, as mentioned above. In addition, it is important to highlight that, in some cases, the COVID-19 pandemic was an important factor when relating to the contextual area. Therefore, the effect of the COVID-19 pandemic has been provided in the studies. In the work by Mistler et al. [28], most women reported no change in sexual health behaviors, and very few reported an increase in sex-related behaviors due to COVID-19. During lockdown, sexually active subjects indicate lower levels of anxiety and depression [32]. Furthermore, other contextual aspects have been considered, for example, Polihronakis et al. [33] showed that marginalization has a direct relationship with internalization and sexual risk behaviors. To understand how discrimination against sexual minorities affects sexual health, more studies need to be conducted to better manage the mental disorders of the LGBTQ+ community [57]. Lastly, psychosocial factors influence HSDD, they interfere in the relationship with the partner, and mental and emotional well-being [30]. More articles show that the problems that affect sexual health are medical in comparison to psychological issues. It has been highlighted the important role that medical aspects have on sexual health, compared to psychological and social aspects. A possible reason could be that the psychological and social aspects are still less relevant than the medical aspects.
Some limitations have been identified in this review. The exclusion criteria of other type of documents (e.g., narrative, qualitative studies) and studies published in other languages limits the scope of information explored in this article. Other systematic reviews were not included in the analysis. Also, setting the age of the samples to 18 years of age could lose relevant aspects on the youngest women. Furthermore, only fully published studies have been included which possibility of publication bias. Nevertheless, this systematic review offers a comprehensive overview of the association in women between PWB and sexual health.
5. Conclusions
In conclusion, through a meticulous analysis of the available research, this review provides information about valuable insights into the possible determinants of female sexual health. The association between PWB and female sexual health has been demonstrated. The studies reviewed found that female clinical samples, anxiety and depression, and general sexual functioning are the most relevant observed outcomes. In this line, the extensive prevalence and life impact of female sexual dysfunctions indicate these are critical public health issues warranting population-level interventions. Sexual health challenges affect a substantial portion of the female population and reduce the quality of life [58]. The results of this systematic review call for implementing public health strategies beyond individual clinical approaches to comprehensively support women’s sexual well-being across the lifespan. In addition, the findings of this study will have significant implications for healthcare professionals. By recognizing the importance of mental and sexual health issues, healthcare professionals will be able to be aware and attend to those issues and play a crucial role in improving women's sexual experiences, satisfaction, and overall quality of life. Also, there will be a pressing need to elevate female sexual and mental wellness as a public health priority and develop policies, programs, and messaging to positively transform women’s experiences at a societal level. For example, the studies by Rezaei et al. [59] and Mahnza et al. [60] demonstrate the benefits of sexual health education programs for women. Rezaei et al. [59] implemented a program in Iran consisting of group sessions and individual consultations. They found positive impacts on female sexual function, notably desire and arousal, as well as improved sexual attitudes. These results align with Mahnza et al.'s findings [60] that sexual health education enhances women's sexual function in general. Beyond improving sexual health, these programs may also prevent issues like unintended pregnancy, sexually transmitted infections, sexual abuse, and violence against women. Sexual health education equips women with the knowledge to make informed choices and build healthy relationships. Therefore, by taking a holistic perspective encompassing mental, emotional, and social well-being, researchers and healthcare providers can gain a deeper understanding of the multidimensional factors influencing women's sexual health and develop impactful interventions to improve the lives of women across diverse communities.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Revised articles about sexual health and psychological well-being.
Author Contributions
“Conceptualization, A.I.A.R. and C.C; methodology, A.I.A.R. and C.C; investigation, A.I.A.R. and C.C; resources, A.I.A.R. and C.C; writing—original draft preparation, A.I.A.R. and C.C; writing—review and editing, A.I.A.R. and C.C; supervision, A.I.A.R. and C.C.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ryff, CD. Eudaimonic well-being: Highlights from 25 years of inquiry. In K. Shigemasu K, Kuwano S, Sato T, Matsuzawa T, Eds.; Diversity in harmony-insights from psychology: Proceedings of the 31st International Congress of Psychology.; Diversity in harmony-insights from psychology: Proceedings of the 31st International Congress of Psychology. John Wiley & Sons, Ltd. 2018; pp. 2018375–395. [Google Scholar]
- Ryff, CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of personality and social psychology. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Ryff, CD. Psychological well-being revisited: Advances in the science and practice of eudaimonia. Psychother Psychosom. 2014, 83, 10–28. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (2006). Defining sexual health: Report of a technical consultation on sexual health, , Geneva. Retrieved from https://www3.paho.org/hq/index.php?option=com_content&view=article&id=2136:2009-defining-sexual-health&Itemid=0&lang=es#gsc.tab=0. 28–31 January.
- Laurent SM, Simons AD. Sexual dysfunction in depression and anxiety: Conceptualizing sexual dysfunction as part of an internalizing dimension. Clin Psychol Rev. 2009, 29, 573–585. [Google Scholar] [CrossRef]
- Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007, 357, 762–774. [Google Scholar] [CrossRef]
- Rehbein-Narvaez R, García-Vázquez E, Madson L. The relation between self-esteem and sexual functioning in collegiate women. J Soc Psychol. 2006, 146, 250–252. [Google Scholar] [CrossRef]
- Woloski-Wruble AC, Oliel Y, Leefsma M, Hochner-Celnikier D. Sexual activities, sexual and life satisfaction, and successful aging in women. J Sex Med. 2010, 7, 2401–2410. [Google Scholar] [CrossRef]
- Davison SL, Bell RJ, LaChina M, Holden SL, Davis SR. The relationship between self-reported sexual satisfaction and general well-being in women. J Sex Med. 2009, 6, 2690–2697. [Google Scholar] [CrossRef]
- McCool-Myers M, Theurich M, Zuelke A, Knuettel H, Apfelbacher C. Predictors of female sexual dysfunction: a systematic review and qualitative analysis through gender inequality paradigms. BMC Womens Health. 2018, 18. [Google Scholar] [CrossRef]
- West SL, Vinikoor LC, Zolnoun D. A systematic review of the literature on female sexual dysfunction prevalence and predictors. Annual review of sex research. 2004, 15, 40–172. [Google Scholar]
- Basson R, Berman J, Burnett A, Derogatis L, Ferguson D, Fourcroy J, et al. Report of the international consensus development conference on female sexual dysfunction: Definitions and classifications. J Sex Marital Ther. 2001, 27, 83–94. [Google Scholar] [CrossRef]
- Enzlin P, Mathieu C, Van den Bruel A, Vanderschueren D, Demyttenaere K. Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes Care. 2003, 26, 409–414. [Google Scholar] [CrossRef]
- Devkota L, Pant SB, Ojha SP, Chapagai M. Prevalence of sexual dysfunction in women with depressive disorder at a tertiary hospital. J Psychosexual Health. 2022, 4, 123–128. [Google Scholar] [CrossRef]
- Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: Prevalence and predictors. JAMA. 1999, 281, 537. [Google Scholar] [CrossRef] [PubMed]
- Kılıç, M. Prevalence and risk factors of sexual dysfunction in healthy women in Turkey. Afr Health Sci. 2019, 19, 2623–2633. [Google Scholar] [CrossRef] [PubMed]
- Du J, Ruan X, Gu M, Bitzer J, Mueck AO. Prevalence of and risk factors for sexual dysfunction in young Chinese women according to the Female Sexual Function Index: an internet-based survey. Eur J Contracept Reprod Health Care. 2016, 21, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Wolpe RE, Zomkowski K, Silva FP, Queiroz APA, Sperandio FF. Prevalence of female sexual dysfunction in Brazil: A systematic review. Eur J Obstet Gynecol Reprod Biol. 2017, 211, 26–32. [Google Scholar] [CrossRef]
- Blümel JE, Chedraui P, Baron G, Belzares E, Bencosme A, Calle A, et al. Sexual dysfunction in middle-aged women: A multicenter Latin American study using the Female Sexual Function Index. Menopause. 2009, 16, 1139–1148. [Google Scholar] [CrossRef]
- MacKenzie H, Dewey A, Drahota A, Kilburn S, Kalra P, Fogg C, Zachariah D. Systematic reviews: what they are, why they are important, and how to get involved. J Clin Prev Cardiol. 2012, 1, 193–202. [Google Scholar]
- Strech D, Sofaer N. How to write a systematic review of reasons. J Med Ethics. 2012, 38, 121–126. [Google Scholar] [CrossRef]
- Macedo A, Capela E, Peixoto M. Sexual satisfaction among lesbian and heterosexual cisgender women: A systematic review and meta-analysis. Healthcare (Basel). 2023, 11, 1680. [Google Scholar] [CrossRef]
- Matthew, J. Page, Joanne E. McKenzie, Patrick M. Bossuyt, Isabelle Boutron, Tammy C. Hoffmann, Cynthia D. Mulrow, Larissa Shamseer, Jennifer M. Tetzlaff, Elie A. Akl, Sue E. Brennan, Roger Chou, Julie Glanville, Jeremy M. Grimshaw, Asbjørn Hróbjartsson, Manoj M. Lalu, Tianjing Li, Elizabeth W. Loder, Evan Mayo-Wilson, Steve McDonald, Luke A. McGuinness, Lesley A. Stewart, James Thomas, Andrea C. Tricco, Vivian A. Welch, Penny Whiting, David Moher, Juan José Yepes-Nuñez, Gerard Urrútia, Marta Romero-García, Sergio Alonso-Fernández. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev Esp Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute (NHLBI). Study Quality Assessment Tools. 2013. Retrieved from https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
- *Dong M, Wu S, Tao Y, Zhou F, Tan J. The impact of postponed fertility treatment on the sexual health of infertile patients owing to the COVID-19 pandemic. Front Med. 2021, 8, 730994. [Google Scholar] [CrossRef] [PubMed]
- *Fogh M, Højgaard A, Rotbøl CB, Jensen AB. The majority of Danish breast cancer survivors on adjuvant endocrine therapy have clinically relevant sexual dysfunction: A cross-sectional study. Acta Oncol. 2021, 60, 61–68. [Google Scholar] [CrossRef] [PubMed]
- *Liñan-Bermudez A, Chafloque-Chavesta J, Pastuso PL, Pinedo KH, Barja-Ore J. Severity of climacteric symptomatology related to depression and sexual function in women from a private clinic. Prz Menopauzalny. 2022, 21, 165–169. [Google Scholar] [CrossRef]
- *Mistler CB, Sullivan MC, Copenhaver MM, Meyer JP, Roth AM, Shenoi SV, Edelman EJ, Wickersham JA, Shrestha R. Differential impacts of COVID-19 across racial-ethnic identities in persons with opioid use disorder. J Subst Abuse Treat. 2021, 129, 108387. [Google Scholar] [CrossRef]
- *Philip EJ, Nelson C, Temple L, Carter J, Schover L, Jennings S, Jandorf L, Starr T, Baser R, DuHamel K. Psychological correlates of sexual dysfunction in female rectal and anal cancer survivors: Analysis of baseline intervention data. J Sex Med. 2013, 10, 2539–2548. [Google Scholar] [CrossRef]
- *Simon JA, Athavale A, Ravindranath R, Hadker N, Sadiq A, Lim-Watson M, Williams L, Krop J. Assessing the burden of illness associated with acquired generalized hypoactive sexual desire disorder. J Womens Health. 2022, 31, 715–725. [Google Scholar] [CrossRef]
- *Dubin JM, Wyant WA, Balaji NC, Efimenko IV, Rainer QC, Mora B, Paz L, Winter AG, Ramasamy R. Is female wellness affected when men blame them for erectile dysfunction? Sex Med. 2021, 9, 100352. [CrossRef]
- *Mollaioli D, Sansone A, Ciocca G, Limoncin E, Colonnello E, Di Lorenzo G, Jannini EA. Benefits of sexual activity on psychological, relational, and sexual health during the COVID-19 breakout. J Sex Med. 2021, 18, 35–49. [Google Scholar] [CrossRef]
- *Polihronakis CJ, Velez BL, Watson LB. Bisexual women's sexual health: A test of objectification theory. Psychol Sex Orientat Gend Divers. 2023, 10, 21–33. [Google Scholar] [CrossRef]
- *Vedovo F, Di Blas L, Aretusi F, Falcone M, Perin C, Pavan N, Rizzo M, Morelli G, Cocci A, Polito C, Gentile G, Colombo F, Timpano M, Verze P, Imbimbo C, Bettocchi C, Pascolo Fabrici E, Palmieri A, Trombetta C. Physical, mental and sexual health among transgender women: A comparative study among operated transgender and cisgender women in a national tertiary referral network. J Sex Med. 2021, 18, 982–989. [Google Scholar] [CrossRef] [PubMed]
- *Vedovo F, Capogrosso P, Di Blas L, Cai T, Arcaniolo D, Privitera S, Palumbo F, Palmieri A, Trombetta C. Longitudinal impact of social restrictions on sexual health in the Italian population. J Sex Med. 2022, 19, 923–932. [Google Scholar] [CrossRef] [PubMed]
- *Cook SC, Valente AM, Maul TM, Dew MA, Hickey J, Jennifer Burger P, Harmon A, Clair M, Webster G, Cecchin F, Khairy P, Alliance for Adult Research in Congenital Cardiology. Shock-related anxiety and sexual function in adults with congenital heart disease and implantable cardioverter-defibrillators. Heart Rhythm. 2013, 10, 805–810. [Google Scholar] [CrossRef] [PubMed]
- *Hertz PG, Turner D, Barra S, Biedermann L, Retz-Junginger P, Schöttle D, Retz W. Sexuality in adults with ADHD: Results of an online survey. Front Psychiatry. 2022, 13, 868278. [Google Scholar] [CrossRef]
- *Mooney KM, Poirier É, Pukall CF. Persistent genital arousal in relationships: A comparison of relationship, sexual, and psychological well-being. J Sex Med. 2022, 19, 234–248. [Google Scholar] [CrossRef]
- Ford J, Finch JF, Woodrow LK, Cutitta KE, Shea J, Fischer A, Hazelton G, Sears SF. The Florida Shock Anxiety Scale (FSAS) for patients with implantable cardioverter defibrillators: Testing factor structure, reliability, and validity of a previously established measure. Pacing Clin Electrophysiol. 2012, 35, 1146–1153. [Google Scholar] [CrossRef]
- Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, Herzberg PY. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Beck AT, Steer RA, Brown GK. Manual for Beck Depression Inventory-II. Psychological Corporation Ed.; USA, 1996.
- Beck AT, Guth D, Steer RA, Ball R. Screening for major depression disorders in medical inpatients with the Beck Depression Inventory for Primary Care. Behav Res Ther. 1997, 35, 785–791. [Google Scholar] [CrossRef]
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Derogatis, LR. Brief Symptom Inventory; Clinical Psychometric Research; USA, 1975.
- Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, Ferguson D, D'Agostino R Jr. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef]
- Vedovo F, Di Blas L, Perin C, Pavan N, Zatta M, Bucci S, Morelli G, Cocci A, Delle Rose A, Caroassai Grisanti S, Gentile G, Colombo F, Rolle L, Timpano M, Verze P, Spirito L, Schiralli F, Bettocchi C, Garaffa G, Palmieri A, Mirone V, Trombetta C. Operated Male-to-Female Sexual Function Index: Validity of the first questionnaire developed to assess sexual function after male-to-female gender affirming surgery. J Urol. 2020, 204, 115–120. [Google Scholar] [CrossRef]
- Sánchez-Sánchez F, Ferrer-Casanova C, Ponce-Buj B, Sipán-Sarrión Y, Jurado-López AR, San Martin-Blanco C, Tijeras-Úbeda MJ, Ferrández Infante A. Diseño y validación de la segunda edición del Cuestionario de Función Sexual de la Mujer, FSM-2. Med Fam Semergen. 2020, 46, 324–330. [CrossRef]
- Lawrance K, Byers ES, Cohen JN. Interpersonal Exchange Model of Sexual Satisfaction Questionnaire. In Handbook of sexuality-related measures, 3rd ed.; Fisher TD, Davis CM, Yarber WL, Davis SL, Eds.; Routledge; USA, 2011, pp. 525–30.
- Joyce CR, Zutshi DW, Hrubes V, Mason RM. Comparison of fixed interval and visual analogue scales for rating chronic pain. Eur J Clin Pharmacol. 1975, 8, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Santos-Iglesias, P. , Mohamed, B., Danko, A., Walker LM. Psychometric validation of the female sexual distress scale in male samples. Arch Sex Behav. 2018, 47, 1733–1743. [Google Scholar] [CrossRef] [PubMed]
- Giraldi A, Rellini A, Pfaus JG, Bitzer, J, Laan, E, Jannini EA, Fugl-Meyer, AR. Questionnaires for Assessment of female sexual dysfunction: A review and proposal for a standardized screener. J Sex Med. 2011, 8, 2681–2706. [Google Scholar] [CrossRef]
- Turchik JA, Garske JP. Measurement of sexual risk taking among college students. Arch Sex Behav. 2009, 38, 936–948. [Google Scholar] [CrossRef]
- Kozee HB, Tylka TL, Augustus-Horvath CL, Denchik A. Development and psychometric evaluation of the Interpersonal Sexual Objectification Scale. Psychol Women Q. 2007, 31, 176–189. [Google Scholar] [CrossRef]
- Sierra JC, Vallejo-Medina P, Santos-Iglesias P, Lameiras Fernández M. Validación del Massachusetts General Hospital-Sexual Functioning Questionnaire (MGH-SFQ) en población española. Aten Primaria. 2012, 44, 516–524. [Google Scholar] [CrossRef]
- Sánchez Fuentes MD, Moyano N, Granados R, Sierra Freire JC. Validation of the Spanish version of the Arizona Sexual Experience Scale (ASEX) using self-reported and psychophysiological measures.
- Juhari JA, Gill JS, Francis B. Coping strategies and mental disorders among the LGBT+ community in Malaysia. Healthcare (Basel). 2022, 10, 1885. [Google Scholar] [CrossRef]
- Bartlik BD, Kolzet JA, Ahmad N, Parveen T, Alvi S. Female Sexual Health. In Principles of Gender-Specific Medicine, 2nd ed.; Legato, M. J., Ed.; USA, 2010, pp. 400–407.
- Rezaei N, Taheri S, Tavalaee Z, Rezaie S, Azadi A. The effect of sexual health education program on sexual function and attitude in women at reproductive age in Iran. J Educ Health Promot. 2021, 10, 140. [Google Scholar] [CrossRef]
- Mahnaz, E. , Nasim, B., Sonia, O. Effect of a structured educational package on women's sexual function during pregnancy. Int J Gynecol Obstet. 2020, 148, 225–230. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram for the systematic review of searches of databases.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



