
Submitted:
28 September 2023
Posted:
28 September 2023
You are already at the latest version
Abstract
We tested the bioactivity of a dalbavancin + heparin (DH) vs. dalbavancin (D) against biofilms of Staphylococcus aureus ATCC43300 (MRSA) and Staphylococcus epidermidis ATCC35984 (MRSE) comparing DH median value of cfu counts and metabolic activity with that obtained for D before and during storage under freezing up to 6 months. The addition of heparin to a dalbavancin lock solution did not affect its bioactivity against staphylococcal biofilms irrespective of its preservation time under freezing.
Keywords:
dalbavancin
; biofilms
; lock therapy
; heparin
; bioactivity
; freezing.
1. Introduction
Antibiotic lock solutions are indicated in addition to systemic therapy for catheter retention when catheter withdrawal cannot be achieved [1]. However, as current guidelines for the management of catheter-related bloodstream infections (C-RBSI) are somewhat outdated, they do not provide for the use of new lipoglycopeptides, such as dalbavancin [2]. We previously assessed the efficacy of a dalbavancin-heparin catheter lock solution against biofilms of Staphylococcus spp., demonstrating that its bioactivity was at least equal to that of vancomycin and that a 6-month freezing did not negatively affect it [3,4]. Moreover, we observed no reduction in the efficacy of heparin in combination with dalbavancin before and during a 6-month freezing period [4].
However, we further needed to assessed whether heparin could affect dalbavancin bioactivity during this freezing process of a stored catheter-lock solution.
2. Results
Overall, considering the clinical criteria, no significant reduction in any of the variables tested was observed at the end of the experiment (month 6) between D and DH solutions against Staphylococci biofilms (Table 1, Figure 1). DH median values were only below 25% lower limit of D values at basal experiments (month 0) for percentage reduction in log cfu counts (15.5% < 20.6%) and metabolic activity (47.4% < 67.1%), and at month 3 for percentage reduction in log cfu counts (9.2% < 17.6%) in MRSA. In MRSE, clinical significance was only observed at basal experiments (month 0) for percentage reduction in log cfu counts (20.1% < 25.7%).
Considering the statistical criteria, no differences were statistically significant in any of the experiments, except in the median percentage reduction of metabolic activity at month 3 in MRSE between DH and D (97.6 vs. 100, p=0.037) (Table 1).
3. Discussion
We demonstrated that heparin (60 UI) does not reduce dalbavancin bioactivity against biofilms of MRSA and MRSE ATCC strains even during a 6-month freezing storage time.
C-RBSI can be achieved by combining systemic and catheter lock therapies in some circumstances in which catheter must be retained [6,7,8,9,10,11]. The current international Guidelines for the Management of Catheter-related infections recommend only vancomycin or cefazolin for the treatment of Gram-positive C-RBSI episodes (BII) [1]. The Clinical Guidelines of the Spanish Society of Clinical Microbiology and Infectious Diseases (SEIMC) and the Spanish Society of Intensive Care Medicine and Coronary Units additionally included teicoplanin and daptomycin (BII) [12]. However, little is known about dalbavancin to be used for catheter savage attempts [13].
Our group previously demonstrated that the efficacy of a heparin-based dalbavancin catheter lock solution against MRSA and MRSE strains was non inferior to vancomycin and that both heparin and dalbavancin remained effective and stable for 7 days in an antimicrobial lock solution at 37ºC, simulating a catheter dwell time of 7 days [3,14,15,16]. Moreover, as it was required to optimize the dalbavancin intravenous vial with a cost-effective approach, we recently demonstrated that a heparin-based dalbavancin catheter lock solution can be stored at –70ºC without seriously affecting its bioactivity against MRSA and MRSE biofilms [4]. However, it was needed to assess whether, in addition, heparin may affect dalbavancin bioactivity when they are combined in a catheter lock solution both before and after the freezing storage period.
Based on our results, we consider that no relevant differences occurred between D and DH solutions against both MRSA and MRSE biofilms regarding percentage reduction of neither log cfu counts nor metabolic activity. In the occasional cases where both statistical and clinical differences were observed between D and DH solutions, they never occurred at the end time of the study (month 6), which is when they would be considered relevant. So, we found no evidence that DH solution bioactivity was reduced over the shelf life with respect to D solution.
The main limitation of the study is that we only tested our experiments on a single ATCC strain of each specie. In addition, bioactivity of D and DH was indirectly calculated by assessing percentage reduction of log cfu counts and metabolic activity of 24-hour formed biofilms.
4. Materials and Methods
We applied an in vitro model to evaluate bioactivity of a heparin (60 IU)–based dalbavancin (1 mg/ml) lock solution vs. a dalbavancin (1 mg/ml) lock solution against biofilm of Staphylococcus aureus ATCC43300 (MRSA) and Staphylococcus epidermidis ATCC35984 (MRSE) before and during a 6-month freezing.
The study was performed in the laboratory of a tertiary teaching hospital in Madrid, Spain. We used an in vitro static microplate model as previously described [5].
We used Xydalba® powder for concentrate solution for infusion 500 mg (Almac Pharma Services Ltd, Seagoe Industrial Estate, Craigavon County Armagh BT63 5UA Reino Unido. Allergan Pharmaceuticals International Ltd., Clonshaugh Business & Technology Park, Dublin 17, D17 E400, Irlanda. Almac Pharma Services, Irlanda. Limited Finnabair Industrial Estate, Dundalk, Co. Louth, A91 P9KD, Irlanda). Xydalba® was reconstituted by slowly adding 25 ml of sterile water for injection and then diluted with 50 mg/ml (5%) glucose solution. An aseptic technique was used for the reconstitution and dilution of Xydalba®. From the reconstituted vial of Xydalba® (20 mg/ml), we prepared a DH solution by transferring 1 ml to 18.6 ml of glucose saline 5% + 0.4 ml heparin sodium (60 IU), Heparin sodium, 5000 IU/5 ml; Hospira Prod. Farm. y Hosp, S.L., Spain; and a D solution by transferring 1 ml to 19 ml of glucose saline 5%. We prepared 3-ml aliquots of each solution and stored them at –70ºC for 6 months.
Frozen lock solutions of D and DH were thawed at room temperature (30 min) before performing the experiments. Biofilms were tested against lock solutions at baseline before freezing (month 0), and during months 3 and 6 of freezing. Data were expressed as median (IQR) percentage reduction of log cfu/ml counts and metabolic activity.
For quantification of bacterial load, wells were vigorously scraped in 100 μl of PBS, and the triplicates of each treatment and controls were mixed separately in a pool. Four 1:100 serial dilutions were performed, and 100 μl of each dilution was plated on blood agar plates and incubated at 37°C for 24 hours. Colonies of the plates were counted, and the percentage reduction in cfu/well was calculated. Colony counts were expressed as the median (IQR) number of cfu/ml and on a logarithmic scale.
For quantification of metabolic activity, 100 μl of XTT/menadione (0.5 mg/ml/1.72 mg/ml) was mixed in a proportion of 10 ml/1 μl and inoculated in each well protected from light. The plate was then incubated at 37°C for 3 hours. Absorbance was measured at 492 nm in a spectrophotometer (Biochrom EZ Read 400), and the percentage reduction in metabolic activity was calculated.
Quantitative variables are expressed as the median and interquartile range (IQR).
For the comparison between DH and D solution results, we defined clinical significance when DH values were within 25% of D values. We arbitrarily choose that 25% cut-off considering it a reasonable value below which there would be no too clinical impact.
We also assessed the statistical significance by comparing median (IQR) percentage reduction values in log cfu/ml counts and metabolic activity of DH solution with those values obtained with D solution at each study periods (months 0, 3, and 6) using the Kruskal-Wallis test.
Statistical significance was set at p<0.05 for all the tests. The statistical analysis was performed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp, Armonk, New York, USA).
5. Conclusions
Heparin does not negatively affect dalbavancin bioactivity against staphylococcal biofilms when they are combined in a catheter lock solution frozen up to 6 months. Our supports should be validated in a large sample size and in other species, such as Enterococci.
Author Contributions
Conceptualization, M.G.; methodology, M.DN, R.H:, and I.M.; software, MJ.PG. and M.DN.; validation, E.C., P.M., C.R. and M.G.; formal analysis, M.DN. and MJ.PG.; investigation, R.H. and I.M.; resources, M.G.; data curation, M.DN. and C.R.; writing—original draft preparation, M.DN.; writing—review and editing, M.G.; visualization, M.G.; supervision, P.M.; project administration, M.G.; funding acquisition, M.G. All authors have read and agreed to the published version of the manuscript.
Funding
M. Guembe is supported by the Miguel Servet Program (ISCIII-MICINN, MS18/00008) of the Health Research Fund (FIS) of the Carlos III Health Institute (ISCIII), Madrid, Spain. M. Díaz-Navarro is supported by the Carlos III Health Institute (ISCIII), Madrid, Spain (FI22/00022). The study was partially financed by grants from the ISCIII (PI21/00344), the Fundación Mutua Madrileña (FMM21/01) and the European Regional Development Fund (FEDER) “A way of making Europe”.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O'Grady NP, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;49(1):1-45. [CrossRef]
- Meeker DG, Beenken KE, Mills WB, Loughran AJ, Spencer HJ, Lynn WB, et al. Evaluation of Antibiotics Active against Methicillin-Resistant Staphylococcus aureus Based on Activity in an Established Biofilm. Antimicrob Agents Chemother. 2016;60(10):5688-94. [CrossRef]
- Díaz-Ruíz C, Alonso B, Cercenado E, Cruces R, Bouza E, Muñoz P, et al. Can dalbavancin be used as a catheter lock solution? J Med Microbiol. 2018;67(7):936-44.
- Rubia M, Cordero A, Pérez-Granda MJ, Cercenado E, Pascual C, Muñoz P, et al. In vitro study to evaluate the bioactivity of freezing a heparin-based dalbavancin lock solution. Antimicrob Agents Chemother. 2020. [CrossRef]
- Peeters E, Nelis HJ, Coenye T. Comparison of multiple methods for quantification of microbial biofilms grown in microtiter plates. J Microbiol Methods. 2008;72(2):157-65. [CrossRef]
- Del Pozo JL, Alonso M, Serrera A, Hernaez S, Aguinaga A, Leiva J. Effectiveness of the antibiotic lock therapy for the treatment of port-related enterococci, Gram-negative, or Gram-positive bacilli bloodstream infections. Diagn Microbiol Infect Dis. 2009;63(2):208-12. [CrossRef]
- Fortún J, Grill F, Martín-Dávila P, Blázquez J, Tato M, Sánchez-Corral J, et al. Treatment of long-term intravascular catheter-related bacteraemia with antibiotic-lock therapy. J Antimicrob Chemother. 2006;58(4):816-21. [CrossRef]
- Kim SH, Kang CI, Kim HB, Youn SS, Oh MD, Kim EC, et al. Outcomes of Hickman catheter salvage in febrile neutropenic cancer patients with Staphylococcus aureus bacteremia. Infect Control Hosp Epidemiol. 2003;24(12):897-904. [CrossRef]
- Park KH, Cho OH, Lee SO, Choi SH, Kim YS, Woo JH, et al. Outcome of attempted Hickman catheter salvage in febrile neutropenic cancer patients with Staphylococcus aureus bacteremia. Ann Hematol. 2010;89(11):1163-9. [CrossRef]
- Beigi AA, Khansoltani S, Masoudpour H, Atapour AA, Eshaghian A, Khademi EF. Influence of intralumenal and antibiotic-lock of vancomycin on the rate of catheter removal in the patients with permanent hemodialysis catheters. Saudi J Kidney Dis Transpl. 2010;21(1):54-8.
- Krishnasami Z, Carlton D, Bimbo L, Taylor ME, Balkovetz DF, Barker J, et al. Management of hemodialysis catheter-related bacteremia with an adjunctive antibiotic lock solution. Kidney Int. 2002;61(3):1136-42. [CrossRef]
- Chaves F, Garnacho-Montero J, Del Pozo JL, Bouza E, Capdevila JA, de Cueto M, et al. Executive summary: Diagnosis and Treatment of Catheter-Related Bloodstream Infection: Clinical Guidelines of the Spanish Society of Clinical Microbiology and Infectious Diseases (SEIMC) and the Spanish Society of Intensive Care Medicine and Coronary Units (SEMICYUC). Enfermedades infecciosas y microbiologia clinica (English ed). 2018;36(2):112-9.
- Sevillano D AL, González N, Buenache N, Suárez A, Gómez-Lus ML, Barberán J, Collado L, Prieto J. Evlauación comparativa de la actividad de la dalbavancina, daptomicina, linezolid y vancomicina en la estrategia de sellado del catéter colonizado por S. aureus resistente a meticilina (SARM) y de S. epidermidis resistente a meticilina (SEMR). Congreso de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica (SEIMC)2017.
- Anthony TU, Rubin LG. Stability of antibiotics used for antibiotic-lock treatment of infections of implantable venous devices (ports). Antimicrob Agents Chemother. 1999;43(8):2074-6. [CrossRef]
- Bookstaver PB, Rokas KE, Norris LB, Edwards JM, Sherertz RJ. Stability and compatibility of antimicrobial lock solutions. Am J Health Syst Pharm. 2013;70(24):2185-98. [CrossRef]
- Morales-Molina JA, Mateu-de Antonio J, Grau S, Segura M, Acosta P. [Stability: a factor to consider in antibiotic-lock solutions]. Enferm Infecc Microbiol Clin. 2010;28(2):104-9. [CrossRef]
Figure 1.
(A). Median percentage reduction in log cfu/ml for dalbavancin-heparin and dalbavancin solutions against MRSA during freezing time. (B). Median percentage reduction in metabolic activity for dalbavancin-heparin and dalbavancin solutions against MRSA during freezing time. (C). Median percentage reduction in log cfu/ml for dalbavancin-heparin and dalbavancin solutions against MRSE during freezing time. (D). Median percentage reduction in metabolic activity for dalbavancin-heparin and dalbavancin solutions against MRSE during freezing time. DH, dalbavancin-heparin; cfu, colony-forming units; MRSA, methicillin-resistant Staphylococcus aureus; MRSE, methicillin-resistant Staphylococcus epidermidis. The markers correspond to the lower limit of 25% of the D value.
Figure 1.
(A). Median percentage reduction in log cfu/ml for dalbavancin-heparin and dalbavancin solutions against MRSA during freezing time. (B). Median percentage reduction in metabolic activity for dalbavancin-heparin and dalbavancin solutions against MRSA during freezing time. (C). Median percentage reduction in log cfu/ml for dalbavancin-heparin and dalbavancin solutions against MRSE during freezing time. (D). Median percentage reduction in metabolic activity for dalbavancin-heparin and dalbavancin solutions against MRSE during freezing time. DH, dalbavancin-heparin; cfu, colony-forming units; MRSA, methicillin-resistant Staphylococcus aureus; MRSE, methicillin-resistant Staphylococcus epidermidis. The markers correspond to the lower limit of 25% of the D value.
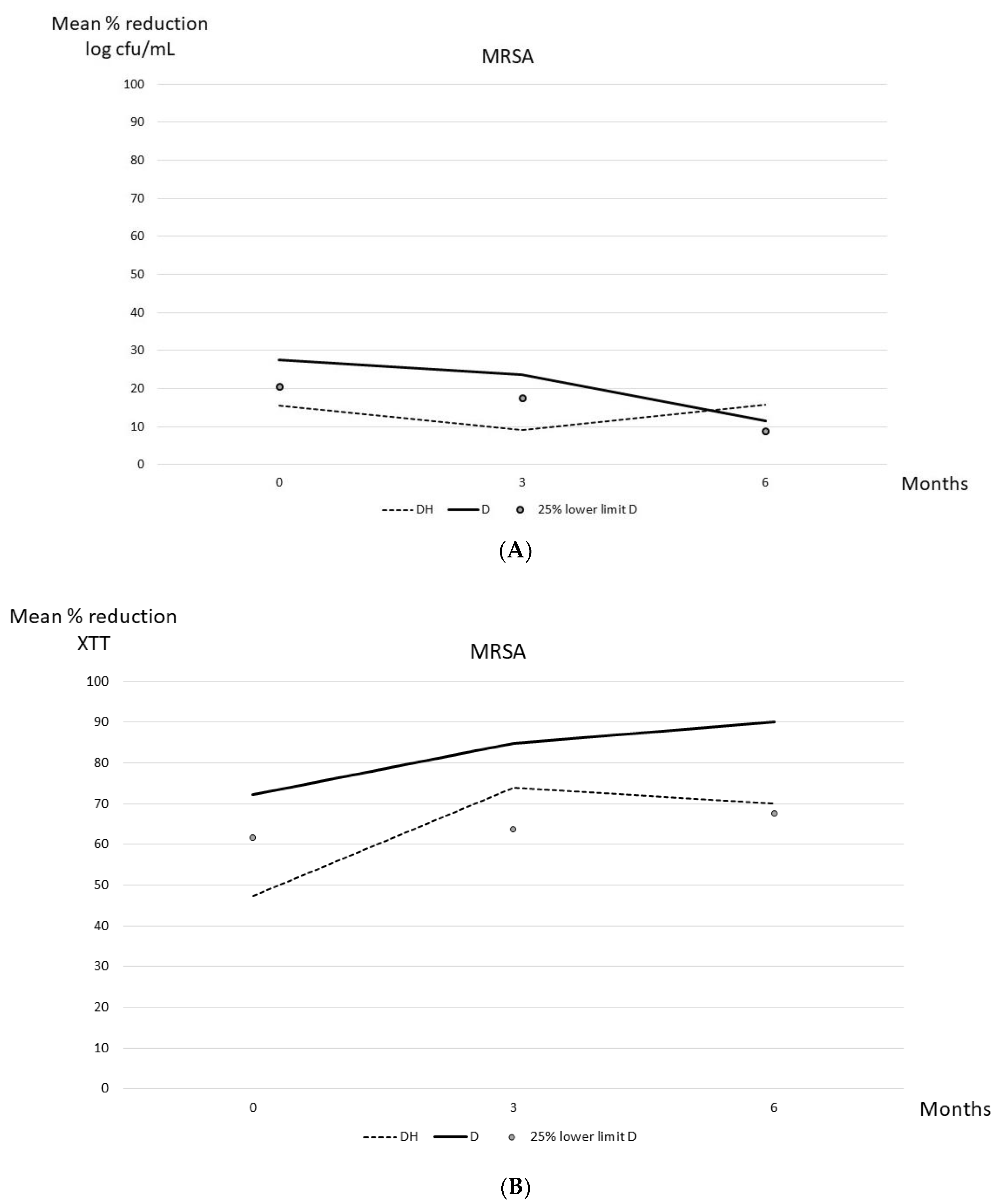
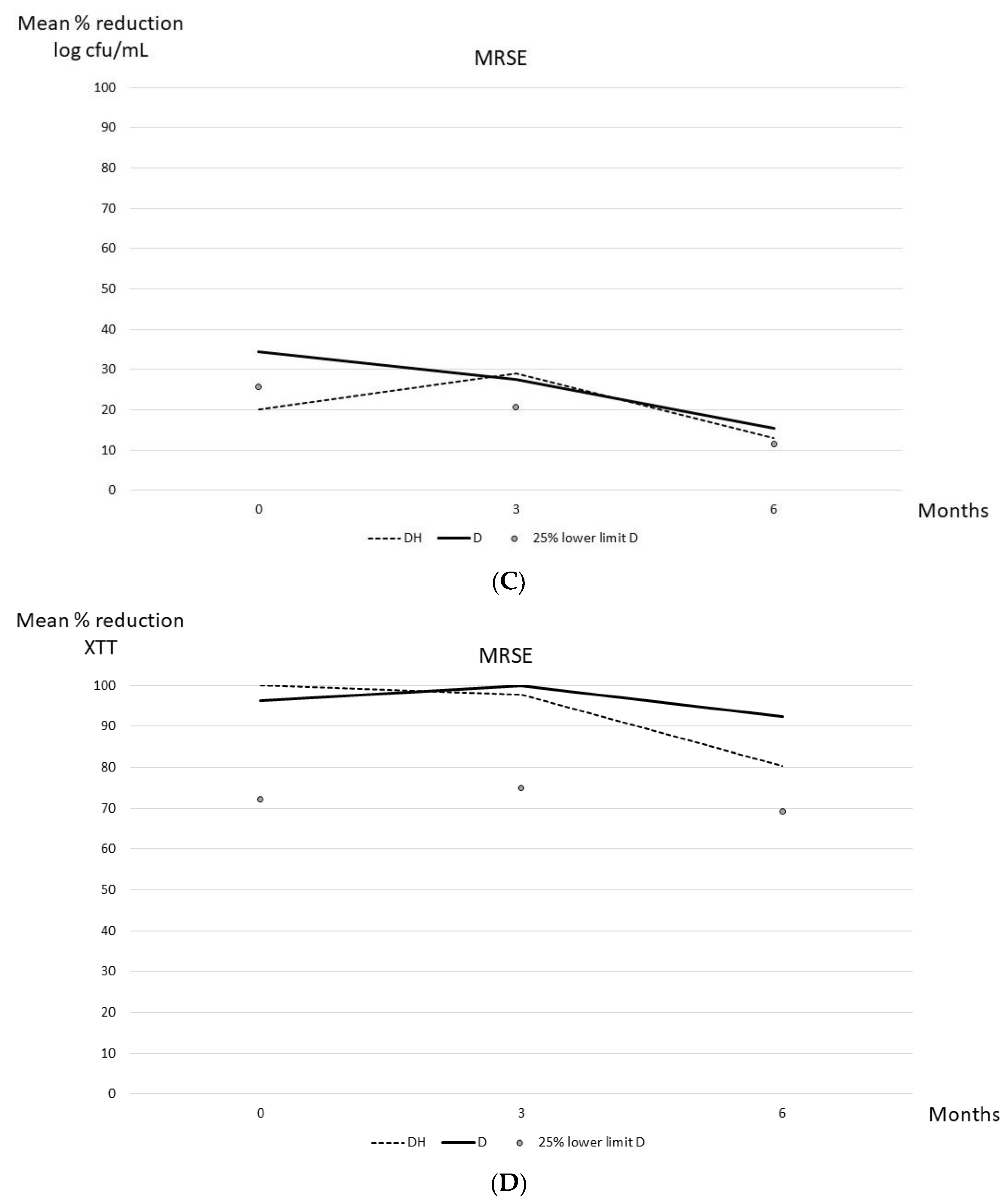

Table 1.
Median (IQR) percentage reduction in log cfu/ml and metabolic activity for dalbavancin alone and dalbavancin-heparin against MRSA and MRSE biofilms during freezing.
Table 1.
Median (IQR) percentage reduction in log cfu/ml and metabolic activity for dalbavancin alone and dalbavancin-heparin against MRSA and MRSE biofilms during freezing.
| MRSA | |||||
|---|---|---|---|---|---|
| Month | D | DH | p | 25% lower limit of D* | |
| Median (IQR) % reduction in log cfu/ml | 0 | 27.5 (27.2-27.5) | 15.5 (15.4-15.5) | 0.05 | 20.6 |
| 3 | 23.5 (23.4-23.5) | 9.2 (8.4-9.2) | 0.05 | 17.6 | |
| 6 | 11.7 (11.3-11.7) | 12.5 (11.6-12.5) | 0.275 | 8.8 | |
| Median (IQR) % reduction in XTT | 0 | 72.3 (0.0-72.3) | 47.4 (35.9-47.4) | 0.827 | 61.7 |
| 3 | 84.9 (84.1-84.9) | 73.9 (70.5-73.9) | 0.05 | 63.7 | |
| 6 | 90.2 (79.8-90.2) | 70.1 (62.8-70.1) | 0.05 | 67.7 | |
| MRSE | |||||
| Month | D | DH | p | ||
| Median (IQR) % reduction in log cfu/ml | 0 | 34.3 (33.9-34.3) | 20.1 (19.9-20.1) | 0.05 | 25.7 |
| 3 | 27.6 (27.2-27.6) | 29.0 (28.9-29.0) | 0.05 | 20.7 | |
| 6 | 15.5 (15.4-15.5) | 13.0 (12.8-13.0) | 0.05 | 11.6 | |
| Median (IQR) % reduction in XTT | 0 | 96.3 (80.0-96.3) | 100 (100-100) | 0.121 | 72.2 |
| 3 | 100 (100-100) | 97.6 (96.0-97.6) | 0.037 | 75.0 | |
| 6 | 92.3 (62.8-92.3) | 80.8 (73.9-80.8) | 0.513 | 69.2 | |
SD, standard deviation; MRSA, methicillin-resistant Staphylococcus aureus; MRSE; methicillin-resistant Staphylococcus epidermidis; D, dalbavancin; DH, dalbavancin-heparin; cfu, colony-forming units. *Values in bold corresponded to DH values that were under the 25% lower limit of D values (clinical significance).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



