Submitted:
29 September 2023
Posted:
29 September 2023
You are already at the latest version
Abstract
The pharmacokinetic profile of fat-soluble vitamins A, E, K1, and D3 co-administered with liquid paraffin or water in an experimental rat model was investigated. Animals received a solution of the four vitamins orally through a probe, followed 10 minutes later by the administration of either the liquid paraffin product dissolved in water (Emuliquen Simple®) or water (control). Vitamin formulations were 20, 50, 0.30 and 0.10 mg/kg for vitamins A, E, K1, and D3, respectively. Blood samples were collected before dosing and at 0.17, 1, 2, 4, 8, and 24 hours post-dosing. Vitamin concentrations were quantified by liquid chromatography coupled with mass spectrometry. No relevant differences in the absorption of vitamins in terms of AUC0-last (area under the curve up to the last measurable concentration) or Cmax in the absence or presence of co-administration of the liquid paraffin product were observed. The difference of these parameters between the treatment groups for all vitamins was in the range of bioequivalence (≤ 20%). The liquid paraffin-based laxative product did not interfere with the absorption of vitamins A, E, K1, and D3 that are ingested in the diet, which is clinically relevant due to the high prevalence of functional constipation in children and adults.
Keywords:
constipation
; laxatives
; liquid paraffin
; fat-soluble vitamins
; vitamin A
; vitamin E
; vitamin D3
; vitamin K1
; pharmacokinetics
; experimental model.
1. Introduction
Chronic constipation is an important health problem for many adults, more common in women than in men, in subjects with sedentary lifestyle and reduced fluids and dietary fiber intake, older people, pregnant women, patients with disorders that affect gut motility or use of medications that slow intestinal transit [1,2,3]. Constipation is a symptom that is described as the feeling of incomplete evacuation, excessive straining or failed or lengthy attempts to defecate, hard stools and/or infrequent bowel movements. Idiopathic chronic constipation is characterized by defecation not following any periodicity pattern in association with pain and/or difficulty during defecation. A relevant feature is the lack of any identifiable etiology, such as anatomical causes (anal stenosis, anal atresia, intestinal structure, etc.); muscular dystrophy; intestinal nerve abnormalities (Hirschsprung disease, spinal cord defects); metabolic and endocrine causes (hypokalemia, hypercalcemia, diabetes, hypothyroidism); drugs (narcotics, anticholinergics, antidepressants); and celiac disease, cystic fibrosis, or inflammatory bowel disease, among others. Functional (non-organic) or retentive constipation is diagnosed when all organic causes have been reasonably excluded.
According to the Rome IV criteria [4], definition of functional constipation should include two or more of the following: straining during more than 25% of defecations: lumpy or hard stools (separated hard lumps like nuts hard to pass or sausage-shape but lumpy); sensation of incomplete evacuation more than 25% of defecations; sensation of anorectal obstruction/blockage more than 25% of defecations; manual maneuvers to facilitate more than 25% defecation (e.g. pelvic floor support, digital evacuation); loose stools rarely present without the use of laxatives; and fewer than three spontaneous bowel movement per week. On the other hand, child/adolescent Rome IV criteria [4] for constipation require a minimum of 1 month of two or more of the following occurring at least once per week: two or fewer defecation in the toilette per week (child ≥ 4 years of age); history or painful or hard bowel movements; history of retentive posturing or excessive volitional stool retention; and at least one episode of fecal incontinence per week.
Despite the use of Rome IV criteria for defining functional constipation in the framework of clinical studies, functional constipation is more simply considered when a person is experiencing persistent constipation symptoms (infrequent bowel movements and/or seemingly incomplete defecation) without any clearly identifiable cause [1].
The prevalence of chronic functional constipation is very high. Population-based epidemiological studies have shown prevalence rates between 12% and 27% [5,6]. In Europe, the prevalence of chronic constipation is 17% increasing to 30% in adults over 65 years of age [7]. In Spain, chronic constipation affects one out of five people, accounting for up to 20% of all gastrointestinal consultations in primary care [8]. On the other hand, chronic functional constipation is associated with a significant impact on health-related quality of life and high use of health care resources. A systematic review on the impact of constipation on quality of life (QoL) in children and adults, 13 studies that used the same SF-36/12 generic QoL tool (10 studies in adults and 3 in children) were selected [9]. Pooled results showed consistent impairment of mental and physical components in both adult and child populations, with mental health effects predominating over physical domains. In fact, the magnitude of the impact was comparable to that seen in other conditions, such as musculoskeletal disorders, allergic, or inflammatory bowel disease. With regard to the impact of constipation on daily activities, more than 60% of patients consider that it affects their school or work performance, being a relevant cause of absenteeism in severe cases (average loss 2.4 days per month) and decreased productivity [10,11].
Regarding diagnosis, a correct medical history, physical examination and indication of appropriate morphological and functional tests to rule out secondary constipation are indispensable. Also, treatment of constipation depends on its pathophysiological cause. In patients with chronic functional constipation, clinical practice guidelines recommend a stepwise approach based on lifestyle modification, hygienic-dietary measures, laxatives and prokinetic drugs [8].
Among the different classes of laxatives, liquid paraffin (mineral oil) acts primarily as a stool softener, and for this reason this type of laxative is not associated with other frequent side effects of osmotic or stimulant laxatives [12], such as abdominal colic, diarrhea, flatulence, electrolyte imbalance, and development of tolerance after long-term laxative abuse. Exogenous lipoid pneumonia is an uncommon complication resulting from aspirating or inhaling fatlike material [13] such as mineral oil found in oil-based nasal drops [14,15,16] or laxatives [17,18].
Another interesting aspect is the possible interaction of paraffin-based laxatives with the absorption of dietary fat-soluble vitamins, although evidence is poor and inconclusive. Taking mineral oil on an empty stomach may reduce this interference and it is recommended that mineral oil should not be taken within 2 hours of meals. In a study of 25 children with chronic constipation treated with mineral oil administered between meals, a reduction in serum levels of beta-carotene was observed, but the treatment had no adverse effect on serum levels of retinol (vitamin A1) or alpha-tocopherol (vitamin E) [19]. In another study, differences in plasma retinol, alpha-tocopherol, and prothrombin time between 19 children given enteral mineral oil for 4 months and 16 controls were not observed [20]. Also, in a group of 16 children treated with low doses of liquid paraffin (0.5 mL/kg/day) during 6 months, stable concentrations of vitamin E were recorded [21]. In a clinical case of a 17-year-old girl, large doses of mineral oil (400 mL/day) during 5 months were not accompanied by alterations of vitamins A and E concentrations and changes of serum levels of calcium, phosphorus, alkaline phosphatase, and prothrombin time as indicators of vitamins D and K, respectively [22]. The global consideration of these data indicates that the use of liquid paraffin as a fecal lubricant does not alter the tissue reserves of fat-soluble vitamins.
However, as far as we are aware, studies assessing the interference of liquid paraffin-based laxatives with the absorption of fat-soluble vitamins in experimental animals or in subjects using this type of stool softener laxative have not been carried out. In a study published in 1975 in a pig model, a possible interference in vitamin A absorption after prolonged administration of paraffin was suggested [23]. The objective of this study was to analyze the pharmacokinetic profile of the fat-soluble vitamins A, E, K1 and D3 in co-administration with liquid paraffin or water in an experimental model in rats.
2. Materials and Methods
2.1. Study Design
The study was carried out in an in vivo rat model. The objective of the study was to determine whether the absorption of fat-soluble vitamins (A, E, K1 and D3) was altered by the concomitant administration of an emulsified liquid paraffin formulation, using the administration of ultrapure water (UP) alone as a control.
The study was performed at the testing facility of Admescope Ltd., Oulu, Finland, and was conducted under the project licence ESAVI/3047/04.10.07/2016, approved by the national Animal Experimental Board of Finland under Directive 2010/63/EU of the European Parliament and the Council of 22 September 2010 on the protection of animals used for scientific purposes.
2.2. Animal Experiment and Formulation Preparation
Male Sprague Dawley rats were purchased from the Laboratory Animal Center, University of Oulu, Finland, with one week acclimatization period, and housed according to relevant EU-directives (e.g. 12 h light cycle, 350 cm2 of floor space per animal, 4 animals per cage, and standard rodent food). The animals were allowed free access to food and water. The formulations of vitamins included 20.0 mg/kg for vitamin A, 50.0 mg/kg for vitamin E, 0.30 mg/kg for vitamin K and 0.10 mg/kg for vitamin D3, and were prepared on the day of dosing in a solution of 1%(v/v) ethanol and 99% (v/v) polyethylene glycol 400 (PEG 400). Doses of vitamins A, E, K1 and D3 were selected according to data published in the literature [24,25,26,27,28,29,30] in order to have detectable concentrations of the four vitamins above the basal endogenous level. The formulation of the liquid paraffin laxative was prepared by adding 18.5 mL of UP-water into a vial containing 1.5 mL of Emuliquen (Emuliquen Simple®, Lainco S.A., Rubí, Barcelona, Spain), the composition of which (per 15 mL) includes liquid paraffin 7.1739 g (active principle) and the excipients lichen extract, arabic gum, glycerol, vanillin, benzoic acid, and purified water up to 15 mL. The tube with Emuliquen formulation was shaken for 30 s to create a homogeneous mixture.
Animals (n = 3 per group) received the compound of the four vitamins (5 mL/kg) p.o. by using an oral gavage. Ten minutes after vitamin administration, animals were administered p.o. either UP-water or 7.5% (v/v) Emuliquen in UP-water at 5 mL7Kg. Blood samples were collected into potassium EDTA tubed by venipuncture of the saphenous vein prior to dosing and at 0.17, 1, 2, 4, 8, and 24 h post-dose. Blood samples were centrifuged at 2700 g for 10 min, and plasma aliquots were frozen and stored at -20°C until analysis.
2.3. Analysis and Pharmacokinetic Parameters
Concentrations of vitamins were quantified by ultra-performance liquid chromatography-mass spectrometry (UPLC-MS) for vitamins D3 and K1 or liquid chromatography with ultraviolet detection (LC-UV) for vitamins A and E. Aliquots of vitamins were diluted with UP-water and proteins precipitated with methanol followed by liquid-liquid extraction using ethyl acetate-cyclohexane (ratio 1:1). Samples were then reconstituted with 100 µL of methanol for A and E vitamin determination, with 100 µL of acetonitrile for K1 vitamin, and with 100 µL of acetonitrile containing 4-phenyl-1,2,4-triazoline-3,5-dione (PTAD) for the quantification of D3 vitamin. In all cases, quality control was performed using internal control samples. The detection limits of the techniques were as follows: 500 ng/mL (range 500-10,000 ng/mL) for A vitamin, 5,000 ng/mL (range 5,000-100,000 ng/mL) for E vitamin, 20 ng/mL (range 20-1000 ng/mL) for K1 vitamin, and 10 ng/mL (range 20-5,000 ng/mL) for D3 vitamin.
The pharmacokinetic parameters were calculated using Waters MassLynx 4.1 and ThermoFisher Excalibur 4.0 of the UPLC-MS software program. The maximum plasma concentration (Cmax) and the time to reach Cmax (Tmax) were derived directly from the plasma concentration data. It was established that two formulations that had a reference range ≤ 20% would be clinically bioequivalent according to the guidelines on bioequivalence research of the European Medicines Agency (EMA) [31].
Figure 1 shows a flow diagram of the study.
3. Results
Results of pharmacokinetic parameters for each vitamin (A, E, K1, D3) in co-administration with the experimental product (liquid paraffin emulsion) or water (control) are shown in Table 1.
No relevant differences were in the absorption of vitamins in terms of AUC0-last (area under the plasma concentration-time curve from time 0 to the last quantifiable time point) or Cmax in the absence or presence of co-administration with the liquid paraffin product were observed. Differences of these parameters between the groups of treatment and vitamins were in the ± 20% range. Individual values and mean values for vitamins A, E, K1 and D3 in co-administration with liquid paraffin or water are shown in Figure 2 for vitamin A, Figure 3 for vitamin E, Figure 4 for vitamin K1, and Figure 5 for vitamin D3. Apart from loose bowel, there were no adverse events observed after p.o. dosing in any of the animals.
4. Discussion
The present pharmacokinetic results obtained in an experimental rat model demonstrated that the absorption of fat-soluble vitamins A, E, K1 and D3 is not interfered by the co-administration of the liquid paraffin-based product (Emuliquen Simple®). These findings are clinically relevant and support the lack of interference of liquid paraffin in the intestinal mechanisms that regulate the absorption of vitamins. Regarding the pharmacological profile of liquid paraffin, the characteristics of this substance are those of a purely mechanical laxative. The drug acts by softening the feces and coats the fecal surface with hydrophobic film. The hydrophobic film prevents the water contained in the fecal bolus from being absorbed by the intestine, so that feces remain soft, thereby facilitating fecal expulsion.
Laxatives accelerate the movement of foods and liquids through the digestive tract, and this potentially reduced transit time may induce a negative impact on vitamin absorption, especially those that are fat soluble, such as vitamins A, D, E, and K, as well as minerals such as calcium, sodium, magnesium, and potassium. Robust evidence supporting the use of a particular type of laxative for the management of chronic functional constipation is lacking. Bassotti et al. [32] have evaluated in detail the European, Spanish, French, and Korean clinical guidelines for the management of chronic idiopathic constipation and, in this respect, osmotic laxatives especially polyethylene glycol represent the first therapeutic approach, followed by stimulant laxatives as second-line option. Interestingly in the French and Spanish guidelines, positive effects of lubricant laxatives (such as paraffin oil) are reported and considered as second-line treatment choice supported by expert recommendations [32]. The tolerability and easy titration of liquid paraffin appears one of the reasons of the popularity acquired by this product for the treatment of encopresis and functional constipation. Liquid paraffin seems to act primarily as a stool lubricant, although there is an osmotic effect due to the conversion of mineral oil to hydroxyl fatty acids. Because of the main action of liquid paraffin as stool lubricant, the use of this product is not associated with electrolyte disturbances, flatulence, abdominal cramps, or diarrhea even after use for prolonged periods. In contrast to side effects with long-term usage associated with other stimulant or osmotic or laxatives, liquid paraffin has an excellent tolerability and safety profile [12]. These features and the effectiveness make liquid paraffin especially attractive for its use in childhood constipation.
In a systematic review of 19 clinical studies and 4 meta-analyses, both nonstimulant and stimulant laxatives provided better relief of constipation symptoms than placebo according to both objective and subjective measures [33]. In two studies included in this systematic review that examined liquid paraffin, compared with either lactulose or polyethylene glycol (PEG) in pediatric patients, the efficacy and safety profile of both products was similar (bowel movements per week, episodes of encopresis, adverse events) [33]. In a systematic review of 8 randomized controlled trials (RCTs) with 1,643 patients aged 0 to 18 years old published in 2013, both polyethylene glycol preparations and liquid paraffin (mineral oil) increased the frequency of bowel motions in constipated children and were also safe [34]. However, interpretation of the pooled analyses is difficult due low methodological quality and heterogeneity of primary studies, inconsistencies in the definition of variables, and risk of bias. These conclusions have not changed in an updated review of 25 studies with 2,310 participants aged 0 to 18 years published in 2016 [35]. However, there are no published data from RCTs, systematic reviews and meta-analyses that have compared the effectiveness of different types of laxatives in the treatment of chronic functional constipation in adult patient populations.
It has been widely believed that ingestion of liquid paraffin may affect the absorption of fat-soluble vitamins, although this consideration seems to be unfounded and based on early studies [12]. Javert and Macri in 1941 documented hypoprothrombinemia during liquid paraffin therapy of variable duration in a small sample of 10 adult patients [36]. Previously, in 1939, Curtis and Balmer [37] showed decreases in serum values of carotene (vitamin A) after some weeks of use of liquid paraffin, but values in the range of carotene deficiency were not found. In a study of serial monitoring (up to 4 months) of serum beta-carotene, retinol (vitamin A1), and alpha-tocopherol (vitamin E) levels during mineral oil therapy in 25 children with chronic constipation in whom mineral oil was administered between meals, concentrations of serum levels of retinol and alpha-tocopherol remained unchanged [19]. More recently, Gal-Ezer and Shaoul [22] reported a case report in a 17-year-old girl illustrating the safety of prolonged administration of mineral oil (5 months) in the treatment of constipation without impairment of fat-soluble vitamin absorption. In a study that evaluated combined high-fiber, laxative (mineral oil), and lubricant therapy on bowel movement frequency, fecal soiling, and nutritional status over a 6-month period in 16 children (4 to 12 years of age), changes in serum levels of vitamin E were not observed [21]. The authors of this study selected evaluation of vitamin E as a marker of fat-soluble vitamin status and the results corroborate the safety of mineral oil on fat-soluble vitamin status. However, in none of these previous studies, pharmacokinetic investigations have been performed.
In this respect, the present study provides original data on the in vivo pharmacokinetics of the absorption of vitamins A, E, K1 and D3 in co-administration with a commonly used liquid paraffin laxative product or water as a control. In order to evaluate the possible interference of liquid paraffin with the absorption of vitamins, this pharmacokinetic study has been carried out in an experimental model in rats, co-administering a solution containing the four fat-soluble vitamins together with the dose of the laxative equivalent to that used in clinical practice for the standard treatment of chronic functional constipation in adults (mg/body surface area). Also, the study was also performed at Admescope Ltd., an independent company located in Oulu, Finland, with proven experience in studies of absorption, distribution, metabolism and excretion of pharmaceutical products in animal models. Dosing through the oral route with a solution of the four vitamins (A, E, K1 and D3) followed by the administration of liquid paraffin or vehicle (water) in a 10 min interval was chosen to simulate the administration of the laxative near the food. The kinetic times were distributed over 24 hours in order to characterize as better as possible, the kinetic profiles of the four vitamins by obtaining detectable plasma concentrations higher than their endogenous basal levels.
5. Conclusions
The present experimental study indicates that the use of Emuliquen Simple® as a liquid paraffin-based laxative does not interfere with the absorption of vitamins A, E, K1 and D3 that are ingested with diet, which is clinically relevant due to the importance of functional constipation as a highly prevalent disorder in children and adults. The special formulation of the product characterized by 75% particle emulsion between 5 and 15 micrometers in size may account for the reduction of the adverse effects related to interference in the absorption of fat-soluble vitamins, being nonexistent in the rat model evaluated in our study. These findings, however, cannot be extrapolated to the use of liquid paraffin alone or to the use of another paraffin formulation different form that used in this study.
Author Contributions
Conceptualization, J.M. and V.R.; methodology, J.M., V.R. and V.M.; formal analysis, V.R., E.K. and V.M.; data curation, E.K. and V. M.; writing-review and editing, J.M., V.R., E.K. and V.M.; supervision, F.P.A.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Study data are available from the authors upon request.
Acknowledgments
The authors thank Lainco, S.A., and Grupo SANED, S.L., for logistic support and Marta Pulido, MD, PhD, for editing the manuscript and editorial assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Basilisco, G.; Coletta, M. Chronic constipation: a critical review. Dig Liver Dis 2013, 45, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.S. Constipation: evaluation and treatment of colonic and anorectal motility disorders. Gastroenterol Clin North Am 2007, 36, 687–711. [Google Scholar] [CrossRef] [PubMed]
- Cullen, G.; O'Donoghue, D. Constipation and pregnancy. Best Pract Res Clin Gastroenterol 2007, 21, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Sobrao, C.W.; Corrêa Neto, I.J.P.; Ambar Pinto, R.; Sobrado, L.F.; Nahas, S.C.; Cecconello, I. Diagnosis and treatment of constipation: a clinical update based on the Rome IV criteria. J Coloproctol 2018, 32, 137–144. [Google Scholar]
- Pinto Sanchez, M.I.; Bercik, P. Epidemiology and burden of chronic constipation. Can J Gastroenterol 2011, 25 (Suppl B), B),11B–15B. [Google Scholar] [CrossRef]
- Higgins, P.D.; Johanson, J.F. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol 2004, 99, 750–759. [Google Scholar] [CrossRef]
- Peppas, G.; Alexiou, V.G.; Mourtzoukou, E.; Falagas, M.E. Epidemiology of constipation in Europe and Oceania: a systematic review. BMC Gastroentrol 2008, 8, 5. [Google Scholar] [CrossRef]
- Escudero Sanchís, A.; Bixquert Jiménez, M. Guía para prevenir y tratar el estreñimiento. Fundación Española de Aparato Digestivo (FEAD). Available online: https://www.saludigestivo.es/wp-content/uploads/2016/03/guia-estrenimiento-para-web-20120425180854.pdf. (accessed on 20 February 2021).
- Belsey, J.; Greenfield, S.; Candy, D.; Geraint, M. Systematic review: impact of constipation on quality of life in adults and children. Aliment Pharmacol Ther 2010, 31, 938–949. [Google Scholar] [CrossRef]
- Mearín, F. Impacto del estreñimiento crónico en la calidad de vida: mucho más importante de lo que parece. Prog Gastroenterol 2013, 36, 443–498. [Google Scholar] [CrossRef]
- Johanson, J.F.; Kralstein, J. Chronic constipation: a survey of the patient perspective. Aliment Pharmacol Ther 2007, 25, 599–608. [Google Scholar] [CrossRef]
- Sharif, F.; Crushell, E.; O’Driscoll, K.; Bourke, B. Liquid paraffin: a reappraisal of its role in the treatment of constipation. Arch Dis Child 2001, 85, 121–124. [Google Scholar] [CrossRef]
- Hadda, V.; Khilnani, G.C. Lipoid pneumonia: an overview. Expert Rev Respir Med 2010, 4, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Alaminos García, P.; Colodro Ruiz, A.; Menduiña Guillén, M.J.; Báñez Sánchez, F.; Pérez Chica, G. Neumonía lipoidea exógena. Presentación de un nuevo caso. An Med Interna (Madrid) 2005, 22, 283–284. [Google Scholar] [CrossRef]
- Aliaga, F.; Chernilo, S.; Fernández, C.; Valenzuela, H.; Rodríguez, J.C. Neumonía lipoidea exógena: uma causa inabitual de nódulos pulmonares. Casos clínicos. Rev Med Chil 2017, 145, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Osman, G.A.; Ricci, A.; Terzo, F.; Falasca, C.; Giovagnoli, M.R.; Bruno, P.; et al. Exogenous lipoid pneumonia induced by nasal decongestant. Clin Respir J 2018, 12, 524–531. [Google Scholar] [CrossRef]
- Bandla, H.P.; Davis, S.H.; Hopkins, N.E. Lipoid pneumonia: a silent complication of mineral oil aspiration. Pediatrics 1999, 103, E19. [Google Scholar] [CrossRef] [PubMed]
- Ohwada, A.; Yoshioka, Y.; Shimanuki, Y.; Mitani, K.; Kumasaka, T.; Dambara, T.; et al. Exogenous lipoid pneumonia following ingestion of liquid paraffin. Intern Med 2002, 41, 483–486. [Google Scholar] [CrossRef]
- Clark, J.H.; Russell, G.J.; Fitzgerald, J.F.; Nagamori, K.E. Serum beta-carotene, retinol, and alpha-tocopherol levels during mineral oil therapy for constipation. Am J Dis Child 1987, 141, 1210–1212. [Google Scholar]
- Ballantine, T.V.N.; Zeigler, D.; Greecher, C.P.; Smith, J.; Karl, S.R. The effect of mineral oil (MO) on fat-soluble vitamin levels. [Abstract]. JPEN J Parenter Enteral Nutr 1986, 10, S18. [Google Scholar]
- McClung, H.J.; Boyne, L.J.; Linsheid, T.; Heitlinger, L.A.; Murray, R.D.; Fyda, J.; et al. Is combination therapy for encopresis nutritionally safe? Pediatrics 1993, 91, 591–594. [Google Scholar] [CrossRef]
- Gal-Ezer, S.; Shaoul, R. The safety of mineral oil in the treatment of constipation--a lesson from prolonged overdose. Clin Pediatr (Phila) 2006, 45, 856–858. [Google Scholar] [CrossRef]
- Tulliez, J.; Bories, G.; Peleran, J.C. The effect of prolonged ingestion of paraffin oil in pigs: selective retention and interference with cholesterol metabolism. C R Acad Sci Hebd Seances Acad Sci D 1975, 280, 2261–2264. [Google Scholar]
- Abuasal, B.; Thomas, S.; Sylvester, P.W.; Kaddoumi, A. Development and validation of a reversed-phase HPLC method for the determination of γ-tocotrienol in rat and human plasma. Biomed Chromatogr 2011, 25, 621–627. [Google Scholar] [CrossRef]
- Craciun, A.M.; Groenen-van Dooren, M.M.; Vermeer, C. Nutritional vitamin K-intake and urinary gamma-carboxyglutamate excretion in the rat. Biochim Biophys Acta 1997, 1334, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Gershkovich, P.; Ibrahim, F.; Sivak, O.; Darlington, J.W.; Wasan, K.M. A simple and sensitive method for determination of vitamins D3 and K1 in rat plasma: application for an in vivo pharmacokinetic study. Drug Dev Ind Pharm 2014, 40, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, H.; Miyata, C.; Nagata, Y.; Urano, S.; Matsushima, Y. Determination of alpha-tocopherol and alpha-tocopherylquinone in rat tissues and plasma by high-performance liquid chromatography with electrochemical detection. Chem Pharm Bull (Tokyo) 2000, 48, 1462–1466. [Google Scholar] [CrossRef]
- Tovar, A.; Ameho, C.K.; Blumberg, J.B.; Peterson, J.W.; Smith, D.; Booth, S.L. Extrahepatic tissue concentrations of vitamin K are lower in rats fed a high vitamin E diet. Nutr Metab (Lond) 2006, 3, 29. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Nomura, S.; Ichikawa, T.; Abe, C.; Ikeda, S. Tissue distribution of vitamin E metabolites in rats after oral administration of tocopherol or tocotrienol. J Nutr Sci Vitaminol (Tokyo) 2011, 57, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Pan, X.; Chen, G.; Li, J.; Liu, L.; Liu, X.; Jin, S.; Xie, L.; Wang, G. Increased exposure of vitamin A by Chrysanthemum morifolium Ramat extract in rat was not via induction of CYP1A1, CYP1A2, and CYP2B1. J Food Sci 2012, 77, H121–127. [Google Scholar] [CrossRef]
- European Medicines Agency (EMA). Committee for Medical Products for Human Use (CMPH). Guideline on the investigation of bioequivalence. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-investigation-bioequivalence-rev1_en.pdf (accessed on 20 February 2021).
- Bassotti, G.; Usai Satta, P.; Bellini, M. Chronic idiopathic constipation in adults: A review on current guidelines and emerging treatment options. Clin Exp Gastroenterol 2021, 14, 413–428. [Google Scholar] [CrossRef] [PubMed]
- Paré, P.; Fedorak, R.N. Systematic review of simulant and nonstimulant laxatives for the treatment of functional constipation. Can J Gastroenterol Hepatol 2014, 28, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.; Naidoo, K.; Akobeng, A.K.; Thomas, A.G. Cochrane Review: Osmotic and stimulant laxatives for the management of childhood constipation (Review). Evid Based Child Health 2013, 8, 57–109. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.; MacDonald, J.K.; Parker, C.E.; Akobeng, A.K.; Thomas, A. Osmotic and stimulant laxatives for the management of childhood constipation. Cochrane Database Syst Rev 2016, Issue 8. Art. No.: CD009118. [CrossRef]
- Javert, C.T.; Macri, C. Prothrombin concentration and mineral oil. Am J Obstet Gynecol 1941, 42, 409–414. [Google Scholar] [CrossRef]
- Curtis, A.C.; Ballmer, R.S. The prevention of carotene absorption by liquid petrolatum. JAMA 1939, 113, 1785–1788. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of the study.
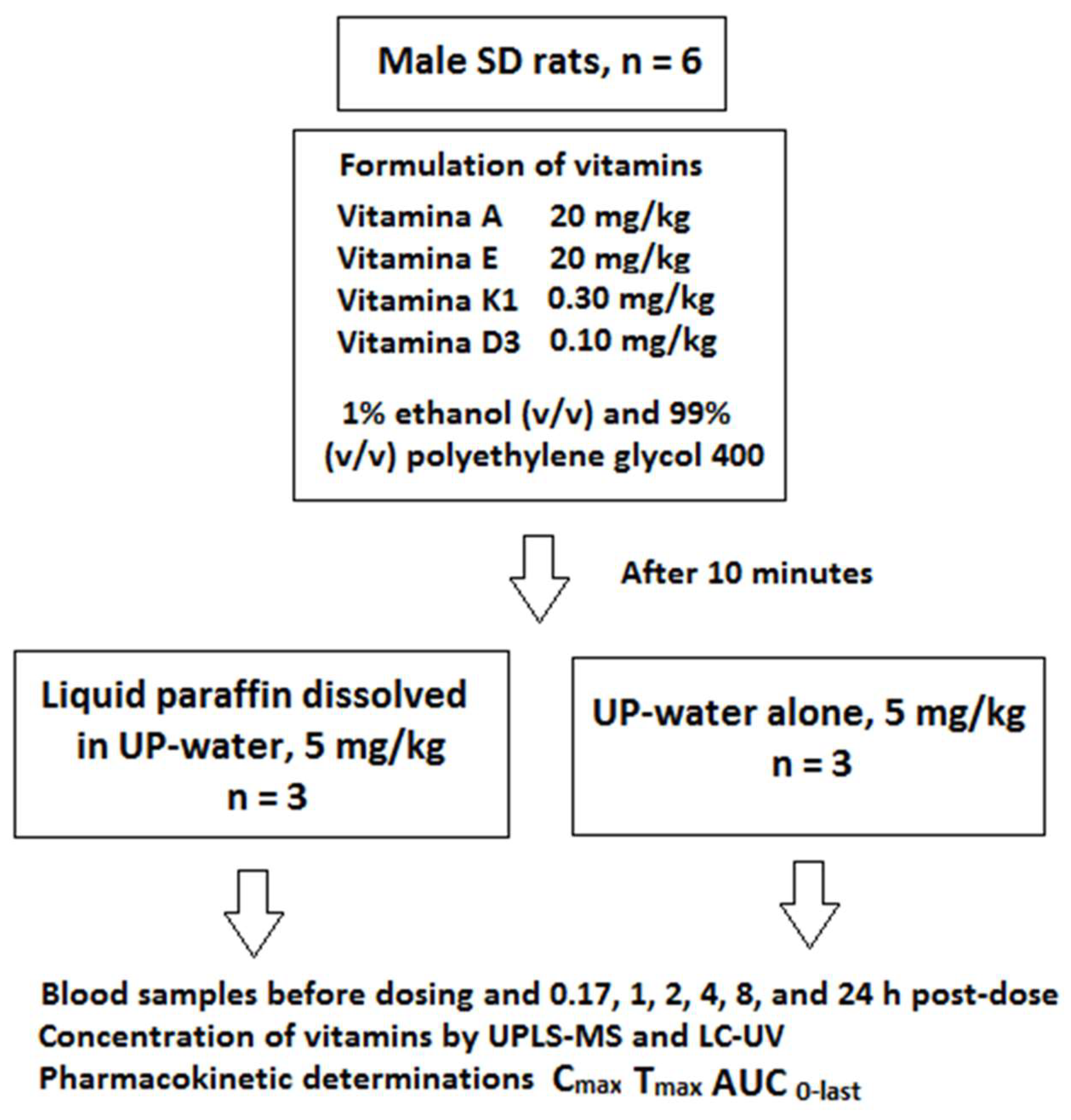
Figure 2.
Individual variations and mean (± standard deviation, SD) concentrations of vitamin A after p.o. administration of 20 mg/kg with co-administration of liquid paraffin or water.
Figure 2.
Individual variations and mean (± standard deviation, SD) concentrations of vitamin A after p.o. administration of 20 mg/kg with co-administration of liquid paraffin or water.
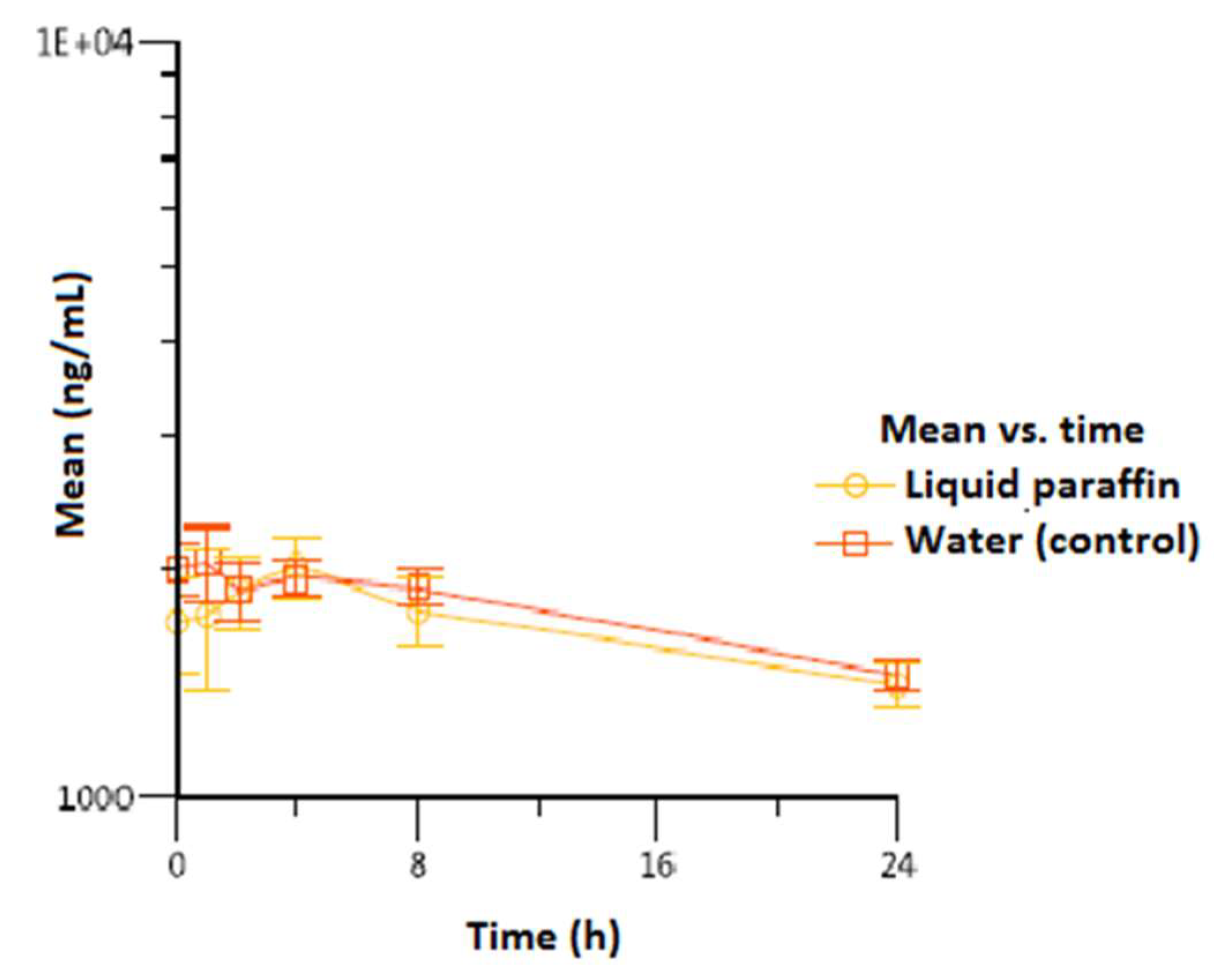
Figure 3.
Individual variations and mean (± standard deviation, SD) concentrations of vitamin E after p.o. administration of 50 mg/kg with co-administration of liquid paraffin or water.
Figure 3.
Individual variations and mean (± standard deviation, SD) concentrations of vitamin E after p.o. administration of 50 mg/kg with co-administration of liquid paraffin or water.
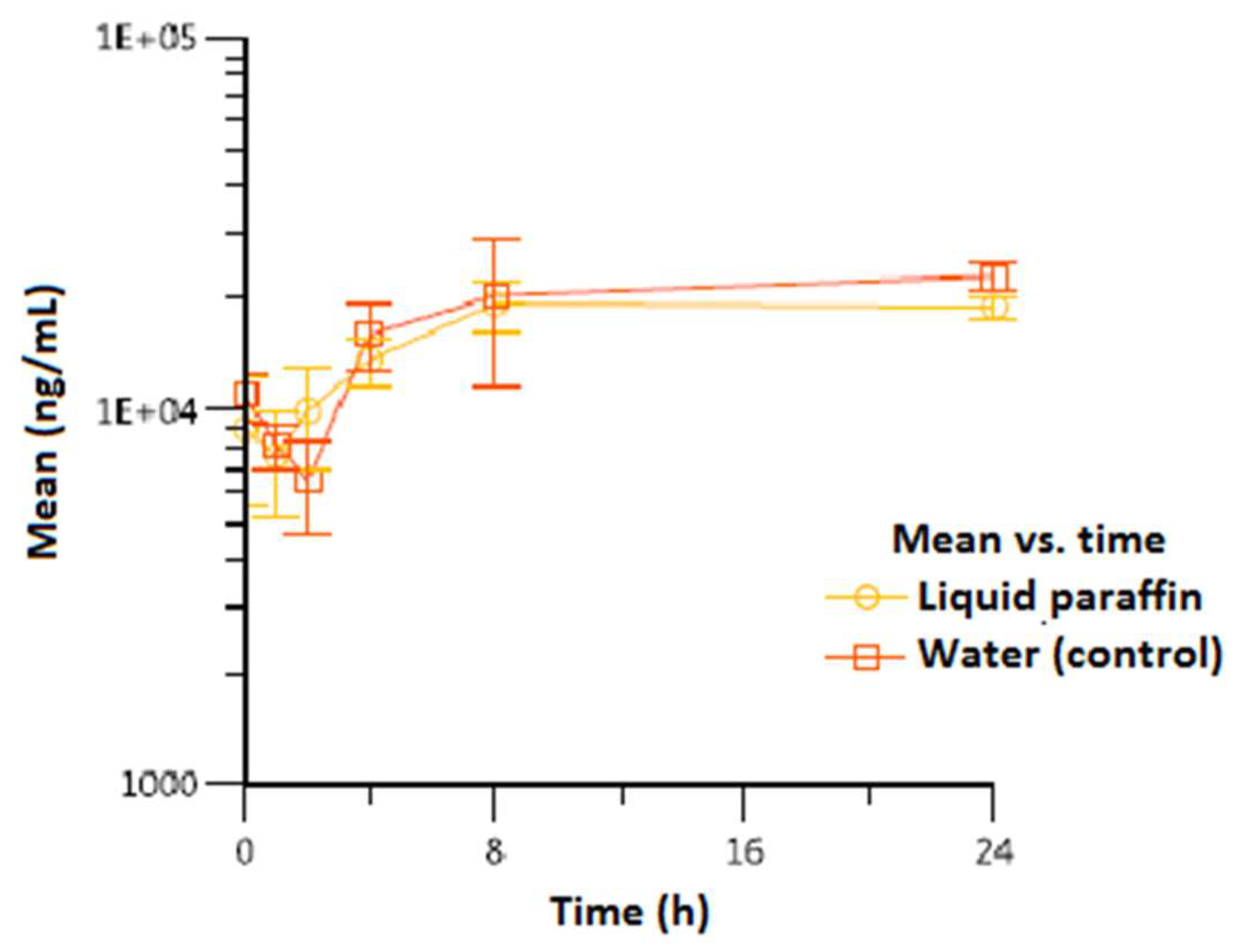
Figure 4.
Individual variations and mean (± standard deviation, SD) concentrations of vitamin K1 after p.o. administration of 0.3 mg/kg with co-administration of liquid paraffin or water.
Figure 4.
Individual variations and mean (± standard deviation, SD) concentrations of vitamin K1 after p.o. administration of 0.3 mg/kg with co-administration of liquid paraffin or water.
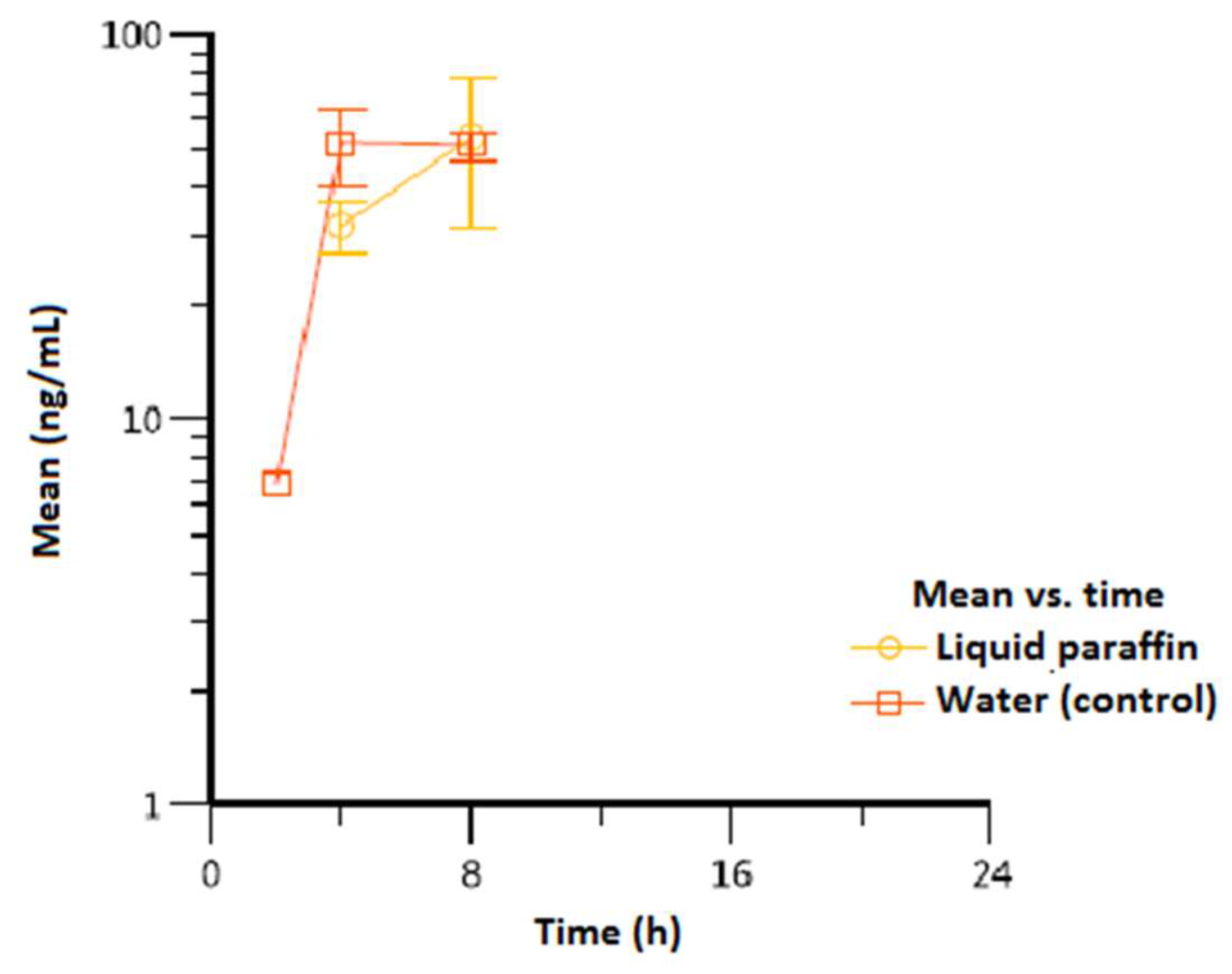
Figure 5.
Individual variations and mean (± standard deviation, SD) concentrations of vitamin D3 after p.o. administration of 0.1 mg/kg with co-administration of liquid paraffin or water.
Figure 5.
Individual variations and mean (± standard deviation, SD) concentrations of vitamin D3 after p.o. administration of 0.1 mg/kg with co-administration of liquid paraffin or water.
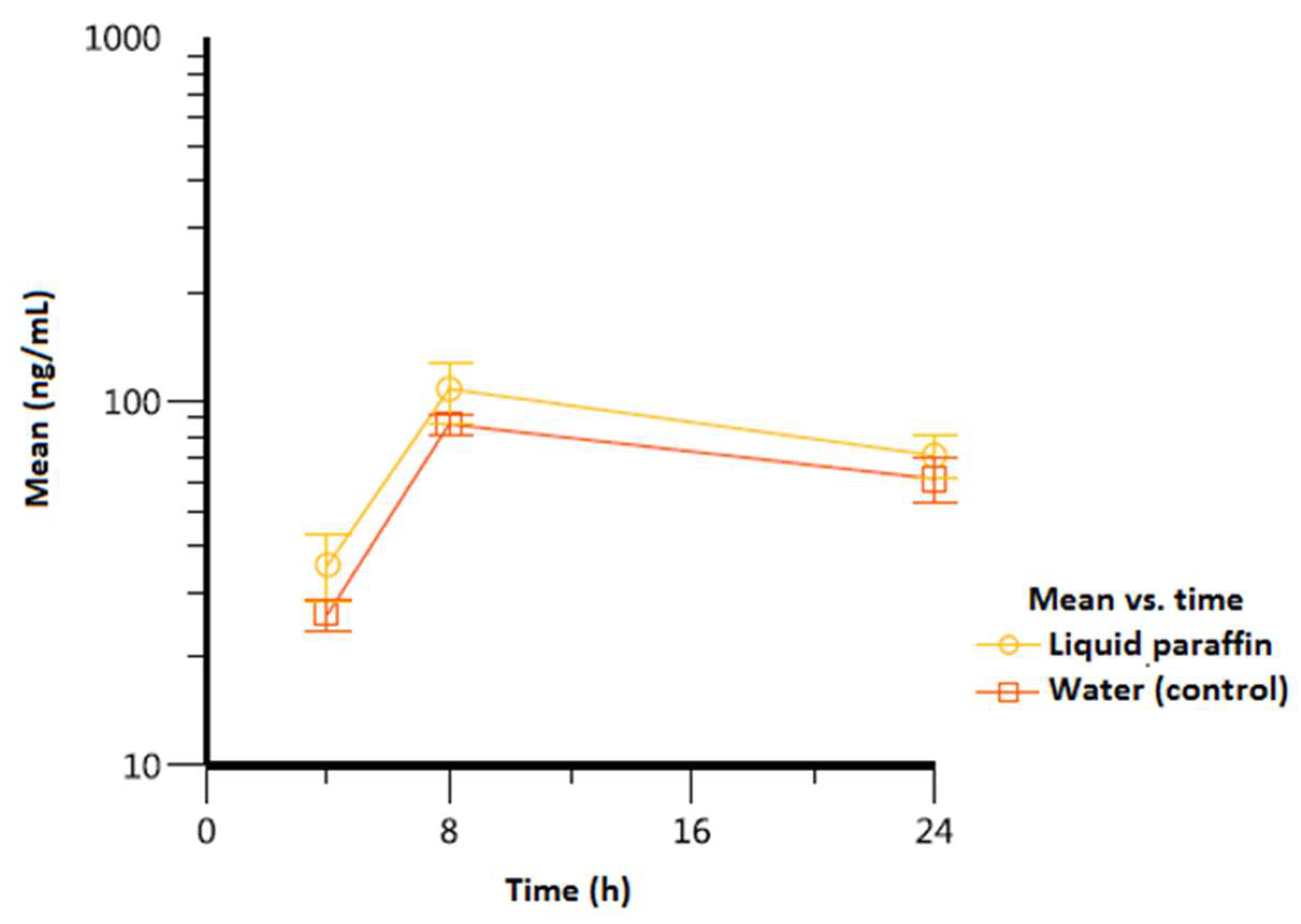

Table 1.
Pharmacokineric results.
| Experimental condition |
Tmax, h per animal* |
Cmax, ng/mL mean (SD) |
Tlast, h per animal* |
Clast, ng/mL mean (SD) |
AUC0-last, h·ng/mL mean (SD) |
|---|---|---|---|---|---|
| Vitamin A | |||||
| Liquid paraffin | 4/4/4 | 1.023 (200) | 24/24/24 | 1.407 (96.1) | 40.358 (4.012) |
| Water (control) | 1/1/4 | 2.130 (130) | 24/24/24 | 1.453 (66.6) | 42.245 (1.717) |
| Vitamin E | |||||
| Liquid paraffin | 24/8/24 | 19.900 (2.784) | 24/24/24 | 18.967 (1.401) | 413.535 (48.526) |
| Water (control) | 24/8/24 | 25.367 (4.636) | 24/24/24 | 22.933 (1.801) | 458.453 (100.118) |
| Vitamin K1 | |||||
| Liquid paraffin | 8/8/8 | 54.1 (22.5) | 8/8/8 | 54.1 (22.5) | 637 (237) |
| Water (control) | 8/8/4 | 57.3 (7.70) | 8/8/8 | 51.8 (4.68) | 686 (57.0) |
| Vitamin D3 | |||||
| Liquid paraffin | 8/8/8 | 108 (20.6) | 24/24/24 | 71.2 (9.42) | 1.796 (136) |
| Water (control) | 8/8/8 | 86.7 (5.49) | 24/24/24 | 61.4 (8.47) | 1.463 (12.7) |
*Individual data for each of the three animals in each group; Tlast: time to the last quantifiable time point; Clast: plasma concentration in the last quantifiable time point; AUC0-last: area under the curve from time 0 to the last quantifiable time point; SD: standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



