Submitted:
29 September 2023
Posted:
29 September 2023
Read the latest preprint version here
Abstract
Starvation of photoreceptors induced by reduced dysregulated ocular blood flow (OBF) is proposed as a common pathway for pathogenesis of retinitis pigmentosa (RP). The current study evaluated the safety and efficacy of ophthalmic nerve stimulation (ONS) as an OBF neuromodulator, combined with ascorbic acid (AA) as a potent anti-oxidant in treatment of RP. Additionally, the initial characteristics of rod responders were identified. Forty participants with simple RP, were enrolled in a prospective open-label intervention. The severity of the disease was clinically graded into five stages. Patients with established diagnosis of RP; aged ≥ 4 years, with BCVA ≥ 20/400 were included. All participants were daily treated with bilateral ONS sessions combined with systemic AA for two weeks. The primary efficiency endpoint was 6 months’ changes in scotopic vision as measured by a 10-items, 100 points, Low Luminance Questionnaire- (LLQ-10). The secondary efficiency points included best corrected visual acuity (BCVA) and contrast sensitivity (CS). Rod responders were defined by ≥ 25points increment of LLQ-10 score. The results showed that ONS combined with AA treatment significantly improved night vision, BCVA and CS in patients with RP. At 6-month visit, twenty-four (60%) patients were identified as rod responders and 16 (40%) patients were non-responders. The mean change in LLQ-10 score was (46.35 ±16.81) in rod responders versus (4.9 ± 7.6) in non-responders (P < 0.0001). A clinically significant improvement of BCVA (≥0.2 logMAR) and CS (≥0.3 log unit) were demonstrated in 44.4% and 56.1% of eyes of rod responders respectively. Collectively, this study sheds light on determinants of rod responsiveness which include patients’ age, duration of night blindness and the stage of RP. It also highlights two therapeutic scenarios; an early disease -modifying intervention that restore night vision and reverse the disease process and a late cone rescue intervention that improve/maintain central vision.
Keywords:
Retinitis pimentosa
; Ocular neuromodulation
; Ophthalmic nerve stimulation
; Ascorbic acid
; night blindness
; Rod responders
1. Introduction
Retinitis pigmentosa (RP) is a group of inherited eye conditions, affecting 1 in 3000 people, with most people becoming legally blind by age of 40s. It is characterized by progressive loss of rods followed by cone photoreceptors death, bone-spicule pigmentation of the retina , optic nerve pallor, attenuated retinal blood vessels and abnormal hemodynamics of the eye [1]. Currently, there is no treatment for RP, apart from Luxturna gene therapy [2], but with limited therapeutic target, since its indication is restricted to group of patients with recessive RPE65 mutation.
RP is not merely caused by genetic factors; in fact, it is a complex multifactorial disorder. Other factors are assumed to contribute to its pathogenesis. Circulatory changes have been observed in the retina and choroid of RP patients, but it has remained unclear whether these play a role in the pathogenesis of the disease. The pulsatile blood flow is significantly reduced in RP patients when compared to healthy volunteers and relative choroidal ischemia is closely associated with visual loss [3]. Furthermore, a study reported a relationship between the choroidal blood flow and reduced focal electroretinography responses [4]. Retinal blood flow is also significantly decreased in RP, probably as a result of vascular remodeling in response to reduced metabolic demand [5]. The ocular blood flow (OBF) is reduced not only in the retina and choroid but also in the retro-ocular vessels [4,6]. Interestingly, signs of reduced OBF have been observed before the appearance of any of fundoscopic features of RP [7]. It has been suggested that vascular dysregulation might play a primary role in pathogenesis of RP [1]. The mechanisms responsible for reduced dysregulated OBF in RP patients are uncertain. It is also uncertain if OBF decline stems from disturbed neural control of ocular circulation or vascular pathology, or both.
The blood supply to the choroid in mammals arises from the ophthalmic artery via the long and short ciliary arteries. Ophthalmic artery and its main branches are all under both parasympathetic and sympathetic neural control with many also under local trigeminal control [8]. The parasympathetic input has a vasodilatory effect, while sympathetic input has a vasoconstrictor effect [8,9].
Stimulation of sensory afferents from the ophthalmic nerve (V1) results in the activation of three pathways that lead to vasodilatation and increased OBF (Figure 1). The first is activation of trigeminovascular system via antidromic impulse [8,9,10]. The nasociliary nerve, which originates from the V1, contains major vasodilatory innervation [11,12], and its stimulation results in the release of vasoactive neuropeptides from the free nerve endings, such as substance P (SP) and Calcitonin gene-related peptide (CGRP) [13,14]. The second pathway results in parasympathetic vasodilation of the ocular vasculature via interactions with the facial nerve and sphenopalatine ganglion [15,16]. The third is an axon reflex between trigeminal nerve and sphenopalatine ganglion [11]. Consistent with this, stimulation of the V1 in experimental animals was found to increase OBF [17], decrease carotid arterial resistance, [15] along with enhanced uveal release of substance P [18].
Oxidative stress plays a central role in pathogenesis and progression of RP. Anti-oxidant interventions have been reported to substantially delay photoreceptor cell death [19]. Therefore, it reasonable to suggest that high-dose of intravenous AA could be beneficial in RP treatment. Preclinical studies showed that a high-dose of AA can restore vascular endothelial function and prevent microcirculatory flow impairment. AA can retrieve vascular responsiveness to vasoconstrictors and preserve endothelial barrier [20]. Additionally, AA exerts sympatholytic effects via central action [21].
Pathogenesis of RP reflects a summation of primary reduced dysregulated OBF, and consecutive unstable oxygen supply, photoreceptors starvation, oxidative stress and chronic neuro-inflammation of the retina. These vascular and cellular processes are ultimately combined to produce rods followed by cones apoptosis. It is our suggestion that hypoxia and starvation of photoreceptors caused by reduced dysregulated OBF represents an initial common pathway in pathogenesis of RP, which can be a target for a novel therapeutic strategy that might halt rods and cones degeneration. Because of complexity of RP, it is unlikely that optimal protection of the rods and cones in the outer retina can be achieved through a single therapy, suggesting that an alternative approach based on combination therapy to be considered. Here we report the safety and efficacy results of ONS paired with systemic ascorbate for treating participants with RP. Additionally, baseline predictive factors for responsiveness to this novel treatment were also defined.
2. Materials and Methods
Forty participants (76 eyes) with RP were recruited into a prospective, open-label interventional study, conducted at Musallam Eye Centers, Palestinian Authority. This study was approved by the Institutional Review Board, and it adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants after explanation of the purpose and possible outcome of therapy.
Following recruitment, all subjects with medical history and established diagnosis of RP completed baseline vision testing, slit lamp examination and fundoscopy. Optical coherence tomography angiography (OCTA) was performed within 2-4 weeks’ prior treatment. The severity of the disease was clinically graded into five stages based on fundoscopy and OCTA findings (Table 1). Inclusion criteria were: patients with established diagnosis of non-syndromic RP; aged ≥ 4 years, with BCVA ≥ 20/400. Exclusion criteria were pregnancy, glaucoma, CRVO and retinal detachment.
To evaluate the therapy outcome, LLQ-10 score changes from baseline to 6 months after treatment were calculated (The primary efficacy endpoint). The LLQ-32 was developed originally for the evaluation of patients with age-related macular degeneration [22]. We have modified such a validated LLQ-32 into a shorter version LLQ-10 (Table 2). LLQ-10 has been used to quantify the participant’s visual dysfunction under low luminance, integrating aspects of visual acuity, mobility, visual field, depth of perception, reading, color vision, dependency on others help, social functions and mental health. Patient-centered outcome measures have been increasingly viewed as necessary in clinical trials, serving as primary endpoints [23,24,25]. Participants rated how much difficulty they have performing each of the activities under low luminance on a 5-point Likert scale. Rod responders were identified as those in whom LLQ-10 score increased by ≥25 points at 6 months after treatment.
The secondary efficiency points include best corrected visual acuity (BCVA) and contrast sensitivity (CS). BCVA was recorded in Snellen equivalents and then transformed to logMAR unit. CS was measured using Pelli- Robson chart under standardized photopic illumination at one meter in each eye, using best correction spectacles. For safety purposes, the vital signs and ECG were monitored before, during and after each session of ocular neuromodulation (ONM). Ocular and non-ocular adverse events were also reported.
ONM protocol included the administration of AA followed by ONS over a period of two weeks. AA was given intravenously in a dose of 3 gm dissolved in 100 ml of saline infused at 5 ml min−1 for 20 min in the first day, followed by a drip infusion of 1 g daily during the rest of the treatment period.
A modulated low magnitude, low frequency vibration, with a frequency of approximately 60 Hz- 90 Hz and stimulation amplitude range of 1.5 μm- 3.5 μm were used for ONS. Modulated frequency and amplitude waveforms were used to avoid adaptation to mechanical stimulus. A hand held and head mounted prototypes of ophthalmic nerve stimulators was applied to different application sites (Figure 2) by using modified commercially available micro-vibrators, along with different types of intranasal and extra-nasal application heads.
Bilateral ONS was applied to the subjects over a session of 30 minutes per day, 6 sessions per week and one day off. Each session included intra-nasal vibrochemical, and extra-nasal vibrotactile stimulation over the nasal bridge and the supraorbital region in both sides (Figure 2A), using appropriate application heads. During intra-nasal vibrochemical stimulation, the nasal application head was covered by rubber cape impregnated by 2% menthol cream (Dermacool plus R) as a transient receptor potential cation channel subfamily M (melastatin) member 8 (TRPM8) agonist. Participants were assessed clinically, and by OCTA, and ILQ-10 at baseline and at 1, 6, 12 and 24 months after treatment.
3. Statistical analysis
The statistical analysis was performed using SPSSR, V. 21. The mean differences in the characteristics of the rod responders and non-responders and the mean change in different parameters of visual functions were compared using the independent sample t-test. The change in visual functions parameters between baseline and different post treatment points were evaluated using paired sample t-test.
Multivariate logistic regression was performed to study the factors that independently predict rod response and to control for confounding factors including age, duration of night blindness, stage of the disease and BCVA at baseline. All tests were two tailed and a p value less than 0.05 was considered significant.
4. Results
Between April 14, 2018 and April 29, 2020, 40 participants (76 eyes) were recruited. The demographics and baseline characteristics of whole cohort are presented in Table 3.
The night vision score in whole cohort improved significantly from (23.1 ± 13.0) at baseline to (55.1 ± 28.6 (p=0.0001) at one month, (52.8 ± 27.2) (p= 0.0001) at 6 months, (52.9 ± 27.4) (p=0.0001) at 12 months and to a value of (56.5 ± 28.0) (p=0.0001) at 24 months after treatment. Twenty-four (60%) patients were identified as rod responders and 16 (40%) patients were non-responders. Figure 3A shows (mean ± SD) of the night vision score as measured by LLQ-10 at each post-treatment visits compared to the baseline in rod responders and non-responders’ groups separately. In rod responders, the night vision score improved significantly from (23.6 ± 11.6) at baseline to (73.5 ± 16.6) (p=0.0001) at one month, (70.0 ± 16.2) (p=0.0001) at 6 months, (69.7 ± 20.5) (p=0.0001) at 12 months and to a value of (68.9 ± 23.7) (p= 0.0001) at 24 months after treatment.
At 6-month visit, the night vision was significantly improved in the whole cohort by (29.8 ±24.7) points as compared to baseline (P < 0.0001). The mean change in LLQ-10 score was (46.35 ±16.81) in rod responders versus (4.9 ± 7.6) in non-responders (p=0.0001). Level 1 and level 2 of scotopic vision were achieved in 12 (38.7%) and 16 (51.6%) patients of rod responders respectively. The rod responders were found to be statistically significantly younger (23.92 ± 12.24 vs 35.06 ± 14.34 yrs) (p=0.01) , with better BCVA (0.45± 0.33 vs 0.71 ± 0.35 Log MAR) (P=0.002) and CS (0.57± 0.50 vs 0.22 ± 0.35) (p=0.001) at baseline. Additionally, the central retina (CRT) (237.2 ± 72.27 µ vs 191.00 ± 76.52 µ) (p=0.01) and ganglion cell layer (GCL) (66.20 ± 16.23 µ vs 49.56 ± 12.29 µ) (p=0.0001) were significantly thicker when compared to non-responders (Table 2). In contrast, relatively thick nerve fiber layer was present in both rod responders and non-responders (42.62 ± 12.15 µ vs 42.86 ± 8.24 µ) (p=0.93; NS) reflecting the chronic nature of neuroinflammation of the retina.
When the stage of disease is considered, all patients with stage 2 (9 patients), 80% patients with stage 3 (12/15) were rod responders. In contrast, only 18% (2/11) of patients with stage 4 were rod responders. Interestingly, in stage 5, the only patient who respond to treatment has central type of RP
Interestingly there is a negative correlation between the duration of night blindness and rod responsiveness. (Figure 1 and Table 2). 81.25% (13/16) of patients who experienced night blindness for 10 years or less were found rod responders. In contrast, only 28.57% (4/14) and 10% (1/10) of patients with >10-20 and >20years of night blindness were found rod responders.
The mean value of BCVA (LogMar) in whole cohort improved significantly from (0.55 ± 0.36) at baseline to (0.34 ± 0.30) (p=0.0001) at one month, (0.39 ± 0.31) (p= 0.0001) at 6 months, (0.43 ± 0.34) (p=0.0001) at 12 months and to a value of (0.43 ± 0.33) log Mar unit (p=0.04) at 24 months after treatment. In rod responders, the mean value of BCVA was significantly improved at all post-treatment visits when compared to baseline. It improved from (0.45 ± 0.33) at baseline to (0.22 ±0.24) (p=0.0001) at one month, (0.23 ± 0.23) (p= 0.0001) at 6 months, (0.30 ± 0.25) (p=0.0001) at 12 months and to a value of (0.33 ± 0.26) log Mar unit (p=0.005) at 24 months after treatment. In contrast, mean BCVA in non-responders was only improved at one (p=0.0001) and 6 months (p= 0.009) after treatment. Figure 3B shows mean change in BCVA at each post-treatment visits compared to the baseline in rod responders and non-responders’ groups. At six months’ visit, a clinically significant improvement of BCVA (improvement of ≥0.2 logMAR, was demonstrated in 44.4% of the eyes of rod responders versus 32 % of eyes of non-responders, but this difference was not statistically significant.
The mean value of CS (Log) in whole cohort improved significantly from (0.42 ± 0.47) at baseline to (0.67 ± 0.53) (p=0.0001) at one month, (0.63 ± 0.53) (p= 0.0001) at 6 months, (0.68 ± 0.54) (p=0.0001) at 12 months and to a value of (0.68 ± 0.51) log unit (p=0.01) at 24 months after treatment. The mean value of CS (Log) in rod responders improved significantly from (0.56 ± 0.50) at baseline to (0.88 ± 0.44) (p=0.0001) at one month, (0.84 ± 0.47) (p= 0.0001) at 6 months, (0.89 ± 0.47) (p=0.0001) at 12 months and to a value of (0.82 ± 0.45) log unit (p=0.03) at 24 months after treatment. The mean changes in CS in rod non-responders were also significantly improved in all post-treatment intervals except at 24 months’ visit. When the mean change in contrast sensitivity is considered, the rod responders showed higher improvement of CS compared to rod non responders (0.32± 0.3 vs 0.16 ± 0.2) (p=0.01) at one month, (0.27±0.26 vs 0.11 ± 0.19) (p=0.004) at 6 months and (0.31 ± 0.35 vs 0.11 ±0.23) log units (p=0.03) at 12 months but no significant difference was found at 24 months. Additionally, at 6 months’ visit, there was a statistically significant difference in the proportion of eyes that showed a clinically significant improvement of CS among the rod responders compared to non- responders (p < 0.002). 56.1% of the eyes of rod responders and 20% of eyes of non-responders had a clinically significant improvement of CS (improvement of ≥0.3 log unit).
Clinically significant regression was noticed in 6 (11.8%) patients 6-12 months. At 24 months’ visit, 20 out of 22 of participants (91%) showed signs of visual regression that justify re-treatment. No serious adverse effects were reported and headache in 5 patients was the only encountered side effect in this study.
Discussion
The current study reported a successful use of ONM as a novel treatment for RP that was previously considered incurable. It has led to a clinically meaningful and statistically significant improvements in visual functions including navigation under low illumination condition, BCVA and CS. We have identified patient characteristics that may predict positive response to treatment. These include younger age, early stage of the disease, and short duration of night blindness at baseline. Additionally, central retinal thickness and ganglion cell layer thickness at baseline, OCT biomarkers, were associated with rod responsiveness.
In this study we found that the most robust improvement in visual function for the subjects with early stages of the disease was night vision as measured by LLQ-10. The process of rod cells apoptosis occurs over years [26], suggesting that there was a much wider window of opportunity for applying ONM for the early rod related stage of RP. Recovery of night vision was likely to be related to reactivation of dormant/starving rods via enhanced oxygen and glucose delivery and shunting metabolites toward aerobic glucose metabolism [27]. A recent study has demonstrated a protective effect of restored glucose transport to mutant rods in RP [28].
In RP, reduced dysregulated OBF, progressive retinal vessel attenuation and reduction of vessel density, along with alteration of the foveal avascular zone have been reported in several studies [1,3,4,5,6,29]. Early development of annular scotoma at the mid-periphery opposite the choroidal watershed zone between the anterior and posterior ciliary arteries [30], supports the notion that photoreceptors damage is primarily of vascular origin. Nevertheless, the unmet oxygen and glucose requirements of mutant rods might be triggering factors for the disease process in RP.
BCVA and CS were not the primary targets of this rod-mediated disease. Nevertheless, the VA and CS were significantly improved. This improvement was maintained for months after treatment. (Figure 3B and Figure 3C). We propose that the reversal of cone dormancy via modulation of OBF might increase the density of functioning cones in the fovea and decrease intercone spacing thereby improving VA and CS. Restoration of glucose delivery to starving cones was found effective in reversal of a state of dormancy in these photoreceptors [27,31].
In normal retina, the action of various proangiogenic factors is in balance with the action of endogenous antiangiogenic factors. There is considerable evidence that VEGF A is a prime regulator of angiogenesis [32]. Pigment epithelium–derived factor, thrombospondin 1, angiostatin, and endostatin, has been identified as endogenous antiangiogenic factors [33,34,35]. In patients with RP, the concentration of VEGF-A in aqueous humors is lower than in non-RP subjects [36] and its level decreases with disease progression [37]. By attempting to redress this imbalance, it might be possible to normalize retinal vessels. One validated mechanism of vascular normalization is enhancement of VEGF signaling. It has been demonstrated that VEGF and VEGF receptors are present in the trigeminal ganglia [38]. Additionally, the angiogenic effect of indirect activation of vagus nerve [39,40] via its neuronal connection with ophthalmic neve might play a role [41,42,43]. We thus hypothesized that ONS promoted angiogenesis of the retina through increasing both VEGF-A and VEGF-B levels in the retina. Sensory neurons of V1 might also promote angiogenesis of the retina via SP signaling in response to antidromic ONS [44]. SP can induce enhancement of migration, proliferation, differentiation of endothelial cells, [45] and recruitment of circulating angiogenic cells and endogenous stem cells to injury site [46,47]. On the other hand; the application of Low-Magnitude Low-Frequency Vibrations on peri-orbital cranial bone induces expression of SDF1, which might be involved in recruitment of endogenous mesenchymal stem cells (MSCs) to the diseased retina [48]. Interestingly, the human cranial bone marrow MSCs have shown greater tendency to differentiate into neuron-like cells than the MSCs derived from iliac crest [49]. Taken together ONS might induce vascular normalization through restoring equilibrium between pro and antiangiogenic activity or enhancement of angiogenic activity via expression of VEGF and SP. Our primary impression indicated that the appearance of a normalized vascular phenotype of the retina (Figure 4) can only be achieved when ONM is applied at the earliest possible time before irreversible vascular remodeling of the retina occurs (vascular normalization window).
Neuroinflammation is a key component of neurodegenerative processes affecting the retina, and thus constitutes a promising target for treatment of RP [50]. Thickening of NFL seen in our study and other studies [51] might be attributed to neuroinflammation of the retina [52]. The specific molecular anti-inflammatory events that occur in the retina as a result of ONM therapy remain to be established. One possible explanation for reduction in inflammation is improved ocular hemodynamics which results in attenuation of retinal hypoxia and ischemia at the cellular level [53]. Significant reduction of TNF-α and IL-6 levels in response to ONS has also been reported [53]. Additionally, the anti-inflammatory effect of indirect activation of vagus nerve via its neuronal connection with ophthalmic neve could not be ruled out [41,42,43]. On the other hand, neuroinflammation of the retina and subsequent cone damage are mediated at least in part by oxidative stress [54]. AA is highly concentrated in the retina [55,56]. Supraphysiological doses of ascorbate have anti-inflammatory effects; hence it is an extremely effective antioxidant and plays a central role in the regulation of intracellular redox state. AA has also sympatholytic effects and has shown to be efficient in improving the endothelium-dependent vasodilatation by restoring nitric oxide activity [57].
Previous clinical studies have evaluated the effect of electrical stimulation on RP [58,59,60]. These studies have made use of a range of electrical stimulation settings, as well as several stimulation sites including transcorneal, transdermal and transorbital electrical stimulation but with limited improvement of vision [58,59,60]. This probably related to poor spatial resolution of electrical stimuli, the site of stimulation and the late timing of intervention. Additionally, electrical stimulation has to deal with multiple challenges, including patient pain, and stimulation induced local inflammatory response. On the other hand, vibro-chemical ONS is emerging as an exciting and might be more advantageous alternative to traditional electrical stimulation. It is proved to be safe, effective and it might provide a long-lasting method for modification of neural circuit of the ocular circulation via external stimulation. Vibrotactile/ Vibro-chemical ONS has the potential of up-regulation of ocular parasympathetic system and trigeminovascular system [9,61,62]. It can selectively activate SP-containing afferents fibers of V1. Co-localization of SP, and TRPM8 in the slowly adapting nociceptive C fibers and mechanoreceptor Aδ fibers of V1 provide an ideal opportunity for selective activation of SP containing neurons. This was achieved by using vibrotactile stimulation and chemical stimulation via TRPM8 agonist (menthol) [63]. Expression of SP in response to ONS may have both neuroprotective and neuro-regenerative effects upon the photoreceptors and other retinal cells via a wide range of effects. These include augmentation of OBF [8,9,17], retinal pigment epithelium proliferation [64], prevention of apoptosis [65] induction of regeneration by the recruitment of endogenous stem cells [46] and suppression of neuroinflammation [66].
Intranasal pathway as a site for vibrochemical ONS has many advantages which include the presence of plenty of mechanoreceptors and chemoreceptors distributed in a specific manner in the nasal mucosa as shown by electrophysiological studies [67]. The nasal vestibule is innervated by branches of nasociliary nerve which contains major vasodilatory innervation [11,12], that contain higher amounts of vasoactive neuropeptides, such as SP and CGRP [13,14]. Administration of vibrochemical stimulation intra- nasally is ideal as it is located closer to the all-important targets to be stimulated. This include anterior ethmoid nerve, sphenopalatine ganglion, and mid-brain area where much of the autonomic functions lie.
Glutamate is the main excitatory neurotransmitter in the retina [68]. It has been also implicated in retrograde signaling [69]. Glutamate could be involved in differential stimulation of the retina, offering more naturalistic vision [70]. Therefore, expressed glutamate in response to ONS may contribute to rapidly improved visual functions noticed immediately after treatment. Furthermore, the neuromodulatory effects of ONS on rod and cone functions appear to be long-lasting. This is likely related to glutamate mediated modulation of existing neuronal circuitry and secondary formation of new permanent neuronal connections in the retina and the visual pathway [71]. Thus, the term neuronal plasticity, which traditionally refers to long lasting changes in neuronal structure and function, would be applicable.
In this study, two therapeutic scenarios of ONM have been recognized; an early disease -modifying intervention that might prevent or reverse the disease process and a late cone rescue intervention that aims to improve/maintain central vision (Figure 5). The maximum net benefit of the early disease modifying intervention is anticipated when ONM is applied at the earliest possible timeframe. Since the affected individuals benefit from the intervention before any significant loss to rods, which contain rod-derived cone viability factor , an essential factor for cone survival [72].
Our results showed that the onset of therapeutic effects of ONM appears within days after treatment, while the peak of its action was reached after 2 weeks. The duration of action of ONM therapy on visual functions was maintained up to 24 months in rod responders (Figure 3). Nevertheless, the long-term follow up indicated that ONM would lose some of its efficacy at some point. Therefore, follow up and re-treatment are mandatory to achieve efficacy, such that the visual improvements are maintained and effects do not diminish over time. It is interesting to note that re-treatment courses of ONM appear to be effective in restoring vision achieved by the primary treatment.
At 6-months, the LLQ-10 score was significantly improved in the whole cohort by 29.6% out of a maximum of 100 points as compared to baseline (P < 0.0001). Similarly, at 6 and 12 months after intervention by gene therapy for patients with RPE65-mediated RP, the mean value of scotopic vision improved by 22.5% as judged by the multi-luminance mobility test (MLMT) [2]. Therefore, vision improvement under low luminance is almost equal in both therapeutic strategies. This comparison, however, is not valid as the MLMT was designed to evaluate the mobility of individual under artificial environment with different illumination levels, whereas the LLQ-10, subjectively evaluate different aspects of daily life under low luminance from patient’s perspectives.
The interpretation of study findings should be considered within the context of few limitations. These include lack of information regarding the genotype, electrophysiology of the retina and OBF measurement. There were no controls, as a placebo group for vibrotactile/vibrochemical ONS was not practical. It is plausible that placebo mechanisms may contribute to short, but not long-term improvement of BCVA. Additionally, remarkable improvement of night vision in patients with early stages of the disease argues against placebo effect.
In conclusion, this study introduces vibrochemical ONS as a novel noninvasive method for treatment of RP, a disease that currently has no treatment. It demonstrates the efficacy and safety of ONM as a universal treatment for different types of RP irrespective of their genetic background. The neuroprotective effects of ONM therapy are probably mediated by modification of the neural circuit of the ocular circulation. Our study provides support for a neuromodulation-based approach to treatment of acute or chronic retinal disorders of vascular origin.
Patents
Ismail Musallam has a pending US and Israeli patents licensed to himself for which he has waived financial interest.
Funding
none.
Acknowledgments
The authors gratefully acknowledge Nurse Tahani Qahooq for her assistance.
Conflicts of Interest
Ismail Musallam has a pending US and Israeli patents licensed to himself for which he has waived financial interest.
References
- Konieczka, K.; Flammer, A.J.; Todorova, M.; Meyer, P.; Flammer, J. Retinitis pigmentosa and ocular blood flow. EPMA J. 2012, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.; Bennett, J.; Wellman, J.A.; Chung, D.C.; Yu, Z.F.; Tillman, A.; et al. Efficacy and safety of voretigene neparvovec (AAV2-hRPE65v2) in patients with RPE65-mediated inherited retinal dystrophy: a randomised, controlled, open-label, phase 3 trial. Lancet (London, England). 2017, 390, 849–860. [Google Scholar] [CrossRef]
- Langham, M.E.; Kramer, T. Decreased choroidal blood flow associated with retinitis pigmentosa. Eye (London, England). 1990, 4 Pt 2, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Falsini, B.; Anselmi, G.M.; Marangoni, D.; D'Esposito, F.; Fadda, A.; Di Renzo, A.; et al. Subfoveal choroidal blood flow and central retinal function in retinitis pigmentosa. Investigative ophthalmology & visual science. 2011, 52, 1064–1069. [Google Scholar]
- Grunwald, J.E.; Maguire, A.M.; Dupont, J. Retinal hemodynamics in retinitis pigmentosa. American journal of ophthalmology. 1996, 122, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Cellini, M.; Strobbe, E.; Gizzi, C.; Campos, E.C. ET-1 plasma levels and ocular blood flow in retinitis pigmentosa. Canadian journal of physiology and pharmacology. 2010, 88, 630–635. [Google Scholar] [CrossRef]
- Wolf, S.; Pöstgens, H.; Bertram, B.; Schulte, K.; Teping, C.; Reim, M. [Hemodynamic findings in patients with retinitis pigmentosa]. Klinische Monatsblatter fur Augenheilkunde. 1991, 199, 325–329. [Google Scholar] [CrossRef]
- Reiner, A.; Fitzgerald, M.E.C.; Del Mar, N.; Li, C. Neural control of choroidal blood flow. Progress in retinal and eye research. 2018, 64, 96–130. [Google Scholar] [CrossRef]
- McDougal, D.H.; Gamlin, P.D. Autonomic control of the eye. Comprehensive Physiology. 2015, 5, 439–473. [Google Scholar]
- Goadsby, P.J.; Edvinsson, L.; Ekman, R. Release of vasoactive peptides in the extracerebral circulation of humans and the cat during activation of the trigeminovascular system. Annals of neurology. 1988, 23, 193–196. [Google Scholar] [CrossRef]
- Suzuki, N.; Hardebo, J.E.; Owman, C. Trigeminal fibre collaterals storing substance P and calcitonin gene-related peptide associate with ganglion cells containing choline acetyltransferase and vasoactive intestinal polypeptide in the sphenopalatine ganglion of the rat. An axon reflex modulating parasympathetic ganglionic activity? Neuroscience. 1989, 30, 595–604. [Google Scholar] [PubMed]
- Hosaka, F.; Yamamoto, M.; Cho, K.H.; Jang, H.S.; Murakami, G.; Abe, S. Human nasociliary nerve with special reference to its unique parasympathetic cutaneous innervation. Anatomy & cell biology. 2016, 49, 132–137. [Google Scholar]
- Suzuki, N.; Hardebo, J.E.; Owman, C. Origins and pathways of cerebrovascular nerves storing substance P and calcitonin gene-related peptide in rat. Neuroscience. 1989, 31, 427–438. [Google Scholar] [CrossRef]
- Atalay, B.; Bolay, H.; Dalkara, T.; Soylemezoglu, F.; Oge, K.; Ozcan, O.E. Transcorneal stimulation of trigeminal nerve afferents to increase cerebral blood flow in rats with cerebral vasospasm: a noninvasive method to activate the trigeminovascular reflex. Journal of neurosurgery. 2002, 97, 1179–1183. [Google Scholar] [CrossRef] [PubMed]
- Lambert, G.A.; Bogduk, N.; Goadsby, P.J.; Duckworth, J.W.; Lance, J.W. Decreased carotid arterial resistance in cats in response to trigeminal stimulation. Journal of neurosurgery. 1984, 61, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Edvinsson, L. The trigeminovascular system and migraine: studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Annals of neurology. 1993, 33, 48–56. [Google Scholar] [CrossRef]
- Stjernschantz, J.; Geijer, C.; Bill, A. Electrical stimulation of the fifth cranial nerve in rabbits: effects on ocular blood flow, extravascular albumin content and intraocular pressure. Experimental eye research. 1979, 28, 229–238. [Google Scholar] [CrossRef]
- Bill, A.; Nilsson, S.F. Control of ocular blood flow. Journal of cardiovascular pharmacology. 1985, 7 (Suppl. 3), S96–102. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Iftikhar, M.; Hafiz, G.; Akhlaq, A.; Tsai, G.; Wehling, D.; et al. Oral N-acetylcysteine improves cone function in retinitis pigmentosa patients in phase I trial. The Journal of clinical investigation. 2020, 130, 1527–1541. [Google Scholar] [CrossRef]
- Oudemans-van Straaten, H.M.; Spoelstra-de Man, A.M.; de Waard, M.C. Vitamin C revisited. Critical care (London, England). 2014, 18, 460. [Google Scholar] [CrossRef]
- Bruno, R.M.; Daghini, E.; Ghiadoni, L.; Sudano, I.; Rugani, I.; Varanini, M.; et al. Effect of acute administration of vitamin C on muscle sympathetic activity, cardiac sympathovagal balance, and baroreflex sensitivity in hypertensive patients. The American journal of clinical nutrition. 2012, 96, 302–308. [Google Scholar] [CrossRef]
- Owsley, C.; McGwin, G.; Jr Scilley, K.; Kallies, K. Development of a questionnaire to assess vision problems under low luminance in age-related maculopathy. Investigative ophthalmology & visual science. 2006, 47, 528–535. [Google Scholar]
- Guidance for industry: patient-reported outcome measures: use in medical product development to support labeling claims: draft guidance. Health and quality of life outcomes. 2006, 4, 79. [CrossRef]
- Heneghan, C.; Goldacre, B.; Mahtani, K.R. Why clinical trial outcomes fail to translate into benefits for patients. Trials. 2017, 18, 122. [Google Scholar] [CrossRef] [PubMed]
- Weldring, T.; Smith, S.M. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health services insights. 2013, 6, 61–68. [Google Scholar] [CrossRef]
- Li, Z.Y.; Kljavin, I.J.; Milam, A.H. Rod photoreceptor neurite sprouting in retinitis pigmentosa. The Journal of neuroscience : the official journal of the Society for Neuroscience. 1995, 15, 5429–5438. [Google Scholar] [CrossRef]
- Wang, W.; Lee, S.J.; Scott, P.A.; Lu, X.; Emery, D.; Liu, Y.; et al. Two-Step Reactivation of Dormant Cones in Retinitis Pigmentosa. Cell reports. 2016, 15, 372–385. [Google Scholar] [CrossRef]
- Wang, W.; Kini, A.; Wang, Y.; Liu, T.; Chen, Y.; Vukmanic, E.; et al. Metabolic Deregulation of the Blood-Outer Retinal Barrier in Retinitis Pigmentosa. Cell reports. 2019, 28, 1323–1334. [Google Scholar] [CrossRef] [PubMed]
- Toto, L.; Borrelli, E.; Mastropasqua, R.; Senatore, A.; Di Antonio, L.; Di Nicola, M.; et al. Macular Features in Retinitis Pigmentosa: Correlations Among Ganglion Cell Complex Thickness, Capillary Density, and Macular Function. Investigative ophthalmology & visual science. 2016, 57, 6360–6366. [Google Scholar]
- Hayreh, S.S. In vivo choroidal circulation and its watershed zones. Eye (London, England). 1990, 4 Pt 2, 273–289. [Google Scholar] [CrossRef]
- Punzo, C.; Kornacker, K.; Cepko, C.L. Stimulation of the insulin/mTOR pathway delays cone death in a mouse model of retinitis pigmentosa. Nature neuroscience. 2009, 12, 44–52. [Google Scholar] [CrossRef]
- Ferrara, N. Vascular endothelial growth factor: molecular and biological aspects. Current topics in microbiology and immunology. 1999, 237, 1–30. [Google Scholar] [PubMed]
- Chader, G.J. PEDF: Raising both hopes and questions in controlling angiogenesis. Proceedings of the National Academy of Sciences of the United States of America. 2001, 98, 2122–2124. [Google Scholar] [CrossRef]
- Talks, K.L.; Harris, A.L. Current status of antiangiogenic factors. British journal of haematology. 2000, 109, 477–489. [Google Scholar] [CrossRef]
- Carmeliet, P.; Jain, R.K. Angiogenesis in cancer and other diseases. Nature. 2000, 407, 249–257. [Google Scholar] [CrossRef]
- Salom, D.; Diaz-Llopis, M.; García-Delpech, S.; Udaondo, P.; Sancho-Tello, M.; Romero, F.J. Aqueous humor levels of vascular endothelial growth factor in retinitis pigmentosa. Investigative ophthalmology & visual science. 2008, 49, 3499–3502. [Google Scholar]
- Cellini, M.; Santiago, L.; Versura, P.; Caramazza, R. Plasma levels of endothelin-1 in retinitis pigmentosa. Ophthalmologica Journal international d'ophtalmologie International journal of ophthalmology Zeitschrift fur Augenheilkunde. 2002, 216, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.Q.; Zhang, M.; Matis, K.I.; Kim, C.; Rosenblatt, M.I. Vascular endothelial growth factor mediates corneal nerve repair. Investigative ophthalmology & visual science. 2008, 49, 3870–3878. [Google Scholar]
- Lv, Y.X.; Zhong, S.; Tang, H.; Luo, B.; Chen, S.J.; Chen, L.; et al. VEGF-A and VEGF-B Coordinate the Arteriogenesis to Repair the Infarcted Heart with Vagus Nerve Stimulation. Cellular physiology and biochemistry : international journal of experimental cellular physiology, biochemistry, and pharmacology. 2018, 48, 433–449. [Google Scholar] [CrossRef]
- Luo, B.; Wu, Y.; Liu, S.L.; Li, X.Y.; Zhu, H.R.; Zhang, L.; et al. Vagus nerve stimulation optimized cardiomyocyte phenotype, sarcomere organization and energy metabolism in infarcted heart through FoxO3A-VEGF signaling. Cell death & disease. 2020, 11, 971. [Google Scholar]
- Rogers, R.C.; Kita, H.; Butcher, L.L.; Novin, D. Afferent projections to the dorsal motor nucleus of the vagus. Brain research bulletin. 1980, 5, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Borovikova, L.V.; Ivanova, S.; Zhang, M.; Yang, H.; Botchkina, G.I.; Watkins, L.R.; et al. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature. 2000, 405, 458–462. [Google Scholar] [CrossRef]
- Wasilczuk, K.M.; Bayer, K.C.; Somann, J.P.; Albors, G.O.; Sturgis, J.; Lyle, L.T.; et al. Modulating the Inflammatory Reflex in Rats Using Low-Intensity Focused Ultrasound Stimulation of the Vagus Nerve. Ultrasound in medicine & biology. 2019, 45, 481–489. [Google Scholar]
- Liu, L.; Dana, R.; Yin, J. Sensory neurons directly promote angiogenesis in response to inflammation via substance P signaling. FASEB journal : official publication of the Federation of American Societies for Experimental Biology. 2020, 34, 6229–6243. [Google Scholar] [CrossRef] [PubMed]
- Ziche, M.; Morbidelli, L.; Pacini, M.; Geppetti, P.; Alessandri, G.; Maggi, C.A. Substance P stimulates neovascularization in vivo and proliferation of cultured endothelial cells. Microvascular research. 1990, 40, 264–278. [Google Scholar] [CrossRef]
- Kim, J.H.; Jung, Y.; Kim, B.S.; Kim, S.H. Stem cell recruitment and angiogenesis of neuropeptide substance P coupled with self-assembling peptide nanofiber in a mouse hind limb ischemia model. Biomaterials. 2013, 34, 1657–1668. [Google Scholar] [CrossRef]
- Kohara, H.; Tajima, S.; Yamamoto, M.; Tabata, Y. Angiogenesis induced by controlled release of neuropeptide substance P. Biomaterials. 2010, 31, 8617–8625. [Google Scholar] [CrossRef]
- Wei, F.Y.; Chow, S.K.; Leung, K.S.; Qin, J.; Guo, A.; Yu, O.L.; et al. Low-magnitude high-frequency vibration enhanced mesenchymal stem cell recruitment in osteoporotic fracture healing through the SDF-1/CXCR4 pathway. European cells & materials. 2016, 31, 341–354. [Google Scholar]
- Shinagawa, K.; Mitsuhara, T.; Okazaki, T.; Takeda, M.; Yamaguchi, S.; Magaki, T.; et al. The characteristics of human cranial bone marrow mesenchymal stem cells. Neuroscience letters. 2015, 606, 161–166. [Google Scholar] [CrossRef]
- Yoshida, N.; Ikeda, Y.; Notomi, S.; Ishikawa, K.; Murakami, Y.; Hisatomi, T.; et al. Laboratory evidence of sustained chronic inflammatory reaction in retinitis pigmentosa. Ophthalmology. 2013, 120, e5–e12. [Google Scholar] [CrossRef]
- Xue, K.; Wang, M.; Chen, J.; Huang, X.; Xu, G. Retinal nerve fiber layer analysis with scanning laser polarimetry and RTVue-OCT in patients of retinitis pigmentosa. Ophthalmologica Journal international d'ophtalmologie International journal of ophthalmology Zeitschrift fur Augenheilkunde. 2013, 229, 38–42. [Google Scholar] [CrossRef] [PubMed]
- García-Ayuso, D.; Di Pierdomenico, J.; Vidal-Sanz, M.; Villegas-Pérez, M.P. Retinal Ganglion Cell Death as a Late Remodeling Effect of Photoreceptor Degeneration. International journal of molecular sciences. 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Chiluwal, A.; Afridi, A.; Chaung, W.; Powell, K.; Yang, W.L.; et al. Trigeminal Nerve Stimulation: A Novel Method of Resuscitation for Hemorrhagic Shock. Critical care medicine. 2019, 47, e478–e84. [Google Scholar] [CrossRef] [PubMed]
- Komeima, K.; Rogers, B.S.; Lu, L.; Campochiaro, P.A. Antioxidants reduce cone cell death in a model of retinitis pigmentosa. Proceedings of the National Academy of Sciences of the United States of America. 2006, 103, 11300–11305. [Google Scholar] [CrossRef]
- Rose, R.C.; Bode, A.M. Ocular ascorbate transport and metabolism. Comparative biochemistry and physiology A, Comparative physiology. 1991, 100, 273–285. [Google Scholar] [CrossRef]
- Hosoya, K.; Minamizono, A.; Katayama, K.; Terasaki, T.; Tomi, M. Vitamin C transport in oxidized form across the rat blood-retinal barrier. Investigative ophthalmology & visual science. 2004, 45, 1232–1239. [Google Scholar]
- Taddei, S.; Virdis, A.; Ghiadoni, L.; Magagna, A.; Salvetti, A. Vitamin C improves endothelium-dependent vasodilation by restoring nitric oxide activity in essential hypertension. Circulation. 1998, 97, 2222–2229. [Google Scholar] [CrossRef]
- Jolly, J.K.; Wagner, S.K.; Martus, P.; MacLaren, R.E.; Wilhelm, B.; Webster, A.R.; et al. Transcorneal Electrical Stimulation for the Treatment of Retinitis Pigmentosa: A Multicenter Safety Study of the OkuStim® System (TESOLA-Study). Ophthalmic research. 2020, 63, 234–243. [Google Scholar] [CrossRef]
- Miura, G.; Sugawara, T.; Kawasaki, Y.; Tatsumi, T.; Nizawa, T.; Baba, T.; et al. Clinical Trial to Evaluate Safety and Efficacy of Transdermal Electrical Stimulation on Visual Functions of Patients with Retinitis Pigmentosa. Scientific reports. 2019, 9, 11668. [Google Scholar] [CrossRef]
- de Rossi, F.; Guidobaldi, M.; Turco, S.; Amore, F. Transorbital electrical stimulation in retinitis pigmentosa. Better results joining visual pattern stimulation? Brain stimulation. 2020, 13, 1173–1174. [Google Scholar] [CrossRef]
- Reiner, A.; Fitzgerald, M.C. CL Neural Control of Ocular Blood Flow. Editors. Ocular Blood Flow. Berlin Heidelberge:springer; 2012.
- Hiraba, H.; Inoue, M.; Gora, K.; Sato, T.; Nishimura, S.; Yamaoka, M.; et al. Facial vibrotactile stimulation activates the parasympathetic nervous system: study of salivary secretion, heart rate, pupillary reflex, and functional near-infrared spectroscopy activity. BioMed research international. 2014, 2014, 910812. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.Y.; Kim, J.H.; Cho, Y.S.; Mah, W.; Bae, Y.C. Quantitative analysis of afferents expressing substance P, calcitonin gene-related peptide, isolectin B4, neurofilament 200, and Peripherin in the sensory root of the rat trigeminal ganglion. The Journal of comparative neurology. 2015, 523, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.S.; Kim, S.; Nam, S.; Um, J.; Kim, Y.H.; Son, Y. Effect of substance P on recovery from laser-induced retinal degeneration. Wound repair and regeneration : official publication of the Wound Healing Society [and] the European Tissue Repair Society. 2015, 23, 268–277. [Google Scholar] [CrossRef]
- Backman, L.J.; Eriksson, D.E.; Danielson, P. Substance P reduces TNF-α-induced apoptosis in human tenocytes through NK-1 receptor stimulation. British journal of sports medicine. 2014, 48, 1414–1420. [Google Scholar] [CrossRef] [PubMed]
- Yoo, K.; Son, B.K.; Kim, S.; Son, Y.; Yu, S.-Y.; Hong, H.S. Substance P prevents development of proliferative vitreoretinopathy in mice by modulating TNF-α. Mol Vis. 2017, 23, 933–943. [Google Scholar]
- Scheibe, M.; van Thriel, C.; Hummel, T. Responses to trigeminal irritants at different locations of the human nasal mucosa. The Laryngoscope. 2008, 118, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Kalloniatis, M.; Tomisich, G. Amino acid neurochemistry of the vertebrate retina. Progress in retinal and eye research. 1999, 18, 811–866. [Google Scholar] [CrossRef]
- Zilberter, Y.; Harkany, T.; Holmgren, C.D. Dendritic release of retrograde messengers controls synaptic transmission in local neocortical networks. The Neuroscientist : a review journal bringing neurobiology, neurology and psychiatry. 2005, 11, 334–344. [Google Scholar] [CrossRef]
- Rountree, C.M.; Inayat, S.; Troy, J.B.; Saggere, L. Differential stimulation of the retina with subretinally injected exogenous neurotransmitter: A biomimetic alternative to electrical stimulation. Scientific reports. 2016, 6, 38505. [Google Scholar] [CrossRef]
- Mattson, M.P. Glutamate and neurotrophic factors in neuronal plasticity and disease. Annals of the New York Academy of Sciences. 2008, 1144, 97–112. [Google Scholar] [CrossRef] [PubMed]
- Aït-Ali, N.; Fridlich, R.; Millet-Puel, G.; Clérin, E.; Delalande, F.; Jaillard, C.; et al. Rod-derived cone viability factor promotes cone survival by stimulating aerobic glycolysis. Cell. 2015, 161, 817–832. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic of neural pathways that control ocular blood flow (OBF). SNS; sympathetic nervous system, PNS; parasympathetic nervous system, TVS: trigemino-vascular system, TG: Trigeminal Ganglion, PPG: pterygopalatine ganglion, SSN: superior salivatory nucleus, SCG: superior cervical ganglion, RVLM: rostro-ventrolateral medulla, SP: substance P, CGRP; calcitonin gene-related peptide, Ach: acetylcholine, NO: nitric oxide, VAP: vasoactive intestinal polypeptide, NA: Noradrenaline, NPY; neuropeptide Y.
Figure 1.
Schematic of neural pathways that control ocular blood flow (OBF). SNS; sympathetic nervous system, PNS; parasympathetic nervous system, TVS: trigemino-vascular system, TG: Trigeminal Ganglion, PPG: pterygopalatine ganglion, SSN: superior salivatory nucleus, SCG: superior cervical ganglion, RVLM: rostro-ventrolateral medulla, SP: substance P, CGRP; calcitonin gene-related peptide, Ach: acetylcholine, NO: nitric oxide, VAP: vasoactive intestinal polypeptide, NA: Noradrenaline, NPY; neuropeptide Y.
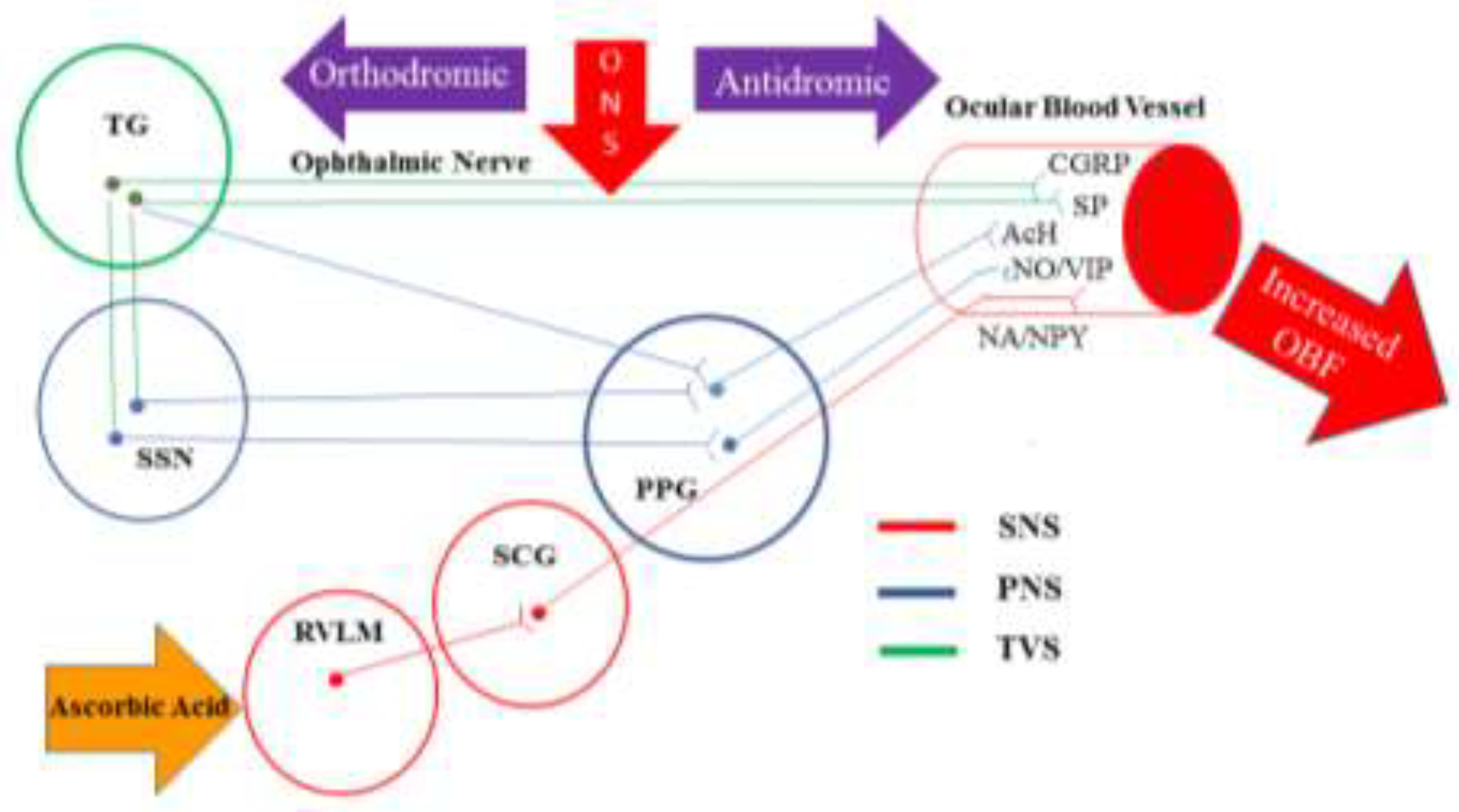
Figure 2.
(A) Sites of ONS; (1) Intranasal: for stimulation of anterior ethmoid nerve at the nasal septum, (2) Nasal bridge: for stimulation of infratrochlear nerve, a branch of nasociliary nerve and external nasal nerve, the terminal branch of external branch of anterior ethmoid nerve, (3) Supraorbital region: for stimulation of supraorbital and supratrochlear nerve, branches of frontal nerve. (B) Handheld vibrotactile ophthalmic nerve stimulator. An intranasal application head is designed to be small enough to fit comfortably and safely within the restricted size of the nasal vestibule and optionally made by polyethyl methacrylate to prevent the warming produced by the vibration. (C) Head mounted vibrotactile ophthalmic nerve stimulator with two application heads over the supraorbital region in both sides.
Figure 2.
(A) Sites of ONS; (1) Intranasal: for stimulation of anterior ethmoid nerve at the nasal septum, (2) Nasal bridge: for stimulation of infratrochlear nerve, a branch of nasociliary nerve and external nasal nerve, the terminal branch of external branch of anterior ethmoid nerve, (3) Supraorbital region: for stimulation of supraorbital and supratrochlear nerve, branches of frontal nerve. (B) Handheld vibrotactile ophthalmic nerve stimulator. An intranasal application head is designed to be small enough to fit comfortably and safely within the restricted size of the nasal vestibule and optionally made by polyethyl methacrylate to prevent the warming produced by the vibration. (C) Head mounted vibrotactile ophthalmic nerve stimulator with two application heads over the supraorbital region in both sides.
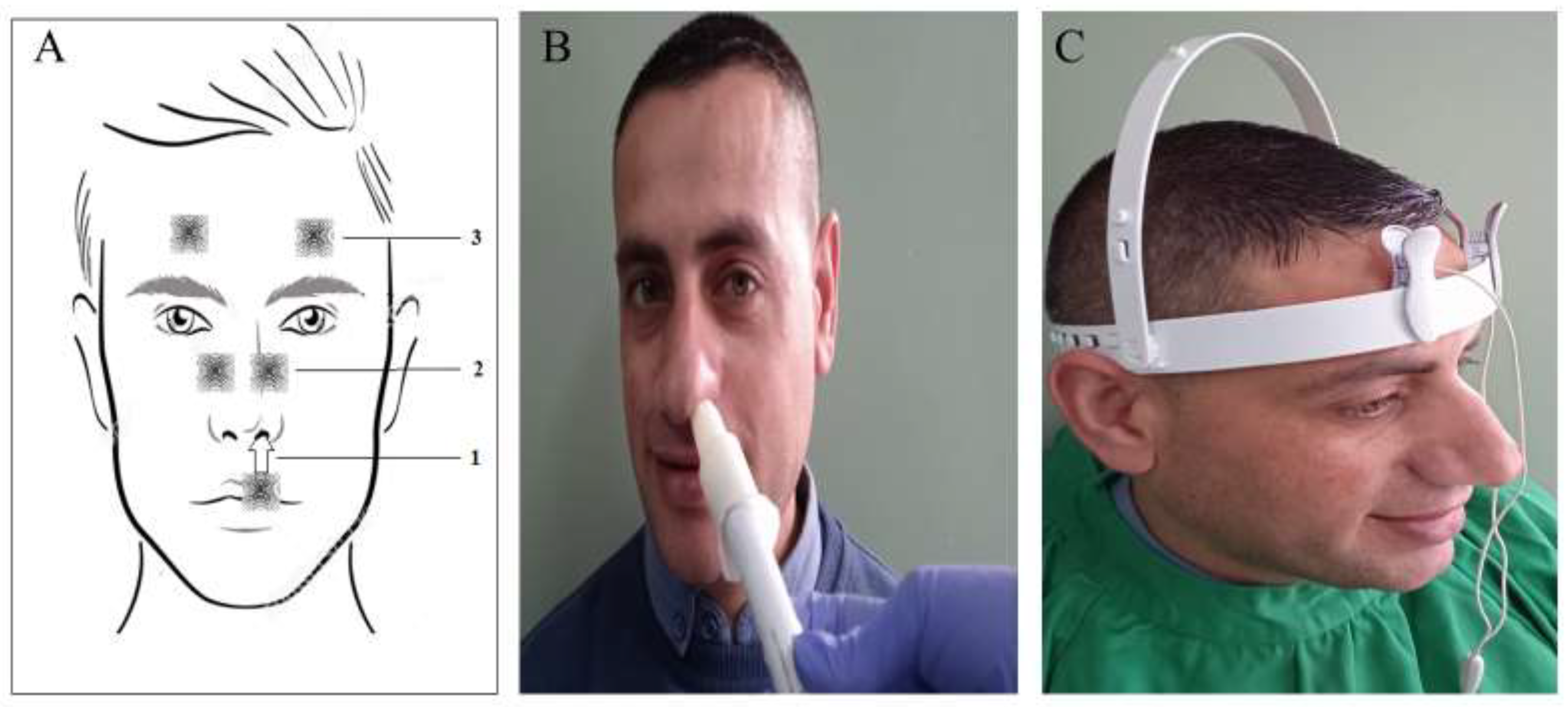
Figure 3.
Changes in visual functions and predictors for rod responders in study participants: (A) Mean value of LLQ-10 score among rod-responders and non-responders at baseline and at post-treatment visits. (B) Mean change (LogMAR) in best corrected visual acuity (BCVA. (C) Mean change in (Log unit) in contrast sensitivity (CS). (D) Distribution of rod responders based on the stage of the disease. (E) Distribution of rod responders according to the duration of night blindness. Responders are shown in blue bare. None-responders in red bare. The number of rod responders and non-responders are included in the graph. (E) Proportion (%) of eyes that showed a clinically significant improvement of BCVA and CS in the rod responders versus non- responders.
Figure 3.
Changes in visual functions and predictors for rod responders in study participants: (A) Mean value of LLQ-10 score among rod-responders and non-responders at baseline and at post-treatment visits. (B) Mean change (LogMAR) in best corrected visual acuity (BCVA. (C) Mean change in (Log unit) in contrast sensitivity (CS). (D) Distribution of rod responders based on the stage of the disease. (E) Distribution of rod responders according to the duration of night blindness. Responders are shown in blue bare. None-responders in red bare. The number of rod responders and non-responders are included in the graph. (E) Proportion (%) of eyes that showed a clinically significant improvement of BCVA and CS in the rod responders versus non- responders.
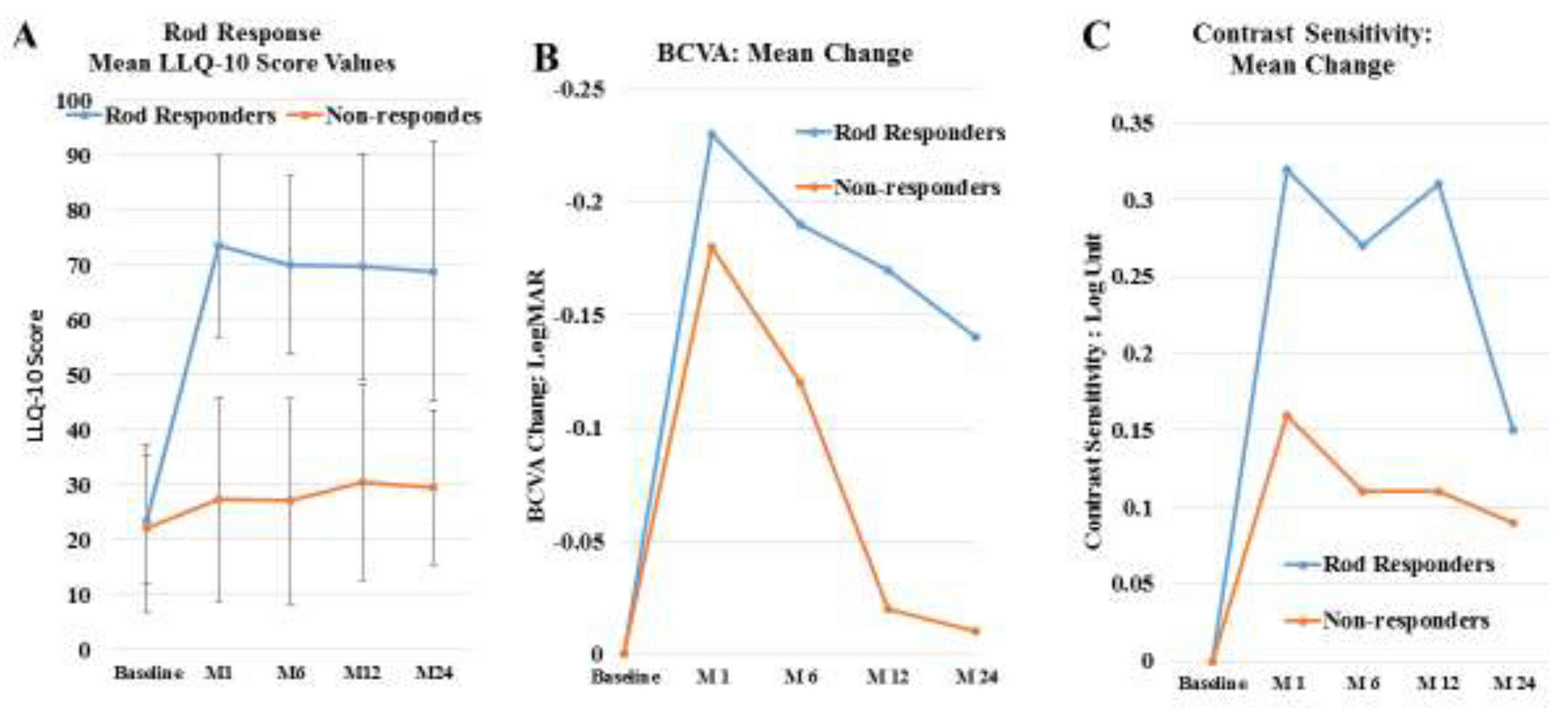
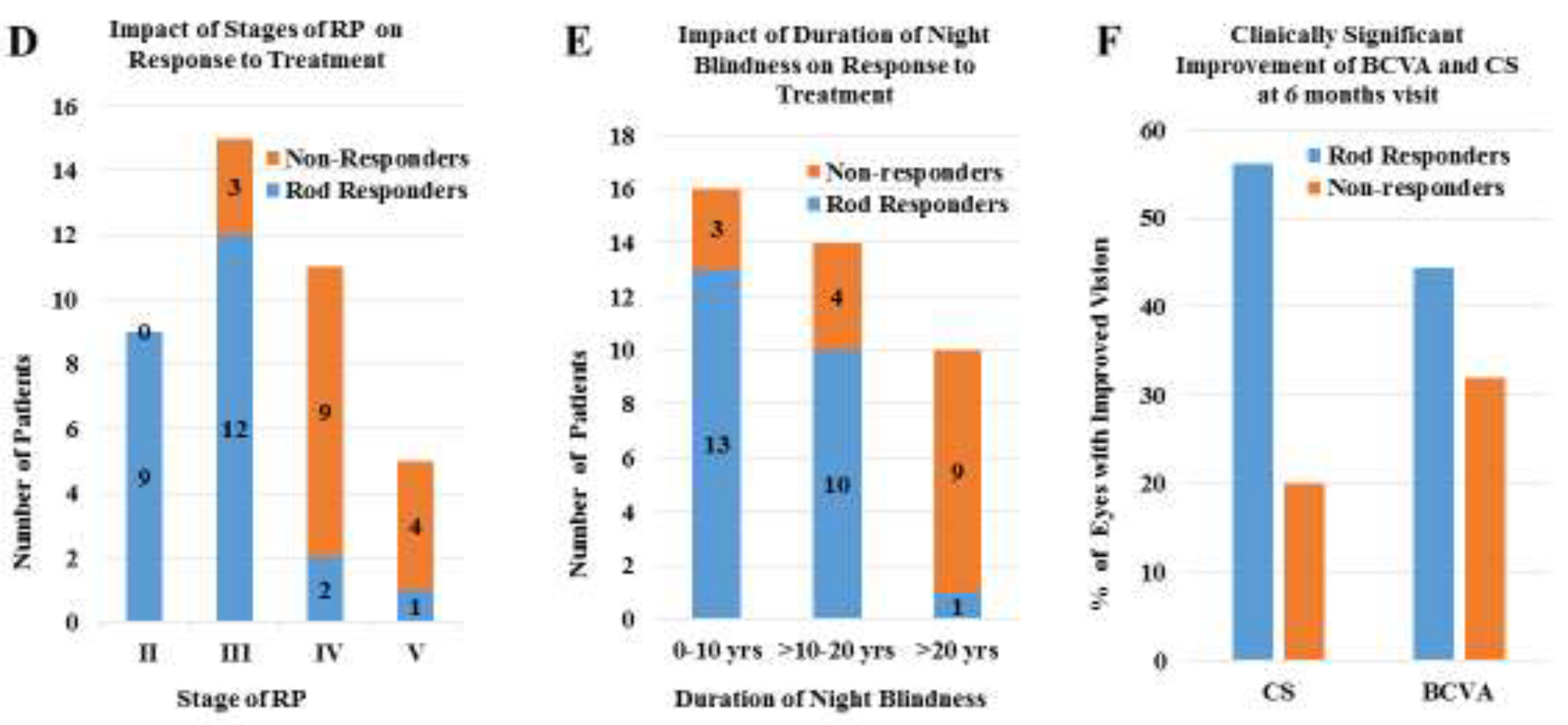
Figure 4.
OCT angio of OD and OS at Baseline and 26 months after ocular neuromodulation therapy. The vascular density increased significantly and enlarged foveal avascular zoon return to normal size at 26 months after ONS and ascorbic acid treatment.
Figure 4.
OCT angio of OD and OS at Baseline and 26 months after ocular neuromodulation therapy. The vascular density increased significantly and enlarged foveal avascular zoon return to normal size at 26 months after ONS and ascorbic acid treatment.
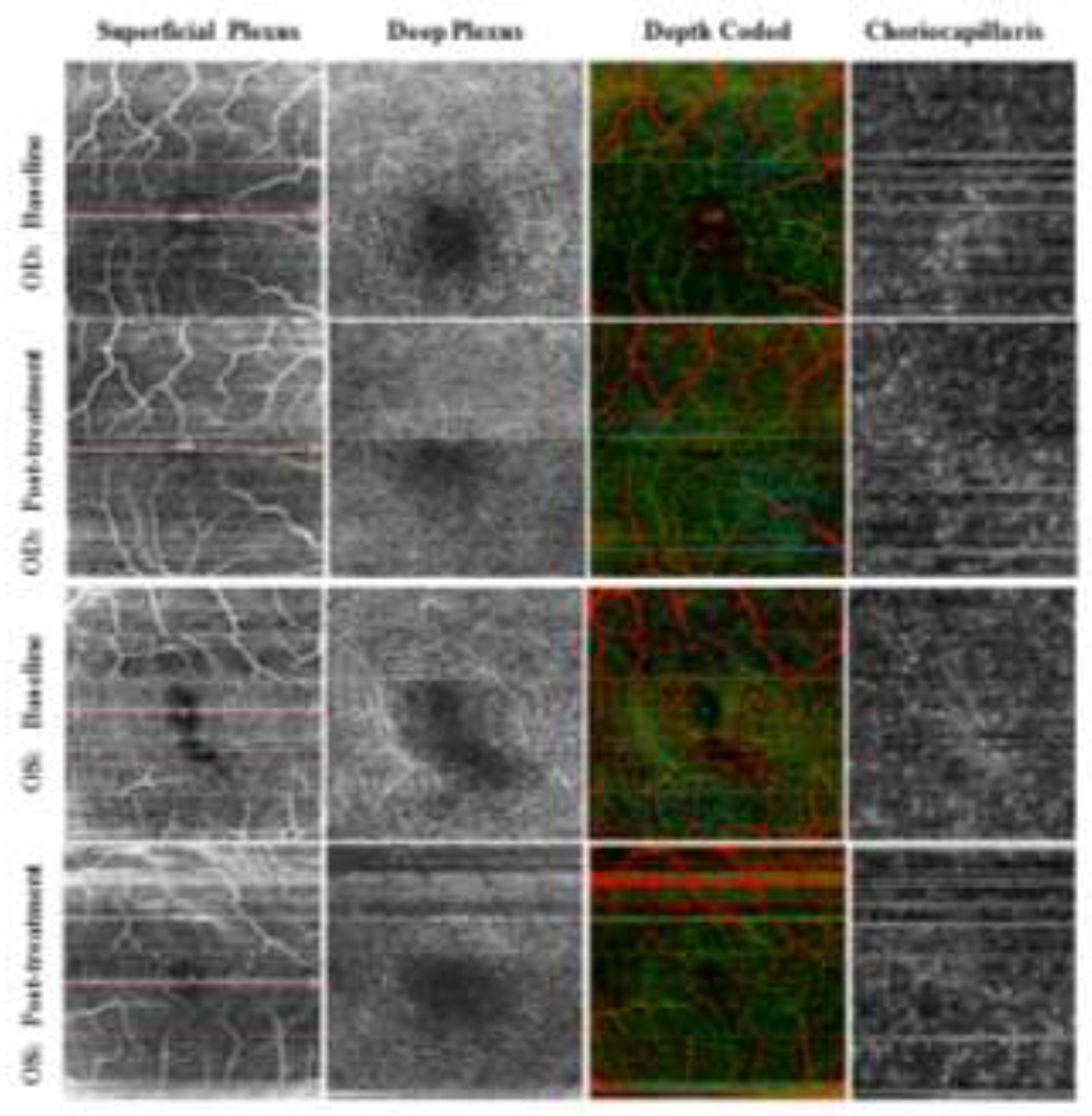
Figure 5.
Photoreceptors degeneration and the effect of ONM therapy on the course of the disease. (A) Natural course of rods (black line) and cones (white line) degeneration in RP. Blue arrow indicates the time of initiation of ONM. (B) and (C) ONM therapy initiated at early rod degeneration phase (stage I and II) respectively. The green line represents an early disease modifying effect of ONM therapy to reverse the disease process via restoration of function of dormant rods. (D) ONM therapy initiated at transitional phase (stage III). The green line represents anticipated modified course of rod and cone photoreceptors. In (E), and (F), the interrupted green line represents a cone rescue strategy wherein ONM therapy is initiated at stage, IV and V respectively (Late cone degeneration phase of RP).
Figure 5.
Photoreceptors degeneration and the effect of ONM therapy on the course of the disease. (A) Natural course of rods (black line) and cones (white line) degeneration in RP. Blue arrow indicates the time of initiation of ONM. (B) and (C) ONM therapy initiated at early rod degeneration phase (stage I and II) respectively. The green line represents an early disease modifying effect of ONM therapy to reverse the disease process via restoration of function of dormant rods. (D) ONM therapy initiated at transitional phase (stage III). The green line represents anticipated modified course of rod and cone photoreceptors. In (E), and (F), the interrupted green line represents a cone rescue strategy wherein ONM therapy is initiated at stage, IV and V respectively (Late cone degeneration phase of RP).
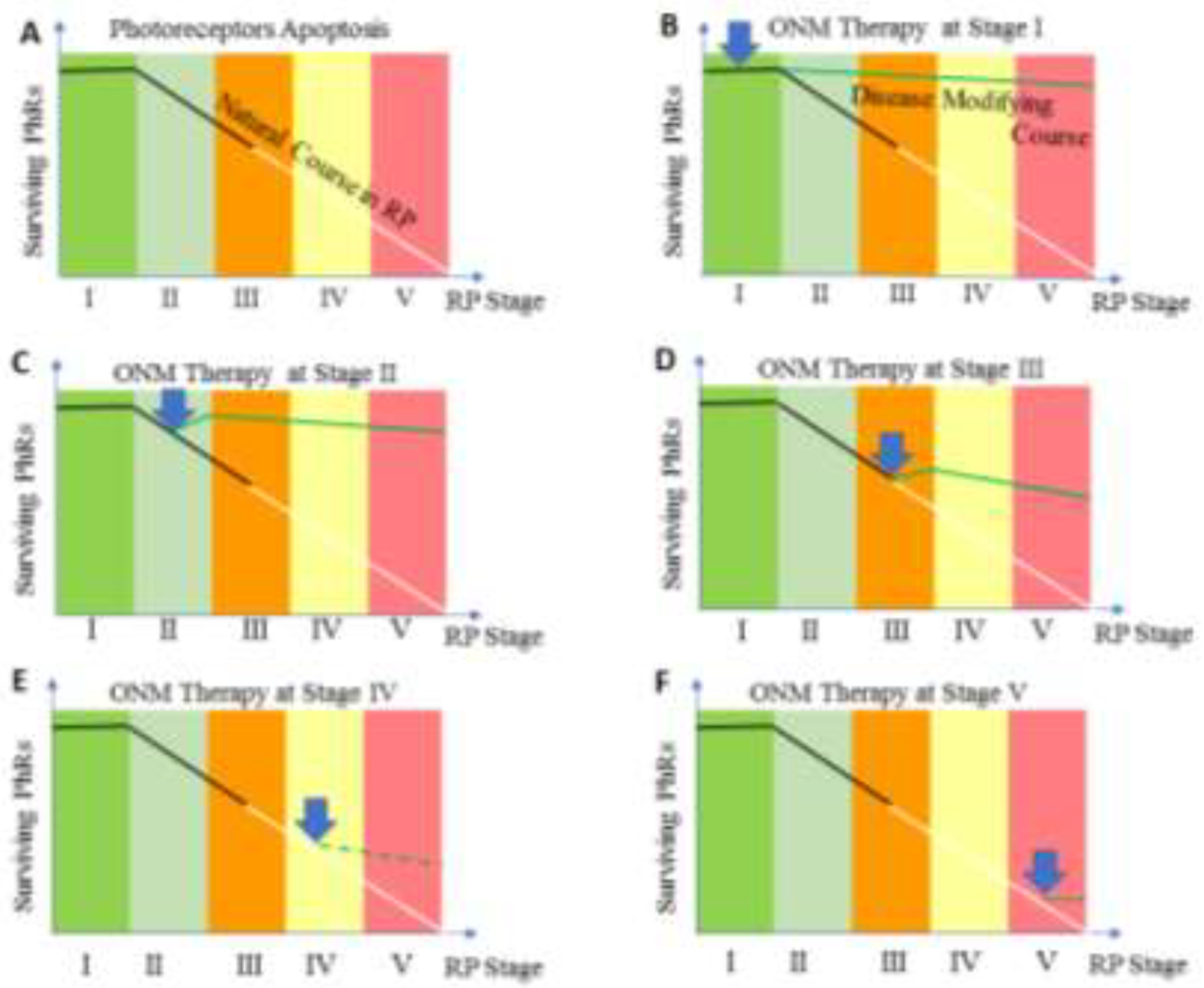

Table 1.
Staging of RP.
| Stage | Clinical Description |
|---|---|
| Stage 1 | Patients may experience mild night vision disturbance. Fundus examination reveals normally looking retina with no pigmentary changes, no visible retinal blood vessels (RBVs) changes, or optic nerve pallor. Positive ERG findings are detected |
| Stage II | Mild to moderate attenuation of RBVs that extend beyond the mid periphery of retina but not reaching ora serrata, no or mild optic disc pallor, bone spicule pigmentary changes are limited to mid-periphery of the retina. |
| Stage III | Moderate to severe attenuation of RBVs that extend up to midperiphery with mild optic nerve pallor. Pigmentary changes are located at mid-periphery and extend centrally reaching the vascular arcade. |
| Stage IV | Severe attenuation of RBVs that ended with formation of a complete vascular arcade, combined with moderate optic nerve pallor. Pigmentary changes are becoming more diffuse and extend centrally to the inside of vascular arcade, but sparing the macula. Central retinal thickness is less than 150 µ as measured by OCTA |
| Stage V | Severe attenuation or complete obliteration of RBVs that ended at a short distance from optic nerve. Optic pallor is remarkable and the macula is involved by pigmentary changes. Stage V is also coined to any retina with central retinal thickness of 100 µ or less as measured by OCTA |
Table 2.
Low Luminance Questionnaire-10 (LLQ-10).
| Q | Subject | Question Text |
|---|---|---|
| 1 | Night Vision | Do you have difficulty seeing at night? |
| 2 | Peripheral vision | Do you have difficulty with your peripheral vision at night? |
| 3 | Reading at dim light | Do you have difficulty reading menus in dimly lit restaurants or reading the newspaper/book without good lighting? |
| 4 | Depth of Perception | Do you have difficulty with depth perception at night? |
| 5 | Color Vision | Do you have difficulty seeing colors at night? |
| 6 | Home life | Do you have difficulty seeing furniture in dimly lit rooms? |
| 7 | Social life | Because of your vision, do you have difficulty going out to nighttime social events such as sport events, the theater, friend’s homes, church, mosque or restaurants? |
| 8 | Parties at dim light | Do you have difficulty seeing in candlelight? |
| 9 | Dependency on others | Do you depend on others to help you because of your vision at night or under poor lighting? |
| 10 | Psychological Stress | Do you worry or are you concerned that you might fall at night because of your vision? |
Scoring Instructions: Each of the 10 questionnaire items should be answered by one of the following: (1) No difficulty at all (10 points). (2) Little difficulty (7.5 points). (3) Some or moderate difficulty. (5 points). (4) A lot of difficulties (2.5 points). (5) Completely blind under these conditions (0 point). The total score on the LLQ-10 is ranged from 0-100, with higher score indicating better vision under low luminance. The scotopic vision difficulties are further classified into four levels of dysfunction according to LLQ-10 score. Level 4; (0-25) which indicates absolute night blindness /Minimal scotopic vison, level 3 severe night blindness (>25-50), level 2; moderate night blindness (>50-75) and level 1 (>75-100) with almost normal scotopic vision. Rod responders were identified as those in whom LLQ-10 score increased by ≥ 25 points at 6 months’ post-treatment.
Table 3.
Demographic, baseline characteristics and determinants of rod responders.
| Total cohort | |
|---|---|
| (40 patients; 76 eye) | |
| Age, Mean ±SD | 28.4 ± 14.1 yrs. |
| 4-52 yrs. | |
| M/F (male %) | 23/17 (57.5%) |
| Inheritance | |
| AR | 21 (52.5%) |
| AD | 2 (5%) |
| Simplex | 17 (42.5%) |
| Rang/ | 2-46 yrs. |
| Mean Duration of night blindness | 16.2 ± 12.3 yrs. |
| Duration | |
| 0-10 yrs. | 16 (40%) |
| >10-20 yrs. | 14 (35%) |
| >20-40 yrs | 10 (25%) |
| Stage of the Disease * | |
| II, no. of patients (%) | 9 (22.5%) |
| III, no. of patients/ (%) | 15 (37.5%) |
| IV, no. of patients (%) | 11 (27.5%) |
| V, no. of patients/ (%) | 5 (12.8%) |
LLQ-10: low luminance questionnaire-10; BCVA: Best corrected visual acuity; CS: contrast sensitivity; CRT: central retinal thickness; NFLT: nerve fiber layer thickness; GCLT: ganglion cell layer thickness, NS (not significant); p value > 0.05. * stage of the disease of the patient is the stage of RP in the better eye.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



