Submitted:
28 September 2023
Posted:
30 September 2023
You are already at the latest version
Abstract
Polycystic ovary syndrome (PCOS) is an insulin resistant state, compensated by hyperinsulinemia. More than 50% of the women with PCOS are obese, and/or have metabolic syndrome. Weight loss improves both metabolic and reproductive outcomes. Not only the energy content, but also the nutrient composition of a diet may be important. This article will present a series of studies from our research comparing effects of dietary protein vs. simple-carbohydrates (CHO). Results of the acute challenge studies demonstrate that simple-CHO intake causes reactive hypoglycemia in one third of the women with PCOS, especially among obese and insulin resistant individuals. Symptoms of hypoglycemia are associated with secretion of cortisol and adrenal androgens. Simple-CHO suppresses the hunger signal ghrelin for a shorter period. During weight loss, women who receive protein supplementation achieve larger amounts of weight- and fat-mass losses. Amino acid compositions of the protein supplements do not affect the improvements in weight and insulin resistance. It is plausible that simple-CHO intake leads to weight gain, or interferes with weight-loss, by causing reactive hypoglycemia, triggering adrenal steroid secretion, and leading to snacking. Since obese women with PCOS are more susceptible to reactive hypoglycemia, a vicious cycle establishes. Restriction of simple-CHO may break this cycle.
Keywords:
reactive hypoglycemia
; postprandial hypoglycemia
; polycystic ovary syndrome
; protein supplements
; whey protein
; weight loss
; adrenal steroids
; ghrelin
1. Introduction
Characteristic features of the polycystic ovary
syndrome (PCOS) include oligomenorrhea/amenorrhea/anovulation,
hyperandrogenemia and cystic ovaries. In addition, women with PCOS have insulin
resistance and hyperinsulinemia even in the absence of obesity. In the USA 69%
of women with PCOS are obese and 64% have metabolic syndrome [1,2]. Weight loss improves both metabolic and
reproductive outcomes in PCOS [3,4,5,6]. Our
earlier research in women without PCOS demonstrated that replacement of dietary
fat with carbohydrates (CHO) can lead to weight loss in free-living conditions [7]. However, those women who did not lose weight on
low-fat/high-CHO diet experienced worsening of the dyslipidemia and increased
inflammatory risk factors [8]. This article
will summarize the results of our nutrition research in women with PCOS.
Potential links between the nutrient composition of the diets and the changes
in anthropometric and metabolic outcomes will be discussed. A unifying
conceptual framework for dietary approach to PCOS will be presented.
A notable finding of our studies was that
simple-CHO intake was associated with reactive hypoglycemia in a significant
number of PCOS patients [9,10] and triggered
adrenal steroid secretion. Hypoglycemia is defined as low blood glucose
concentrations that can cause harm to an individual. Glucose level below 70
mg/dL is considered mild, and below 54 mg/dL is considered serious
hypoglycemia. Mild hypoglycemia leads to adrenergic symptoms such as tremors,
palpitations, sweating, hunger and paresthesia. Serious hypoglycemia causes
additional neuroglycopenic symptoms such as headache, dizziness, confusion,
amnesia, seizure and coma [11].
Hypoglycemia occurring within four hours after a
meal is called reactive or postprandial hypoglycemia [12].
This condition is frequently undermined by the medical community for several
reasons: Hypoglycemic symptoms can occur without biochemical evidence of low
blood glucose. There is no accurate method to diagnose postprandial
hypoglycemia. Oral glucose tolerance test (OGTT) over-estimates the problem
since 10% of the individuals tested with extended (5-hour) OGTT develop blood
glucose below 50 mg/dl. Mixed meal challenge can elicit neuroglycopenic
symptoms in the absence of hypoglycemia. Because of these limitations, reactive
hypoglycemia is considered significant when it develops after bariatric
surgery, significant alcohol intake, or in the rare case of hereditary fructose
intolerance or insulinoma.
- (1)
- Our goal was to determine the optimal diet for weight loss in women with PCOS, and we addressed the following questions:
- (2)
- Does replacement of dietary fat with CHO vs. protein influence the amount of weight loss and body composition?
- (3)
- What are the acute metabolic and endocrine effects of CHO and protein intake in PCOS?
- (4)
- Do amino acid compositions of dietary proteins affect weight-loss and/or insulin resistance?
1.2. Comparing low-fat/high-CHO vs. low-fat/high-protein diets during weight loss in women with PCOS
1.2.1. Acute effects of simple-CHO vs. protein
Thirty-three women who fulfilled the National
Institutes of Health criteria for PCOS participated in this 2-month-long,
free-living, randomized, single-blinded study [13].
To achieve a final energy reduction of 450 kcal/day, the daily energy intake
was reduced by 700 kcal, and a 240-kcal supplement containing either whey
protein (WP) or simple-CHO was added. The powdered supplements contained
either sugar-free WP isolate (96% pure) or simple sugars (glucose plus maltose)
and were packaged in individual, identical-looking pouches to allow blinding.
Because whey is naturally calcium enriched, and calcium can independently
promote weight loss, calcium contents of the supplements were equalized by
adding tricalcium phosphate to the carbohydrate supplement. Whey protein
supplement was sweetened by adding a non-calorie sugar substitute; both
supplements were similarly flavored. Most participants consumed the supplements
as a partial meal replacement for breakfast.
First the effects of oral whey protein (WP) vs.
simple-sugar intakes were examined during 5-hour challenge studies. Even though
WP did not change plasma glucose concentrations (Figure 1A), it increased plasma insulin 5-fold
(Figure 1B), indicating that WP is a
potent insulin secretagogue. Another significant difference was seen in plasma
ghrelin levels. Ghrelin is a gastrointestinal hormone secreted in the stomach
and duodenum. It is a “hunger signal”. It is suppressed by food intake and
rises to signal hunger when the stomach empties. While both simple-sugar and WP
suppressed ghrelin similarly, after the simple-sugar intake ghrelin started to
rise after two hours. Whereas, after WP ghrelin remained suppresses during the
five-hour testing (Figure 1C). This
observation suggested that protein intake may provide satiety for a longer
period as compared to simple-sugar.
1.3. Postprandial hypoglycemia after simple-sugar vs. protein
During the previous studies significant number of
PCOS patients developed the symptoms of hypoglycemia after the simple-sugar
consumption. The next study focused on these symptoms and adrenal function [9]. Since the standard test to evaluate is 5-hour
oral glucose test (OGTT), responses to glucose vs. WP were compared. The
adrenal response was defined based on cortisol changes during OGTT. Those
subjects who had a minimum increase of 7.2 μg/dL (200 nM) in cortisol were
defined as “responders” because such a response is considered positive during Cortrysin
stimulation testing. Nine subjects had a 10.7±1.0 µg/dL increase in cortisol
(responders); 10 subjects had a 3.5±0.6 µg/dL decrease (non-responders); and 11
subjects had an intermediate response of a 4.3±1.0 µg/dL increase (p <
0.0001). The changes in DHEA concentrations followed a similar pattern: Δ =
14.4 ± 1.7 ng/mL in the responders, Δ = 0.4 ± 0.9 ng/mL in the non-responders,
and Δ = 3.6 ± 1.2 ng/mL in the intermediates (P=.0003) (Figure 2A).
Responders had higher glucose at 1 hour (194 ± 13
vs. 131 ± 12 mg/dL, p<.05) but lower nadir glucose later during the
test (61.4 ± 2.2 vs. 70.2 ± 2.3 mg/dL, P=.0002). Responders also had
higher insulin response at 2 hours as compared to non-responders (159 ± 31 vs.
54 ± 29 mU/mL, P<.05) (Figure 2B).
The key clinical symptoms related to the autonomic
response, neuroglycopenia, and malaise (sweating, shaking, hunger, weakness,
confusion, drowsiness, behavior, speech difficulty, incoordination, nausea, and
headache) were monitored using the Hypoglycemia Symptoms Logs program developed
in collaboration with William Horn and Nancy Keim, PhD [9]. The symptoms were recorded hourly on a 0–100
scale on hand-held tablets. The data were transferred from the tablets to an
Excel spreadsheet for analysis and were plotted against time. When responders
were compared to non-responders, the symptoms diverged at 3rd hour.
The responders had higher scores in shakiness, sweatiness, weakness, and hunger
(Figure 2C).
When the baseline characteristics of responders were compared to those of non-responders, the responders were more obese (BMI: 37.0±1.6 vs. 31.7±1.8 kg/m2, p< 0.05) and had higher serum leptin (28.9±1.7 vs. 24.1±1.1 ng/ml, p<0.03). The responders also had lower and sex hormone binding globulin (SHBG) (33.9±3.1 vs. 58.6±6.7 nmol/L, p = 0.022).
These results indicated that one third of the women with PCOS developed physiologically significant reactive hypoglycemia stimulating adrenal steroid secretion. These patients were more obese and insulin resistant as compared to those who did not develop hypoglycemia.
1.4. Effects of dietary CHO vs. protein on anthropometric outcomes during weight loss intervention:
These studies compared the effects of WP vs. simple CHO on the changes in weight and body composition [13]. Twenty-four women who fulfilled the National Institutes of Health criteria for PCOS completed the 2-month, free-living, randomized, single-blinded study. Habitual energy intake was reduced by 700 kcal, and a 240-kcal supplement containing either WP or simple-CHO was added. The final energy restriction was -450 kcal/day. After randomization,13 participants first received the simple-CHO supplement, and 11 participants received the WP-supplement. 7-day food records were analyzed using NutritionistPro (Redmond, WA).
The baseline energy intakes were similar (1947±166 kcal/d in the WP; 1770±157 kcal/d in the simple-CHO groups). Energy intake decreased similarly (by 476 and 400 kcal/day, respectively). Protein intake increased from 20% to 33% in the WP group and decreased from 22% to 17% in the simple-CHO group. Body composition was determined using electrical bioimpedance.
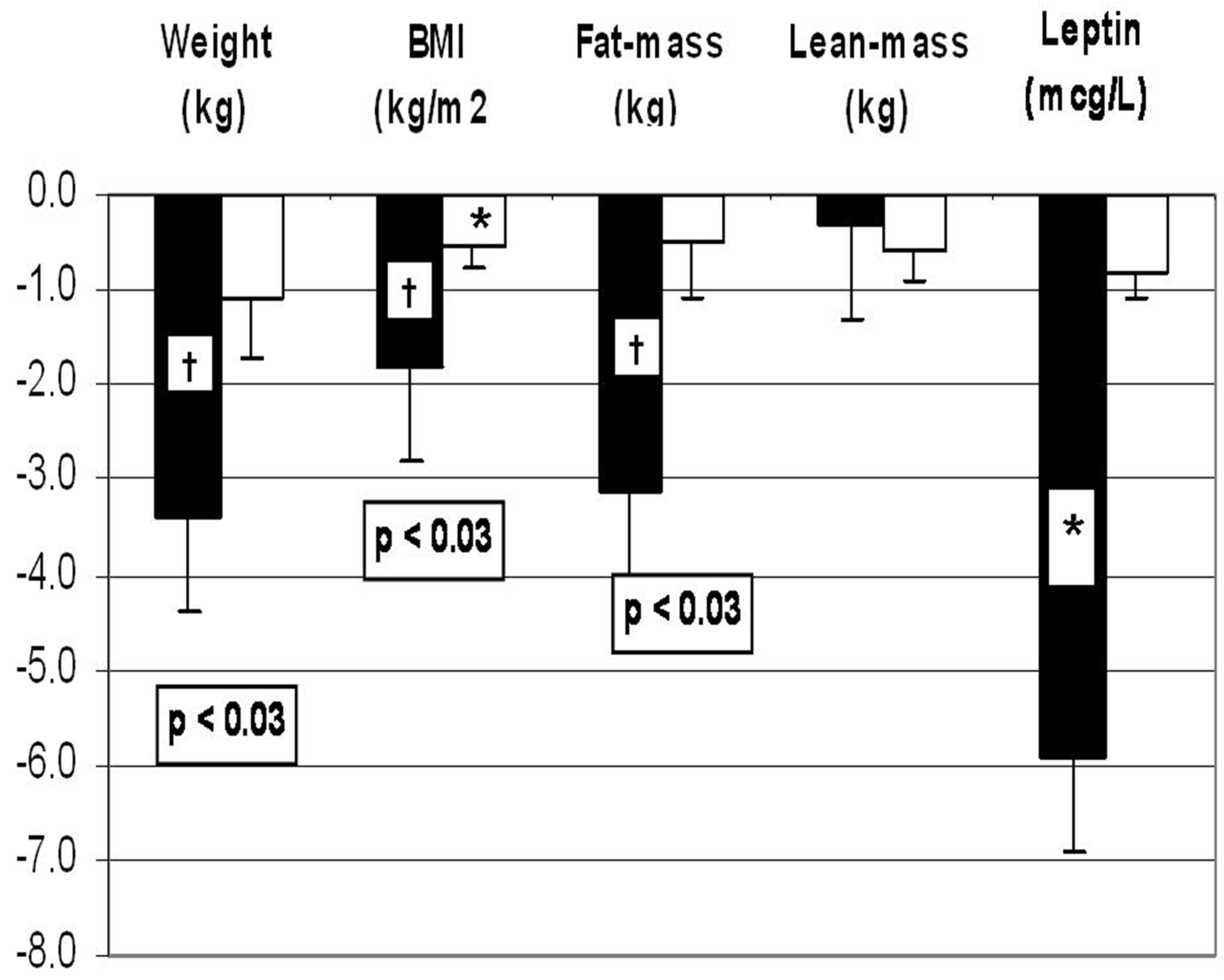
Those receiving WP lost more weight (-3.3 +/- 0.8 kg vs. -1.1 +/- 0.6 kg, p <0.03) and more fat mass (-3.1 +/- 0.9 kg vs. -0.5 +/- 0.6 kg, P< 0.03). Serum leptin was determined as an independent measure of fat mass, and it decreased from 37.2 ± 3.9 µg/L to 31.3 ± 3.4 µg/L in the WP group but did not change in the simple-CHO group (Figure 3).
Whey protein recipients had larger decreases in serum cholesterol (-33.0 +/- 8.4 mg/dL vs. -2.3 +/- 6.8 mg/dL), high-density lipoprotein cholesterol (-4.5 +/- 1.3 mg/dL vs. -0.4 +/- 1.3 mg/dL), and apoprotein B (-20 +/- 5 mg/dL vs. 3 +/- 5 mg/dL) as compared to simple-CHO group as well.
These results indicated that women with PCOS may lose more weight and fat-mass on hypocaloric high-protein diet as compared to high-simple-CHO diet.
1.5. Effects of amino acid composition of dietary protein on weight loss and metabolic parameters in women with PCOS
Whey protein comprises 60% essential amino acids (EAA) and 23% branch-chain amino acids (BCAA) [14]. The literature related measurements of plasma metabolome indicated that plasma BCAA concentrations correlate with insulin resistance [15,16]. Since PCOS and metabolic syndrome are insulin resistant states, it is important to determine whether WP, a rich source of BCAA, can exacerbate insulin resistance. To evaluate this possibility, WP was compared to gelatin (a form of collagen) during weight loss in women with metabolic syndrome. Gelatin differs from WP significantly in its AA content [17]. It is an incomplete protein, missing the essential AA tryptophan, while it is enriched with proline and hydroxyproline. Whey protein contains three times more BCAA as compared to gelatin.
In an 8-wk double-blinded, placebo-controlled, randomized weight-loss intervention, 29 women with metabolic syndrome received either gelatin-based or WP-based supplements (Glanbia, Inc. Twin Falls, ID), 20 g/day. The metabolome of 27 participants (WP: n = 16) and (gelatin: n = 11) were investigated at the beginning and at the end of the intervention using GC-time-of-flight mass spectrometry [18].
Before the intervention, plasma BCAA correlated with homeostasis model assessment of insulin resistance (HOMA) (r = 0.52, 0.43, and 0.49 for Leu, Ile, and Val, respectively; all P < 0.05). However, after the weight-loss intervention these correlations disappeared. There was no difference in plasma abundances (reported as quantifier ion peak height ÷ 100) of BCAA between the WP and gelatin supplementation groups (Ile: Gelatin: 637 ± 18 vs. WP: 744 ± 65), (Leu: Gelatin: 1210 ± 33; WP: 1380 ± 79), and (Val: Gelatin: 2080 ± 59; WP: group: 2510 ± 230).
These findings suggested composition of dietary protein did not affect the anthropometric or metabolic outcomes. Whey protein supplementation did not cause insulin resistance when compared to gelatin. Weight loss was the important determinant of insulin resistance.
2. Discussion and a unifying hypothesis
Our studies indicated that
- One third of the women with PCOS developed physiologically significant reactive hypoglycemia after simple-sugar intake and secreted of cortisol and adrenal androgens.
- Adrenal steroid secretion coincided with the hypoglycemic symptoms.
- Whey protein intake stimulated insulin secretion but did not cause hypoglycemia.
- Whey protein supplement suppressed the hunger signal ghrelin for a longer period as compared to simple-CHO supplement.
- A weight loss diet containing WP supplement was associated with greater weight loss and fat mass loss and decrease in leptin when compared to the diet containing simple-CHO supplement.
- When WP supplement was compared to gelatin supplement, there was no difference in the amount of weight loss or the improvement in insulin sensitivity, despite lower essential AA- and BCAA content of gelatin.
The literature supports that women with PCOS are susceptible to reactive hypoglycemia. Altuntas et al. tested 64 lean subjects with PCOS with extended OGTT and reported prevalence of reactive hypoglycemia as 50% [19]. Mumm et al. compared 88 women with PCOS to 34 age and BMI matched controls using 5-hour OGTT [20]. Seventeen percent of the women with PCOS but none of the controls developed hypoglycemia. Obese women with PCOS who developed reactive hypoglycemia had higher cumulative insulin response as compared to those who did not develop hypoglycemia.
The literature suggests that women with PCOS may respond to hypoglycemia differently than control women. Sam et al. compared 10 women with PCOS to nine age-, BMI- and ethnicity matched controls using hypoglycemic clamp and found that women with PCOS had three-fold higher glucagon response [21]. The other counter-regulatory hormones such as growth hormone or cortisol did not show differential responses. Gennarelli et al. used insulin-induced hypoglycemia to compare the counter regulatory hormones in women with PCOS vs. control women [22]. Obese women with PCOS were less symptomatic and had blunted noradrenaline response as compared to the obese controls. Lean women with PCOS had greater increase in growth hormone as compared to lean controls.
Our studies focused on the clinical presentation of hypoglycemia. We showed that one third of women with PCOS developed hypoglycemic symptoms during the 5-hour OGTT. The symptomatic patients had lower nadir glucose, and secreted cortisol and adrenal androgens during the symptoms. They were also more obese and insulin resistant than the asymptomatic women with PCOS. The link between the hypoglycemic symptoms and the adrenal hormone secretion indicates that the clinical symptoms are important clues pointing to triggering of the adrenals. The link between the hypoglycemic symptoms and obesity suggests that hypoglycemia may alter eating/snacking behavior, as observed by Kishimoto, in men with subclinical hypoglycemia [23].
Since PCOS is an insulin resistant state and a significant number of the patients may have obesity and metabolic syndrome, several studies attempted to identify the optimal diet for weight loss and maintenance in PCOS. We found that a high-protein diet containing WP was superior to a high-CHO diet in achieving weight-loss and fat-mass loss. Studies of plasma metabolome by Ooi et al. showed that branch-chain AA supplementation may increase fat-oxidation [24], offering a potential mechanism for our observation. A meta-analysis including 24 studies by Wycherly et al. compared energy restricted high-protein/low-fat vs. standard-protein weight loss diets and found that high-protein diets caused larger amounts of weight-loss and fat-mass loss and lowered plasma triglycerides more than the standard-protein diets [25]. There were no differences in changes in plasma insulin and other lipids. Even though all these studies included obese, insulin resistant patients, only two focused on PCOS. One of these was our study summarized earlier which found favorable effects of high-protein diet [13]. The other study from Stames et al. did not find any difference between the high protein vs. high-CHO diets [26]. Moran et al. reviewed the results of five studies in 137 women with PCOS [27]. The differences in study populations and dietary interventions did not permit a meta-analysis. It appeared that monounsaturated fat-enriched diet caused greater weight loss. Low-glycemic index and/or low-CHO diets improved menstrual regularity and quality of life, and elicited greater reductions in insulin resistance, fibrinogen, total, and high-density lipoprotein cholesterol [28,29]. High-protein diet improved depression and self-esteem [30], whereas high-CHO diet increased free androgen index. Most importantly, regardless of dietary composition, weight loss improved the presentation of PCOS. Sorensen et al. compared high-protein vs. standard protein diets in a 6-month study in 27 women with PCOS and reported greater weight and fat-mass losses with the high-protein diet [31].
Our initial high-protein weight loss studies used WP supplementation. Whey protein contains high amounts of essential AA and BCAA. Studies of plasma metabolome indicated that plasma BCAA correlated with insulin resistance [16,32]. Therefore, we compared WP to gelatin, a protein which is relatively poor in BCAA content; there was no difference in weight or fat-mass loss, or the change in insulin sensitivity [18]. It appeared that the protein content of the diet but not the AA composition of the protein was the important factor for weight loss.
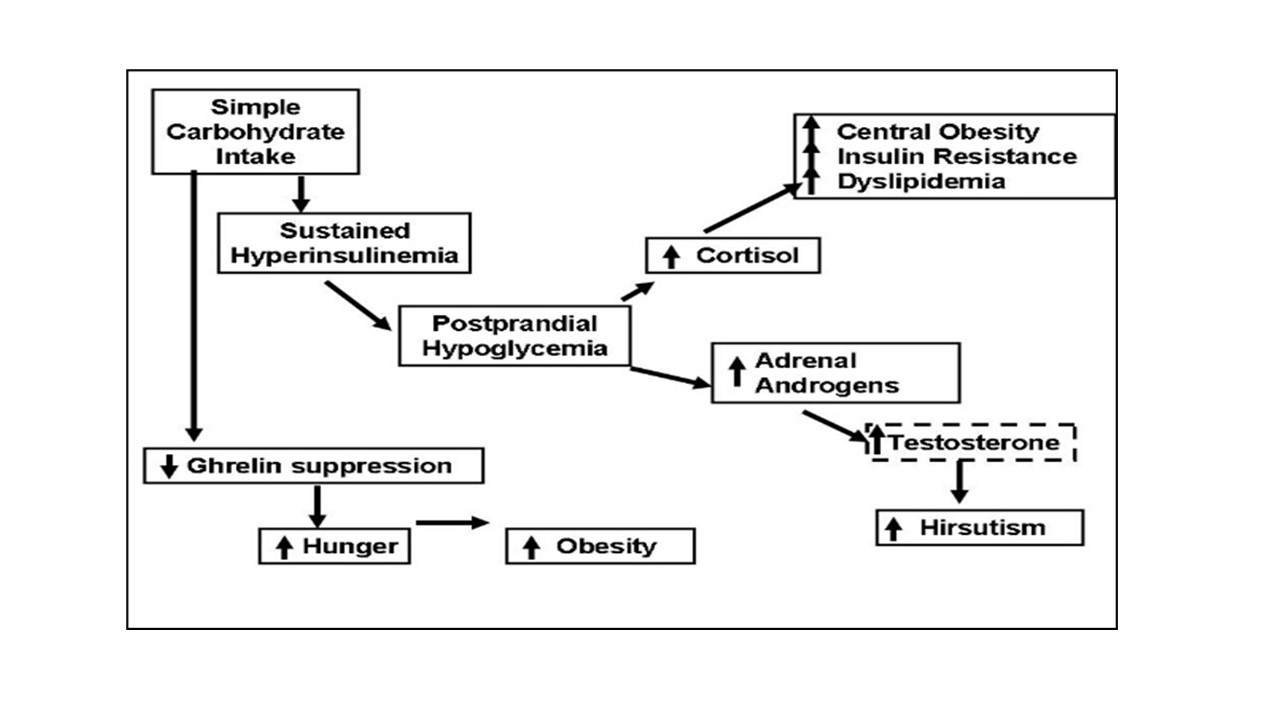
In clinical practice, symptoms suggesting reactive hypoglycemia occur mostly during mid-morning and/or mid-afternoon and may include “getting hungry; craving sugar/carbohydrate”, “losing concentration /getting sleepy”, “developing headaches/sweating”. Typically, these complaints are preceded by a breakfast or a lunch enriched with simple-CHO. Patients attempt to relieve the symptoms by eating CHO-rich snacks. We propose that this frequent snacking behavior contributes to obesity.
Here we present a unifying concept linking simple-CHO intake to reactive hypoglycemia and hunger, which in turn leads to frequent snacking and obesity.
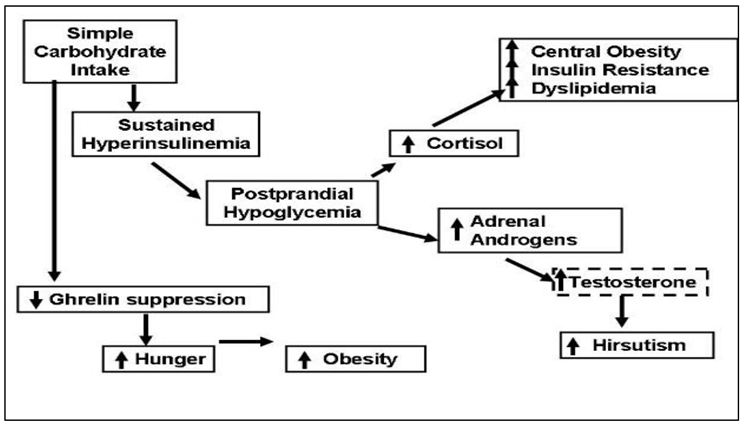
1. Polycystic ovary syndrome is an insulin resistant state, compensated by hyperinsulinemia. Simple -CHO intake results in large amounts of insulin secretion. Insulin levels in the circulation remains elevated after emptying of the stomach and this causes reactive hypoglycemia. Protein intake also stimulates insulin secretion but does not cause hypoglycemia, possibly because protein intake stimulates glucagon which facilitates glycogenolysis in the liver [33]. In addition, amino acids, especially alanine, serve as glucose precursors for gluconeogenesis [34].
2. Reactive hypoglycemia triggers adrenergic response, as evidenced by the symptoms of tremors, sweating, and stimulates steroid hormone secretion from the adrenals. Cortisol causes central fat deposition, insulin resistance and dyslipidemia. This concept is supported by our observation that the women with hypoglycemic symptoms were more obese and insulin resistant. Adrenal androgens convert to testosterone in the peripheral tissues and increase hirsutism. We found that the women with hypoglycemic symptoms had 1.7 times higher testosterone/DHEAS molar ratio as compared to those without hypoglycemic symptoms.
3. Even though protein and CHO are equally effective in suppressing the hunger signal ghrelin, the effect of CHO does not last as long. Moran et al. reported no difference between the suppressive effects of oral protein vs. CHO challenges during a 3-hour test [35]. We saw that suppressive effects of CHO vs. protein intakes differed after the 3rd hour. After protein intake ghrelin remained suppressed for 5 hours; after simple-CHO intake ghrelin started to rise by the 3rd hour and returned to the baseline by the 5th hour.
In summary, the evidence from our research suggests that simple-CHO intake causes reactive hypoglycemia in a significant number of women with PCOS. Reactive hypoglycemia leads to hypoglycemic symptoms and triggers adrenal steroid secretion. In addition, simple-CHO intake suppresses the hunger signal for a short time. All of these factors may encourage snacking between meals and lead to obesity. Since obesity increases the risk of reactive hypoglycemia, a vicious cycle emerges. Limiting simple-CHO intake and increasing protein intake can break this vicious cycle by preventing reactive hypoglycemia and frequent snacking, and consequently may improve the anthropometric, endocrine, and metabolic outcomes in PCOS.
Conflicts of Interest
The author declares no conflict of interest.
References
- Carmina E, Legro RS, Stamets K, Lowell J, and Lobo RA. Difference in body weight between American and Italian women with polycystic ovary syndrome: influence of the diet. Hum Reprod. 2003;18(11):2289-93.
- Glueck CJ, Papanna R, Wang P, Goldenberg N, and Sieve-Smith L. Incidence and treatment of metabolic syndrome in newly referred women with confirmed polycystic ovarian syndrome. Metabolism. 2003;52(7):908-15.
- Haase, C.L.; Varbo, A.; Laursen, P.N.; Schnecke, V.; Balen, A.H. Association between body mass index, weight loss and the chance of pregnancy in women with polycystic ovary syndrome and overweight or obesity: a retrospective cohort study in the UK. Hum Reprod 2023, 38, 471–481. [Google Scholar] [CrossRef]
- Marzouk, T.M.; Sayed Ahmed, W.A. Effect of Dietary Weight Loss on Menstrual Regularity in Obese Young Adult Women with Polycystic Ovary Syndrome. Journal of pediatric and adolescent gynecology 2015, 28, 457–461. [Google Scholar] [CrossRef]
- Ravn, P.; Haugen, A.G.; Glintborg, D. Overweight in polycystic ovary syndrome. An update on evidence based advice on diet, exercise and metformin use for weight loss. Minerva Endocrinol 2013, 38, 59–76. [Google Scholar]
- Thomson, R.L.; Buckley, J.D.; Moran, L.J.; Noakes, M.; Clifton, P.M.; Norman, R.J.; Brinkworth, G.D. The effect of weight loss on anti-Mullerian hormone levels in overweight and obese women with polycystic ovary syndrome and reproductive impairment. Hum Reprod 2009, 24, 1976–1981. [Google Scholar] [CrossRef]
- Mueller-Cunningham, W.M.; Quintana, R.; Kasim-Karakas, S.E. An ad libitum, very low-fat diet results in weight loss and changes in nutrient intakes in postmenopausal women. J Am Diet Assoc 2003, 103, 1600–1606. [Google Scholar] [CrossRef]
- Kasim-Karakas, S.E.; Tsodikov, A.; Singh, U.; Jialal, I. Responses of inflammatory markers to a low-fat, high-carbohydrate diet: effects of energy intake. Am J Clin Nutr 2006, 83, 774–779. [Google Scholar] [CrossRef]
- Gurusinghe, D.; Gill, S.; Almario, R.U.; Lee, J.; Horn, W.F.; Keim, N.L.; Kim, K.; Karakas, S.E. In polycystic ovary syndrome, adrenal steroids are regulated differently in the morning versus in response to nutrient intake. Fertil Steril 2010, 93, 1192–1199. [Google Scholar] [CrossRef]
- Kasim-Karakas, S.E.; Cunningham, W.M.; Tsodikov, A. Relation of nutrients and hormones in polycystic ovary syndrome. Am J Clin Nutr 2007, 85, 688–694. [Google Scholar] [CrossRef]
- Field, J.B. Hypoglycemia. Definition, clinical presentations, classification, and laboratory tests. Endocrinol Metab Clin North Am 1989, 18, 27–43. [Google Scholar] [CrossRef]
- Brun, J.F.; Fedou, C.; Mercier, J. Postprandial reactive hypoglycemia. Diabetes Metab 2000, 26, 337–351. [Google Scholar]
- Kasim-Karakas, S.E.; Almario, R.U.; Cunningham, W. Effects of protein versus simple sugar intake on weight loss in polycystic ovary syndrome (according to the National Institutes of Health criteria). Fertil Steril 2009, 92, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Gorissen, S.H.M.; Crombag, J.J.R.; Senden, J.M.G.; Waterval, W.A.H.; Bierau, J.; Verdijk, L.B.; van Loon, L.J.C. Protein content and amino acid composition of commercially available plant-based protein isolates. Amino Acids 2018, 50, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Newgard, C.B. Interplay between lipids and branched-chain amino acids in development of insulin resistance. Cell Metab 2012, 15, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab 2009, 9, 311–326. [Google Scholar] [CrossRef]
- Eastoe, J.E. The amino acid composition of mammalian collagen and gelatin. Biochem J 1955, 61, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, B.D.; Comerford, K.B.; Karakas, S.E.; Knotts, T.A.; Fiehn, O.; Adams, S.H. Whey protein supplementation does not alter plasma branched-chained amino acid profiles but results in unique metabolomics patterns in obese women enrolled in an 8-week weight loss trial. J Nutr 2015, 145, 691–700. [Google Scholar] [CrossRef]
- Altuntas, Y.; Bilir, M.; Ucak, S.; Gundogdu, S. Reactive hypoglycemia in lean young women with PCOS and correlations with insulin sensitivity and with beta cell function. Eur J Obstet Gynecol Reprod Biol 2005, 119, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Mumm, H.; Altinok, M.L.; Henriksen, J.E.; Ravn, P.; Glintborg, D.; Andersen, M. Prevalence and possible mechanisms of reactive hypoglycemia in polycystic ovary syndrome. Hum Reprod 2016, 31, 1105–1112. [Google Scholar] [CrossRef]
- Sam, S.; Vellanki, P.; Yalamanchi, S.K.; Bergman, R.N.; Dunaif, A. Exaggerated glucagon responses to hypoglycemia in women with polycystic ovary syndrome. Metabolism 2017, 71, 125–131. [Google Scholar] [CrossRef]
- Gennarelli, G.; Holte, J.; Stridsberg, M.; Niklasson, F.; Berne, C.; Backstrom, T. The counterregulatory response to hypoglycaemia in women with the polycystic ovary syndrome. Clin Endocrinol (Oxf) 1997, 46, 167–174. [Google Scholar] [CrossRef]
- Kishimoto, I. Subclinical Reactive Hypoglycemia with Low Glucose Effectiveness-Why We Cannot Stop Snacking despite Gaining Weight. Metabolites 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Ooi, D.S.Q.; Ling, J.Q.R.; Ong, F.Y.; Tai, E.S.; Henry, C.J.; Leow, M.K.S.; Khoo, E.Y.H.; Tan, C.S.; Chong, M.F.F.; Khoo, C.M.; et al. Branched Chain Amino Acid Supplementation to a Hypocaloric Diet Does Not Affect Resting Metabolic Rate but Increases Postprandial Fat Oxidation Response in Overweight and Obese Adults after Weight Loss Intervention. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Moran, L.J.; Clifton, P.M.; Noakes, M.; Brinkworth, G.D. Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: a meta-analysis of randomized controlled trials. Am J Clin Nutr 2012, 96, 1281–1298. [Google Scholar] [CrossRef] [PubMed]
- Stamets, K.; Taylor, D.S.; Kunselman, A.; Demers, L.M.; Pelkman, C.L.; Legro, R.S. A randomized trial of the effects of two types of short-term hypocaloric diets on weight loss in women with polycystic ovary syndrome. Fertil Steril 2004, 81, 630–637. [Google Scholar] [CrossRef]
- Moran, L.J.; Ko, H.; Misso, M.; Marsh, K.; Noakes, M.; Talbot, M.; Frearson, M.; Thondan, M.; Stepto, N.; Teede, H.J. Dietary composition in the treatment of polycystic ovary syndrome: a systematic review to inform evidence-based guidelines. Journal of the Academy of Nutrition and Dietetics 2013, 113, 520–545. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.C.; Gower, B.A.; Darnell, B.E.; Ovalle, F.; Oster, R.A.; Azziz, R. Role of diet in the treatment of polycystic ovary syndrome. Fertil Steril 2006, 85, 679–688. [Google Scholar] [CrossRef]
- Marsh, K.A.; Steinbeck, K.S.; Atkinson, F.S.; Petocz, P.; Brand-Miller, J.C. Effect of a low glycemic index compared with a conventional healthy diet on polycystic ovary syndrome. Am J Clin Nutr 2010, 92, 83–92. [Google Scholar] [CrossRef]
- Galletly, C.; Moran, L.; Noakes, M.; Clifton, P.; Tomlinson, L.; Norman, R. Psychological benefits of a high-protein, low-carbohydrate diet in obese women with polycystic ovary syndrome--a pilot study. Appetite 2007, 49, 590–593. [Google Scholar] [CrossRef]
- Sorensen, L.B.; Soe, M.; Halkier, K.H.; Stigsby, B.; Astrup, A. Effects of increased dietary protein-to-carbohydrate ratios in women with polycystic ovary syndrome. Am J Clin Nutr 2012, 95, 39–48. [Google Scholar] [CrossRef]
- Newgard, C.B. Interplay between lipids and branched-chain amino acids in development of insulin resistance. Cell Metab 2012, 15, 606–614. [Google Scholar] [CrossRef]
- Ichikawa, R.; Takano, K.; Fujimoto, K.; Kobayashi, M.; Kitamura, T.; Shichiri, M.; Miyatsuka, T. Robust increase in glucagon secretion after oral protein intake, but not after glucose or lipid intake in Japanese people without diabetes. J Diabetes Investig 2023. [Google Scholar] [CrossRef]
- Ishikawa, E.; Aikawa, T.; Matsutaka, H. The roles of alanine as a major precursor among amino acids for hepatic gluconeogenesis and as a major end product of the degradation of amino acids in rat tissues. J Biochem 1972, 71, 1097–1099. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Noakes, M.; Clifton, P.M.; Wittert, G.A.; Le Roux, C.W.; Ghatei, M.A.; Bloom, S.R.; Norman, R.J. Postprandial ghrelin, cholecystokinin, peptide YY, and appetite before and after weight loss in overweight women with and without polycystic ovary syndrome. Am J Clin Nutr 2007, 86, 1603–1610. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Changes in plasma glucose and insulin (1A), cortisol and dehydroepiandosterone (DHEA) and total plasma ghrelin during oral-glucose-tolerance (n= 28) and protein challenge (n= 23) tests, (Mean ± SEM). Differences between responses to the two treatments are expressed through treatment-by-time interaction effect. Overall, the interaction effect is highly significant (p< 0.001). Key timepoint p values are shown on the graph. All tests are based on the Wald test performed by using a linear mixed model applied to all available data.
Figure 1.
Changes in plasma glucose and insulin (1A), cortisol and dehydroepiandosterone (DHEA) and total plasma ghrelin during oral-glucose-tolerance (n= 28) and protein challenge (n= 23) tests, (Mean ± SEM). Differences between responses to the two treatments are expressed through treatment-by-time interaction effect. Overall, the interaction effect is highly significant (p< 0.001). Key timepoint p values are shown on the graph. All tests are based on the Wald test performed by using a linear mixed model applied to all available data.
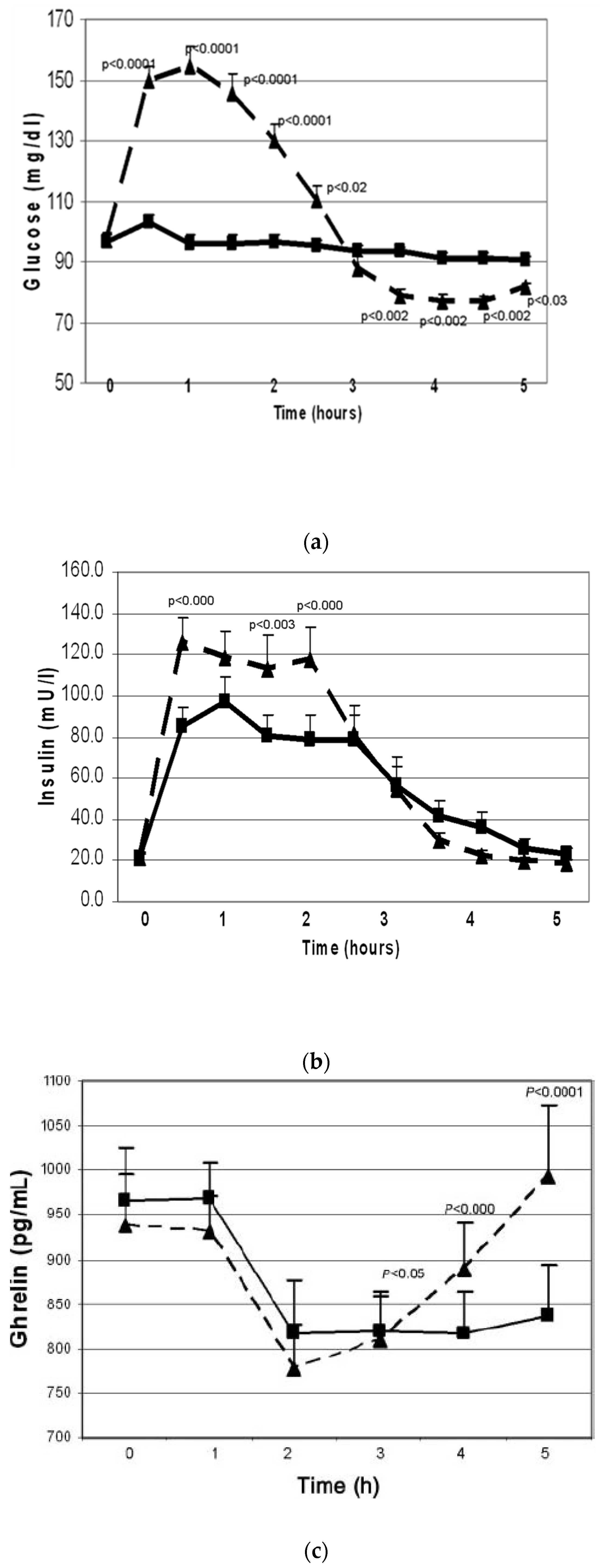
Figure 2.
Changes in cortisol and DHEA (2A), glucose and insulin (2B) and clinical symptoms (2C) in responders (n = 9, solid line) vs. non-responders (n = 10, broken line) during oral glucose tolerance test (Mean±SEM, *; p < 0.05 when responders and non-responders are compared to each other).
Figure 2.
Changes in cortisol and DHEA (2A), glucose and insulin (2B) and clinical symptoms (2C) in responders (n = 9, solid line) vs. non-responders (n = 10, broken line) during oral glucose tolerance test (Mean±SEM, *; p < 0.05 when responders and non-responders are compared to each other).
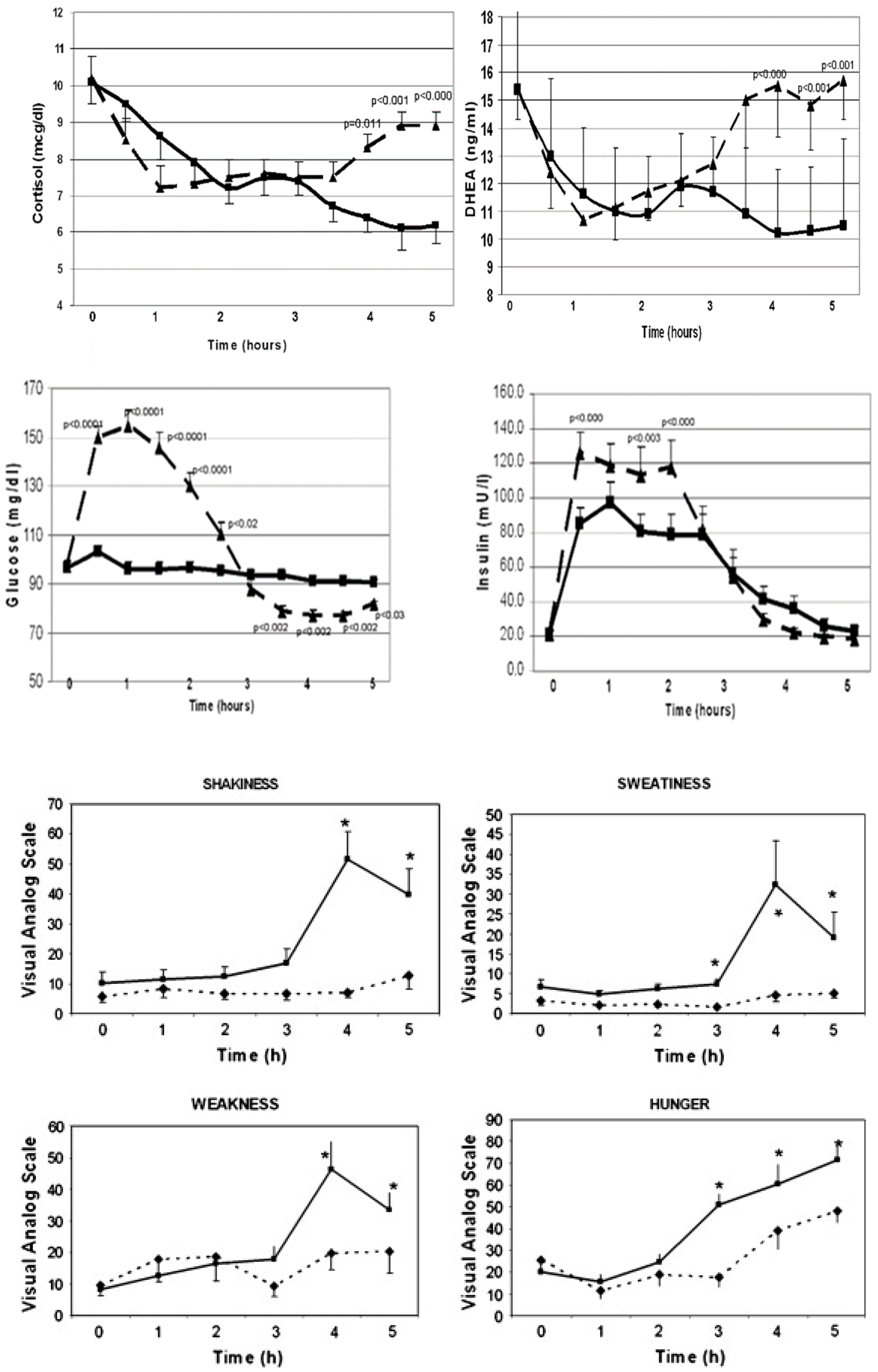
Figure 3.
Effects of whey protein (black columns) vs. simple-carbohydrate (CHO) supplements on weight, body mass index (BMI), fat mass, and plasma leptin concentrations during two months of weight loss intervention. *: p <0.05 and ᵻ: p < 0.01 when compared to before weight loss baseline; numeric p values indicate the differences between the WP vs. simple CHO supplements. Changes in the variables over time were analyzed using mixed-model analysis of variance methods. Post hoc comparisons between time points were conducted using paired t-tests. A significance level of .05 was used to determine statistical significance of observed differences. Post hoc comparisons between the treatment groups with respect to contemporaneous changes in the same response measures were based on two-sample t-tests.
Figure 3.
Effects of whey protein (black columns) vs. simple-carbohydrate (CHO) supplements on weight, body mass index (BMI), fat mass, and plasma leptin concentrations during two months of weight loss intervention. *: p <0.05 and ᵻ: p < 0.01 when compared to before weight loss baseline; numeric p values indicate the differences between the WP vs. simple CHO supplements. Changes in the variables over time were analyzed using mixed-model analysis of variance methods. Post hoc comparisons between time points were conducted using paired t-tests. A significance level of .05 was used to determine statistical significance of observed differences. Post hoc comparisons between the treatment groups with respect to contemporaneous changes in the same response measures were based on two-sample t-tests.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



