
Submitted:
29 September 2023
Posted:
30 September 2023
You are already at the latest version
Abstract
The oncogenicity of the human cytomegalovirus (CMV) is debated to this day. In recent years, mounting evidence addresses an anti-cancer effect via T cell-mediated CMV-targeted tumor de-struction. However, the data mostly comes from single-center studies and in vitro experiments. Broad geographic coverage is required to offer a global perspective. This study examined the correlation between country-specific CMV seroprevalence (n=73) and age-standardized inci-dence rates for 34 tumors using data obtained from the International Agency for Research on Cancer of the World Health Organization. The association between CMV and cancer incidences in 10-year age increments was also analyzed. The study revealed a worldwide inverse correlation between CMV seroprevalence and incidences of 88.2% tumors. Notably, this inverse link persists for all cancers combined (Spearman’s ρ= -0.732, p= 0.001). An antithetical and significant correlation is also observed in particular age groups for the vast majority of tumors. Our results corroborate the conclusions of previous studies and indicate that this phenomenon holds true on a global scale. It applies to a wide spectrum of cancer histologies, suggesting a common under-lying mechanism – CMV-stimulated T cell tumor targeting. Although these results further advance the notion of CMV-based therapies, further in-depth investigation of host-virus interactions is warranted.
Keywords:
Cytomegalovirus
; oncogenesis
; oncoprotection
; cancer
; global
; T cell
1. Introduction
The human cytomegalovirus (CMV), a widespread and globally prevalent agent of infection, affects approximately 83% of the world’s population [1]. However, the extent of viral presence varies considerably worldwide, with seroprevalence reaching up to 100% in specific populations [2]. Following initial exposure, CMV establishes a lifelong infection within the host, typically without causing symptoms in the general population. This is sharply contrasted with the serious illness it can provoke in individuals with compromised immune systems.
Although not categorized as an oncogenic virus, this pathogen has been linked to a wide array of cancers [3,4,5,6], and the debate over whether it possesses oncogenic potential has been extensive. Over the past few decades, however, an accumulating body of evidence suggests that the virus may, in fact, exhibit anti-tumor properties [7,8,9,10,11,12,13]. Recently, this phenomenon was observed on a global scale for the first time in malignancies originating from the B-cell lineage [7]. The underlying rationale for this type of anti-cancer behavior is rooted in a virus-focused immune response, where CMV molecules expressed on tumor cells serve as target antigens. For quite some time, researchers have been exploring viral antigens present within cancer cells as promising candidates for tumor-specific cancer immunotherapy [12]. These approaches encompass strategies such as cytotoxic T-lymphocyte (CTL) or dendritic cell (DC)-based vaccines. The existing evidence substantiates the idea that CMV-derived antigens can function as potent inducers of immune responses against infected cancer cells.
Despite a number of single-center and in vitro investigations conducted thus far, there have been no comprehensive global studies exploring the potential protective influence of CMV against cancer. Additionally, the question of whether an individual’s age plays a significant role in this context has yet to be resolved. In this research, we aim to examine the connection between CMV seroprevalence and the occurrence of some of the most prevalent and histologically varied tumors on a global scale. Furthermore, we seek to determine whether the suggested anti-cancer effects are consistent across distinct age groups. Building upon previous similar research, we present an outlook on CMV as a plausible agent for preventing the onset of cancer across various demographic, geopolitical, and socio-economic strata.
2. Materials and Methods
To investigate the potential anti-oncogenic effects of CMV, we have explored the correlation between country-specific age-standardized cancer incidence rates and corresponding CMV seroprevalences.
The age-adjusted annual incidence rates (per 105 individuals) specific to 34 cancer categories have been documented across 185 countries and are sourced from the Global Cancer Observatory (GLOBOCAN), a division of the World Health Organization [14]. Incidences were observed jointly for males and females, encompassing the full listed age range (0-85+ years).
The prevalence of cytomegalovirus was depicted through country-specific viral seroprevalence data for a total of 73 countries. This information was gathered by Zuhair and colleagues [1], who conducted a systematic survey of published literature to provide insights into the worldwide prevalence of CMV IgG antibodies. The list of investigated malignancies is presented in Table 1.
The same data sources were then used to inquire into the potential time-dependent relation between CMV infection and cancer. Namely, we asked whether there is a specific age range where the association between CMV and cancer incidence would appear more marked. Incidences for all mentioned malignancies were subsequently disaggregated into 10-year age intervals, again, as provided by the GLOBOCAN. Known cancer incidence rates for each age interval were then compared with the corresponding country-specific CMV prevalence (Table 2).
In both cases, comparison between age-standardized annual cancer incidence rates and country-specific CMV seroprevalence was statistically analyzed by using the Spearman’s rank correlation test. P-values were used to denote corresponding levels of statistical significance.
3. Results
An inverse correlation was evident between the prevalence of CMV and 88.2% (30/34) of the estimated age-adjusted tumor incidence rates, demonstrating a high degree of statistical significance (p < 0.001) in 73.5% (25/34) of instances. Noteworthy is the persistence of this statistical association when considering incidence rates for the entirety of combined cancers (Spearman’s ρ = -0.732, p < 0.001; shown in Figure 1). This observation suggests a plausible protective influence of the virus against the aforementioned neoplastic conditions on a global scale.
Strikingly, no discernible correlation surfaced between the CMV pervasiveness and the frequency of Kaposi’s sarcoma (Spearman’s ρ = -0.007, p = 0.953; shown in Figure 2). This is in line with the hypothesized CMV-galvanized T-cell tumoricidal activity; the T-cell immune response is severely impaired in individuals afflicted by HIV/AIDS, who prominently present with Kaposi’s sarcoma.
Conversely, CMV was significantly and positively correlated with nasopharyngeal carcinoma (Spearman’s ρ = +0.226, p = 0.023; shown in Figure 3) and gallbladder cancer (Spearman’s ρ = +0.316, p = 0.006), which constitutes 5.88% of studied tumors. All malignancies and their corresponding association with CMV are represented in Table 1.
The detailed examination of the relationship between CMV prevalence and worldwide cancer rates in specific age groups is presented in Table 2. The significant and opposite correlation observed at the country level manifests in specific age brackets for 94.1% (32/34) tumors. Notably, this link tends to be more pronounced in older age groups for most cancer types, with exceptions such as Kaposi’s sarcoma, cervical carcinoma, and malignant liver dyscrasia, which predominantly exhibit a protective effect in individuals under 40 years old. Finally, the correlation is still highly significant and speaks in favor of oncoprotection for all tumors combined, regardless of the age group.
A positive correlation in the case of nasopharyngeal carcinoma and gallbladder cancer is observed once again, suggesting the oncogenic potential of CMV in these types of cancers. Notably, the virus’s pro-tumor impact in individuals with gallbladder cancer is significantly more prevalent between the ages of 20 and 70. A similar pattern is discernible for cervical carcinoma, which is linked to individuals aged over 50.
In a smaller number of cases (23.3%), CMV appears to have an association with the development of tumors in specific age brackets, even in cases where CMV generally correlates with cancer prevention when examining combined incidence rates. It’s noteworthy that here the pro-tumor effect becomes apparent at a younger age, which is in stark contrast to the oncoprotective effect observed in older individuals. The neoplasia where this is the case are those of the hypopharynx, larynx, lip/oral tumors, liver, oropharynx, esophagus, stomach and multiple myeloma.
4. Discussion
So far, there have been various studies both supporting and challenging the idea of CMV oncogenicity. Our research aimed to provide further perspectives on this issue by presenting a global viewpoint. Additionally, we have explored the potential time-dependent effect of CMV infection in a variety of tumor histologies.
Cytomegalovirus and Oncoprotection – from T-Cells to Vaccines
Characterizing CMV solely as a contributor to oncogenesis is all but an outdated concept. Accumulating evidence not only supports its role in oncomodulation, but also points towards its potential for oncoprotection [7,9,10,15,16].
In recent years, the perspective of CMV functioning as a safeguard against cancer has gained traction. Notably, recent clinical studies have reported apparent anti-tumor effects of CMV in individuals with colorectal cancer and bronchogenic carcinoma [9,10]. Furthermore, patients with B-cell malignancies were noted to have a significantly lower incidence of CMV seropositivity compared to the control group [7]. A conspicuous absence of HCMV DNA was described in studies reviewing pleomorphic adenomas [17], Warthin’s tumors [17], epithelial ovarian cancer [18], papillary thyroid cancer [19], pediatric medulloblastomas [20], and central nervous system tumors [21]. Based on histopathological and clinical data in the case of cervical cancers, Thompson et al. report that there is no substantiated evidence to suggest a connection between CMV-positive cancers and any atypical histologic cell types or a more aggressive clinical demeanor [22].
In patients who have undergone allogeneic hematopoietic stem cell transplantation (HSCT), CMV reactivation has been associated with a marked reduction in leukemia relapse risk [8]. This is corroborated by the observation that prompt CMV replication may mitigate risk of relapse concerning non-Hodgkin lymphomas [23], acute myeloid leukemia [24,25,26], and pediatric acute leukemia in the wake of HSCT [27]. In a cohort of patient with myeloproliferative disorders, reactivation of CMV following HSCT was linked to a slight decrease in the risk of early relapse [28]. Similar associations were reported in solid organ transplant (SOT) patients; Geris and colleagues conclude that CMV status did not correlate with the risk of developing most cancers in SOT recipients [29]. Moreover, the same authors acknowledge an inverse correlation between CMV and diffuse large B-cell lymphoma (DLBCL), which is in accordance with our previous study [7]. A comparable outcome was noted in an experimental model involving murine CMV, where the virus negatively influenced the progression of B-cell lymphoma [30].
Over a century ago, speculation began to arise that certain viruses carry the capacity for tumor regression and remission [31]. It was found much later that these viruses possess an innate predilection for cancer cells, which both destroy the infected cells and set off host anti-cancer immunological mechanisms [32]. Additionally, oncolytic viruses, whose main purpose is to lyse tumor cells, have also been noted in coxsackievirus, adenovirus, and herpes simplex virus [33].
Recently, Ye et al. described an association between the highly conserved US31 CMV gene and its role in suppressing tumor proliferation and metastasis [34]. Further manipulation of the tumor microenvironment is managed through the virus’ transformative effects on various cellular genes and signaling pathways [35,36,37,38]. In addition to its direct interactions with host genes, human cytomegalovirus can also activate and influence the overall genetic landscape of tumor cells [39]. This encompasses promoting apoptosis [35,38,40,41], influencing the production of cytokines and chemokines [37], and inducing a vigorous activating effect on immune cells penetrating the tumor [35]. Further evidence comes from the fact that tumor growth is delayed by primary infection of tumor nodules [42].
In terms of cellular modifications, murine CMV has been observed to both engage [43] and infect [36] macrophages at the tumor site, where they are modified to enhance antitumor immune responses and effectively hinder oncogenesis [38,43]. Also noted is an immune response which principally activates natural killer (NK) cells [39,44,45,46,47,48], followed by CD4+ and CD8+ cytotoxic T-lymphocytes [39,48,49,50], high-affinity antibodies [39], and enduring memory T-cells [48]. Cytomegalovirus’ novel implications in vaccine vectors serve to evoke a robust T-cell response [51]. Harnessing this intense immune system reaction, most recent preclinical and clinical studies regarding CMV as an anti-cancer vaccine have shown encouraging results [52,53]. Additionally, CMV promoters have proven to successfully govern p53 tumor suppressor gene therapy when used as a chemotherapeutic for human ovarian carcinoma [54]. Specifically, the hypothesized CMV-mediated tumoricidal activity is posited to be modulated through an intact T-cell immune response, which is significantly compromised in individuals afflicted by HIV/AIDS – a subgroup that prominently presents with Kaposi’s sarcoma. In this research, no correlation between CMV oncoprotection and Kaposi’s sarcoma cumulated incidences was found. Considering that a fully functional T-cell repertoire is mandatory for anti-tumor activity, the absence of an association further bolsters the conjecture regarding CMV’s potential oncopreventive capacity.
A significant advantage of CMV as an anti-cancer vaccine is its potential to target multiple tumor-associated antigens (TAAs), which induces a wide range of immune responses [55]. This approach is particularly sought-after because of its ability to differentiate physiological and pathological tumor cells for targeted therapy [56]. This theory was successfully put to the test to achieve effective therapy in the treatment of gliomas [55]. By incorporating TAAs into the CMV vector, it is possible to induce targeted immune responses against the antigens specifically expressed by a patient’s tumor cells. This approach holds promise for personalized immunotherapy [55,57], tailoring the vaccine to the unique characteristics of each patient’s precise tumor.
Research concerned with targeting CMV as the biomarker in question poses as selective immunotherapy in the treatment of medulloblastoma [58], glioblastoma multiforme [59], as well as pancreatic cancer and brain tumors by the means of B-lymphocytes [57], all of which yield promising results. Immune recognition and elimination of CMV-infected tumor cells contribute to the anti-tumor properties attributed to the virus. The projected use of CMV vectors both prophylactically and therapeutically [49,50] can be harnessed and applied to suicide gene therapy to enhance the effectiveness of pharmacological therapeutics through selectively induced cell death [60]. Enhanced tumor regression and long-lasting oncoprotection have been indicated when immune checkpoint blockade is used synergistically with CMV administration [36,42].
Cytomegalovirus is undoubtedly emerging as a strong anti-cancer vaccine candidate [61]. Although more controlled trials are warranted, we believe that this discovery of a worldwide putative oncopreventive effect of CMV can advance the notion of CMV as an agent of active immunization against a wide range of malignant dyscrasia.
At What Time Could CMV offer its Greatest Protection?
Apart from this study, so far there has been no comprehensive or global research into possible time-dependent oncogenesis (or oncoprotection) linked with CMV infection. It is worthwhile noting, however, that congenital CMV infection correlated with the development of childhood blood cancer in certain studies [21,62], indicating that early infection might predispose for neoplastic events.
In our investigation, the purported oncoprotective effect of CMV had a propensity for older age groups for most cancer types. This suggests that an infection taking place at a later stage in life might offer protection against developing cancer, as opposed to an infection occurring earlier. Alternatively, it advocates for an onco-preventive effect that is more pronounced in tumors that develop in older populations. Nevertheless, this correlation remains robust when considering the cumulative incidence of all types of malignancies collectively. Finally, some tumors exhibit this contrasting correlation across all age groups, indicating a potential tumor-inhibiting effect irrespective of the timing of the initial infection.
The anti-cancer property notwithstanding, in certain age groups CMV acts as a de facto agent of oncogenesis (Table 2). This is most obvious for nasopharyngeal carcinoma and gallbladder cancer. The link with NPC has already described in literature [63], which further corroborates our findings from a global perspective. Interestingly enough, in specific cases (23.3%) of malignancies where CMV generally correlated with cancer-prevention, in some age groups its effect would be statistically recognized as oncogenic (Table 2). This pro-tumor agency was apparent in younger age groups.
The dual nature of CMV (pro- and anti-oncogenic) observed herein, that manifested solely when discrete age brackets were analyzed, may point to an outcome (tumor genesis or tumor prevention) predicated on the time of first infection. Evidence indicates that acquiring the infection earlier in life or congenitally increases the individual’s susceptibility to cancer development [21,62], whereas encountering CMV at a later stage may offer protective effects. However, the conclusions should be taken with caution, as correlation does not always confer causation (Cf. Study limitations).
Arguments in Favor of CMV Oncogenesis
To date, the role of CMV as a potential underlying factor of malignancies is still debated. Its oncogenic role has indeed been postulated numerous times [64,65,66], with the virus posited to be involved in over 90% of the most frequently presenting tumors [67]. CMV is purported to possess the ability to influence cellular processes and pathways, potentially increasing the cell’s susceptibility to developing malignancies by interfering with the cellular pathways associated with the cell cycle, apoptosis, angiogenesis, cell invasion, and the immune response of the host [68,69]. Furthermore, it has been proposed that CMV may promote tumor growth [61].
Polz-Gruszka D et al. have detected CMV DNA in fresh-frozen tumor tissue fragments from 10% of patients with oral squamous cell carcinoma [70]. Cytomegalovirus has been reported as a risk factor for glioma, neuroblastoma, as well as breast cancer [3,4,71,72,73,74]. Persons suffering from breast cancer who were CMV seropositive or had CMV DNA in tumor tissue were significantly more likely to develop Stage IV metastatic tumors, hinting at an adverse oncomodulatory role of the virus which promotes metastases [75]. An adverse effect of CMV was also noted elsewhere regarding the same pathology [76]. Furthermore, viral protein expression was found to relate with shorter overall survival in patients with breast cancer [77]; CMV IE2 gene expression was also associated with this tumor [78]. In a recent study by Paradowska and colleagues, a significant proportion (70%) of epithelial ovarian cancers (EOC) contained CMV DNA; moreover, the pathogen was significantly more prevalent in EOC than benign tumors [79]. Evidence suggest that CMV is involved in the pathology of colorectal cancer (CrC) and inflammatory bowel disease [80,81,82,83,84]. Cytomegalovirus infection was also associated with a poor prognosis in CrC patients, where three viral genes (UL82, UL42, and UL117) were linked to poor patient survival outcomes [80]. The virus was postulated to play a role in the tumorigenesis of malignant gliomas [69,83,85,86,87,88,89,90,91,92,93], notably the extremely destructive glioblastoma multiforme (GBM) [68,94,95], although not considered to have a role in development of non-GBM infantile brain tumors. Both CMV and Epstein-Barr virus (EBV) were detected in the exhaled breath condensate of lung cancer patients, and consequently potentially implicated in lung carcinogenesis by the authors [96]. In patients with head and neck malignancies, CMV seropositivity itself was not found to impinge on survival; however, the authors propose that high titers and active CMV virus in the tumor environment may be linked to inferior outcomes [97]. The study conducted by Sarshari and colleagues found that CMV, EBV, and human herpesvirus 6 might play a role in initiating and development gastritis and gastric cancer [5]; the potential risk for gastric and gastrointestinal cancer was acknowledged elsewhere [74,98].
Cytomegalovirus has been also associated with prostate cancer [64,83,99], colon and cervical carcinoma [6,100,101], as well as epithelial ovarian cancer [102]. Recently, congenital CMV infection was put forward as a risk factor for childhood acute lymphoblastic leukemia [62]. CMV infections have been noted to cause chronic inflammatory processes, which in and of itself serves as both a precursor and cornerstone of malignancy [103,104,105,106,107,108,109,110]. The virus is known to directly seize tumor-promoting cellular events while simultaneously overriding immunosuppressive mechanisms [67].
At minimum, CMV has a role in oncomodulation [111], as it supports the proliferation and longevity of cancer [112,113,114] while increasing its malignant potential by inducing transformation into its malignant phenotypes [83,85,113]. This is achieved by means of large-scale derangement of cellular signaling pathways, disordered enzyme expression, and chronic inflammation [83,84,113] amplifying the pressure associated with the fragile process of DNA replication, which precipitates both genomic injury and volatility [115]. However, it is worthwhile noting that not all oncomodulatory effects need be detrimental to the host. Namely, it has been observed that CMV may inhibit migration of specific breast cancer cells [116].
Some high-risk CMV strains were even implicated to have a catalytic role in the explicit transformation of primary cells [112,117,118,119]. Most notably, Cobbs observed that CMV not only has the capacity for epithelial cell modification, but is implicated in epithelial to mesenchymal (EMT) transformation in tumor cells and vice versa. It is important to note that EMT has been suggested as the causative agent of cell-to-cell adhesion loss, deranged cellular polarity and cytoskeleton transfiguration [120], hence facilitating a critical role in tumor progression and functioning as a primary target of interest in anticancer therapy [121]. Cytomegalovirus could present as a causative agent to GBM through ARG2 upregulation [86] and STAT3 signaling [68], which is often used as an early tumor biomarker. Chemokine receptor US28 binds and activates a proliferative response that is capable of promoting tumorigenesis [122]. CMV can cause sequestrations and deactivates p53, which proves to be important in our understanding of the virus’ tumorigenic properties [123].
Study Limitations
Recognizing the study’s constraints is essential. The country’s overall CMV prevalence, as obtained from Zuhair et al. [1], may not precisely mirror the virus’s distribution among different age groups. Nevertheless, this CMV prevalence can reasonably serve as a proxy, given that significant associations calculated for combined incidence rates generally remain consistent when examining their individual age-specific incidences.
Furthermore, the correlation we used in statistical analysis does not necessarily infer causation, although the inverse association between CMV prevalence and cancer age-standardized incidence rates is striking, as it covers a large proportion of neoplasia the world over. A number of factors contribute to CMV seropositivity: age [124,125,126], gender [124,127,128], socioeconomic status [129,130,131], current smoking [129], level of education [129], number of sexual partners [129], childcare practices [125], different cultural conditions or customs related to breastfeeding [125], to name some of them. Racial/ethnic background is also related to SES [132,133]. CMV seropositivity may serve as a proxy for any of these parameters, which may obscure the true cause of the oncoprotective effect noted in our work. However, none of these by itself comes across as good an oncoprotective candidate as CMV seems to be.
Ultimately, a thorough and strong understanding of the relationship between tumors and CMV is likely to emerge through extensive molecular analyses and prospective studies involving large population cohorts.
5. Conclusions
The elevated CMV prevalence is linked to diminished tumor occurrence across various population demographics worldwide. Combined with reduced relapse hazards evident in malignancies displaying CMV reactivation, they collectively emphasize oncoprotective attributes of the virus. This effect is also observable in specific age intervals for a wide spectrum of tumor histologies. Supported by previous in vitro studies, these findings challenge the earlier belief that CMV acts as an etiologic factor in the manifestation of cancer and steer the prevailing opinion towards its possible oncoprotective nature. Cytomegalovirus is a complex and multifaceted virus and the ramifications following infection are far from black and white. The studies so far collectively contribute to a comprehensive understanding regarding the correlation between CMV and its oncoprotective nature. However, these conclusions warrant further scrutiny and emphasize the need for in-depth investigation to elucidate the underlying mechanisms responsible for the virus’ oncoprotective nature, while keeping in mind the epidemiological consequences influenced by the processes cited above.
Author Contributions
Conceptualization: MJ, TK, AK, and MT-B; Funding acquisition: TJ, BM and MT-B; Writing—original draft preparation: MJ, TK, AK and ID, Writing—review and editing: MJ, TK, ID, TJ, BM and MT-B; Investigation and Methodology: MJ and TK; Project administration, Supervision, Resources: TJ, AK, BM and MT-B.
Funding
This work was supported by the Ministry of Science, Technological Development and Innovation (MSTDI) of the Republic of Serbia, grant number 200110. Any opinions, findings, conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of MSTDI.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All Data are either publicly accessible or available from the corresponding author upon reasonable request.
Acknowledgments
Conducting this study would have been unfeasible without the indispensable and comprehensive data provided by the WHO’s GLOBOCAN. The authors wish to express their appreciation for the dedication of all those responsible for maintaining these crucial databases.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Zuhair M, Smit GSA, Wallis G, Jabbar F, Smith C, Devleesschauwer B, Griffiths P. Estimation of the worldwide seroprevalence of cytomegalovirus: A systematic review and meta-analysis. Rev Med Virol. 2019, 29, e2034. [Google Scholar] [CrossRef] [PubMed]
- Fowler K, Mucha J, Neumann M, Lewandowski W, Kaczanowska M, Grys M, Schmidt E, Natenshon A, Talarico C, Buck PO, Diaz-Decaro J. A systematic literature review of the global seroprevalence of cytomegalovirus: possible implications for treatment, screening, and vaccine development. BMC Public Health. 2022, 22, 1659. [Google Scholar] [CrossRef]
- Pandey, JP. Immunoglobulin GM Genes, Cytomegalovirus Immunoevasion, and the Risk of Glioma, Neuroblastoma, and Breast Cancer. Front Oncol. 2014, 29, 236. [Google Scholar] [CrossRef] [PubMed]
- Nehme Z, Pasquereau S, Haidar Ahmad S, El Baba R, Herbein G. Polyploid giant cancer cells, EZH2 and Myc upregulation in mammary epithelial cells infected with high-risk human cytomegalovirus. EBioMedicine. 2022, 80, 104056. [Google Scholar] [CrossRef]
- Sarshari B, Mohebbi SR, Ravanshad M, Shahrokh S, Aghdaei HA, Zali MR. Detection and quantification of Epstein-Barr virus, cytomegalovirus, and human herpesvirus-6 in stomach frozen tissue of chronic gastritis and gastric cancer patients. Microbiol Immunol. 2022, 66, 379–385. [Google Scholar] [CrossRef]
- Doniger J, Muralidhar S, Rosenthal LJ. Human cytomegalovirus and human herpesvirus 6 genes that transform and transactivate. Clin Microbiol Rev. 1999, 12, 367–382. [Google Scholar] [CrossRef]
- Janković M, Knežević A, Todorović M, Đunić I, Mihaljević B, Soldatović I, Protić J, Miković N, Stoiljković V, Jovanović T. Cytomegalovirus infection may be oncoprotective against neoplasms of B-lymphocyte lineage: single-institution experience and survey of global evidence. Virol J. 2022, 19, 155. [Google Scholar] [CrossRef]
- Bigley AB, Baker FL, Simpson RJ. Cytomegalovirus: an unlikely ally in the fight against blood cancers? Clin Exp Immunol. 2018, 193, 265–274. [Google Scholar] [CrossRef]
- Rashid S, Ardeljan A, Frankel LR, Cardeiro M, Kim E, Nagel BM, Takabe K, Rashid O. Human Cytomegalovirus (CMV) Infection Associated With Decreased Risk of Bronchogenic Carcinoma: Understanding How a Previous CMV Infection Leads to an Enhanced Immune Response Against Malignancy. Cureus. 2023, 15, e37265. [Google Scholar] [CrossRef]
- Nagel B, Frankel L, Ardeljan A, Cardeiro M, Rashid S, Takabe K, Rashid OM. The Association of Human Cytomegalovirus Infection and Colorectal Cancer: A Clinical Analysis. World J Oncol. 2023, 14, 119–124. [Google Scholar] [CrossRef]
- Daei Sorkhabi A, Sarkesh A, Saeedi H, Marofi F, Ghaebi M, Silvestris N, Baradaran B, Brunetti O. The Basis and Advances in Clinical Application of Cytomegalovirus-Specific Cytotoxic T Cell Immunotherapy for Glioblastoma Multiforme. Front Oncol. 2022, 12, 818447. [Google Scholar] [CrossRef] [PubMed]
- Ahn J, Shin C, Kim YS, Park JS, Jeun SS, Ahn S. Cytomegalovirus-Specific Immunotherapy for Glioblastoma Treatments. Brain Tumor Res Treat. 2022, 10, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Schuessler A, Walker DG, Khanna R. Cytomegalovirus as a novel target for immunotherapy of glioblastoma multiforme. Front Oncol. 2014, 4, 275. [Google Scholar] [CrossRef]
- Available online: https://gco.iarc.fr/.
- Gustafsson RKL, Jeffery HC, Yaiw K-C, Wilhelmi V, Kostopoulou ON, Davoudi B, Rahbar A, Benard M, Renné T, Söderberg-Nauclér C & Butler LM. Direct infection of primary endothelial cells with human cytomegalovirus prevents angiogenesis and migration. J Gen Virol. 2015; 96(12).
- Ozel I, Duerig I, Domnich M, Lang S, Pylaeva E, Jablonska J. The Good, the Bad, and the Ugly: Neutrophils, Angiogenesis, and Cancer. Cancers (Basel). 2022, 14, 536. [Google Scholar] [CrossRef]
- Laane CJ, Murr AH, Mhatre AN, Jones KD, and Lalwan AK. Role of Epstein-Barr virus and cytomegalovirus in the etiology of benign parotid tumors. Head Neck. 2002, 24, 443–450. [Google Scholar] [CrossRef]
- Ingerslev K, Høgdall E, Skovrider-Ruminski W. et al. The prevalence of EBV and CMV DNA in epithelial ovarian cancer. Infect Agents Cancer. 2019;14(7).
- Huang TS, Lee JJ, & Cheng SP. No evidence of association between human cytomegalovirus infection and papillary thyroid cancer. World J Surg Onc. 2014;12(41).
- Vermeulen JF, van Hecke W, Jansen MK, Spliet WG, Broekhuizen R, Bovenschen N. No evidence for human cytomegalovirus infection in pediatric medulloblastomas. Neuro Oncol. 2016, 18, 1461–1462. [Google Scholar] [CrossRef]
- Wiemels JL, Talbäck M, Francis S, Feychting M. Early Infection with Cytomegalovirus and Risk of Childhood Hematologic Malignancies. Cancer Epidemiol Biomarkers Prev. 2019, 28, 1024–1027. [Google Scholar] [CrossRef]
- Thompson CH, Rose BR, Elliott PM. Cytomegalovirus and cervical cancer: failure to detect a direct association or an interaction with human papillomaviruses. Gynecol Oncol. 1994, 54, 40–46. [Google Scholar] [CrossRef]
- Koldehoff M, Ross SR, Dührsen U, Beelen DW, Elmaagacli AH. Early CMV-replication after allogeneic stem cell transplantation is associated with a reduced relapse risk in lymphoma. Leuk Lymphoma. 2017, 58, 822–833. [Google Scholar] [CrossRef]
- Elmaagacli AH, Steckel NK, Koldehoff M, Hegerfeldt Y, Trenschel R, Ditschkowski M, Christoph S, Gromke T, Kordelas L, Ottinger HD, Ross RS, Horn PA, Schnittger S, Beelen DW. Early human cytomegalovirus replication after transplantation is associated with a decreased relapse risk: evidence for a putative virus-versus-leukemia effect in acute myeloid leukemia patients. Blood. 2011, 118, 1402–1412. [Google Scholar] [CrossRef] [PubMed]
- Green ML, Leisenring WM, Xie H, Walter RB, Mielcarek M, Sandmaier BM, Riddell SR, Boeckh M. CMV reactivation after allogeneic HCT and relapse risk: evidence for early protection in acute myeloid leukemia. Blood. 2013, 122, 1316–1324. [Google Scholar] [CrossRef] [PubMed]
- Litjens NHR, van der Wagen L, Kuball J, Kwekkeboom J. Potential Beneficial Effects of Cytomegalovirus Infection after Transplantation. Front Immunol. 2018, 9, 389. [Google Scholar] [CrossRef] [PubMed]
- Inagaki J, Noguchi M, Kurauchi K, Tanioka S, Fukano R, Okamura J. Effect of Cytomegalovirus Reactivation on Relapse after Allogeneic Hematopoietic Stem Cell Transplantation in Pediatric Acute Leukemia. Biol Blood Marrow Transplant. 2016, 22, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Peric Z, Wilson J, Durakovic N, Ostojic A, Desnica L, Vranjes VR, Marekovic I, Serventi-Seiwerth R, Vrhovac R. Early human cytomegalovirus reactivation is associated with lower incidence of relapse of myeloproliferative disorders after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018, 53, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Geris JM, Spector LG, Pfeiffer RM, Limaye AP, Yu KJ and Engels EA. Cancer risk associated with cytomegalovirus infection among solid organ transplant recipients in the United States. Cancer. 2022, 128, 3985–3994. [Google Scholar] [CrossRef]
- Erlach KC, Podlech J, Rojan A, Reddehase MJ. Tumor control in a model of bone marrow transplantation and acute liver-infiltrating B-cell lymphoma: an unpredicted novel function of cytomegalovirus. J Virol. 2002, 76, 2857–2870. [Google Scholar] [CrossRef]
- Kelly E, Russell SJ. History of oncolytic viruses: genesis to genetic engineering. Mol Ther. 2007, 15, 651–659. [Google Scholar] [CrossRef]
- Russell SJ, Peng KW, Bell JC. Oncolytic virotherapy. Nat Biotechnol. 2012, 30, 658–670. [Google Scholar] [CrossRef]
- Cao GD, He XB, Sun Q, Chen S, Wan K, Xu X, Feng X, Li PP, Chen B, Xiong MM. The Oncolytic Virus in Cancer Diagnosis and Treatment. Front Oncol. 2020, 10, 1786. [Google Scholar] [CrossRef]
- Ye S, Hu Y, Chen C, Chen S, Tong X, Zhu H, Deng B, Hu X, Sun X, Chen X, Shi X, Gu R, Xie W, Guo G, Xing D, Shen X, Xue X, Shen S. The Human Cytomegalovirus US31 Gene Predicts Favorable Survival and Regulates the Tumor Microenvironment in Gastric Cancer. Front Oncol. 2021, 11, 614925, Erratum in: Front Oncol. 2021 Jun 17;11:715746. [Google Scholar] [CrossRef]
- Herbein G, Nehme Z. Tumor Control by Cytomegalovirus: A Door Open for Oncolytic Virotherapy? Mol Ther Oncolytics. 2020, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Erkes DA, Wilski NA, Snyder CM. Intratumoral infection by CMV may change the tumor environment by directly interacting with tumor-associated macrophages to promote cancer immunity. Hum Vaccin Immunother. 2017, 13, 1778–1785. [Google Scholar] [CrossRef] [PubMed]
- Wilski NA, Stotesbury C, Del Casale C, Montoya B, Wong E, Sigal LJ, Snyder CM. STING Sensing of Murine Cytomegalovirus Alters the Tumor Microenvironment to Promote Antitumor Immunity. J Immunol. 2020, 204, 2961–2972. [Google Scholar] [CrossRef] [PubMed]
- Erlach KC, Böhm V, Seckert CK, Reddehase MJ, Podlech J. Lymphoma cell apoptosis in the liver induced by distant murine cytomegalovirus infection. J Virol. 2006, 80, 4801–4819. [Google Scholar] [CrossRef]
- Jackson SE, Redeker A, Arens R, et al. CMV immune evasion and manipulation of the immune system with aging. GeroScience. 2017;39, 273–291.
- Kumar A, Coquard L, Pasquereau S, Russo L, Valmary-Degano S, Borg C, Pothier P, Herbein G. Tumor control by human cytomegalovirus in a murine model of hepatocellular carcinoma. Mol Ther Oncolytics. 2016, 3, 16012. [Google Scholar] [CrossRef]
- Koldehoff M, Lindemann M, Opalka B, Bauer S, Ross RS, Elmaagacli AH. Cytomegalovirus induces apoptosis in acute leukemia cells as a virus-versus-leukemia function. Leuk Lymphoma. 2015, 56, 3189–3197. [Google Scholar] [CrossRef]
- Erkes DA, Xu G, Daskalakis C, Zurbach KA, Wilski NA, Moghbeli T, Hill AB, Snyder CM. Intratumoral Infection with Murine Cytomegalovirus Synergizes with PD-L1 Blockade to Clear Melanoma Lesions and Induce Long-term Immunity. Mol Ther. 2016, 24, 1444–1455. [Google Scholar] [CrossRef]
- Wilski NA, Del Casale C, Purwin TJ, Aplin AE, Snyder CM. Murine Cytomegalovirus Infection of Melanoma Lesions Delays Tumor Growth by Recruiting and Repolarizing Monocytic Phagocytes in the Tumor. J Virol. 2019, 93, e00533–19. [Google Scholar] [CrossRef]
- Picarda G, Benedict CA; Cytomegalovirus: Shape-Shifting the Immune System. J Immunol 15 June 2018; 200 (12): 3881–3889. 15 June.
- Lee S, Doualeh M, Affandi JS, Makwana N, Irish A, Price P. Functional and clinical consequences of changes to natural killer cell phenotypes driven by chronic cytomegalovirus infections. J Med Virol. 2019, 91, 1120–1127. [Google Scholar] [CrossRef]
- Wilkinson GWG, Tomasec P, Stanton RJ, Armstrong M, Prod’homme V, Aicheler R, McSharry BP, Rickards CR, Cochrane D, Llewellyn-Lacey S, Wang ECY, Griffin CA, & Davison AJ. Modulation of natural killer cells by human cytomegalovirus. J Clin Virol. 2008, 41, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Lisnić B, Lisnić VJ, Jonjić S. NK cell interplay with cytomegaloviruses. Curr Opin Virol. 2015, 15, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Jackson SE, Mason GM, Wills MR. Human cytomegalovirus immunity and immune evasion. Virus Res. 2011, 157, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Tršan T, Vuković K, Filipović P, Brizić AL, Lemmermann NAW, Schober K, Busch DH, Britt WJ, Messerle M, Krmpotić A, & Jonjić S. Cytomegalovirus vector expressing RAE-1γ induces enhanced anti-tumor capacity of murine CD8+ T cells. Eur. J. Immunol. 2017, 47, 1354–1367. [Google Scholar] [CrossRef]
- Qiu Z, Huang H, Grenier JM, Perez OA, Smilowitz HM, Adler B, Khanna KM. Cytomegalovirus-Based Vaccine Expressing a Modified Tumor Antigen Induces Potent Tumor-Specific CD8(+) T-cell Response and Protects Mice from Melanoma. Cancer Immunol Res. 2015, 3, 536–546. [Google Scholar] [CrossRef]
- Quinn M, Erkes DA, Snyder CM. Cytomegalovirus and immunotherapy: opportunistic pathogen, novel target for cancer and a promising vaccine vector. Immunotherapy. 2016, 8, 211–221. [Google Scholar] [CrossRef]
- Hartman ZC, Wei J, Glass OK, Guo H, Lei G, Yang X-Y, Osada T, Hobeika A, Delcayre A, Le Pecq J-B, Morse MA, Clay TM, & Lyerly HK. Increasing vaccine potency through exosome antigen targeting. Vacc. 2011, 29, 9361–9367. [Google Scholar] [CrossRef]
- Liu J, Jaijyan DK, Tang Q, Zhu H. Promising Cytomegalovirus-Based Vaccine Vector Induces Robust CD8+ T-Cell Response. Int J Mol Sci. 2019, 20, 4457. [Google Scholar] [CrossRef]
- Mujoo K, Maneval DC, Anderson SC, Gutterman JU. Adenoviral-mediated p53 tumor suppressor gene therapy of human ovarian carcinoma. Oncogene. 1996, 12, 1617–1623. [Google Scholar]
- De Leon G, Nair S, Xie W, Drake J, Mitchell D. IT-06: PERSONALIZED IMMUNOTHERAPY FOR THE TREATMENT OF GLIOBLASTOMA. Neuro Oncol. 2014 Nov;16(Suppl 5):v111. [CrossRef]
- Rooney CM, Leen AM, Vera JF, & Heslop HE. T lymphocytes targeting native receptors. Immunol Rev. 2014, 257, 39–55. [Google Scholar] [CrossRef] [PubMed]
- Meng Q, Valentini D, Rao M, Dodoo E, Maeurer M. CMV and EBV targets recognized by tumor-infiltrating B lymphocytes in pancreatic cancer and brain tumors. Sci Rep. 2018, 8, 17079. [Google Scholar] [CrossRef] [PubMed]
- Hortal AM, Vermeulen JF, Van Hecke W, Bovenschen N. Oncogenic role of cytomegalovirus in medulloblastoma? Cancer Lett. 2017, 408, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Daei Sorkhabi A, Sarkesh A, Saeedi H, Marofi F, Ghaebi M, Silvestris N, Baradaran B, Brunetti O. The Basis and Advances in Clinical Application of Cytomegalovirus-Specific Cytotoxic T Cell Immunotherapy for Glioblastoma Multiforme. Front Oncol. 2022, 12, 818447. [Google Scholar] [CrossRef] [PubMed]
- Düzgüneş N, Cheung J, Konopka K. Non-viral suicide gene therapy in cervical, oral and pharyngeal carcinoma cells with CMV- and EEV-plasmids. J Gene Med. 2018 Oct;20(10-11):e3054. [CrossRef]
- Wilski NA, Snyder CM. From Vaccine Vector to Oncomodulation: Understanding the Complex Interplay between CMV and Cancer. Vaccines (Basel). 2019, 7, 62. [Google Scholar] [CrossRef]
- Francis SS, Wallace AD, Wendt GA, Li L, Liu F, Riley LW, Kogan S, Walsh KM, de Smith AJ, Dahl GV, Ma X, Delwart E, Metayer C, Wiemels JL. In utero cytomegalovirus infection and development of childhood acute lymphoblastic leukemia. Blood. 2017, 129, 1680–1684. [Google Scholar] [CrossRef]
- Ahmed HG, Suliman RSA, Ashankyty IM, Albieh ZA, Warille AA. Role of human Cytomegalovirus in the etiology of nasopharyngeal carcinoma. J Cancer Res Ther. 2018, 14, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Geder L, Sanford EJ, Rohner TJ, Rapp F. Cytomegalovirus and cancer of the prostate: in vitro transformation of human cells. Cancer Treatment Reports. 1977, 61, 139–146. [Google Scholar]
- Herbein, G. Tumors and Cytomegalovirus: An Intimate Interplay. Viruses. 2022, 14, 812. [Google Scholar] [CrossRef]
- Melnick M, Sedghizadeh PP, Allen CM, Jaskoll T. Human cytomegalovirus and mucoepidermoid carcinoma of salivary glands: cell-specific localization of active viral and oncogenic signaling proteins is confirmatory of a causal relationship. Exp Mol Pathol. 2012, 92, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Nauclér CS, Geisler J, Vetvik K. The emerging role of human cytomegalovirus infection in human carcinogenesis: a review of current evidence and potential therapeutic implications. Oncotarget. 2019, 10, 4333–4347. [Google Scholar] [CrossRef]
- Cobbs, CS. Cytomegalovirus and brain tumor: epidemiology, biology and therapeutic aspects. Curr Opin Oncol. 2013, 25, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Barami, K. Oncomodulatory mechanisms of human cytomegalovirus in gliomas. J Clin Neurosci. 2010, 17, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Polz-Gruszka D, Stec A, Dworzański J, Polz-Dacewicz M. EBV, HSV, CMV and HPV in laryngeal and oropharyngeal carcinoma in Polish patients. Anticancer Res. 2015, 35, 1657–1661. [Google Scholar]
- Wolmer-Solberg, N.; Baryawno, N.; Rahbar, A.; Fuchs, D.; Odeberg, J.; Taher, C.; Wilhelmi, V.; Milosevic, J.; Mohammad, A.A.; Martinsson, T.; et al. Frequent detection of human cytomegalovirus in neuroblastoma: A novel therapeutic target? Int. J. Cancer 2013, 133, 2351–2361. [Google Scholar] [CrossRef]
- Herbein G, Kumar A. The oncogenic potential of human cytomegalovirus and breast cancer. Front Oncol. 2014, 4, 230. [Google Scholar] [CrossRef]
- Taher, Chato & Boniface, Jana & Mohammad, Abdul-Aleem & Religa, Piotr & Hartman, Johan & Yaiw, Koon-Chu & Frisell, Jan & Rahbar, Afsar & Söderberg-Nauclér, Cecilia. (2013). High Prevalence of Human Cytomegalovirus Proteins and Nucleic Acids in Primary Breast Cancer and Metastatic Sentinel Lymph Nodes. PloS one. 8. e56795. [CrossRef]
- Zhang L, Guo G, Xu J, Sun X, Chen W, Jin J, Hu C, Zhang P, Shen X, Xue X. Human cytomegalovirus detection in gastric cancer and its possible association with lymphatic metastasis. Diagn Microbiol Infect Dis. 2017, 88, 62–68. [Google Scholar] [CrossRef]
- Yang Z, Tang X, Hasing ME, Pang X, Ghosh S, McMullen TPW, Brindley DN, Hemmings DG. Human Cytomegalovirus Seropositivity and Viral DNA in Breast Tumors Are Associated with Poor Patient Prognosis. Cancers (Basel). 2022, 14, 1148. [Google Scholar] [CrossRef]
- Youssry S, Hussein A, Ramadan R, Alkarmouty A, Elsheredy A. The association of human cytomegalovirus with biomarkers of inflammation and immune activation in breast cancer. Breast Dis. 2022, 41, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Touma J, Pantalone MR, Rahbar A, Liu Y, Vetvik K, Sauer T, Söderberg-Naucler C, Geisler J. Human Cytomegalovirus Protein Expression Is Correlated with Shorter Overall Survival in Breast Cancer Patients: A Cohort Study. Viruses. 2023, 15, 732. [Google Scholar] [CrossRef] [PubMed]
- Cui J, Wang Q, Wang HB, Wang B, Li L. Protein and DNA evidences of HCMV infection in primary breast cancer tissues and metastatic sentinel lymph nodes. Cancer Biomark. 2018, 21, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Paradowska E, Jabłońska A, Studzińska M, Wilczyński M, Wilczyński JR. Detection and genotyping of CMV and HPV in tumors and fallopian tubes from epithelial ovarian cancer patients. Sci Rep. 2019, 9, 19935. [Google Scholar] [CrossRef]
- Fang Y, Wang Q, Huang K, Zhang M, Pei S, Li L, Peng Y, Lan L, Zheng X. Human cytomegalovirus-induced immune regulation is correlated with poor prognosis in patients with colorectal cancer. Clin Exp Med. 2023, 23, 427–436. [Google Scholar] [CrossRef]
- Chen HP, Chan YJ. The oncomodulatory role of human cytomegalovirus in colorectal cancer: implications for clinical trials. Front Oncol. 2014, 4, 314. [Google Scholar] [CrossRef]
- Marongiu L, Venturelli S, Allgayer H. Involvement of HHV-4 (Epstein-Barr Virus) and HHV-5 (Cytomegalovirus) in Inflammatory Bowel Disease and Colorectal Cancer: A Meta-Analysis. Cancers (Basel). 2022, 14, 5085. [CrossRef]
- Soroceanu L, Cobbs CS. Is HCMV a tumor promoter? Virus Res. 2011, 157, 193–203. [Google Scholar] [CrossRef]
- Harkins L, Volk AL, Samanta M, Mikolaenko I, Britt WJ, Bland KI, Cobbs CS. Specific localisation of human cytomegalovirus nucleic acids and proteins in human colorectal cancer. Lancet. 2002, 360, 1557–1563. [Google Scholar] [CrossRef]
- Michaelis M, Doerr HW, Cinatl J. The story of human cytomegalovirus and cancer: increasing evidence and open questions. Neoplasia. 2009, 11, 1–9. [Google Scholar] [CrossRef]
- Costa H, Xu X, Overbeek G, Vasaikar S, Patro CP, Kostopoulou ON, Jung M, Shafi G, Ananthaseshan S, Tsipras G, Davoudi B, Mohammad AA, Lam H, Strååt K, Wilhelmi V, Shang M, Tegner J, Tong JC, Wong KT, Söderberg-Naucler C, Yaiw KC. Human cytomegalovirus may promote tumor progression by upregulating arginase-2. Oncotarget. 2016, 7, 47221–47231. [Google Scholar] [CrossRef] [PubMed]
- Cobbs CS, Harkins L, Samanta M, Gillespie GY, Bharara S, King PH, Nabors LB, Cobbs CG, Britt WJ. Human cytomegalovirus infection and expression in human malignant glioma. Cancer Res. 2002, 62, 3347–3350. [Google Scholar]
- Joseph GP, McDermott R, Baryshnikova MA, Cobbs CS, Ulasov IV. Cytomegalovirus as an oncomodulatory agent in the progression of glioma. Cancer Lett. 2017, 384, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Farias KPRA, Moreli ML, Floriano VG, da Costa VG. Evidence based on a meta-analysis of human cytomegalovirus infection in glioma. Arch Virol. 2019, 164, 1249–1257. [Google Scholar] [CrossRef]
- Bhattacharjee B, Renzette N, Kowalik TF. Genetic analysis of cytomegalovirus in malignant gliomas. J Virol. 2012, 86, 6815–6824. [Google Scholar] [CrossRef] [PubMed]
- Maleki F, Sadigh ZA, Sadeghi F, Muhammadnejad A, Farahmand M, Parvin M, Shirkoohi R. Human cytomegalovirus infection in Iranian glioma patients correlates with aging and tumor aggressiveness. J Med Virol. 2020, 92, 1266–1276. [Google Scholar] [CrossRef] [PubMed]
- Yang T, Liu D, Fang S, Ma W, Wang Y. Cytomegalovirus and Glioblastoma: A Review of the Biological Associations and Therapeutic Strategies. Journal of Clinical Medicine. 2022, 11, 5221. [Google Scholar] [CrossRef]
- Libard S, Popova S. N., Amini R.-M, Kärjä V, Pietiläinen T, Hämäläinen K.M., Sundström C, Hesselager G, Bergqvist M, Ekman S, et al. Human Cytomegalovirus Tegument Protein pp65 Is Detected in All Intra- and Extra-Axial Brain Tumours Independent of the Tumour Type or Grade. PLoS ONE 2014, 9, e108861. [Google Scholar]
- Habibi Z, Hajizadeh M, Nozarian Z, Safavi M, Monajemzadeh M, Meybodi KT, Nejat F, Vasei M. Cytomegalovirus DNA in non-glioblastoma multiforme brain tumors of infants. Childs Nerv Syst. 2021, 37, 1581–1586. [Google Scholar] [CrossRef]
- Ranganathan P, Clark PA, Kuo JS, Salamat MS, Kalejta RF. Significant association of multiple human cytomegalovirus genomic Loci with glioblastoma multiforme samples. J Virol. 2012, 86, 854–864. [Google Scholar] [CrossRef]
- Carpagnano GE, Lacedonia D, Natalicchio MI, Cotugno G, Zoppo L, Martinelli D, Antonetti R, Foschino-Barbaro MP. Viral colonization in exhaled breath condensate of lung cancer patients: Possible role of EBV and CMV. Clin Respir J. 2018, 12, 418–424. [Google Scholar] [CrossRef]
- Nelson HH, Contestabile E, Hunter-Schlichting D, Koestler D, Pawlita M, Waterboer T, Christensen BC, Petersen CL, Miller JS, Kelsey KT. Human cytomegalovirus alters immune cell profile with potential implications for patient survival in head and neck cancer. Carcinogenesis. 2022, 43, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Lv YL, Han FF, An ZL, Jia Y, Xuan LL, Gong LL, Zhang W, Ren LL, Yang S, Liu H, Liu LH. Cytomegalovirus Infection Is a Risk Factor in Gastrointestinal Cancer: A Cross-Sectional and Meta-Analysis Study. Intervirology. 2020;63(1-6):10-16. [CrossRef]
- Samanta M, Harkins L, Klemm K, Britt WJ, Cobbs CS. High prevalence of human cytomegalovirus in prostatic intraepithelial neoplasia and prostatic carcinoma. J Urol. 2003, 170, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Stevenson K, Macnab JC. Cervical carcinoma and human cytomegalovirus. Biomed Pharmacother. 1989, 43, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Gaekwad SS, Gujjari SK. Cytomegalovirus occurrence in chronic periodontitis and in carcinoma of the cervix: an exploratory study. J Clin Diagn Res. 2012, 6, 1442–1447. [Google Scholar] [CrossRef]
- Yin M, Chen A, Zhao F, Ji X, Li C, Wang G. Detection of human cytomegalovirus in patients with epithelial ovarian cancer and its impacts on survival. Infect Agent Cancer. 2020, 15, 23. [Google Scholar] [CrossRef]
- D’Orazi G, Cordani M, Cirone M. Oncogenic pathways activated by pro-inflammatory cytokines promote mutant p53 stability: clue for novel anticancer therapies. Cell Mol Life Sci. 2021, 78, 1853–1860. [Google Scholar] [CrossRef]
- Grivennikov SI, Karin M. Inflammation and oncogenesis: a vicious connection. Curr Opin Genet Dev. 2010, 20, 65–71. [Google Scholar] [CrossRef]
- Greten FR, Grivennikov SI. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity. 2019, 51, 27–41. [Google Scholar] [CrossRef]
- Qu X, Tang Y, Hua S. Immunological Approaches Towards Cancer and Inflammation: A Cross Talk. Front Immunol. 2018, 9, 563. [Google Scholar] [CrossRef] [PubMed]
- Singh N, Baby D, Rajguru JP, Patil PB, Thakkannavar SS, Pujari VB. Inflammation and cancer. Ann Afr Med. 2019, 18, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Balkwill F, Charles KA, Mantovani A. Smoldering and polarized inflammation in the initiation and promotion of malignant disease. Cancer Cell. 2005, 7, 211–217. [Google Scholar] [CrossRef]
- Colotta F, Allavena P, Sica A, Garlanda C, Mantovani A. Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis. 2009, 30, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 140(6):883–99.
- Michaelis M, Doerr HW, Cinatl J Jr. Oncomodulation by human cytomegalovirus: evidence becomes stronger. Med Microbiol Immunol. 2009, 198, 79–81. [Google Scholar] [CrossRef]
- Herbein, G. High-Risk Oncogenic Human Cytomegalovirus. Viruses. 2022, 14, 2462. [Google Scholar] [CrossRef]
- Cinatl J Jr, Vogel JU, Kotchetkov R, Wilhelm Doerr H. Oncomodulatory signals by regulatory proteins encoded by human cytomegalovirus: a novel role for viral infection in tumor progression. FEMS Microbiol Rev. 2004, 28, 59–77. [Google Scholar] [CrossRef]
- Goerig NL, Frey B, Korn K, Fleckenstein B, Überla K, Schmidt MA, Dörfler A, Engelhorn T, Eyüpoglu I, Rühle PF, Putz F, Semrau S, Gaipl US, Fietkau R. Frequent occurrence of therapeutically reversible CMV-associated encephalopathy during radiotherapy of the brain. Neuro Oncol. 2016, 18, 1664–1672. [Google Scholar] [CrossRef]
- Merchut-Maya JM, Bartek J Jr, Bartkova J, Galanos P, Pantalone MR, Lee M, Cui HL, Shilling PJ, Brøchner CB, Broholm H, Maya-Mendoza A, Söderberg-Naucler C, Bartek J. Human cytomegalovirus hijacks host stress response fueling replication stress and genome instability. Cell Death Differ. 2022, 29, 1639–1653. [Google Scholar] [CrossRef]
- Yang R, Liang J, Xu GX, Ding LM, Huang HM, Su QZ, Yan J, Li YC. Human cytomegalovirus glycoprotein B inhibits migration of breast cancer MDA-MB-231 cells and impairs TGF-β/Smad2/3 expression. Oncol Lett. 2018, 15, 7730–7738. [Google Scholar] [CrossRef]
- Geisler J, Touma J, Rahbar A, Söderberg-Nauclér C, Vetvik K. A Review of the Potential Role of Human Cytomegalovirus (HCMV) Infections in Breast Cancer Carcinogenesis and Abnormal Immunity. Cancers (Basel). 2019, 11, 1842. [Google Scholar] [CrossRef] [PubMed]
- Herbein, G. The Human Cytomegalovirus, from Oncomodulation to Oncogenesis. Viruses. 2018, 10, 408. [Google Scholar] [CrossRef] [PubMed]
- Cobbs, CS. Cytomegalovirus is a tumor-associated virus: armed and dangerous. Curr Opin Virol. 2019, 39, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Roche, J. The Epithelial-to-Mesenchymal Transition in Cancer. Cancers (Basel). 2018, 10, :52. [Google Scholar] [CrossRef] [PubMed]
- Marcucci F, Stassi G, De Maria R. Epithelial-mesenchymal transition: a new target in anticancer drug discovery. Nat Rev Drug Discov. 2016, 15, 311–325. [Google Scholar] [CrossRef]
- Maussang D, Verzijl D, van Walsum M, Leurs R, Holl J, Pleskoff O, Michel D, van Dongen GA, Smit MJ. Human cytomegalovirus-encoded chemokine receptor US28 promotes tumorigenesis. Proc Natl Acad Sci U S A. 2006, 103, :13068–73. [Google Scholar] [CrossRef]
- Wang, J. , Belcher, J., Marker, P. et al. Cytomegalovirus inhibits p53 nuclear localization signal function. J Mol Med 78, 642–647 (2001). [CrossRef]
- Hecker M, Qiu D, Marquardt K, Bein G, Hackstein H. Continuous cytomegalovirus seroconversion in a large group of healthy blood donors. Vox Sang. 2004, 86, 41–44. [Google Scholar] [CrossRef]
- Staras SAS, Dollard SC, Radford KW, Flanders WD, Pass RF, Cannon MJ. Seroprevalence of cytomegalovirus infection in the United States, 1988- 1994. Clin Infect Dis. 2006, 43, 1143–1151. [CrossRef]
- Ahlfors, K. IgG antibodies to cytomegalovirus in a normal urban Swedish population. Scand J Infect Dis. 1984, 16, 335–337. [Google Scholar] [CrossRef]
- Varga M, Görög D, Kári D, Környei E, Kis É, Túryné HJ, et al. Cytomegalovirus seroprevalence among solid organ donors in Hungary: correlations with age, gender, and blood group. Transplant Proc. 2011, 43, 1233–1235. [Google Scholar] [CrossRef] [PubMed]
- Bate SL, Dollard SC, Cannon MJ. Cytomegalovirus seroprevalence in the United States: the national health and nutrition examination surveys, 1988-2004. Clin Infect Dis. 2010, 50, 1439–1447. [CrossRef] [PubMed]
- Lachmann R, Loenenbach A, Waterboer T, Brenner N, Pawlita M, Michel A, et al. Cytomegalovirus (CMV) seroprevalence in the adult population of Germany. PLoS One. 2018, 13, e0200267. [Google Scholar] [CrossRef]
- Cannon MJ, Schmid DS, Hyde TB. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev Med Virol. 2010, 20, 202–213. [Google Scholar] [CrossRef]
- Marshall GS, Rabalais GP, Stewart JA, Dobbins JG. Cytomegalovirus seroprevalence in women bearing children in Jefferson County, Kentucky. Am J Med Sci. 1993, 305, 292–296. [Google Scholar] [CrossRef]
- Clarke CA, Glaser SL, Gomez SI, Wang SS, Keegan TH, Yang J, et al. Lymphoid malignancies in US Asians: incidence rate differences by birthplace and acculturation. Cancer Epidemiol Biomarkers Prev. 2011, 20, 1064–1077. [Google Scholar] [CrossRef]
- Li Y, Wang Z, Yi D, Ma S. Racial Differences in Three mayor NHL Subtypes: Descriptive epidemiology. Cancer Epidemiol. 2015, 39, 8–13. [Google Scholar] [CrossRef]
- Janković M, Milićević O, Todorović-Balint M, Đunić I, Mihaljević B, Jovanović T, Knežević A. Cytomegalovirus seropositivity relates inversely to cancer incidences across races and ethnicities: implications for oncoprevention. medRxiv 2023.08.26.23294534. [CrossRef]
Figure 1.
The graph represents CMV seroprevalences plotted against annual age-standardized cancer incidence rates for 73 countries (per 100 000) population. The statistically significant and inverse correlation between the two parameters (Spearman’s ρ = -0.732; p<0.001) suggests a possible oncopreventive role of CMV: with a higher prevalence of the virus comes a lower incidence of tumors.
Figure 1.
The graph represents CMV seroprevalences plotted against annual age-standardized cancer incidence rates for 73 countries (per 100 000) population. The statistically significant and inverse correlation between the two parameters (Spearman’s ρ = -0.732; p<0.001) suggests a possible oncopreventive role of CMV: with a higher prevalence of the virus comes a lower incidence of tumors.
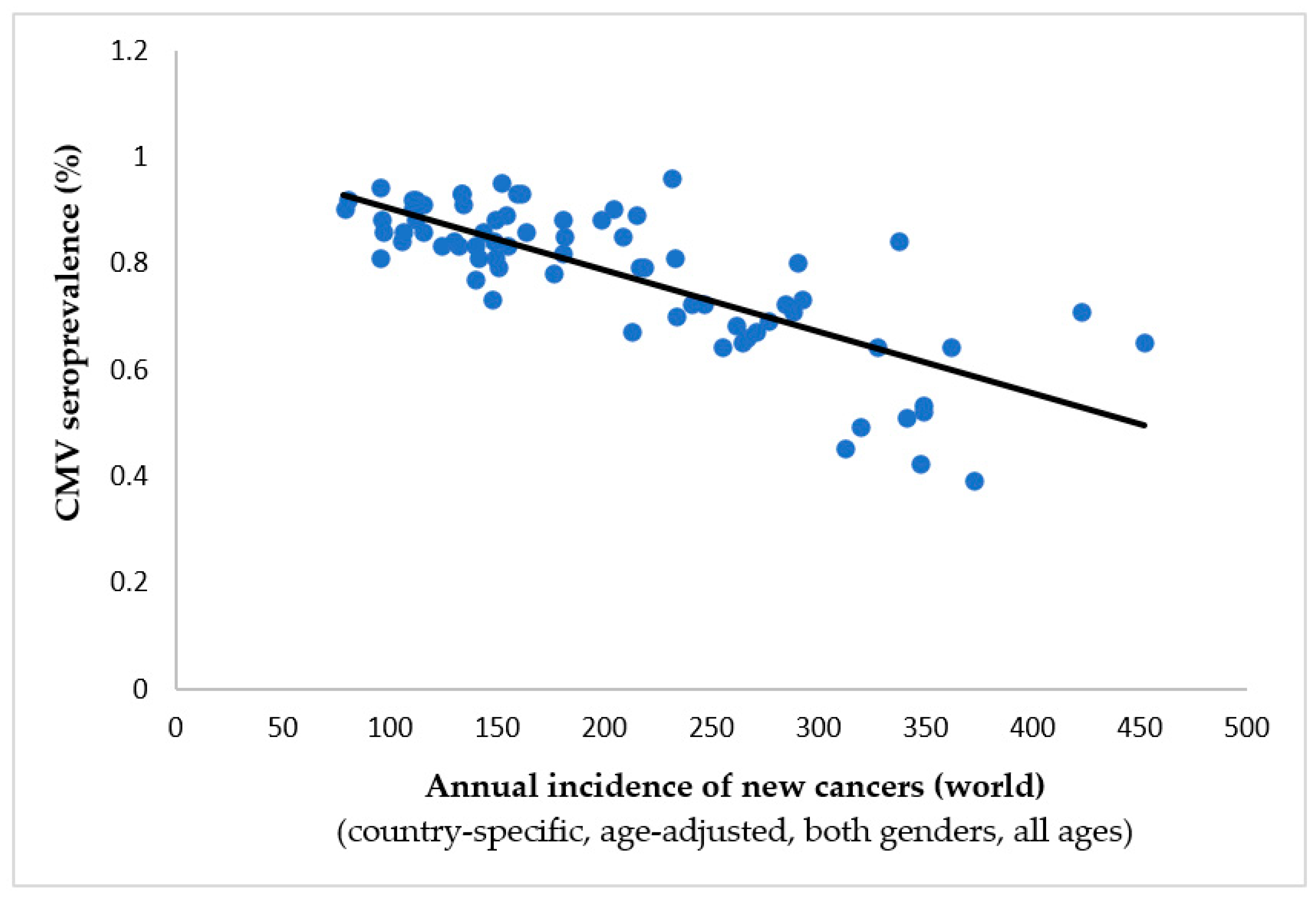
Figure 2.
Annual incidence for Kaposi’s sarcoma plotted against country specific CMV seroprevalence (Spearman’s ρ = -0.007, p = 0.953). In contrast to the inverse correlation noted between the pervasiveness of CMV and the overall cumulative tumor incidence rates (as seen in Figure 1), there is no discernible link in this case. This implies that CMV does not provide protection against cancer in this particular scenario.
Figure 2.
Annual incidence for Kaposi’s sarcoma plotted against country specific CMV seroprevalence (Spearman’s ρ = -0.007, p = 0.953). In contrast to the inverse correlation noted between the pervasiveness of CMV and the overall cumulative tumor incidence rates (as seen in Figure 1), there is no discernible link in this case. This implies that CMV does not provide protection against cancer in this particular scenario.
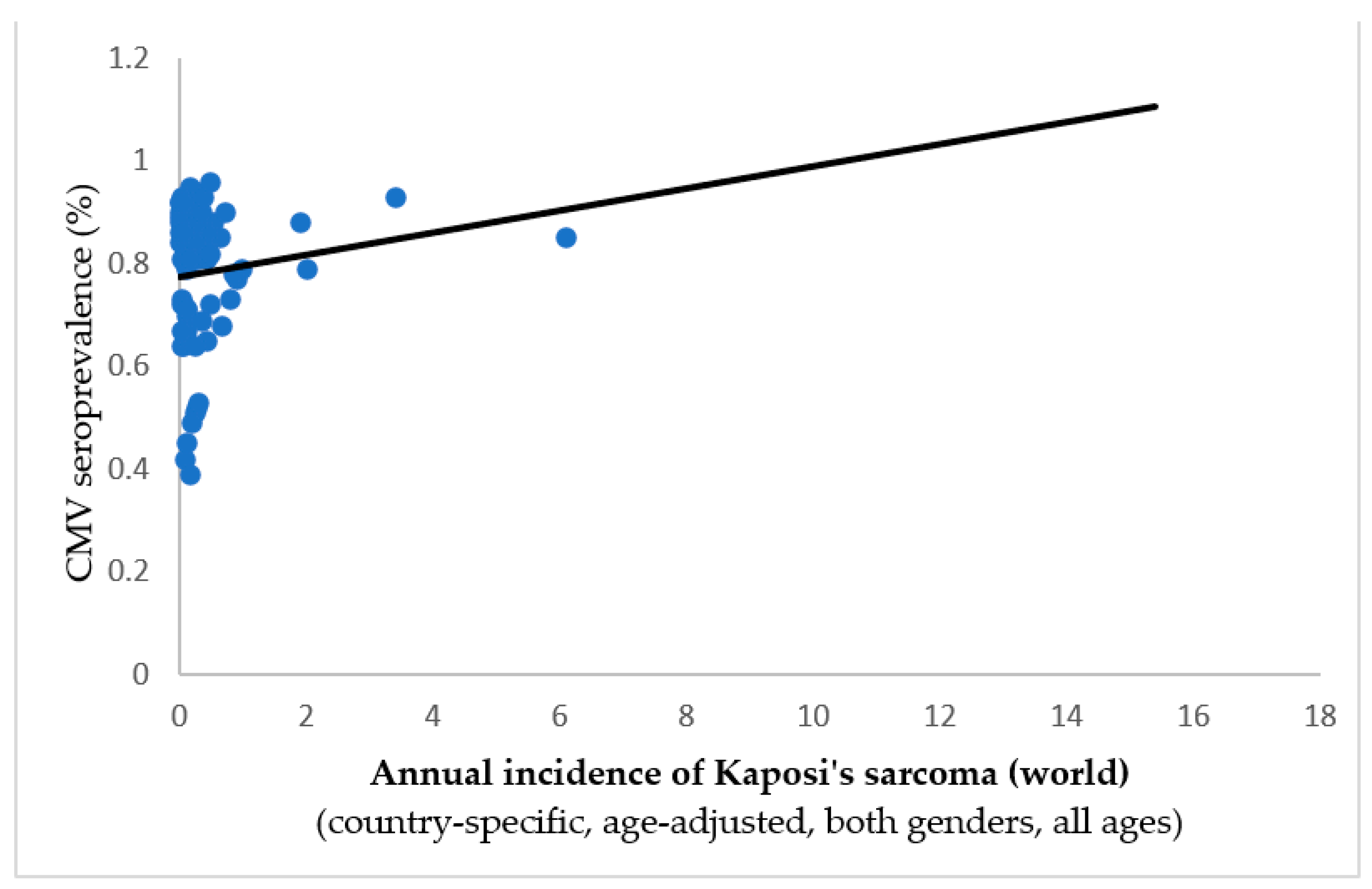
Figure 3.
The chart illustrates the relationship between CMV seroprevalence and the incidence rates of nasopharyngeal carcinoma in 73 countries across the globe. This stands out as one of just two types of cancer where a significant and positive connection has been identified at the country level (Spearman’s ρ = +0.266, p = 0.023), suggesting a potential carcinogenic impact of CMV in this particular case.
Figure 3.
The chart illustrates the relationship between CMV seroprevalence and the incidence rates of nasopharyngeal carcinoma in 73 countries across the globe. This stands out as one of just two types of cancer where a significant and positive connection has been identified at the country level (Spearman’s ρ = +0.266, p = 0.023), suggesting a potential carcinogenic impact of CMV in this particular case.
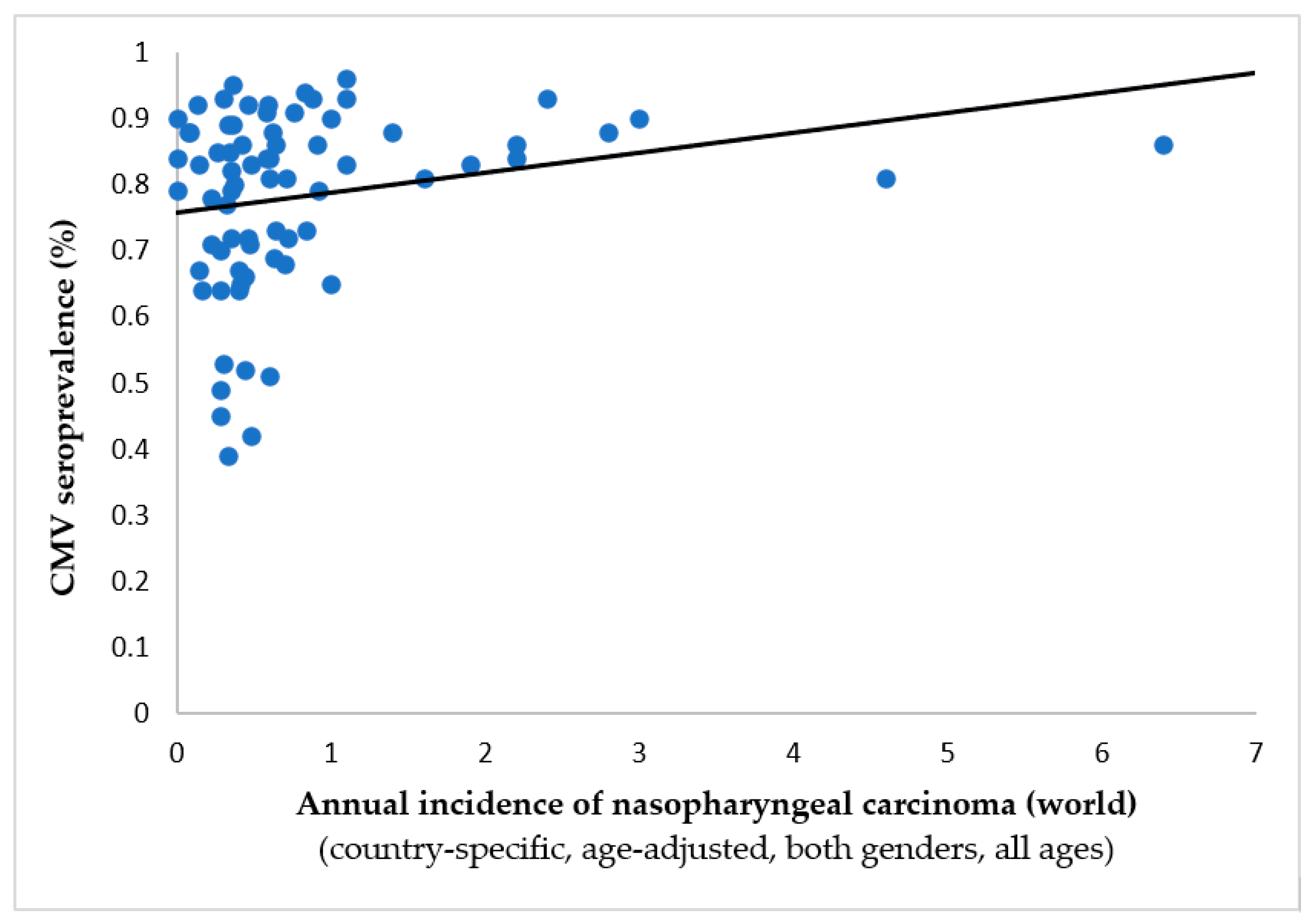

Table 1.
Predominant tumors as documented by the World Health Organization’s GLOBOCAN, along with their connection to global CMV prevalence. An inverse correlation suggests that CMV provides oncoprotection—as CMV prevalence increases, tumor incidence decreases. Asterisks denote statistically significant correlations.
Table 1.
Predominant tumors as documented by the World Health Organization’s GLOBOCAN, along with their connection to global CMV prevalence. An inverse correlation suggests that CMV provides oncoprotection—as CMV prevalence increases, tumor incidence decreases. Asterisks denote statistically significant correlations.
| Tumor/localization | Spearman’s ρ | p-value | Inverse correlation to CMV prevalence |
|---|---|---|---|
|
-0.763 | 0.001* | Yes |
|
-0.754 | 0.001* | Yes |
|
-0.732 | 0.001* | Yes |
|
-0.726 | 0.001* | Yes |
|
-0.719 | 0.001* | Yes |
|
-0.711 | 0.001* | Yes |
|
-0.692 | 0.001* | Yes |
|
-0.671 | 0.001* | Yes |
|
-0.665 | 0.001* | Yes |
|
-0.663 | 0.001* | Yes |
|
-0.656 | 0.001* | Yes |
|
-0.651 | 0.001* | Yes |
|
-0.633 | 0.001* | Yes |
|
-0.633 | 0.001* | Yes |
|
-0.632 | 0.001* | Yes |
|
-0.618 | 0.001* | Yes |
|
-0.617 | 0.001* | Yes |
|
-0.574 | 0.001* | Yes |
|
-0.551 | 0.001* | Yes |
|
-0.548 | 0.001* | Yes |
|
-0.541 | 0.001* | Yes |
|
-0.532 | 0.001* | Yes |
|
-0.519 | 0.001* | Yes |
|
-0.461 | 0.001* | Yes |
|
-0.432 | 0.001* | Yes |
|
-0.377 | 0.001* | Yes |
|
-0.35 | 0.002* | Yes |
|
0.316 | 0.006* | No |
|
0.266 | 0.023* | No |
|
-0.224 | 0.056 | Yes |
|
-0.165 | 0.164 | Yes |
|
-0.149 | 0.208 | Yes |
|
0.118 | 0.319 | No |
|
-0.085 | 0.473 | Yes |
|
-0.007 | 0.953 | Yes |
|
0.007 | 0.951 | No |
* Adapted from: Jankovic et al. (2023), preprint, medRxiv.org [134].
Table 2.
Tumor incidence rates across different age categories (in 10-year intervals) are correlated with country-specific CMV prevalence to investigate the potential oncoprotective role of CMV. We highlight p-values that support oncoprotection, indicating a significant and inverse correlation between viral prevalence and age-standardized tumor incidence rates, by color-coding them in green for easy reference. Conversely, p-values suggesting a pro-oncogenic effect are marked in red. Tumors with at least one age category indicating a potential and significant anti-tumor effect of CMV are identified with a † symbol. Note that the oncoprotective effect is somewhat skewed towards older populations in many tumors.
Table 2.
Tumor incidence rates across different age categories (in 10-year intervals) are correlated with country-specific CMV prevalence to investigate the potential oncoprotective role of CMV. We highlight p-values that support oncoprotection, indicating a significant and inverse correlation between viral prevalence and age-standardized tumor incidence rates, by color-coding them in green for easy reference. Conversely, p-values suggesting a pro-oncogenic effect are marked in red. Tumors with at least one age category indicating a potential and significant anti-tumor effect of CMV are identified with a † symbol. Note that the oncoprotective effect is somewhat skewed towards older populations in many tumors.
| Tumor* | Statistical measures | Age intervals (years) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0-9 | 10-19 | 20-29 | 30-39 | 40-49 | 50-59 | 60-69 | ≥70 | ||
| Gallbladder | Spearman’s ρ | N/A | .154 | .297 | .394 | .416 | .423 | .290 | .147 |
| p-value | N/A | .193 | .011 | .001 | <.001 | <.001 | .013 | .215 | |
| Bladder† | Spearman’s ρ | -.082 | .120 | -.185 | -.167 | -.254 | -.427 | -.517 | -.552 |
| p-value | .490 | .311 | .118 | .158 | .030 | <.001 | <.001 | <.001 | |
| Colorectum† | Spearman’s ρ | .089 | -.394 | -.205 | -.373 | -.604 | -.648 | -.648 | -.662 |
| p-value | .452 | .001 | .082 | .001 | <.001 | <.001 | <.001 | <.001 | |
| Kaposi’s sarcoma† | Spearman’s ρ | -.642 | .218 | -.083 | -.242 | -.101 | .044 | .006 | .031 |
| p-value | <.001 | .064 | .486 | .040 | .394 | .709 | .959 | .792 | |
| Cervix uteri† | Spearman’s ρ | -.016 | -.017 | -.427 | -.220 | .036 | .249 | .373 | .400 |
| p-value | .895 | .884 | <.001 | .061 | .761 | .034 | .001 | <.001 | |
| Corpus uteri† | Spearman’s ρ | -.196 | -.071 | -.180 | -.294 | -.576 | -.644 | -.672 | -.655 |
| p-value | .096 | .549 | .128 | .012 | <.001 | <.001 | <.001 | <.001 | |
| Hypopharynx† | Spearman’s ρ | .050 | .205 | .307 | .187 | -.235 | -.335 | -.425 | -.378 |
| p-value | .674 | .081 | .008 | .114 | .045 | .004 | <.001 | .001 | |
| Larynx† | Spearman’s ρ | .377 | .219 | .359 | .047 | -.103 | -.212 | -.236 | -.004 |
| p-value | .001 | .063 | .002 | .693 | .388 | .072 | .045 | .972 | |
| Lip/Oral† | Spearman’s ρ | .375 | .244 | -.218 | -.438 | -.501 | -.536 | -.528 | -.528 |
| p-value | .001 | .038 | .064 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Liver† | Spearman’s ρ | -.378 | .076 | .239 | .353 | .088 | -.056 | -.071 | .057 |
| p-value | .001 | .523 | .042 | .002 | .458 | .639 | .548 | .631 | |
| Lung† | Spearman’s ρ | -.092 | -.120 | -.312 | -.308 | -.373 | -.558 | -.579 | -.501 |
| p-value | .438 | .311 | .007 | .008 | .001 | <.001 | <.001 | <.001 | |
| Melanoma† | Spearman’s ρ | -.242 | -.692 | -.769 | -.786 | -.746 | -.749 | -.722 | -.722 |
| p-value | .039 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Mesothelioma† | Spearman’s ρ | .129 | -.090 | .076 | -.235 | -.373 | -.516 | -.544 | -.595 |
| p-value | .278 | .448 | .524 | .045 | .001 | <.001 | <.001 | <.001 | |
| Non-melanoma skin cancer† | Spearman’s ρ | .173 | -.099 | -.345 | -.411 | -.531 | -.589 | -.633 | -.709 |
| p-value | .144 | .403 | .003 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Nasopharynx | Spearman’s ρ | .210 | .233 | .157 | .138 | .184 | .150 | .138 | .425 |
| p-value | .074 | .047 | .185 | .246 | .119 | .204 | .244 | <.001 | |
| Oropharynx† | Spearman’s ρ | .389 | .239 | .180 | -.423 | -.582 | -.643 | -.657 | -.611 |
| p-value | .001 | .042 | .127 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Esophagus† | Spearman’s ρ | .298 | .406 | .208 | .192 | -.091 | -.211 | -.243 | -.025 |
| p-value | .011 | <.001 | .077 | .104 | .445 | .073 | .039 | .833 | |
| Pancreas† | Spearman’s ρ | .052 | -.230 | -.155 | -.360 | -.594 | -.649 | -.620 | -.611 |
| p-value | .662 | .050 | .189 | .002 | <.001 | <.001 | <.001 | <.001 | |
| Penis† | Spearman’s ρ | .171 | -.021 | .037 | -.188 | -.317 | -.337 | -.453 | -.495 |
| p-value | .148 | .863 | .756 | .112 | .006 | .004 | <.001 | <.001 | |
| Prostate† | Spearman’s ρ | -.058 | .029 | .185 | -.126 | -.602 | -.663 | -.708 | -.542 |
| p-value | .628 | .807 | .118 | .289 | <.001 | <.001 | <.001 | <.001 | |
| Salivary glands† | Spearman’s ρ | .198 | -.078 | -.226 | -.276 | -.417 | -.359 | -.126 | -.429 |
| p-value | .093 | .509 | .055 | .018 | <.001 | .002 | .287 | <.001 | |
| Testis† | Spearman’s ρ | -.319 | -.653 | -.694 | -.707 | -.728 | -.728 | -.486 | -.097 |
| p-value | .006 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | .415 | |
| Thyroid† | Spearman’s ρ | -.266 | -.489 | -.467 | -.491 | -.499 | -.550 | -.544 | -.363 |
| p-value | .023 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | .002 | |
| Vulva† | Spearman’s ρ | .044 | -.003 | -.192 | -.384 | -.549 | -.544 | -.642 | -.745 |
| p-value | .709 | .980 | .103 | .001 | <.001 | <.001 | <.001 | <.001 | |
| All cancers† | Spearman’s ρ | -.642 | -.672 | -.731 | -.784 | -.756 | -.726 | -.720 | -.678 |
| p-value | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Vagina† | Spearman’s ρ | -.033 | .126 | <.001 | -.125 | -.257 | -.103 | -.189 | -.376 |
| p-value | .785 | .287 | .999 | .291 | .028 | .385 | .110 | .001 | |
| Stomach | Spearman’s ρ | .283 | .145 | .079 | .039 | -.042 | -.055 | -.081 | -.097 |
| p-value | .015 | .221 | .504 | .746 | .723 | .644 | .496 | .413 | |
| Ovary† | Spearman’s ρ | -.121 | -.181 | -.071 | -.188 | -.284 | -.395 | -.517 | -.454 |
| p-value | .308 | .124 | .551 | .111 | .015 | .001 | <.001 | <.001 | |
| Brain/CNS† | Spearman’s ρ | -.649 | -.577 | -.654 | -.607 | -.529 | -.477 | -.455 | -.452 |
| p-value | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| All cancers excl. non-melanoma skin† | Spearman’s ρ | -.645 | -.667 | -.733 | -.785 | -.753 | -.726 | -.717 | -.656 |
| p-value | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Breast† | Spearman’s ρ | .050 | .182 | -.239 | -.645 | -.674 | -.696 | -.700 | -.661 |
| p-value | .674 | .124 | .042 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Kidney† | Spearman’s ρ | -.493 | -.016 | -.365 | -.693 | -.736 | -.731 | -.728 | -.744 |
| p-value | <.001 | .893 | .002 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Hodgkin lymphoma† | Spearman’s ρ | .174 | -.622 | -.676 | -.681 | -.575 | -.478 | -.389 | -.229 |
| p-value | .141 | <.001 | <.001 | <.001 | <.001 | <.001 | .001 | .051 | |
| Non-Hodgkin lymphoma† | Spearman’s ρ | -.036 | -.005 | -.437 | -.590 | -.593 | -.618 | -.610 | -.552 |
| p-value | .762 | .968 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | |
| Multiple myeloma† | Spearman’s ρ | .235 | .110 | .055 | -.356 | -.483 | -.577 | -.644 | -.627 |
| p-value | .045 | .355 | .645 | 0.002 | <.001 | <.001 | <.001 | <.001 | |
| Leukemia† | Spearman’s ρ | -.495 | -.236 | .108 | -.165 | -.472 | -.630 | -.645 | -.543 |
| p-value | <.001 | .044 | .364 | .164 | <.001 | <.001 | <.001 | <.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



