Submitted:
30 September 2023
Posted:
01 October 2023
You are already at the latest version
Abstract
The number of people affected by eye conditions is growing every year, due to the popularity of electronic devices and an aging population. In the world of medicine, accomplishing eye medication administration has always been a difficult task. Despite the fact that there are many eye drops on the market, most of them have important limitations due to quick clearance mechanisms and ocular barriers. One solution with tremendous potential is the contact lens used as medication delivery vehicle to bypass this constraint. Therapeutic contact lenses for ocular medication delivery have attracted a lot of attention because they have the potential to improve ocular bioavailability, patient compliance, and reduce side effects. However, it is essential not to compromise essential features such as water content, optical transparency, and modulus in order to target successful in vitro and in vivo sustained drug delivery profile from impregnated contact lenses. Aside from difficulties like drug stability and burst release, the changing of lens physical and chemical properties caused by therapeutic or non-therapeutic components can limit the commercialization potential of pharmaceutical-loaded lenses. Research has progressed towards bioinspired techniques and smart materials to improve the efficacy of drug-eluting contact lenses. The bioinspired method uses bioinspired polymeric materials to improve biocompatibility, a specialized molecule recognition technique called molecular imprinting, or a stimuli-responsive system to improve biocompatibility and support drug delivery efficacy of drug-eluting contact lenses. This review encompasses strategies of material design, lens manufacturing and drug impregnation under the current auspices in ophthalmic therapies and projects an outlook onto future opportunities in the field of eye conditions management by means of active principles-eluting contact lens.
Keywords:
contact lens
; drug delivery
; bioavailability
; composite
; gas-permeable
; hydrogel
1. Introduction
In their landmark Patent 3,220,960 issued in 1965, Otto Wichterle and Drahoslav Lim pioneered the notion of administering medications via contact lenses, which led to the development of the poly (2-hydroxyethyl methacrylate) (PHEMA)-based contact lens. The inventors described the diffusion of antibacterial boric acid through PHEMA devices, including lenses, for later release to the [1]. Following this discovery, some early exploratory experiments focused on soaking contact lens in a drug solution, then inserting the lens into the eye [2]. Since then, contact lenses with drug release for therapeutic purposes have become one of the most promising platforms for improving bioavailability of ophthalmic drugs, which play an important role in the treatment of corneal and ocular surface diseases (OSDs).
Topical, intracameral, subconjunctival, retrobulbar, and systemic routes of administration are some available methods for the treatment of eye conditions. Topical administration, which includes eye drops and ointments, is a non-invasive and frequently employed method of treating anterior segment illnesses, accounting for more than 90% of all ophthalmic formulations [2]. Because of the high turnover rate and restoration time of the tear film, topically applied eye drops are quickly washed out into the nasolacrimal duct and removed by scleral blood and lymphatic drainage [3].As a result, only 1–5% of the injected medication is received by the target tissue, and the bioavailability for drug delivery to the anterior chamber is less than 5% for lipophilic molecules and less than 0.5 percent for hydrophilic molecules [4]. To counteract for the limited bioavailability, eye drops must be administered often, which may lead to poor patient compliance, especially in chronic ocular illnesses as glaucoma and dry eye disease [5].
Contact lenses, in this setting, became drug-releasing devices that essentially transcend the aforementioned constraints while also providing additional benefits. As a result, the use of contact lenses as drug-carrier systems has been intensively studied in recent years owing to the potential to maximize bioavailability, hence improving efficiency and therapeutic compliance [5]. Based on the material used in preparation, contact lenses may be classified as hard or soft. Hard lenses are often constructed of a rigid gas permeable material, while soft contact lenses are made of a flexible hydrogelthat permits oxygen to cross through to the cornea [6]. They provide pain relief, hydrating the corneal epithelium, improving corneal wound healing, and forming a mechanical barrier between the cornea and the external environment. Bullous keratopathy, corneal erosions, corneal epithelial abnormalities, and postsurgical diseases such as post-keratoplasty and post–laser vision correction are all treated using therapeutic lenses [7].
Designing enhanced therapeutic contact lenses is quite a tricky task, since most of the paths chosen by scientists when researching for better materials often includes taking the trial-and-error approach. Trial-and-error means time consuming experiments which can lead to nothing newly discovered the majority of the times. It also includes costly procedures and repetitive tasks that waste valuable time and also financial resources that could be used in other better ways within the R&D process.
Computer simulations, on the other hand, have proved to be a good fit for choosing and adjusting appropriate biomaterials when trying to develop new medical devices. They are also a match to imaging in bio-nanotechnology, spanning the length scale well and temporal scales up to several nanoseconds for atomic level descriptions and much longer for coarser descriptions. Recent developments in computer hardware and software, as well as the introduction of multi-scale simulation methodologies, have enabled the progress in the design of new medical devices with improved properties [8,9,10].
A combined approach, computer simulations and real design, allows scientists to adjust certain parameters based on the most promising in silico results in order to meet real-world clinical needs. Such achievements are being realized primarily because molecular modeling is able to generate nanoscale pictures with atomic and even electronic resolution, to predict the nanoscale mechanisms of new biological and inorganic materials for biomedical applications [11,12].
With the fast development of computer simulation and complex actual design /research and technology was provided feasible way to analyze complex system behavior and evaluate the intervention effects and resulted in great progress in therapeutic contact lenses [13].
The aforementioned combined approaches allowed the obtainment of effective designs able to maintain therapeutic concentrations of medication on the ocular tissue and arebecoming the most common ophthalmic drug administration [7].
Accordingly, the novel developed TCLs are successful for corneal and OSDs care however contraindications and complications such as infective keratitis, corneal anesthesia, corneal hypoxia, corneal allergies and inflammation, unsustained drug release, and poor lens fit are some of the main challenges that still has to considered [7].
Some excellent review papers of CLs fabrication and application were recently published and are providing a comprehensive overview of the most successful materials, preparation methodologies, and recent achievements on OSDs care [14,15,16].
Thanks to rapid advancement of the field, complex TCLs which display drug release over an extended period based on new materials obtained by sophisticated fabrication techniques were lately proposed. This updated review presents the various materials and techniques to fabricate and deliver drugs through CLs and goes one step further examining their advantages and shortcomings. First, the different materials adopted to tune the release profile of the CLs are addressed. Subsequently, manufacturing methods for producing TCLs that contain and release active ingredients followed by the latest scientific results which demonstrate the potential of these ground-breaking noninvasive drug delivery systems are largely discussed. Another main goal is to overviewthe latest advances in the treatment and/or prophylaxis of eye pathologies (i.e., glaucoma, cataract, corneal diseases, and keratoconus) by TCLs. In addition, this review discusses the latest developments in novel therapies for keratoconus condition. The last but not the least the current paper it gives an overview of the future perspectives and challenges in the field of TCLs for OSDs.
2. Material design and contact lenses fabrication
2.1. Main Materials used in contact lenses fabrication
Current ocular treatments are outperformed by contemporary contact lenses materials in terms of drug delivery. It is necessary to further modify the base polymer structure of these devices in order to support and enhance the therapeutic outcome [17]. The most prevalent alteration techniques are molecular grafts, particle encapsulation, and soaking [18]. Despite proof of the improved performance of these materials, additional work is required to bring them to the stage of commercialization. The greatest market hurdle is the cost of clinical trials and the manufacturing needs.
However, the functionalities of a material used for contact lenses fabrication can be employed as multifunctional drug-binding mechanisms. For instance, the insertion of ionic monomers can generate binding sites for a polar medication, allowing the lens to hold the drug until it is administered to the eye [2].
Double-network/interpenetrating hydrogels and pH-responsive polymers are two classes of materials that have experienced rapid growth. Although there has been considerable interest in areas such as liquid crystal contact lenses [19,20,21], the number of research articles in these areas remains relatively low in comparison to other technologies.
Double-network/interpenetrating hydrogels create a new composite gel by linking the gel networks of two gels [22]. Instead of a typical copolymer gel, the network of one gel is interlaced with the network of the other gel. This is a small but essential distinction; for instance, two polymers having different functional groups, meaning they cannot be copolymerized, could create a double network gel whose density could be tweaked in order to support optimal ophthalmic bioactive molecules [23]. Figure 1A exhibits a schematic representation of different hydrogels structure, demonstrating the main structure difference between traditional single polymer networks, double-network and cross-linked double network. Temperature- and pH-responsive hydrogels are based one macromolecules whose conformational shape change when exposed to a certain temperature or acidic/basic conditions. pH variations in the body (e.g. caused by inflammation [24]) induces protonation, and therefore conformational changes in the polymer, enabling the release of the drug. As such, their potential as drug-delivery mechanisms for biomedical devices growing [24,25,26]. Figure 1B, C exhibits a schematic representation pH-responsive hydrogels in both acidic and basic medium.
The terms “hard” and “soft” are frequently employed as broad labels for contact lenses. Hard contact lenses are gas-permeable durable devices, whereas soft contact lenses are constructed of a flexible, high-water-content network which facilitates gas permeability dependent on the water ratio content. Although hard lenses are often referred to as rigid gas-permeable lenses (RGPs), this is not strictly correct since numerous counterexamples could be brought forward [29,30,31]. A soft contact lens (SCL), on the other hand, is a very flexible, oxygen-permeable polymer with higher water content. Because of their flexibility, SCLs adapt to the shape of a user’s eye significantly faster than stiff lenses. SCLs can be disposed of on a daily, weekly, or monthly basis [32,33]. These broad definitions of contact lenses can provide some insight into their material qualities, but not always. Materials used in hard and soft lenses, frequently overlap. Although they both use silicone materials, there are differences in the chemical composition, structuration, gel network, water content, etc. Derivatives can help to broaden the spectrum of feasible contact lenses and their attributes. Contact lenses features are fairly extensive, and there is a plethora of existing devices on the market to reflect this [18]. Table 1 summarizes the main polymer materials used for the fabrication and the CLs features derived from used material.
In terms of drug accommodation, silicone hydrogels and other hydrogels are believed to be the optimal materials for the fabrication of contact lenses [34]. Early hydrogel contact lenses made by polymerizing 2-hydroxyethyl methacrylate (HEMA) didn’t let enough oxygen into the eye. The addition of different hydrophilic monomers to HEMA polymer formulations increased the water content and made it easier for oxygen to pass through. However, HEMA-based hydrogels cannot be worn for more than 6-7 days [34]. Silicone hydrogel lenses, on the other hand, allow an important amount of oxygen to pass through and can be worn for 29 days [35].
Contact lenses facilitate drug flow to the eye surface for more than 30 minutes, which, compared to the eye drop delivery of roughly two minutes is highly advantageously. This means that the bioavailability of drug on the cornea is superior because contact lenses deliverthe loaded bioactive drugs for longer extentthan conventional eye drops devices. As a result, the amount of the drug in the body’s bloodstream is cut down, and so are the possible side effects. Drug-filled contact lenses can be worn by patients for a longer time, which reduces the number of times they need to be administered medication [36].
At first, there were no investigations on medication release from contact lenses. The first drug-infused hydrogel contact lens was created in 1965. The lenses were immersed in an aqueous solution containing 1 percent homatropine, which elicited full pupil dilatation in patients for longer than eye drops alone. Following this, there was interest in the delivery of pilocarpine using contact lenses for the treatment of glaucoma and an increasing number of studies began examining contact lens efficacy via in vitro and in vivo experiments addressing various ophthalmic conditions [16].
Under optimal conditions, there is at least a 50% corneal bioavailability for the drug supplied by contact lenses. In attempt to more correctly predict the corneal bioavailability, a mathematical model for drug transport from contact lenses has been devised; however it neglects some contact lens issues, such as swelling and the interaction with the lodging network [37]. It has been proven that the rate of radial diffusion, the rate of drug equilibrium between the contact lens and the tear film, and the ratio of drug uptake by the cornea are the three most influential parameters on corneal bioavailability. Predictions place corneal bioavailability between 50 and 70 percent [34].
Poly methyl methacrylate (PMMA), cellulose acetate butyrate (CAB), siloxy methacrylate (SMA), and fluoro-siloxymethacrylates (FSA) are some of the polymers that can be utilized to make stiff contact lenses. Mulle and Ohring were the first to develop rigid PMMA contact lenses in 1936. CAB was approved by the FDA in 1978 as an alternative for PMMA due to its superior gas permeability. SMA sparked the development of a new generation of contact lenses with exceptional stiffness and gas permeability by combining a methacrylate backbone with siloxane groups. Surface wetness was a prevalent concern due to SMA’s high lipophilicity, which resulted in surface scratches and a build-up of lipid surface deposits [34].
Soft contact lenses have the advantages of comfort and biological tissue compatibility over earlier hard contact lenses. Because oxygen dissolved in water can be provided to the cornea, the oxygen permeability of a hydrogel contact lens is primarily determined by its water content. N-vinyl pyrrolidone (NVP) is a typical hydrophilic monomer that is widely used to raise the water content of soft contact lenses [39]. However, NVP can also increase the relative evaporation rate of water, resulting in a rough surface on the lens. This phenomenon is not suitable for soft contact lens wearers, but it can help with drug loading and release in lenses with drugs [18]. Pores were generated within the hydrogels during polymerization by adding NVP and 20 percent to 40% V/V water to the HEMA contact lens in one study. Hydrogels with microstructural changes had more water content, which improved drug loading and resulted in a more optimal release profile [30]. Furthermore, when poly(vinyl pyrrolidone) is copolymerized with HEMA, it was found an increasing surface hydrophilicity and reduce surface friction. Conversely, ion ligand copolymerization of the highly negatively charged anionic methacrylic acid (MAA) monomer with 3-Methacryloxypropyltris(trimethylsiloxy)silane (MPTS) and HEMA can improve cationic drug loading i.e. Gatifloxacin (GFLX) and Moxifloxacin (MFLX) antibiotics [40]. The released antibiotics volume of the new MAA-MPTS-HEMA lenses was found to be considerably higher throughout 72 hours than that of the commercial, etafilcon A and polymacon (P < 0.01) lenses. Furthermore, the concentration found in the cornea and aqueous humor was higher than those for the eye drop groups.The carboxyl groups of MAA, on the other hand, attract positively charged proteins like lysozyme, resulting in a large accumulation of protein on both surfaces of the lens.
The corneal edema caused by overnight lens usage, which promotes excessive water build-up (favoring bacterial growth), was addressed by adding silicone to the hydrogel which increase oxygen permeability and decreased the equilibrium water content. Silicone hydrogel contact lenses are often made out of i) silicone-based polymers such as poly-dimethylsiloxane (PDMS), tris-trimethylsiloxysilyl (TPVC), tris(trimethylsiloxy)- methacryloxy-propylsilane (TRIS), or other siloxane macromers and ii) as well as hydrophilic monomers like HEMA, N, N-dimethylacrylamide (DMA), or NVP. TRIS-DMA-NVP-HEMA contact lenses overcome the most limitations related to the aforementioned compositions by presenting the best balance between oxygen permeability, equilibrium water content, hydrophilicity and reduced protein film formation [32]. Consequently, soft contact lenses with tailored features could be achieved according to specific requirements by combining the materials with required properties and the appropriate fabrication method. Another study investigated a complex composition based on TRIS-NVP-MAA-poly(ethylene glycol) methacrylate (PEGMA). The hydrogel presents a nice balance between oxygen permeability, water absorption capacity, contact angle, modulus and protein adsorption when compared to some commercial contact lenses (e.g. Acuvue Advances or Cooper vision). The contact angles of the TRIS-NVP-MAA-PEGMA based CLS were lower than that of Pure Vision and similar to that of Acuvue Oasys and Acuvue Advance. The modulus ranged from 1.42 MPa to 0.69 MPa depending on the PGEMA content while the moduli of commercial CLs range from 0.3 to 1.52 MPa e.g. CIBA Vision moduli are higher (1.0–1.52 MPa) On the other hand the friction coefficient varied between 0.288 to 0.075 as the PEGMA content increased while that of Clariti 1 day, (CooperVision) is 0.069. Another design parameter is oxygen permeability, which range between 73.0 barrers to 45.3 barrers and place TRIS-NVP-MAA-PEGMA contact lenses comparable or superior to 1-Day Acuvue (21.4 barrers), Biomedics XC (44 barrers), and Biomedics 38 (8.4 barrers) commercial contact lenses [41].
2.2. Manufacturing methods
Manufacturers have created a number of ways for producing contact lenses that contain and release active ingredients. Lathe-cutting, spin-casting, and cast-moulding are now the most extensively utilized contact lens manufacturing procedures. Diverse manufacturing procedures will have to comply with significantly different techniques adapted with respect to material specificities. The characteristics of the final lens may be affected by these various material manufacturing stages. Solid buttons of dehydrated material are used to make lathed lenses. The buttons are typically bulk polymerized over a long period of time [42]. Spin-casting is the process of injecting a mixture of monomers into a mold that is spun at a computer-controlled speed. The form of the lens front surface is determined by the shape of the mold. The centrifugal force created by the mold’s spin speed, the surface tension and friction forces between the mold and the polymer, and the influences of gravity all influence the form of the lens’ back surface [42]. Spin-casting is much faster than button manufacturing in the lathing process, generally requiring less than an hour to polymerise the finished lens. In the cast-moulding process a small amount of monomer is placed between two casts to directly form the lens. The polymerisation process is very fast which is one of the reasons why this is the method of choice for bulk (disposable) lens manufacture [42].
In terms of necessary materials, design flexibility, and complicated geometries, all of these techniques are limited to some level. Additive manufacturing (AM) methods may be preferable for producing personalized, multi-functional and smart contact lenses [43].The additive manufacturing, also known as 3D printing technique, is the most emerging technology in the manufacturing field, especially because of its control over dimensions with the help of a computer aided design (CAD) model of the object piled up into a 3D architecture with high accuracy. The technology is appealing since it saves time and money while also requiring little post-processing of printed goods. Compared to other traditional manufacturing technologies, AM allows for precise item replication and the production of multiple products at the same time [44,45]. Selective laser sintering (SLS), fused deposition modeling (FDM), photocuring stereoscopic printing, stereolithography apparatus (SLA), and digital light printing (DLP)are some of the 3D printing processes used to manufacture contact lenses [46]. Because of the excellent resolution of the printing and the small thickness of the printable layers, light-curing-based 3D printing methods (such as SLA and DLP) are frequently used in the fabrication of such optical devices [47,48].
3. Embodying bioactive molecules into contact lenses
Several strategies have been developed for loading drugs in contact lenses e.g. soaking into a drug solution; layered structure for drug-eluting or drug-barrier (coatings); incorporation of functional molecules, molecular imprinting, supercritical fluid method, colloidal nanoparticles [49]. Table 2 summarizes the main strategies currently used to embody active molecules within contact lenses.
3.1. Soaking Method
It is the simplest and least expensive way to load drugs into contact lenses by soaking[50]. It has worked well for loading ophthalmic drugs like timolol, dexamethasone, pilocarpine, pirfinedone, aminoglycosides, and fluoroquinolones into contact lenses [34].
Soaking can be carried out by either putting drugs into the contact lens or by sticking them to the polymer matrix. Molecular diffusion is what drives drug delivery into contact lenses because there is a big difference in concentration between the soaking solution and the aqueous phase of the contact lens. This means that molecular diffusion is also the main way drugs are released from the lens. It takes a few minutes to a few hours for drugs with a low molecular weight, between 300 and 500 Da to be released[51]. Drugs with a high molecular weight, like hyaluronic acid, have a hard time getting into the water channels of a contact lens and stay on the surface [52]. This is because different types of contact lenses have different affinity for drugs. This means that the type of lens also affects the amount of drugs that can be put in and taken out. Even though soaking is a good way to embed bioactive molecules, drawbacks such as burst release have been highlighted and many hydrogels release the whole amount of drug in few hours.
To address this issue, putting a diffusion barrier in the polymer matrix can help the drug stay in the lens for a longer time. However, the choice of a diffusion barrier needs to be addressed carefully because it needs to be safe, clear, and allow oxygen to pass through the contact lens [51].Vitamin E is a hydrophobic liquid that is a strong antioxidant. It is also biocompatible and could have therapeutic benefits. Vitamin E does not impact light transmissibility since it has a shorter wavelength than visible light. It has been used as a diffusion barrier, making it hard for drug molecules to spread in the soaking method, affecting how ions and oxygen move through the gel. Most vitamin E-aggregates that form are in the hydrophilic polymer region of the gel. Even though vitamin E-aggregates lengthen the time it takes for a drug to be released, hydrophilic drugs move through a vitamin E-filled hydrogel in a different way than hydrophobic drugs. In a recent study commercially available ACUVUE TruEye CLs were loaded with vitamin E barriers for extended and simultaneous release of timolol and dorzolamide, hydrophilic drugs usually prescribed in glaucoma conditions. Extended release to up to 2 days for both timolol and dorzolamide drugs is achieved by loading lenses with vitamin E barriers. Both timolol and dorzolamide revealed superior IOP reduction compared to eye drops (about 6 fold lower drug loading) [53]. In another recent study same commercially available CLs were modified with vitamin E by soaking method, although, this time vitamin E was dissolved in ethanol-water solutions to minimize swelling. After that the transport of timolol, a hydrophilic glaucoma drug, was assessed. The Vitamin E barrier was successfully incorporated into contact lenses by soaking in solutions of vitamin E in water and ethanol. The aforementioned protocol was successful in extending hydrophilic drug release and lowered the swelling degree a beneficial aspect as minimizes the possibility of lens damage during loading of vitamin E [54].
Despite obvious advantages of using vitamin E barrier to control the drug delivery, limitations related to the reduction of ions and oxygen permeability, alteration of CLs mechanical properties and protein adsorption due to the hydrophobic nature of Vitamin E have to be considered [52].
3.2. Incorporation of Functional Molecules within Contact Lenses
Increasing affinity is advantageous because it will make it easier for drugs to be loaded and released, so other ways have been suggested. In one example, ion components are added to contact lenses before they are polymerized. Then, the lenses are soaked in a drug solution, which makes them more likely to interact better with drugs. In some studies, copolymerization was used to load all ionic components with acrylic/vinyl groups into the hydrogel matrix (e.g. HEMA, methacrylamide propyl-trimenthylammonium chloride (MAPTAC), 2-methacryloxyethyl acid phosphate (MOEP) and MAA) [55]. The complex aforementioned hydrogel containing cationic functional group in its side chain proved to be able to store the anionic drug i.e. azulene on ion-exchange reaction, and the complex composition is successful to prevent the size change and control the drug delivery [55]. Dexamethasone 21-disodium phosphate-filled HEMA contact lenses with the cationic surfactant, cetalkonium chloride, were designed. Dexamethasone 21-disodium phosphate, ionic drug, can then be stuck to the charged surfactant that covers the surfaces of the polymer matrix. Surfactant can be added to either pre-monomer mixtures or pre-made lenses. When 10 percent of the lens is made up of surfactant, the drug stays in the lens for 25 times longer than in ACUVE contact lens. Good wettabilty, excellent transparency and low protein adsorption are other features that characterize the HEMA / cetalkonium chloride lenses [56].
Cyclodextrin-based (CD) contact lenses have been widely used in the pharmaceutical field to deliver hydrophobic drugs. CD lens are praised for their high potential to increase drug bioavailability and stability. Contact lenses are made from different monomers that have reactive double bonds when they are mixed together with free radicals. By copolymerization, CDs made from acrylic or vinyl can be turned into drug-CDs complexes that can be put into contact lenses. CDs loaded natamycin effect was assayed in silicone-hydrogel contact lenses fabricated form DMA, TRIS and HEMA contact lenses. It was found that silicone-hydrogel and HEMA contact lenses both increased the amount of drug that was released, particularly the TRIS formulation [57]. Also, adding CDs to preformed polymer networks HEMA and HEMA-glycidyl methacrylate (GMA) (reaction of polymer glycidyl groups and the hydroxyl groups of CDs) strongly impacts the phenomenon of protein deposition (high decrease) and the affinity of the network for loading miconazole (high increase). Furthermore constant delivery was observed for over 14 days and complete prevented Candida albicans biofilm formation as indicated by in vitro microbiological test [58]. In addition, direct crosslinking of CDs to the contact lens materials has been looked into. Poly-CDs that were made by crosslinking with citric acid were used as carriers for ethoxzolamide in one study. Then, they were loaded into HEMA-based matrix. The poly-CDs-HEMA composition was able to load higher doses of drug and sustain its release for 6 days [59].
3.3. Molecular Imprinted Contact Lenses
Molecular imprinting technology is one of the most advanced methods to load drug templates into contact lenses. During the polymerization reaction, cavities are made in the contact lens that can conveniently lodge drug molecules. Drugs can be loaded into the lens by soaking method because of the high affinity of cavities in the lens. If functional monomers are not used, there will be no imprinting. However, if there are too many functional monomers, the drugs stay in the material instead of being released. Conversely, cross-linking agents can make contact lenses more durable and less likely to swell in water, but too many of them can make the network structure stiff, and slow down the rate at which drugs can get out of the lenses [65]. In a recent study of Zhao et al., molecularly imprinted hydrogel CLs were prepared for atropine delivery, with non-imprinted hydrogel (for control) and MAA and methacrylamide (MAm) functional comonomers. MAA / MAm exhibited atropine release time to up to 72 h combined with good surface wettability, biocompatibility, light transmission, and water content which recommend them as promising systems for efficient ocular drug delivery for myopia [60]. In another study imprinted and non-imprinted hydrogels with various contents of the methacrylic acid functional monomer, HEMA, and EGDMA were prepared for acyclovir (ACV) and valacyclovir (VACV) drugs delivery. ACV and VACV are the first choice against herpes simplex virus ocular keratitis. MAA/HEMA/EGDMA-ACV-imprinted hydrogels were not efficient for drug loading and release. Conversely, high affinity of the hydrogel for VACV was noticed. Very likely this is based on electrostatic interactions of the acrylic acid group and the VACV lateral chain. VACV-imprinted hydrogels deliver the drug in a constant manner for 10h, and relevant amount of drug is accumulated in the cornea with the possibility to be delivered to the posterior segment. Furthermore the VACV-imprinted hydrogels display swelling, light transmission and mechanical properties similar to those of the commercial contact lenses [17].
3.4. Supercritical fluid method
Supercritical fluid method (SFM) implies first the drug to be dissolved in the supercritical solvent, then to be put together with the framework of the contact lens. It is a convenient manner to load both hydrophilic and hydrophobic drugs into contact lenses by using the right supercritical fluid solvents. Despite the fact that the release profile from lenses loaded through this method is moreextended when compared to the one achieved by the widely spread soaking method, the burst release is a common disadvantage that has not been overcome. However, the coupled method of supercritical fluid-aided molecular imprinting is believed to substantiate two interests: larger amounts of drugs which can be loaded into soft contact lenses and targeting an extended time of release [61]. An example of the use of supercritical fluid method is to load flurbiprofen into Hilafilcon B contact lenses using supercritical fluid CO2. The release profile of the drug from the contact lens loaded via SFM versus the one loaded conventionally confirmed the hypothesis i.e. larger amounts of drugs loaded and unsustained release of the drug. Later research studies have shown that supercritical fluid method give fewer promising results, the best result was to extend the drug retention time to few hours [16,66]. This finding should be carefully considered as further research is needed. To surmount such limitation combined approach supercritical fluid and imprinting was proposed. Yanez et al. anticipated that by combining the aforementioned methods, limitations related to loading the drug in preformed CLs and of the molecular imprinting in which the drug has to be selected before polymerization might result in drug-tailored networks. Commercial Hilafilcon B CLs were treated by SFM for flurbiprofen loading. The treated SFM CLs were able to load flurbiprofen to a higher extent than using water-based methods. The interaction flurbiprofen– Hilafilcon B CLs direct the formation of specific cavities able to chemically and structurally recognize flurbiprofen, and are believed to be responsible for higher flurbiprofen sorption and for the more sustained release profile [61].
3.5. Colloidal nanoparticles
Colloidal nanoparticles have been used a lot in ocular delivery since they can support extended drug stays onto the cornea. Drugs can also be put inside colloidal nanoparticles to keep them from being broken down by enzymes in ocular environment. Nanoparticles loaded into a contact lens matrix make a drug delivery system that lasts longer than either the nanoparticles or the lens alone [3]. In the delivery system, the drug moves through the nanoparticles to reach the contact lens matrix, and then moves through the hydrogel matrix to reach the tissues inside the eye. Some types of nanoparticles, such as polymeric nanoparticles, liposomes, micelles and emulsions have already been successfully loaded into contact lenses. In addition to the drug-filled nanoparticles mentioned above, pure nanoparticles that don’t contain any drugs can also be put into contact lenses. Silver nanoparticles are strong antibacterial agents as they can inactivate enzymes and disable DNA replication [34].ElShaer and coworker investigated the ocular administration of Prednisolone loaded in poly (lactic-co-glycolic acid) (PLGA) nanoparticles, prepared by single emulsion solvent evaporation method. Prednisolone-PLGA nanoparticles presented an average particle size of 347.1 ± 11.9 nm with a polydispersity index of 0.081. CLs fabricated by HEMA (80%), MAA (19%) and EGDMA (1%) were loaded Prednisolone-PLGA nanoparticles. Nanoparticles loaded contact lenses exhibited almost unchanged hydration, light transmission and wettability and showed a sustained drug release over 24 h; while 10% of encapsulated prednisolone was released [62].
Liposomal delivery is another advanced drug-delivery system that increases the bioavalabilty, encapsulation, and ensure targeted and sustained release. In a recent study Zerillo and co-workers examine the effect of Ozodrop® and Ozodrop® gel (ozonated oil in liposomes and hypromellose) on suppression and/or formation of biofilms on Dailies AquaComfort PLUS commercial CLs. The study outcomes indicated that Ozodrop® and Ozodrop® gel have an exceptional inhibitory effect on eradication and formation of biofilm produced by Pseudomonas aeruginosa and Staphylococcus aureus [63].
Loading drugs within CLs might affects key features such as optical, swelling or contact angle due to drug precipitation in the polymer matrix. By designing micelles in the contact lens aimed to dissolve drug precipitates seems to be a promising method to overcome aforementioned challenge. Maulvi et al., fabricated DMA/siloxane/ NVP/EGDMA/ HEMA CLs loaded with Pluronic® F-68/Gatifloxacin. Pluronic® F-68 was meant to build micelles and provide better uptake and sustained drug release. The gatifloxacin-pluronic-loaded CLs exhibited excellent optical transmittance, swelling, and drug loading capacity and sustained drug release [64].
4. Non-interventional future perspectives in keratoconus
The versatility of the polymeric supports used in the fabrication of the contact lenses offers the possibility to incorporate numerous active compounds, carefully paired with specific impregnation techniques within the polymer supports. So far, within this review we have catalogued a series of contact lenses envisaged as drug vehicles solutions proposed for ocular conditions such as: glaucoma, conjunctivitis, cataract, diabetic macular edema, retinoblastoma, fungal or bacterial inflammations, etc. Nonetheless, an important ophthalmic disorder, keratoconus, with a prevalence estimated at 1.38 per 1000 individuals worldwide [67], has not, to the best of the authors’ knowledge, been addressed from this standpoint by any review paper. However, based on the currently available options for keratoconus treatment, we hypothesize a possible alternative treatment in line with the topic of the present paper.
Keratoconus is a non-inflammatory, degenerative corneal condition that manifests with the thinning and bulging of the cornea (the transparent front of the eye). Changes in corneal collagen structure and organization, abnormalities in the extracellular matrix, and keratocyte apoptosis in the anterior stroma and Bowman lamina are all typical phenomena that contribute to the disease’s biomechanical corneal deterioration [68]. Children and young people are more likely to have the illness, which may worsen with time.
Keratoconus has been treated with a variety of medicinal and surgical techniques. Rigid gas-permeable (RGP) contact lenses are the first-line therapy for keratoconus patients [69]. Spectacles may help improve eyesight in the early stages of the condition, but as the disease advances, rigid gas permeable contact lenses are frequently the best option. If the disease worsens, corneal transplantation may be the only option. Various contact lens designs and fits have been created to meet the unique requirements of this disease, which usually worsens. Corneal scarring, severe thinning, and contact lens sensitivity are all indications for corneal transplantation (keratoplasty) [70]. Keratoconus is the most prevalent reason for keratoplasty for young people in high-income nations [71].
In recent years, the above-mentioned treatment strategies have been supplemented by collagen cross-linking (CLX) using UVA light and riboflavin (vitamin B2). This is a novel strategy that tackles stromal instability directly. It is the only treatment for keratoconus that can halt the disease from progressing, unlike all other treatments [72] CXL using UVA light and riboflavin is a relatively novel therapy that has been shown to delay disease development in its early stages. When paired with intracorneal ring segments, the improvement in vision is larger than when the segments are used alone [71].
A promising solution on this issue could be the employment of gas permeable contact lenses paired with riboflavin as the therapeutic agent for controlled and prolonged release on the eye’s surface. Moreover, with wearing these contact lenses, and exposing to sunlight (which includes UVA light) the process of crosslinking could be achieved in time. Figure 2 presents the distinctiveness between the two approaches currently used for keratoconic eye care; rigid contact lens wear (traditional standard procedure) and cornea collagen photochemical cross-linking with riboflavin with UV-A light. In the CLX approach corneal tissues has to be removed as riboflavin cannot pass the corneal epithelium (high molecular weight).
The corneal stroma is mostly composed of collagen type I, while collagen types III, V, and VI are also present. The corneal stroma has the mechanical strength to build the eye’s anterior coat while preserving the high degree of transparency essential for light transmission. Collagen fibers and fibrils are formed starting from collagen’s precursor, procollagen. Procollagen has two additional peptides, one at each end, that are removed through enzymatic pathways and undergoes posttranslational modifications to form the collagen molecules. The enzyme lysyl oxidase is responsible for the oxidation of the amino acids lysine and hydroxylysine to their respective aldehydes, which then condense with other aldehydes to produce intramolecular and intermolecular cross-links [72].
Additional cross-link induction may be done by several ways, for example, nonenzymatic glycation, irradiation using UV light with or without photosensitizer, and aldehyde reactions. Therapeutic cross-linking was intended to improve corneal stiffness and delay or even stop the course of keratoconus by actively increasing the degree of covalent bonding between and within extracellular matrix components including collagen type I and proteoglycans [73]. Riboflavin serves as a photomediator, significantly enhancing UVA light absorption when exposed to the corneal stoma. It has been shown that UVA radiation is absorbed around 30% inside the lamellae of the corneal stroma, but when combined with the photomediator characteristics of riboflavin, this absorption jumps to 95% [74].
Following exposure, riboflavin is excited into a triplet state therefore creating reactive oxygen species: singlet oxygen and superoxide anions subsequently react with accessible groups near-by [73]. It has to be specified that the precise mechanism of the riboflavin/UVA crosslinking reaction it is not exactly and fully understanded but there have been made multiple suppositions that could be verified. It is plausible that this phenomenon happens through creation of additional chemical bonds between histidine, hydroxyproline, hydroxylysine, tyrosine, and threonine amino-acid residues [72,74]. Importantly, riboflavin may promote cross-linking of other macromolecules, such as proteoglycans, inside the corneal stroma, either to one another or to collagen molecules [75]. Corneal treatment based on cross-linking collagen using UVA light and riboflavin remains the foundation preventive approach; however, the current major challenge of research is increasing oxygen accessibility and developing new approaches to improve riboflavin permeability during the procedure. Apart from fast oxygen depletion predominantly when higher UVA irradiances are used and inadequate riboflavin penetration through the tissue challenges related to the depth-dependent riboflavin gradient within the tissue [76] extended treatment period, and potential endothelial toxicity in thin corneas has to be overcome. Recently, protocols combining simultaneously stop keratoconus progression and correct refractive error were have greatly evolved, exhibiting vast promise to help clinicians better manage patients [77]. Conversely, advances in regenerative medicine and tissue engineering bring innovative treatment at the cellular level and therefore prevent the requirement for invasive surgeries. In this review, we describe the advances in the diagnosis and treatment of keratoconus primarily focusing on newly emerging approaches and strategies.
5. Conclusions
Contact lenses are increasingly being seen as a tool for specialized ophthalmic therapies that require adequate drug delivery to the eye. As a result, practitioners rely on the development of new lenses to better deliver these therapies, which is dependent on material scientists tailoring new materials. With a significant change in lifestyle, contact lens research for therapeutic purposes has increased dramatically. Developing contact lenses platforms for ocular drug delivery is a novel and effective therapeutic approach for a variety of ocular diseases while avoiding the limitations of traditional eye drops. However, further study is needed before drug-loaded contact lenses may be marketed to ensure efficacy, safety, and comfort for patients. The majority of contact lens drug-incorporating approaches, such as drug-soaked contact lenses, vitamin E-modified contact lenses, molecular imprinting and the supercritical fluid method (or hybrid processes) involve loading the drug into the manufactured contact lens. The various studies included in this review show that the main problem remains promoting extended ocular medication release from contact lenses. Indeed, as an inexpensive and frequent way of incorporating active substances into contact lenses, soaking results in minimal drug absorption and rapid burst release. Among the alternatives, embedding of pharmaceuticals into contact lenses coupled with the use of vitamin E as a diffusion barrier and adjuvant active component for the treatment of ocular illnesses have shown to be particularly effective in extending drug release. Also, it has been discovered that incorporating drug-loaded liposomes and micelles into contact lenses is a fit way to minimize the drug leaking that characterizes soaked lenses, but given the small number of studies available, more research is needed to support this data. Although the recently proposed molecular imprinting utilizing supercritical CO2 has the potential to overcome some of the drawbacks of conventional molecular imprinting, more research into its application is required. It is critical to emphasize that, in addition to providing high drug loadings and long-term release, a good approach for fabricating therapeutic contact lenses must also ensure basic features such as the lens’ clarity, water content and gas permeability features. To avoid the premature and unwanted release of the laden medicine, other phases such as sterilization, packaging, and storage of therapeutic contact lenses have to be addressed as well.
The rigid and soft CLs have found application also for treatment of keratoconus corneal condition which is a progressive disease described by cornea thinning and bulging and loss of stiffness. Even though different approaches are applied in the keratoconus treatment non-surgical techniques aims generally to stop the progression and improve vision quality. Different therapeutic approaches are used such as wear of rigid contact lenses or corneal collagen crosslinking. Riboflavin photochemical corneal collagen crosslinking is an FDA approved procedure for strengthens the corneal tissue and is curetelly the golden standard. Conventional CXL procedure is currently the most applied and trusted method in clinical practice.
In conclusion, new contact lens materials will continue to extend the boundaries of materials science in order to better customize to the needs of an expanding contact lenses-using population.
Author Contributions
Conceptualization, M.I.; resources, M.I.; writing—original draft preparation G.M.V., A.T.; writing—review and editing, M.I., M.M.; project administration, A.T.; funding acquisition, M.I.All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by SEE 2014-2021, THE EDUCATION, SCHOLARSHIPS, APPRENTICESHIPS AND YOUTH ENTREPRENEURSHIP PROGRAMME, grant number 21-COP-0017, project Mixed Reality e-learning platform dedicated to Medical Engineering (REALME).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- P. Dixon, C.S., S. Gause, K. H. Hsu, K. C. Powell, and A. Chauhan. Therapeutic contact lenses: a patent review. Oct. 2015, vol. 25. review. Oct. 2015, vol. 25. [CrossRef]
- Choi, S.W.; Kim, J. Therapeutic Contact Lenses with Polymeric Vehicles for Ocular Drug Delivery: A Review. Materials 2018, 11. [Google Scholar] [CrossRef] [PubMed]
- Janagam, D.R.; Wu, L.; Lowe, T.L. Nanoparticles for drug delivery to the anterior segment of the eye. Adv Drug Deliv Rev 2017, 122, 31–64. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Prausnitz, M.R.; Edwards, A. Model of transient drug diffusion across cornea. J Control Release 2004, 99, 241–258. [Google Scholar] [CrossRef] [PubMed]
- Holgado, M.A.; Anguiano-Domínguez, A.; Martín-Banderas, L. Contact lenses as drug-delivery systems: a promising therapeutic tool. Archivos de la Sociedad Española de Oftalmología (English Edition) 2020, 95, 24–33. [Google Scholar] [CrossRef]
- Chatterjee, S.; Upadhyay, P.; Mishra, M.; M, S.; Akshara, M.R.; N, K.; Zaidi, Z.S.; Iqbal, S.F.; Misra, S.K. Advances in chemistry and composition of soft materials for drug releasing contact lenses. RSC Adv 2020, 10, 36751–36777. [Google Scholar] [CrossRef] [PubMed]
- Lim L, L.E. Therapeutic Contact Lenses in the Treatment of Corneal and Ocular Surface Diseases-A Revie. Asia Pac J Ophthalmol 2020. [CrossRef]
- Lu, D.; Aksimentiev, A.; Shih, A.Y.; Cruz-Chu, E.; Freddolino, P.L.; Arkhipov, A.; Schulten, K. The role of molecular modeling in bionanotechnology. Phys Biol 2006, 3, S40–S53. [Google Scholar] [CrossRef]
- Muraru, S.; Ionita, M. Super Carbonaceous Graphene-based structure as a gas separation membrane: A Non-Equilibrium Molecular Dynamics Investigation. Composites Part B: Engineering 2020, 196. [Google Scholar] [CrossRef]
- Filipecka-Szymczyk, K.; Makowska-Janusik, M.; Marczak, W. Molecular Dynamics Simulation of Hydrogels Based on Phosphorylcholine-Containing Copolymers for Soft Contact Lens Applications. Molecules 2023, 28. [Google Scholar] [CrossRef]
- Tonner, R. Molecular Modeling Basics. By Jan H. Hensen. ChemPhysChem 2011, 12, 2352. [Google Scholar] [CrossRef]
- Joshua, B. Fernandes, Y.Y., Jeffery B. Klauda. Molecular dynamics simulations of the human ocular lens with age and cataract. 2022, Volume 1864. [CrossRef]
- Esteban-Ibañez, E.; Montagud-Martínez, D.; Sawides, L.; Zaytouny, A.; de Castro, A.; Sisó-Fuertes, I.; Barcala, X.; Piñero, D.P.; Furlan, W.D.; Dorronsoro, C.; et al. 2023. [CrossRef]
- Behnam Abdi, M.M., Fatemeh Hassanpour, Emel Kirbas Cilingir, Sepideh K. Kalajahi, Paria H. Milani, Mahsa Ghanbarzadeh, Daddi Fadel, Melissa Barnett, Christopher N. Ta, Roger M. Leblanc, Anuj Chauhan, Farhang Abbasi. Therapeutic contact lenses for the treatment of corneal and ocular surface diseases: Advances in extended and targeted drug delivery. International Journal of Pharmaceutics 2023, Volume 638. [CrossRef]
- Franco, P.; De Marco, I. Contact Lenses as Ophthalmic Drug Delivery Systems: A Review. Polymers 2021, 13. [Google Scholar] [CrossRef]
- Rykowska, I.; Nowak, I.; Nowak, R. Soft Contact Lenses as Drug Delivery Systems: A Review. Molecules 2021, 26. [Google Scholar] [CrossRef] [PubMed]
- Varela-Garcia, A.; Gomez-Amoza, J.L.; Concheiro, A.; Alvarez-Lorenzo, C. Imprinted Contact Lenses for Ocular Administration of Antiviral Drugs. Polymers 2020, 12. [Google Scholar] [CrossRef]
- Musgrave, C.S.A.; Fang, F. Contact Lens Materials: A Materials Science Perspective. Materials 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.; Morgan, P.; Gleeson, H.; Jones, J. Switchable Liquid Crystal Contact Lenses for the Correction of Presbyopia. Crystals 2018, 8. [Google Scholar] [CrossRef]
- Jones, J.C.; Wahle, M.; Bailey, J.; Moorhouse, T.; Snow, B.; Sargent, J. Polarisation independent liquid crystal lenses and contact lenses using embossed reactive mesogens. Journal of the Society for Information Display 2020, 28, 211–223. [Google Scholar] [CrossRef]
- Milton, H.E.; Morgan, P.B.; Clamp, J.H.; Gleeson, H.F. Electronic liquid crystal contact lenses for the correction of presbyopia. Opt Express 2014, 22, 8035–8040. [Google Scholar] [CrossRef]
- Toader G, P.A. , Diacon A, Rusen E, Mocanu A, Brincoveanu O, Alexandru M, Zorila FL, Bacalum M, Albota F, Gavrila AM, Trica B, Rotariu T, Ionita M, Istrate M. Nanocomposite Hydrogel Films Based on Sequential Interpenetrating Polymeric Networks as Drug Delivery Platforms. Polymers 2023. [Google Scholar] [CrossRef]
- Panteli, P.A.; Patrickios, C.S. Multiply Interpenetrating Polymer Networks: Preparation, Mechanical Properties, and Applications. Gels 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kim, H.J.; Noh, H. pH Sensitive Soft Contact Lens for Selective Drug-Delivery. Macromolecular Research 2018, 26, 278–283. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Choksi, H.H.; Desai, A.R.; Patel, A.S.; Ranch, K.M.; Vyas, B.A.; Shah, D.O. pH triggered controlled drug delivery from contact lenses: Addressing the challenges of drug leaching during sterilization and storage. Colloids Surf B Biointerfaces 2017, 157, 72–82. [Google Scholar] [CrossRef]
- Toader, G.; Podaru, I.A.; Rusen, E.; Diacon, A.; Ginghina, R.E.; Alexandru, M.; Zorila, F.L.; Gavrila, A.M.; Trica, B.; Rotariu, T.; et al. Nafcillin-Loaded Photocrosslinkable Nanocomposite Hydrogels for Biomedical Applications. Pharmaceutics 2023, 15. [Google Scholar] [CrossRef]
- Vega, S.L.; Kwon, M.Y.; Burdick, J.A. Recent advances in hydrogels for cartilage tissue engineering. Eur Cell Mater 2017, 33, 59–75. [Google Scholar] [CrossRef]
- Tan, R.Y.H.; Lee, C.S.; Pichika, M.R.; Cheng, S.F.; Lam, K.Y. PH Responsive Polyurethane for the Advancement of Bio medical and Drug Delivery. Polymers (Basel) 2022, 14. [Google Scholar] [CrossRef]
- Chang, H.-C.; Hsu, M.-Y.; Hsiao, W.-T.; Shum, P.J.-T. Finite Element Modeling of an Elderly Person’s Cornea and Rigid Gas Permeable Contact Lenses for Presbyopic Patients. Applied Sciences 2018, 8. [Google Scholar] [CrossRef]
- Garcia-Millan, E.; Koprivnik, S.; Otero-Espinar, F.J. Drug loading optimization and extended drug delivery of corticoids from pHEMA based soft contact lenses hydrogels via chemical and microstructural modifications. Int J Pharm 2015, 487, 260–269. [Google Scholar] [CrossRef]
- Xue Y, Z.J. , Chen Z, Xue F, Zeng L, Qu X, Zhou X. Factors Affecting Long-Term Compliance with Rigid Gas-Permeable Contact Lens Wear in Patients with Keratoconus. J Clin Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.P.; Yang, M.C. Synthesis and Characterization of Silicone Contact Lenses Based on TRIS-DMA-NVP-HEMA Hydrogels. Polymers (Basel) 2019, 11. [Google Scholar] [CrossRef]
- Moore, J.; Lopes, B.T.; Eliasy, A.; Geraghty, B.; Wu, R.; White, L.; Elsheikh, A.; Abass, A. Simulation of the Effect of Material Properties on Soft Contact Lens On-Eye Power. Bioengineering (Basel) 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Xue, Y.; Hu, G.; Lin, T.; Gou, J.; Yin, T.; He, H.; Zhang, Y.; Tang, X. A comprehensive review on contact lens for ophthalmic drug delivery. J Control Release 2018, 281, 97–118. [Google Scholar] [CrossRef]
- Reindel, W.; Mosehauer, G.; Rah, M.; Proskin, H.; Steffen, R. Clinical Performance of Samfilcon A, a Unique Silicone Hydrogel Lens, on a 7-Day Extended Wear Basis. Clin Ophthalmol 2020, 14, 3457–3464. [Google Scholar] [CrossRef] [PubMed]
- Gulsen, D.; Chauhan, A. Ophthalmic drug delivery through contact lenses. Invest Ophthalmol Vis Sci 2004, 45, 2342–2347. [Google Scholar] [CrossRef] [PubMed]
- Gause, S.; Hsu, K.H.; Shafor, C.; Dixon, P.; Powell, K.C.; Chauhan, A. Mechanistic modeling of ophthalmic drug delivery to the anterior chamber by eye drops and contact lenses. Adv Colloid Interface Sci 2016, 233, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Efron, N. Rigid Lens Materials. In Contact Lens Practice; 2018; pp. 115-122.e111.
- Tetsunosuke Kunitomo, K.H.K., Yokohama; Syoji Nagaoka, Kamakura; Takeshi; Yoshioka, K.H.; Tanzawa, K., all of Japan. CROSS-LINKED N-VNYL PYRROL DONE POLYMER COMPOSITION SUITABLE FOR CONTACT LENSEs. United States Patent 1976.
- Kakisu, K.; Matsunaga, T.; Kobayakawa, S.; Sato, T.; Tochikubo, T. Development and efficacy of a drug-releasing soft contact lens. Invest Ophthalmol Vis Sci 2013, 54, 2551–2561. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Phuong-Dung Tran, M.-C.Y. , Nur Hasanah, Phuong Lan Tran-Nguyen. Effect of poly(ethylene glycol) methacrylate on the ophthalmic properties of silicone hydrogel contact lenses. Colloids and Surfaces B: Biointerfaces. [CrossRef]
- Efron, C.M.-C.a.N. Impact of manufacturing technology and material composition on the mechanical properties of hydrogel contact lenses. Ophthalmic and Physiological Optics 2004. [Google Scholar] [CrossRef]
- Chia, H.N.; Wu, B.M. Recent advances in 3D printing of biomaterials. J Biol Eng 2015, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Leow, W.R.; Chen, X. 3D Printing of Flexible Electronic Devices. Small Methods 2018, 2. [Google Scholar] [CrossRef]
- Hittini, S.; Salih, A.E.; Alam, F.; Shanti, A.; Lee, S.; Polychronopoulou, K.; AlSafar, H.; Almaskari, F.; Butt, H. Fabrication of 3D-Printed Contact Lenses and Their Potential as Color Blindness Ocular Aids. Macromolecular Materials and Engineering 2023, 308. [Google Scholar] [CrossRef]
- Alam, F.; Elsherif, M.; AlQattan, B.; Salih, A.; Lee, S.M.; Yetisen, A.K.; Park, S.; Butt, H. 3D Printed Contact Lenses. ACS Biomater Sci Eng 2021, 7, 794–803. [Google Scholar] [CrossRef]
- Vaidya, N.; Solgaard, O. 3D printed optics with nanometer scale surface roughness. Microsyst Nanoeng 2018, 4, 18. [Google Scholar] [CrossRef]
- Vallejo-Melgarejo, L.D.; Reifenberger, R.G.; Newell, B.A.; Narváez-Tovar, C.A.; Garcia-Bravo, J.M. Characterization of 3D-printed lenses and diffraction gratings made by DLP additive manufacturing. Rapid Prototyping Journal 2019, 25, 1684–1694. [Google Scholar] [CrossRef]
- Toffoletto, N.; Saramago, B.; Serro, A.P. Therapeutic Ophthalmic Lenses: A Review. Pharmaceutics 2020, 13. [Google Scholar] [CrossRef] [PubMed]
- Anthony Soluri*, A.H.; , a. L.J. Delivery of Ketotifen Fumarate by Commercial Contact Lens Materials. American Academy of Optometry 2012. [Google Scholar] [CrossRef]
- Lokendrakumar C Bengani, K.-H.H. , Samuel Gause &; Chauhan†, A. Contact lenses as a platform for ocular drug delivery. Expert Opin. Drug Delivery 2013. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Soni, T.G.; Shah, D.O. A review on therapeutic contact lenses for ocular drug delivery. Drug Deliv 2016, 23, 3017–3026. [Google Scholar] [CrossRef]
- Hsu, K.H.; Carbia, B.E.; Plummer, C.; Chauhan, A. Dual drug delivery from vitamin E loaded contact lenses for glaucoma therapy. Eur J Pharm Biopharm 2015, 94, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Zhen Liu, M.O. , Anuj Chauhan Transport of Vitamin E from Ethanol/Water Solution into Contact Lenses and Impact on Drug Transport. Drug Transport. J Ocul Pharmacol Ther. 2022. [Google Scholar] [CrossRef]
- Uchida, R.; Sato, T.; Tanigawa, H.; Uno, K. Azulene incorporation and release by hydrogel containing methacrylamide propyltrimenthylammonium chloride, and its application to soft contact lens. J Control Release 2003, 92, 259–264. [Google Scholar] [CrossRef]
- Bengani, L.C.; Chauhan, A. Extended delivery of an anionic drug by contact lens loaded with a cationic surfactant. Biomaterials 2013, 34, 2814–2821. [Google Scholar] [CrossRef]
- Phan, C.M.; Subbaraman, L.N.; Jones, L. In vitro drug release of natamycin from beta-cyclodextrin and 2-hydroxypropyl-beta-cyclodextrin-functionalized contact lens materials. J Biomater Sci Polym Ed 2014, 25, 1907–1919. [Google Scholar] [CrossRef]
- dos Santos, J.F.; Torres-Labandeira, J.J.; Matthijs, N.; Coenye, T.; Concheiro, A.; Alvarez-Lorenzo, C. Functionalization of acrylic hydrogels with alpha-, beta- or gamma-cyclodextrin modulates protein adsorption and antifungal delivery. Acta Biomater 2010, 6, 3919–3926. [Google Scholar] [CrossRef]
- Garcia-Fernandez, M.J.; Tabary, N.; Martel, B.; Cazaux, F.; Oliva, A.; Taboada, P.; Concheiro, A.; Alvarez-Lorenzo, C. Poly-(cyclo)dextrins as ethoxzolamide carriers in ophthalmic solutions and in contact lenses. Carbohydr Polym 2013, 98, 1343–1352. [Google Scholar] [CrossRef]
- Wang, Z.L., Ting; Li, Xinhua; Wu, Haitao; Li, Yuhang; Hao, Lingyun. Preparation of Molecularly Imprinted Hydrogel Contact Lenses for Extended Atropine Eluting. Journal of Biomedical Nanotechnology 2023, Volume 19. 19. [CrossRef]
- Yanez, F.; Martikainen, L.; Braga, M.E.; Alvarez-Lorenzo, C.; Concheiro, A.; Duarte, C.M.; Gil, M.H.; de Sousa, H.C. Supercritical fluid-assisted preparation of imprinted contact lenses for drug delivery. Acta Biomater 2011, 7, 1019–1030. [Google Scholar] [CrossRef]
- ElShaer, A.; Mustafa, S.; Kasar, M.; Thapa, S.; Ghatora, B.; Alany, R.G. Nanoparticle-Laden Contact Lens for Controlled Ocular Delivery of Prednisolone: Formulation Optimization Using Statistical Experimental Design. Pharmaceutics 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Zerillo, L.; Polvere, I.; Varricchio, R.; Madera, J.R.; D’Andrea, S.; Voccola, S.; Franchini, I.; Stilo, R.; Vito, P.; Zotti, T. Antibiofilm and repair activity of ozonated oil in liposome. Microb Biotechnol 2022, 15, 1422–1433. [Google Scholar] [CrossRef] [PubMed]
- Maulvi, F.A.; Parmar, R.J.; Desai, A.R.; Desai, D.M.; Shukla, M.R.; Ranch, K.M.; Shah, S.A.; Shah, D.O. Tailored gatifloxacin Pluronic(R) F-68-loaded contact lens: Addressing the issue of transmittance and swelling. Int J Pharm 2020, 581, 119279. [Google Scholar] [CrossRef] [PubMed]
- Hiratani, H.; Mizutani, Y.; Alvarez-Lorenzo, C. Controlling drug release from imprinted hydrogels by modifying the characteristics of the imprinted cavities. Macromol Biosci 2005, 5, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Li, Y.; Jin, R.; Shrestha, T.; Choi, J.S.; Lee, W.J.; Moon, M.J.; Ju, H.T.; Choi, W.; Yoon, K.C. The Efficiency of Cyclosporine A-Eluting Contact Lenses for the Treatment of Dry Eye. Curr Eye Res 2019, 44, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Hassan Hashemi, M., Samira Heydarian, PhD, Elham Hooshmand, MSc,Mohammad Saatchi, PhD,; Abbasali Yekta, P., Mohamadreza Aghamirsalim, MD,k Mehrnaz Valadkhan, M.Sc,; Mehdi Mortazavi, M., Alireza Hashemi, MD, and Mehdi Khabazkhoob, PhD. The Prevalence and Risk Factors for Keratoconus: A Systematic Review and Meta-Analysis. Cornea 2019, 1. [CrossRef]
- Ashar, J.N., & Vadavalli, P. K. Long-term Results of Riboflavin Ultraviolet A Corneal Collagen Cross-linking for Keratoconus in Italy: The Siena Eye Cross Study. American Journal of Ophthalmology 2010. [CrossRef]
- Hwang, J.S.; Lee, J.H.; Wee, W.R.; Kim, M.K. Effects of multicurve RGP contact lens use on topographic changes in keratoconus. Korean J Ophthalmol 2010, 24, 201–206. [Google Scholar] [CrossRef]
- Zohar Meiri, B.S.K., MD, Amir Rosenblatt, MD, Tal Sarig, MSc,; Liat Shenhav, B., and David Varssano, MD. Efficacy of Corneal Collagen Cross-Linking for the Treatment of Keratoconus: A Systematic Review and Meta-Analysis. Cornea 2016. [CrossRef]
- Sykakis, E.; Karim, R.; Evans, J.R.; Bunce, C.; Amissah-Arthur, K.N.; Patwary, S.; McDonnell, P.J.; Hamada, S. Corneal collagen cross-linking for treating keratoconus. Cochrane Database Syst Rev 2015, CD010621. [Google Scholar] [CrossRef]
- Hovakimyan, M.; Guthoff, R.F.; Stachs, O. Collagen cross-linking: current status and future directions. J Ophthalmol 2012, 2012, 406850. [Google Scholar] [CrossRef] [PubMed]
- Adamiak, K.; Sionkowska, A. Current methods of collagen cross-linking: Review. Int J Biol Macromol 2020, 161, 550–560. [Google Scholar] [CrossRef]
- tissue, I.o.c.-l.i.c. Induction of cross-links in corneal tissue. Experimental Eye Research 1998. [Google Scholar] [CrossRef]
- McCall, A.S.; Kraft, S.; Edelhauser, H.F.; Kidder, G.W.; Lundquist, R.R.; Bradshaw, H.E.; Dedeic, Z.; Dionne, M.J.; Clement, E.M.; Conrad, G.W. Mechanisms of corneal tissue cross-linking in response to treatment with topical riboflavin and long-wavelength ultraviolet radiation (UVA). Invest Ophthalmol Vis Sci 2010, 51, 129–138. [Google Scholar] [CrossRef]
- Seiler, T.G.; Ehmke, T.; Fischinger, I.; Zapp, D.; Stachs, O.; Seiler, T.; Heisterkamp, A. Two-Photon Fluorescence Microscopy for Determination of the Riboflavin Concentration in the Anterior Corneal Stroma When Using the Dresden Protocol. Invest Ophthalmol Vis Sci 2015, 56, 6740–6746. [Google Scholar] [CrossRef] [PubMed]
- Atalay, E.; Ozalp, O.; Yildirim, N. Advances in the diagnosis and treatment of keratoconus. Ther Adv Ophthalmol 2021, 13, 25158414211012796. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) Schematic representation of different hydrogels, (a) traditional single polymer networks b, c, d) double networks and e, f) cross-linked double networks. This figure is from an open access journal under a CC-BY license source [27]. pH-responsive polymer (B) consisting of amino group (–NH2) and loaded drug. In a basic pH environment, the amino groups are ionized and keep the drug within the polymer network, for acidic pH the amino groups were protonated (NH3+) and electrostatic repulsion between the polymer and drug positive groups take place, releasing the encapsulated drug. (C) pH-responsive polymer containing a carboxylic group (–COOH) loaded with drug. In the acidic pH environment, the acidic group is unionized and encapsulates the drug in the polymer matrix. For basic pH, the -COOH group ionizes increases of electron charge density and releases the incorporated drug. These figures have been taken from an open access journal under a CC-BY license source [28].
Figure 1.
(A) Schematic representation of different hydrogels, (a) traditional single polymer networks b, c, d) double networks and e, f) cross-linked double networks. This figure is from an open access journal under a CC-BY license source [27]. pH-responsive polymer (B) consisting of amino group (–NH2) and loaded drug. In a basic pH environment, the amino groups are ionized and keep the drug within the polymer network, for acidic pH the amino groups were protonated (NH3+) and electrostatic repulsion between the polymer and drug positive groups take place, releasing the encapsulated drug. (C) pH-responsive polymer containing a carboxylic group (–COOH) loaded with drug. In the acidic pH environment, the acidic group is unionized and encapsulates the drug in the polymer matrix. For basic pH, the -COOH group ionizes increases of electron charge density and releases the incorporated drug. These figures have been taken from an open access journal under a CC-BY license source [28].
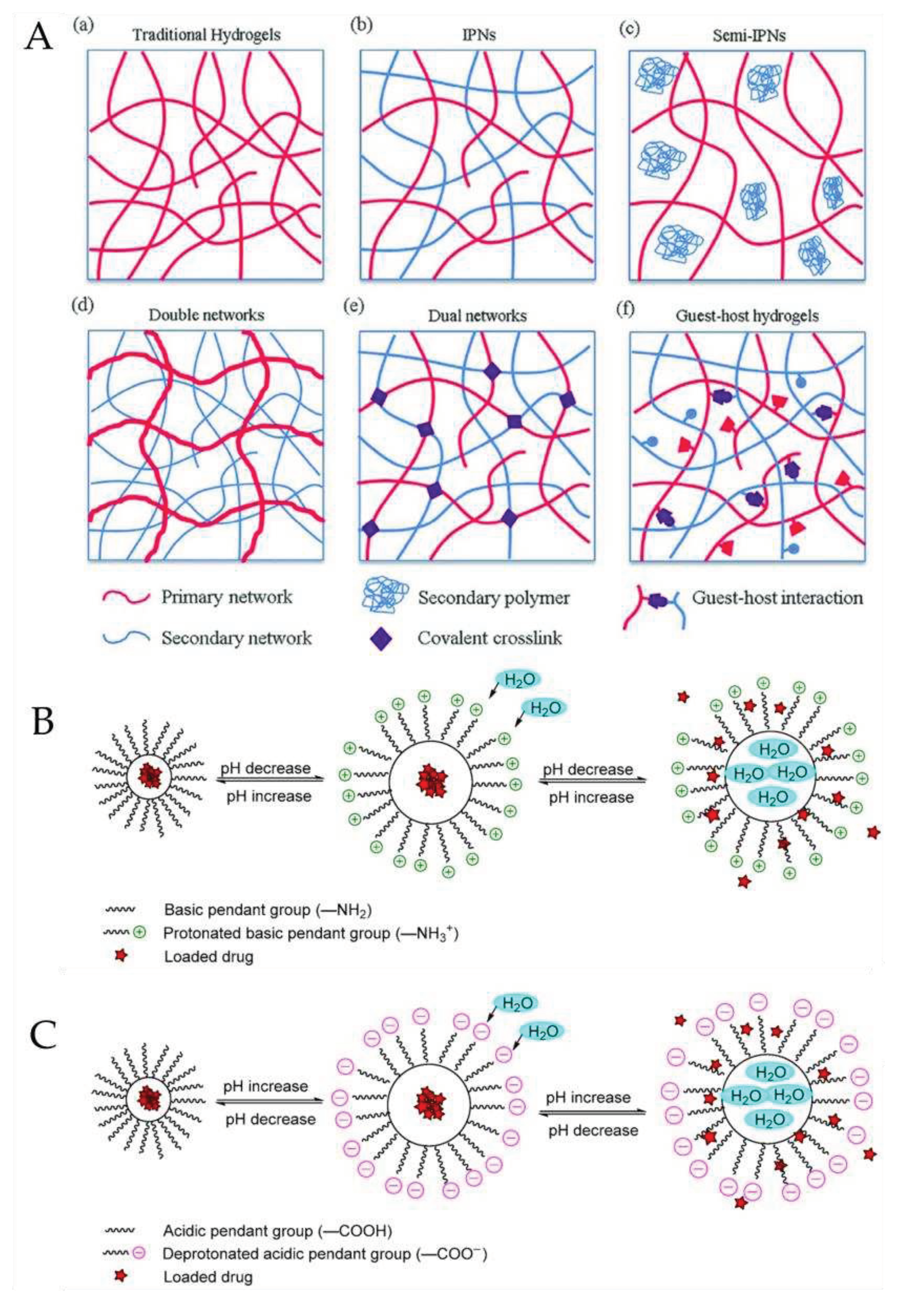
Figure 2.
Schematic representation of aeratoconic eye, current treatment approaches for keratoconus i.e. rigid contact lens wear and cornea collagen photochemical cross-linking with riboflavin with UV-A light.
Figure 2.
Schematic representation of aeratoconic eye, current treatment approaches for keratoconus i.e. rigid contact lens wear and cornea collagen photochemical cross-linking with riboflavin with UV-A light.
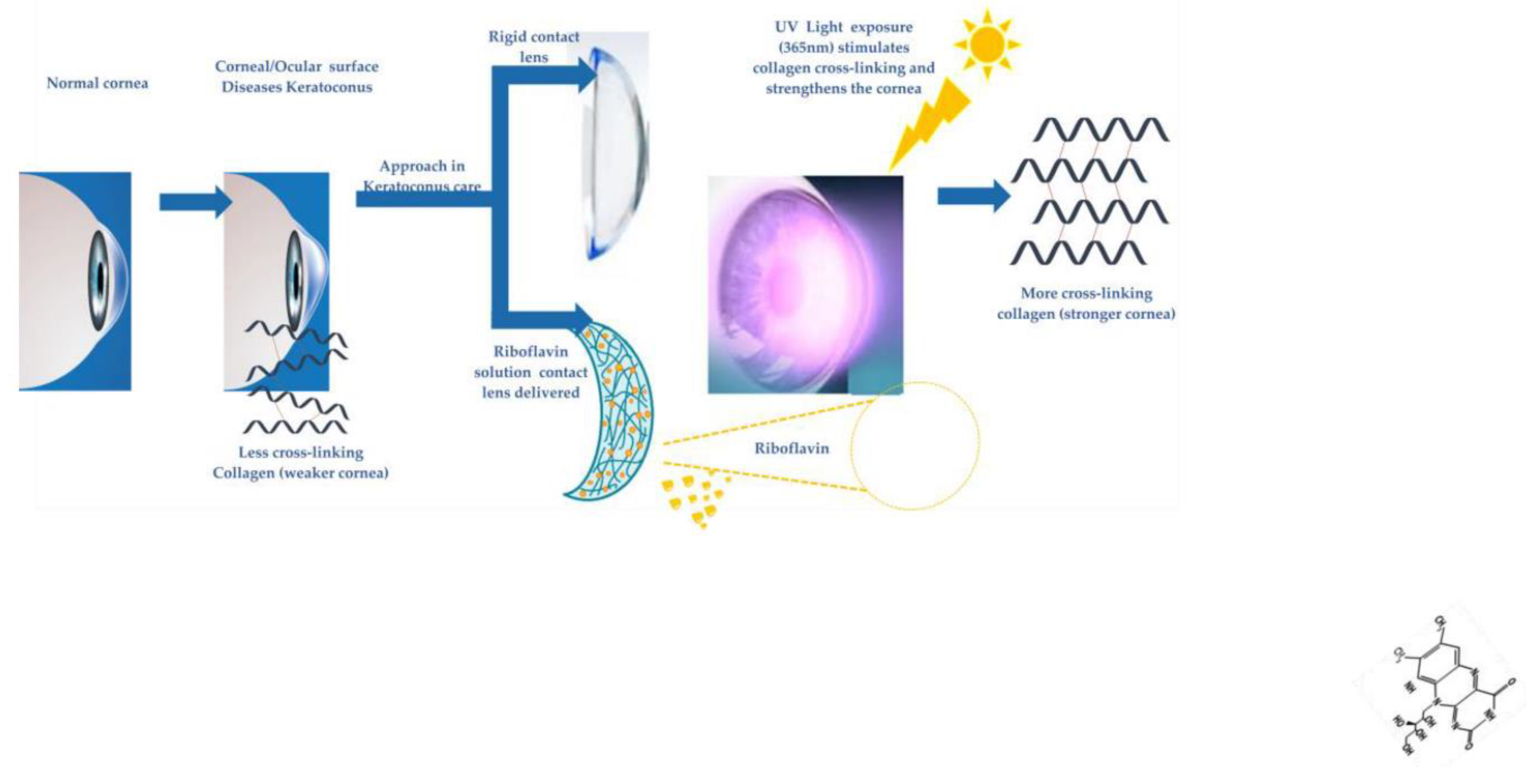

Table 1.
Comparison of CLs features fabricated based on different materials.
| Lens Type | Material(monomer) | Features | Reference |
|---|---|---|---|
| Rigid | Methyl methacrylate | -low permeability -stiff |
[31] |
| Cellulose acetate butyrate | -superior gas permeability to PMMA -stiff |
[34] | |
| Siloxy methacrylate | -exceptional gas permeability -low surface wetness -lipid surface deposits |
[32] | |
| Fluoro-siloxymethacrylate | -gas permeability higher than PMMA -improved wettability -no clinically considerable balance of advantages over PMMA |
[38] | |
| Soft | Hydroxyethyl-methacrylate | -not enough O2 permeability | [30,33] |
| N-vinyl pyrrolidone | -high water content -increase the relative evaporation rate of water -beneficial effect on drug loading and release |
[39] | |
| HEMA-co-NVP | -high water content when compared to pure polymer -higher O2permeability -improved drug loading and more optimal drug release |
[30] | |
| HEMA-co-HEMA-co-MPTS | -excellent cationic drug loading -improved drug release (Gatifloxacin and Moxifloxacin) compared to commercial etafilcon A and polymacon and eye drops |
[40] | |
| TRIS-DMA-NVP-HEMA | -best balance oxygen permeability, equilibrium water content, hydrophilicity and reduced protein film formation compared to simpler formulations | [32] | |
| TRIS-NVP-MAA-PEGMA | -the overall oxygen permeability, friction coefficient, water absorption capacity, contact angle, modulus and protein adsorption are superior to some of the commercial contact lenses (e.g.Acuvue Advances or Cooper vision). | [41] |
Table 2.
The main strategies currently used to embody active molecules within contact lenses.
| Lens Type | Backbone Monomers | Features | Drug | Drug loading techniques | Ref. |
|---|---|---|---|---|---|
| 1 | ACUVUE TruEye CLs with vitamin E barriers | -vitamin E modification increases the release duration of both drugs to about 2 days -reduces IOP with lower drug dose compared to eye drops |
timolol and dorzolamide simultameously loaded | Soaking Method | [53] |
| 2 | ACUVUE TruEye CLs with vitamin E barriers | -effective at sustaining release of timolol -reduced swelling which reduce lens damage |
timolol | Soaking Method | [54] |
| 3 | HEMA/MAPTAC /MOEP/MAA | -prevent the size change -efficient drug delivery |
azulene | Incorporation of Functional Molecules | [55] |
| 4 | HEMA/ cetalkonium chloride |
-drug release duration (50h) -good wettability -low protein absorption -excellent transparency of lenses |
dexamethasone 21-disodium phosphate | Incorporation of Functional Molecules | [56] |
| 5 | HEMA / DMA/TRIS/CDs | -improve the water solubility of natamycin -more effective to deliver natamycin |
natamycin / methacrylated beta-cyclodextrin (Mβ-CD) natamycin / methacrylated 2-hydroxypropyl-β-cyclodextrin |
Incorporation of Functional Molecules | [57] |
| 6 | HEMA / HEMA–co-GMA/α-, β- and γ-cyclodextrins functionalized | -reduced protein sorptin -HEMA γ-cyclodextrins has the higest loading for miconazole -sustained miconazole delivery for over 14days -high efficiency for against biofilm formation |
miconazole | Incorporation of Functional Molecules | [58] |
| 7 | poly-CDs-HEMA | -high drug doses loaded -sustained drug release for 6 days |
ethoxzolamide | Incorporation of Functional Molecules | [59] |
| 8 | MAA and methacrylamide (MAm) functional comonomers | - atropine release for up to 72 h -good balance light transmission, water content, and contact angle |
atropine | Molecularly Imprinted | [60] |
| 9 | MAA/HEMA/EGDMA | -ACV-imprinted hydrogels were not effective in terms of drug loading -VACV-imprinted hydrogels has a sustained release profile for 10 h, -relevant amount of VACV is accumulated in the cornea. -promising for delivery to the posterior segment |
acyclovir valacyclovir | Molecularly Imprinted | [17] |
| 10 | Hilafilcon B commercial | -higher flurbiprofen loaded -sustained release profiles |
flurbiprofen | supercritical fluid (SCF)-assisted molecular imprinting | [61] |
| 11 | HEMA/MAA EGDMA / Prednisolone loaded PLGA nanoparticles | -slow drug release of drug over 24 h -release of 10.8% encapsulated drug -insignificant changes in light transmission, wettability, and hydration by loading Prednisolone loaded PLGA nanoparticles |
Prednisolone | Colloidal nanoparticles | [62] |
| 12 | Dailies AquaComfort PLUS | -inhibit / eradication the formation of Pseudomonas aeruginosa and Staphylococcus biofilm | Ozodrop® Ozodrop® gel |
Liposome | [63] |
| 13 | DMA/siloxane/ NVP/EGDMA/ HEMA loaded Pluronic® F-68/gatifloxacin | -Pluronic® F-68 improves the drug uptake and sustained drug delivery -excellent optical transmittance, swelling and mechanical features |
Gatifloxacin/ Pluronic® F-68 | Micelles | [64] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



