
Submitted:
01 October 2023
Posted:
02 October 2023
You are already at the latest version
Abstract
Background: Patients with allergic rhinitis (AR) have bothersome symptoms that may assess using the visual analog scale (VAS). Asthma frequently is associated with AR. The present study investigated the role of VAS in children with newly-diagnosed AR. Methods: Parameters were VAS for nasal and asthma symptoms, and doctor’s perception of these diseases, medication use, and asthma comorbidity. Results: 67% of AR children had asthma. Severity of perceived nasal symptoms was associated with more intense asthma symptoms and doctor’s perception of disease severity (p<0.001 and p=0.02, re-spectively. Conclusions: Allergic rhinitis frequently is associated with asthma in child-hood. Symptom perception assessment using VAS is a simple tool for assessing their intensity. Moreover, the severity of nasal symptoms is associated with asthma symptom severity. Therefore, asthma should be carefully considered in AR children and require appropriate symptom perception assessment.
Keywords:
Allergic rhinitis
; asthma
; symptoms
; perception
; visual analog scale
1. Introduction
Allergic rhinitis (AR) frequently affects children as its prevalence may be more than 40% of the general population [1]. Allergic rhinitis recognizes a type 2 immunopathological mechanism characterized by a function defect of T regulatory cells and polarization of T helper 2 cells [2]. This deranged immune response promotes eosinophilic infiltrate at the target organ, the so-called type 2 inflammation [3]. Typically, allergic inflammation occurs when the patient exposes themself to the allergen and persists until the allergen exposure exists [4]. Type 2 inflammation, in turn, causes the symptoms’ appearance [3]. As a result, allergen exposure represents the necessary condition for inflammation and symptoms presence.
Patients with AR usually experience four nasal symptoms: itching, sneezing, watery rhinorrhea, and nasal congestion [5]. Nasal itching, sneezing, and nasal discharge mainly depend on histamine release, whereas nasal obstruction expresses type 2 inflammation.
Nasal symptoms are, as per definition, a subjective perception. As a result, measuring their intensity rigorously and precisely takes a lot of work. In clinical trials, a four-point scale is usually considered [6]. This scale starts from 0, such as no symptoms, and progressively increases to 1 (mild symptoms), 2 (moderate), and 3 (severe). However, this scoring may have some limitations, as the severity is not standardized and, in practice, requires the mediation of a doctor.
Therefore, for some time, the visual analog scale (VAS) has been adopted also for patients with AR [7]. Namely, VAS is a psychometric tool that intercepts the patient’s perception concerning the symptoms’ severity.
The different studies explored the clinical usefulness of VAS in AR. Interestingly, it has been reported that VAS scores significantly correlated with rhinomanometry values [8]. In addition, VAS is presently considered a reliable measure for assessing symptoms' severity. Accordingly, VAS is a relevant reported outcome measure.
VAS has been fruitfully used for asthmatic patients. In this regard, VAS scores have been reported to significantly correlate with spirometry outcomes and perception of bronchodilation with asthma [9,10].
Based on this background, the present study aimed to investigate the role of VAS assessment of nasal and asthma symptoms in children with AR newly diagnosed.
2. Materials and Methods
2.1. Study Design
This cross-sectional study included children with newly diagnosed allergic rhinitis and consecutively visited at a pediatric third-level allergy clinic (Allergy Center of the IRCCS Istituto G. Gaslini). The patients were recruited and evaluated in July 2023. The inclusion criteria were age ranging from 8 to 16 years and diagnosis of allergic rhinitis. The exclusion criteria were current respiratory infections, severe chronic disorders (e.g., metabolic disorders, autoimmunity, neuropsychiatric diseases, cancer), and current medications, including immune suppressants, psychiatric drugs, and chemotherapy, able to interfere with interpreting the results.
Children could have asthma comorbidity.
The diagnosis of allergic rhinitis was performed according to validated criteria defined by Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines [11]. In particular, AR is diagnosed when there is consistency between sensitization (such as the production of allergen-specific IgE) and symptom occurrence after exposure to the sensitizing allergen.
The diagnosis of asthma was performed according to the criteria established by the Global Initiative for Asthma (GINA) guidelines. As stated by these guidelines, the two defining features of asthma are (i) a history of variable respiratory symptoms (i.e., wheezing, shortness of breath, chest tightness, and cough) over time and in intensity, worsening at night or on waking, triggered by exercise, laughter, allergens, or cold air, and occurring or worsening with viral infections; and (ii) variable airflow limitation, documented by spirometry and functional tests [12].
VAS scoring was used to assess asthma and nasal symptoms. [13]. The VAS consisted of one ruler asking for symptom perception [13]. In this study, the VAS was a 10-cm vertical line on which 0 implied the most severe respiratory symptoms, while 10 corresponded to no respiratory symptoms. Initially, patients were instructed to put a mark on the line indicating their symptom perception at that moment. Thus, the lower the numerical score the patient (or doctor) marks, the greater the perceived symptom severity. With a movable marker, the subject could mark any point on the 10-cm segment that best described his/her perception. No interval marker was visible on the line.
Demographic data, nasal and asthma symptoms' severity assessed by visual analogic scale (VAS), medications used for AR (antihistamines and intranasal corticosteroids), and asthma treatment were evaluated.
The Istituto Giannina Gaslini Ethics Committee of Genoa approved the procedure (code number: 22253/2017). The parents signed an informed consent.
2.2. Outcomes
The primary outcome was the VAS measurement. Therefore, patients were further stratified into two sub-groups: patients with normal or abnormal VAS for nasal symptoms severity. The cut-off for normal VAS value was 6, as previously defined [9,13].
Secondary outcomes were the variables observed, including asthma comorbidity, medication use, and doctor's perception of nasal and asthma symptoms’ severity.
2.3. Parameters
The methodology has been reported in detail elsewhere [14]. Clinical data included gender, age, current use of medications for AR (antihistamines and intranasal corticosteroids), allergen immunotherapy (AIT), asthma treatment, and symptoms' severity perception by children and physicians.
2.4. Statistical Analysis
Variables were described as mean with standard deviation or frequency with percentage. Differences in continuous variables were assessed by the Student T-test or corresponding non-parametric Mann-Whitney U test based on data distribution. Any relationship between discrete categorical data was explored by the Chi-Square Test, or Fisher’s exact test, as appropriate. P values ≤ 0.05 were considered statistically significant. Statistical analysis was conducted using SPSS Statistical Package, Version 24.0 (IBM Corp., Armonk, NY, USA).
3. Results
The present study included 150 children, 56 (37.3%) 12 females and 94 (62.7%) males; the mean age was 11.8 years, with allergic rhinitis. Clinical data are reported in detail in Table 1.
The mean VAS score for nasal symptoms' severity, assessed by children, was 6.3. The doctor's perception of AR severity was 7.0. Fifty (75) percent of children with AR used antihistamines and 16% (24) intranasal corticosteroids. Twenty-six (17.3%) used AIT. Only 10 (6.7%) children had mono-sensitization. One hundred (67.1%) children also had asthma, and 46 (46%) were under active treatment. The mean VAS score for asthma symptoms’ severity was 7.0. The doctor’s perception of asthma severity was 7.0.
Successively, children were stratified considering the VAS score as normal or abnormal (<6), as reported in Table 2.
Exactly half of the sample (75 children) had normal VAS values. Comparing the two sub-groups, children with abnormal VAS scores for AR had significantly lower VAS scores for asthma symptoms' severity and doctor's perception of asthma severity than children with normal VAS scores for nasal symptoms (p<0.001 and p=0.012, respectively), as reported in Figure 1 and Figure 2.
4. Discussion
Allergic rhinitis is a common medical condition in childhood. Although AR is not a severe disease, the symptoms impact patients' quality of life, school performance, and sleep quality [15]. There is robust evidence that AR significantly affects children and adolescents [16-19]. Fatigue, impaired attention and learning, memory defects, and, seldom, also depression may reduce the school performance. Nasal obstruction is a relevant factor that contributes to sleep pattern. In addition, sneezing and rhinorrhea, resulting in the need to blow one's nose frequently, result in a stigma for children with AR. Therefore, these nasal symptoms heavily contribute to reduce the quality of life of children with AR.
Consequently, nasal symptoms may be very bothersome and require effective relief [20]. In this regard, different strategies have been proposed, including preventive recommendations, such as allergen avoiding, nasal lavage, medications, non-pharmacological remedies, allergen immunotherapy, and, in very selected patients, nasal surgery. The most valuable approaches are obviously based on documented evidence.
Pharmacological remedies for AR essentially include antihistamines and intranasal corticosteroids, mostly topically administered.
However, AR is frequently self-managed by parents and is believed to be a simple disease [21]. Namely, AR self-management constitutes an actual modality of approaching this disease, bypassing real doctor's visits. Of course, self-management may present relevant biases, including inadequate disease control and inappropriate prescriptions. However, self-management may be performed in different ways: directly by parents of children with AR independently acting, asking advice from relatives/friends, or interacting with healthcare providers (physicians, pharmacists, nurses). Some researchers investigated this issue in different settings. Particularly, a relevant role is played by the pharmacist who may provide advice and recommendation based on a scientific background.
In any case, AR severity assessment plays a central role in self-management [22]. The visual analog scale is ideal for autonomously assessing nasal symptoms' severity and reliably reflecting their intensity [23]. Moreover, VAS is also a reliable tool for managing subjects with AR and asthma in clinical practice [24].
However, limited access to physical visits, mainly after the COVID-19 pandemic, promotes self-care strategies, including self-diagnosis, OTCs use, and complementary therapies [25]. However, telemedicine allows real-time synchronous interaction between patients and healthcare providers that have been recognized to be an essential part of clinical practice by many doctors [26]. Moreover, telemedicine consistently receives high patient satisfaction from allergic subjects [27,28]. In this regard, the MASK (Mobile Airways Sentinel Network) app is highly ranked by European and Asian AR patients, as reported further. Indeed, the MASK app is easily accessible, user-friendly, and compatible with AR self-management [26]. Moreover, the MASK app may be considered a system engaging, highly intuitive, and appealing [28]. In this regard, the benefits of mobile technology include the possibility of self-monitoring using an electronic diary, personalized feedback, and individual education on ideal approaches [29]. These aspects can implement self-management and adherence to treatments [30].
The MASK-air® app was designed to implement AIRWAYS-ICPs [31]. Furthermore, MASK-air® consists of a patient-centered app; it presently is available in 27 countries and 19 languages with around 35,000 users [32]. This intensive use made it possible to acquire much information on AR patients. In particular, there is evidence that AR patients are poorly adherent to treatment [33], most patients use self-medications [34], on-demand treatments [35], and switch therapies [36]. In addition, a recent pediatric study conducted on 76 children with AR provided evidence the MASK-air® app is a useful instrument for evaluating the response to treatments by measuring the perceived symptoms [37].
Especially, the importance of this app, documented and validated by this large body of studies, is mainly based on the fact that the tool for measuring symptom intensity that in turn governs the choice of optimal treatment is the VAS. Thus, it seems clear that the VAS represents a simple and reliable tool for measuring the intensity of perceived nasal symptoms. In this context, the present study investigated the role of VAS in assessing children with newly diagnosed AR and its impact on some clinical variables.
The findings showed some interesting insights. Firstly, the male gender is prevalent; this result is consistent with the literature data that report this point [24]. Antihistamines are predominant, whereas intranasal corticosteroids are rare; this finding confirms the well-known literature [38]. However, this finding conflicts with the documented superiority of corticosteroids in relieving nasal complaints [39]. Indeed, corticosteroids exert a potent anti-inflammatory activity on type 2 inflammation; so, significantly reduce the intensity of nasal symptoms, mainly concerning nasal obstruction, closely linked to allergic inflammation [40].
Although it is the only causal treatment for respiratory allergy, allergen immunotherapy (AIT) was prescribed only in 17% of children. Also, polysensitization is practically observed in almost all children, confirming the relevance of this phenomenon and its clinical significance [41]. Currently, it can be observed that the vast majority of individuals with RA are polysensitized. This phenomenon has practical implications especially in the choice of allergen to be used for AIT. In other words, it is important to define the allergen that is most responsible for the onset of allergic symptoms. Perhaps this difficulty in interpretation may be an obstacle to the more widespread use of AIT [42].
More interestingly, the present study reported that asthma affected about one/third of children with AR. This outcome underscores the importance of asthma comorbidity in AR and highlights the close link between AR and asthma [43].
On the other hand, the most impressive results of the present study concerned the significant association between the perception of the most bothersome nasal symptoms and the perception of the most intense asthma symptoms. This finding confirms the strict correlation between AR and asthma and concerning symptom perception in children. Moreover, this finding is consistent with the recent point of view that patients with AR associated with asthma present a distinct phenotype from patients with AR alone [44]. Namely, the ARIA-MeDALL hypothesis has been inspired by the recent evidence on polysensitization and multimorbidity, advances in mHealth identifying new phenotypes, updated epidemiologic studies, genomic data, and therapeutic trials [44]. Based on this background, the ARIA-MeDALL hypothesis proposed that AR alone and AR and asthma multimorbidity represent two distinct diseases, characterized by different genetic background, sensitization patterns, symptom severity, and treatment response [44]. Of course, this hypothesis needs to be tested for the confirmation of these concepts. This point is meaningful and deserves adequate attention in clinical practice managing patients with AR. Namely, asthma should always be investigated in AR children. Anyway, the present study confirmed that children with AR and asthma and perceiving intense nasal symptoms accordingly had intense asthma symptoms.
Another relevant outcome provided by the present study is the further confirmation of the usefulness of VAS in managing children with AR. In fact, VAS is a reliable tool for measuring nasal symptom severity perceived by the patient. In particular, VAS score properly reflected the nasal obstruction severity assessed by an objective method, such as rhinomanometry [7]. Moreover, VAS was a valuable measure for assessing the grade of asthma control in asthmatic children [9]. Accordingly, it was proposed that at home management of asthma using VAS for measuring the asthma symptom perception by children could suggest the best strategy for suspecting bronchial obstruction. In addition, VAS may reliably document the response to bronchodilation agents [10].
The present study had limitations, including the relatively low number of subjects, the need for more functional and biological data, and the cross-sectional design. However, the findings reflect real-life practice and reinforce the concept of united airways disease.
5. Conclusions
Allergic rhinitis frequently is associated with asthma in childhood. Symptom perception assessment using VAS is a simple tool for assessing their intensity. Moreover, the severity of nasal symptoms is associated with asthma symptom severity. Therefore, asthma should be carefully considered in AR children and require appropriate symptom perception assessment.
Author Contributions
Conceptualization, M.A.T. and G.C.; methodology, I.S.; formal analysis, I.S.; investigation, X.Y., writing—original draft preparation, G.C..; writing—review and editing, M.A.T.All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Istituto G. Gaslini (protocol code number: 22253/2017, approved on 2017).
Informed Consent Statement
Informed consent was obtained from parents of all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhang, Y.; Lan, F.; Zhang, L. Advances and highlights in allergic rhinitis. Allergy 2021, 76, 3383–3389. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Melén, E.; Haahtela, T.; Koppelman, G.H.; Togias, A.; Valenta, R.; Akdis, C.A. Rhinitis associated with asthma is distinct from rhinitis alone: The ARIA-MeDALL hypothesis. Allergy 2023, 78, 1169–1203. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wang, Z.; Zhu, Y.; Zhu, X.; Guo, L.; Fu, Y.; Zhang, Q.; Mou, X.; Liu, Y. MiR-223-3p regulates the eosinophil degranulation and enhances the inflammation in allergic rhinitis by targeting FBXW7. Int Immunopharmacol 2023, 118, 110007. [Google Scholar] [CrossRef] [PubMed]
- Ricca, V.; Landi, M; Ferrero, P.; Bairo, A.; Tazzer, C.; Ciprandi, G. Minimal persistent inflammation is also present in patients with seasonal allergic rhinitis. J Allergy Clin Immunol 2000, 105, 54–57. [CrossRef] [PubMed]
- Siddiqui, Z.A.; Walker, A.; Pirwani, M.M.; Tahiri, M.; Syed, I. Allergic rhinitis: diagnosis and management. Br J Hosp Med 2022, 83, 1–9. [Google Scholar] [CrossRef]
- Li, A.R.; Zhang, K.; Reddy, P.D.; Nguyen, S.A.; Miglani, A.; Fried, J.; Nguyen, M.I.; Schlosser, R.J. Systematic review of measures of disease severity in rhinitis. Int Forum Allergy Rhinol 2021, 11, 1367–1377. [Google Scholar] [CrossRef]
- Ciprandi, G.; Mora, F.; Cassano, M.; Gallina, A.M.; Mora, R. Visual analog scale (VAS) and nasal obstruction in persistent allergic rhinitis. Otolaryngol Head Neck Surg 2009, 141, 527–529. [Google Scholar] [CrossRef]
- Mora, F.; Cassano, M.; Mora, R.; Gallina, A.M.; Ciprandi, G. V.A.S. the follow-up of turbinectomy. Rhinology 2009, 47, 450–453. [Google Scholar]
- Tosca, M.A.; Silvestri, M.; Olcese, R.; Pistorio, A.; Rossi, G.A.; Ciprandi, G. Breathlessness perception assessed by visual analogue scale and lung function in children with asthma: a real-life study. Pediatr Allergy Immunol 2012, 23, 537–542. [Google Scholar] [CrossRef]
- Tosca, M.A.; Silvestri, M.; Rossi, G.A.; Ciprandi, G. Perception of bronchodilation assessed by Visual Analogue Scale in children with asthma. Allergol Immunopathol (Madr) 2013, 41, 359–363. [Google Scholar] [CrossRef]
- Bousquet, J.; Schünemann, H.J.; Togias, A.; Bachert, C.; Erhola, M.; Hellings, P.W.; Klimek, L.; Pfaar, O.; Wallace, D.; Ansotegui, I.; et al. Next-generation Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol 2020, 145, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma Global Strategy for Asthma Management and Prevention (2023). 2023. Available online: www.ginasthma.org (accessed on 13 September 2023).
- Tosca, M.A.; Del Barba, P.; Licari, A.; Ciprandi, G. . The Measurement of Asthma and Allergic Rhinitis Control in Children and Adolescents. Children (Basel) 2020, 7, 43. [Google Scholar] [CrossRef] [PubMed]
- Tosca, M.A.; Marseglia, G.L.; Ciprandi, G. The real-world "ControL'Asma" study: a nationwide taskforce on asthma control in children and adolescents. Allergologia et Immunopathologia 2021, 49, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Schuler IV, C.F.; Montejo, J.M. Allergic Rhinitis in Children and Adolescents. Immunol Allergy Clin North Am 2021, 41, 613–625. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Blaiss, M.S.; Naclerio, R.M. Burden of allergic rhinitis: allergies in America, Latin America, and Asia-Pacific adult surveys. Allergy Asthma Proc 2012, 33 (Suppl 1), S113–41. [Google Scholar] [CrossRef]
- Meltzer, E.O. Allergic rhinitis: burden of illness, quality of life, comorbidities, and control. Immunol Allergy Clin North Am 2016, 36, 235–248. [Google Scholar] [CrossRef]
- Muliol, J.; Maurer, M.; Bousquet, J. Sleep and allergic rhinitis. J Investig Allergol Clin Immunol 2008, 18, 415–419. [Google Scholar]
- Colas, C.; Galera, H.; Anibarro, B. Disease severity impairs sleep quality in allergic rhinitis (The SOMNIAAR study). Clin Exp Allergy 2012, 42, 1080–1087. [Google Scholar] [CrossRef]
- Bousquet, J.; Anto, J.M.; Bachert, C.; Baiardini, I.; Bosnic-Anticevich, S.; Melén, E.; Palomares, O.; Scadding, G.K.; Togias, A. , Toppila-Salmi, S. Allergic rhinitis. Nat Rev Dis Primers 2020, 6, 95. [Google Scholar] [CrossRef]
- Carr, W.W.; Yawn, B.P. Management of allergic rhinitis in the era of effective over-the-counter treatments. Postgrad Med 2017, 129, 572–580. [Google Scholar] [CrossRef]
- Bousquet, J.; Schunemann, H.J.; Fonseca, J.; Samolinski, B.; Bachert,, C. MACVIA-ARIA Sentinel NetworK for Allergic Rhinitis (MASK-Rhinitis): The New Generation Guideline Implementation. Allergy 2015, 70, 1372–1392. [CrossRef] [PubMed]
- Del Cuvillo, A.; Santos, V.; Montoro, J.; Bartra, J.; Davila, I.; Ferrer, M.; Jauregui, I.; Sastre, J.; Mullol, J.; Valero, A. Allergic rhinitis severity can be assessed using a visual analogue scale in mild, moderate and severe. Rhinology 2017, 55, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Tosca, M.A.; Pistorio, A.; Silvestri, M.; Marseglia, G.L.; Ciprandi, G. The comparison between children and adolescents with asthma provided by the real-world "ControL'Asma" study. J Asthma 2022, 59, 1531–1536. [Google Scholar] [CrossRef]
- Abdullah, B.; Snidvongs, K.; Lestari Poerbonegoro, N.; Sutikno, B. Reshaping the Management of Allergic Rhinitis in Primary Care: Lessons from the COVID-19 Pandemic. Int J Environ Res Pub Health 2022, 19, 13632. [Google Scholar] [CrossRef] [PubMed]
- Thong, H.K.; Wong, D.K.C.; Gendeh, H.S.; Saim, L.; Athar, P.P.; Saim, A. Perception of telemedicine among medical practitioners in Malaysia during COVID-19. J Med Life 2021, 14, 468–480. [Google Scholar] [CrossRef] [PubMed]
- Thomas, I.; Siew, L.; Rutkowski, K. Synchronous Telemedicine in Allergy: Lessons Learned and Transformation of Care During the COVID-19 Pandemic. J Allergy Clin Immunol Pract 2021, 9, 170–176.e1. [Google Scholar] [CrossRef]
- Waibel, K.H.; Bickel, R.A.; Brown, T. Outcomes from a Regional Synchronous Tele-Allergy Service. J Allergy Clin Immunol Pract 2019, 7, 1017–1021. [Google Scholar] [CrossRef]
- Tan, R.; Cvetkovski, B.; Kritikos, R.; O’Hehir, R.E.; Lourenco, O.; Bousquet, J. Identifying an effective mobile health application for the self-management of allergic rhinitis and asthma in Australia. J Asthma 2019, 57, 1–15. [Google Scholar] [CrossRef]
- Thakkar, J.; Kurup, R.; Laba, T.L.; Santo, K.; Thiagalingam, A.; Rodgers, A. Mobile telephone text messaging for medication adherence in chronic disease: A meta-analysis. JAMA Intern Med 2016, 176, 340–349. [Google Scholar] [CrossRef]
- Bousquet J, Addis A, Adcock I, Agache I, Agusti A, Alonso A, et al. Integrated care pathways for airway diseases (AIRWAYS-ICPs). Eur Respir J 2014, 44, 304–323.
- Bousquet, J.; Arnavielhe, S.; Bedbrook, A.; Bewick, M.; Laune, D.; Mathieu-Dupas, E. MASK 2017: ARIA digitally-enabled, integrated, person-centred care for rhinitis and asthma multimorbidity using real-world-evidence. Clin Transl Allergy 2018, 8, 45. [Google Scholar] [CrossRef] [PubMed]
- Menditto, E.; Costa, E.; Midao, L.; Bosnic-Anticevich, S.; Novellino, E.; Bialek, S. Adherence to treatment in allergic rhinitis using mobile technology. The MASK Study. Clin Exp Allergy 2019, 49, 442–460. [Google Scholar] [CrossRef] [PubMed]
- Bedard, A.; Basagana, X.; Anto, J.M.; Garcia-Aymerich, J.; Devillier, P.; Arnavielhe, S. Mobile technology offers novel insights on control and treatment of allergic rhinitis. The MASK study. J Allergy Clin Immunol 2019, 144, 135–143.e6. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Pinto, B.; Sa-Sousa, A.; Vieira, R.J.; Amaral, R.; Klimek, L.; Czarlewski, W. Behavioural patterns in allergic rhinitis medication in Europe: A study using MASK-air((R)) real-world data. Allergy 2022, 77, 2699–2711. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, O.; Suarthana, E.; Rifflart, C.; Lemiere, C.; Le Moual, N.; Bousquet, J. The Impact of Work-Related Rhinitis on Quality of Life and Work Productivity: A General Workforce-Based Survey. J Allergy Clin Immunol Pract 2020, 8, 1583–1591.e5. [Google Scholar] [CrossRef]
- Mitsias, D.I.; Dimou, M.V.; Lakoumentas, J.; Alevizopoulos, K.; Sousa-Pinto, B.; Fonseca, J.A.; Bousquet, J. Effect of nasal irrigation on allergic rhinitis control in children; complementarity between CARAT and MASK outcomes. Clin Transl Allergy 2020, 10, 9. [Google Scholar] [CrossRef]
- Brown, T. Diagnosis and Management of Allergic Rhinitis in Children. Pediatr Ann 2019, 48, e485–e488. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Wallace, D.; Friedman, H.S.; Navaratnam, P.; Scott, E.P.; Nolte, H. Meta-analyses of the efficacy of pharmacotherapies and sublingual allergy immunotherapy tablets for allergic rhinitis in adults and children. Rhinology 2021, 59, 422–432. [Google Scholar] [CrossRef]
- Ciprandi, G.; Cirillo, I.; Vizzaccaro, A.; Milanese, M.; Tosca, M.A. Nasal obstruction in patients with seasonal allergic rhinitis: relationships between allergic inflammation and nasal airflow. Int Arch Allergy Immunol 2004, 134, 34–40. [Google Scholar] [CrossRef]
- Weaver-Agostoni, J.; Kosak, Z.; Bartlett, S. Allergic Rhinitis: Rapid Evidence Review. Am Fam Physician 2023, 107, 466–473. [Google Scholar]
- Paller, A.S.; Spergel, J.M.; Mina-Osorio, P.; Irvine, AD. The atopic march and atopic multimorbidity: Many trajectories, many pathways. J Allergy Clin Immunol 2019, 143, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Passalacqua, G.; Ciprandi, G.; Pasquali, M.; Guerra, L.; Canonica, G.W. An update on the asthma-rhinitis link. Curr Opin Allergy Clin Immunol 2004, 4, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Melén, E.; Haahtela, T.; Koppelman, G.H.; Togias, A.; Valenta, R.; Akdis, C.A.; Czarlewski, W.; Rothenberg, M.; Valiulis, A.; et al. Rhinitis associated with asthma is distinct from rhinitis alone: The ARIA-MeDALL hypothesis. Allergy 2023, 78, 1169–1203. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
VAS scores for asthma symptoms in patients with abnormal or normal VAS for nasal symptoms.
Figure 1.
VAS scores for asthma symptoms in patients with abnormal or normal VAS for nasal symptoms.
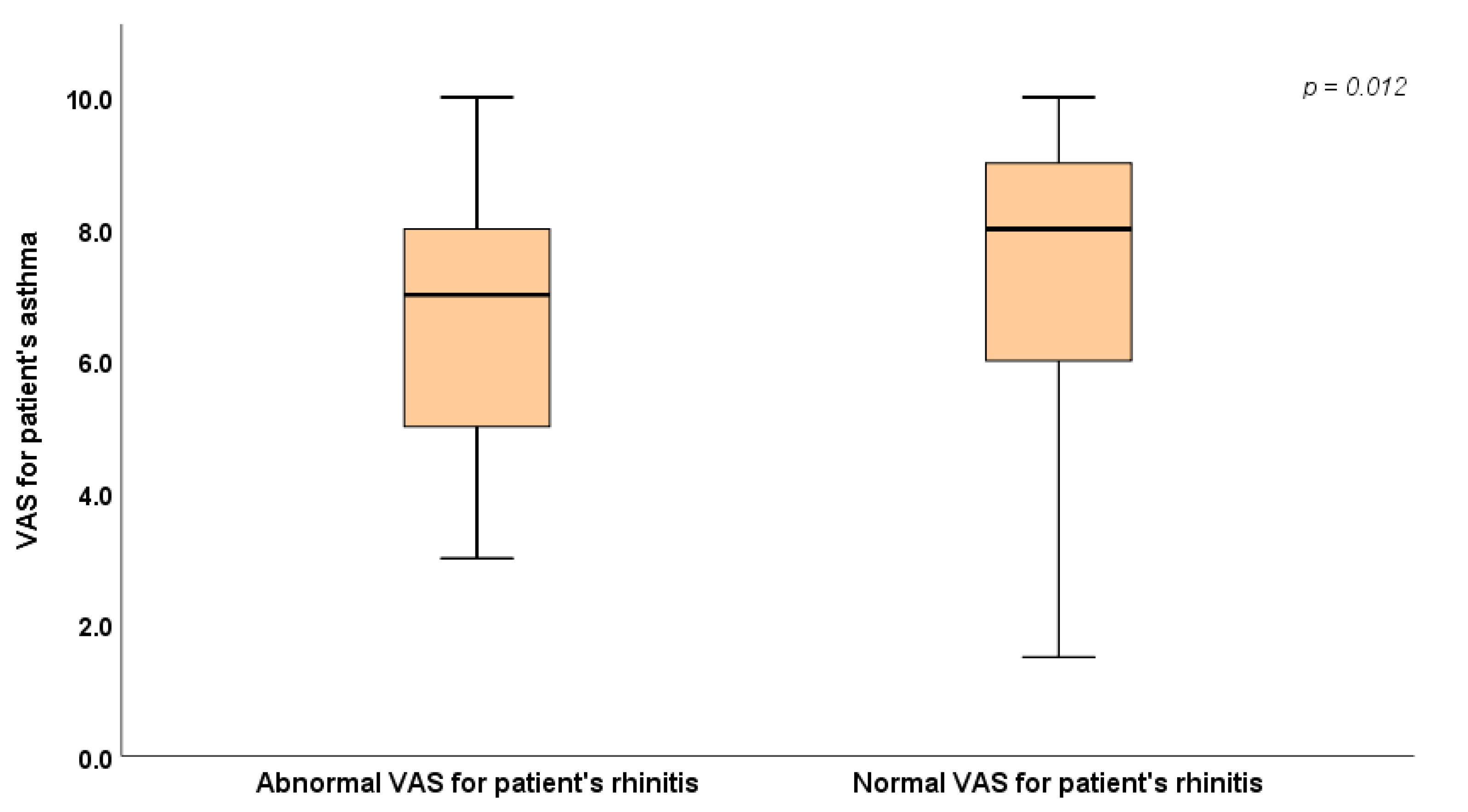
Figure 2.
VAS scores for asthma symptoms assessed by doctor in patients with abnormal or normal VAS for nasal symptoms.
Figure 2.
VAS scores for asthma symptoms assessed by doctor in patients with abnormal or normal VAS for nasal symptoms.
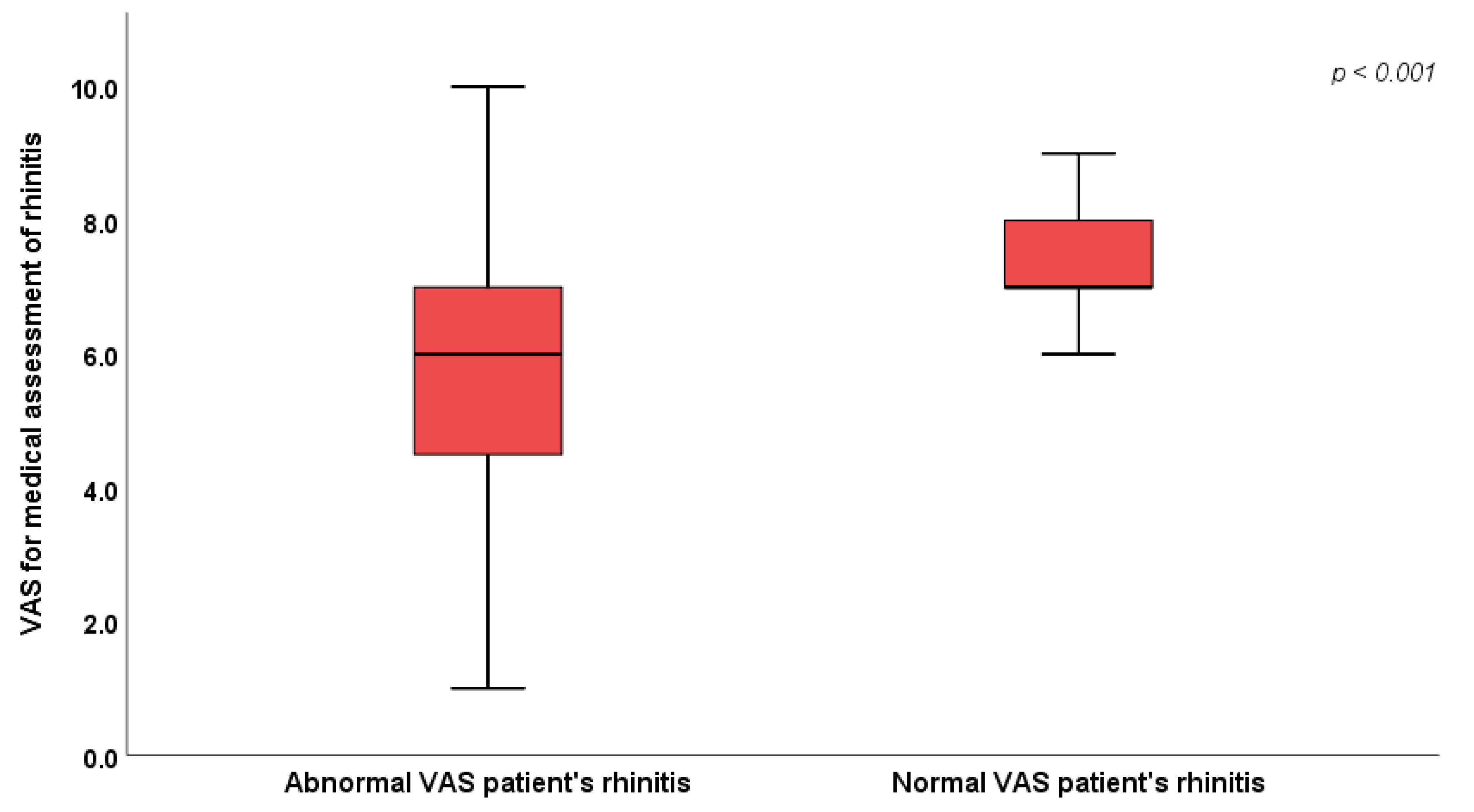

Table 1.
Demographic and clinical characteristics.
| Sex | Female | 56 (37.3%) |
|---|---|---|
| Male | 94 (62.7%) | |
| Age | 11.8 ± 3.06 | |
| VAS for nasal symptoms’ severity (perceived by patients) | 6.3 (5.0 - 8.0) | |
| VAS for doctor’s assessment of rhinitis | 7.0 (6.0 - 8.0) | |
| Antihistamines | 75 (50.0%) | |
| Intranasal Corticosteroids | 24 (16.0%) | |
| Specific allergen immunotherapy (AIT) | 26 (17.3%) | |
| Sensitizations | Mono-sensitization | 10 (6.7%) |
| Poly-sensitization | 140 (93.3%) | |
| Asthma comorbidity | 100 (67.1%) | |
| Treatment for asthma | 46 (46.0%) | |
| VAS for asthma symptoms’ severity (perceived by patients with asthma) | 7.0 (6.0 - 8.5) | |
| VAS for medical assessment of asthma | 7.0 (5.0 - 9.0) | |
Table 2.
Intergroup comparison between patients with normal (>6) or abnormal VAS for nasal symptoms.
Table 2.
Intergroup comparison between patients with normal (>6) or abnormal VAS for nasal symptoms.
| Abnormal (N = 75) | Normal (N = 75) | p | ||
|---|---|---|---|---|
| Sex | Female | 30 (40.0%) | 26 (34.7%) | 0.50 |
| Male | 45 (60.0%) | 49 (65.3%) | ||
| Age | 12.1 ± 2.98 | 11.6 ± 3.15 | 0.29 | |
| Antihiostamines | No | 35 (46.7%) | 40 (53.3%) | 0.41 |
| Yes | 40 (53.3%) | 35 (46.7%) | ||
| Intranasal Corticosteroids | No | 61 (81.3%) | 65 (86.7%) | 0.37 |
| Yes | 14 (18.7%) | 10 (13.3%) | ||
| Specific allergen immunotherapy (AIT) | No | 63 (84.0%) | 61 (81.3%) | 0.67 |
| Yes | 12 (16.0%) | 14 (18.7%) | ||
| Mono- or poly-sensitization | Mono-sensitization | 3 (4.0%) | 7 (9.3%) | 0.19 |
| Poly-sensitization | 72 (96.0%) | 68 (90.7%) | ||
| Asthma comorbidity | No | 27 (36.0%) | 22 (29.7%) | 0.42 |
| Yes | 48 (64.0%) | 52 (70.3%) | ||
| Treatment for asthma | No | 27 (55.1%) | 27 (52.9%) | 0.83 |
| Yes | 22 (44.9%) | 24 (47.1%) | ||
| VAS for medical assessment of rhinitis | 6.0 (4.0 – 7.0) | 7.0 (7.0 – 8.0) | <0.001* | |
| VAS for patient's asthma (subgroup of patients with asthma) | 7.0 (5.0 - 8.0) | 8.0 (6.0 - 9.0) | 0.012* | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



