
Submitted:
03 October 2023
Posted:
04 October 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
At present Coronavirus disease-2019 (COVID-19) is one of the leading contributing factor to mortality and the impact of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection on the sinonasal tract has become more prominent, particularly with the rising awareness of olfactory dysfunction (OD). We extracted data from published papers available in electronic databases (Wiley online library, PubMed, and Nature). We used the following search terms alone or with combinations - Olfactory dysfunction, SARS-CoV-2, mechanism and treatments. We found worldwide up to 98% of patients confirmed OD due to COVID-19. Current studies have implied that regardless of the high self-reported recovery rate, 25–40% of patients after 1 or 2 months and approximately 15%–28% of patients at six months struggle to fully restore their sense of smell. Moreover, female sex, younger and older age, active smoking, and chronic lung disease are reported as the associated risk factors of OD. Although the pathophysiological mechanism of action(s) of the OD is yet to be explored in depth, central nervous system (CNS) entrance, olfactory bulb (OB) and sustentacular cell damage, neural routes inflammation, non-neuronal cells damage, decreased OB volume and deregulation of olfactory receptor genes are among the commonly reported mechanisms for the development of OD.
Keywords:
COVID-19
; SARS-CoV-2
; mechanism of action
; smell loss
; olfactory dysfunction
; anosmia
; treatment
1. Introduction
The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) triggers the respiratory viral infection known as Coronavirus disease-2019 (COVID-19) [1]. The first COVID-19 case was identified in December 2019 in Wuhan, China [2] and rapidly spreading worldwide [1,3]. As of July 2023, approximately 767 million COVID-19 cases were confirmed while more than 6.9 million people died globally (https://covid19.who.int/). The term "post-acute sequela of SARS-CoV-2 infection" (PASC) covers a wide spectrum of multi-systemic symptoms which appear 4 or more weeks after infection, regardless of infection severity [4]. These symptoms last more than 24 weeks or 6 months [5,6]. Among all the sequelae, one emerging global health concern is persistent post-viral olfactory dysfunction (OD) [7]. Although many patients recover spontaneously from their OD [8], persistent smell loss is typically the most common post-viral symptoms which are seriously impacting the quality of life [8,9,10].
Persistent OD symptoms include complete lack of olfactory sense (Anosmia), reduced olfactory sense (Hyposmia), distorted olfactory sense (Parosmia), and sensing odors that do not exist (Phantosmia) [11]. Among all symptoms, patients with Parosmia reported a distorted smell commonly described as a "smoky or burnt odor" [12,13]. Parosmia is prevalent among patients with OD, such as conventional post-viral OD, and is less likely to happen in COVID-19-induced OD [11,14]. Statistics from the first wave of the COVID-19 in 2020 reported smell loss in 5-85% of individual afflicted with the SARS-CoV-2 virus based on mild and severe cases [15,16,17,18,19,20,21,22,23,24], however, a comprehensive meta-analysis decreased the figure to 77% using objective olfactory function tests method [25]. Intriguingly, study by Chiesa-Estomba et al. (2020) reported that most people quickly recover their sense of smell within 10 ± 6 days as smell restoration was as rapid as its loss [26]. However, newer data on OD have suggested that 25-40% of patients after 1-2 months [27,28] and around 15%-28% of patients after 6 months [28,29] do not completely restore their sense of smell. Additionally, patients with COVID-19 also frequently report alterations to their sense of smell which is 40–50% of people on average, globally [15,30]. When objectively assessed, up to 98% of patients confirm OD [31].
Recently, Butowt et al. (2023) reported that the degeneration of support cells which are infected in the olfactory epithelium (OE) induces altered mucus composition and retraction of the cilia on olfactory receptor neurons [32]. Additionally, Chee et al. (2023) explained there are variations in susceptibility to the key receptors necessary virus to enter, angiotensin-converting enzyme 2 (ACE2) and transmembrane serine protease 2 (TMPRSS2) across various populations of people and different SARS-CoV-2 variants [33]. Karimian et al. (2022) also mentioned that TMPRSS2 may facilitate OD [34]. However, an in-depth study of all possible mechanism of action is yet to be reported. Current literature review scrutinizes the novel cellular and molecular mechanism of actions involved in persistent OD induced by SARS-CoV-2. We pointed out the risk factors associated with persistent OD. We also discuss the prevalence, recent treatments along with different chemical compounds to treat OD as PASC in the future. In addition to that, we also explore the limitations, potential OD-induced diseases, and future perspectives.
2. Epidemiology of Persistent OD Induced by COVID-19
The COVID-19-induced OD is considered as a specific indicator of COVID-19 diagnosis since i) a high percentage of patients possess the symptoms [35,36,37,38], ii) is the earliest symptom compared to other symptoms, and iii) in some patients with COVID-19, it appears as the only symptom [12,23]. Persistent OD is found to be more common in patients infected with wild-type SARS-CoV-2 and less common in Omicron and Delta variants (B.1.617.2) infected patients [39,40]. The possible reason suggested by National Institute of Infectious Diseases that the viral RNA amount decreases after six days of infections and no detection of infectious virus since diagnosis or symptom after 10 days (https://www.niid.go.jp/niid/en/2019-ncov-e/10884-covid19-66-en.html). The incidence of COVID-19-induced OD ranges from 32-87% [36,37]. However, it affects 50-75% of the individuals who are diagnosed with COVID-19 in the acute stage [23,41,42].
3. Role of Host Factors in OD
COVID-19-induced OD is more prevalent among young adults (ranging from 20-40 years old), women, and people with relatively mild disease [43,44,45]. Compared to male patients, female patients were more inclined to have persistent OD symptoms [29,46,47,48,49]. Possible reasons could be explained by the findings that women have more cells than men in the olfactory bulb (OB) which is a dedicated part of the brain for olfaction [50]. Moreover, several studies [51,52,53,54] have found that women have higher odor-identification abilities than men. The female endocrine system and the impact of estrogen on the perception of smell have also been discussed as possible explanations for gender variations in olfactory performance [52,55]. However, no significant gender differences in intranasal volume have been reported [56,57].
The distribution of OD varies by geographic area as well. The prevalence of OD in Western countries exceeds 50%, whereas it is only about 30% in Asian countries suggesting the role of host genetics in the development of OD [58,59]. Other cultural habits of Asian people including- using masks and other face coverings in public [60], and eating and drinking materials containing phytochemicals with antiviral effects may also explain higher prevalence of OD among them.
4. Association of Different Variants of SARS-CoV-2 with OD
Prevalence of persistent OD varies within different variants of SARS-CoV-2 [61]. First, the so-called wild type was first overtaken by B.1.1.7 (a variant of concern (VOC) alpha) at the starting of 2021, but it was rapidly supplanted by the considerably more deadly B.1.1617.2 (VOC delta); however, B.1.1.529 (VOC omicron), which was not discovered until late in November 2021, has already propagated globally [62]. According to a study by Vaira et al. (2022), self-reported olfactory loss occurs in 72.4%, 75.4%, 65.6%, and 18.1% of cases of the D614G mutation group, Alpha group, Delta group, and Omicron group, respectively. Additionally, psychophysical testing showed that the prevalence of OD in the D614G mutation group, Alpha, Delta, and Omicron groups, was 80.6%, 83.0%, 65.6%, and 36.3%, respectively and there were no statistically significant variations between the D614G, Alpha, and Delta groups [63]. According to epidemiological research where factors including age, gender, and co-morbidities showed the frequency of OD was lowest among Omicron variations, then the Delta variant, and finally the Alpha variant [62,64,65]. Numerous individuals who had minor COVID-19 infections throughout both Gamma and Omicron waves had a lower rate of reporting OD than individuals who had infections at the time of the initial lineages, according to Cardoso et al. (2022) (original lineages 52.6%, Alpha 29.0%, Gamma 27.5%, Delta 41.2%, Omicron 5.8%) (Figure 1) [33,64,66].
5. Risk Factors of OD
Considering the persistent nature of OD in a significant percentage of people even after two years of disease onset, it is critical measuring the clinical as well as the demographic factors linked to OD in COVID-19 patients. There are some debates about the age and persistence of OD in COVID-19. Studies by Nalbandian et al. (2021) and Groff et al. (2021) identified a connection between age and the occurrence of OD in prolonged COVID-19 [67,68]. However, increased co-morbidities and prescription drugs in elderly individuals could additionally impact the clinical course of OD [69,70]. Additionally, fever, cough, expectoration, stuffy nose, nasal congestion, purulent nasal, sore throat, foul breath, and xerostomia (oral dryness) are typical symptoms observed in patients with OD and patients who have suffered from three or more upper respiratory symptoms were prone to experience OD [71].
Based on the findings of multivariate analysis, risk factors associated with reporting a loss of smell were younger age [67,68], asthma [72], emphysema [73], female sex [29,46,47,48,49], or cough [49,71,74]. A clinical risk category approach by Johnson et al. (2022) [72], revealed the high-risk patients and individuals who were most likely to get serious infections and poor clinical outcomes. Moreover, age elder than 65 years, chronic lung disease (e.g. chronic obstructive pulmonary disease , idiopathic pulmonary fibrosis, asthma, liver cirrhosis, emphysema, cystic fibrosis, and bronchiectasis), active smoker, congestive heart failure, end-stage renal disease, active chemotherapy, history of diabetes or obesity with body mass index over 40 were considered to form this category [72]. The findings of different studies investigating the parameters of OD in epidemiological and clinical level are summarized in Table 1.
6. Pathophysiological Mechanisms of Actions of OD
SARS-CoV-2 penetrates the host system by connecting to two key receptors ACE2 and TMPRSS2 [87]. The OE contains a significant amount of ACE2 and TMPRSS2 receptors, particularly in sustentacular non-neural and neural stem cells [88,89]. Almost all Coronaviruses i.e. SARS-CoV [90], MERS-CoV [91], and HCoV-229E [92] are neuroinvasive. In case of COVID-19, ACE2 expression has been detected within olfactory neurons [93], suggesting that SARS-CoV-2 could affect the development of olfactory sense by entering the central nervous system through olfactory nerves [94]. The possible mechanism of action(s) is described below (Figure 2):
6.1. Central Nervous System (CNS) Entrance
SARS-CoV-2 travels via axons within ensheathing or transneuronal cell to enter the host via CNS [95,96]. However, Neuropilin-1 (NRP-1), a trans-membrane glycoprotein functioning as a receptor for various ligands has been identified in the mitral cell of the OB, a region designated for smelling [97,98]. Mitral cells also express ACE2 and TMPRSS2 receptors and Neuropilin-1 has been implicated in viral retrograde axonal transport which may facilitate SARS-CoV-2 entry [98,99,100].
Additionally, interference of NRP-1 with semaphorine-3A (SEMA3A), a protein crucial for neuronal development [101,102], may lead to damage of axon and neuronal death eventually resulting in OD [103]. When SARS-CoV-2 enters pericytes, the blood-brain barrier is disrupted as a consequence of the production of many proinflammatory cytokines e.g. interferon-y (INF-y), interleukin-1 (IL-1), IL-6, IL-12, and tumor necrosis factor-alpha (TNFɑ) [104,105]. This subsequently leads to neurotoxicity, microvascular damage, and hypoperfusion to olfactory sensory neurons (OSNs), resulting in neuronal death and ultimately OD [106,107,108,109,110].
6.2. OB and Sustentacular Cell Damage
The transneuronal pathway of OSNs appears to be the quickest and most devastating route for SARS-CoV-2 to infect the OB [111,112]. Although, study by Khan et al. (2021) did not find evidence demonstrating the direct attack inflicted by SARS-CoV-2 on the olfactory route [113]. Direct damage is unlikely to be a factor in viral invasion since OSNs lack the ACE2 and TMPRSS2 required for SARS-CoV-2 entry [107,114]. Based on postmortem studies, sustentacular cells in the olfactory mucosa have been a primary target cell type with no data supporting the infection of OSNs in the OB parenchyma [113]. In sustentacular cells of the olfactory sensory epithelium (OSE), ACE2 expression occurs one hundred times greater than in the respiratory epithelium [115]. At the upper portion of the nasal canal, the increased expression of ACE2 may result in an unusually elevated viral load [116,117]. Consequently, leads to alteration to the olfactory pathway through sustentacular cell damage rather than direct damage on OSNs [118].
6.3. Neural Routes Inflammation
The terminal nerve (Nervus terminals or Cranial Nerve 0) and the trigeminal nerve are two nerves that run near the OB [119]. The trigeminal nerve forms an alternate pathway through CNS since the endings control the OE and branch to reach the OB [120,121,122,123]. Both nerves have ACE2 and TMPRSS2 receptors and packed ramification in the sinus cavities, OSE, and around the Cribriform plate [89,124]. Evidences suggest that SARS-CoV-2 compromises Gonadotropin-releasing hormone secreting neurons located in terminal nerve, implying the involvement of terminal nerve [125,126]. Additionally, every branch of the trigeminal nerve has been discovered to be carrying the virus. [127].
6.4. Non-Neuronal Cells Damage
SARS-CoV-2 infection can negatively influence non-neuronal cells in the olfactory sensory epithelium, such as Bowman's glands, basal cells, and stem cells which generate new OSNs and olfactory ensheathing cells [128,129]. Surprisingly, SARS-CoV-2 infection triggers significant death of cells and infiltration of immune cells, which immediately impairs the regularity of the OE structure and ultimately leading to OD [129]. Moreover, the origin of this infection is most likely to be peripheral indicating the short latency and rapid remission of COVID-19-induced OD [119].
6.5. Decreased OB Volume
Changes in the volume of OB may trigger persistent OD in COVID-19 and there have been multiple observations of decreased OB volume in COVID-19 patients with OD [130,131,132]. The virus invades the CNS by penetrating the interface of neural-mucosal within olfactory mucosa, and then passes through the designated neuroanatomical locations [127]. The OB volume may decrease during the chronic stage of COVID-19 due to neuroinflammation and neuroglial reaction triggered by direct SARS-CoV-2 virus damage to the OB and related neuroanatomical structures [131].
6.6. Deregulation of Olfactory Receptor Genes
Infection with SARS-CoV-2 may elevate the expression of G protein signaling 2 (RGS2), a crucial regulator of odorant receptors [133]. Moreover, there was a considerable increase in RGS2 expression during the initial stages of infection, and it was highly linked with PTGS2- prostaglandin endoperoxide synthase 2, IL1B - Interleukin 1 Beta , CXCL8- C-X-C Motif Chemokine Ligand 8, NAMPT- Nicotinamide phosphoribosyltransferase, and other inflammatory markers [134]. These findings suggest that OD, especially Anosmia in COVID-19 patients may be caused by the upregulated RGS2 expression [135]. Additionally, RGS2 is hypothesized for the activatation of Golf, a Gsα-like G protein, upon odorant binding [136]. Golf-mediated Adenylate cyclase III (ACIII) activation boosts intracellular cyclic adenosine monophosphate (cAMP) levels, enabling a cyclic-nucleotide-gated channel to open. The passage of cations (Na+, Ca2+) via this channel results in an action potential generation, permiting the primary neuron to communicate with brain [137]. But SARS-CoV-2 may upregulate G protein leading to OD.
6.7. Drug-Induced OD
Zinc supplements are routinely prescribed during Covid-19 disease [138]. Study by Debbaneh et al. (2023) [139] reported zinc products and fluticasone propionate are found to be associated with OD, specifically reduced olfaction. Moreover, Varenicline and Fluticasone propionate are found to be linked to altered smell, although antineoplastic and immunomodulatory medications were responsible for 21.6% of olfactory adverse reactions and taken all of these together may indicate that drugs used during COVID-19 infections could give rise to OD [139].
7. Current Therapeutic Options
Researchers have recently discovered possible treatments for post-viral OD e.g. olfactory training [140,141,142,143], platelet-rich plasma [144,145,146], corticosteroid treatments [147,148,149], anti-neuroinflammatory therapy with co-ultra micronized palmitoylethanolamide with luteolin [150,151,152,153]. In addition, various medications and dietary supplements have been suggested for the treatment of non-conductive smell problems, including post-viral OD e.g. minocycline [154], theophylline [155], insulin [156] , caroverine [157], sodium citrate [158], alpha-lipoic acid [159], tokishakuyakusan (herbal medicine) [160], and vitamin A [161]. Nevertheless, the efficiency of most of these treatments remains unreliable.
Recently, a novel acellular secretome therapy (ST266) [162] and monoclonal antibodies [163,164] have gained attention for the future treatments of OD. ST266 is a novel biologic amnion-derived multipotent progenitor cells that contain secreted anti-inflammatory cytokines and growth factors [165,166] and monoclonal antibodies e.g. sarilumab appear to provide the best results with significant improvements in olfactory test measurements; however, high-quality trials with larger sample sizes are required for further analysis [167].
8. Limitations and Knowledge Gaps
Since the onset of the pandemic, significant progress has been conducted regarding comprehending sinonasal pathology in infection with SARS-CoV-2. Nevertheless, olfactory analysis is subjective and reviews are retroactive in nature [7,168,169], as a result the projection of the actual effect of OD may be inaccurate. Besides, a hypothesis linking the mechanism of actions and the development of OD to recovery rates has not yet been determined. Additionally, it is uncertain if the degree of smell loss and how rapidly it returns could be utilized to figure out the degree of severity a COVID-19 infection will be [170]. Understanding the real impact of the virus and improving the ability to forecast upper respiratory tract symptoms would also benefit from studies investigating molecular pathways, cytokine responses, and distinct SARS-CoV-2 variations at different stages of infection [171]. In addition, in-depth research is required to improve procedures for estimating the prevalence of sensory loss. Insights into the pathways causing OD in COVID-19 may shed light on other neurological symptoms reported in these patients [135].
9. Future Perspectives and Conclusions
Although OD is still a substantial and lasting side effect of the COVID-19 pandemic, more awareness can encourage research which facilitates the development of essential therapeutic alternatives. Recently, many individuals suffering from persistent OD reported decreased standards of life and display more signs of depression and anxiety [172,173]. Moreover, OD could trigger abnormal eating patterns e.g. higher consumption of sugar and salt or anorexia, which could lead to malnutrition and sudden weight loss [174,175]. Interestingly, OD has been one of the earliest symptoms of Parkinson’s disease, Alzheimer’s disease, and other Lewy body diseases [176,177,178]. Many of these diseases, which have started with OD, might progress to dementia [179,180]. Although it is not currently an effective diagnostic tool, the loss of olfactory function could influence the brain alterations which contribute to various disorders [176,177,178]. Further research is yet to be done to understand the mechanism of inducing different diseases by OD.
With numerous findings that emerged in the literature, clinicians must include a standard of care evaluation of olfactory function when treating individuals with a suspected or confirmed COVID-19 diagnosis. Regular in-home olfactory self-evaluation may be a useful place to start, given that psychophysical testing may not be feasible for many patients. In a nutshell, longitudinal evaluations of chemosensory function could assist in identifying individuals who may need further care and non-pharmacological therapies if they have a chronic olfactory impairment. In consideration of the growing significance of genetic variation for viral cell entrance and immune response to virus infection, future research must assess background of the genetic host which may impact the clinical phenotype as well as a response to vaccinations and medications [171].
Authors Contribution
Conceptualization, A.A.; Methodology, A.A. and N.T.; Validation, A.A, N.D., N.T. and N.K.; Writing – Original Draft Preparation, N.T. and N.K.; Writing – Review & Editing, A.A. N.D., N.T. and N. K.; Visualization, N.T.; Supervision, A.A.; Project Administration, N.D.
Funding
The authors did the review from their common interest and did not get any funds or remuneration for it.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability
Data was extracted from published papers available in electronic databases (Wiley online library, PubMed, and Nature) in the English language. Keywords used alone or with combination: Olfactory dysfunction, COVID-19, SARS-CoV-2, mechanism, smell loss, treatments.
Conflicts of Interest
The corresponding author declares no conflict of interest.
References
- Pan, A., et al., Association of Public Health Interventions With the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA, 2020. 323(19): p. 1915-1923. [CrossRef]
- Kim, H., Outbreak of novel coronavirus (COVID-19): What is the role of radiologists? European Radiology, 2020. 30(6): p. 3266-3267. [CrossRef]
- Brito, D.T.M., et al., The possible benefits of vitamin D in COVID-19. Nutrition, 2021. 91-92: p. 111356. [CrossRef]
- Parker, A.M., et al., Addressing the post-acute sequelae of SARS-CoV-2 infection: a multidisciplinary model of care. The Lancet Respiratory Medicine, 2021. 9(11): p. 1328-1341. [CrossRef]
- Huang, C., et al., 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet, 2021. 397(10270): p. 220-232. [CrossRef]
- Fernández-de-las-Peñas, C., et al., Defining Post-COVID Symptoms (Post-Acute COVID, Long COVID, Persistent Post-COVID): An Integrative Classification. International Journal of Environmental Research and Public Health, 2021. 18(5): p. 2621.
- Tan, B.K.J., et al., Prognosis and persistence of smell and taste dysfunction in patients with covid-19: meta-analysis with parametric cure modelling of recovery curves. Bmj, 2022. 378: p. e069503. [CrossRef]
- Patel, Z.M., et al., International consensus statement on allergy and rhinology: Olfaction. International Forum of Allergy & Rhinology, 2022. 12(4): p. 327-680. [CrossRef]
- Said, M., et al., Clinical factors associated with lower health scores in COVID-19-related persistent olfactory dysfunction. Int Forum Allergy Rhinol, 2022. 12(10): p. 1242-1253. [CrossRef]
- Burges Watson, D.L., et al., Altered smell and taste: Anosmia, parosmia and the impact of long Covid-19. PLoS One, 2021. 16(9): p. e0256998. [CrossRef]
- Koyama, S., E. Mori, and R. Ueha, Insight into the mechanisms of olfactory dysfunction by COVID-19. Auris Nasus Larynx, 2022. p. [CrossRef]
- Koyama, S., R. Ueha, and K. Kondo, Loss of Smell and Taste in Patients With Suspected COVID-19: Analyses of Patients' Reports on Social Media. J Med Internet Res, 2021. 23(4): p. e26459. [CrossRef]
- Parma, V., et al., More Than Smell-COVID-19 Is Associated With Severe Impairment of Smell, Taste, and Chemesthesis. Chem Senses, 2020. 45(7): p. 609-622. [CrossRef]
- Koyama, S., et al., Possible Use of Phytochemicals for Recovery from COVID-19-Induced Anosmia and Ageusia. Int J Mol Sci, 2021. 22(16): p. [CrossRef]
- Lechien, J.R., et al., Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. European Archives of Oto-Rhino-Laryngology, 2020. 277(8): p. 2251-2261. [CrossRef]
- Parma, V., et al., More Than Smell—COVID-19 Is Associated With Severe Impairment of Smell, Taste, and Chemesthesis. Chemical Senses, 2020. 45(7): p. 609-622. [CrossRef]
- Bagheri, S., et al., Coincidence of COVID-19 epidemic and olfactory dysfunction outbreak. Med J Islam Repub. Iran, 2020.
- Hopkins, C., P. Surda, and N. Kumar, Presentation of new onset anosmia during the COVID-19 pandemic. Rhinology, 2020. 58(3): p. 295-298. [CrossRef]
- Gane, S.B., C. Kelly, and C. Hopkins, Isolated sudden onset anosmia in COVID-19 infection. A novel syndrome? Rhinology, 2020. 58(3): p. 299-301. [CrossRef]
- Lechien, J.R., et al., Objective olfactory testing in patients presenting with sudden onset olfactory dysfunction as the first manifestation of confirmed COVID-19 infection. medRxiv, 2020. p. 2020.04.15.20066472. [CrossRef]
- Menni, C., et al., Loss of smell and taste in combination with other symptoms is a strong predictor of COVID-19 infection. MedRxiv, 2020. p. 2020.04. 05.20048421.
- Mao, L., et al., Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol, 2020. 77(6): p. 683-690. [CrossRef]
- Lechien, J.R., et al., Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol, 2020. 277(8): p. 2251-2261. [CrossRef]
- Haldrup, M., M.I. Johansen, and A.W. Fjaeldstad, Lugte-og smagstab som primære symptom på COVID-19. Ugeskr Læger, 2020. 182: p. V04200205.
- Hannum, M.E., et al., Objective Sensory Testing Methods Reveal a Higher Prevalence of Olfactory Loss in COVID-19–Positive Patients Compared to Subjective Methods: A Systematic Review and Meta-Analysis. Chemical Senses, 2020. 45(9): p. 865-874. [CrossRef]
- Chiesa-Estomba, C.M., et al., Patterns of smell recovery in 751 patients affected by the COVID-19 outbreak. Eur J Neurol, 2020. 27(11): p. 2318-2321. [CrossRef]
- Gerkin, R.C., et al., Recent Smell Loss Is the Best Predictor of COVID-19 Among Individuals With Recent Respiratory Symptoms. Chem Senses, 2021. 46: p. [CrossRef]
- Blomberg, B., et al., Long COVID in a prospective cohort of home-isolated patients. Nature Medicine, 2021. 27(9): p. 1607-1613. [CrossRef]
- Klein, H., et al., Onset, duration and unresolved symptoms, including smell and taste changes, in mild COVID-19 infection: a cohort study in Israeli patients. Clin Microbiol Infect, 2021. 27(5): p. 769-74. [CrossRef]
- von Bartheld, C.S., M.M. Hagen, and R. Butowt, Prevalence of Chemosensory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis Reveals Significant Ethnic Differences. ACS Chem Neurosci, 2020. 11(19): p. 2944-2961. [CrossRef]
- Moein, S.T., et al., Smell dysfunction: a biomarker for COVID-19. Int Forum Allergy Rhinol, 2020. 10(8): p. 944-950. [CrossRef]
- Butowt, R., K. Bilinska, and C.S. von Bartheld, Olfactory dysfunction in COVID-19: new insights into the underlying mechanisms. Trends Neurosci, 2023. 46(1): p. 75-90. [CrossRef]
- Chee, J., et al., Pathophysiology of SARS-CoV-2 Infection of Nasal Respiratory and Olfactory Epithelia and Its Clinical Impact. Curr Allergy Asthma Rep, 2023. 23(2): p. 121-131. [CrossRef]
- Karimian, A., M. Behjati, and M. Karimian, Molecular mechanisms involved in anosmia induced by SARS-CoV-2, with a focus on the transmembrane serine protease TMPRSS2. Arch Virol, 2022. 167(10): p. 1931-1946. [CrossRef]
- Beltrán-Corbellini, Á., et al., Acute-onset smell and taste disorders in the context of COVID-19: a pilot multicentre polymerase chain reaction based case-control study. Eur J Neurol, 2020. 27(9): p. 1738-1741. [CrossRef]
- Tong, J.Y., et al., The Prevalence of Olfactory and Gustatory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis. Otolaryngol Head Neck Surg, 2020. 163(1): p. 3-11. [CrossRef]
- Ibekwe, T.S., A.J. Fasunla, and A.E. Orimadegun, Systematic Review and Meta-analysis of Smell and Taste Disorders in COVID-19. OTO Open, 2020. 4(3): p. 2473974x20957975. [CrossRef]
- Liang, Y., et al., Neurosensory dysfunction: A diagnostic marker of early COVID-19. Int J Infect Dis, 2020. 98: p. 347-352. [CrossRef]
- Butowt, R., K. Bilińska, and C. von Bartheld, Why Does the Omicron Variant Largely Spare Olfactory Function? Implications for the Pathogenesis of Anosmia in Coronavirus Disease 2019. J Infect Dis, 2022. 226(8): p. 1304-1308. [CrossRef]
- Klimek, L., et al., Olfactory dysfunction is more severe in wild-type SARS-CoV-2 infection than in the Delta variant (B.1.617.2). World Allergy Organ J, 2022. 15(6): p. 100653. [CrossRef]
- Vaira, L.A., et al., Olfactory and gustatory function impairment in COVID-19 patients: Italian objective multicenter-study. Head Neck, 2020. 42(7): p. 1560-1569. [CrossRef]
- Andrews, P.J., et al., Olfactory and taste dysfunction among mild-to-moderate symptomatic COVID-19 positive health care workers: An international survey. Laryngoscope Investig Otolaryngol, 2020. 5(6): p. 1019-1028. [CrossRef]
- Lechien, J.R., et al., Prevalence and 6-month recovery of olfactory dysfunction: a multicentre study of 1363 COVID-19 patients. J Intern Med, 2021. 290(2): p. 451-461. [CrossRef]
- Speth, M.M., et al., Olfactory Dysfunction and Sinonasal Symptomatology in COVID-19: Prevalence, Severity, Timing, and Associated Characteristics. Otolaryngol Head Neck Surg, 2020. 163(1): p. 114-120. [CrossRef]
- Whitcroft, K.L. and T. Hummel, Olfactory Dysfunction in COVID-19: Diagnosis and Management. Jama, 2020. 323(24): p. 2512-2514. [CrossRef]
- Hintschich, C.A., et al., Persisting olfactory dysfunction in post-COVID-19 is associated with gustatory impairment: Results from chemosensitive testing eight months after the acute infection. PLoS One, 2022. 17(3): p. e0265686. [CrossRef]
- Bussière, N., et al., Chemosensory Dysfunctions Induced by COVID-19 Can Persist up to 7 Months: A Study of Over 700 Healthcare Workers. Chem Senses, 2021. 46: p. [CrossRef]
- Petrocelli, M., et al., Six-month smell and taste recovery rates in coronavirus disease 2019 patients: a prospective psychophysical study. J Laryngol Otol, 2021. 135(5): p. 436-441. [CrossRef]
- Tan, B.K.J., et al., Prognosis and persistence of smell and taste dysfunction in patients with covid-19: meta-analysis with parametric cure modelling of recovery curves. BMJ, 2022. 378: p. e069503. [CrossRef]
- Oliveira-Pinto, A.V., et al., Sexual Dimorphism in the Human Olfactory Bulb: Females Have More Neurons and Glial Cells than Males. PLOS ONE, 2014. 9(11): p. e111733. [CrossRef]
- Brand, G. and J.L. Millot, Sex differences in human olfaction: between evidence and enigma. Q J Exp Psychol B, 2001. 54(3): p. 259-70. [CrossRef]
- Sorokowski, P., et al., Sex Differences in Human Olfaction: A Meta-Analysis. Front Psychol, 2019. 10: p. 242. [CrossRef]
- Oleszkiewicz, A., et al., Updated Sniffin' Sticks normative data based on an extended sample of 9139 subjects. Eur Arch Otorhinolaryngol, 2019. 276(3): p. 719-728. [CrossRef]
- Larsson, M., M. Lövdén, and L.-G. Nilsson, Sex differences in recollective experience for olfactory and verbal information. Acta Psychologica, 2003. 112(1): p. 89-103. [CrossRef]
- Doty, R.L. and E.L. Cameron, Sex differences and reproductive hormone influences on human odor perception. Physiol Behav, 2009. 97(2): p. 213-28. [CrossRef]
- Schriever, V.A., et al., Size of nostril opening as a measure of intranasal volume. Physiol Behav, 2013. 110-111: p. 3-5. [CrossRef]
- Verbeurgt, C., et al., Profiling of olfactory receptor gene expression in whole human olfactory mucosa. PLoS One, 2014. 9(5): p. e96333. [CrossRef]
- Pereira, N.L., et al., COVID-19: Understanding Inter-Individual Variability and Implications for Precision Medicine. Mayo Clin Proc, 2021. 96(2): p. 446-463. [CrossRef]
- Kim, J.W., et al., Regional and Chronological Variation of Chemosensory Dysfunction in COVID-19: a Meta-Analysis. J Korean Med Sci, 2021. 36(4): p. e40. [CrossRef]
- Kemmelmeier, M. and W.A. Jami, Mask Wearing as Cultural Behavior: An Investigation Across 45 U.S. States During the COVID-19 Pandemic. Front Psychol, 2021. 12: p. 648692. [CrossRef]
- Hintschich, C.A., et al., Prevalence of acute olfactory dysfunction differs between variants of SARS-CoV-2—results from chemosensitive testing in wild type, VOC alpha (B.1.1.7) and VOC delta (B.1617.2). European Archives of Oto-Rhino-Laryngology, 2022. 279(11): p. 5445-5447. [CrossRef]
- Hintschich, C.A., et al., Prevalence of acute olfactory dysfunction differs between variants of SARS-CoV-2-results from chemosensitive testing in wild type, VOC alpha (B.1.1.7) and VOC delta (B.1617.2). Eur Arch Otorhinolaryngol, 2022. 279(11): p. 5445-5447. [CrossRef]
- Vaira, L.A., et al., Prevalence of olfactory dysfunction in D614G, alpha, delta and omicron waves: a psychophysical case-control study. Rhinology journal, 2022. 0(0): p. 0-0. [CrossRef]
- Cardoso, C.C., et al., Olfactory Dysfunction in Patients With Mild COVID-19 During Gamma, Delta, and Omicron Waves in Rio de Janeiro, Brazil. Jama, 2022. 328(6): p. 582-583. [CrossRef]
- Menni, C., et al., Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: a prospective observational study from the ZOE COVID Study. Lancet, 2022. 399(10335): p. 1618-1624. [CrossRef]
- Laracy, J.C., et al., Comparison of coronavirus disease 2019 (COVID-19) symptoms at diagnosis among healthcare personnel before and after the emergence of the omicron variant. Infect Control Hosp Epidemiol, 2022. p. 1-3. [CrossRef]
- Nalbandian, A., et al., Post-acute COVID-19 syndrome. Nat Med, 2021. 27(4): p. 601-615. [CrossRef]
- Groff, D., et al., Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw Open, 2021. 4(10): p. e2128568. [CrossRef]
- Reis, D., et al., Long-term prevalence of taste and olfactory dysfunction in COVID-19 patients: A cross-sectional study. Oral Dis, 2022. 28 Suppl 2: p. 2516-2521. [CrossRef]
- Cristillo, V., et al., Age and subtle cognitive impairment are associated with long-term olfactory dysfunction after COVID-19 infection. J Am Geriatr Soc, 2021. 69(10): p. 2778-2780. [CrossRef]
- Wang, J., et al., Prevalence of taste and smell dysfunction in mild and asymptomatic COVID-19 patients during Omicron prevalent period in Shanghai, China: a cross-sectional survey study. BMJ Open, 2023. 13(3): p. e067065. [CrossRef]
- Johnson, B.J., et al., Patient factors associated with COVID-19 loss of taste or smell patient factors in smell/taste loss COVID-19. Laryngoscope Investig Otolaryngol, 2022. 7(6): p. 1688-1694. [CrossRef]
- Shiue, I., Adult taste and smell disorders after heart, neurological, respiratory and liver problems: US NHANES, 2011-2012. Int J Cardiol, 2015. 179: p. 46-8. [CrossRef]
- Healey, Q., et al., Symptoms and signs of long COVID: A rapid review and meta-analysis. J Glob Health, 2022. 12: p. 05014. [CrossRef]
- Güney, B., et al., Changes in olfactory bulbus volume and olfactory sulcus depth in the chronic period after COVID-19 infection. Acta Oto-Laryngologica, 2021. 141(8): p. 786-790. [CrossRef]
- Tan, C.J.-W., et al., Neuroradiological Basis of COVID-19 Olfactory Dysfunction: A Systematic Review and Meta-Analysis. The Laryngoscope, 2022. 132(6): p. 1260-1274. [CrossRef]
- Hoang, M.P., et al., Self-reported olfactory and gustatory dysfunction and psychophysical testing in screening for COVID-19: A systematic review and meta-analysis. International Forum of Allergy & Rhinology, 2022. 12(5): p. 744-756. [CrossRef]
- Pires, Í.d.A.T., et al., Intensive Olfactory Training in Post-COVID-19 Patients: A Multicenter Randomized Clinical Trial. American Journal of Rhinology & Allergy, 2022. 36(6): p. 780-787. [CrossRef]
- de Melo, E.G.M., et al., Association between chemosensory dysfunctions and inflammatory biomarkers in patients with SARS-CoV-2 infection: a systematic review and meta-analysis. Inflammopharmacology, 2022. 30(6): p. 2079-2087. [CrossRef]
- Rashid, R.A., A. Zgair, and R.M. Al-Ani, Effect of nasal corticosteroid in the treatment of anosmia due to COVID-19: A randomised double-blind placebo-controlled study. American Journal of Otolaryngology, 2021. 42(5): p. 103033. [CrossRef]
- García-Meléndez, D.D., et al., Persistent olfactory dysfunction in mild COVID-19 patients: A descriptive study of the characteristics and association with other symptoms. Medicina Clínica, 2022. p. [CrossRef]
- Pendolino, A.L., et al., A multicenter real-life study to determine the efficacy of corticosteroids and olfactory training in improving persistent COVID-19-related olfactory dysfunction. Laryngoscope Investigative Otolaryngology, 2023. 8(1): p. 46-54. [CrossRef]
- Speth, M.M., et al., Olfactory Dysfunction and Sinonasal Symptomatology in COVID-19: Prevalence, Severity, Timing, and Associated Characteristics. Otolaryngology–Head and Neck Surgery, 2020. 163(1): p. 114-120. [CrossRef]
- Kim, J.-W., et al., Regional and Chronological Variation of Chemosensory Dysfunction in COVID-19: a Meta-Analysis. J Korean Med Sci, 2021. 36(4): p.
- Tong, J.Y., et al., The Prevalence of Olfactory and Gustatory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis. Otolaryngology–Head and Neck Surgery, 2020. 163(1): p. 3-11. [CrossRef]
- Hajikhani, B., et al., Olfactory and gustatory dysfunction in COVID-19 patients: A meta-analysis study. Physiol Rep, 2020. 8(18): p. e14578. [CrossRef]
- Hoffmann, M., et al., SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell, 2020. 181(2): p. 271-280.e8. [CrossRef]
- Lechien, J.R., et al., ACE2 & TMPRSS2 Expressions in Head & Neck Tissues: A Systematic Review. Head Neck Pathol, 2021. 15(1): p. 225-235. [CrossRef]
- Sungnak, W., et al., SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat Med, 2020. 26(5): p. 681-687. [CrossRef]
- Glass, W.G., et al., Mechanisms of host defense following severe acute respiratory syndrome-coronavirus (SARS-CoV) pulmonary infection of mice. J Immunol, 2004. 173(6): p. 4030-9. [CrossRef]
- Li, K., et al., Middle East Respiratory Syndrome Coronavirus Causes Multiple Organ Damage and Lethal Disease in Mice Transgenic for Human Dipeptidyl Peptidase 4. J Infect Dis, 2016. 213(5): p. 712-22. [CrossRef]
- Talbot, P.J., et al., Neurotropism of human coronavirus 229E. Adv Exp Med Biol, 1993. 342: p. 339-46. [CrossRef]
- Cecchini, M.P., et al., Persistent chemosensory dysfunction in a young patient with mild COVID-19 with partial recovery 15 months after the onset. Neurol Sci, 2022. 43(1): p. 99-104. [CrossRef]
- Li, Y.C., W.Z. Bai, and T. Hashikawa, The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol, 2020. 92(6): p. 552-555. [CrossRef]
- Lima, M., et al., Unraveling the Possible Routes of SARS-COV-2 Invasion into the Central Nervous System. Curr Treat Options Neurol, 2020. 22(11): p. 37. [CrossRef]
- Dubé, M., et al., Axonal Transport Enables Neuron-to-Neuron Propagation of Human Coronavirus OC43. J Virol, 2018. 92(17): p. [CrossRef]
- Cantuti-Castelvetri, L., et al., Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science, 2020. 370(6518): p. 856-860. [CrossRef]
- Bilinska, K., et al., Expression of the SARS-CoV-2 Entry Proteins, ACE2 and TMPRSS2, in Cells of the Olfactory Epithelium: Identification of Cell Types and Trends with Age. ACS Chem Neurosci, 2020. 11(11): p. 1555-1562. [CrossRef]
- Chen, M., et al., Elevated ACE-2 expression in the olfactory neuroepithelium: implications for anosmia and upper respiratory SARS-CoV-2 entry and replication. Eur Respir J, 2020. 56(3): p. [CrossRef]
- Zhou, Z., et al., Understanding the neurotropic characteristics of SARS-CoV-2: from neurological manifestations of COVID-19 to potential neurotropic mechanisms. J Neurol, 2020. 267(8): p. 2179-2184. [CrossRef]
- Wang, L.H. and S.M. Strittmatter, A family of rat CRMP genes is differentially expressed in the nervous system. J Neurosci, 1996. 16(19): p. 6197-207. [CrossRef]
- Reza, J.N., I. Gavazzi, and J. Cohen, Neuropilin-1 is expressed on adult mammalian dorsal root ganglion neurons and mediates semaphorin3a/collapsin-1-induced growth cone collapse by small diameter sensory afferents. Mol Cell Neurosci, 1999. 14(4-5): p. 317-26. [CrossRef]
- Kirschenbaum, D., et al., Inflammatory olfactory neuropathy in two patients with COVID-19. Lancet, 2020. 396(10245): p. 166. [CrossRef]
- Toor, S.M., et al., T-cell responses and therapies against SARS-CoV-2 infection. Immunology, 2021. 162(1): p. 30-43. [CrossRef]
- Cazzolla, A.P., et al., Taste and Smell Disorders in COVID-19 Patients: Role of Interleukin-6. ACS Chemical Neuroscience, 2020. 11(17): p. 2774-2781. [CrossRef]
- Mastrangelo, A., M. Bonato, and P. Cinque, Smell and taste disorders in COVID-19: From pathogenesis to clinical features and outcomes. Neuroscience Letters, 2021. 748: p. 135694. [CrossRef]
- Cooper, K.W., et al., COVID-19 and the Chemical Senses: Supporting Players Take Center Stage. Neuron, 2020. 107(2): p. 219-233. [CrossRef]
- Wei, G., et al., Olfactory Dysfunction in Patients With Coronavirus Disease 2019: A Review. Frontiers in Neurology, 2022. 12: p. [CrossRef]
- Xydakis, M.S., et al., Post-viral effects of COVID-19 in the olfactory system and their implications. The Lancet Neurology, 2021. 20(9): p. 753-761. [CrossRef]
- Khan, S. and J. Gomes, Neuropathogenesis of SARS-CoV-2 infection. Elife, 2020. 9: p. [CrossRef]
- Kishimoto-Urata, M., et al., Prolonged and extended impacts of SARS-CoV-2 on the olfactory neurocircuit. Sci Rep, 2022. 12(1): p. 5728. [CrossRef]
- Käufer, C., et al., Microgliosis and neuronal proteinopathy in brain persist beyond viral clearance in SARS-CoV-2 hamster model. eBioMedicine, 2022. 79: p. [CrossRef]
- Khan, M., et al., Visualizing in deceased COVID-19 patients how SARS-CoV-2 attacks the respiratory and olfactory mucosae but spares the olfactory bulb. Cell, 2021. 184(24): p. 5932-5949.e15. [CrossRef]
- Brann, D.H., et al., Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Science Advances, 2020. 6(31): p. eabc5801. [CrossRef]
- Chen, M., et al., Evolution of nasal and olfactory infection characteristics of SARS-CoV-2 variants. bioRxiv, 2022. p. 2022.04.12.487379. [CrossRef]
- Hou, Y.J., et al., SARS-CoV-2 Reverse Genetics Reveals a Variable Infection Gradient in the Respiratory Tract. Cell, 2020. 182(2): p. 429-446.e14. [CrossRef]
- Zou, L., et al., SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. New England Journal of Medicine, 2020. 382(12): p. 1177-1179. [CrossRef]
- Liao, B., et al., Long-term Consequences of COVID-19: Chemosensory Disorders. Curr Allergy Asthma Rep, 2023. 23(2): p. 111-119. [CrossRef]
- Kay, L.M., COVID-19 and olfactory dysfunction: a looming wave of dementia? Journal of Neurophysiology, 2022. 128(2): p. 436-444. [CrossRef]
- Glezer, I., et al., Viral infection and smell loss: The case of COVID-19. Journal of Neurochemistry, 2021. 157(4): p. 930-943. [CrossRef]
- Araújo, L., V. Arata, and R.G. Figueiredo, Olfactory Disorders in Post-Acute COVID-19 Syndrome. Sinusitis, 2021. 5(2): p. 116-122.
- de Melo, G.D., et al., COVID-19–related anosmia is associated with viral persistence and inflammation in human olfactory epithelium and brain infection in hamsters. Science Translational Medicine, 2021. 13(596): p. eabf8396. [CrossRef]
- Ylikoski, J., M. Markkanen, and A. Mäkitie, Pathophysiology of the COVID-19 – entry to the CNS through the nose. Acta Oto-Laryngologica, 2020. 140(10): p. 886-889. [CrossRef]
- Park, G.C., et al., ACE2 and TMPRSS2 immunolocalization and oral manifestations of COVID-19. Oral Diseases, 2022. 28(S2): p. 2456-2464. [CrossRef]
- Bilinska, K., C.S. von Bartheld, and R. Butowt, Expression of the ACE2 Virus Entry Protein in the Nervus Terminalis Reveals the Potential for an Alternative Route to Brain Infection in COVID-19. Frontiers in Cellular Neuroscience, 2021. 15: p. [CrossRef]
- Ramakrishnan, S., et al., Acquisition of spontaneous electrical activity during embryonic development of gonadotropin-releasing hormone-3 neurons located in the terminal nerve of transgenic zebrafish (Danio rerio). Gen Comp Endocrinol, 2010. 168(3): p. 401-7. [CrossRef]
- Meinhardt, J., et al., Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nature Neuroscience, 2021. 24(2): p. 168-175. [CrossRef]
- Brann, D.H., et al., Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Sci Adv, 2020. 6(31): p. [CrossRef]
- Ye, Q., et al., SARS-CoV-2 infection in the mouse olfactory system. Cell Discov, 2021. 7(1): p. 49. [CrossRef]
- Frosolini, A., et al., Magnetic Resonance Imaging Confirmed Olfactory Bulb Reduction in Long COVID-19: Literature Review and Case Series. Brain Sciences, 2022. 12(4): p. 430.
- Güney, B., et al., Changes in olfactory bulbus volume and olfactory sulcus depth in the chronic period after COVID-19 infection. Acta Otolaryngol, 2021. 141(8): p. 786-790. [CrossRef]
- Yildirim, D., et al., A Comparative Olfactory MRI, DTI and fMRI Study of COVID-19 Related Anosmia and Post Viral Olfactory Dysfunction. Acad Radiol, 2022. 29(1): p. 31-41. [CrossRef]
- Sinnarajah, S., et al., RGS2 regulates signal transduction in olfactory neurons by attenuating activation of adenylyl cyclase III. Nature, 2001. 409(6823): p. 1051-1055. [CrossRef]
- Zazhytska, M., et al., Non-cell-autonomous disruption of nuclear architecture as a potential cause of COVID-19-induced anosmia. Cell, 2022. 185(6): p. 1052-1064.e12. [CrossRef]
- Avnat, E., et al., Elevated Expression of RGS2 May Underlie Reduced Olfaction in COVID-19 Patients. Journal of Personalized Medicine, 2022. 12(9): p. 1396.
- Jones, D.T. and R.R. Reed, G<sub>olf</sub>: an Olfactory Neuron Specific-G Protein Involved in Odorant Signal Transduction. Science, 1989. 244(4906): p. 790-795. [CrossRef]
- Ebrahimi, F.A.W. and A. Chess, Olfactory G proteins: Simple and complex signal transduction. Current Biology, 1998. 8(12): p. R431-R433. [CrossRef]
- Tabatabaeizadeh, S.A., Zinc supplementation and COVID-19 mortality: a meta-analysis. Eur J Med Res, 2022. 27(1): p. 70. [CrossRef]
- Debbaneh, P., et al., Drug-induced olfactory and gustatory dysfunction: Analysis of FDA adverse events reporting system. Auris Nasus Larynx, 2023. p. [CrossRef]
- Hummel, T., et al., Position paper on olfactory dysfunction. Rhinol Suppl, 2017. 54(26): p. 1-30. [CrossRef]
- Wang, L., L. Chen, and T. Jacob, Evidence for peripheral plasticity in human odour response. J Physiol, 2004. 554(Pt 1): p. 236-44. [CrossRef]
- Whitcroft, K.L. and T. Hummel, Clinical Diagnosis and Current Management Strategies for Olfactory Dysfunction: A Review. JAMA Otolaryngol Head Neck Surg, 2019. 145(9): p. 846-853. [CrossRef]
- Konstantinidis, I., et al., Use of olfactory training in post-traumatic and postinfectious olfactory dysfunction. Laryngoscope, 2013. 123(12): p. E85-90. [CrossRef]
- Everts, P., et al. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. International Journal of Molecular Sciences, 2020. 21,. [CrossRef]
- Farrag, T.Y., et al., Effect of Platelet Rich Plasma and Fibrin Sealant on Facial Nerve Regeneration in a Rat Model. The Laryngoscope, 2007. 117(1): p. 157-165. [CrossRef]
- Yan, C.H., et al., Use of platelet-rich plasma for COVID-19–related olfactory loss: a randomized controlled trial. International Forum of Allergy & Rhinology. n/a(n/a): p. [CrossRef]
- Seo, B.S., et al., Treatment of postviral olfactory loss with glucocorticoids, Ginkgo biloba, and mometasone nasal spray. Arch Otolaryngol Head Neck Surg, 2009. 135(10): p. 1000-4. [CrossRef]
- Schriever, V.A., et al., Treatment of smell loss with systemic methylprednisolone. Rhinology, 2012. 50(3): p. 284-9. [CrossRef]
- Kim, D.H., et al., Prognosis of Olfactory Dysfunction according to Etiology and Timing of Treatment. Otolaryngol Head Neck Surg, 2017. 156(2): p. 371-377. [CrossRef]
- Aiyegbusi, O.L., et al., Symptoms, complications and management of long COVID: a review. J R Soc Med, 2021. 114(9): p. 428-442. [CrossRef]
- Di Stadio, A., et al., Ultramicronized Palmitoylethanolamide and Luteolin Supplement Combined with Olfactory Training to Treat Post-COVID-19 Olfactory Impairment: A Multi-Center Double-Blinded Randomized Placebo- Controlled Clinical Trial. Curr Neuropharmacol, 2022. 20(10): p. 2001-2012. [CrossRef]
- D'Ascanio, L., et al., Randomized clinical trial "olfactory dysfunction after COVID-19: olfactory rehabilitation therapy vs. intervention treatment with Palmitoylethanolamide and Luteolin": preliminary results. Eur Rev Med Pharmacol Sci, 2021. 25(11): p. 4156-4162. [CrossRef]
- De Luca, P., et al., Effect of Ultra-Micronized Palmitoylethanolamide and Luteolin on Olfaction and Memory in Patients with Long COVID: Results of a Longitudinal Study. Cells, 2022. 11(16): p. [CrossRef]
- Kern, R.C., et al., Treatment of olfactory dysfunction, II: studies with minocycline. Laryngoscope, 2004. 114(12): p. 2200-4. [CrossRef]
- Henkin, R.I., I. Velicu, and L. Schmidt, An open-label controlled trial of theophylline for treatment of patients with hyposmia. Am J Med Sci, 2009. 337(6): p. 396-406. [CrossRef]
- Rezaeian, A., Effect of Intranasal Insulin on Olfactory Recovery in Patients with Hyposmia: A Randomized Clinical Trial. Otolaryngol Head Neck Surg, 2018. 158(6): p. 1134-1139. [CrossRef]
- Quint, C., et al., The quinoxaline derivative caroverine in the treatment of sensorineural smell disorders: a proof-of-concept study. Acta Otolaryngol, 2002. 122(8): p. 877-81.
- Whitcroft, K.L., et al., Intranasal sodium citrate solution improves olfaction in post-viral hyposmia. Rhinology, 2016. 54(4): p. 368-374. [CrossRef]
- Hummel, T., S. Heilmann, and K.B. Hüttenbriuk, Lipoic acid in the treatment of smell dysfunction following viral infection of the upper respiratory tract. Laryngoscope, 2002. 112(11): p. 2076-80. [CrossRef]
- Ogawa, T., et al., Recovery over time and prognostic factors in treated patients with post-infectious olfactory dysfunction: a retrospective study. Annals of Otology, Rhinology & Laryngology, 2020. 129(10): p. 977-982.
- Reden, J., et al., Olfactory function in patients with postinfectious and posttraumatic smell disorders before and after treatment with vitamin A: a double-blind, placebo-controlled, randomized clinical trial. The Laryngoscope, 2012. 122(9): p. 1906-1909.
- Bhutani, D.L., et al., Resolution of COVID-19 induced anosmia following treatment with ST266. Otolaryngol Case Rep, 2022. 25: p. 100475. [CrossRef]
- Tsetsos, N., K. Markou, and I. Konstantinidis, Effect of monoclonal antibodies on olfactory dysfunction caused by chronic rhinosinusitis with nasal polyps: a systematic review and meta-analysis. Int Forum Allergy Rhinol, 2020. 10(7): p. 893-900. [CrossRef]
- Wood, D.A., A. Aleem, and D. Davis, Providing Access To Monoclonal Antibody Treatment Of Coronavirus (COVID-19) Patients In Rural And Underserved Areas, in StatPearls. 2023, StatPearls Publishing.
- Khan, R.S., et al., Intranasal delivery of a novel amnion cell secretome prevents neuronal damage and preserves function in a mouse multiple sclerosis model. Scientific Reports, 2017. 7(1): p. 1-12.
- Grinblat, G.A., et al., RGC neuroprotection following optic nerve trauma mediated by intranasal delivery of amnion cell secretome. Investigative Ophthalmology & Visual Science, 2018. 59(6): p. 2470-2477.
- Tsetsos, N., K. Markou, and I. Konstantinidis, Effect of monoclonal antibodies on olfactory dysfunction caused by chronic rhinosinusitis with nasal polyps: a systematic review and meta-analysis. International Forum of Allergy & Rhinology, 2020. 10(7): p. 893-900. [CrossRef]
- Karamali, K., M. Elliott, and C. Hopkins, COVID-19 related olfactory dysfunction. Curr Opin Otolaryngol Head Neck Surg, 2022. 30(1): p. 19-25. [CrossRef]
- Yong, S.J., Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments. Infect Dis (Lond), 2021. 53(10): p. 737-754. [CrossRef]
- Hopkins, C., L.A. Vaira, and G. De Riu, Self-reported olfactory loss in COVID-19: is it really a favorable prognostic factor? Int Forum Allergy Rhinol, 2020. 10(7): p. 926. [CrossRef]
- Chee, J., et al., Pathophysiology of SARS-CoV-2 Infection of Nasal Respiratory and Olfactory Epithelia and Its Clinical Impact. Current Allergy and Asthma Reports, 2023. 23(2): p. 121-131. [CrossRef]
- Neuland, C., et al., Health-related and specific olfaction-related quality of life in patients with chronic functional anosmia or severe hyposmia. Laryngoscope, 2011. 121(4): p. 867-72. [CrossRef]
- Kohli, P., et al., The Association Between Olfaction and Depression: A Systematic Review. Chem Senses, 2016. 41(6): p. 479-86. [CrossRef]
- Mattes, R.D., et al., Dietary evaluation of patients with smell and/or taste disorders. Am J Clin Nutr, 1990. 51(2): p. 233-40. [CrossRef]
- Aschenbrenner, K., et al., The influence of olfactory loss on dietary behaviors. Laryngoscope, 2008. 118(1): p. 135-44. [CrossRef]
- Attems, J., L. Walker, and K.A. Jellinger, Olfactory bulb involvement in neurodegenerative diseases. Acta Neuropathologica, 2014. 127(4): p. 459-475. [CrossRef]
- Wilson, R.S., et al., Lewy Bodies and Olfactory Dysfunction in Old Age. Chemical Senses, 2011. 36(4): p. 367-373. [CrossRef]
- Yoo, H.S., et al., Olfactory dysfunction in Alzheimer's disease– and Lewy body–related cognitive impairment. Alzheimer's & Dementia, 2018. 14(10): p. 1243-1252. [CrossRef]
- Kay, L.M., COVID-19 and olfactory dysfunction: a looming wave of dementia? J Neurophysiol, 2022. 128(2): p. 436-444. [CrossRef]
- Takeda, A., et al., Olfactory dysfunction and dementia in Parkinson's disease. J Parkinsons Dis, 2014. 4(2): p. 181-7. [CrossRef]
Figure 1.
Prevalence of OD by different evaluation methods in SARS-CoV-2 variants. No data regarding VOC Gamma in psychophysical evaluation was reported. OD, Olfactory dysfunction; VOC, Variant of concern; NR, Not reported.
Figure 1.
Prevalence of OD by different evaluation methods in SARS-CoV-2 variants. No data regarding VOC Gamma in psychophysical evaluation was reported. OD, Olfactory dysfunction; VOC, Variant of concern; NR, Not reported.
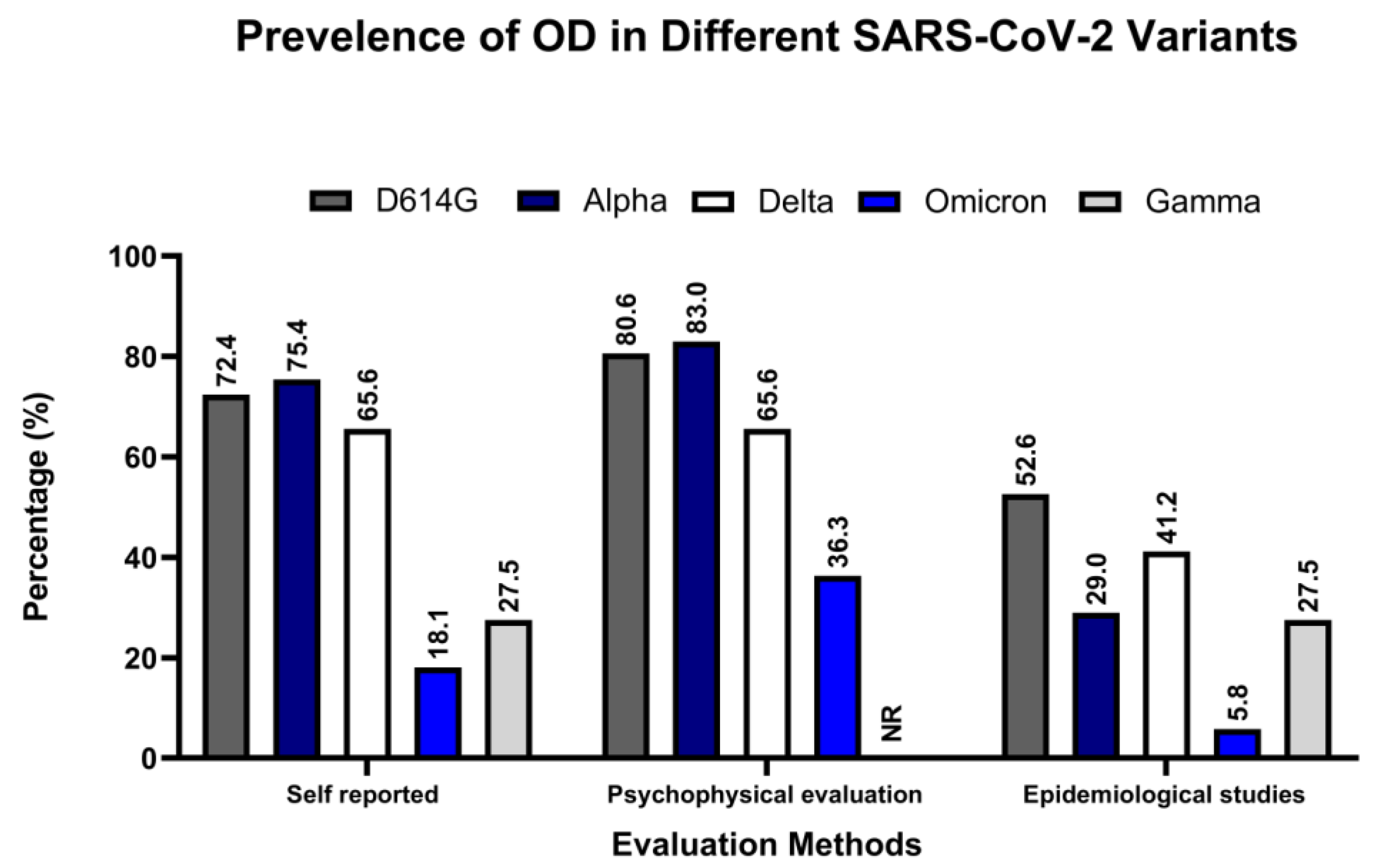
Figure 2.
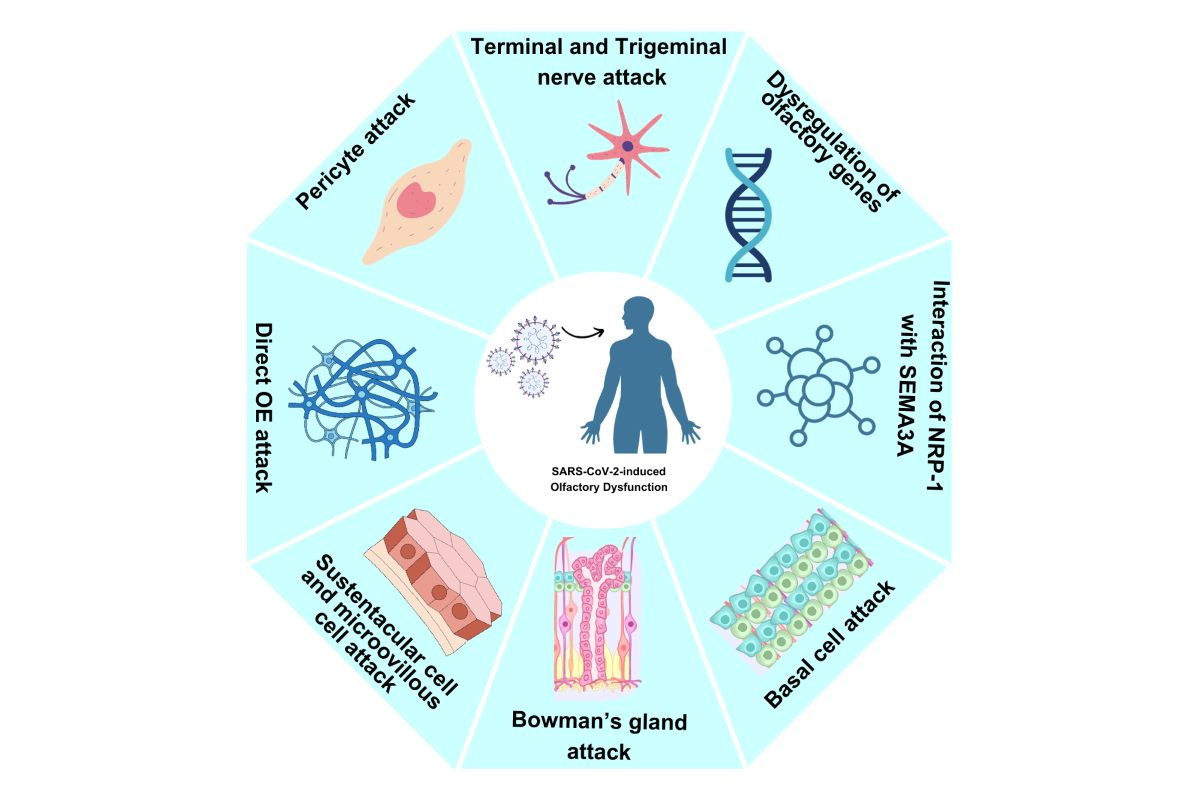
Mechanism of action(s) of OD. (a) SARS-CoV-2 binds to the ACE2 and TMPRSS2 receptor and enter host. (b) It attacks pericytes causing blood-brain barrier disruption due to IL-1, IL-6, IL-12, INF-y, and TNFɑ release; (c) Trigeminal nerve and terminal nerve attack by attaching to ACE2 and TMPRSS2 receptors present there; (d) or direct attack on OE; (e) Damage to OB and sustentacular cell; (f) Bowman's glands, basal cells, stem cells infections; (g) Interferes the interaction of NRP-1 with SEMA3A; (h) and lastly, dysregulates olfactory receptor gene. OD: Olfactory dysfunction; IL-1:Interleukin-; IL-6: Interleukin-6; IL-12: Interleukin-12; INF-y: Interferon-y; TNFɑ: Tumor necrosis factor-alpha; mOSN: Mature Olfactory sensory neurons; iOSN: Immature olfactory sensory neurons; ACIII: Adenylate cyclase III; OE: Olfactory epithelium; OB: Olfactory bulb; SARS-CoV-2: Severe acute respiratory syndrome coronavirus-2; RGP-2: Regulator G protein signaling 2; NRP-1: Neuropilin-1; SEMA3A: Semaphorine-3A; OEC: Olfactory unsheating cell; GBC: Globose basal cell; TMPRSS2: Transmembrane serine protease 2; ACE2: Angiotensin-converting enzyme 2; ATP: Guanosine triphosphate; GDP: Guanosine diphosphate; cAMP: Cyclic adenosine monophosphate; OSN: Olfactory sensory neurons.
Figure 2.
Mechanism of action(s) of OD. (a) SARS-CoV-2 binds to the ACE2 and TMPRSS2 receptor and enter host. (b) It attacks pericytes causing blood-brain barrier disruption due to IL-1, IL-6, IL-12, INF-y, and TNFɑ release; (c) Trigeminal nerve and terminal nerve attack by attaching to ACE2 and TMPRSS2 receptors present there; (d) or direct attack on OE; (e) Damage to OB and sustentacular cell; (f) Bowman's glands, basal cells, stem cells infections; (g) Interferes the interaction of NRP-1 with SEMA3A; (h) and lastly, dysregulates olfactory receptor gene. OD: Olfactory dysfunction; IL-1:Interleukin-; IL-6: Interleukin-6; IL-12: Interleukin-12; INF-y: Interferon-y; TNFɑ: Tumor necrosis factor-alpha; mOSN: Mature Olfactory sensory neurons; iOSN: Immature olfactory sensory neurons; ACIII: Adenylate cyclase III; OE: Olfactory epithelium; OB: Olfactory bulb; SARS-CoV-2: Severe acute respiratory syndrome coronavirus-2; RGP-2: Regulator G protein signaling 2; NRP-1: Neuropilin-1; SEMA3A: Semaphorine-3A; OEC: Olfactory unsheating cell; GBC: Globose basal cell; TMPRSS2: Transmembrane serine protease 2; ACE2: Angiotensin-converting enzyme 2; ATP: Guanosine triphosphate; GDP: Guanosine diphosphate; cAMP: Cyclic adenosine monophosphate; OSN: Olfactory sensory neurons.
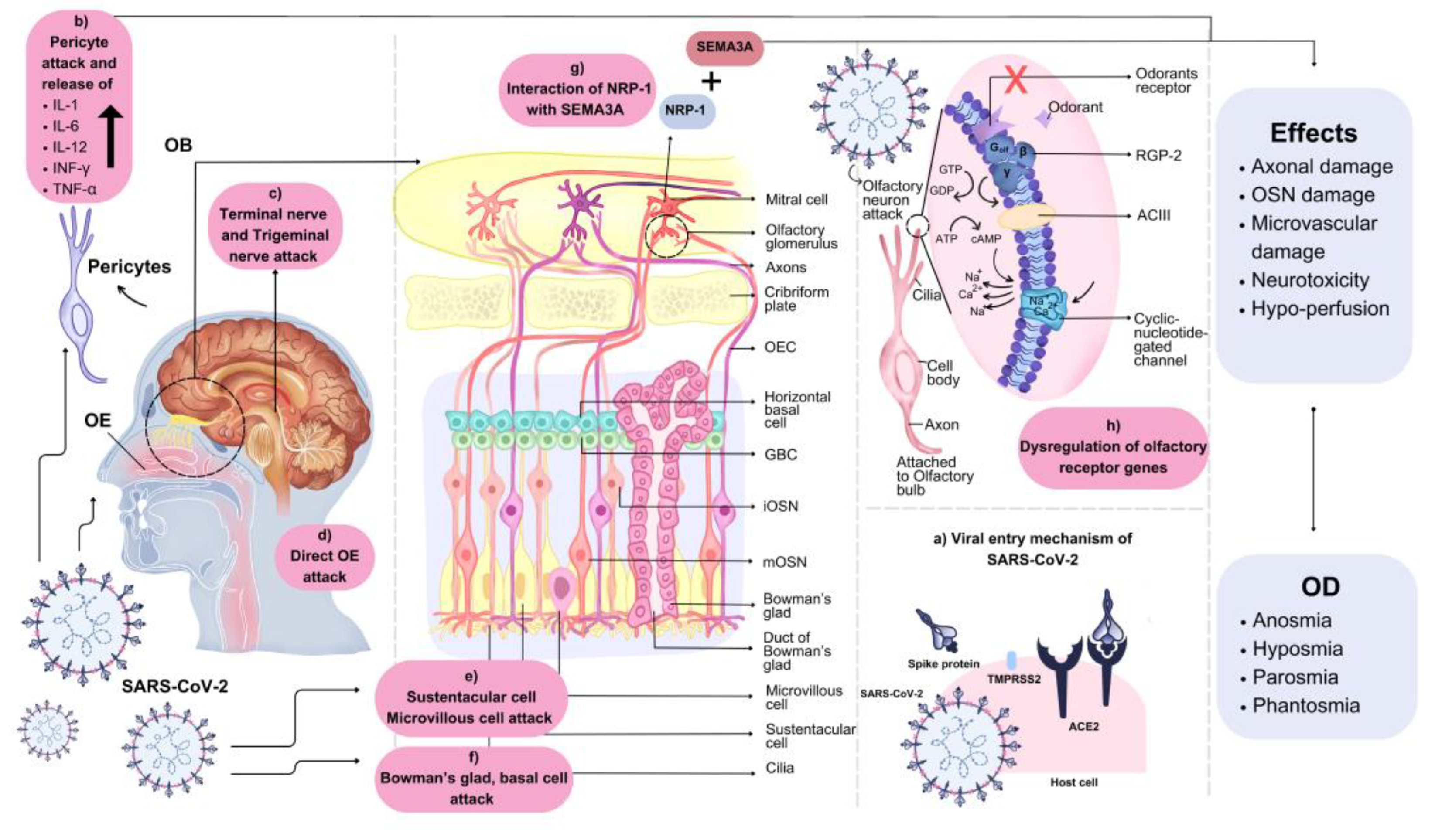

Table 1.
Summary of different regions, patients, age, prevalence, recovery duration and other symptoms of OD.
Table 1.
Summary of different regions, patients, age, prevalence, recovery duration and other symptoms of OD.
| Ref. | Study design andregion | Number of Participants | Mean participantage (Year) | OD prevalence | Recovery duration | Common Symptoms |
|---|---|---|---|---|---|---|
| [49] | Systematic Review, Meta-Analysis; Europe, America, Asia | 3699 | 30.0–55.8 | 3–11% | 30–180 days | Cough, fatigue, rhinorrhea, sore throat, muscle, and joint pains. |
| [75] | Meta-analysis; Turkey | 41 | 40.27 ± 14.5 | 45% | 10–12 months | NR |
| [74] | Systematic reviews and meta-analysis; Europe, Asia, North America, and Australia. | 10643 | 35–64 | 17% | >12 weeks | Fatigue, dyspnoea, myalgia, cough. |
| [76] | Systematic Review and Meta-Analysis. | 16-91 | 34.3– 45.4 | 63% | 2 months | Nasal obstruction, mucosal congestion. |
| [77] | Cohort, Case-control; North America, Europe, South America, Australia, and Africa, Asia. | 42902 | 28–67 | 43.9% | NR | Headache and rhinorrhea. |
| [78] | A Multicenter Randomized Clinical Trial; Curitiba, Londrina, and Brazil. | 80 | 36.7 ± 10.3 | 82.5% | 1–2 weeks | Headache and nausea. |
| [79] | Systematic reviews and meta-analysis; Turkey, The United Kingdom, Morocco, China, Spain, Italy, and the United States | 3218 | NR | 26.9% | NR | Fever, dry cough, headache, dyspnoea, myalgia or arthralgia, fatigue, diarrhea, and vomiting. |
| [80] | Randomized double-blind placebo-controlled study; Iraq. | 276 | 29 | NR | 1–4 weeks | Nasal obstruction, rhinorrhea, sneezing, and facial pain. |
| [81] | Observational, descriptive, and single-center study. | 86 | 37.2 | 70.9% | 2 weeks | Brain fog. |
| [82] | A multicenter real-life cohort study; London, United Kingdom, Padua, Italy. | 44 | 40.5 | 81.8% | 6–12 months | Nasal Obstruction and rhinorrhoea. |
| [83] | Prospective, cross-sectional; Aarau. | 103 | 46.8 | 61.2% | NR | Nasal obstruction, cough, mucus production, rhinorrhea. |
| [25] | A systematic review and meta-analysis. | 7,178 | NR | 98.3% | >2 weeks | Nasal obstruction, postnasal drip, or runny nose. |
| [84] | Meta-Analysis; Asia, Europe, Middle East East, Latin America, North America and Africa. | 13,527 | 44– 52.7 | 51.4% | NR | NR |
| [85] | Systematic Review and Meta-analysis; North America, Europe, and Asia. |
1627 | 36.9– 61.6 | 52.73% | NR | Nasal congestion, Peripheral nervous system complications, taste impairment. |
| [86] | Meta-analysis; France, Italy, China, Iran, Singapore, USA, Germany. |
1,354 | 34 –65 | 61.3% | NR | Fever, myalgia, chills, dyspnea, sore throat, cough. |
Ref., References; NR, Not reported; OD, Olfactory dysfunction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



