
Submitted:
03 October 2023
Posted:
04 October 2023
You are already at the latest version
Abstract
The metastatic disease is a complex and sequential process that involves the migration of tumor cells from the primary site to distant areas. This metastatic pathway is not always predictable. Therefore, this paper presents three rare cases of unusual metastases, due to their primary site: two metastases of a clear cell renal cell carcinoma, one gingival and one nasal, as well as a mandibular metastasis of a hepatocellular carcinoma. In all cases, an incisional biopsy was performed in order to sign out the diagnosis. After microscopical examination of morphological Hematoxylin and Eosin stained slides, for all cases, immunohistochemical reactions were performed to support the primary tumor site. Two cases had a previous histopathological diagnosis of a primary tumor, while for the third case, the metastatic lesion represented the first manifestation of the neoplastic disease, with an unfavorable prognosis.
Keywords:
Head and neck
; unusual metastases
; immunohistochemistry
; renal clear cell carcinoma
; hepatocellular carcinoma
1. Introduction
Clear cell renal cell carcinoma is the most common subtype of the renal carcinoma and usually gives hematogenous metastases in the brain, lung, liver and bone, via the inferior vena cava. Renal cell carcinoma metastasis in the head and neck organs are uncommon, accounting for only 6% of metastases, most commonly involving the thyroid, parotid gland and sinuses [1,2]. If the disease is advanced, the risk of metastasis in the head and neck region is raised, being about 15%, while in localized disease, the risk is only around 1% [3]. The data show that the renal cell carcinoma is the third most common infra clavicular malignancy to metastasize to the head and neck region. The most cases described in the English literature presented a history of primary renal tumor, and patients often had advanced metastatic disease [4,5].
Hepatocellular carcinoma is the most common primary hepatic tumor and the sixth most common malignancy in the world. It is considered the second most common cause of death from cancer worldwide. The improvement in intrahepatic tumor control and prolonged survival has led to an increased incidence of extrahepatic metastasis. The most frequent sites of metastasis are bones, followed by the lungs and lymph nodes. Oral bone metastasis is a soft-tissue mass, which may occur with pain, swelling and local mass effects of osteolysis which hinder the patient’s quality of life. Radiotherapy can be used as a palliative treatment and its efficacy in this regard has been reported in previous studies. The most common sites of a bone metastasis from hepatocellular carcinoma are the spine, pelvis, ribs and long bone. About 1% of the hepatocellular carcinoma’s metastases show oral involvement, the most frequent affected site being the posterior angle of the mandible. Less common, metastatic sites such as the mandible was first reported by Dick et al. in 1957. Since then, mandibular metastases of hepatocellular carcinomas have been described in several case reports and small case series. Consequently, there have been few reports on the role of radiotherapy in these rare cases, which is the main palliative treatment for a bone metastasis from hepatocellular carcinoma [6,7,8].
2. Aim
The aim of this study was to assess unconventional head and neck metastases of clear cell renal cell carcinoma and hepatocellular carcinoma and to establish the primary site of the tumor based on their immunohistochemical profile.
3. Patients, Materials and Methods
The current paper presents one gingival and one sinonasal metastasis of clear cell renal cell carcinoma, as well as a mandibular metastasis of hepatocellular carcinoma. Patients were diagnosed in the Emergency City Hospital of Timisoara, affiliated with the "Victor Babes" University of Medicine and Pharmacy, Timisoara, Romania. The eligible patients for this paper were selected from the database of the hospital and the inclusion criteria were: patients older than 18, available pathological report of the lesions, highlighted using morphological histological stains, supported by immunohistochemically reactions. The demographic data of the patients, their biological investigations and data related to their medical background were taken from the patient observation sheet.
The patients were biopsied between January 2021 and December 2022. The harvested specimens were fixed in 4% v/v buffered formaldehyde, sent to Service of Pathology and processed with usual histological technique. Four-micrometer-thick sections were cut using a semi-automated Leica RM2235 rotary microtome, displayed on SuperFrost™ microscope slides and stained with Hematoxylin and Eosin (HE). The histopathological diagnosis was completed using immunohistochemical (IHC) reactions. All the data regarding the antibodies used for IHC reactions are centralized in Table 1.
All the patients signed the informed consent to approve the participation in this study and signed the Patient Informed Consent. The Consent of Ethics Committee from Municipal Clinical Emergency Hospital, Timişoara. Both the Ethics Committees of both "Victor Babes" University of Medicine and Pharmacy and of Municipal Clinical Emergency Hospital, Timisoara, approved the study.
4. Results
Case 1
A 67-year-old male patient presented to the Oro-Maxillo-Facial Surgery Clinic with a soft tissue mass located on the right mandibular alveolar ridge. The lesion had an irregular shape, and 1.5/2/3 cm in size. At palpation, mobility to the underlying mandibular bone structure was noted, with a discrete hemorrhagic phenomenon in the moment of examination. The patient denied local sensitivity, spontaneous pain or any disturbances. The onset of symptoms was approximately three years ago. The patient had no history of neoplastic disease.
The native computed tomography scan revealed the presence of a mandibular tissue mass, without any osteolysis and upper right cervical adenopathy of 1.7 cm, respectively, upper left cervical adenopathy of 1 cm in diameter. Because of the high blood level of the creatinine value, intravenous contrast media could not be used.
Under local anesthesia, an incisional biopsy of the mandibular tissue mass was performed, and the harvested fragments were examined microscopically.
The histopathological examination in Hematoxylin-Eosin staining revealed a malignant tumor proliferation consisting of large polyhedral cells, arranged in nests and lobules, with important cytonuclear atypia. Tumor cells had large, pale cytoplasm and enlarged, oval or irregularly contoured, pleomorphic and vesicular nuclei, with eosinophilic macronucleoli. The tumor stroma showed fine connective septa with a delicate vascular network and extravasated erythrocytes (Figure 1 and Figure 2). A presumptive diagnosis of malignant tumor was made.
The immunohistochemical reactions were asked for in order to confirm the phenotype of the tumor cells and to differentiate between carcinoma, achromic melanoma with epithelioid cells, leiomyosarcoma or rhabdomyosarcoma, angiosarcoma and even a Kaposi’s sarcoma. and the site of primary malignancy. The tumor cells were immunohistochemically positive for CK AE1/AE3 and vimentin (Figure 3) and negative immunohistochemical for S100 protein, HMB45, Melan-A, SMA, desmin, CD31, CD34 and HHV8, confirming the epithelial origin of the tumor.
The next step was to establish the cytokeratin profile of the tumor using the cytokeratins 7, 20, 8/18 and 5 (Figure 4 and Figure 5). Because of the concomitant positivity of tumor cells for pan cytokeratin AE1/AE3 and vimentin, the antibodies panel was completed with EMA (Figure 6), RCC and CD10 (Figure 7). The tumor cells phenotype was CK AE1/AE3+, CK8/18+, vimentin+, RCC+, CD10+, CK7-, CK20-, CK5-, EMA-.
Based on the immunohistochemical profile, the diagnosis of mandibular metastasis of eosinophilic variant of clear cell renal cell carcinoma was established.
Case 2
A 79-year-old female patient, with a history of clear cell renal cell carcinoma, diagnosed and surgically removed with free margins approximately 20 years ago, presented herself to the Otorhinolaryngology Department with a polypoid tissue mass at the level of the nasal fossa. The lesion was 1/0.9/0.7 cm in size. The lesion was painless, but slightly hemorrhagic at the exploratory examination. The patient observed the occurrence of the lesion six months prior to the presentation, with slow growing character.
Under local anesthesia, an excisional biopsy of the tissue mass was performed and the harvested fragments were sent to the Service of Pathology, in buffered formaldehyde.
The histopathological examination of Hematoxylin-Eosin stained slides revealed a malignant tumor proliferation consisting of large polyhedral cells with compact and alveolar cellular arrangements, and moderate clear cytoplasm, rounded nucleus and fine granular chromatin pattern with small inconspicuous nucleoli (Figure 8). The malignant cells delineated variable sized cyst filled with eosinophilic acellular material. The tumor stroma showed delicate fibrous septa, rich, branched vascular network and areas of fibrinoid necrosis (Figure 9). On HE stained slides, the presumptive diagnosis of clear cell carcinoma was raised. Based on personal history of the patient, the suppositional diagnosis of nasal septum metastasis from clear cell renal cell carcinoma was made.
Immunohistochemical reactions were performed in order to phenotype the tumor cells and to sustain the renal origin. The tumor cells showed positivity for CK8/18 and negativity for CK7 (Figure 10), CK20 and CK5 (Figure 11). The positive reactions for EMA, CD10 (Figure 12), vimentin and RCC (Figure 13) sustained the renal origin. Based on the immunohistochemical profile and the history of clear cell renal carcinoma, the diagnosis of nasal metastasis of a clear cell renal cell carcinoma was signed out.
Case 3
A 63-year-old male patient, with several comorbidities (cerebrovascular accident, high blood pressure) presented in the Oro-Maxillo-Facial Surgery Clinic accusing the presence of an abnormal masse, with spontaneous pain response and on palpation in the right masseter region, of about 3-4 cm, imprecisely delimited, apparently fixed to the underlying mandibular bone plane, of relatively low consistency. Anamnestic, the patient established the appearance of the lesion 2 months before the current presentation, with a continuous and rapid growth. In the past, the patient underwent surgical removal (in 2018) and radio-chemotherapy oncological treatment (in 2019) for a liver carcinoma.
The computed tomography scan with contrast media revealed the presence of a tissue mass in the masticatory space on the right side. The dimensions of the lesion were 5.5/3.6 cm in axial plane. The lesion was moderately inhomogeneous (Figure 14), because of the necrotic areas (Figure 15), most probably with mandibular starting point, that infiltrates both the masseter and adjacent pterygoid muscle, that lyses the mandibular condyle (Figure 16) and the proximal segment of the vertical branch of the right mandible, avoiding the ipsilateral parapharyngeal space. The formation did not show a definite delimitation from the right parotid gland, instead it showed the lack of visualization of the jugular vein on the right side and no significant cervical lymphadenopathy.
In March 2021, an incisional biopsy was performed. Several tumor samples were taken by extraoral approach. The collected tissue was sent to the Service of Pathology of Timisoara’s Emergency City Hospital, for the histopathological examination.
Microscopic examination revealed a cellular proliferation with trabecular pattern, composed of polygonal cells, with moderate cytonuclear pleomorphism and abundant granular eosinophilic cytoplasm. Some tumor cells were binucleated, with large, rounded nuclei, irregularly dispersed chromatin with inconspicuous nucleoli. Tumor cells bordered optically empty "sinusoidal-like" spaces. The tumor was circumscribed by a pseudocapsule of fibrous connective tissue (Figure 17). Based on the HE microscopic aspects of the tumor and the history of hepatocellular carcinoma, mandibular metastasis from the liver tumor was suspected.
Additional immunohistochemical reactions were used in order to sustain the presumptive diagnosis of hepatocellular carcinoma. The cytokeratins profile showed CK 8/18 positivity and CK7 (Figure 18), CK20 and CK5 negativity (Figure 19). The hepatic origin was sustained by immunohistochemical positivity for HepPar-1, AFP (Figure 20) and CD 10 (Figure 21a) and negativity for monoclonal CEA (Figure 21b).
The morphological aspects correlated with the immunohistochemical profile, associated with the patient's history, established the final diagnosis of mandibular bone metastasis with primary hepatic site.
5. Discussion
Metastases of Clear Cell Renal Carcinoma
Renal cell carcinoma is the sixth most common cancer in men and the 10th most common in women, with a higher incidence and a wide variety of environmental and genetic risk factors associated with its development [1,9]. Common symptoms include palpable abdominal mass and hematuria, but most of the patients are asymptomatic until there is disseminated metastatic disease. Renal carcinoma is an aggressive malignancy, about 40% of patients having metastatic disease at the time of diagnosis [1]. Clear cell renal cell carcinoma is the most common microscopic subtype of renal cell carcinoma characterized by malignant large epithelial cells with abundant clear cytoplasm. It has higher preference for vascular invasion than for lymphatic invasion which leads to a higher incidence of renal vein involvement. This is associated with increased likelihood for distant metastasis rather than locoregional lymphatic spread which is the common pattern of spread for other subtypes of renal cell carcinoma [4]. Renal metastases in the head and neck areas are uncommon, accounting 6% of metastases, most commonly involving the thyroid, parotid gland and sinuses [1,2].
The presence of a sinonasal or gingival proliferation with clear cells is a diagnostic challenge for the pathologist, especially in the absence of a history of clear cell carcinoma, differential diagnosis including: squamous cell carcinoma with clear cell change, mucoepidermoid carcinoma, salivary clear cell carcinoma, epithelial-myoepithelial carcinoma, achromic melanoma, alveolar rhabdomyosarcoma and metastatic clear cell variant of follicular thyroid carcinoma [10,11,12,13].
Sinonasal renal cell-like adenocarcinoma occurs from the small seromucous glands and has similar cytologic characteristics to clear cell renal carcinoma. In the case of clear cell tumor proliferation, a previous nephrectomy or computed tomography to assess the kidney is necessary, but the diagnosis is always supported by immunohistochemistry [14]. Sinonasal renal cell-like adenocarcinoma was described for first time by Zur et al. in 2002 with the terminology of "renal cell-like tumor" based on similar aspects to renal clear cell carcinoma. The World Health Organization classification of Head and Neck Tumors 4th edition included this rare tumor as a morphologically unique entity of low-grade sinonasal non-intestinal-type adenocarcinomas [15,16].
Microscopically, renal clear cell carcinoma metastases present medium-sized cells, with compact and alveolar cellular arrangements, as well as moderate clear cytoplasm, rounded nucleus and fine granular chromatin pattern with small inconspicuous nucleoli. The tumor stroma shows delicate fibrous septa and rich, branched vascular network. While sinonasal renal cell-like adenocarcinoma is composed of mixtures of follicular to glandular structures with intervening fibrous septa without abundant vascular network. The neoplastic cells are uniform, cuboidal to polyhedral, with abundant clear to eosinophilic cytoplasm. There are slightly irregular to shrunken nuclei with coarse chromatin. Sinonasal renal cell-like adenocarcinoma is positive for CK7 and negative for vimentin, with CD10 of variable expression, while in the selected case the tumors cells are CD10, CK8/18 and CK AE1/AE3 intense and diffuse positive, with negative reaction for CK7 and CK5. EMA can also be expressed in both pathologies. Therefore, the morphological and immunohistochemical aspects should be correlated with the clinical, anamnestic and radiologic data to define the final diagnosis [17,18].
Squamous cell carcinoma with clear cell change, microscopically consists of islands and lobules of polyhedric cells with intense eosinophilic cytoplasm and nuclei with condensed chromatin on the nuclear membrane, giving vesicular appearance and multiple nucleoli, marked cytonuclear pleomorphism, mitoses, unicellular keratinization or parakeratotic pearls. The cells present intense positive immunohistochemical reaction for CK5.
Mucoepidermoid carcinoma is an admixture of epidermoid, squamous cell some with mucinous differentiation and goblet cells. The intracytoplasmic mucin is present in both, mucoepidermoid carcinoma and metastasis of clear cell renal cell carcinoma, but goblet curls and macro-cysts filled with extravasated mucin are not characteristic for clear cell renal cell carcinoma.
Salivary clear cell carcinoma, most frequently occurs in intraoral salivary gland sites and is mainly composed of polygonal epithelioid tumor cells arranged into sheets and separated by dense hyalinized stroma.
Epithelioid melanoma, thyroid carcinoma and epithelial-myoepithelial carcinoma were ruled out because the patients had no history of these.
Jaw Bone Metastasis of Hepatocellular Carcinoma
Hepatocellular carcinoma is the sixth most frequently diagnosed cancer. The management of hepatocellular carcinoma has been improved due to the enhancement of surgical and chemotherapeutic interventions. Although the life expectancy of patients with hepatocellular carcinoma has increased, distant metastasis remains a challenge in the treatment of this disease. There are two mechanisms of metastasis from the liver to the maxillofacial territory. The first mechanism involves the hepatic artery and the portal vein. When tumor tissues affect these vessels, metastatic dissemination would reach the lung first and then the maxillofacial area. It has been postulated that there may be a connection between the azygos or hemiazygos veins and the vertebral venous plexus, which creates another route for hematogenous spread. There would consequently be free communication between the venous systems of the neck, thorax, abdomen and pelvis and the non-valve vertebral venous plexus, which extends from the cranial base to the coccyx. Any increase in the intra-abdominal pressure can result in an ascendant flow through the vertebral venous plexus. In such cases, hepatocellular carcinoma cells could reach the maxillofacial territory through these hematogenous routes and metastasize into the mandible [20,21,22].
In the bones of the jaw, the mandible is a frequent site for metastases (80-85%). This predisposition could be explained by the presence of a sinusoidal vascular network rich in hematopoietic tissue that favors the spread of the tumor cells. The presence of distant metastases is related to the histopathological subtype of the hepatocellular carcinoma, the degree of cellular differentiation, but also the local anatomy and tissue characteristics of the bone [23]. In the process of metastasis, dissemination of the cells from primary site or thrombus mixed with carcinoma cells may contribute to the formation of metastatic lesions. The specific structure of the mandible, lower blood flow rates in the canal and abrupt alteration to this can result in the permanent implantation of a tumor thrombus [24]. Additionally, Van der Waal et al. [25] found that there was an increasing risk for tumor embolus formation with low blood flow in the red bone marrow. Up to 25% of the adult mandibular marrow cavity is occupied by red bone marrow, mainly in the regions of the third molars and premolars, which become the principal targets for tumor metastasis [16].
In the presented case, the history of hepatocellular carcinoma and the positivity of liver cell line markers, respectively HepPar-1, AFP and CD10, associated with the negative reaction for CK7 and CEA, led to the diagnosis. However, there are difficult cases in which the presence of metastasis is the first manifestation of the disease and sometimes the tumor can be poorly differentiated. In such cases, the use of cell line markers and subsequent ones specific to the tumor site are required [20,26,27].
Studies have shown increased sensitivity and specificity using a combination of markers. Hepatocellular carcinoma is positive for certain cytokeratins, particularly low molecular weight cytokeratins (CK8/18), and for pCEA (usually with canalicular staining). HepPar-1 is an antigen reflecting hepatocytic differentiation, and it stains both normal fetal and adult liver as well as neoplastic tumor, including 80% to 100% of hepatocellular carcinoma. The staining is usually of a granular, cytoplasmic pattern. Some researchers have reported decreased staining with more poorly differentiated tumor. AFP is an oncofetal glycoprotein that is positive in approximately 70% of hepatocellular carcinoma cases. However, AFP has limitations in its sensitivity and specificity for hepatocellular carcinoma, therefor its utilization should be correlated with HepPar-1 and CD10 and the cytokeratin immunohistochemical profile [28].
The prognosis of patients with hepatocellular carcinoma metastases is poor and the radical resection of metastases has been controversial. Palliative surgery could be performed in patients who reported spontaneous bleeding, severe pain and dysphagia caused by large tumor sizes, while palliative treatment such as radiotherapy, chemotherapy, and immunotherapy are used to relieve the pain and prolong the patient's life [29,30].
6. Conclusions
Rarely, hepatocellular carcinoma and renal cell carcinoma metastasize to the oral cavity and such cases have a poor prognosis due to the delay in the diagnosis. Bearing in mind the possibility of unpredictable metastases from unusual primary sites as kidney and liver in the head and neck region, even if there is no history of these malignancies, will help the pathologists to choose the antibodies panel and to include targeted markers for these primary sites. Publishing all these rare metastatic cases will help the physicians to be aware of the possibility of the metastatic disease even if the primary tumor is not known.
Author Contributions
Conceptualization, R.M.C.; methodology, F.B.; software, M.R.; validation, R.M.C., F.B. A.N.; formal analysis, R.M.C.; investigation, R.M.C., M.R.; resources, F.B., R.M.C.; data curation, R.M.C.; writing—original draft preparation, R.M.C.; writing—review and editing, F.B.; visualization, M.R.; supervision, F.B.; project administration, R.M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethical committee of the institution (CECS No. E-5175/25.09.2023).
Informed Consent Statement
Informed consent was obtained from the subjects involved in the study.
Acknowledgments
We acknowledge the help of all of our colleagues.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lenkeit:, C.; Bank, J.; Shirazi, M. Renal Cell Carcinoma in the Head and Neck: Case Presentation of a Patient With a Rare Metastatic Pattern. Curēus 2020, 12, e11894. [Google Scholar] [CrossRef]
- Lieder, A.; Guenzel, T.; Lebentrau, S.; Schneider, C.; Franzen, A. Diagnostic relevance of metastatic renal cell carcinoma in the head and neck: An evaluation of 22 cases in 671 patients. Int Braz J Urol 2017, 43, 202–208. [Google Scholar] [CrossRef]
- Remenschneider, A.K.; Sadow, P.M.; Lin, D.T.; Gray, S.T. Metastatic Renal Cell Carcinoma to the Sinonasal Cavity: A Case Series. J. Neurol. Surg. Rep. 2013, 74, 67–72. [Google Scholar]
- Ali, R.A.; Mohamed, K.E. Metastatic Clear Cell Renal Cell Carcinoma Presenting with a Gingival Metastasis. Clin Pract. 2016, 10, 847. [Google Scholar] [CrossRef]
- Morita, Y.; Kashima, K.; Suzuki, M.; Kinosada, H.; Teramoto, A.; Matsumiya, Y.; Uzawa, N. Differential Diagnosis between Oral Metastasis of Renal Cell Carcinoma and Salivary Gland Cancer. Diagnostics 2021, 11, 506. [Google Scholar] [CrossRef]
- Yu, S.; Estess, A.; Harris, W.; Dillon, J. A rare occurrence of hepatocellular carcinoma metastasis to the mandible: report of a case and review of the literature. J. Oral Maxillofac. Surg. 2012, 70, 1219–1223. [Google Scholar] [CrossRef]
- Pesis, M.; Taicher, S.; Greenberg, G.; Hirshberg, A. Metastasis to the jaws as a first manifestation of hepatocellular carcinoma: report of a case and analysis of 41 cases. J Craniomaxillofac Surg 2014, 42, 1997–2001. [Google Scholar] [CrossRef]
- Dick, A.; Mead, S.G.; Mensh, M.; Schatten, W.E. Primary hepatoma with metastasis to the mandible. Am. J. Surg. 1957, 94, 846–850. [Google Scholar] [CrossRef]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef]
- Sarău, C.A.; Poenaru, M.; Balica, N.C.; Baderca, F. Rare sinonasal lesions. Rom J Morphol Embryol. 2017, 58, 1541–1547. [Google Scholar]
- Trandafir, C.M.; Tischer, A.A.; Horhat, I.D.; Balica, N.C.; Sitaru, A.M.; Guran, K.; Morar, R.; Baderca, F.; Jifcu, E.M.; Moţ, I.C.; Burlacu, O.N.; Poenaru, M.; Sarău, C.A. Fortuitous discovery of melanomas in the ENT Department - a histopathological and immunohistochemical study. Rom J Morphol Embryol. 2020, 6, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- Baderca, F.; Vincze, D.; Balica, N.; Solovan, C. Mucosal melanomas in the elderly: challenging cases and review of the literature. Clin Interv Aging. 2014, 9, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Rakitovan, M.; Nicoara, A.; Closca, R.M.; Balica, N.C.; Stefanescu, E.H.; Baderca, F. Leiomyoma with Uncommon Localization-Incisive Papilla and Palatal Fibromucosa: A Case Report. Medicina (Kaunas) 2023, 59, 1346. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Yangi, L.; Wang, L.; Zuo, W.; Shuanghu Yuan, S.; Yu, J.; Yu, Q.; Xudong Hu, X.; Wang, S.; Liu, N.; Zhang, H.; Yuchun Wei, Y. Primary clear cell carcinoma of nasal cavity: report of six cases and review of literature. Int. J. Clin. Exp. Med. 2014, 7, 5469–5476. [Google Scholar] [PubMed]
- Zur, K.B.; Brandwein, M.; Wang, B.; et al. Primary description of a new entity, renal cell-like carcinoma of the nasal cavity: van Meegeren in the house of Vermeer. Arch Otolaryngol Head Neck Surg 2002, 128, 441–447. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017; pp. 24–26. [Google Scholar]
- Chen, Z.; Wang, Z.; Shi, H.; Liu, Q. Renal cell -like carcinoma of the nasal cavity: a case report and review of the literature. Diagnostic Pathol 2017, 12. [Google Scholar]
- Morvan, J.B.; Veyrières, J.B.; Mimouni, O.; Cathelinaud, O.; Allali, L.; Verdalle, P. Clear-cell renal carcinoma metastasis to the base of the tongue and sphenoid sinus: two very rare atypical ENT locations. Eur Ann Otorhinolaryngol Head Neck Dis. 2011, 128, 91–94. [Google Scholar] [CrossRef]
- Sikka, S.; Sikka, P.; Kaur, G.; Shetty, D.C. A review of histopathological and immunohistochemical parameters in diagnosis of metastatic renal cell carcinoma with a case of gingival metastasis. J Cancer Res Ther 2013, 9, 105–107. [Google Scholar] [CrossRef]
- Du, C.; Feng, Y.; Li, N.; Wang, K.; Wang, S.; Gao, Z. Mandibular metastasis as an initial manifestation of hepatocellular carcinoma: A report of two cases. Oncol. Lett. 2015, 9, 1213–1216. [Google Scholar] [CrossRef]
- Piccirillo, M.; Granata, V.; Albino, V.; et al. Can hepatocellular carcinoma (HCC) produce unconventional metastases? Four cases of extrahepatic HCC. Tumori J. 2013, 99, 19–23. [Google Scholar] [CrossRef]
- Yu, S.; Estess, A.; Harris, W.; Dillon, J. A rare occurrence of hepatocellular carcinoma metastasis to the mandible: report of a case and review of the literature. J. Oral Maxillofac. Surg. 2012, 70, 1219–1223. [Google Scholar] [CrossRef] [PubMed]
- Nawale, K.K.; Vyas, M.; Kane, S.; Patil, A. Metastatic tumors in the jaw bones: A retrospective clinicopathological study of 12 cases at Tertiary Cancer Center. J Oral Maxillofac Pathol 2016, 20, 252–255. [Google Scholar]
- Miller, M.E.; McCall, A.A.; Juillard, G.F.; et al. Hepatocellular carcinoma metastatic to the mandible. Ear Nose Throat J 2013, 92, 17–19. [Google Scholar]
- Van der Waal, R.I.; Buter, J.; van der Waal, I. Oral metastases: report of 24 cases. Br J Oral Maxillofac Surg 2003, 41, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Li, Z.; Song, Q.; Qian, L.; Xie, B.; Zhu, J. Clinicopathological features and differential diagnosis of hepatocellular carcinoma in extrahepatic metastases. Medicine (Baltimore) 2018, 97. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Morales, J.M.; Dorantes-Heredia, R.; Chable-Montero, F.; Vazquez-Manjarrez, S.; Méndez-Sánchez, N.; Motola-Kuba, D. Bone metastases as the initial presentation of hepatocellular carcinoma. Two case reports and a literature review. Ann Hepatol 2014, 13, 838–842. [Google Scholar] [CrossRef]
- Dabbs, D.J. Diagnostic immunohistochemistry: theranostic and genomic applications, 5th ed.; Elsevier: Philadelphia, PA, 2019; pp. 576–582. [Google Scholar]
- Hong, J.H.; Lee, K.; Kim, J.; Ahn, K.M. Prognosis of hepatocellular carcinoma metastasizing to the oral cavity. Maxillofac. Plast. Reconstr. Surg. 2021, 43. [Google Scholar] [CrossRef]
- Hongwei, Liu.; Qingxia, Xu.; Fanzhong, Lin.; Jianjun, Ma. Hepatocellular carcinoma metastasis to the mandibular ramus: a case report. Int. J. Clin. Exp. Pathol. 2019, 12, 1047–1051.
Figure 1.
Microscopic imaging – HE-staining of gingival mucosa with tumoral proliferation: (a) ob. 5x; (b) ob. 20x.
Figure 1.
Microscopic imaging – HE-staining of gingival mucosa with tumoral proliferation: (a) ob. 5x; (b) ob. 20x.
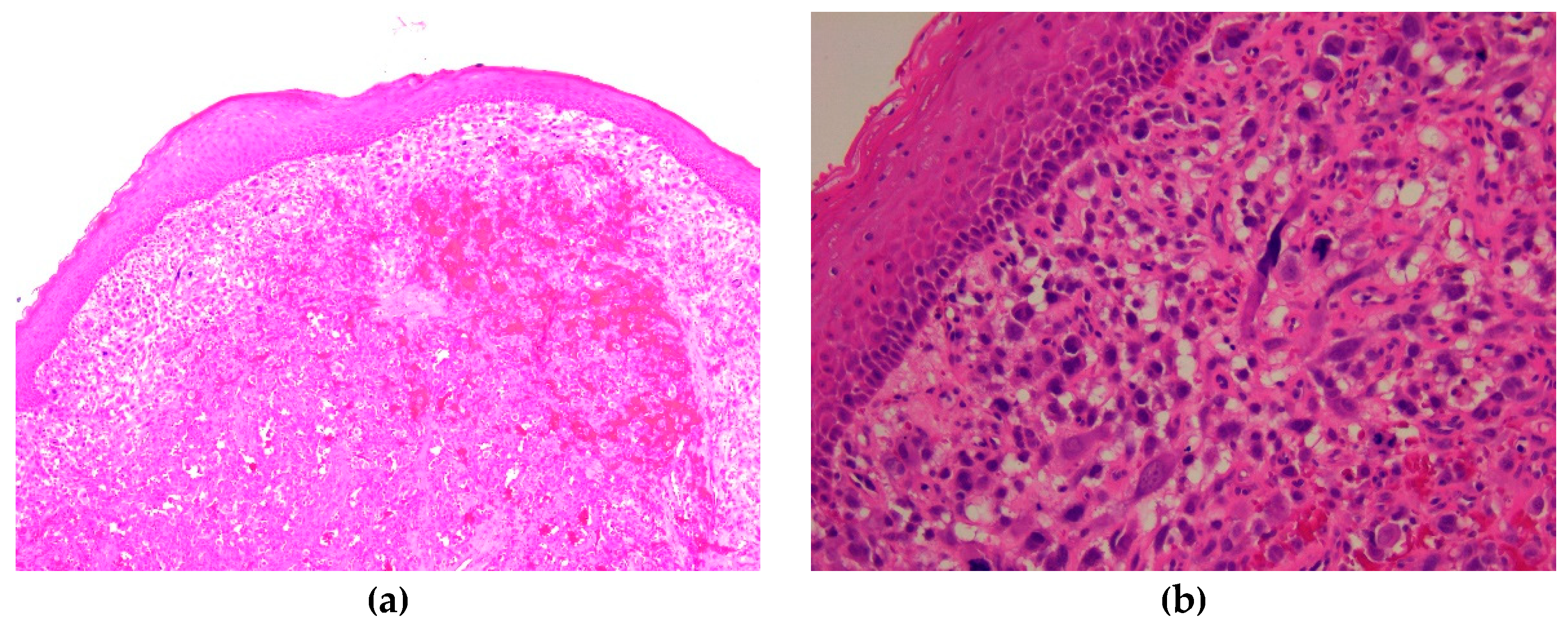
Figure 2.
Microscopic imaging – HE-staining: (a) tumor cells, ob. 40x; (b) gingival mucosa with tumor cells, ob. 40x.
Figure 2.
Microscopic imaging – HE-staining: (a) tumor cells, ob. 40x; (b) gingival mucosa with tumor cells, ob. 40x.
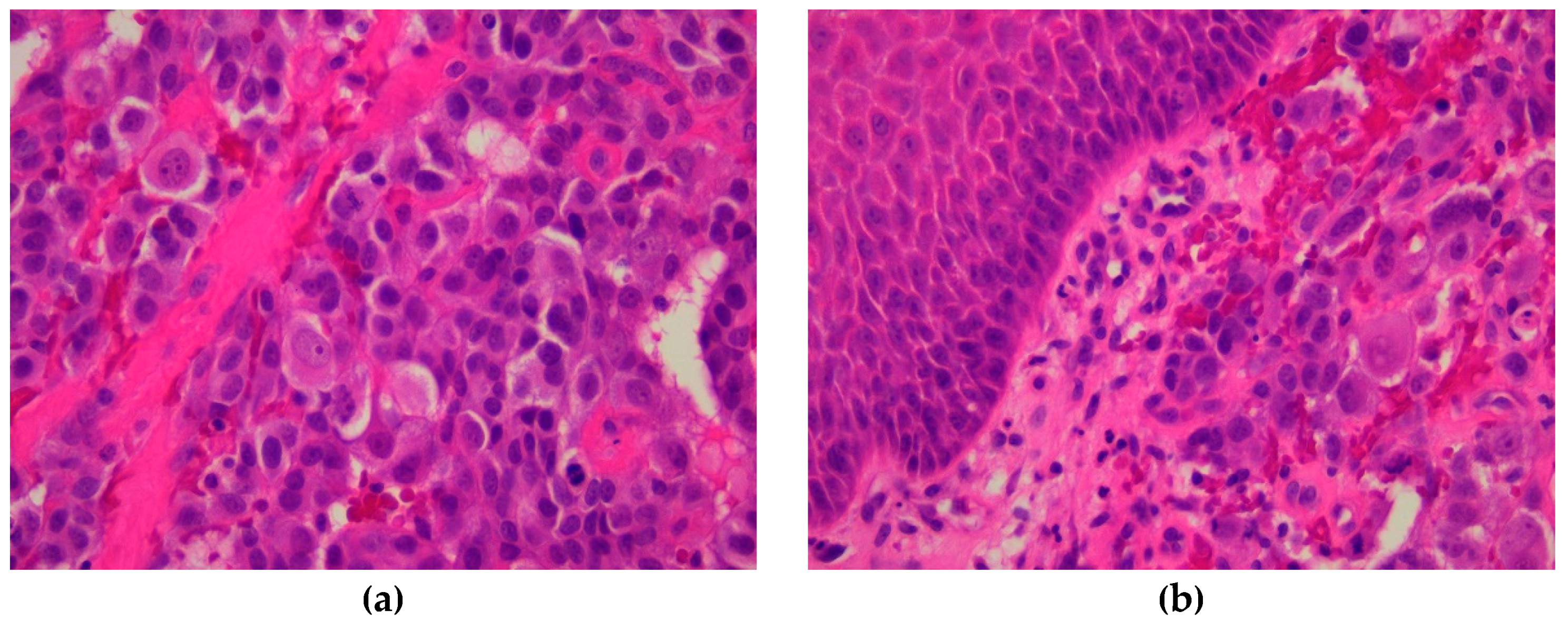
Figure 3.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for CK AE1/AE3, ob. 40x; (b) positive reaction for vimentin, ob. 40x.
Figure 3.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for CK AE1/AE3, ob. 40x; (b) positive reaction for vimentin, ob. 40x.
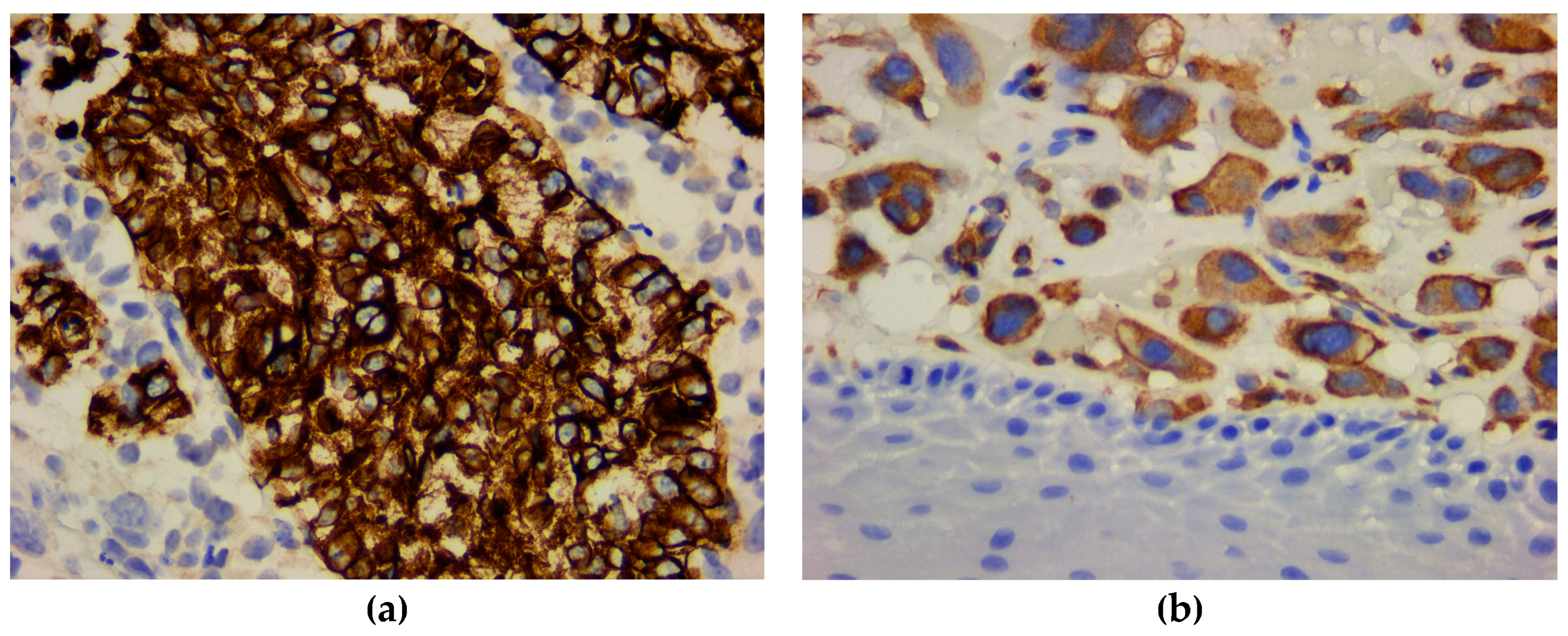
Figure 4.
Microscopic imaging – immunohistochemical profile: (a) strong positive reaction for CK8/18, ob. 40x; (b) negative reaction for CK7, ob. 40x.
Figure 4.
Microscopic imaging – immunohistochemical profile: (a) strong positive reaction for CK8/18, ob. 40x; (b) negative reaction for CK7, ob. 40x.

Figure 5.
Microscopic imaging – immunohistochemical profile: (a) negative reaction for CK20, ob. 40x; (b) negative reaction for CK5 with internal positive control on the covering parakeratinized stratified squamous epithelium of gingival mucosa, ob. 40x.
Figure 5.
Microscopic imaging – immunohistochemical profile: (a) negative reaction for CK20, ob. 40x; (b) negative reaction for CK5 with internal positive control on the covering parakeratinized stratified squamous epithelium of gingival mucosa, ob. 40x.
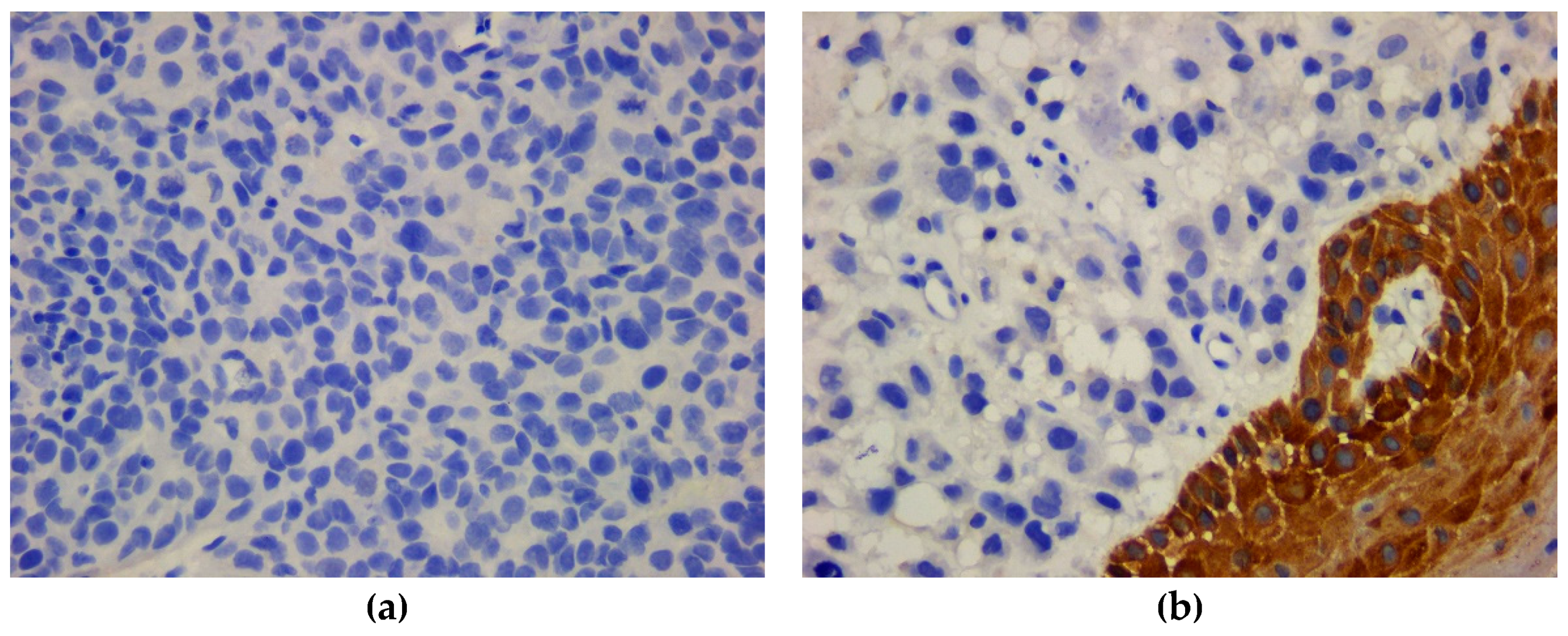
Figure 6.
Microscopic imaging – immunohistochemical profile: negative reaction for EMA with internal positive control on the covering parakeratinized stratified squamous epithelium of gingival mucosa, ob. 40x.
Figure 6.
Microscopic imaging – immunohistochemical profile: negative reaction for EMA with internal positive control on the covering parakeratinized stratified squamous epithelium of gingival mucosa, ob. 40x.
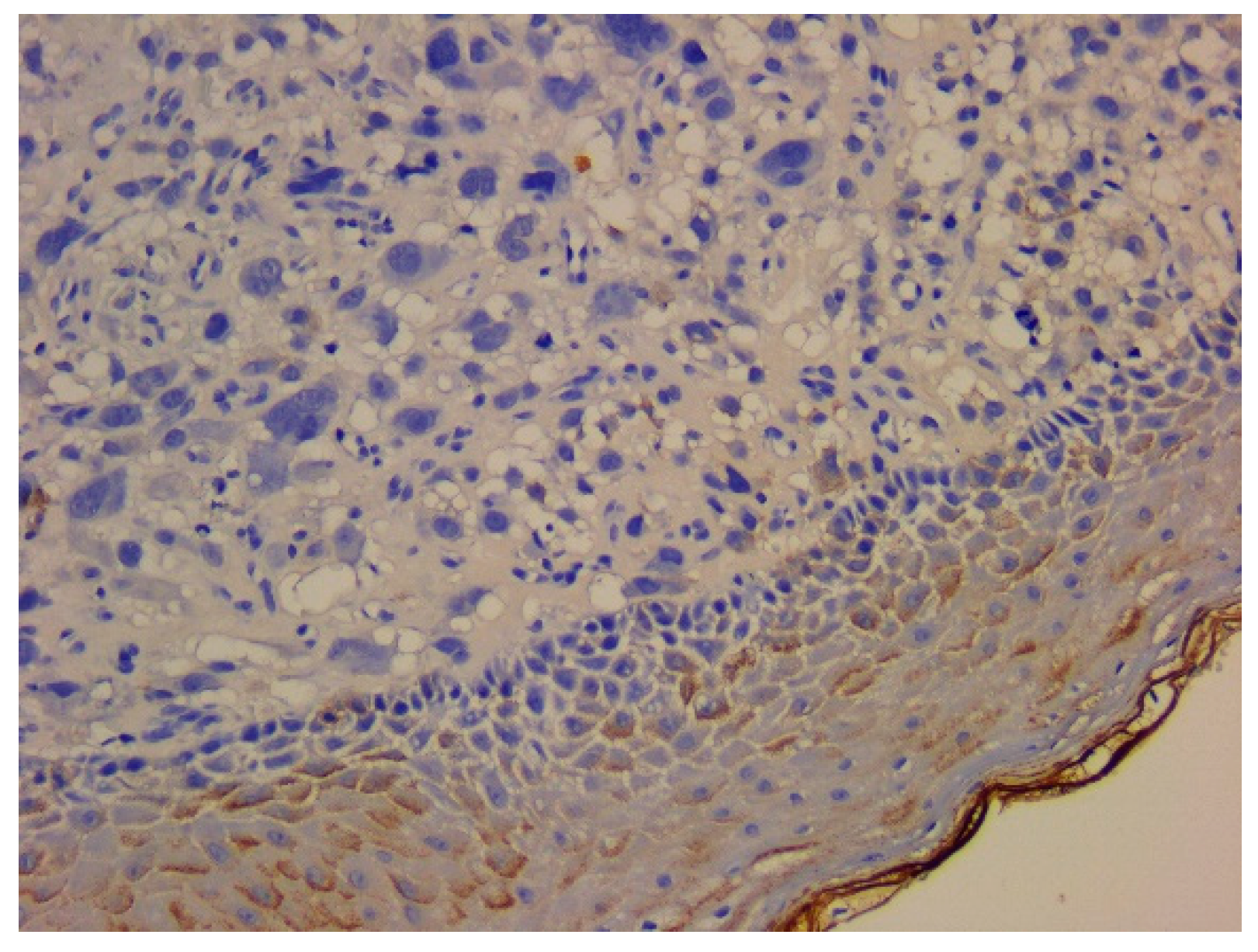
Figure 7.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for CD10, ob. 40x; (b) positive reaction for RCC, ob. 40x.
Figure 7.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for CD10, ob. 40x; (b) positive reaction for RCC, ob. 40x.
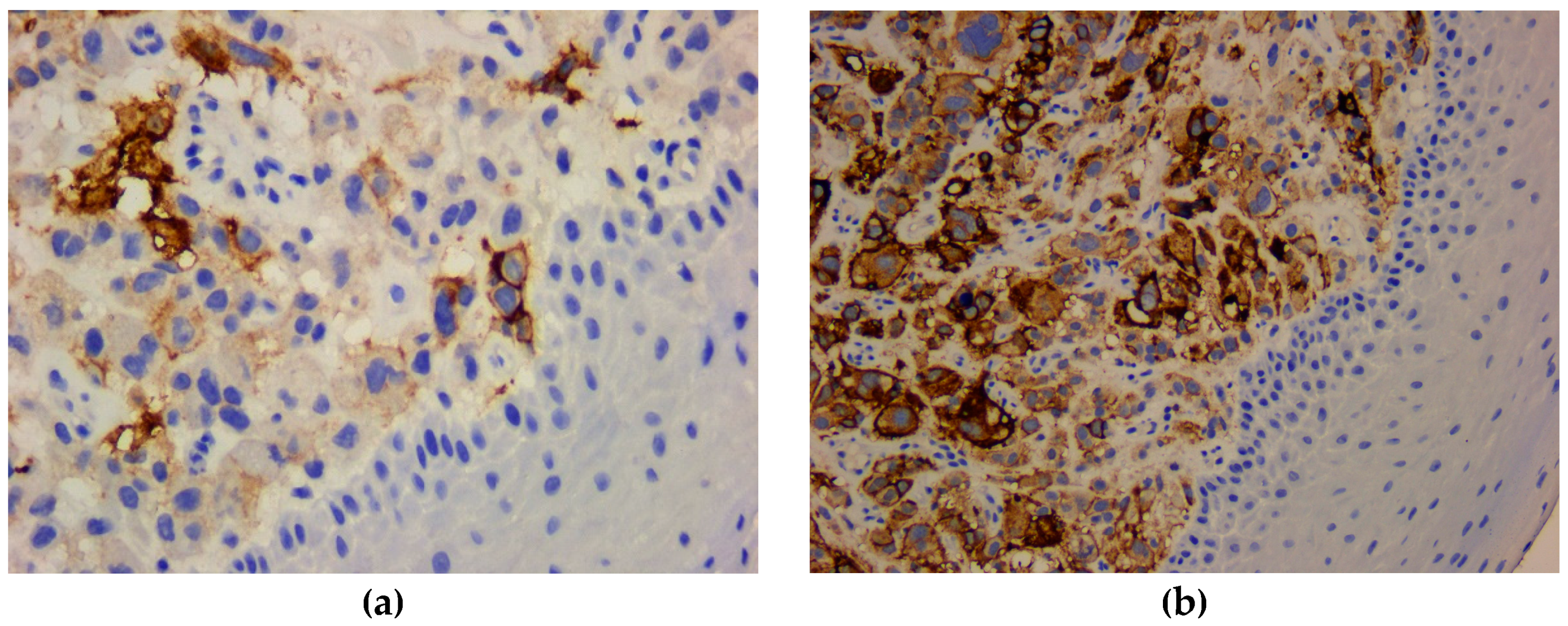
Figure 8.
Microscopic imaging – HE-stained slides: (a) nasal mucosa with tumoral proliferation, ob. 5x; (b) tumoral cells with acinar and nested pattern, ob. 20x.
Figure 8.
Microscopic imaging – HE-stained slides: (a) nasal mucosa with tumoral proliferation, ob. 5x; (b) tumoral cells with acinar and nested pattern, ob. 20x.
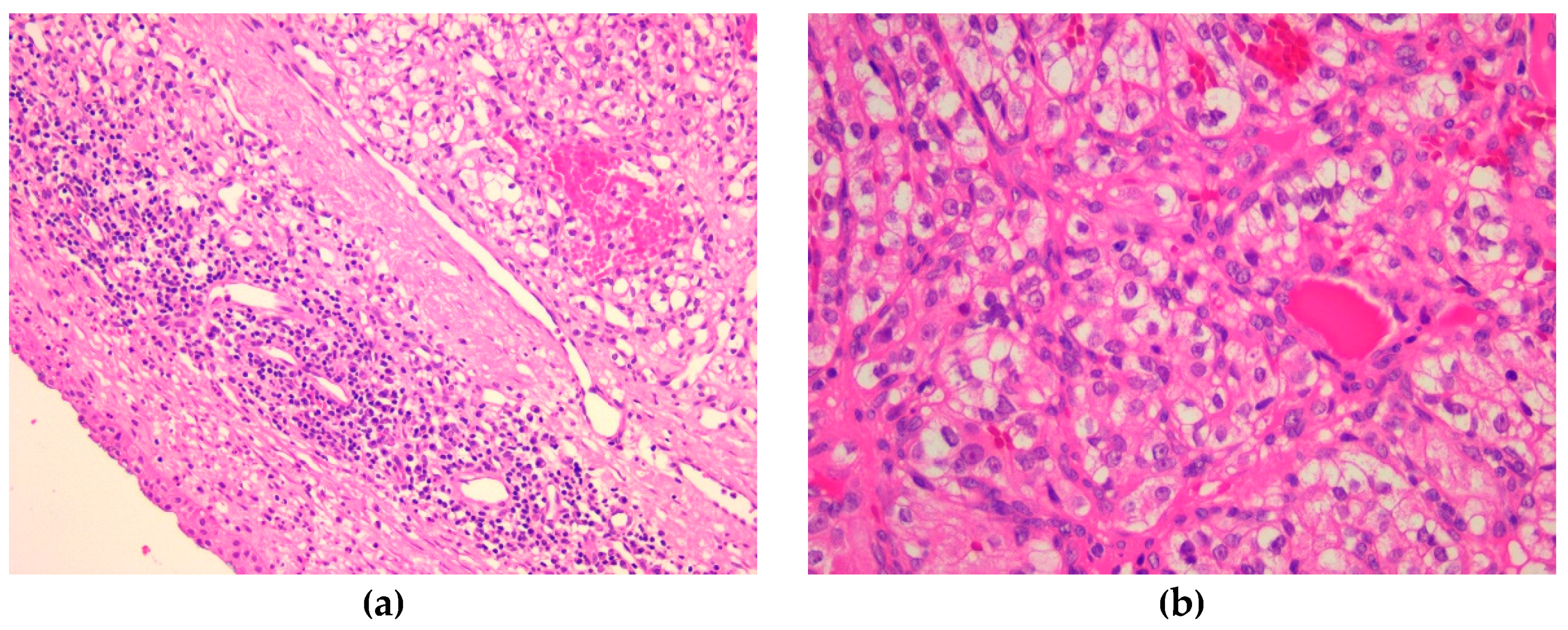
Figure 9.
Microscopic imaging – HE-stained slides: (a) tumoral proliferation with hemorrhage, ob. 40x; (b) tumoral proliferation with hemorrhage and cyst formation, ob. 40x.
Figure 9.
Microscopic imaging – HE-stained slides: (a) tumoral proliferation with hemorrhage, ob. 40x; (b) tumoral proliferation with hemorrhage and cyst formation, ob. 40x.
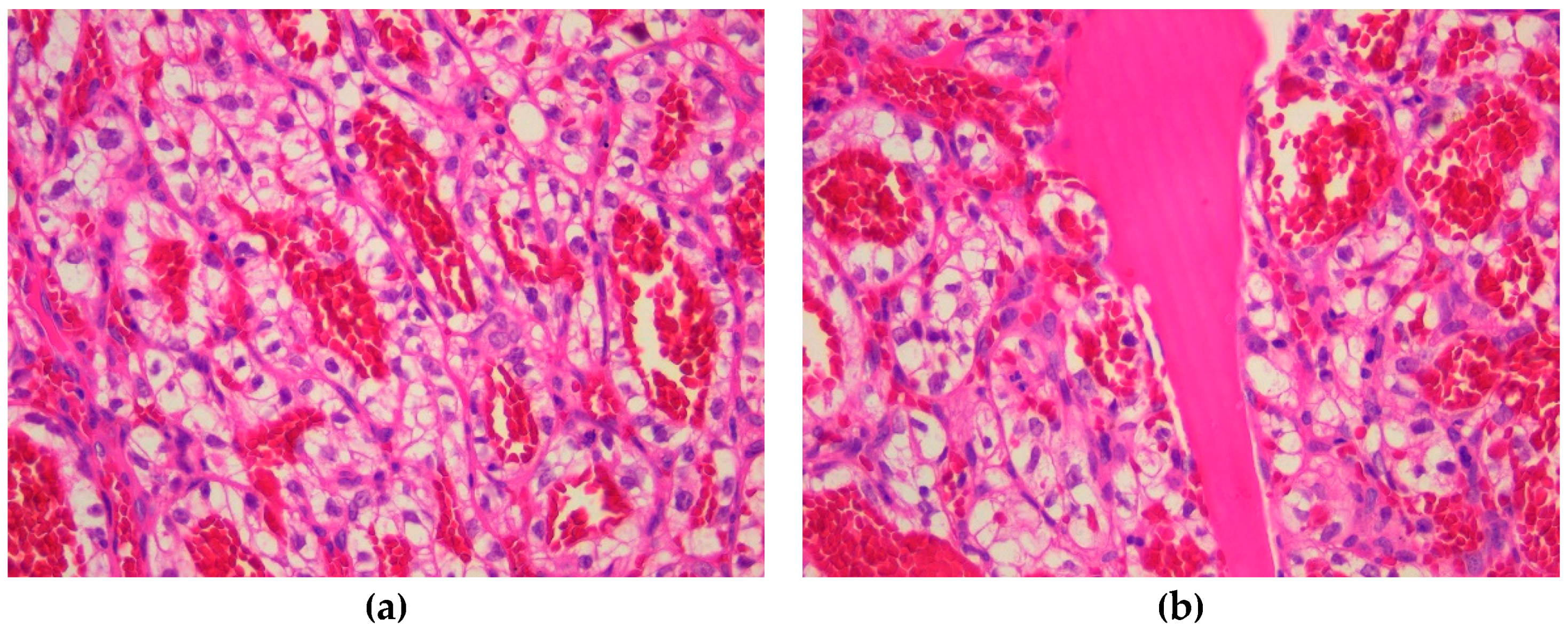
Figure 10.
Microscopic imaging – immunohistochemical profile: (a) strong positive reaction for CK8/18 with internal positive control of the nasal mucosa, ob. 20x; (b) negative reaction for CK7 with internal positive control of the nasal mucosa, ob. 20x.
Figure 10.
Microscopic imaging – immunohistochemical profile: (a) strong positive reaction for CK8/18 with internal positive control of the nasal mucosa, ob. 20x; (b) negative reaction for CK7 with internal positive control of the nasal mucosa, ob. 20x.
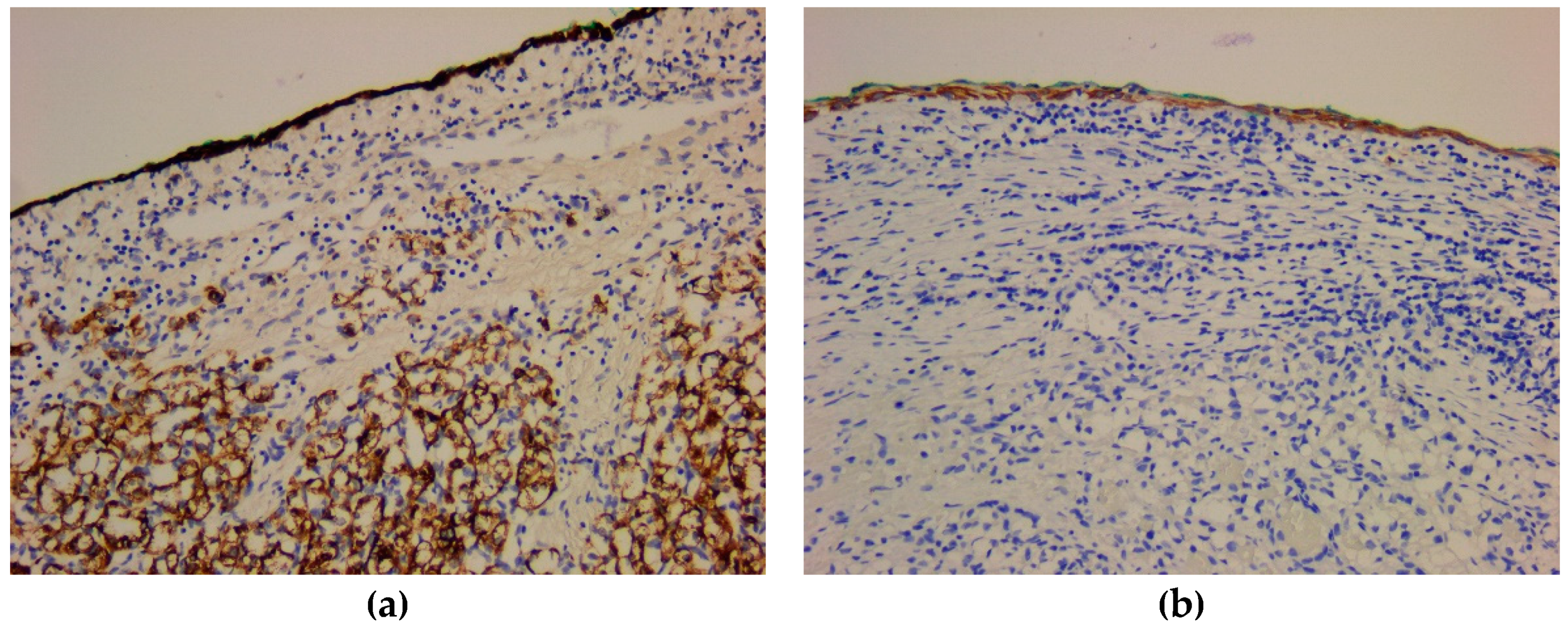
Figure 11.
Microscopic imaging – immunohistochemical profile: (a) negative reaction for CK20, ob. 40x; (b) negative reaction for CK5 with internal positive control of the nasal mucosa, ob. 20x.
Figure 11.
Microscopic imaging – immunohistochemical profile: (a) negative reaction for CK20, ob. 40x; (b) negative reaction for CK5 with internal positive control of the nasal mucosa, ob. 20x.
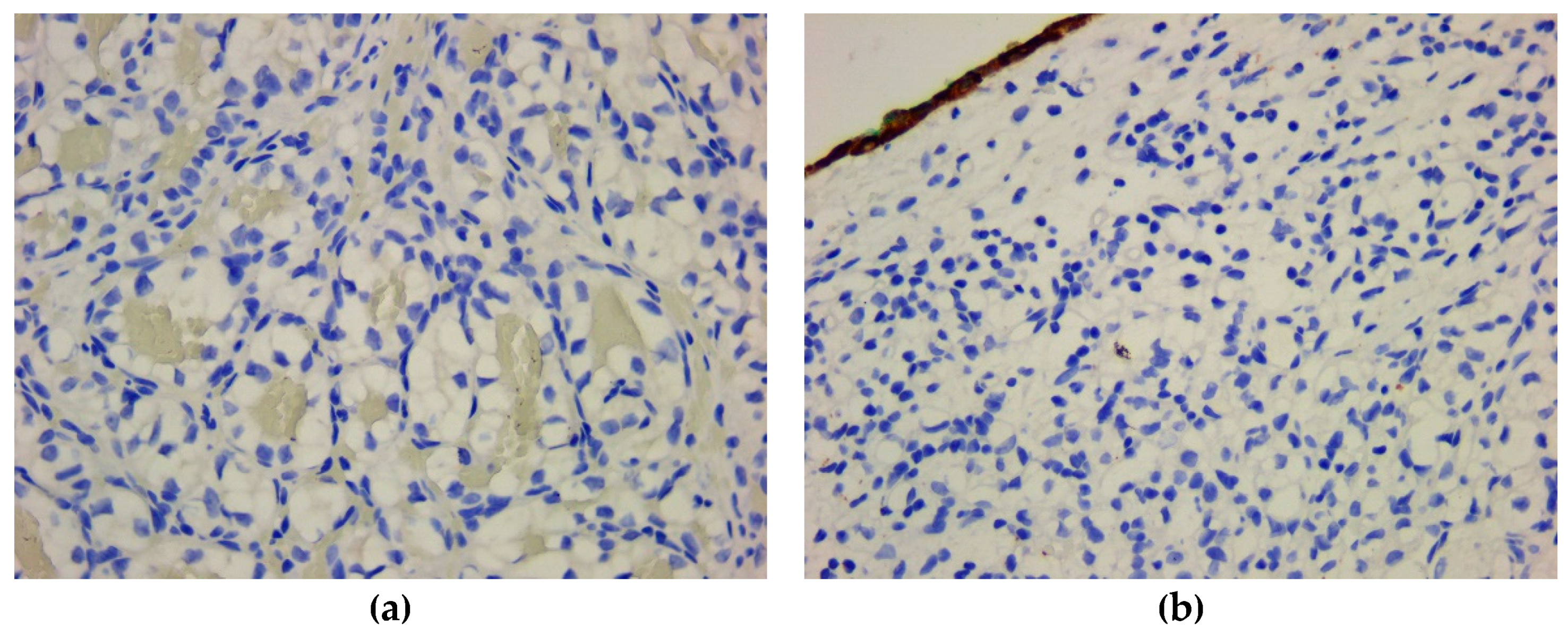
Figure 12.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for CD10, ob. 40x; (b) positive reaction for EMA, ob. 40x.
Figure 12.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for CD10, ob. 40x; (b) positive reaction for EMA, ob. 40x.
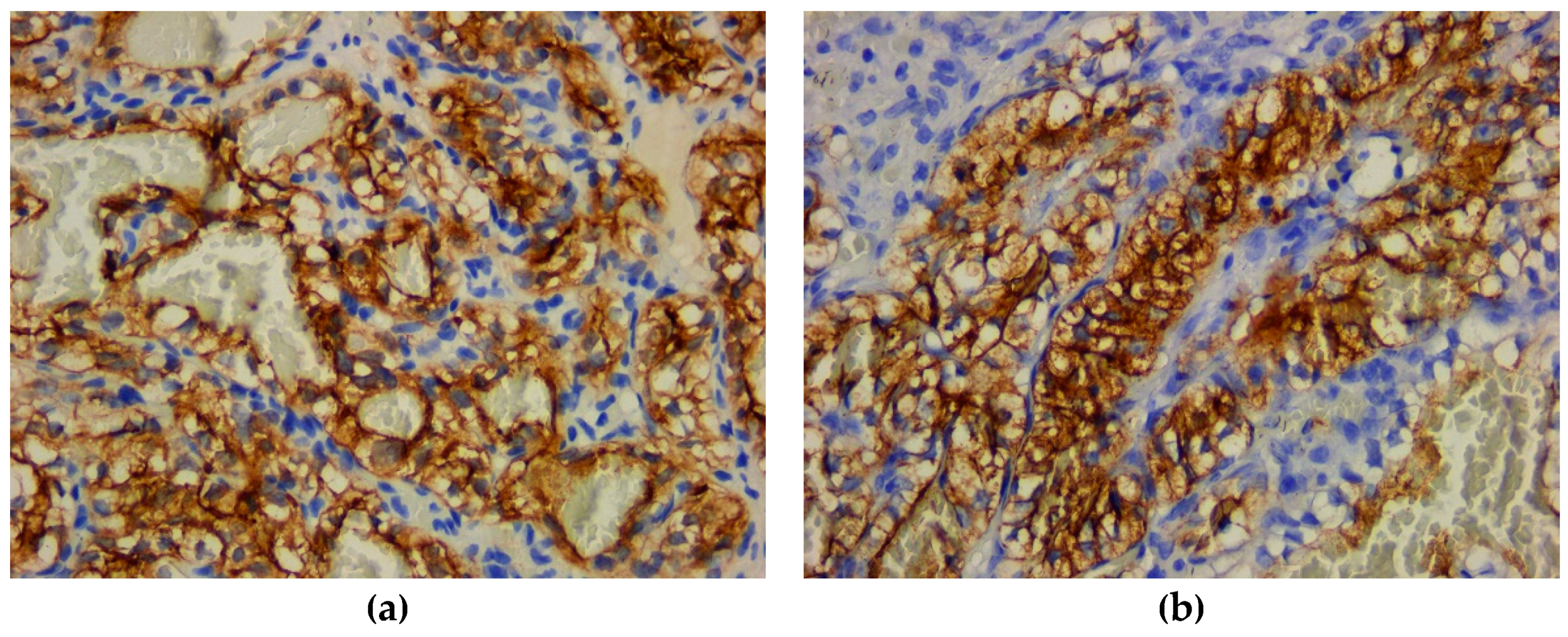
Figure 13.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for vimentin, ob. 40x; (b) positive reaction for RCC, ob. 40x.
Figure 13.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for vimentin, ob. 40x; (b) positive reaction for RCC, ob. 40x.
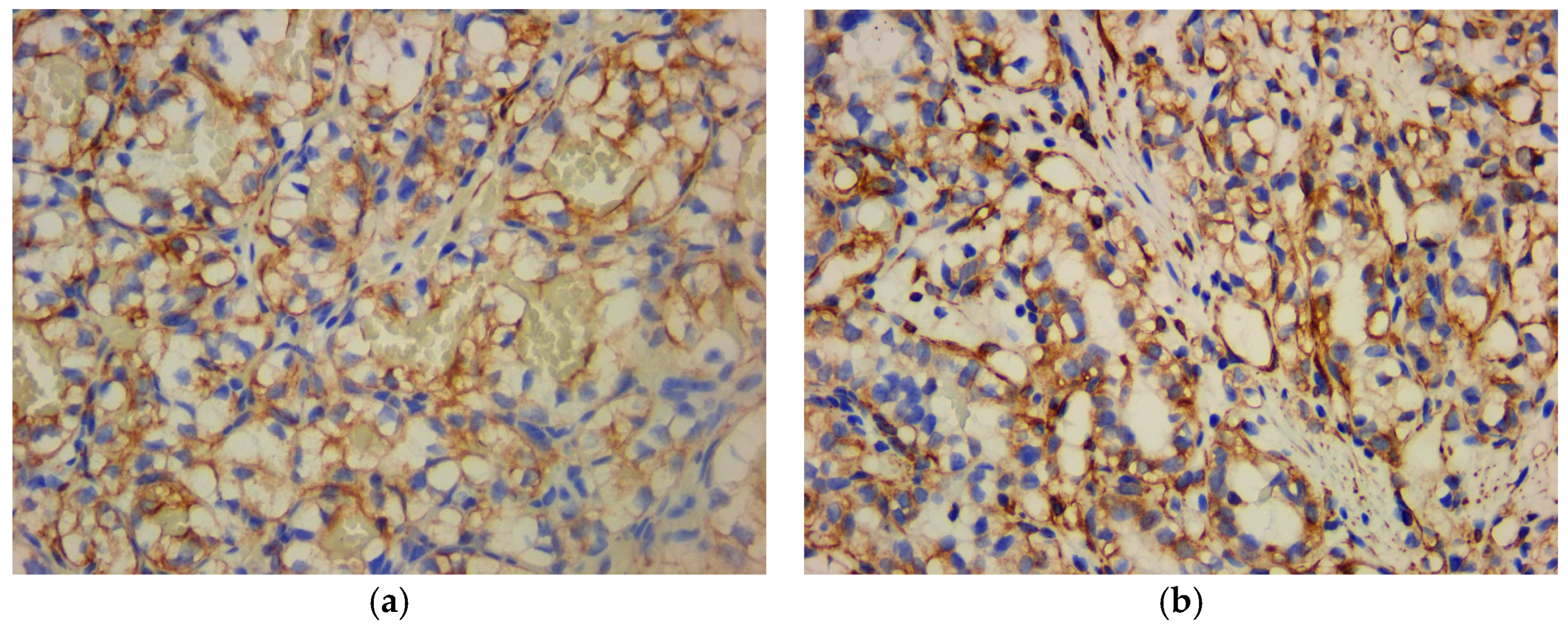
Figure 14.
Computed Tomography imaging - tissue mass at the level of the right masticatory space (arrow).
Figure 14.
Computed Tomography imaging - tissue mass at the level of the right masticatory space (arrow).
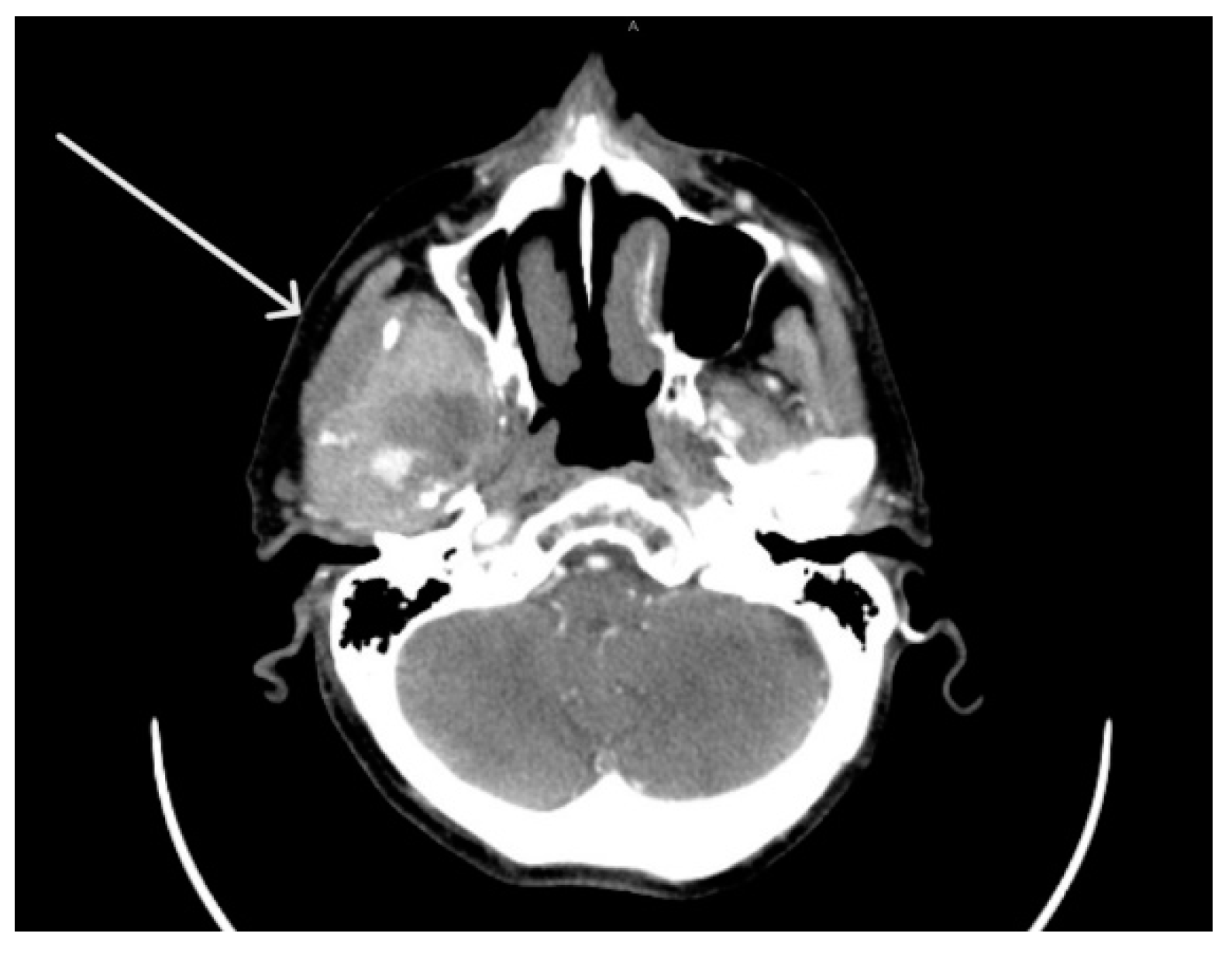
Figure 15.
Computed Tomography imaging – heterogenous lesion with necrotic areas (arrow).

Figure 16.
Computed Tomography imaging - lyses of the right mandibular condyle (arrows): (a) axial imaging; (b) Three-dimensional reconstruction.
Figure 16.
Computed Tomography imaging - lyses of the right mandibular condyle (arrows): (a) axial imaging; (b) Three-dimensional reconstruction.
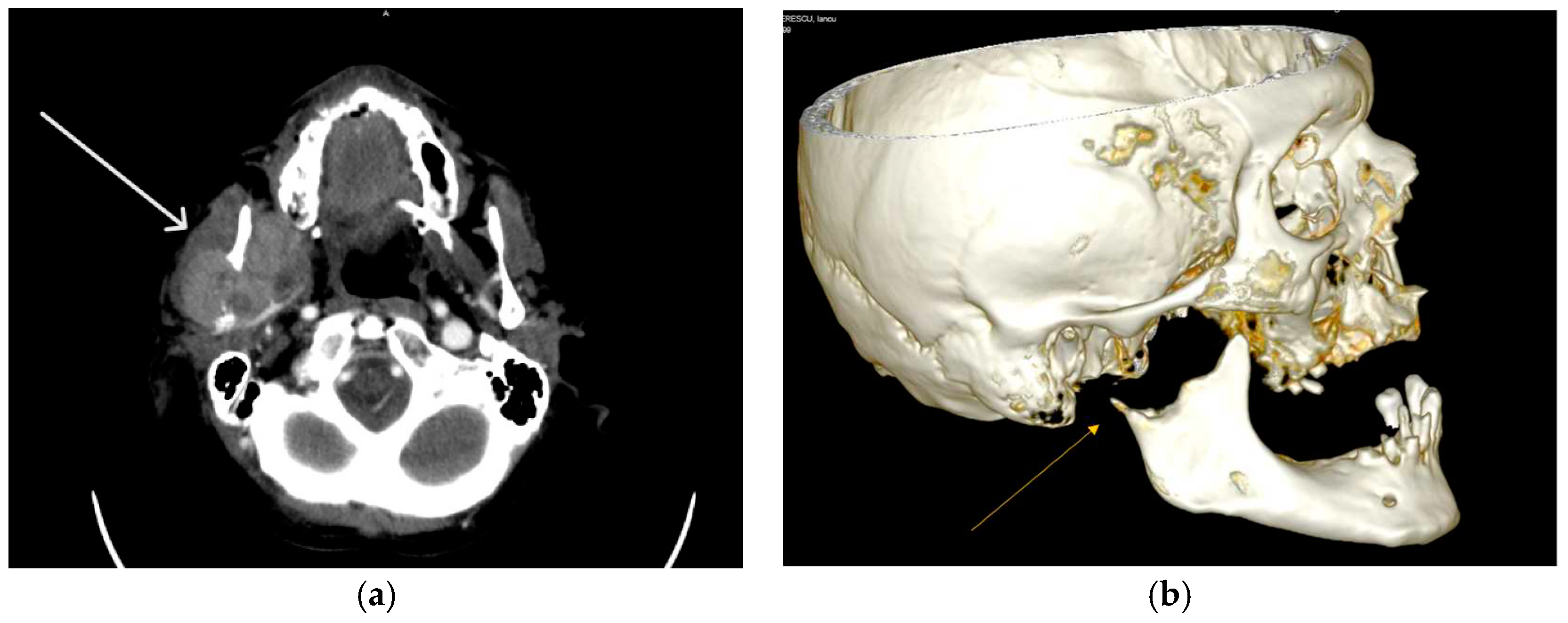
Figure 17.
Microscopic imaging – HE-staining: (a) tumor circumscribed by a pseudocapsule of fibrous connective tissue, ob. 5x; (b) tumoral cells with trabecular pattern and sinusoidal-like spaces, ob. 40x.
Figure 17.
Microscopic imaging – HE-staining: (a) tumor circumscribed by a pseudocapsule of fibrous connective tissue, ob. 5x; (b) tumoral cells with trabecular pattern and sinusoidal-like spaces, ob. 40x.
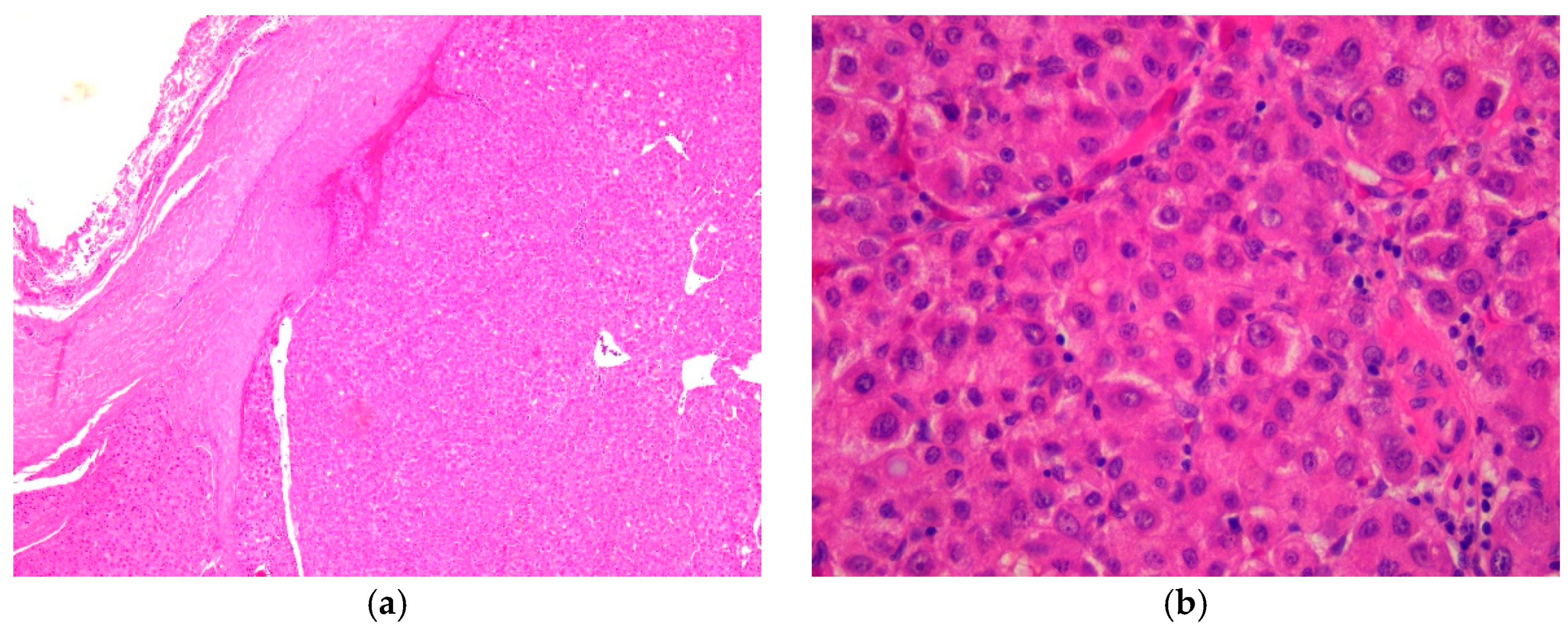
Figure 18.
Microscopic imaging – immunohistochemical profile: (a) strong positive reaction for CK8/18, ob. 40x; (b) negative reaction for CK7, ob. 40x.
Figure 18.
Microscopic imaging – immunohistochemical profile: (a) strong positive reaction for CK8/18, ob. 40x; (b) negative reaction for CK7, ob. 40x.
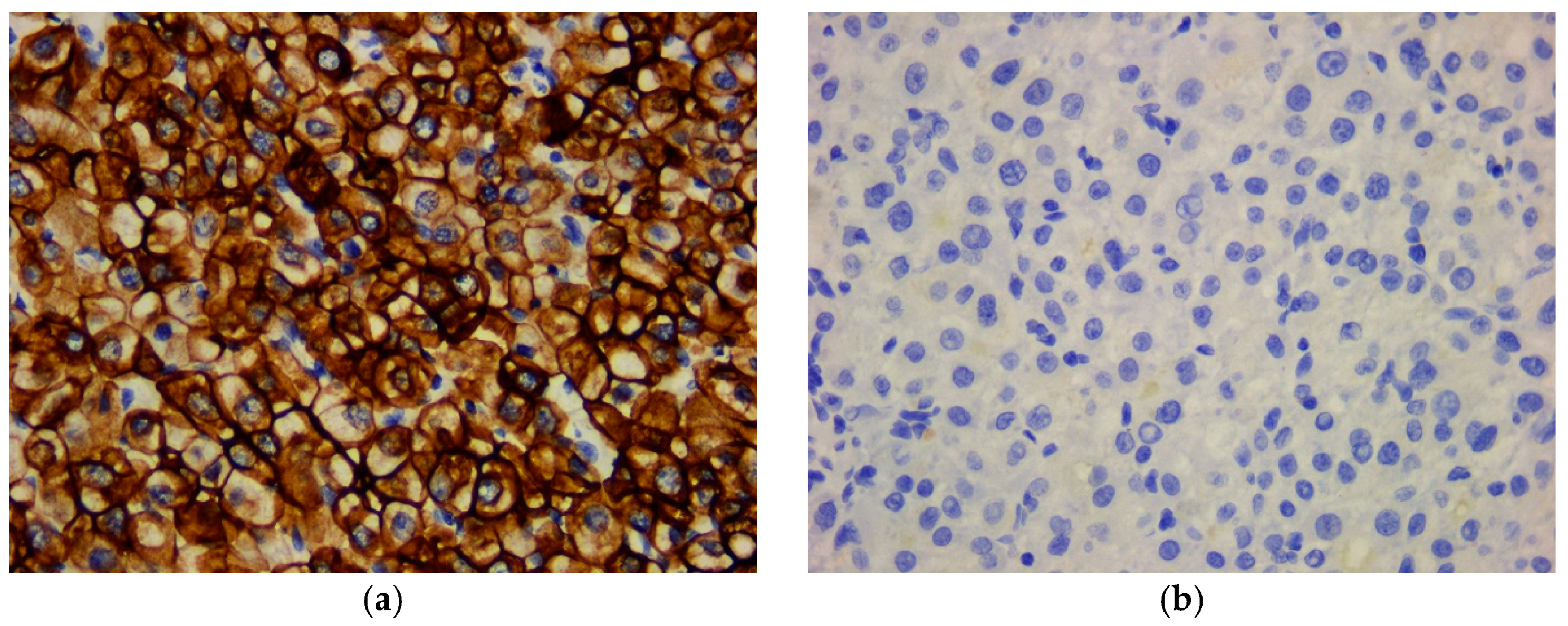
Figure 19.
Microscopic imaging – immunohistochemical profile: (a) negative reaction for CK20, ob. 40x; (b) negative reaction for CK5, ob. 40x.
Figure 19.
Microscopic imaging – immunohistochemical profile: (a) negative reaction for CK20, ob. 40x; (b) negative reaction for CK5, ob. 40x.
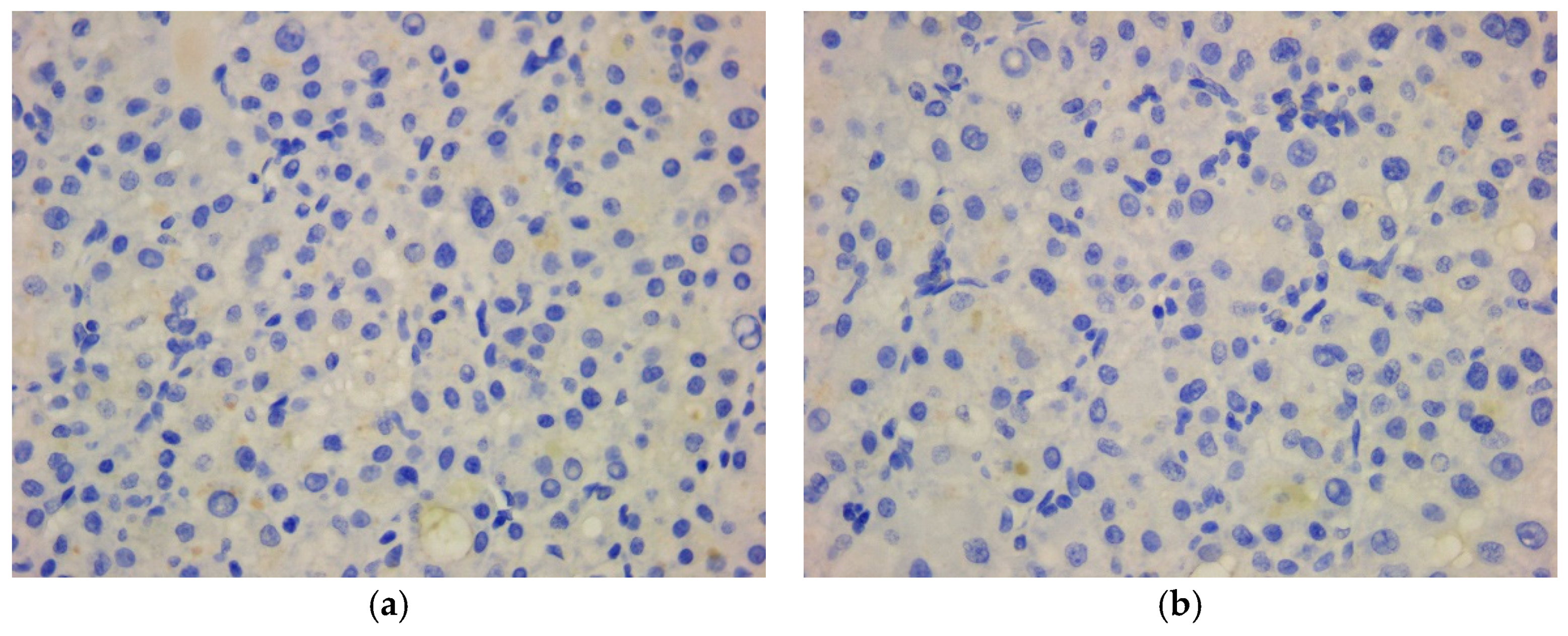
Figure 20.
Microscopic imaging – immunohistochemical profile: (a) strong positive reaction for HepPar-1, ob. 40x; (b) moderate positive reaction for AFP, ob. 40x.
Figure 20.
Microscopic imaging – immunohistochemical profile: (a) strong positive reaction for HepPar-1, ob. 40x; (b) moderate positive reaction for AFP, ob. 40x.
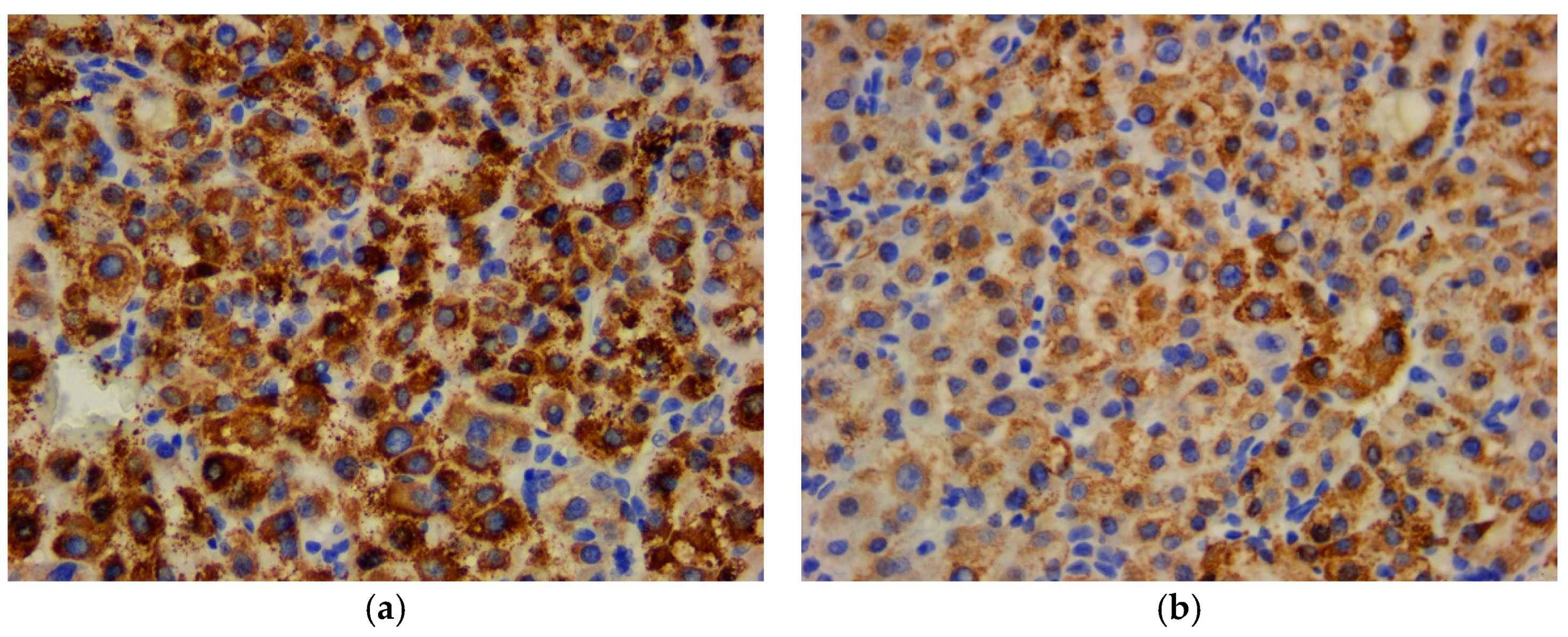
Figure 21.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for CD10, canalicular pattern, ob. 40x; (b) negative reaction for CEA, ob. 40x.
Figure 21.
Microscopic imaging – immunohistochemical profile: (a) positive reaction for CD10, canalicular pattern, ob. 40x; (b) negative reaction for CEA, ob. 40x.
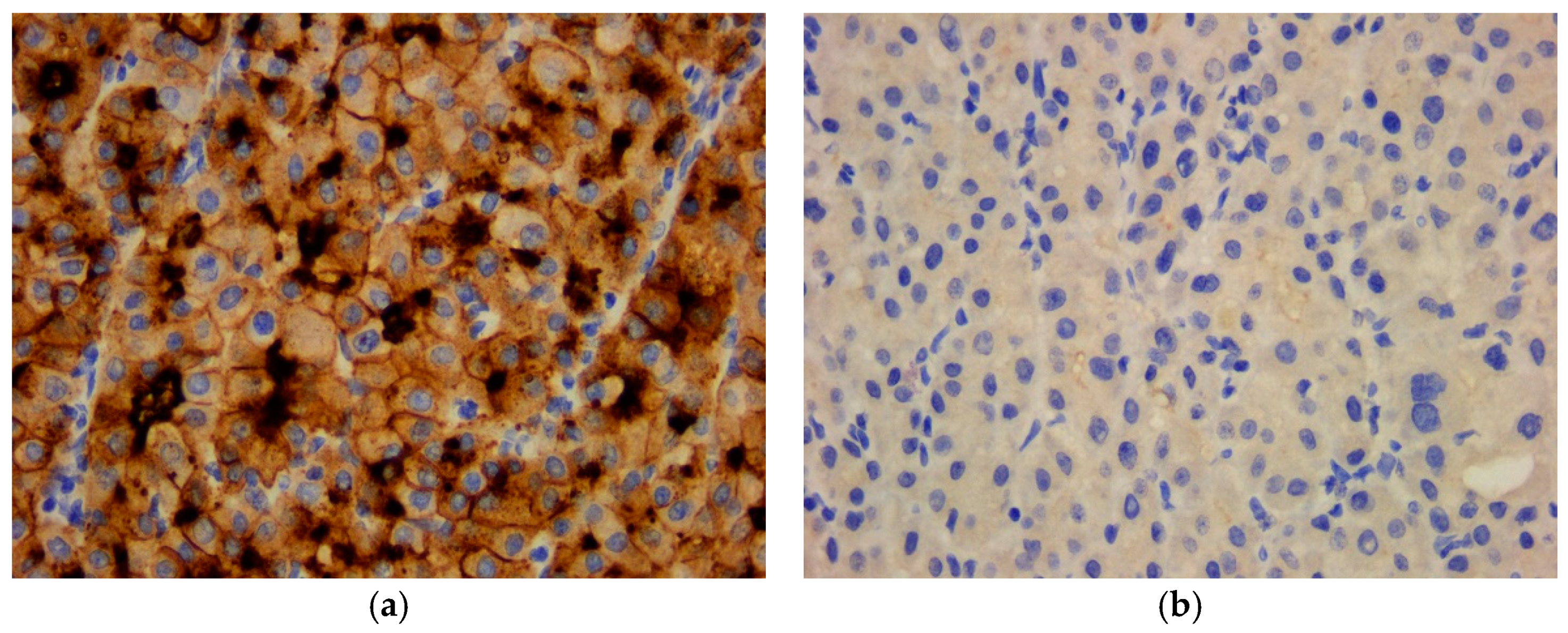

Table 1.
Data related to the antibodies used for immunohistochemical reactions.
| ANTIBODY | SUBSTRATE | CLONE | DILUTION |
|---|---|---|---|
| CK AE1/AE3 1 | Mouse, Monoclonal | AE1/AE3 | 1:100 |
| EMA 2 | Mouse, Monoclonal | GP1.4 | 1:300 |
| CK8/18 3 | Mouse, Monoclonal | 5D3 | 1:100 |
| CK5 4 | Mouse, Monoclonal | XM26 | 1:100 |
| CK7 5 CK20 6 CEA 7 CD10 9 |
Mouse, Monoclonal Mouse, Monoclonal Mouse, Monoclonal Mouse, Monoclonal |
307M-94 L26 II-7 56C6 |
1:100 1:150 RTU 8 RTU |
| AFP 10 HepPar-1 11 S100 protein |
Mouse, Monoclonal Mouse, Monoclonal Rabbit, Polyclonal |
C3 OCH1ES EP32 |
1:100 RTU 1:100 |
| HMB45 12 | Mouse, Monoclonal | HMB45 | 1:60 |
| Melan-A | Mouse, Monoclonal | A103 | 1:50 |
| CD34 13 CD31 14 |
Mouse, Monoclonal Mouse, Monoclonal |
QBEnd/10 1A10 |
RTU 1:75 |
| SMA 15 | Mouse, Monoclonal | asn-1 | 1:50 |
| Desmin | Mouse, Monoclonal | DE-R-11 | 1:75 |
| Vimentin | Mouse, Monoclonal | V9 | 1:800 |
| Ki67 index HHV8 16 RCC 17 |
Mouse, Monoclonal Mouse, Monoclonal Mouse, Monoclonal |
MM1 13B10 66.4.C2 |
1:200 RTU RTU |
1 CK AE1/AE3 (pan cytokeratin AE1/AE3); 2 EMA (epithelial membrane antigen); 3 CK8/18 (cytokeratin 8/18); 4 CK5 (cytokeratin 5); 5 CK7 (cytokeratin 7); 6 CK20 (cytokeratin 20); 7 CEA (carcinoembryonic antigen); 8 RTU (ready-to-use); 9 CD10 (cluster of differentiation 10); 10AFP (alpha fetoprotein); 11 HepPar-1 (Hepatocyte Paraffin 1); 12 HMB45 (Human Melanoma Black); 13 CD34 (cluster of differentiation 34); 14 CD31 (cluster of differentiation 31); 15 SMA (smooth muscle actin); 16 HHV8 (human herpes virus 8); 17 RCC (renal cell carcinoma).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



