
Submitted:
03 October 2023
Posted:
04 October 2023
You are already at the latest version
Abstract
Aim of our study was to retrospectively evaluate whether the oral administration of L. crispatus (M247) could increase pregnancy and live birth rates in women undergoing assisted reproductive technology procedures. Enrolled women (N=160) were divided into two groups: treated (N=80) or untreated (N=80) with the probiotic strain. The odds ratio for a treated woman to get a positive pregnancy test (PPT) was 1.56. In women aged 30–40 years, M247 increased the probability of a PPT in correlation with the progressive rise in BMI, reaching 47% (35% in controls) with a BMI of 35 (odds ratio: 2.00). The CAID statistics showed that in a woman of the blastocyst subgroup, below 43 years, with a BMI over 18.6, treatment with M247 increased the chance of a PPT from 28.4% to 44.5% (odds ratio: 2.08; p<0.05). Considering live births, rate of probiotic group was 12.5% versus 7.5% (odds ratio=1.76). Considering only the blastocyst subgroup, the treatment increased the number of live births by 200% (odds ratio: 3.64; p=0.05). As confirmed also by statistical indices like NNT, NNH and LHH, the use of M247 demonstrated a risk-benefit ratio to the full advantage of the benefits.
Keywords:
vaginal microbiota
; D3-embryos
; D5-blastocysts
; ICSI
; FIVET
; ART
1. Introduction
Infertility, defined as a disease by the WHO, is an increasing problem worldwide [1]. Infertility is estimated to affect between 8% and 12% of reproductive-aged couples; the 12-month prevalence of infertility globally is around 9% and more than 7 million children have been born by assisted reproductive technology (ART) procedure [2,3,4]. It is worth noting that in some areas infertility rates are much higher, reaching about 30% [5]. In spite of many known causes of infertility, including ovulation failure, tubal factor infertility, male factors, and ovarian or uterine factors, in about 20%–25% of couples looking for fertility treatment, the cause, or the causes, remain unexplained [6]. The high prevalence of infertility worldwide makes the identification of modifiable predictors of a successful fertility treatment pertinent. Recently, thanks to some studies concerning an association between unexplained recurrent pregnancy loss (RPL) and the structure of the vaginal microbiota, it has been suggested that the cervicovaginal microbiota may be a useful area of investigation into possible causes of RPL [7]. Vaginal bacterial communities are inter-ethnically classified in five different Community State Types (CST IV) according to bacterial richness and Lactobacillus spp. dominance [8]. Communities expressing low richness and L. crispatus dominance (CST I) correlate with a low obstetric-gynaecological risk. Those characterized by high richness and poor Lactobacillus dominance (CST IV) correlate mostly with vaginal discomfort and/or obstetric-gynaecological diseases [9].
Regarding fertility, systematic review and meta-analysis have identified a negative correlation between vaginal microbiota with high Lactobacillus content and female infertility. A recent study has also correlated the L. crispatus pre-pregnancy dominance with a better chance of getting pregnant within 12 months [10,11]. Two well-known negative predictors for pregnancy are polycystic ovary syndrome (PCOS) and obesity and in both cases, a number of observational studies describe a higher prevalence of non-Lactobacillus dominated vaginal microbiota; among the Lactobacillus-dominated consortia, L. crispatus was reported to be the least common [12,13,14,15,16]. Reviews and meta-analysis describe a strong correlation between abnormal vaginal microbiota (CST IV) and failure of in vitro fertilization (IVF) with an odds ratio of 0.70 [17]. Similarly, the vaginal microbiota profile observed at the time of embryo transfer in women undergoing IVF or intracytoplasmic sperm injection (ICSI) with donated oocytes, showed a higher proportion of samples dominated by L. crispatus in women achieving a positive pregnancy test, clinical pregnancy, and live birth compared with those who did not [18]. Moreover, recurrent implantation failure (RIF) is significantly more common in women with a non-Lactobacillus dominated vaginal microbiota [19]. Again, the clinical pregnancy rate after intrauterine insemination positively correlates with a dominance of vaginal L. crispatus [20]. Despite this, the idea of a womb stably colonized by microbial communities in a healthy pregnancy remains a subject of debate [21]; the correlation observed between fertility and vaginal microbiota could be based on the possible existence of an endometrial microbiota, whose eubiosis, dominated by the genus Lactobacillus and particularly by the species L. crispatus in a similar way to what is observed in cervicovaginal samples, would reduce endometrial inflammatory phenomena, favouring the onset of pregnancy [22,23,24,25].
To our knowledge, the only attempt to positively affect the vaginal microbiota to restore a Lactobacillus-dominated composition by means of a probiotic prior to fertility treatment failed [26]. As a possible explanation, the authors suggested that perhaps the use of L. crispatus strains would have a better chance of working. In fact, the trial was performed using a probiotic product containing strains of L. gasseri and L. rhamnosus. A double-blind, placebo-controlled multicentre trial to evaluate the reproductive outcomes of IVF patients with abnormal vaginal microbiota treated with the likely most investigated strain of L. crispatus (strain CTV-05) is currently ongoing [27]. Since January 2020, we in our department started to use the well-documented M247 strain of L. crispatus in women undergoing IVF [28]. This study is therefore concerned with the retrospective analysis of the results gathered from January 2020 to December 2021. As the aim of our work was to highlight a possible significant role of L. crispatus in favouring pregnancy rates, we have retrospectively compared the results from probiotic treatment with those obtained before its introduction at the U.O.S.D. PMA of Conegliano Hospital (Treviso, Italy).
2. Materials and methods
2.1. The study
This retrospective, controlled, observational and open-label study was carried out at the U.O.S.D. PMA of Conegliano Hospital (Treviso, Italy), registered on https://clinicaltrials.gov./ (identifier: NCT05871242) and approved by the local (Treviso and Belluno) Ethics Committee for Clinical Trials, with approval number 1111 on 5 June 2023. Informed written consent was obtained from all 160 women who took part in the study. The aim of the study was to retrospectively evaluate the role played by the oral administration of a nutraceutical containing as a single active ingredient the probiotic L. crispatus M247 in women undergoing ART procedures. The retrospective analysis of the results obtained with the use of the probiotic strain concerns women (N=80; Probiotic Group) enrolled in our hospital department from January 2020 to December 2021. The retrospective evaluation of the Control Group (N=80;) concerns women enrolled in the same hospital department before January 2020. The primary outcome of our analysis was to evaluate to what extent the oral administration of L. crispatus could affect the rate of positive pregnancy tests, defined as a β-hCG (human chorionic gonadotropin) ≥50 IU/L on day 10 after embryo transfer [29]. Secondary outcomes were the number of live births, and the probiotic tolerability and consequent general wellbeing of the women in the study, which were functional factors to avoid drop out.
As shown in Figure 1, regarding ART procedures, our analysis considered women undergoing a vitrified/warmed cycle, oocytes, embryos at cleavage stage on day-3 (D3) and at blastocyst stage on day-5 (D5) and women undergoing a fresh IVF cycle using either conventional methods or ICSI for fertilization. Regarding the subgroup ‘vitrified/warmed oocytes’, all 26 women (13 of the Probiotic Group and 13 of the Control Group) were fertilized by ICSI; both in the Probiotic Group and in Control Group two women underwent embryo transfer after two days and 11 women had the transfer after three days. Regarding the subgroup ‘vitrified/warmed D3-embryos’, 28 women (14 women of the Probiotic Group and 14 of the Control Group) were fertilized using the ICSI method and six (three of the Probiotic Group and three of the Control Group) were fertilized using conventional IVF methods. Regarding the subgroup ‘vitrified/warmed D5-blastocysts’, 66 women (33 of the Probiotic Group and 33 of the Control Group) were fertilized by ICSI method and eight (four of the Probiotic Group and four of the Control Group) were fertilized by conventional IVF methods. Lastly, 26 women (13 of the Probiotic Group and 13 of the Control Group) underwent fresh embryo transfer. Of these, eight women per group were fertilized by conventional IVF methods and five per group by ICSI. In seven out of 13 per group, embryo transfer was performed on day 3 of embryo development; for the remaining six per group, embryo transfer was performed after five days. Since it was not a routine practice for our department, preimplantation genetic testing for aneuploidies was not conducted on transferred embryos. During the recruitment of all women for this study, the exclusion criteria observed were the presence of submucous uterine myomas and/or uterine malformations.
The following were evaluated for each woman: age, BMI, anamnestic factor of infertility, vaginal-rectal swab prior to ovarian synchronization treatment, antibiotic therapy, endometrial preparation (hormone therapy) and β-hCG. To reduce any possible bias in our retrospective analysis, we compared the results of women who had received the same ovarian synchronization with oestrogen-progestogen for 60 days using the same endometrial preparation technique (oestrogen and subsequently oestrogen and progesterone). The same criteria were used to evaluate the endometrium (trilaminar aspect with a thickness of at least 7 mm) and blood progesterone value (before progesterone administration) not exceeding 1.5 mg. The same medical personnel were involved and used the same type of catheter (for embryo transfer manoeuvre). The same laboratory staff (for vitrification and warming, IVF or ICSI, and embryo transfer) were involved in both studies. In addition, regarding frozen-thawed cycles, we compared women whose oocytes or embryos were cryopreserved using the same vitrification/warmed protocol.
2.2. Embryo culture and vitrification/warming protocol
Embryo culture was conducted in a controlled atmosphere (37°C, 6% CO2 and 5% O2), in petri plates with microdroplets (50 microliter) of Geri® medium (Genea Biomedx, Australia) covered with mineral oil (Oil For Tissue Culture – Fujifilm, Irvine Scientific, Japan). For vitrification, VT801 medium (Kitazato, Japan) or Vitrification Freeze Kit (Fujifilm, Irvine Scientific, Japan) were used. For thawing, VT802 medium (Kitazato, Japan) or Vitrification Thaw Kit (Fujifilm, Irvine Scientific, Japan) were used.
2.3. Probiotic product
The probiotic product used in our clinical study (Crispact®) was formulated in sachets. Each sachet contained not less than 20 billion colony forming units (CFU) of L. crispatus M247 (LMGP-23257) [30]. The product was manufactured by Labomar S.p.A. (Istrana, Treviso, Italy) and traded by Pharmextracta S.p.A. (Pontenure, Piacenza, Italy). The product was notified to the Italian Health Authorities (01 March 2019) with the notification number 115450.
2.4. Statistical analysis
The study sample was assessed using methods of descriptive statistics. The ART procedures (cryopreserved oocytes, D3-embryos, D5-blastocysts, IVF and ICSI), vaginal-rectal swab and endometrial therapy were analyzed using the SAS categorical data analysis (JMP14 software). The probability of a positive pregnancy test was investigated using the multiple logistic regression model and prediction profiles involving the following variables: participant’s response to therapy (pregnancy, no pregnancy), treatment (or not) with the probiotic, age, BMI, vaginal-rectal swab, hormonal therapy. The same variables were employed in a segmentation model (CHAID) to assess relationships with the response variable. Regarding live births, Pearson and Fisher’s exact test and odds ratio were evaluated. The chosen level of significance for all analyses performed was p<0.05. Continuous variables were analyzed using descriptive statistics and multivariate analysis. Nominal or ordinal variables were evaluated using the chi-square technique. All data processing and statistical analysis procedures were performed on a Macintosh iMac computer. All statistical calculation and evaluations are available upon reasonable requests.
3. Results
3.1. Safety
Our retrospective analysis was conducted on 160 infertile women. The mean age of the investigated sample was 37.55 ± 4.79 years (range of age: 21 to 46; median value: 38). Twenty-five percent of all participants were younger than 35 years, 75% did not exceed the age of 41 and 90% were not older than 43 years. The modal ages were: 41 (11.9% of the sample), 35 (10%), 31 (7.5%) and 36 (7.5%). For further details see Supplementary File 1. These 160 women were divided in two groups of 80 women (Figure 1), one group was treated with a probiotic product containing L. crispatus M247 (probiotic group) and the other group was untreated (Control Group). Probiotic treatment was well-tolerated and adverse events were almost superimposable in both groups for type (constipation, flatulence, bloating, gastralgia, nausea, and headache), incidence (9 subjects in the Probiotic Group, 11.25%; 10 subjects in the Control Group, 12.50%), severity (mild and transient), and duration (2 to 3 days each) (data not shown).
3.2. Pregnancy rates
As shown in Table 1, after 90 days of probiotic administration, a positive pregnancy test, defined as a β-hCG (human chorionic gonadotropin) ≥50 IU/L on day 10 after embryo transfer, globally concerned 19 women of the Probiotic Group (23.75%) versus 14 of the Control Group (17.50%). Among the various subgroups, the greatest number, corresponding to almost half of all enrolled women, was seen in women identified as ‘D5-blastocysts’, with a total of 37 subjects per group. In this subgroup, the probiotic treatment group returned 15 positive pregnancy tests from 37 women (40.54% of the sample) while in the Control Group the same outcome was achieved in 8 of 37 women (21.62% of the sample; p=0.0787). The clearest difference concerned women under the age of 40. The pregnancy rate in this age bracket was 13 out of 29 (44.8%) in the Probiotic Group versus 7 out of 29 (24.1%) in the Control Group (p=0.0974). This suggests that age and probiotic treatment positively influence the chances of pregnancy. Indeed, the odds ratio of getting pregnant was 7.45 for a woman aged between 30 and 40 years, independently by treatment, and 1.56 for a woman treated with the strain M247 independently by age (Supplementary File 2; Table 1).
To better understand to what extent parameters such as probiotic treatment and age could influence the global observed pregnancy rate (PR) and also to investigate the role played by BMI in such an outcome, we analysed the role played by these three prediction profilers using the multiple logistic model. For example, considering the Control Group and setting the age and BMI values by default respectively as 20–30 and 22, the PR was 9.9% (Figure 2). When the same settings were used for women in the Probiotic Group, the PR increased to 14.7% (Figure 3). However, in the age range 30–40 years, the impact of probiotic treatment increased and determined a PR of 34.8% (Figure 4). Within the same age range, the impact of the treatment becomes even more evident in women with a BMI progressively increasing to a value of 35. As shown in Figure 5, with these parameters, the PR was 46.6% (versus 35%) with an odds ratio of 2.00.
After analysing the possible role on a positive pregnancy test by the simpler prediction profilers (treatment, age, and BMI), we tried to integrate into our statistical approach the different fertilization and transfer procedures used in our study. Since the segmentation analysis allows an exploration of the relationships between the different variables by progressively dividing the initial sample into groups that are increasingly homogeneous, we used the regression tree model to identify which parameters significantly modify the probabilities of positive pregnancy test. According to our data, the most important predictor in this case was the parameter ‘age’, with a cut-off of 43. This predictor in fact divided the 160 analysed women in two groups characterized by different probabilities of returning a positive pregnancy test. One group, all aged below 43, had an average probability of getting a positive pregnancy test of 25%; a second group, all aged over 43, had a probability of 0.07%. As shown in Table 2, when considering only women below 43 years old, women of the subgroup ‘D5-blastocysts’, treated with the probiotic and having a BMI of at least 18.6, had a 44.5% probability to get a positive pregnancy test (odds ratio: 2.08; p<0.05), while for the women in the Control Group undergoing the same procedure and with same age and BMI, the probability dropped to 28.4%.
Since the women involved in the Control Group were selected from women managed in our hospital department earlier than those actually treated with the probiotic, we have tried to evaluate the rate of comparability between the two groups. The mean ages were not significantly different. In fact, the age of the women of the Probiotic Group was 37.53 ± 5.12; and that of the Control Group was 37.56 ± 4.63 (data not shown). Similarly, regarding BMI, the two groups were not significantly different being 22.14 ± 3.13 and 21.81 ± 3.09 and 17.8–37.3 and 17.51–36.05 the BMI and the BMI ranges of the Probiotic Group and of the Control Group respectively (data not shown). Regarding the ART procedures, vitrified/warmed oocyte or embryos (D3 or D5) or fresh embryos were adopted in a numerically identical manner in the two groups (Figure 1 and Table 3). Similarly, vaginal-rectal swab (Table 4) and antibiotic or antifungal treatment (data not shown), demonstrated no significant differences between the two groups. Regarding hormonal treatment (Table 5), the administration of FSH, LH and menotropins, used prior of vaginal progesterone application in women undergoing ART with fresh embryos, were not significantly different between the two groups. By contrast, in the progesterone route of administration, a significant difference was observed in women undergoing a vitrified/warmed cycle (vaginally applied progesterone was mostly adopted in the Control Group and injected progesterone mostly adopted in the Probiotic Group). However, the Pearson analysis, which was performed to evaluate if these differences could have affected the result, returned a non-significant result (p=0.2059; Supplementary File 3). Regarding the anamnestic factors of infertility (tubaric factor, reduced ovarian reserve, polyabortivity, past failure, male factor, endometriosis and idiopathic factor), these were not significantly different between the two groups and none of these factors significantly correlated with a positive pregnancy test either in the Probiotic or the Control Group (Supplementary File 4).
3.3. Live birth rates
Regarding live births (Table 6), out of 19 clinical pregnancies in the Probiotic Group, 10 women delivered a healthy child (live birth rate: 52.6%) and out of 14 clinical pregnancies in the Control Group, 6 women delivered a healthy child (live birth rate: 42.9%) with an odds ratio of 1.48. Similar results were returned by considering 10 and 6 live births respectively out of 80 women (live birth rate: 12.5% versus 7.5%) with an odds ratio of 1.76.
We then analysed the relationship between the live births in the two groups and the ART applied. As shown in Table 7, out of 10 live births in the Probiotic Group, nine belonged to the subgroup D5-blastocysts versus three out of six in the Control Group. If we consider the number of women in this subgroup, 37 per group, with a live birth rate of 24.3% for the Probiotic Group, versus 8.1% for the Control Group (odds ratio: 3.64; p=0.05) a positive role exerted by the probiotic is indicated. Considering the mother-child dyad, no significant difference between the two groups have been observed concerning the mother’s age and BMI, gestational time, child’s weight and sex, and mode of delivery (data not shown).
Finally, to evaluate the global clinical meaning of our results, we used three statistical indices obtained by using the live birth rates calculated from 80 women per group [31,32,33]. The first is known as NNT (Number Needed to Treat) and it is the estimated number of patients who need to be treated to have one additional patient to benefit (versus control). The second is known as NNH (Number Needed to Harm) and it is the estimated number of patients who need to be treated for one additional patient to experience side effects or adverse events (versus control). The third is known LLH (Likelihood to be Helped or Harmed) and indicates the overall likelihood that a patient may benefit or experience harm from the treatment compared to control. As shown in Figure 6, the indices were respectively: (i) 20 (calculated as 100/5.0, where 5.0 corresponds to the difference between the live birth ratio of the Probiotic Group and the one of the Control Group); (ii) 80 (calculated as 1/11.25-12.50, where 11.25 and 12.50 are the incidences of side effects occurring respectively in the Probiotic and in the Control Group, see text at the beginning of the Results section) and (iii) 4 (calculated as 1/20:1/80), indicating for the probiotic a risk-benefit ratio to the full advantage of the benefits.
4. Discussion
Female causes of infertility include sexually transmitted infections, tuboperitoneal abnormalities, endometriosis, uterine anatomical abnormalities, as well as autoimmune, genetic and endocrine disorders [34,35]. As in some cases the cause of female infertility still remains unknown, a dysbiotic vaginal microbiota, that is a not Lactobacillus dominated or, more precisely, a not L. crispatus dominated, has been proposed as a possible additional factor [36]. ART are the most advanced approach to infertility treatment. Despite their progress, the implantation rate of transferred embryos remains low. Success or failure in ART has been attributed to a woman’s age, weight, endometrial receptivity, embryo quality and to the transfer technique used [37,38]. However, in many cases, the reasons for failure still remain unclear and an imbalanced vaginal microbiota has been proposed as a possible contributing factor. Indeed, a recent study observed that women with CST IV (that is not-Lactobacillus dominated), or with CST III (that is L. iners dominated) or with CST II (L. gasseri dominated), had a lower ART success rate than women with the L. crispatus-predominant vaginal microbiota, that is CST I [39].
To analyse if the treatment with a probiotic containing the species L. crispatus could affect the success of ART, we retrospectively analysed results routinely obtained in our hospital department over two years in which we treated 80 unfertile women with M247 orally, using a well-documented and safe strain of L. crispatus described to be both a gut and a vaginal colonizer and also clinically capable of exerting an anti-HPV role [40,41,42]. Our analysis, performed by comparing two extremely similar groups of women, shows that, independent of the ART procedure adopted, treatment with the strain M247 increased the chance of a positive pregnancy test by 56%. The age and BMI ranges particularly favoured by treatment with the probiotic were 30–40 (years) and 22–35 (kg/cm2), respectively. Within this range of age and with a BMI of 35, treatment with the probiotic increased the chance of a positive pregnancy test by 34%, versus an identical control independent of the ART procedure adopted. Besides age and BMI, the ART procedure adopted also demonstrated a favourable outcome. In fact, a woman subjected to embryo transfer with a D5-blastocysts, below 43 years, with a BMI over 18.6, and treated with the strain M247 had a significantly higher chance of getting a positive pregnancy test, an increase of 66.3% versus an identical control.
While these results seem to demonstrate that the use of L. crispatus M247 may significantly increase the chance of pregnancy, they do not help us to understand exactly why. Of course, our assumption is that the probiotic colonizes the woman’s vaginal environment, enriching and/or restoring an eubiotic (CST I; L. crispatus dominated) vaginal bacterial community. A trial on HPV infected women and a very recent clinical case report have in fact demonstrated the capability of the strain M247 to effectively restore a CST I [40,41]. Moreover, a study performed using a probe to specifically detect the strain M247, has shown that following oral treatment, the strain M247 is indeed found first in the gut and then the vaginal environment of treated volunteers [43].
Being a retrospective analysis of data obtained in our clinical routine, and since the sampling and investigation of the vaginal microbiota is not routinely done either before or after treatment with the probiotic, it is impossible for us to demonstrate this possibility. Undeniably, having data available from which to deduce that the administered strain was capable of colonizing women treated with the probiotic, with particular reference to those in which positive pregnancy test was later demonstrated, allows us to confirm some recent results which have apparently demonstrated a causative and anti-disease role of the species L. crispatus: in the few cases of vaginal microbiota transplantation so far performed, in which CST IV women were transplanted with vaginal secretions from CST I women, the authors clearly demonstrated a shift of CST, from CST IV to CST I, together with the resolution of the ‘problem’, be it an intractable bacterial vaginosis condition or an infertility problem [44,45].
Similarly, the possibility that faecal dysbiosis is a possible contributing cause of female infertility cannot be ruled out. In fact, numerous studies discuss the potential influence of gut microbiota on female fertility [46,47,48]. Some studies have indeed highlighted the role of the M247 strain in counteracting dysbiosis and intestinal inflammation [49,50,51]. It is therefore possible that the strain used in our study played a decisive role in re-establishing a certain intestinal eubiosis. Because the gut microbiota of the enrolled women were not analysed, we do not have the data to demonstrate this.
The analysis of the data obtained clearly indicates that maternal age is decisive in favouring, or not, a pregnancy. It is well recognised that increasing age contributes to difficulties in becoming pregnant. Fertility rates begin to decline gradually at the age of 30, more so at 35, and markedly at 40 [52]. At this age, even with fertility treatments, women have more difficulty getting pregnant or may deliver an abnormal foetus [53]. That said, the range in which the intake of the probiotic strain seems to play a favourable role compared to the control also includes rather ‘elevated’ ages close to 40, in which the success of ART normally tends to fall due to the decline of ovarian reserves, the reduction of oocyte competence and the high increase of embryo aneuploidies [53,54]. Our results could therefore indicate that the clinical effect of the probiotic is more evident in conditions in which age begins to become a discriminating element of failure. Noteworthy is the fact that as age increases, the percentage of women with non-Lactobacillus dominated vaginal microbiota also increases [55]. A similar pattern is seen with BMI. Higher BMI values are certainly not considered to favour pregnancy and higher BMI values has long been considered to be a negative element in ART and in cases of euploid embryo transfer [56,57,58]. Our data seems to show a more pronounced effect from the probiotic in BMI ranges considered unfavourable for pregnancy, such as those above 30. As previously mentioned for age, for BMI there is a certain correlation between weight gain and reduced vaginal eubiosis [16]. It may therefore be that the probiotic influences those categories of women for whom the existence of a dysbiotic vaginal microbiota is described as more probable.
Regarding the ART method adopted, our analysis indicates blastocysts transfer as the method in which the probiotic seems to determine the greatest clinical success. One might wonder whether, as in the case of age and BMI, this procedure is the one favouring the least positive outcome and therefore the one in which the probiotic could show its greatest effects in restoring a correct vaginal eubiosis. However, we can also assume that the effect clearly identified in this subgroup is linked to a numerical issue, to the extent that any other method is so weakly represented in our study demonstrate any possible therapeutic effect.
The number of women enrolled in our analysis is the first among the many limitations of our study. Indeed, in addition to the known limitations of non-prospective, non-randomized and non-blind studies, the results of which have maybe a lower predictive value in general terms, 160 women is perhaps too few in number to distinguish the effect of a probiotic in relation to the different procedures adopted. Having said that, our approach has been focused on obtaining the most controlled data possible, to the best of what can be done in a retrospective study. The analyses have indeed shown us that the two groups are extremely superimposable, both in anthropometric terms and in terms of antibiotic, antifungal and hormonal treatment and that therefore the data obtained with our analysis are of sufficient quality.
In the attempt to understand how comparable the two groups were, we discovered a single difference between the two groups: the method of administration of the progesterone. Progesterone was mainly administered orally in the Control Group and mainly by injection in the probiotic-treated group. Statistical analysis, however, did not show any influence of this difference on the final result. Similarly, our study demonstrated no influence of other parameters such as the vaginal-rectal swab results or the antibiotic and/or antifungal therapy adopted.
A further limitation intrinsic to our retrospective analysis, is the lack of information regarding the ploidy of the implanted embryos. This aspect would have allowed a better interpretation of the results obtained.
Within the framework of the obvious caution necessary when considering the results of non-blind, open-label and retrospective studies, our analysis would seem to show that the administration of L. crispatus during the adoption of ART methods should in any case be considered safe and potentially advantageous to the extent that it would seem to increase the possibility of a positive pregnancy test by about 50%, regardless of age, BMI and procedure adopted. This chance is further increased in women between 30 and 40 years of age and with a BMI greater than 22 and would further increase as the BMI increases, at least up to a value of 35. It is also possible that of all methods, the ART method using a 5-day blastocyst may highlight a greater success for the probiotic. In our study, in women under 43 years of age and with a BMI of at least around 20, this success was found to be significant (p<0.05) with a net doubling of the chances of a positive pregnancy test. Larger, randomized, controlled, prospective, and double-blind studies are urgently needed to confirm the validity of what we have observed.
Of the women in our study who had a positive pregnancy test, we can report 10 and 6 live births from a total of 19 and 14 women in the Probiotic Group and Control Group respectively. Despite the fact that these results are non-significant, the calculation of the odds ratio demonstrated an increase (by about 50 and 80% according to the number of women considered, see Table 6) in the possibility of giving birth to a healthy child for women treated with the probiotic compared to women in the Control Group.
When evaluating exclusively the number of live births in relation to the ART method adopted, it appeared evident that the transfer of blastocysts was the one in which the effect of the probiotic was most evident with the number of live births three times higher than that observed in controls. Blastocyst transfer is considered the method most capable of replicating the physiology of the natural intrauterine implant. It is therefore possible that in these conditions, the recovery of a vaginal eubiosis, an element that we hypothesize could have occurred as a consequence of the treatment with the probiotic, could have a particularly relevant positive impact for procreative purposes.
Finally, using specific statistical indices capable of extrapolating the risk-benefit ratio deriving from treating, or not, a woman with the L. crispatus M247 strain, we have observed (i) a NNT value indicating that few patients need to be treated to achieve positive results; (ii) a NNH value suggesting that the treatment is less likely to cause harm compared to control; and (iii) a LLH value showing a higher likelihood of benefits compared to harms associated with the treatment. Taken together, these results indicate that there is a good overall probability that women undergoing ART may benefit from oral treatment with L. crispatus M247.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
AB conceived the study. FDP, AB and GF wrote the paper. FS, MC, LR, MP, VDP, LF, DM, SD, SS performed experiments. FDP, AB, LG, NZ, MR, AB and MC analysed data. All Authors revised the manuscript before submission.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Data Availability Statement
Clinical Trial Registration: www.clinicaltrials.gov; identifier NCT05871242.
Acknowledgments
The Authors would like to thank Donna McCormack for editing and correcting the text in English.
Conflicts of Interest
FDP is a board member of Pharmextracta. AB and MC are Pharmextracta consultants. The other Authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
References
- Buhl Borgstrøm MB, Ahrendt Bjerregaard A, Olsen SF, Gabrielsen A, Humaidan P, Kesmodel US. Food & Fertility Study: study protocol for a Danish multicentre prospective cohort study investigating the association between food intake and semen quality, pregnancy and birth outcomes in infertile women and men. BMJ Open. 2023, 13, e068354. [Google Scholar]
- Boivin J, Bunting L, Collins JA, Nygren KG. International estimates of infertility prevalence and treatment-seeking: potential need and demand for infertility medical care. Hum Reprod. 2007, 22, 1506–1512. [Google Scholar] [CrossRef] [PubMed]
- Ombelet W, Cooke I, Dyer S, Serour G, Devroey P. Infertility and the provision of infertility medical services in developing countries. Hum Reprod Update. 2008, 14, 605–621. [Google Scholar] [CrossRef] [PubMed]
- Pinborg, A. Short- and long-term outcomes in children born after assisted reproductive technology. BJOG. 2019, 126, 145–148. [Google Scholar] [CrossRef]
- Becker G, Castrillo M, Jackson R, Nachtigall RD. Infertility among low-income Latinos. Fertil Steril. 2006, 85, 882–887. [Google Scholar] [CrossRef]
- Hull MG, Cahill DJ. Female infertility. Endocrinol Metab Clin North Am. 1998, 27, 851–876. [Google Scholar] [CrossRef]
- Mori R, Hayakawa T, Hirayama M, Ozawa F, Yoshihara H, Goto S, et al. Cervicovaginal microbiome in patients with recurrent pregnancy loss. J Reprod Immunol. 2023, 157, 103944. [Google Scholar] [CrossRef]
- Ravel J, Gajer P, Abdo Z, Schneider GM, Koenig SS, McCulle SL, et al. Vaginal microbiome of reproductive-age women. Proc Natl Acad Sci U S A. 2011, 108 (Suppl. 1), 4680–4687. [Google Scholar] [CrossRef]
- Greenbaum S, Greenbaum G, Moran-Gilad J, Weintraub AY. Ecological dynamics of the vaginal microbiome in relation to health and disease. Am J Obstet Gynecol. 2019, 220, 324–335. [Google Scholar] [CrossRef]
- Hong X, Ma J, Yin J, Fang S, Geng J, Zhao H, et al. The association between vaginal microbiota and female infertility: a systematic review and meta-analysis. Arch Gynecol Obstet. 2020, 302, 569–578. [Google Scholar] [CrossRef]
- Hong X, Zhao J, Yin J, Zhao F, Wang W, Ding X, et al. The association between the pre-pregnancy vaginal microbiome and time-to-pregnancy: a Chinese pregnancy-planning cohort study. BMC Med. 2022, 20, 246. [Google Scholar]
- Hoeger KM, Dokras A, Piltonen T. Update on PCOS: Consequences, Challenges, and Guiding Treatment. J Clin Endocrinol Metab. 2021, 106, e1071–e1083. [Google Scholar] [CrossRef] [PubMed]
- Silvestris E, de Pergola G, Rosania R, Loverro G. Obesity as disruptor of the female fertility. Reprod Biol Endocrinol. 2019, 16, 22. [Google Scholar]
- Gu Y, Zhou G, Zhou F, Li Y, Wu Q, He H, et al. Gut and Vaginal Microbiomes in PCOS: Implications for Women’s Health. Front Endocrinol (Lausanne). 2022, 13, 808508. [Google Scholar] [CrossRef] [PubMed]
- Hong X, Qin P, Huang K, Ding X, Ma J, Xuan Y, et al. Association between polycystic ovary syndrome and the vaginal microbiome: A case-control study. Clin Endocrinol (Oxf). 2020, 93, 52–60. [Google Scholar] [CrossRef]
- Oh HY, Seo SS, Kong JS, Lee JK, Kim MK. Association between Obesity and Cervical Microflora Dominated by Lactobacillus iners in Korean Women. J Clin Microbiol. 2015, 53, 3304–3309. [Google Scholar] [CrossRef]
- Singer M, Borg M, Ouburg S, Morré SA. The relation of the vaginal microbiota to early pregnancy development during in vitro fertilization treatment-A meta-analysis. J Gynecol Obstet Hum Reprod. 2019, 48, 223–229. [Google Scholar] [CrossRef]
- Vergaro P, Tiscornia G, Barragán M, García D, Rodriguez A, Santaló J, et al. Vaginal microbiota profile at the time of embryo transfer does not affect live birth rate in IVF cycles with donated oocytes. Reprod Biomed Online. 2019, 38, 883–891. [Google Scholar] [CrossRef]
- Fu M, Zhang X, Liang Y, Lin S, Qian W, Fan S. Alterations in Vaginal Microbiota and Associated Metabolome in Women with Recurrent Implantation Failure. mBio. 2020, 11, e03242–19. [Google Scholar]
- Amato V, Papaleo E, Pasciuta R, Viganò P, Ferrarese R, Clementi N, et al. Differential Composition of Vaginal Microbiome, but Not of Seminal Microbiome, Is Associated With Successful Intrauterine Insemination in Couples With Idiopathic Infertility: A Prospective Observational Study. Open Forum Infect Dis. 2019, 7, ofz525. [Google Scholar]
- Kennedy KM, de Goffau MC, Perez-Muñoz ME, Arrieta MC, Bäckhed F, Bork P, et al. Questioning the fetal microbiome illustrates pitfalls of low-biomass microbial studies. Nature. 2023, 613, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Moreno I, Simon C. Deciphering the effect of reproductive tract microbiota on human reproduction. Reprod Med Biol. 2018, 18, 40–50. [Google Scholar]
- Moreno I, Garcia-Grau I, Perez-Villaroya D, Gonzalez-Monfort M, Bahçeci M, Barrionuevo MJ, et al. Endometrial microbiota composition is associated with reproductive outcome in infertile patients. Microbiome. 2022, 10, 1. [Google Scholar]
- Toson B, Simon C, Moreno I. The Endometrial Microbiome and Its Impact on Human Conception. Int J Mol Sci. 2022, 23, 485. [Google Scholar] [CrossRef] [PubMed]
- Peuranpää P, Holster T, Saqib S, Kalliala I, Tiitinen A, Salonen A, et al. Female reproductive tract microbiota and recurrent pregnancy loss: a nested case-control study. Reprod Biomed Online. 2022, 45, 1021–1031. [Google Scholar] [CrossRef]
- Jepsen IE, Saxtorph MH, Englund ALM, Petersen KB, Wissing MLM, Hviid TVF, et al. Probiotic treatment with specific lactobacilli does not improve an unfavorable vaginal microbiota prior to fertility treatment-A randomized, double-blinded, placebo-controlled trial. Front Endocrinol (Lausanne). 2022, 13, 1057022. [Google Scholar] [CrossRef]
- Haahr T, Freiesleben NC, Pinborg A, Nielsen HS, Hartvig V, Mikkelsen AL, et al. Effect of clindamycin and a live biotherapeutic on the reproductive outcomes of IVF patients with abnormal vaginal microbiota: protocol for a double-blind, placebo-controlled multicentre trial. BMJ Open. 2020, 10, e035866. [Google Scholar] [CrossRef]
- Bertuccioli A, Cardinali M, Zonzini G, Cazzaniga M, Di Pierro F. Lactobacillus crispatus M247: Characteristics of a Precision Probiotic Instrument for Gynecological and Urinary Well-Being. Microbiology Research. 2022, 13, 963–971. [Google Scholar] [CrossRef]
- Fan J, Wang M, Wang C, Cao Y. Advances in human chorionic gonadotropin detection technologies: a review. Bioanalysis. 2017, 9, 1509–1529. [Google Scholar] [CrossRef]
- Di Pierro F, Polzonetti V, Patrone V, Morelli L. Microbiological Assessment of the Quality of Some Commercial Products Marketed as Lactobacillus crispatus-Containing Probiotic Dietary Supplements. Microorganisms. 2019, 7, 524. [Google Scholar] [CrossRef]
- Altman, DG. Confidence intervals for the number needed to treat. BMJ. 1998, 317, 1309–1312. [Google Scholar] [CrossRef] [PubMed]
- Friedman, JH. Number needed to treat (NNT); number needed to harm (NNH). Med Health R I. 2012, 95, 2–3. [Google Scholar] [PubMed]
- Andrade, C. Likelihood of Being Helped or Harmed as a Measure of Clinical Outcomes in Psychopharmacology. J Clin Psychiatry. 2017, 78, e73–e75. [Google Scholar] [CrossRef]
- Deyhoul N, Mohamaddoost T, Hosseini M. Infertility-related risk factors: a systematic review. Int J Women’s Health Reprod Sci. 2017, 5, 24–29. [Google Scholar] [CrossRef]
- Haller-Kikkatalo K, Salumets A, Uibo R. Review on autoimmune reactions in female infertility: antibodies to follicle stimulating hormone. Clin Dev Immunol. 2012, 2012, 762541. [Google Scholar]
- Ravel J, Moreno I, Simón C. Bacterial vaginosis and its association with infertility, endometritis, and pelvic inflammatory disease. Am J Obstet Gynecol. 2021, 224, 251–257. [Google Scholar] [CrossRef]
- Farquhar C, Marjoribanks J. Assisted reproductive technology: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2018, 8, CD010537. [Google Scholar]
- Korrovits P, Lapp E, Mändar R. Couple-related factors of ART outcome. Clin Exp Obstet Gynecol. 2016, 43, 747–750. [Google Scholar] [CrossRef]
- Koort K, Sõsa K, Türk S, Lapp E, Talving E, Karits P, et al. Lactobacillus crispatus-dominated vaginal microbiome and Acinetobacter-dominated seminal microbiome support beneficial ART outcome. Acta Obstet Gynecol Scand. 2023, 102, 921–934. [Google Scholar] [CrossRef]
- Di Pierro F, Bertuccioli A, Cazzaniga M, Zerbinati N, Guasti L. A clinical report highlighting some factors influencing successful vaginal colonization with probiotic Lactobacillus crispatus. A clinical report highlighting some factors influencing successful vaginal colonization with probiotic Lactobacillus crispatus. Minerva Medica 2023, 114. [Google Scholar]
- Di Pierro F, Criscuolo AA, Dei Giudici A, Senatori R, Sesti F, Ciotti M, Piccione E. Oral administration of Lactobacillus crispatus M247 to papillomavirus-infected women: results of a preliminary, uncontrolled, open trial. Minerva Obstet Gynecol. 2021, 73, 621–631. [Google Scholar]
- Dellino M, Cascardi E, Laganà AS, Di Vagno G, Malvasi A, Zaccaro R, et al. Lactobacillus crispatus M247 oral administration: Is it really an effective strategy in the management of papillomavirus-infected women? Infect Agent Cancer. 2022, 17, 53.
- Di Pierro F, Bertuccioli A, Cattivelli D, Soldi S, Elli M. Lactobacillus crispatus M247: A possible tool to counteract CST IV. Nutrafoods. 2018, 17, 169–172.
- Lev-Sagie A, Goldman-Wohl D, Cohen Y, Dori-Bachash M, Leshem A, Mor U, et al. Vaginal microbiome transplantation in women with intractable bacterial vaginosis. Nat Med. 2019, 25, 1500–1504. [Google Scholar] [CrossRef] [PubMed]
- Wrønding T, Vomstein K, Bosma EF, Mortensen B, Westh H, Heintz JE, et al. Antibiotic-free vaginal microbiota transplant with donor engraftment, dysbiosis resolution and live birth after recurrent pregnancy loss: a proof-of-concept case study. eClinicalMedicine. 2023, 2023, 102070. [Google Scholar]
- Chadchan SB, Singh V, Kommagani R. Female reproductive dysfunctions and the gut microbiota. J Mol Endocrinol. 2022, 69, R81–R94. [Google Scholar] [CrossRef]
- Jiang I, Yong PJ, Allaire C, Bedaiwy MA. Intricate Connections between the Microbiota and Endometriosis. Int J Mol Sci. 2021, 22, 5644. [Google Scholar] [CrossRef]
- Salliss ME, Farland LV, Mahnert ND, Herbst-Kralovetz MM. The role of gut and genital microbiota and the estrobolome in endometriosis, infertility and chronic pelvic pain. Hum Reprod Update. 2021, 28, 92–131. [Google Scholar] [CrossRef]
- Voltan S, Martines D, Elli M, Brun P, Longo S, Porzionato A, et al. Lactobacillus crispatus M247-derived H2O2 acts as a signal transducing molecule activating peroxisome proliferator activated receptor-gamma in the intestinal mucosa. Gastroenterology. 2008, 135, 1216–1227. [Google Scholar] [CrossRef]
- Castagliuolo I, Galeazzi F, Ferrari S, Elli M, Brun P, Cavaggioni A, et al. Beneficial effect of auto-aggregating Lactobacillus crispatus on experimentally induced colitis in mice. FEMS Immunol Med Microbiol. 2005, 43, 197–204. [Google Scholar] [CrossRef]
- Voltan S, Castagliuolo I, Elli M, Longo S, Brun P, D’Incà R, et al. Aggregating phenotype in Lactobacillus crispatus determines intestinal colonization and TLR2 and TLR4 modulation in murine colonic mucosa. Clin Vaccine Immunol. 2007, 14, 1138–1148. [Google Scholar] [CrossRef] [PubMed]
- Pantazis A, Clark SJ. A parsimonious characterization of change in global age-specific and total fertility rates. PLoS One. 2018, 13, e0190574. [Google Scholar]
- Liu K, Case A, Reproductive Endocrinology And Infertility Committee. Advanced reproductive age and fertility. J Obstet Gynaecol Can. 2011, 33, 1165–1175. [Google Scholar] [CrossRef] [PubMed]
- Cimadomo D, Fabozzi G, Vaiarelli A, Ubaldi N, Ubaldi FM, Rienzi L. Impact of Maternal Age on Oocyte and Embryo Competence. Front Endocrinol (Lausanne). 2018, 9, 327. [Google Scholar] [CrossRef] [PubMed]
- Curtiss N, Balachandran A, Krska L, Peppiatt-Wildman C, Wildman S, Duckett J. Age, menopausal status and the bladder microbiome. Eur J Obstet Gynecol Reprod Biol. 2018, 228, 126–129. [Google Scholar] [CrossRef]
- Satpathy HK, Fleming A, Frey D, Barsoom M, Satpathy C, Khandalavala J. Maternal obesity and pregnancy. Postgrad Med. 2008, 120, E01–E09. [Google Scholar]
- Sermondade N, Huberlant S, Bourhis-Lefebvre V, Arbo E, Gallot V, Colombani M, et al. Female obesity is negatively associated with live birth rate following IVF: a systematic review and meta-analysis. Hum Reprod Update. 2019, 25, 439–451. [Google Scholar] [CrossRef]
- Fabozzi G, Cimadomo D, Allori M, Vaiarelli A, Colamaria S, Argento C, et al. Maternal body mass index associates with blastocyst euploidy and live birth rates: the tip of an iceberg? Reprod Biomed Online. 2021, 43, 645–654. [Google Scholar] [CrossRef]
Figure 1.
Representative diagram of the various groups and subgroups retrospectively analysed in the study. V/W: Vitrified/warmed; IVF: in vitro fertilization; ICSI (intracytoplasmic sperm injection); D3: day-3; D5: day-5.
Figure 1.
Representative diagram of the various groups and subgroups retrospectively analysed in the study. V/W: Vitrified/warmed; IVF: in vitro fertilization; ICSI (intracytoplasmic sperm injection); D3: day-3; D5: day-5.
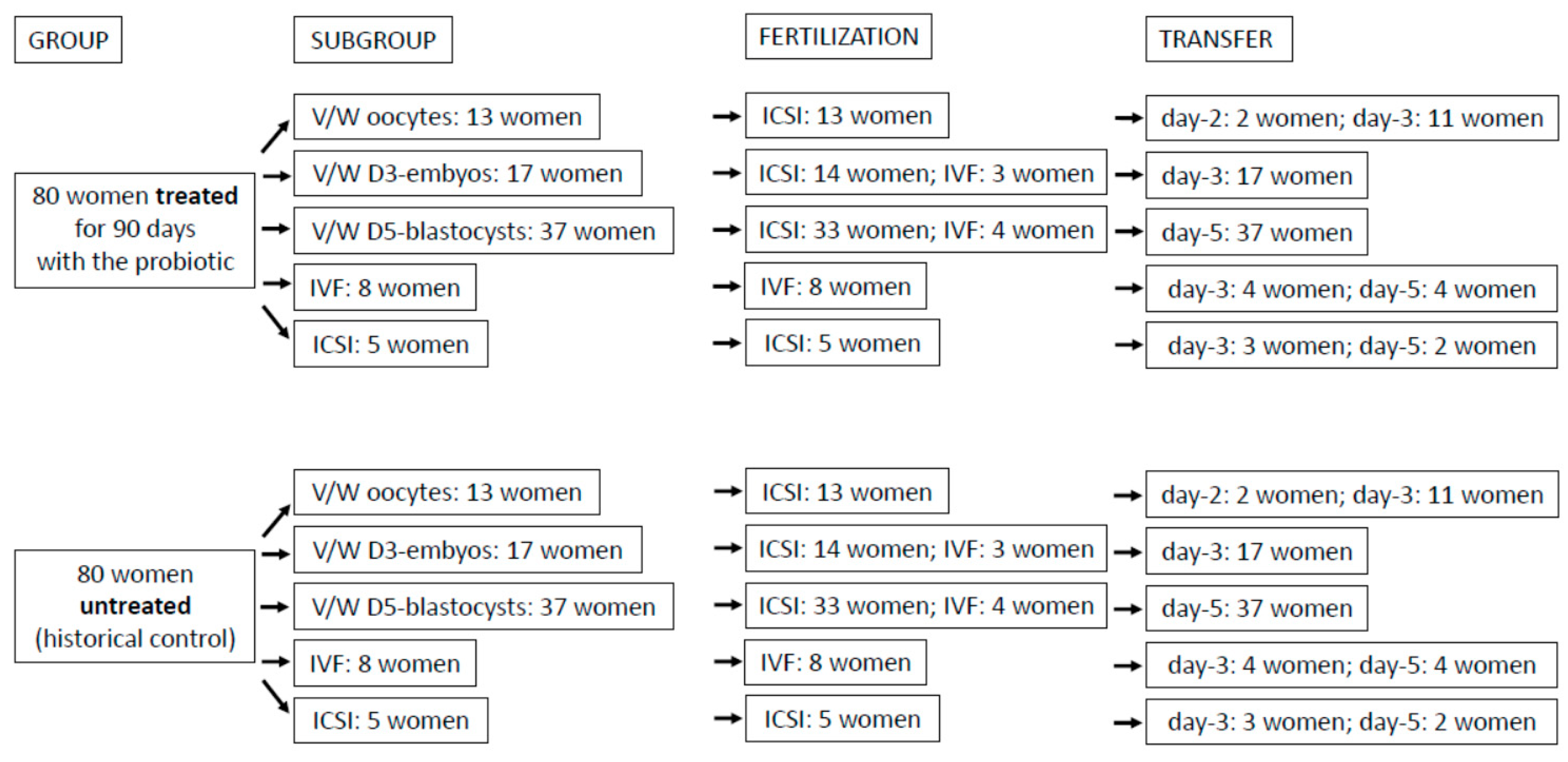
Figure 2.
Multiple logistic model approach to evaluate the role of probiotic treatment, age, and BMI on pregnancy rate. Setting the age and BMI values respectively as 20-30 and 22, the pregnancy rate of the control group is 9.9%.
Figure 2.
Multiple logistic model approach to evaluate the role of probiotic treatment, age, and BMI on pregnancy rate. Setting the age and BMI values respectively as 20-30 and 22, the pregnancy rate of the control group is 9.9%.
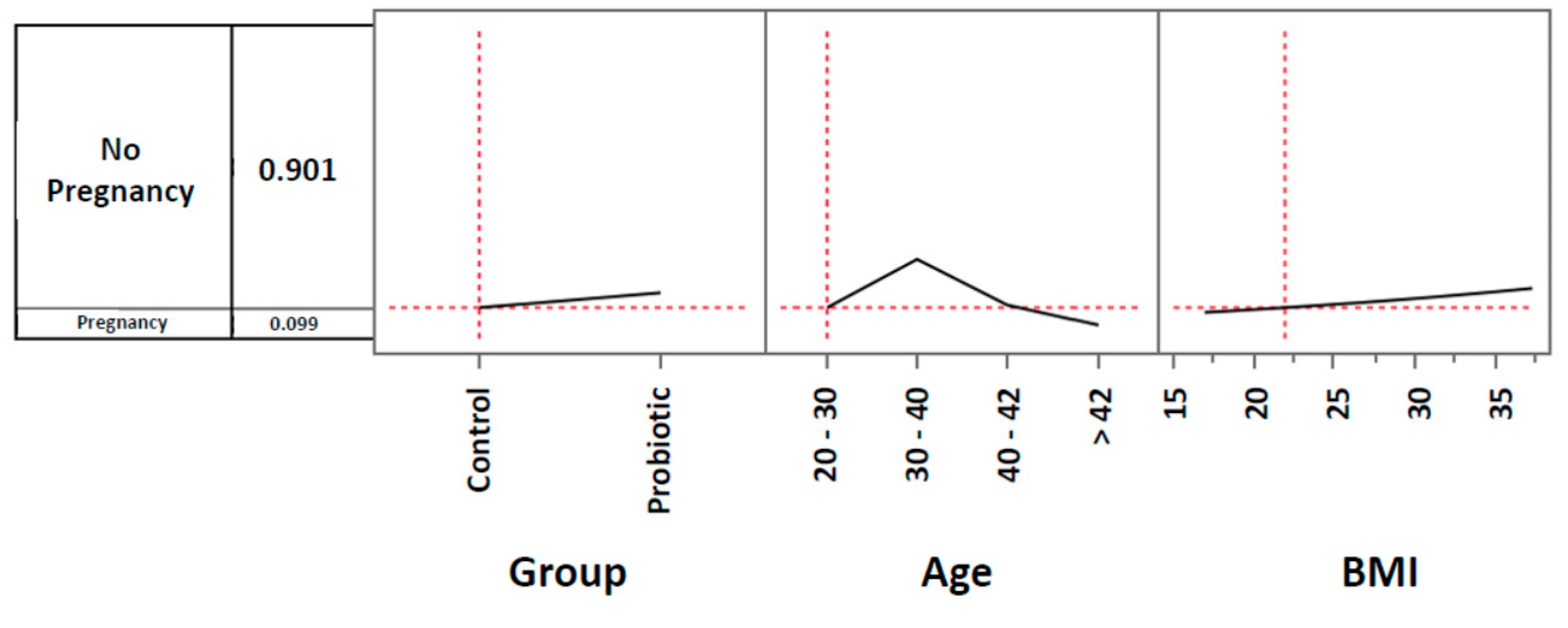
Figure 3.
Multiple logistic model approach to evaluate the role of probiotic treatment, age and BMI on pregnancy rate. Setting the age and BMI values respectively as 20-30 and 22, the pregnancy rate of the probiotic group is 14.7%.
Figure 3.
Multiple logistic model approach to evaluate the role of probiotic treatment, age and BMI on pregnancy rate. Setting the age and BMI values respectively as 20-30 and 22, the pregnancy rate of the probiotic group is 14.7%.
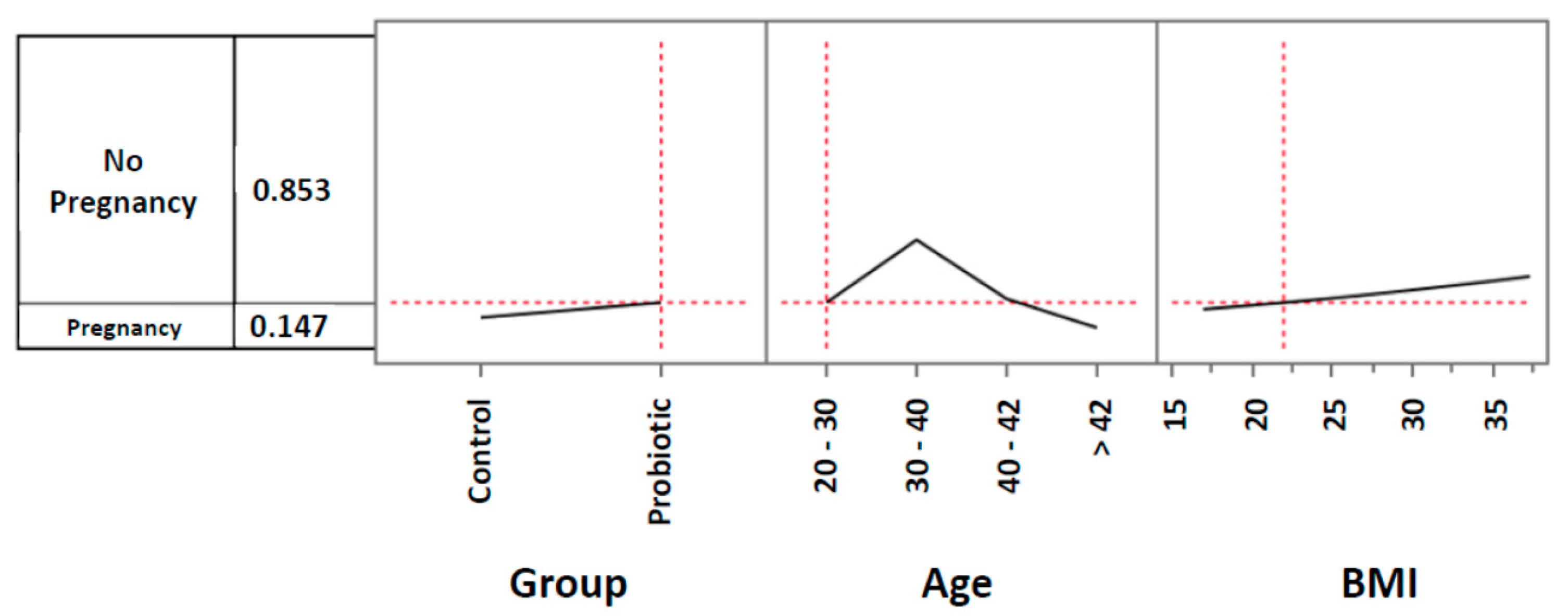
Figure 4.
Multiple logistic model approach to evaluate the role of probiotic treatment, age and BMI on pregnancy rate. In the 30–40-year age range the impact of probiotic treatment increases and determines a pregnancy rate of 34.8%.
Figure 4.
Multiple logistic model approach to evaluate the role of probiotic treatment, age and BMI on pregnancy rate. In the 30–40-year age range the impact of probiotic treatment increases and determines a pregnancy rate of 34.8%.
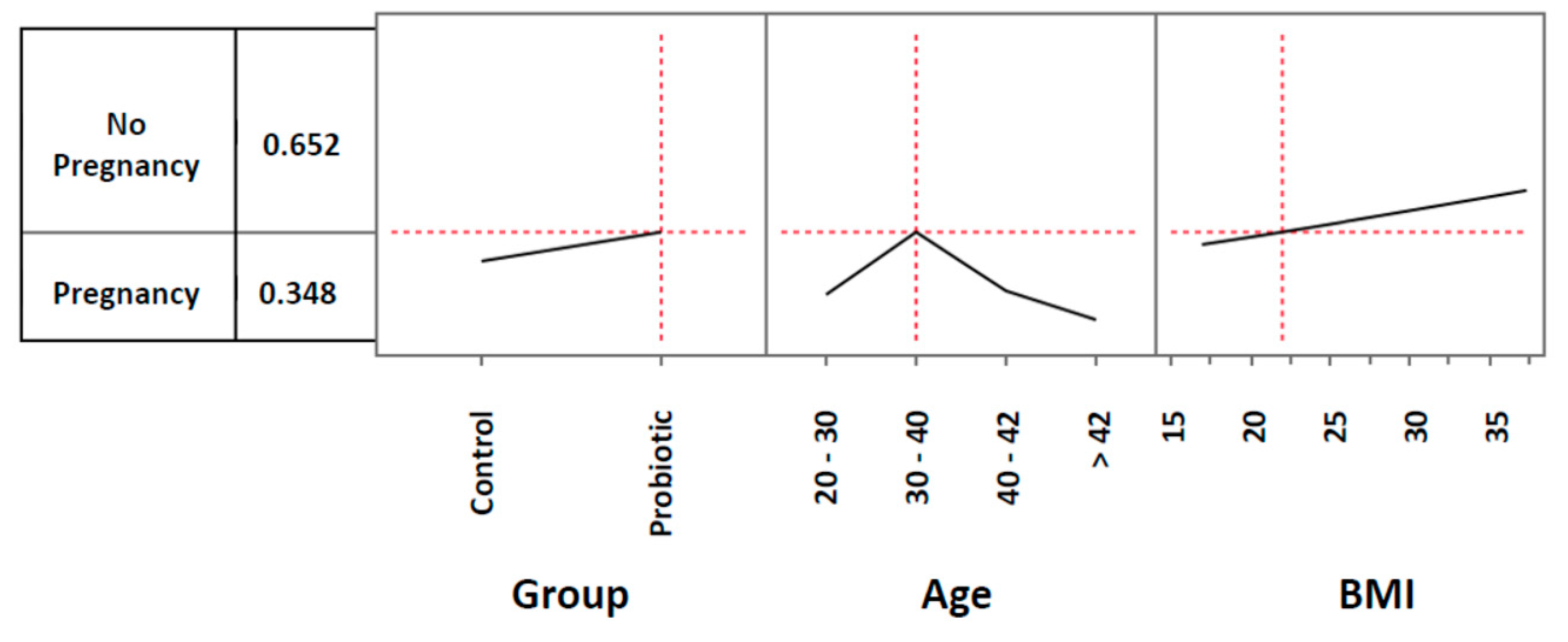
Figure 5.
Multiple logistic model approach to evaluate the role of probiotic treatment, age and BMI on pregnancy rate. In the 30–40-year age range, the impact of the treatment becomes even more evident when considering women with a BMI progressively increasing to a value of 35. With these parameters, the pregnancy rate increases to 46.6%. *Odds ratio: 2.00 (lower 95%: 0.789284; upper 95%: 5.451833).
Figure 5.
Multiple logistic model approach to evaluate the role of probiotic treatment, age and BMI on pregnancy rate. In the 30–40-year age range, the impact of the treatment becomes even more evident when considering women with a BMI progressively increasing to a value of 35. With these parameters, the pregnancy rate increases to 46.6%. *Odds ratio: 2.00 (lower 95%: 0.789284; upper 95%: 5.451833).
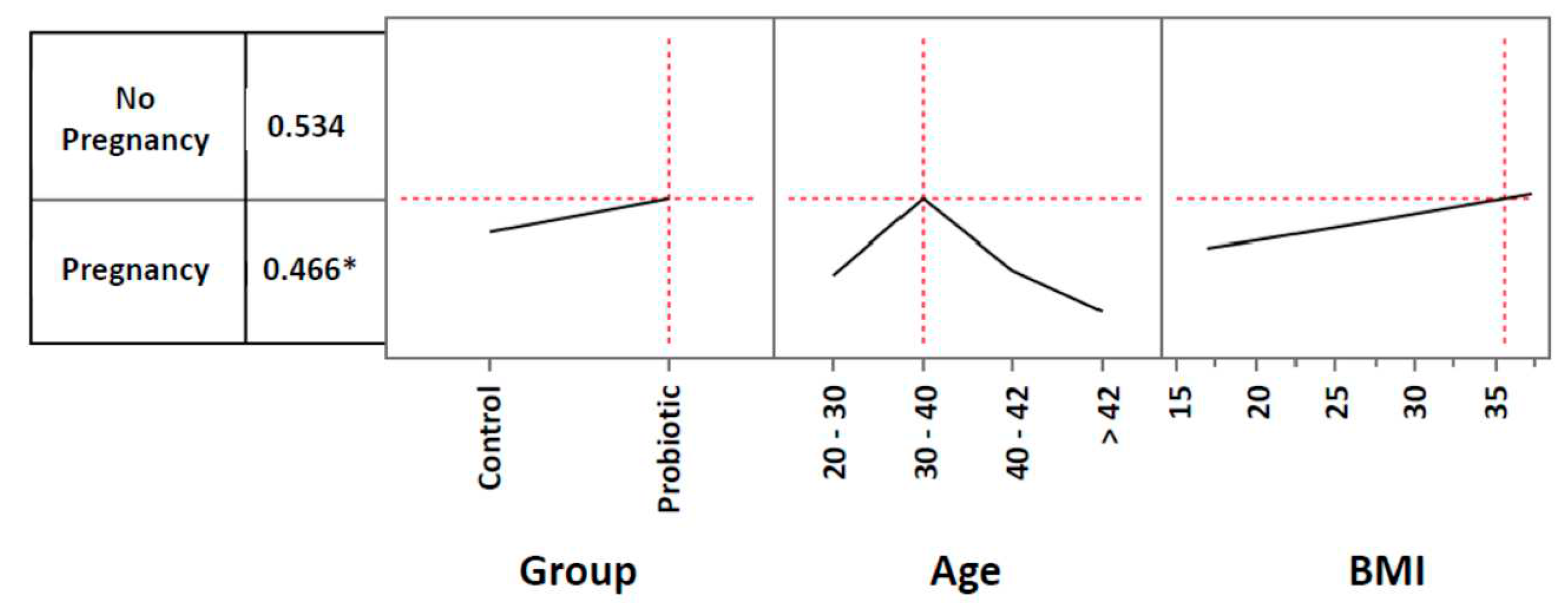
Figure 6.
NNT (Number Needed to Treat), NNH (Number Needed to Harm) and LLH (Likelihood to be Helped or Harmed). The indices are respectively: 20 (calculated as 100/5.0, where 5.0 corresponds to the difference between the LB ratio of the Probiotic Group and the one of the Control Group); 80 (calculated as 1/11.25-12.50, where 11.25 and 12.50 are the incidences of side effects occurring respectively in the Probiotic and in the Control Group) and 4 (calculated as 1/20:1/80).
Figure 6.
NNT (Number Needed to Treat), NNH (Number Needed to Harm) and LLH (Likelihood to be Helped or Harmed). The indices are respectively: 20 (calculated as 100/5.0, where 5.0 corresponds to the difference between the LB ratio of the Probiotic Group and the one of the Control Group); 80 (calculated as 1/11.25-12.50, where 11.25 and 12.50 are the incidences of side effects occurring respectively in the Probiotic and in the Control Group) and 4 (calculated as 1/20:1/80).
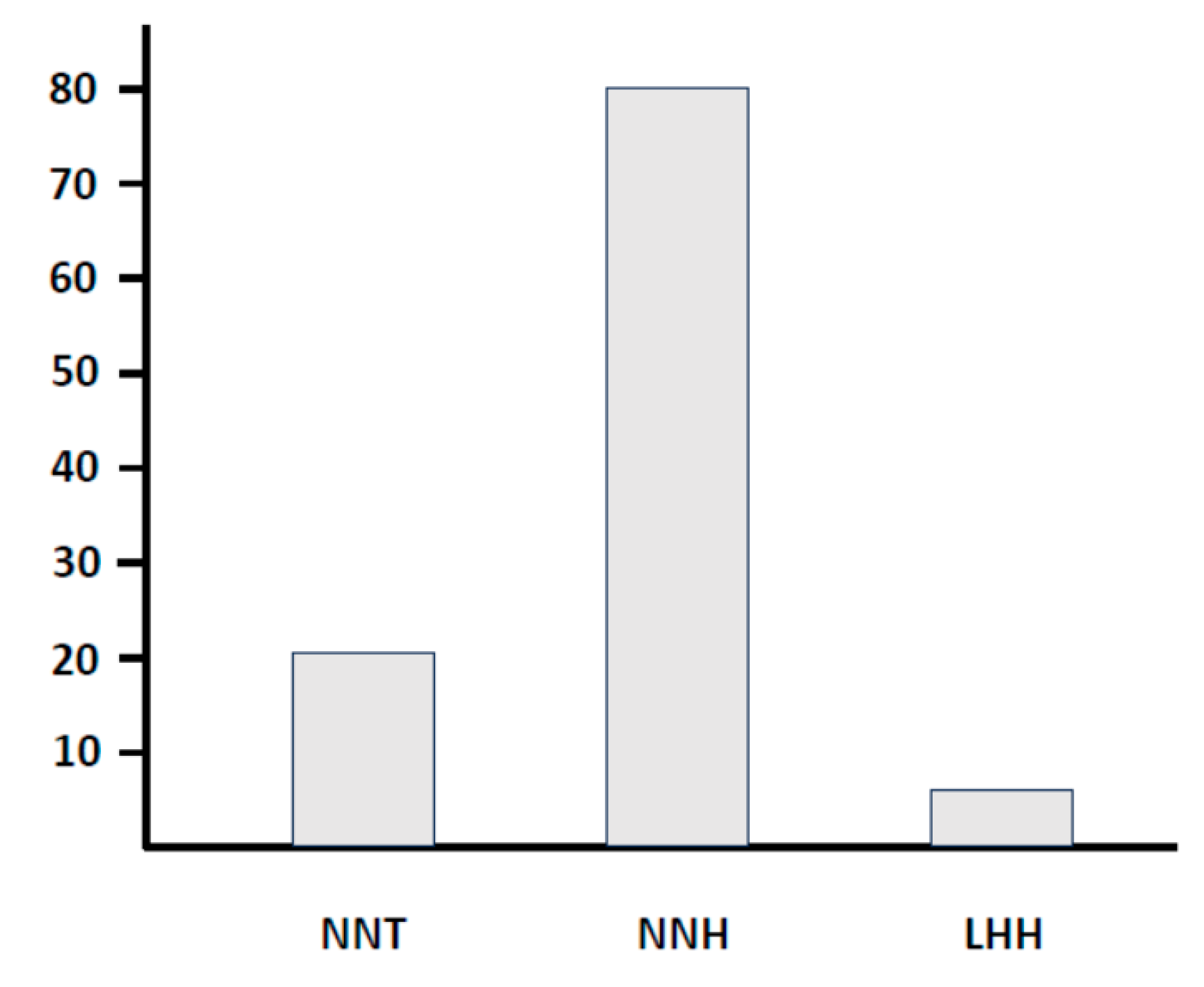

Table 1.
Pregnancy rates observed in all subgroups after 90 days, defined by procedure and age.
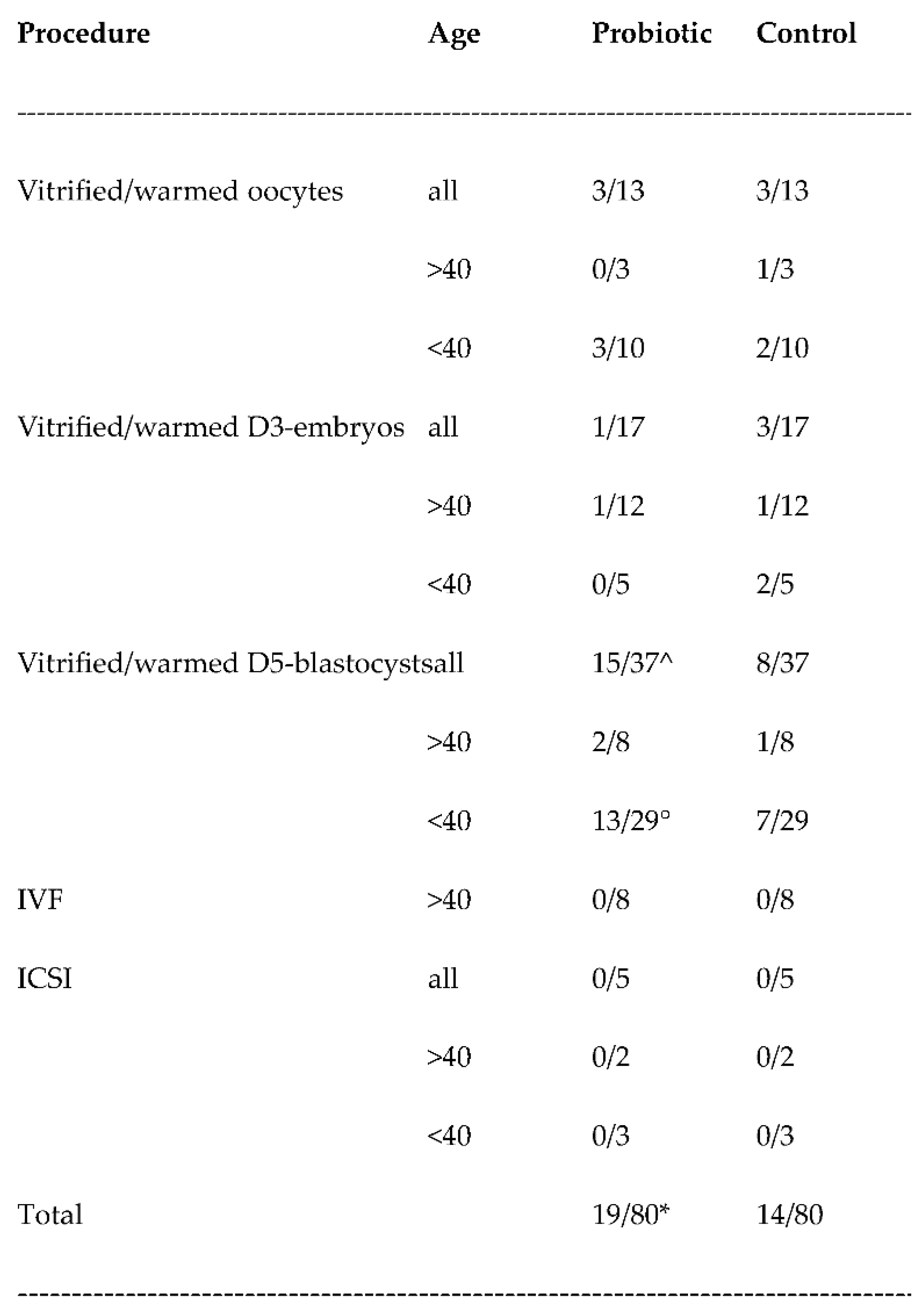
Age is expressed in years. Numbers refers to the number of women of each subgroup. IVF: In vitro fertilization. ICSI: Intracytoplasmic sperm injection. *Odds ratio: 1.56 (lower 95%: 0.6976; upper 95%: 3.4953); ^p=0.0787; °p=0.0974.
Table 2.
Probability of getting a positive pregnancy test according to the regression tree model.
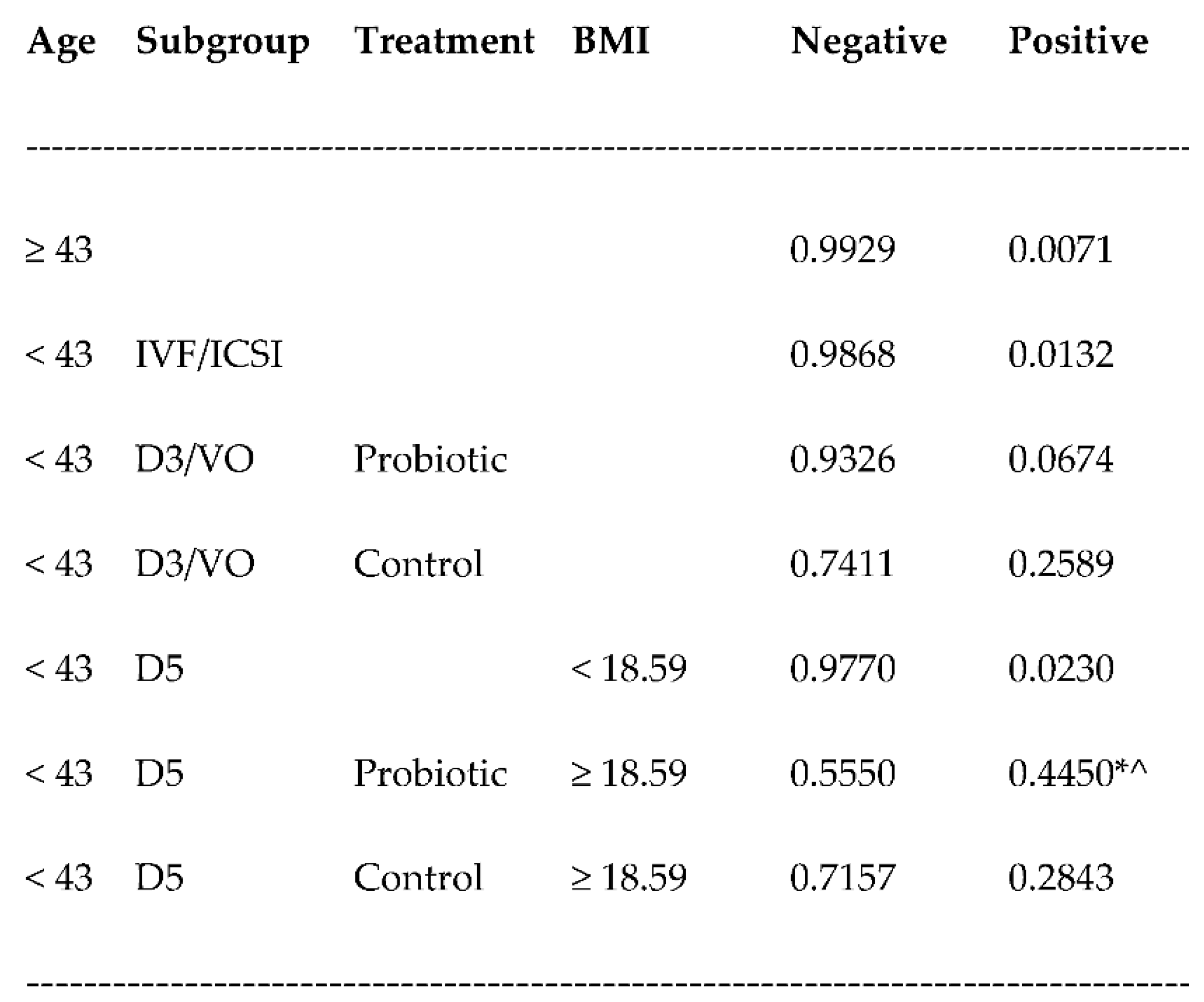
Age is expressed in years. Numbers refers to the probability of having a pregnancy (Positive) or not having it (Negative). IVF: In vitro fertilization. ICSI: Intracytoplasmic sperm injection. D3: day-3 embryos. VO: vitrified oocytes. D5: day-5 blastocysts. *Odd ratio: 2.08 (lower 95%: 0.779193; upper 95%: 5.552413;). ^p<0.05.
Table 3.
Assisted reproductive technology (ART) procedures adopted in the two groups.
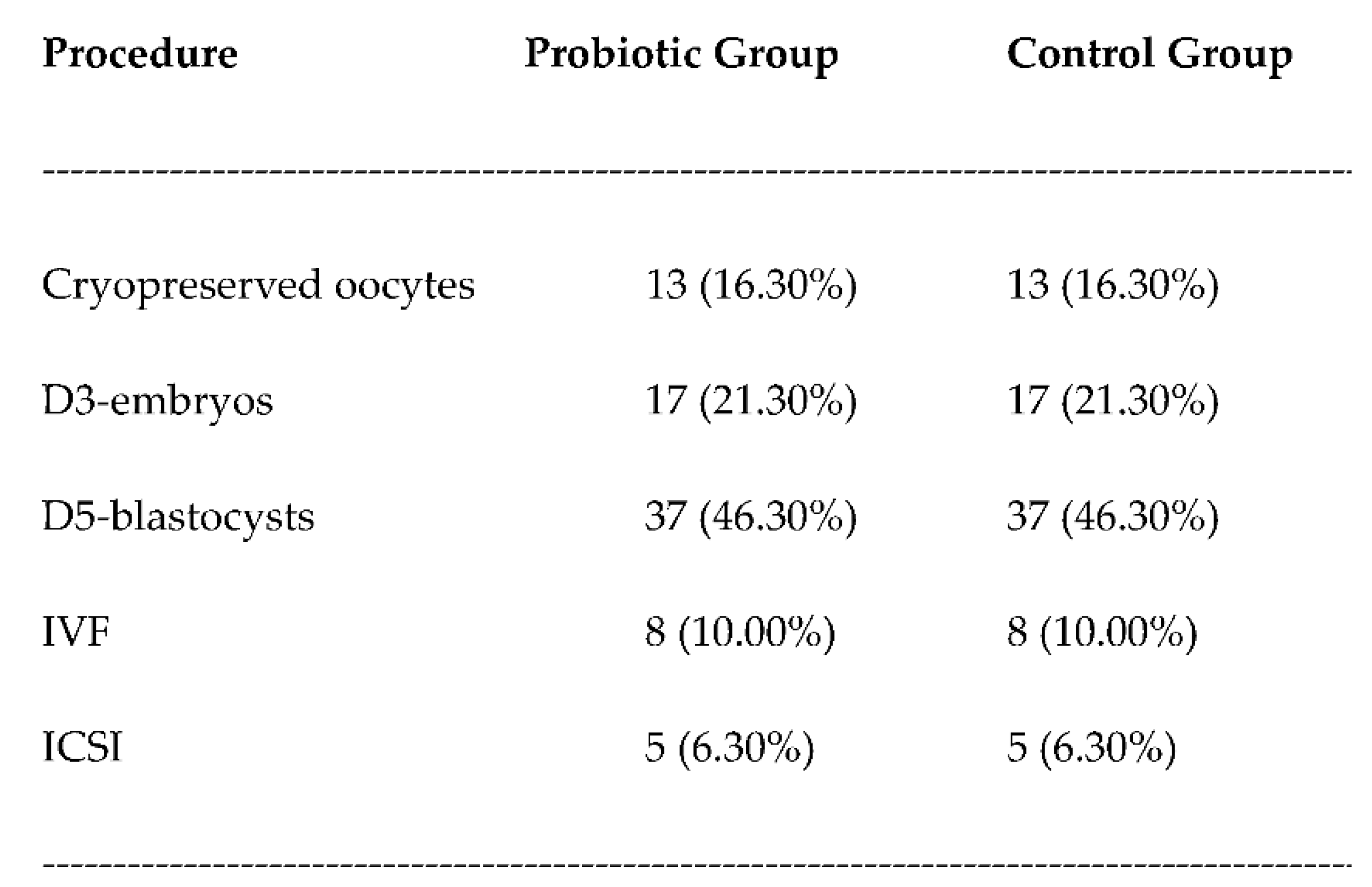
Numbers refers to the number of women of each group. In brackets the percentage values. IVF: In vitro fertilization. ICSI: Intracytoplasmic sperm injection.
Table 4.
Vaginal-rectal swab result in the two groups.
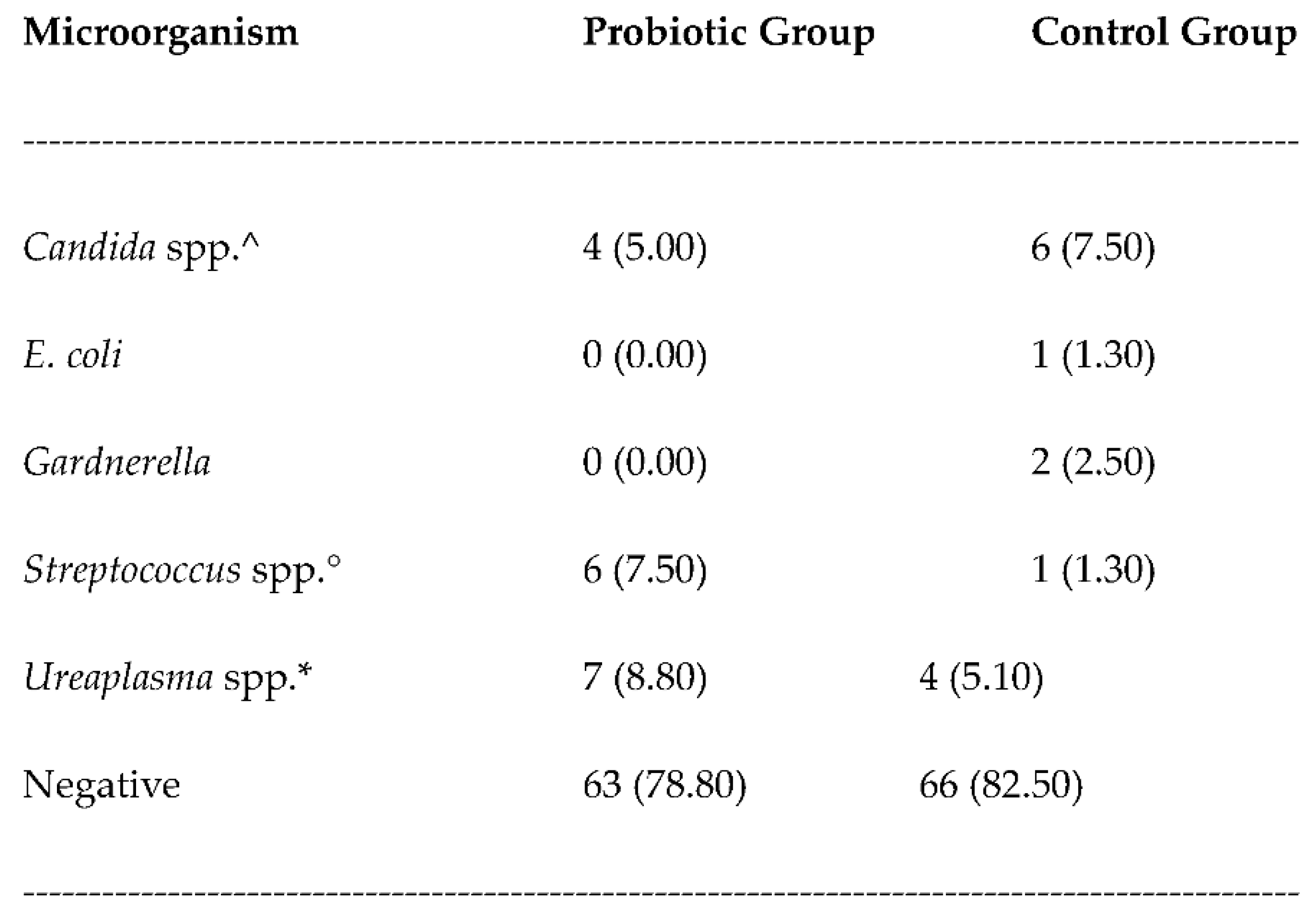
Numbers refers to the number of women of each group. In brackets the percentage values. ^C. albicans; C. glabrata. °S. agalactiae; S. pyogenes. *U. parvum, U. urealyticum.
Table 5.
Hormonal treatments adopted in the two groups.
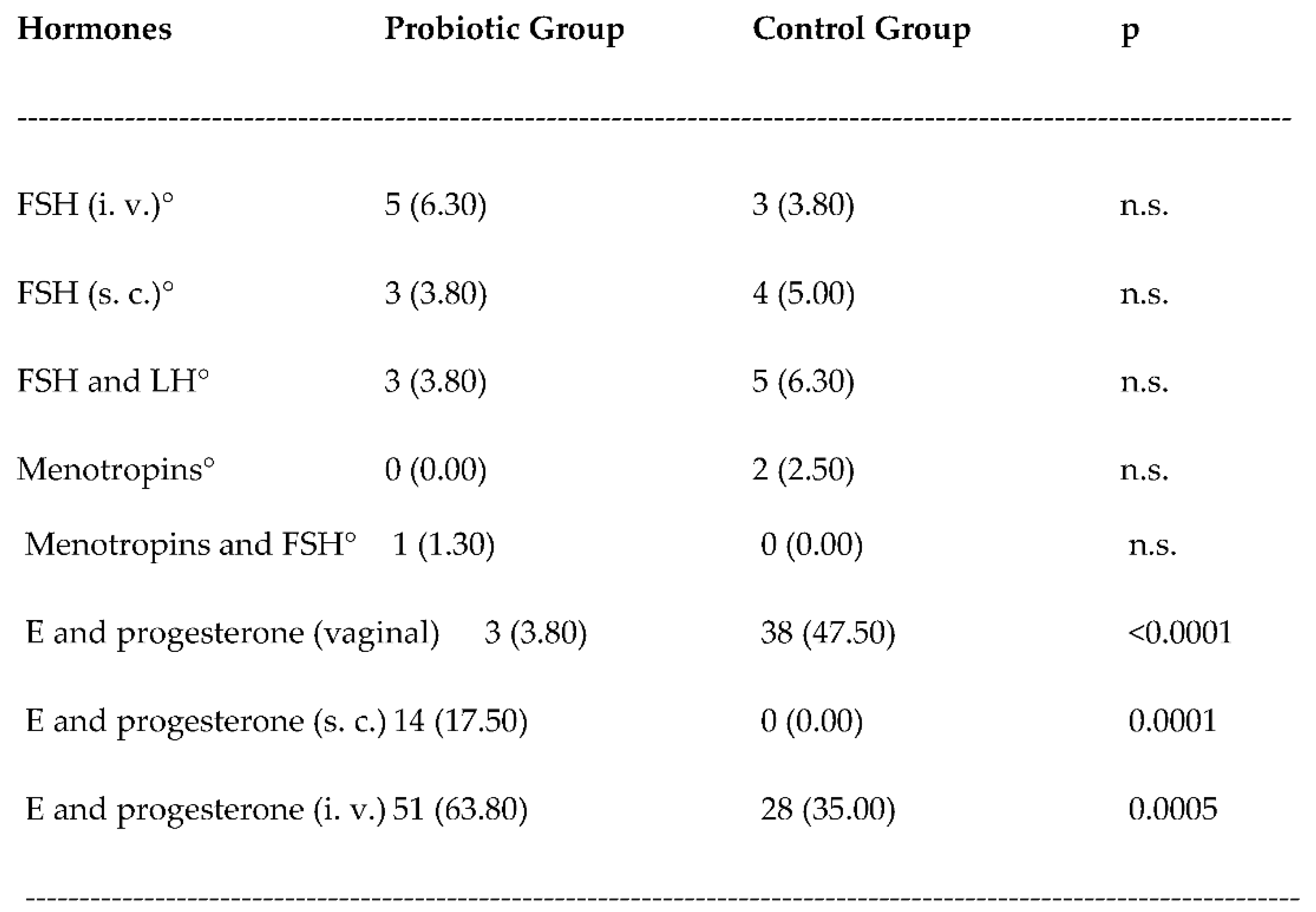
Numbers refers to the number of women of each group. In brackets the percentage values. FSH: Follicle Stimulating Hormone. LH: Luteinizing Hormone. s. c.: subcutaneously. i. v.: intravenously. E: oestradiol valerate. n. s.: not significant. °All women of these subgroups were also treated with vaginal progesterone.
Table 6.
Live births (LB) in the two groups, considering only the women in the two groups with a positive pregnancy test.
Table 6.
Live births (LB) in the two groups, considering only the women in the two groups with a positive pregnancy test.
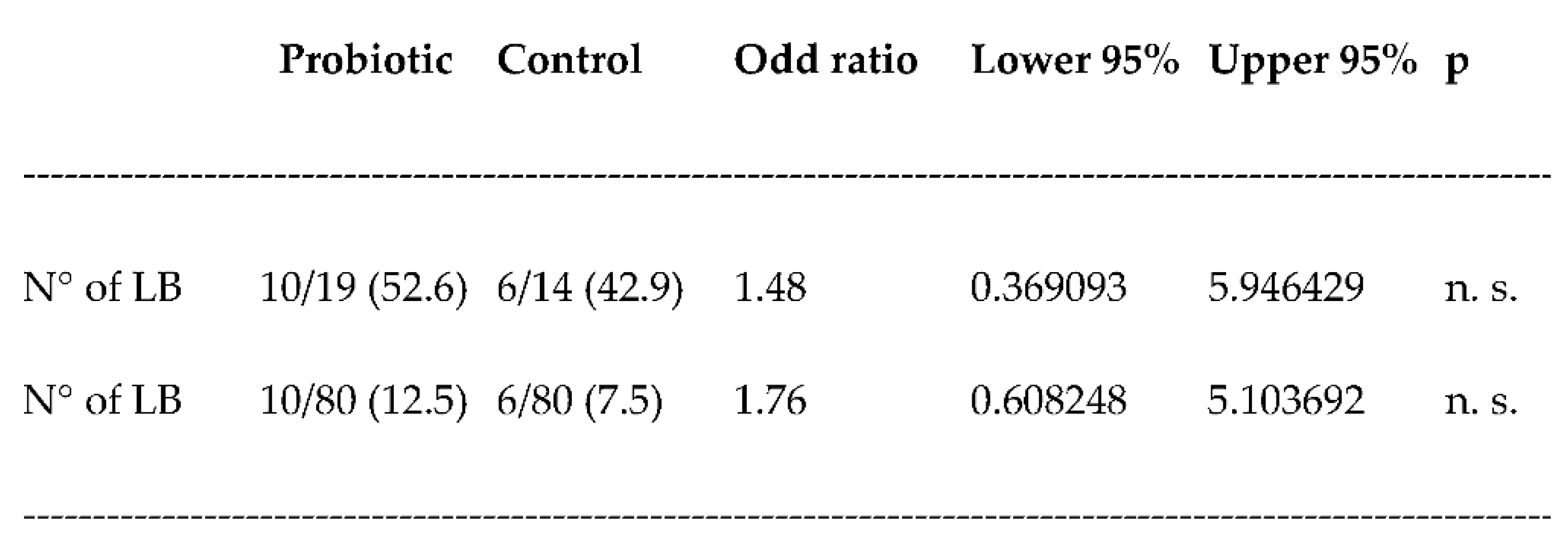
Numbers refers to the number of women of each group. In brackets the LB rates in %. n. s.: not significant.
Table 7.
Live births (LB) and LB rate in the two groups according to the ART method applied.
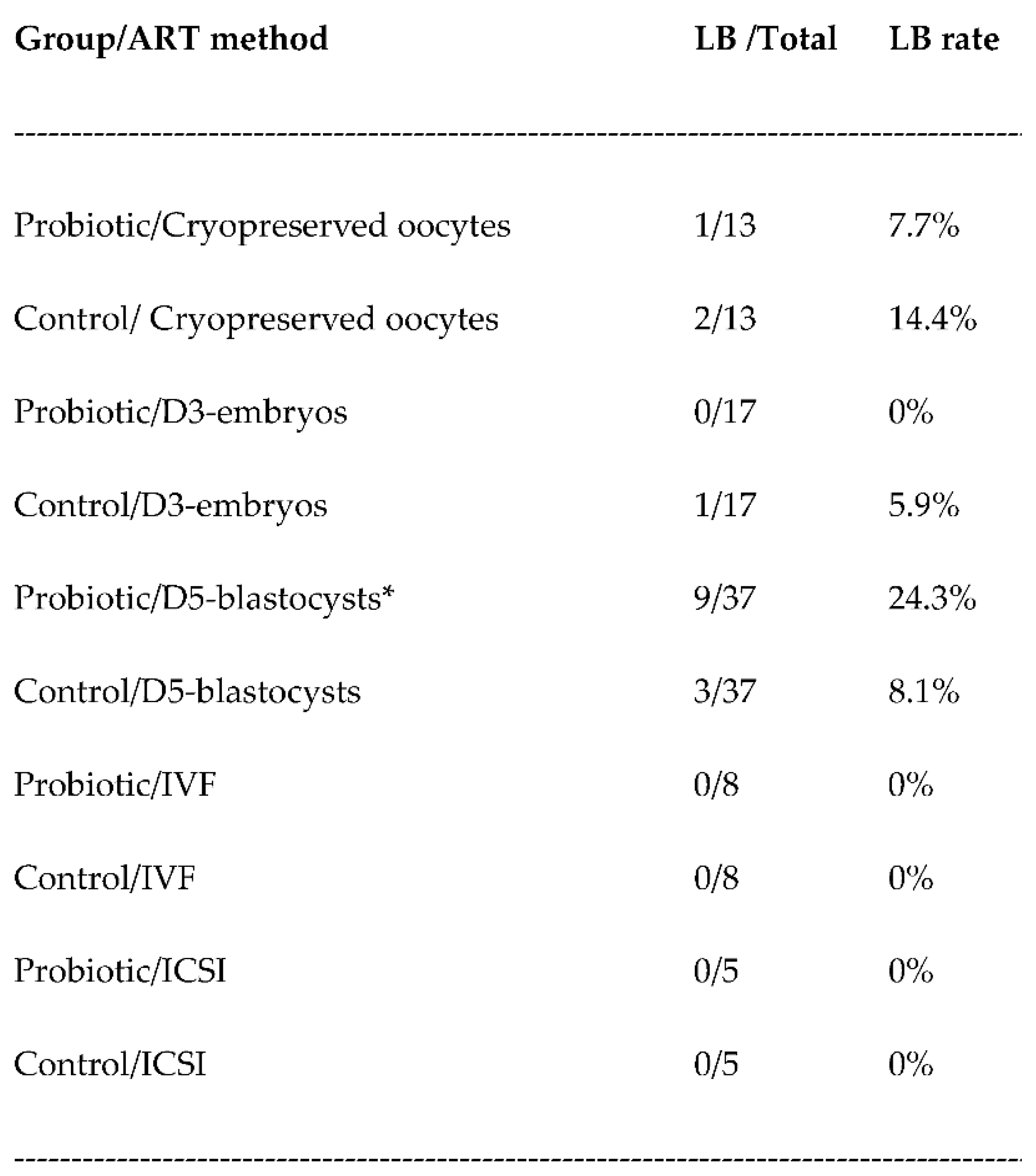
ART: assisted reproductive technology. IVF: In vitro fertilization. ICSI: Intracytoplasmic sperm injection. D3: day-3 embryos. D5: day-5 blastocysts. Numbers refers to the number of women of each group. *Odds ratio: 3.64 (lower 95%: 0.899122; upper 95%: 14.75929); p=0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



