Submitted:
02 October 2023
Posted:
09 October 2023
You are already at the latest version
Abstract
Background and Aims: Paramedics attend an unprecedented number of drug poisoning events daily in British Columbia (BC), Canada due to the ongoing public health crisis related to an increasingly toxic and unregulated supply of illicit drugs. Paramedics have the potential to support alternative models of care to reduce harm, but their perspectives towards harm reduction initiatives are polarized. Understanding the drug-related substance use content in paramedic curriculum documents is important for deploying effective harm mitigating programs. The objective of this study was to understand what drug-related substance use content currently exists within paramedic curriculum documents in British Columbia. Methods: We performed a document analysis of curriculum documents in BC’s paramedic training institutions, the primary program textbook, and the 2011 National Occupational Competency Profile (NOCP). We used the Checklist for Assessment and Reporting of Document Analysis (CARDA) tool to perform our analysis. We analysed and coded documents both inductively and deductively and subsequently combined, refined, and used the codes to inform the development of themes via reflexive thematic analysis. Results: Of the 44 documents analysed, 22 included codes relevant to the research questions. Paramedics are primarily taught to care for people who use drugs in an acute drug-poisoning response only, with little consideration of holistic care, and no meaningful mention of harm reduction. Some stigmatizing language was found within the content. Conclusions: Many opportunities to introduce holistic models of care for people who use drugs along the entire continuum of care are unaddressed by paramedic curriculum documents in BC. Curriculum developers should include people who have lived and living experience of drug use in the co-design of educational programs involving their care. Further qualitative analyses are required to evaluate the relationship between paramedic education and provider-based stigma.
Keywords:
Emergency Health Services
; Addiction
; Substance Use Disorder
; Paramedicine
Introduction
Paramedics in British Columbia (BC) manage an incidence of drug-related harm that is unmatched by any other paramedic service in Canada [1]. In 2021, BC paramedics attended 35,525 drug poisoning events, a 31% increase from the previous year, and an 189% increase from 2015, prior to the announcement of a public health emergency by the provincial government [2]. Since this declaration, more than 11,000 BC residents have died due to illicit drug toxicity, and in 2022 drug poisoning deaths account for more deaths than homicides, suicides, drownings, motor vehicle incidents, and fire related deaths combined [3].
Although paramedics play an important role in the resuscitation phase in their response to a toxic drug event, their role in the post-resuscitation phase, where they must support the patient’s next steps in navigating the healthcare system means they are uniquely positioned to reduce drug-related harm [4]. People who experience an out of hospital drug poisoning event who are not conveyed to the emergency department (ED) are at a significantly higher risk of short- and long-term mortality [5,6,7], and in BC approximately 50% of such calls currently refuse ED conveyance. As such, it has never been more important for paramedics to be empowered to act as system navigators, offering alternative destination pathways, and concurrent harm reduction initiatives and programs [8]. Despite this, in some areas that have introduced harm mitigating programs paramedics appear to express polarizing views on their utility, describing sentiments that initiatives such as NLB (Naloxone Leave Behind) are not feasible, and do not decrease drug-related deaths [9].
Further, paramedic students demonstrate significantly lower levels of empathy for people who use drugs than any other patient population [10,11,12] which in general tends to decline further as their training progresses. This is a cause for concern, and it remains unclear what influence entry to practice education has on paramedics’ empathy towards people who use drugs. Empathy can be taught and developed, yet this is not routinely included in paramedic curricula in Canada [13].
What is included in paramedic education in Canada is an emphasis on linear responsive models that prioritize patient stabilization and transportation in the out-of-hospital setting [14]. The curriculum in general poorly represents complex, contemporary practice, which is a cause for concern, considering the evolving demands of paramedic work, including their involvement in public health crises they weren’t best prepared for [15,16]. A narrow focus on the medical aspects of drug use ignores the complex social and structural determinants of health that influence drug use patterns and outcomes [17]. These individuals often face a range of intersecting health and social challenges, such as poverty, mental illness, social isolation, and homelessness, that may exacerbate their drug use and increase their risk of drug-related harm [18].
Therefore, a more comprehensive, holistic approach that addresses the complex health and social needs of people who use drugs is necessary [4]. We aimed to investigate potential contributors to healthcare provider-based stigma in paramedic education and determine whether current paramedic education in BC adequately prepares paramedics to provide holistic care for people who use drugs. Identifying gaps in paramedic education is crucial to enable paramedics to play a more significant role in reducing drug-related harm in BC.
Methods
Design and Context
Didactic curriculum documents from the two paramedic training institutes in British Columbia were included: the Justice Institute of British Columbia (JIBC) and Columbia Paramedic Academy. Both the Primary Care Paramedic (PCP) and Advanced Care Paramedic (ACP) program curriculum documents were included. These programs vary in length and methods of delivery from a 4.5-month entry-to-practice certificate program (PCP) to a 20-month advanced diploma program (ACP). Didactic program materials are delivered both virtually as well as face to face, and practice education takes place in both out-of-hospital and in-hospital settings. Both part-time and full-time curriculum documents were included in the analysis. The curriculum documents were created by curriculum developers and faculty within both institutes. In addition, we analyzed the primary paramedic textbook for both schools: Nancy Caroline’s Emergency Care in the Streets (8th Edition) [19], and the national accreditation guidance document - the Paramedic Association of Canada’s 2011 National Occupational Competency Profile (NOCP). The NOCP outlines the competencies of paramedic practice within Canada, and although not intended to be a curriculum blueprint, it serves as a guiding framework for many educational institutions to inform curriculum design [20].
We elected to conduct a document analysis following a conversation in which we explored paramedic attitudes towards harm reduction initiatives, and low student empathy scores towards people who use drugs. Further, we noted in the literature that practicing paramedics appeared polarized towards the idea of integrating harm reduction initiatives into their practice [21,22]. To better understand where these perspectives are potentially formed, we sought to evaluate entry-to-practice paramedic education and the documents that shape and inform such education. The protocol for this study can be found at http://osf.io/sr9wj.
We sought to determine the presence of certain words or concepts within texts or sets of texts [8], and the culture and time of which these are a part. We employed a summative approach to strengthen the analysis by providing insight into complex models of human thought and language [23]. This was done by counting and comparisons, habituality of keywords and content, followed by the interpretation of the basic context.
We followed a four-stage process when analyzing documents which contained the steps outlined in both the Checklist for Assessment and Reporting of Document Analysis (CARDA) and O’Leary [24,25] (see Appendix). First, we planned by identifying our research question, determining the inclusion and exclusion criteria, and creating a search strategy. Second, we selected relevant documents and screened them for eligibility. Third, we extracted relevant data from the documents. Finally, we analyzed and synthesized the data to answer our research questions.
Procedure
We performed a document analysis utilizing the CARDA (See Appendix 1), as well as O’Leary’s eight- step planning process [25]. Contingency planning was discussed early between us, and we decided that if one document was not available, the analyses would continue, but if two or more documents were not available the scope of the work would be amended to appropriately address the research questions.
We requested the curriculum documents via e-mail from the respective program lead instructors in August 2022. We acquired an online digital copy of Emergency Care in the Streets 8th Edition from Jones and Bartlett Learning. The 2011 NOCP is open access and available to the public and we downloaded it from the Paramedic Association of Canada’s website. For this study, drug-related substance use referred to the use of illicit and controlled drugs.
To maintain focus on the research questions, the education institutions will remain anonymized in the results.
Analysis
The first author (JB) systematically read the curriculum documents and coded all phrases relating to drug-related substance use both inductively and deductively. Coded data was reviewed by AB. We developed 10 interview questions as informed by O’Leary (2014). The development of the questions was reflexive in nature and questions were adapted following discussion between us after initial analysis of the included documents. The questions were not adapted once coding commenced.
We coded questions against each document to gain a comprehensive understanding of the data:
- Who is the audience?
- Why was the content included?
- When/where was the text produced?
- How does the document reflect the time that it was written?
- How would the intended audience be likely to interpret the content?
- How would a non-intended audience likely interpret the content?
- What does the text say and what is the context?
- What language does the text use?
- What is the tone of the text?
- Does the author(s) choice of words reveal covert assumptions along with an overt message?
Further, we made annotations to capture underlying tones or covert meanings within the texts. Documentation of relationships, sentiments, common findings, and preliminary themes were recorded in a research journal, and we stored these as memos in NVivo (v12, QSR International, 2022). We sorted text phrases of the documents which mentioned drug-related substance use (e.g., substance abuse, drug abuse, addiction, substance misuse) into a language parent code to evaluate the potential existence of stigmatising or outdated terminology. We iteratively interpreted the meaning of extracted phrases pertaining to drug-related substance use. Doubts concerning the inclusion of codes, text phrases, and their position within the thematic analysis were journaled, and discussed between us. We undertook reflexive thematic analysis informed by Braun and Clarke (2018) by gaining familiarity with the data in the form of visual data representation, followed by the grouping and collapsing of codes in the remaining phases, with consultation between us during each phase of the analysis ensuring trustworthiness standards were met throughout [26].
Measures to Ensure Trustworthiness
To ensure rigor and trustworthiness in the validity of our research, we assessed the potential risk of bias and evaluated the quality of the documents. We explored the document’s agenda and possible sources of bias, and assessed the documents based on criteria such as relevance, validity, and reliability as described by O’Leary (2014). By following the CARDA checklist, we ensured that our document analysis research design was systematic and rigorous. We aimed to ensure credibility through prolonged engagement with the data. Raw data were stored and organized in archives. Efforts to maintain dependability included documented reflexive journal entries, annotations, and a well described audit trail of code genesis which included saved notes that highlight the rationale for code inclusion and exclusion. Confirmability was ensured by a clear audit trail of codes, and detailed notes regarding the study characteristics, concepts, and themes all of which were underpinned by a reflexive approach [27].
Positionality Statement
The lead researcher (JB) is a Caucasian, female, postgraduate educated paramedic, and subject matter expert on the paramedic response to the drug poisoning crisis in British Columbia. She is a leader of paramedic practice within her organization, with 10 years of experience. She has three years of experience as a paramedic researcher and has an interest in qualitative approaches to socially responsive models of health care delivery. AB is a Caucasian, male, doctoral-educated paramedic researcher with over 25 years of experience in out-of-hospital care, and methodological expertise including document analysis. We approached this study from a phenomenological lens, aiming at construing the meaning of the document on a surface level, and any underlying meaning. We have experience as educators collectively with seven different institutions in Canada, including the two institutes studied. We do not personally have lived or living experience of drug use and addiction, but we have experience working with people who use drugs. Together, our approach to this analysis aimed to employ both meaningful interpretation and documented objectivity to inform holistic analysis of the documents.
Results
A total of 44 documents were identified, procured, and analysed, comprising 42 curriculum documents, the NOCP, and the textbook. For the NOCP, we analyzed one document (NOCP main document), for the textbook, we analyzed a total of five chapters: Chapter 3 (Public Health), Chapter 13 (Principles of Pharmacology), Chapter 14 (Medication Administration), Chapter 27 (Toxicology), and Chapter 28 (Psychiatric Emergencies) were analysed. Text phrases pertaining to drug-related substance use were discovered in 22 of these documents. Only one of 22 documents described harm reduction as a component of paramedic practice.
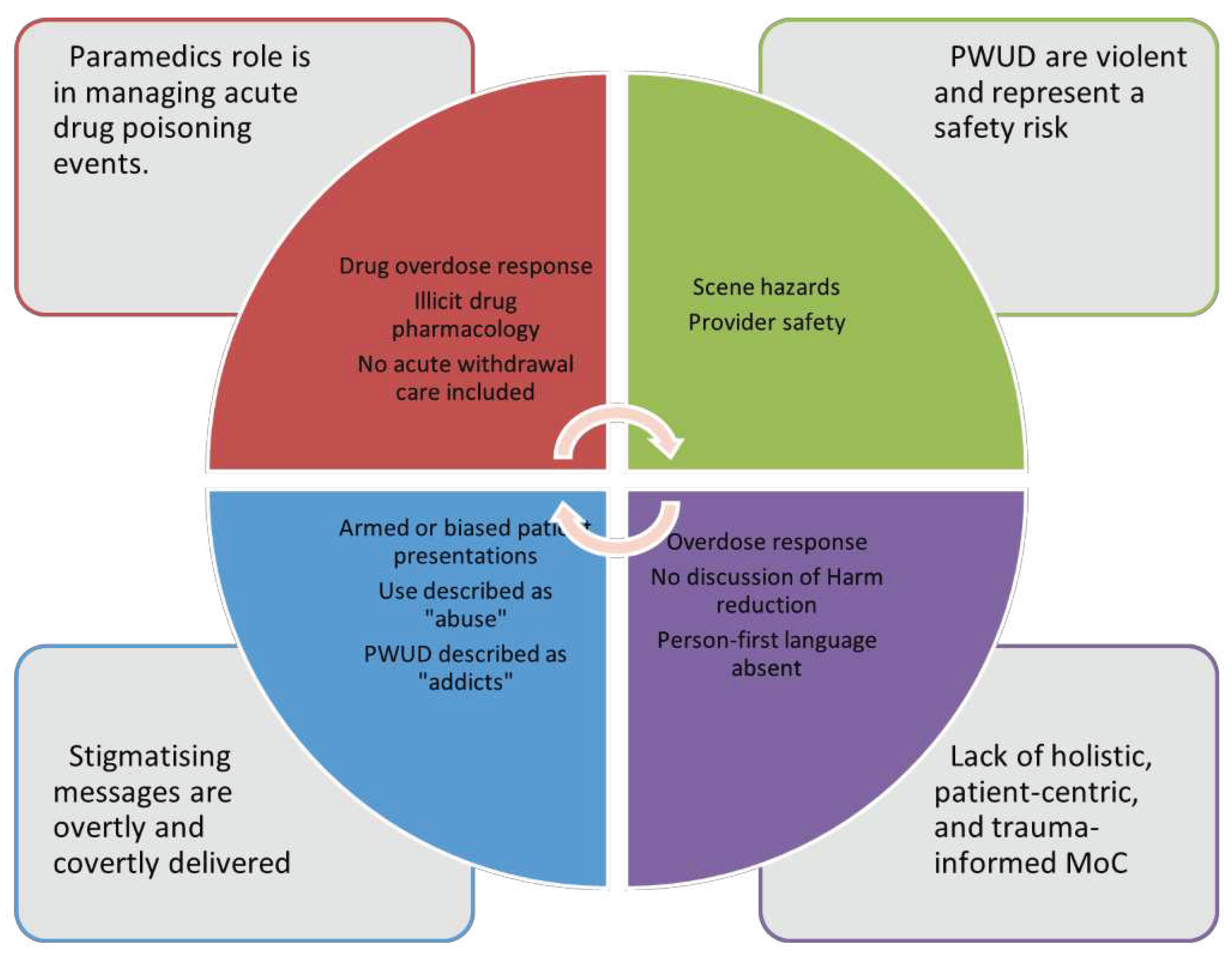
Using Braun and Clarke’s framework for reflexive thematic analysis, we developed four themes.
- The Paramedic Role: Acute drug poisoning events are the only time paramedics can intervene
- Patient Population: People who use drugs are often violent and represent a safety risk to paramedics
- Words Matter: Stigmatising messages are overtly and covertly delivered to paramedic students
- Models of Care: Lack of holistic, patient-centric, and trauma-informed practices.
Figure 1.
Thematic Analysis.
The Paramedic Role: Acute Drug Poisoning Events Are the Only Time Paramedics Can Intervene
There was a universal focus on resuscitation as the paramedic role in caring for people who use drugs. Despite paramedics encountering people who use drugs in many settings and contexts, the only one described by the documents was in the setting of an acute drug poisoning, normally described as an ‘overdose’. From a clinical perspective no content addressed the treatment of a patient in acute illicit drug withdrawal. Phrases and words were extracted if they pertained to care provided during an acute drug poisoning event (See Figure 2).
The 2011 NOCP included a new competency area for health promotion and public safety. Despite this, no competencies within the document included drug-related harm reduction or expanding contexts of paramedic practice. Further, the recognition and treatment of acute
withdrawal was not included in the document. Within the “Toxicological Illness” section of the NOCP, drug-related substance addiction, overdose prevention, harm reduction, screening, and acute withdrawal were not described. The phrase "toxicological syndromes" was used throughout pertaining specifically to drug poisonings and did not discuss or reference substance use or addiction outside of this context.
Other texts focused solely on patient assessment and treatment of a person experiencing a drug poisoning event with little mention of the paramedic role outside of this response. Drug poisoning response curriculum included and highlighted a step-based approach that focused on airway management, quality ventilation, and the administration of naloxone to restore patient respiration. Curriculum documents introduced students to drug paraphernalia, including different drug presentations, and drug supplies.
Despite the increasingly toxic and unregulated supply of illicit substances that exist in British Columbia, little drug-related educational content addressed this contamination. When articulating the role of the paramedic in the drug poisoning crisis, texts described “the rapid recognition of opioid overdose followed by appropriate treatment” as a cornerstone. Statements that included patient education and identification of “those at risk of opioid abuse” suggested that paramedics do have a greater role to play, however these statements were not expanded upon.
The emphasis of drug-related response discovered within the texts is placed on opioid reversal and management, with significantly less attention on the care of people who use non-opioid illicit substances such as methamphetamine, cocaine, and other drugs. Care for special populations that include approaches to youth who use drugs, or elderly who use drugs was not discovered in any of the documents.
Patient Population: People Who Use Drugs Are Often Violent and Represent a Safety Risk to Paramedics
Several phrases that spoke to the hazards and risks that paramedics may be exposed to whilst caring for people who use drugs were included. Although most scene hazards pertained to risk of patient combativeness or violence, some documents included environmental hazards including exposure to sharps, such as used needles.
Figure 3.
Word Cloud for Theme Two.
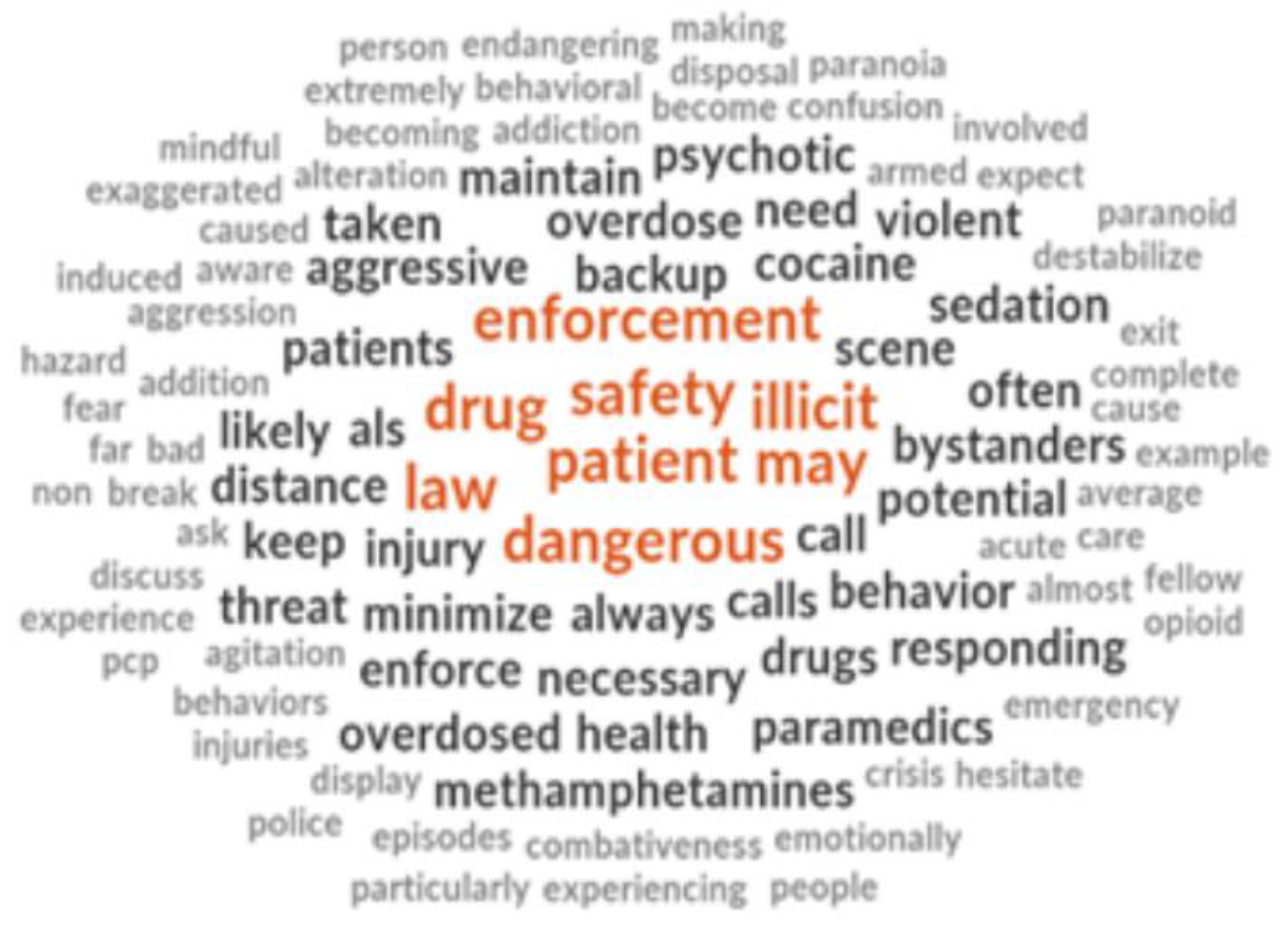
Many phrases made broad sweeping statements surrounding the relationship between illicit drug use and aggressive and dangerous behaviors. (Note that throughout this manuscript, the emphasis in quotes is ours)
“Aggressive and dangerous behaviors are often caused by the use of illicit drugs” (5, p.1466)
Fear-inspiring statements were discovered.
“Be aware that patients who have taken an overdose may be extremely dangerous” (5, p.1406)
“Their behavior can quickly become violent, so always be mindful of your exit strategy when on scene. Do not hesitate to ask for law enforcement support if the scene seems likely to destabilize.” (5, p.1414)
Prejudice towards the use of stimulants in the absence of supporting evidence or pathophysiological explanations or grounding were included.
“In addition to the threat from bystanders, the risk of a patient becoming aggressive is always present, particularly when cocaine or methamphetamines are involved.” (5, p.507)
Some statements imply stigmatising assumptions broadly about people who use drugs such as their mental state and their inherent risk of threat.
“Such people are often paranoid, emotionally unstable, and almost always armed, making them a far more serious threat than an average patient with a non–drug-induced behavioral emergency.” (5, p.507)
Documents further described the relationship between patient violence and paramedic care, and at times emphasized the risks that people who use drugs pose to paramedic safety by using inappropriate humor. One example was a PowerPoint slide that referenced a children’s book titled “Go to sleep” on the topic of people experiencing stimulant related drug poisoning. The slide included expletives and implied that people experiencing stimulant poisoning will likely need to be sedated by paramedics.
Words Matter: Stigmatising Messages are Overtly and Covertly Delivered to Paramedic Students
Stigmatising messages were discovered in the included documents in both overt and covert ways. Specifically, messages were considered stigmatising if they used language no longer accepted as person-centered or trauma-informed, or where covert assumptions or statements were made (NIDA). Covert assumptions were defined as statements that implied negative connotation without explicitly stating such.
Figure 4.
Word Cloud for Theme Three.
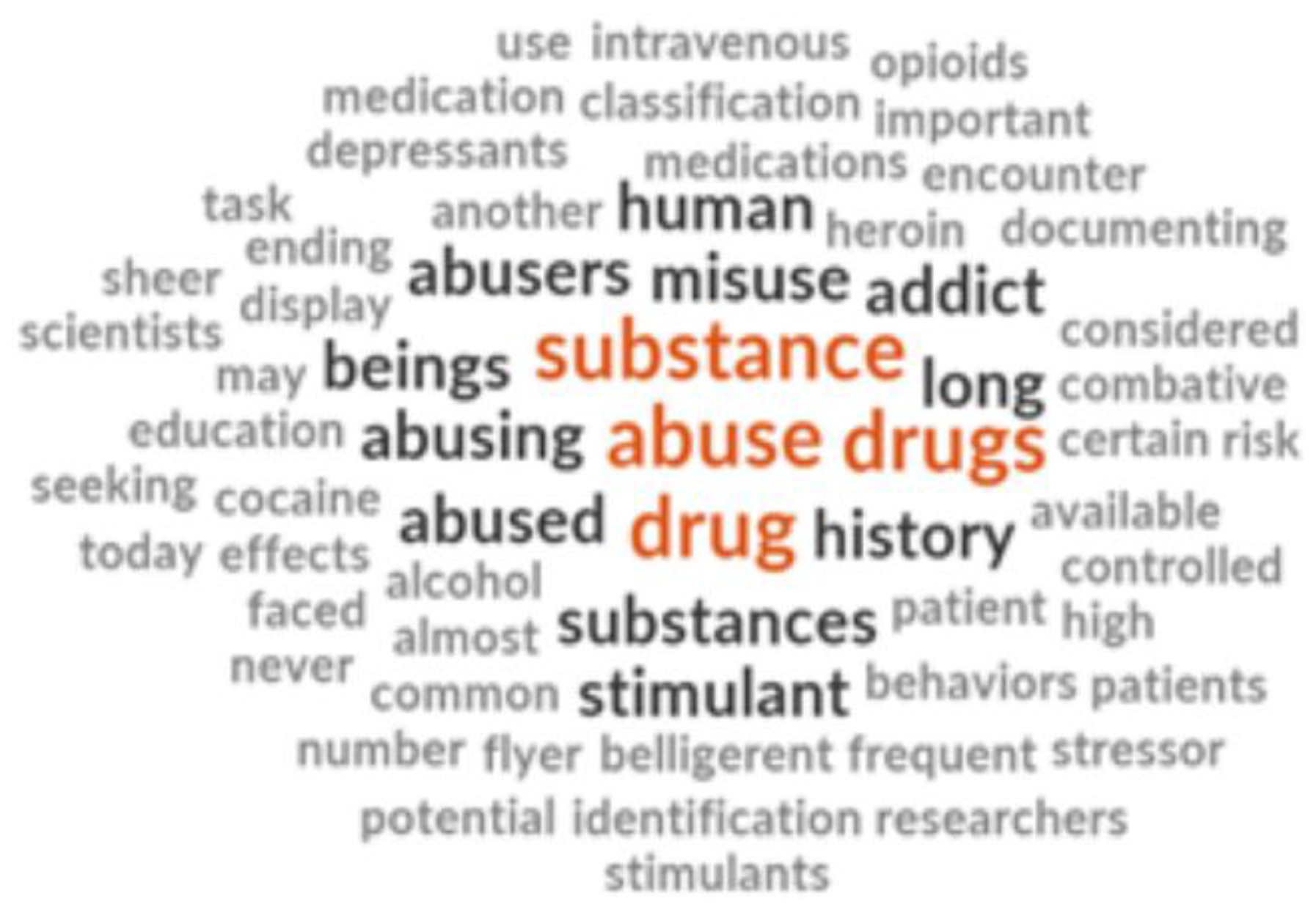
Our analysis led to the discovery of inferences regarding people who use drugs who were often referred to as drug “abusers”, “misusers”, and “addicts”.
Substance use was often referred to as substance “abuse”. Abuse is no longer accepted as holistic terminology, as it has been found to have a high association with negative judgements and punishment (Kelly and Westerhoff, 2010).
“Human beings have a long history of abusing drugs.”
“You are almost certain to encounter patients who abuse medications.” (5, p.639)
“Drug-seeking” behavior is mentioned as common in people who use drugs, without much to qualify what this means in the out-of-hospital setting and its relevance to care provided by paramedics. In some instances, associations are made between socioeconomic status and substance use.
“Understanding the complex nature of substance-related disorders is your first step in providing professional, competent, and compassionate care to all affected people, from the homeless drug addict to the substance-dependent businessperson” (5, p.1476)
Despite this language, there are notes within the document that suggested facilitating classroom discussions regarding stigma, and professionalism whilst caring for people who use drugs. This suggests that conversations are indeed taking place (or at least are intended to take place) surrounding the intersectionality between mental health, addiction, and drug-related stigma in the classroom. What these conversations sound like, or the conclusions those participating in them come to, we don’t know.
“Discuss stigma and mental health associated with addiction.”
“Watch Video: ‘Bringing Out the Dead’. Discussion: Professional or not?”
The use of person-first language was almost entirely absent from the included texts except for one statement. The statement also emphasized the risk this patient presentation poses to paramedics without any complementary statements explaining the causes of an “acute psychotic break”, or how to care for this presentation.
“A person with a drug addiction experiencing an acute psychotic break poses its own unique threats.” (5, p.1457)
Models of Care: Lack of Holistic, Person-Centered, and Trauma-Informed Practices
Language within all included documents was found to be largely biomedical in nature. Deviations from biomedical terminology existed in only eight phrases which were coded as representing holistic care options. Phrases were considered holistic if they addressed the person who uses drugs with respect to the social determinants of health, not the drug use itself, and if the focus of care was placed outside of the response to the drug poisoning event alone (see Figure 5).
Despite the language within the texts being predominantly biomedical and responsive, some holistic messages were observed. Examples of paramedics leading the expansion of their role to a more holistic entity are included in the reporting of a public awareness campaign named “Stop Heroin”, where one paramedic describes her role as being historically limited by its responsive model.
“When it comes to drug use and overdoses, EMS has always been ’reactive.’ Someone overdoses, we give Narcan, transport.” (5, p.81).
The campaign was started and led by a paramedic who felt limited in her role.
“I decided that, as the organization that sees these situations firsthand, we should be part of the conversation, and hopefully, have a hand in developing a meaningful solution to the problem that is plaguing our county”. (5, p.81)
The documents hint at holistic and integrative approaches to care of people who use drugs.
“Determining the most effective treatment for substance-related disorders requires an integrative approach of examining the social, biologic, cultural, cognitive, and psychological dimensions of the problem.” (5, p.1476)
“Discussion about Addiction vs. Dependence in context of opioids and alcohol”
“Apart from the physical effects of substance abuse, addiction carries a social stigma that can lead to feelings of isolation, paranoia, and depression” (5, p.1403)
Instead of exploring these approaches however, responsive, and resuscitative models of care are reemphasized, and at times further care is downplayed as being outside of the paramedic’s scope.
“As a paramedic, you may be unable to explore all these areas during a short transport to the medical facility, particularly because much of your time will be devoted to ensuring the safety of your crew and managing the patient’s ABCs.” (5, p.1476)
Although there were statements within the documents that addressed titrating naloxone doses to avoid precipitation of acute withdrawal, the end goals appeared to be anchored in preventing the risk of violence, and less about avoiding uncomfortable symptomatology.
Discussion
Paramedic-led harm reduction approaches face barriers to their implementation due to stigma and low empathy scores among paramedic trainees for people who use drugs [11,13,21,22]. We sought to evaluate if stigma and preconceived negative perspectives of people who use drugs existed in paramedic curriculum documents in BC. We analysed the curriculum from two paramedic education institutions, a core textbook, and a national competency document. Our analysis highlighted that the paramedic role is described as limited by drug poisoning response and management, people who use drugs are often portrayed as violent and representing a safety risk to paramedics, stigmatising messages are overtly and covertly delivered to paramedic students, and there is a significant lack of holistic, person-centric, and trauma-informed practices introduced to paramedic students within the intended curriculum.
Whilst opioid toxicity reversal and drug poisoning response remain essential, paramedics are increasingly responding to events where co-intoxicants complicate reversal, leading to multiple high doses of naloxone administration, and unresolved coma, despite complete opioid toxidrome reversal [28,29,30]. Drug contamination or adulteration notwithstanding, out-of-hospital treatment of a drug poisoning event has time and time again proven insufficient in reducing drug-related harm and mortality [31,32]. This is evidenced by soaring death tolls as reported in the British Columbia Coroner Service (BCCS) Death Review Panel which highlighted that illicit drug toxicity is the leading cause of unnatural death in the province [3]. Equally alarming is the climbing frequency of non-conveyance to the ED by paramedics following a drug poisoning event and the correlating increases in risk of short- and long-term mortality [6,8]. Lending to concerns around non conveyance is the decreasing prevalence of 911 activation by the community of people who use drugs [33].
As the degree of drug toxicity and drug-related mortality increases whilst the incidence of 911 calling and ED conveyance decreases, the opportunity for paramedics to enact holistic models of care that include harm reduction programs is narrowing. A shift is required to recalibrate the focus of the paramedic role in caring for people who use drugs, one that is currently not reflected in, (and may indeed be hindered by) paramedic student education as explored in this analysis. The description of these responsive models of care is further limited by the focus placed on resuscitation. Under-explored areas of response include care of people who use non-opioid illicit substances, targeted approaches to care of youth, elderly, and Indigenous patients, and care of patients in acute withdrawal.
Missing entirely from the findings of our analysis is the opportunity to expand on the downstream negative effects of leaving a patient who does not wish to be conveyed to the ED in acute withdrawal. The pathophysiological milieu that manifests as a person is placed into acute withdrawal, and how this impacts a paramedic's perception of their presentation is worthy of consideration in the curriculum. Similar attention should be placed on why these symptoms arise and how, for example, neurochemical changes that take place may be perceived by the paramedic as unappreciativeness, or violent and aggressive predispositions.
The increasing incidence of violence against paramedics and occupational risks has been described as a serious public health problem [34,35,36,37] While paramedic safety should take utmost priority, curriculum developers must be mindful with their choice of language, being careful not to use language that generalizes, or make assumptions about an entire patient demographic [38,39]. The use of absolute and definitive language around patient violence has the potential to create negative associations for paramedic students. Statements such as “these patients are almost always armed” or “aggression is almost always caused by drugs” has the potential to cause preconceived ideas that may strain the relationship between the paramedic and people who use drugs prior to any actual patient encounter. Because of these preconceived notions regarding violence, paramedics may begin their interaction with people who use drugs “on edge”, potentially leading to a demeanor that could be inadvertently perceived by people who use drugs as negatively authoritative or non-empathetic [40]. Of course, it is not words alone that influence how communication is perceived; negative tone, closed off body language, or general approach that may come off as disapproving or judgmental may all contribute to a negative interaction, regardless of the words used themselves [41]. Additional education related to communication and the importance of language with special respect to those who may have had previous negative interactions with the public safety or health care system may be beneficial. Without such additional education, paramedics may be unaware of how their language is being perceived. Not only are students being taught a medical language by which to communicate, they are further being taught occupational language norms by which they will eagerly adapt into their own vocabulary.
The utilisation of person-first and inclusive language creates an environment where people feel like they can seek assistance when required [42]; however, we found the use of person-first language within this analysis was almost non-existent. Inversely, when people are spoken to or about in ways that may be perceived as dehumanizing, they are less likely to reach out for help, and are more likely to use drugs alone placing them at higher risk [43]. It is important to consider that not all stigmatising language is intentional or overt, and that the intent of the message is not always the impact, especially in patients who may have long-standing experiences of intergenerational trauma, and discrimination [44]. The use of person-centric and trauma-informed language will be essential in the shift towards holistic models of patient care delivery and should be reflected in curriculum documents [45].
By introducing such concepts into paramedic education, we can begin to offer opportunities for paramedics to positively influence the journey of people who use drugs through the healthcare system. Initiatives such as alternative care pathways, take home naloxone programs, and treatment of acute withdrawal have the potential to not only reduce patient harm, but to reduce the harm bestowed upon paramedics performing a role that is increasingly perceived as restrictive, limiting, and ineffective. The effects these models of care have on resilience, compassion, and empathy have been described in qualitative analysis across the globe. Locally this was demonstrated by Williams-Yuen et al., (2020) who evaluated the ways BC paramedics experience the overdose crisis [32]. Paramedics described an emotional burden associated with the ongoing crisis, correlated directly with one’s capacity to help. Because paramedics begin expressing diminished levels of empathy for people who use drugs long before they begin clinical practice, it is timely to ensure curriculum integrates education on empathy, emotional burden, moral distress, and we suggest holistic models of care that involve harm reduction may combat many of these distressing associations.
Involving people who have lived and living experience of drug use in the co-design of programs that involve their care is a meaningful way to address gaps in curriculum design [46,47,48]. Patients, as the end users of paramedic services, play an important role as stakeholders in directing their goals of care more broadly. Engaging the patient voice in health professions education can enrich the educational experience whilst promoting justice and empowering a compassionate approach amongst health care providers [49]. Efforts to engage patients should be considered early, to avoid any unintended tokenistic views or perceptions. Engagement with marginalized and underserved populations should be driven by principles of ethical engagement, and in general, should be compensated opportunities [50].
Limitations
The ability to analyse what paramedics in BC are taught about drug-related substance use is limited by the nature of our analysis of didactic learning documents. In academia lives the intended curriculum, the enacted curriculum, and the experienced curriculum which vary in content [51]. This paradigm of what lives within curriculum documents versus what is taught is a complex commonality of health education history and culture, the scope of which lies outside the purpose of this study. Without observing the context, tone, language, instructor biases, supplementary information, deviations from curriculum guidance, or sidebar conversations delivered to paramedic students by lecturers, it is impossible to conceptualise the full scope of what paramedics learn about drug-related substance use. In addition, we were unable to collect drug-related curriculum documents from one of the schools ACP programs due to the curriculum being under development and not finalised or prepared for release.
Conclusions
Our analysis of paramedic curriculum documents in BC has highlighted the presence of stigmatizing language and negative preconceptions towards people who use drugs, which may be hindering the implementation of paramedic-led harm reduction approaches. The paramedic role is currently described as limited to drug poisoning response, which is insufficient to reduce drug-related harm and mortality. The increasing degree of drug toxicity and mortality and decreasing incidence of 911 calling and ED conveyance necessitates a shift towards holistic models of care. The language used in paramedic education needs to be mindful and inclusive to avoid preconceived notions, negative associations, and to facilitate positive interactions with people who use drugs.
The importance of contemporary drug-related substance use education for paramedic students is becoming apparent in the context of the ongoing public health crisis related to an increasingly toxic supply of drugs in BC. Future drug-related substance use curriculum development should aim to reflect the evolving role of the paramedic in the drug poisoning crisis. Academic program design leaders should consider the ethical engagement of people who have lived and living experience of drug use as stakeholders in the co-design of curriculum that involves their care. Harm reduction, and the many opportunities that paramedics have to positively influence a patient's journey through the healthcare system should receive equal attention in the curriculum to that afforded to the emergency drug poisoning response.
Funding
None.
Acknowledgements
None.
Conflicts of Interest
None.
References
- Belzak, L.; Halverson, J. The opioid crisis in Canada: A national perspective. Health Promot. Chronic Dis. Prev. Can. 2018, 38, 224–233. [Google Scholar] [CrossRef]
- BCEHS. 2021 Overdose Numbers [Internet]. Available online: http://www.bcehs.ca/about site/Documents/Overdose%20Information%202021.pdf (accessed on 10 November 2022).
- British Columbia Coroner Service. BC Coroners Service Review Panel: A Review of Illicit Drug Toxicity Deaths [Internet]. Vancouver. 2022. Available online: https://www2.gov.bc.ca/assets/gov/birth-adoption-death-marriage-and-divorce/deaths/coroners-service/death-review-panel/review_of_illicit_drug_toxicity_deaths_2022.pdf (accessed on 10 November 2022).
- Bolster, J.; Armour, R.; O’Toole, M.; Lysko, M.; Batt, A. The Paramedic Role in Caring for People Who Use Illicit and Controlled Drugs. Paramedicine 2023. [Google Scholar] [CrossRef]
- Stoove, M.A.; Dietz, P.M.; Jolley, D. Overdose deaths following previous non-fatal heroin overdose: Record linkage of ambulance attendance and death registry data. Drug Alcohol. Rev. 2009, 28, 347–352. [Google Scholar] [CrossRef]
- Ashburn, N.P.; Ryder, C.W.; Angi, R.M.; Snavely, A.C.; Nelson, R.D.; Bozeman, W.P.; McGinnis, H.D.; Winslow, J.T.; Stopyra, J.P. One-Year Mortality and Associated Factors in Patients Receiving Out-of-Hospital Naloxone for Presumed Opioid Overdose. Ann. Emerg. Med. 2020, 75, 559–567. [Google Scholar] [CrossRef]
- Weiner, S.G.; Baker, O.; Bernson, D.; Schuur, J.D. One-Year Mortality of Patients After Emergency Department Treatment for Nonfatal Opioid Overdose. Ann. Emerg. Med. 2020, 75, 13–17. [Google Scholar] [CrossRef]
- Moe, J.; A Puzzling Trend: Denying Ambulance Transport Post-Overdose [Internet]. Vancouver: Jessica Moe. 2020. Available online: https://www.bcemergencynetwork.ca/lounge/denying-ambulance-transport-post-overdose/?unapproved=201109&moderation-hash=343f8c52b7dfb466c666d0e233a8ed43#comment-201109 (accessed on 10 November 2022).
- Martin, R.A.; Duk, D.; Holcombe, J.; Buccheit, R.; Mendiratta, A.; Whittle, J.S. Exploring Barriers to Implementing an Emergency Medical Services Naloxone Leave Behind Program. J. Emerg. Med. 2022. [Google Scholar]
- Williams, B.L.; Earl, B.M. Measurement of Empathy Levels in Undergraduate Paramedic Students. Prehospital Disaster Med. 2013, 28, 145–149. [Google Scholar] [CrossRef]
- Kus, G.; Wilson, B. Exploring empathy levels among Canadian paramedic students. Faculty Staff. Publications - Public. Safety. 2018, 33. [Google Scholar] [CrossRef]
- Pegano, R.; Ricketts, J.B. Empathy levels in Canadian paramedic students: A longitudinal study. Fac. Staff. Publ. Public Saf. 2018, 11, 1492–1488. [Google Scholar] [CrossRef]
- Kus, L. Exploring empathy levels among Canadian paramedic students. Int. J. Paramed. Pract. 2018. [Google Scholar] [CrossRef]
- Batt, A. Do we preach what we practice? The development of competency frameworks in healthcare professions. Thesis. 2017.
- Batt, A.M.; Williams, B.; Brydges, M.; Leyenaar, M.; Tavares, W. New ways of seeing: Supplementing existing competency framework development guidelines with systems thinking. Adv. Health Sci. Educ. Theory Pract. 2021, 26, 1355–1371. [Google Scholar] [CrossRef] [PubMed]
- Batt, A.; Poirier, P.; Bank, J.; Bolster, J.; Bowles, R.; Donelon, B.; Dunn, N.; Essington, T.; Johnston, W. Developing the National Occupational Standard for Paramedics in Canada - Update 1. 2022, 45, 6–8.
- Substance Abuse and Mental Health Services Administration (US); Office of the Surgeon General (US). Facing Addiction in America: The Surgeon General's Report on Alcohol, Drugs, and Health [Internet]. Washington (DC): US Department of Health and Human Services. 2016 Nov. CHAPTER 7, VISION FOR THE FUTURE: A PUBLIC HEALTH APPROACH. Available online: https://www.ncbi.nlm.nih.gov/books/NBK424861/ (accessed on 10 November 2022).
- McNaughton, C. Transitions through homelessness, substance use, and the effect of material marginalization and psychological trauma. Drugs Educ. Prev. Policy 2009, 15, 177–188. [Google Scholar] [CrossRef]
- American Academy of Orthopaedic Surgeons; Pollak, A. N.; Elling, B.; Aehlert, B. Nancy Caroline's emergency care in the streets, 8th ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2018. [Google Scholar]
- Paramedic Association of Canada. National Occupational Competency Profile for Paramedics [Internet]. 2011. Available online: https://paramedic.ca/documents/2011-10-31-Approved-NOCP-English-Master.pdf (accessed on 10 November 2022).
- Bessen S, Metcalf SA, Saunders EC; et al. Barriers to naloxone use and acceptance among opioid users, first responders, and emergency department providers in New Hampshire, USA. Int. J. Drug Policy. 2019, 74, 144–151. [Google Scholar] [CrossRef]
- Kruis, N.E.; McLean, K.; Perry, P. Exploring first responders’ perceptions of medication for addiction treatment: Does stigma influence attitudes? J Subst Abuse Treatment. 2021, 131. [Google Scholar] [CrossRef]
- Bowen, G.A. Document Analysis as a Qualitative Research Method. Qual. Res. J. 2009, 9, 27–40. [Google Scholar] [CrossRef]
- O'Leary. The Essential Guide to Doing Your Research Project. Thousand Oaks, CA: SAGE Publications, Inc. 2014.
- Cleland, J.; MacLeod, A.; Ellaway, R.H. CARDA: Guiding document analyses in health professions education research. Med. Educ. 2023, 57, 406–417. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis, Qualitative Research in Sport. Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16. [Google Scholar] [CrossRef]
- Mayer, S.; Boyd, J.; Collins, A.; Kennedy, M.C.; Fairbairn, N.; McNeil, R. Characterizing fentanyl-related overdoses and implications for overdose response: Findings from a rapid ethnographic study in Vancouver, Canada. Drug Alcohol. Depend. 2018, 1, 69–74. [Google Scholar] [CrossRef]
- Ciccarone, D. Fentanyl in the US heroin supply: A rapidly changing risk environment. Int. J. Drug Policy 2017, 46, 107–111. [Google Scholar] [CrossRef]
- Fairbairn, N.; Coffin, P.O.; Walley, A.Y. Naloxone for heroin, prescription opioid, and illicitly made fentanyl overdoses: Challenges and innovations responding to a dynamic epidemic. Int. J. Drug Policy 2017, 46, 172–179. [Google Scholar] [CrossRef] [PubMed]
- McCann, T.V.; Savic, M.; Ferguson, N.; Bosley, E.; Smith, K.; Roberts, L.; Emond, K.; Lubman, D.I. Paramedics' perceptions of their scope of practice in caring for patients with non-medical emergency-related mental health and/or alcohol and other drug problems: A qualitative study. PLoS ONE 2018, 13, 13. [Google Scholar] [CrossRef] [PubMed]
- Williams-Yuen, J.; Minaker, G.; Buxton, J.; et al. ‘You’re not just a medical professional’: Exploring paramedic experiences of overdose response within Vancouver’s downtown eastside. PLoS ONE 2020, 15, e0239559. [Google Scholar] [CrossRef] [PubMed]
- Karamouzian, M.; Kuo, M.; Crabtree, A.; Buxton, J.A. Correlates of seeking emergency medical help in the event of an overdose in British Columbia, Canada: Findings from the Take Home Naloxone program. Int. J. Drug Policy 2019, 71, 157–163. [Google Scholar] [CrossRef]
- Maguire BJ, O'Neill BJ. Emergency Medical Service Personnel's Risk From Violence While Serving the Community. Am. J. Public. Health 2017, 107, 1770–1775. [Google Scholar] [CrossRef]
- Hokee, M.Y.; Makkink, A.W.; Vincent-Lambert, C. Workplace violence against paramedic personnel: A protocol for a scoping review. BMJ Open 2023, 13, e067246. [Google Scholar] [CrossRef]
- Spelten, E.; van Vuuren, J.; O’Meara, P. Workplace violence against emergency health care workers: What Strategies do Workers use? BMC Emerg. Med. 2022, 22, 78. [Google Scholar] [CrossRef]
- Murray, R.M.; Davis, A.L.; Shepler, L.J. A Systematic Review of Workplace Violence Against Emergency Medical Services Responders. NEW SOLUTIONS A J. Environ. Occup. Health Policy 2020, 29, 487–503. [Google Scholar] [CrossRef]
- Government of Canada. Stigma: Why Words Matter [Internet]. 2022. Available online: https://www.canada.ca/content/dam/hc-sc/documents/services/publications/healthy-living/stigma-why-words-matter.pdf (accessed on 10 November 2022).
- Canadian Centre on Substance Use and Addiction. Available online: https://www.ccsa.ca/sites/default/files/2019-09/CCSA-Language-and-Stigma-in-Substance-Use-Addiction-Guide-2019-en.pdf (accessed on 10 November 2022).
- Ellis, K.; Walters, S.; Friedman, S.R.; Ouellet, L.J.; Ezell, J.; Rosentel, K.; Pho, M.T. Breaching Trust: A Qualitative Study of Healthcare Experiences of People Who Use Drugs in a Rural Setting. Front. Sociol. 2020, 10, 593925. [Google Scholar] [CrossRef]
- MedPro. Nonverbal Communication as an Essential Element of Patient-Centred Care. Available online: https://www.medpro.com/nonverbal-communication-patient-centered-care (accessed on 10 November 2022).
- Partnership to End Addiction. Words Matter: The Language of Addiction. Available online: https://drugfree.org/article/shouldnt-use-word-addict/ (accessed on 10 November 2022).
- Canadian Public Health Association. Language Matters [Internet]. 2019. Available online: https://www.cpha.ca/sites/default/files/uploads/resources/stbbi/language-tool-e.pdf (accessed on 10 November 2022).
- Lavalley, J.; Kastor, S.; Tourangeau, M. Western Aboriginal Harm Reduction Society; Goodman A, Kerr T. You just have to have other models, our DNA is different: The experiences of indigenous people who use illicit drugs and/or alcohol accessing substance use treatment. Harm Reduct. J. 2020, 24, 19. [Google Scholar] [CrossRef]
- Agata MP Atayde Sacha, C. Hauc, Lily G. Bessette, Heidi Danckers & Richard Saitz (2021) Changing the narrative: A call to end stigmatizing terminology related to substance use disorders. Addict. Res. Theory 2021, 29, 359–362. [Google Scholar]
- Brown, G.; Crawford, S.; Perry, G.E. Achieving meaningful participation of people who use drugs and their peer organizations in a strategic research partnership. Harm Reduct. J. 2019, 16, 37. [Google Scholar] [CrossRef] [PubMed]
- Claborn, K.R.; Creech, S.; Whittfield, Q.; Parra-Cardona, R.; Daugherty, A.; Benzer, J. Ethical by Design: Engaging the Community to Co-design a Digital Health Ecosystem to Improve Overdose Prevention Efforts Among Highly Vulnerable People Who Use Drugs. Front. Digit. Health 2022, 26, 880849. [Google Scholar] [CrossRef] [PubMed]
- Ti, L.; Tzemis, D.; Buxton, J. Engaging people who use drugs in policy and program development: A review of the literature. Subst. Abus. Treat. Prev. Policy. 2012, 7, 47. [Google Scholar] [CrossRef] [PubMed]
- Rowland, P.; Kumagai, A.K. MD. K. MD. Dilemmas of Representation: Patient Engagement in Health Professions Education. Acad. Med. 2018, 93, 869–873. [Google Scholar] [CrossRef]
- Souleymanov, R.; Kuzmanović, D.; Marshall, Z.; et al. Ethics Community-Based Res. People Who Use Drugs: Results A Scoping. Rev. BMC Med. Ethics. 2016, 17, 25. [Google Scholar]
- Clemmons. Using the Intended–Enacted–Experienced Curriculum Model to Map the Vision and Change Core Competencies in Undergraduate Biology Programs and Courses. CBE Life Sci. Educ. 2022, 21, 6. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Word Cloud for Theme One.
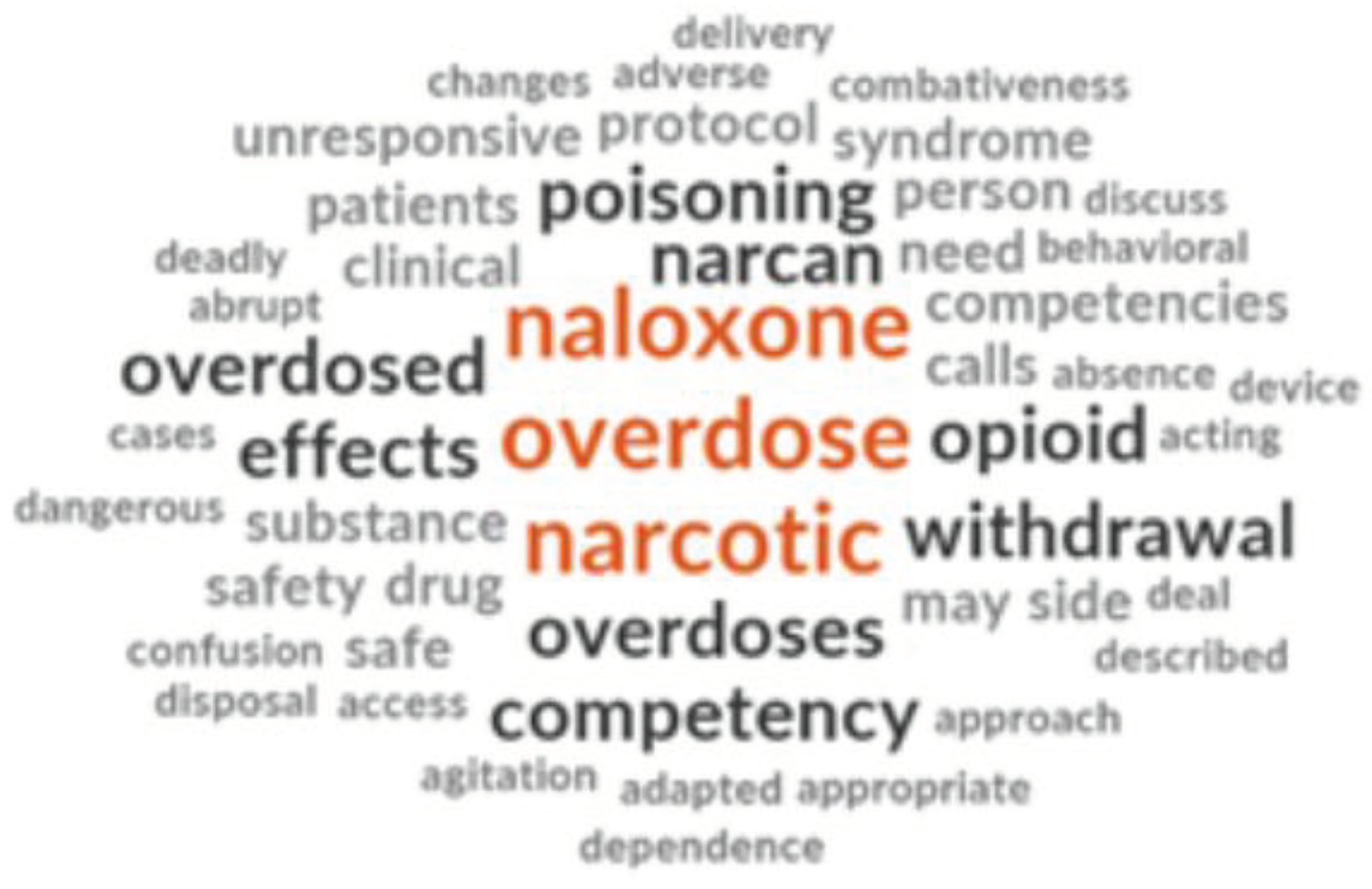
Figure 5.
Word Cloud for Theme Four.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



