
Submitted:
05 October 2023
Posted:
09 October 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
COVID-19 has rapidly spread worldwide since December 2019. During the pandemic, SARS-CoV-2 repeatedly mutated from Alpha to Omicron. The severity and mortality are related to age, sex, and underlying diseases (respiratory, cerebrovascular, cardiovascular, metabolic, cancer, and immune diseases). We retrospectively studied 44 hospitalized stroke patients infected with the SARS-CoV-2 Omicron variant. The mortality rate of hospitalized stroke patients with COVID-19 was 6 (13.6%). The cause of death was coagulopathy in 3 cases of ischemic stroke. High modified Rankin Scale score(mRS)of stroke patient was correlated with severity of COVID-19. The timing of vaccination is inversely correlated with COVID-19 severity. In conclusion, stroke patients with COVID-19 have high mortality rates attributed to coagulopathy. Stroke patients with high mRS scores are more likely to develop severe COVID-19. In high mRS scores, therapy for severe COVID-19 should be administered.
Keywords:
Stroke
; COVID-19
; SARS-CoV-2 Omicron variant
; modified Ranking scale
; coagulopathy
1. Introduction
COVID-19 is an infectious disease caused by SARS-CoV-2 virus. It spread rapidly worldwide since December 2019, leading to an unprecedented pandemic. During the pandemic, SARS-CoV-2 repeatedly mutated from Alpha to Omicron [1].
The novel coronavirus SARS-CoV-2 belongs to the Betacoronavirus family and is a single-stranded RNA virus with an envelope [2]. Previously, coronaviruses that infected humans, including human coronavirus (hCoV)-OC43, hCoV-HKU, and hCoV-229E, caused only mild cold-like symptoms [3]. However, SARS coronavirus (SARS-CoV) in 2003 and Middle East Respiratory Syndrome coronavirus (MERS-CoV) in 2012 were highly pathogenic and caused severe respiratory symptoms.
SARS-CoV originated in China and spread worldwide when infected individuals traveled on airplanes. The mortality rate for those infected with the virus was approximately 10%. In contrast, MERS-CoV originated in the Arabian Peninsula and had a mortality rate of 35% [4]. These two viruses are believed to have had intermediate animal hosts before infecting humans—bats for SARS-CoV and camels for MERS-CoV.
The source of SARS-CoV-2 remains unclear. However, the coronavirus RaTG13, with which it shares over 96% genetic similarity, has been isolated from bats. This finding suggests that bats may also have been an intermediate host for SARS-CoV-2 infection in humans [5]. SARS-CoV-2 also closely resembles SARS-CoV structurally. Both viruses have a membrane-spanning Spike (S) protein on their surfaces [6]. Infection occurs when the S protein binds to the host cell receptor angiotensin-converting enzyme 2 (ACE2) and enters the cell.
The S protein consists of a receptor-binding domain (RBD) in the S1 region and a fusion-promoting S2 region. The latter facilitates fusion between the virus membrane and the host cell membrane. This membrane fusion is activated by cleavage of the S1 and S2 regions, mediated by host cell proteases that include transmembrane protease serine 2 (TMPRSS2) and cathepsins. Infection can occur through one of two pathways, either involving the cell surface or the late endosomes. TMPRSS2-mediated cleavage of the S protein is crucial for the cell surface pathway; it is induced by furin, which is highly expressed in the cardiovascular system [6]. Consequently, serine protease inhibitors can inhibit SARS-CoV-2 entry into cultured cells. Proteases, like elastase, produced by neutrophils can cause structural changes in S proteins, suggesting a role for inflammatory cells during SARS-CoV-2 infection. After the internalization of ACE2 in the late endosome pathway, the S protein undergoes a structural change induced by proteases, which is accompanied by a decrease in pH within the endosome. Neuropilin-1 has been identified as a coreceptor for infection and contributes to enhanced viral entry [7].
In addition to the initial cold-like symptoms, patients with COVID-19 often have taste and smell abnormalities. This disease is characterized by inflammation of the respiratory system. Severe pneumonia in patients with COVID-19 can lead to acute respiratory distress syndrome (ARDS), which can be fatal. ARDS in patients with COVID-19 is characterized by diffuse alveolar damage. The interaction between SARS-CoV-2 and the ACE2 receptor is a crucial factor in determining the tissue tropism of the virus and its progression from infection to severe disease. ACE2 is widely distributed in the tissue of the respiratory and circulatory systems, including airway and alveolar epithelial cells and vascular endothelial cells. When SARS-CoV-2 enters the nasal passages infects cells in the nasal epithelium and then in the airway epithelium. High expression of ACE2 and TMPRSS2 has been observed in nasal and airway ciliated epithelial cells and in type II alveolar epithelial cells. Once infection has been established in the upper respiratory tract and the virus transitions to the lower respiratory tract, it leads to pneumonia. Importantly, ACE2 is highly expressed in vascular endothelial cells. The severity of COVID-19 disease increases due to infection of vascular endothelial cells, which subsequently leads to pulmonary vascular inflammation, thrombosis, angiogenesis, and other complications. An increase in blood D-dimer level is correlated with disease severity. Vascular damage is involved in vasculitis and thrombosis in COVID-19 patients [8].
The interferon (IFN) pathway plays an important role in viral defense. However, dysfunction of the IFN pathway is observed in severe COVID-19 disease, and excessive IFN production exacerbates pneumonia caused by COVID-19 infection. During the early stages of viral infection, both Type I (IFN-α, IFN-β) and Type III (IFN-λ) IFNs are expressed. This leads to induction of IFN-stimulated genes (ISGs), which activate various immune cells, causing migration to the site of infection. This migration is facilitated by chemokine secretion [9].
Expression of genes associated with chemokines and inflammatory cytokines significantly increases in SARS-CoV-2 infection, while ISG expression has been reported to be low [10]. In patients with COVID-19, serum concentrations of inflammatory cytokines like IL-6, CCL8, and CXCL8 increase, while those of IFN-β and IFN-λ remain low. Furthermore, older males have a higher risk for progression to severe disease; anti-IFN antibodies have been detected at a higher rate in males. These findings suggest that the presence of anti-IFN antibodies may be a factor contributing to disease severity [11]. In other words, inflammatory cytokines increase leading to a cytokine storm.
In contrast, higher levels of type I and III IFNs in the lungs of patients with COVID-19 are associated with a higher mortality rate [12]. Furthermore, the IFN pathway induces expression of ACE2 [16]. Dysfunction of the IFN pathway in response to SARS-CoV-2 infection, consequently, triggers a systemic cytokine storm. A cytokine storm can cause increased vascular permeability, hyperactivation of the coagulation-fibrinolysis system, disseminated intravascular coagulation (DIC), ARDS, and respiratory failure [13]. In contrast, neutralizing antibodies against IL-6 are effective.
ACE2 is the receptor for SARS-CoV-2 but also functions as the enzyme that converts angiotensin II to angiotensin-(1-7) [14]. ACE2 expression in the lungs decreases during SARS-CoV-2 infection; its expression has been reported to decrease in hamsters infected with SARS-CoV-2, and replenishing ACE2-like enzymes is associated with improvement in COVID-19 pneumonia. Therefore, increasing ACE2 enzymatic activity or inhibiting the RAS system may be effective in improving symptoms of ARDS caused by SARS-CoV-2 infection. Administration of ARBs or ACEi improves the prognosis of patients with COVID-19. In addition, low-molecular-weight agonists of angiotensin II type 2 receptors decrease the severity of COVID-19 [15].
Regarding the clinical course, the incubation period of SARS-CoV-2 infection ranges from 2–14 days, with an average length of approximately five days. Common symptoms of COVID-19 are fever, cough, sore throat, muscle aches, joint pain, headache, and chest pain; However, these symptoms are not specific to COVID-19. More specific symptoms are loss of taste and smell. In the first week after symptom onset, patients with COVID-19 have symptoms resembling those of a typical upper respiratory tract infection. Subsequent development of pneumonia can cause such symptoms as shortness of breath and difficulty breathing, while rapid breathing and cyanosis are observed in severe cases. Shock with low blood pressure and disturbances in consciousness can occur in the presence of a cytokine storm. Thrombosis can cause a stroke or myocardial infarction. If pulmonary embolism occurs, there may be rapid deterioration in respiration.
Risk factors for severe COVID-19 disease are advanced age and underlying medical conditions, including cardiovascular disease, heart failure, cardiac arrhythmias, diabetes, cancer, and chronic respiratory diseases. Severe cases of COVID-19 are more common in males, smokers, patients with peripheral artery disease or chronic obstructive pulmonary disease, and certain other medical conditions. Severe cases are less common in individuals under the age of 40 [16]. COVID-19 outbreaks have been reported in elder care facilities, where the disease poses a higher risk of severe disease for individuals with underlying medical conditions. Infection and mortality rates were elevated due to these outbreaks [17].
During the COVID-19 pandemic, 80% of affected individuals experienced mild symptoms and recovered naturally. Treatment was primarily focused on the 20% of individuals who developed moderate-to-severe disease. However, antiviral drugs that suppress viral replication could be used for approximately one week after onset of COVID-19, when it typically involves cold-like symptoms and loss of smell and taste. Additionally, approximately 20% of infected individuals experience pneumonia and progression to severe disease due to an excessive inflammatory response. The current approach to treating patients with moderate-to-severe disease involves combined use of antiviral and anti-inflammatory drugs. It has become common to add anticoagulant drugs like heparin to treat coagulopathy [16].
COVID-19 is characterized by respiratory syndrome and coagulopathy, including myocardial and cerebral infarctions. A major type of cerebral infarction in COVID-19 is large vessel occlusion (LVO) [18]. According to symptoms, oxygen saturation, and underlying diseases, COVID-19 patients are classified into mild, moderate, and severe. Most patients infected with COVID-19 are classified as mild cases. Occasionally, they are classified as severe and result in death. The severity and mortality of COVID-19 are related to age, sex, and underlying diseases (respiratory, cerebrovascular, cardiovascular, metabolic, cancer, and immune diseases)[19]. The clinical features of stroke patients infected with the SARS-CoV-2 Omicron variant is not fully known. In addition, the features and mechanisms of coagulopathy and respiratory syndromes associated with COVID-19 in stroke patients have scarcely been clarified [20]. Furthermore, the severe risk of COVID-19 in stroke patients remains unknown [21]. Therefore, in our study, we present the clinical features of hospitalized patients infected with the Omicron variant and propose appropriate management of stroke patients diagnosed with COVID-19.
2. Materials and Methods
2.1. Stroke Patients Infected with COVID-19
In this study, we retrospectively examined the clinical features of hospitalized stroke patients infected with the SARS-CoV-2 Omicron variant at our hospital from November 2022 to February 2023. Investigated variables are as follows: number, sex, and age of hospitalized stroke patients infected with the SARS-CoV-2 Omicron variant; stroke type and subclassification; symptoms; complications; drugs used for COVID-19; times of COVID-19 vaccination; median days from onset of stroke to infection with COVID-19; modified Rankin scale score (mRS) on COVID-19 onset; severity and mortality of COVID-19; images of a representative mortalized case. Furthermore, correlation between severity of COVID-19 and the following surveyed values were analyzed. The surveyed values are as follows: age, over 80 years or under ; sex, male of female; period from stroke to COVID-19 onset, over 50 days or under; times of vaccination; mRS; stroke type, ischemic or hemorrhagic; and subtype of ischemic stroke, atherosclerotic, cardiogenic, or lacunar.
2.2. Statistics
The data were analyzed using Chi-square test or Mann–Whitney U-test, as appropriate. The criterion for significant differences was p<0.05.
2.3. Ethics
Written informed consent for the publication of research details and clinical images was obtained from the patients. This study was approved by the hospital’s Institutional Review Board (No.2023-2).2.3.
3. Results
3.1. Characteristics of the Hospitalized Stroke Patients with COVID-19
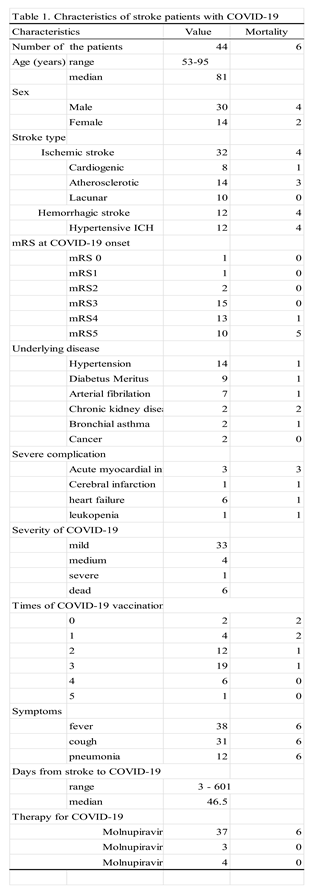
Forty-four stroke patients at our hospital were infected with the SARS-CoV-2 Omicron variant between November 2022 and February 2023. The age of the 44 patients ranged from 53 to 95 years, with a median age of 81 years. The study population consisted of 30 males and 14 females. The type of stroke was ischemic in 32 patients (cardiogenic, 8; atherosclerotic, 14; lacunar, 10) and hemorrhagic in 14 patients who were all hypertensive. The mRS scores at COVID-19 onset was mRS0, 1; mRS1, 1; mRS2, 2; mRS3, 15; mRS4, 13; mRS5, 10, with a median of 4. Underlying diseases included hypertension (n = 14), diabetes mellitus (n = 9), arterial fibrillation (n = 7), chronic kidney disease (n = 2), bronchial asthma (n = 2), and cancer (n = 2). Major complications with COVID-19 were acute myocardial infarction, 3 ; cerebral infarction,1; and severe leukopenia, 1. The severity of COVID-19 was mild: 33 moderate; 4 severe; 1 dead; and 6 severe. Six of 7 severe cases were dead. The mortality rate of post-stroke patients with COVID-19 is 13.6%. The number of COVID-19 vaccinations was as follows: none, 2; once, 4; twice, 12; 3; 19; 4; 6; 5; and 1. Hospitalized stroke patients were easily infected with COVID-19 regardless of vaccination time. Symptoms included fever (n = 38), cough (n = 31), pneumonia (n = 12), heart failure (n = 6), and leukopenia (n = 1). The period from stroke to COVID-19 ranged from 3 to 601 days, with a median of 46.5 days. The therapy for COVID-19 was molnupiravir only (n=37), molnupiravir and dexamethasone (3), and molnupiravir, dexamethasone, and anti-coagulant (n=4).
3.2. Mortalized Patients with COVID-19
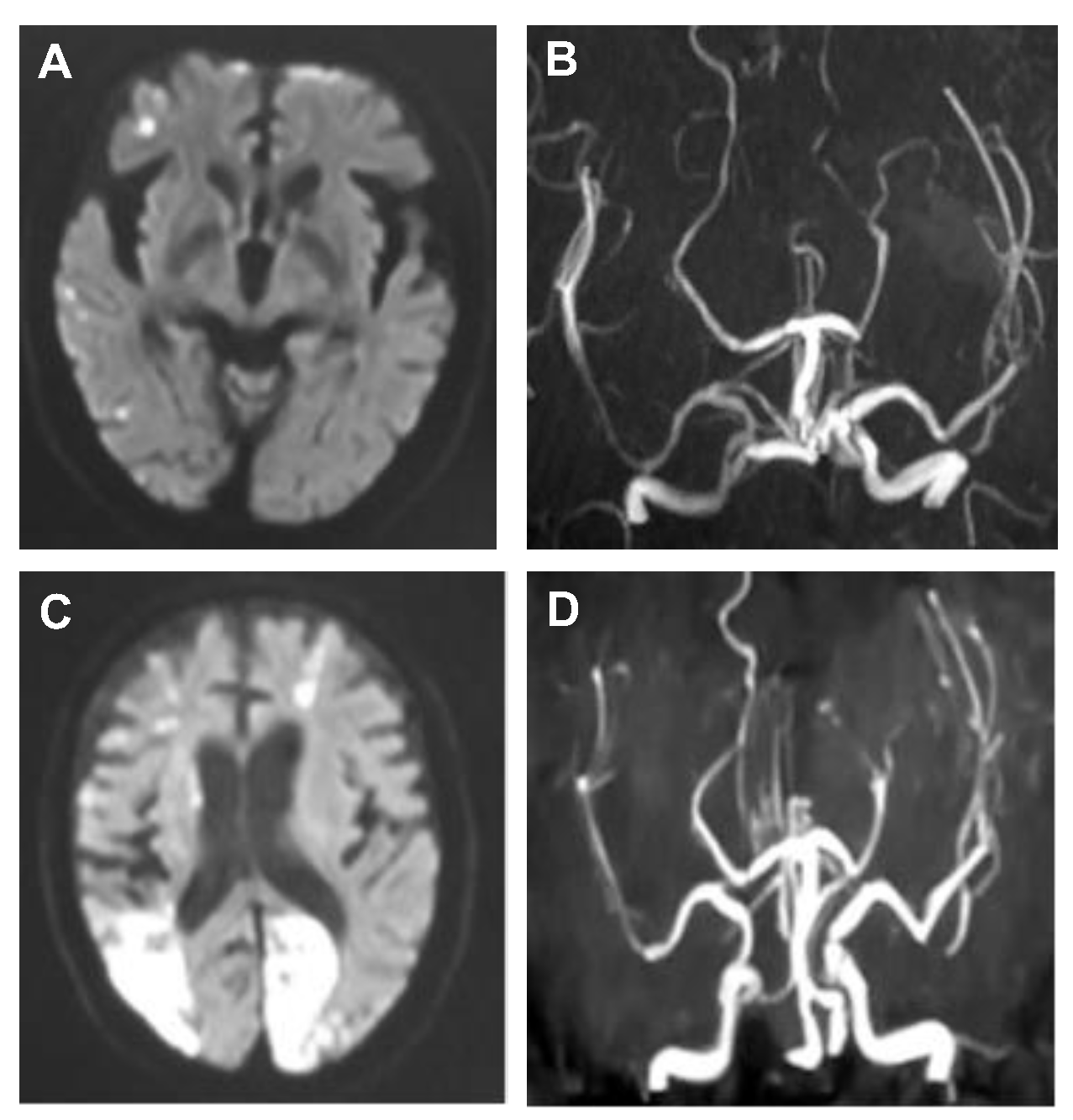
Among stroke patients with COVID-19, six died (mortality ratio, 13.6%), as s hown in Table 3. The average age of the patients who died was 83.8 years, median, 85 years). Among the patients, there were 4 males and 2 females. The mRS score at the time of stroke occurrence was 5 in 5 of the 6 patients, and the remaining patient had an mRS score of 4. The average number of vaccine doses received was 1.2, with a median of one dose. The causes of death were as follows: 3 cases, pneumonia; myocardial infarction, 2 cases; and cerebral infarction with myocardial infarction, one. The stroke types were cerebral infarction (CI) in four patients (three atherosclerotic and one cardiogenic) and intracerebral hemorrhage in two. The underlying diseases included 2 cases of chronic kidney disease, 1 case each of diabetes mellitus, bronchial asthma, chronic heart failure, hypertension, and arterial fibrillation. The median duration from stroke to COVID-19 onset was 70 days. COVID-19 symptoms were present in all patients, including fever, cough, and pneumonia, with two patients showing pulmonary edema. Critical complications associated with COVID-19 included myocardial infarction in 3 of 6 cases, acute kidney injury in 1 case, two instances of LVO-type cerebral infarction in 1 case, and severe leukopenia (< 500/mm3) in 1 case. COVID-19 treatment consisted exclusively of molupiravir in all cases. One of the deceased patients experienced a significant decline in mRS score after contracting COVID-19 on the 11th day of hospitalization for cerebral infarction, leading to LVO-type cerebral infarctions 10 and 18 days after disease onset. MRI images are provided for reference.
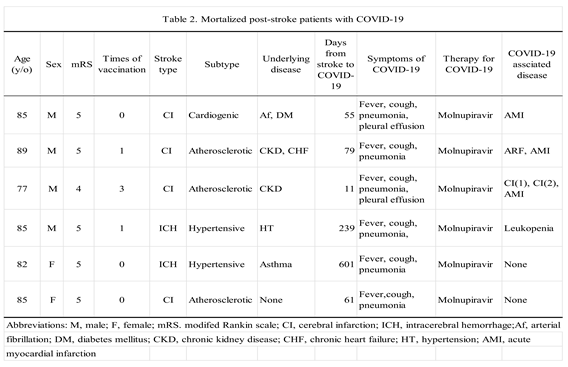
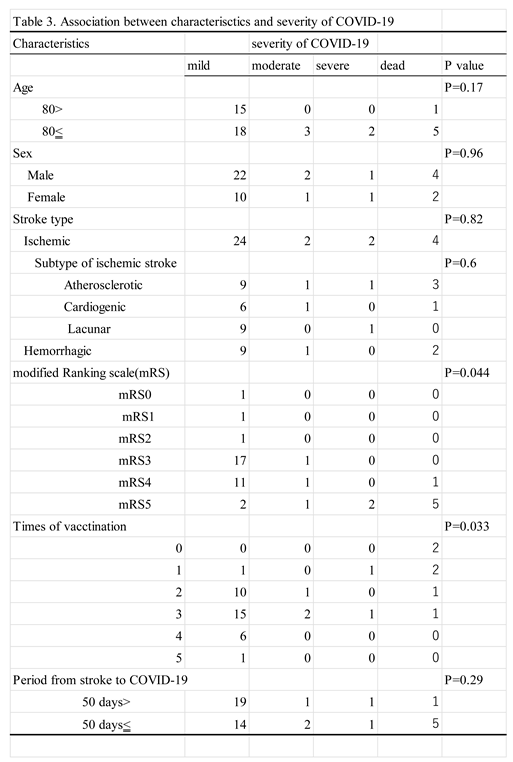
Figure 1.
MRIs of a dead ischemic stroke case following cerebral infarctions associated with COVID-19. A, Diffusion weighted image (DWI) at admission with cerebral infarction. Scattered high intensity spots in right cerebral hemisphere are seen. B, MR angiography at admission with cerebral infarction. A large vessel occlusion is not seen. C, DWI on 20 days after COVID-19 infection. High intensity areas in left occipital lobe and right parietal lobe are seen. D, A branch of left posterior cerebral artery and a branch of right middle cerebral artery are occluded.
Figure 1.
MRIs of a dead ischemic stroke case following cerebral infarctions associated with COVID-19. A, Diffusion weighted image (DWI) at admission with cerebral infarction. Scattered high intensity spots in right cerebral hemisphere are seen. B, MR angiography at admission with cerebral infarction. A large vessel occlusion is not seen. C, DWI on 20 days after COVID-19 infection. High intensity areas in left occipital lobe and right parietal lobe are seen. D, A branch of left posterior cerebral artery and a branch of right middle cerebral artery are occluded.
3.3. Association between Variables of the Patients
The mRS and severity of COVID-19 were found to be significantly correlated (P=0.044). These results demonstrate that stroke patients with higher mRS scores experienced more severe COVID-19 than those with lower mRS scores. The mean mRS of all patients with COVID-19 is mRS 3.5, whereas the mean mRS of severe cases and deaths is mRS 4.8. Significant differences between mRS of mortalized COVID-19 patients with stroke and mRS of survived patients were identified (P=0.015). There was no significant difference in the risk of COVID-19 severity between patients with ischemic stroke and those with hemorrhagic stroke, and there was no significant difference between ischemic stroke subtypes. The patients of 80 years or more did not show a significant difference in the risk of COVID-19 severity compared to the patients under 80 years (p=0.17). Similarly, there was no significant difference in COVID-19 severity between sexes (p=0.96). The number of days between stroke onset and COVID-19 manifestation, whether >50 days or < 50 days, did not result in a significant difference in the severity of COVID-19 (p=0.29). A significant association was found between the number of COVID-19 vaccine doses and disease severity (p=0.033), with fewer doses correlating to a higher risk of disease severity. Higher mortality rates have
been observed in patients with chronic kidney disease and bronchial asthma.
4. Discussion
The COVID-19 pandemic significantly transformed stroke care, with decreased numbers of patient visits, delayed medical consultations, and decreased use of recombinant tissue plasminogen activator intravenous therapy and mechanical thrombectomy. A higher mortality rate has been found in patients aged 70 and above who have underlying conditions such as myocardial infarction, a history of stroke, arrhythmia, and high blood pressure [21]. A history of stroke increased the likelihood of severe complications from COVID-19 by 2.55 times [22]. Patients with COVID-19 who had a history of stroke were more likely to develop ARDS and had lower discharge and higher mortality rates. Another report showed that the incidence rate of stroke was 4.6%, and stroke was more common in elderly patients with hypertension, diabetes, or a history of prior stroke [23]. Ischemic strokes were more common approximately two weeks after onset of COVID-19 symptoms [24]. Despite prophylaxis with low-molecular-weight heparin, a thrombotic complication rate of 7.7% was still observed. There was a higher prevalence of thromboses in the venous system and more cases of stroke than myocardial infarction in the arterial system [25].
A study that analyzed 9,358 COVID-19 patients under the age of 50 years using multinational databases showed that 33.2% of patients had severe COVID-19 that required hospitalization. Ischemic stroke occurred in 64 (0.7%) patients, and there was no significant gender difference [26]. Hypertension, diabetes, heart failure, nicotine dependence, obesity, chronic obstructive pulmonary disease, history of prior stroke, and renal failure were significantly more common among patients with stroke. These patients had a mortality rate of 15.6%, which was significantly higher than the mortality rate of 0.6% in non-stroke cases. Stroke associated with COVID-19 led to poor outcomes even in younger individuals [27]. COVID-19 was an independent risk factor for LVO (p=0.011) [28]. Patients with ischemic stroke who had a history of respiratory infection within one week had a higher proportion of LVO than patients without such a history, highlighting the need for further investigation into the specificity of LVO in COVID-19 infection [29]. Regarding laboratory data, D-dimer level was elevated, and tests for lupus anticoagulant and cardiolipin were occasionally positive.
A study of clinical types and outcomes found that the proportion of cryptogenic stroke was high (65.6%), and the in-hospital mortality rate was also high (63.6%) [30]. A study that investigated COVID-19 with stroke found that of 844 consecutive patients with COVID-19, 20 (2.4%) had ischemic stroke and 8 (0.9%) had hemorrhagic stroke. Patients with ischemic stroke had an average age of 64 years, with one patient (5%) below the age of 50 years. Among them, 95% of patients had hypertension and 60% had diabetes. The median time from onset of COVID-19 symptoms to stroke diagnosis was 21 days. Of the ischemic strokes, 40% were cardioembolic, 5% were lacunar, and 35% were cryptogenic [31]. A study investigating therapy for 174 patients with COVID-19 with stroke [32] found that 34 (19.7%) patients received intravenous thrombolysis and 21 (12.1%) patients underwent mechanical thrombectomy. There were 48 deaths (27.6%): 22 due to COVID-19 and 26 due to stroke. Among 96 patients who had disability information available, 49 (51%) had severe disability at discharge. The study also found that 31 of 2,132 (1.5%) patients with COVID-19 had a stroke while 3 of 1,516 (0.2%) patients with influenza had a stroke. The incidence of stroke in patients with COVID-19 was, therefore, approximately 7.5 times higher than in patients with influenza [33].
At the onset of stroke, SARS-CoV-2 enters cells through ACE2 receptors [34]. As previously described, ACE2 is expressed in the lungs, heart, kidneys, and vascular endothelium, making these organs potential targets for the virus [35]. Damage to the heart increases the risk of thrombosis, and the associated endothelial damage can lead to vascular diseases, including stroke. Since severe COVID-19 disease can lead to an uncontrolled immune response, resulting in a cytokine storm, coagulation abnormalities like elevated D-dimer levels may be a mechanism of stroke onset [36]. COVID-19 remained an independent risk factor for stroke (p=0.001) [37].
In patients with COVID-19, ischemic stroke is more common than hemorrhagic stroke, with rare cases of cerebral venous thrombosis. Stroke occurs more frequently than acute coronary syndrome or myocardial infarction. Patients with COVID-19 who have cardiovascular risk factors such as hypertension, diabetes, or a history of prior stroke are at higher risk of developing a stroke. Even when these events occur at a younger age, outcomes may be unfavorable. Thus, there may be an increase in the number of cases involving large vessel diseases. Many cases involve covert or cryptogenic ischemic strokes. Stroke can potentially occur in patients with both mild and severe COVID-19 disease. Elevated D-dimer levels were frequently observed. There is a potential association between lupus anticoagulant and anticardiolipin antibodies. A significant number of patients experienced poor clinical outcomes. These observations highlight the diverse and complex nature of how stroke can presents in patients with COVID-19.
In the present study we retrospectively studied the clinical features of 44 hospitalized patients with prior stroke who were infected with the Omicron variant of SARS-CoV-2 in a single hospital. All patients had a COVID-19-severity risk of cerebrovascular disease. The median patient age was 81 years. Most patients are at risk at advanced age[37]. Severe risk of COVID-19 of the patients younger than 80 years are not significantly lower than that of the patients 80 years and older (P=0.17), probably because of the small number of patients. Males are at severe risk of COVID-19 [37]. However, in this study, a significant difference in the risk of severe COVID-19 was not identified by sex. In addition, a significant difference in the risk of severe COVID-19 between the ischemic and hemorrhagic stroke types was not identified in this study. Furthermore, a significant difference between the subtypes of ischemic stroke was not recognized; however, the result might be derived from the small number of ischemic cases. In this study, a high mRS score at the onset of COVID-19 was significantly correlated with a severe risk of COVID-19, as a previous study showed a correlation between a high mRS score before stroke and a severe risk of COVID-19 [38]. Underlying diseases, except for cerebrovascular disease, are associated with severe risk factors for COVID-19, including renal disease, hypertension, diabetes mellitus, cardiovascular disease, and liver disease. In addition, history of smoking, current smoking, and obesity are associated with a high risk of mortality [37]. On the other hand, in this study, the following major complications were identified: acute myocardial infarction, acute cerebral infarction of LVO-type, acute heart failure, and leukopenia. A previous study reported the following cardiovascular diseases: acute heart failure and myocardial infarction [37]. Another study reported acute LVO in the brain[18]. In this study, the times of COVID-19 vaccination was significantly inversely correlated with a severe risk of COVID-19 (P=0.033) [39]. In this study, the median period from stroke onset to COVID-19 was 46.5 days. COVID-19 clusters in hospitals occurred during the median period. To date various guidelines for COVID-19 have been proposed. Oral nirmatrelvir/ritonavir and molnupiravir are used for outpatients or mildly hospitalized patients, whereas intravenous remdesivir and sotrovimab are mainly used for hospitalized patients with moderate or severe disease. Dexamethasone was administered in combination with these drugs. In this study, molnupiravir was administered to most patients. Patients who died also received molnupiravir, whereas those who were treated with remdesivir and dexamethasone survived. The risk reduction ratio for molnupiravir was 30%, whereas that for remdesivir was 87% [40]. High-risk reduction drugs such as remdesivir or sotrovimab should be used in patients with a highly severe risk of COVID-19.
The mortality rate of COVID-19 was reported to be over 40% among hospitalized patients before the emergence of the Omicron variant of SARS-CoV-2 [3]. Subsequently, this rate decreased to below 10% among hospitalized patients, with variations by country [41, 42]. In this study, among the 42 cases, six (13.6%) exhibited a mortality rate exceeding 10%, which can be attributed to the influence of stroke in patients. Severe complications, including myocardial infarction in 3 of 6 cases and cerebral infarction in 1 case, were observed in fatal cases, suggesting the involvement of COVID-19-associated coagulopathy [43]. Additional administration of anticoagulants such as heparin or direct oral anticoagulant and antiplatelet agents is considered necessary. Furthermore, all fatal cases received only molnupiravir as initial treatment for COVID-19, indicating the potential necessity of administering remdesivir and dexamethasone from the outset.
5. Limitations
We retrospectively studied hospitalized stroke patients infected with the SARS-CoV-2 Omicron variant at a single hospital. The small sample size of 44 cases in this study may have led to statistically insignificant results for some events that previous reports showed were statistically significant. Further studies are necessary to determine the complications associated with COVID-19 in stroke patients and appropriate therapy for COVID-19 in stroke patients.
6. Conclusion
In hospitalized stroke patients infected with the Omicron variant, the clinical features include a higher mortality rate compared to that of ordinary Omicron variant-infected patients. We also observed a correlation between high mRS at COVID-19 onset and disease severity. COVID-19-induced coagulopathy can lead to myocardial and cerebral infarction in patients with ischemic stroke, resulting in mortality. Therefore, the additional administration of anticoagulants and antiplatelet agents is necessary.
Author Contributions
Conceptualization, H.K. and K.M.; methodology, H.K. and S.M.; software, S.M.; validation, K.M. and Y.Y. and Z.Z.; formal analysis, S.K.; investigation, S.Y. and S.F; resources, S.T. and K.N.; data curation, Y.S. and S. T; writing—original draft preparation, H.K.; writing—review and editing, H.K and K.M.; visualization, K.M. and S.F.; supervision, S.F.; project administration, H.K and S.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the hospital’s Institution-al Review Board (No.2023-2) in 2023.
Informed Consent Statement
Written informed consent for the publication of research details and clinical images was obtained from the patients.
Data Availability Statement
The raw data supporting the results of this article will be made available by the authors without undue reservation.
Acknowledgments
We thank Ms. Sumie Takeshita, Ms. Akemi Ohno, and Ms. Tamami Nitta for nursing care; Ms. Masako Furukawa and Mr. Masahiro Ohdate for clerkship; Ms. Masako Sasaki and Ms. Hideko Haraoka and Ms. Masako Sasaki for technical assistance. .
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chow, E.J.; Uyeki, T.M.; Chu, H.Y. The effects of the COVID-19 pandemic on community respiratory virus activity. Nat. Rev. Microbiol. 2022, 21, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterization and epidemiology of 2019 novel coronavirus:implications for virus origins and receptor binding. Lancet. 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Ye, Z.W.; Yuan, S.; Yuen, K.S.; Fung, S.Y.; Chan, C.P.; Jin, D.Y. Zoonotic origins of human coronaviruses. Int. J. Biol. Sci. 2020, 16, 1686–1697. [Google Scholar] [CrossRef] [PubMed]
- Petrosillo, N.; Viceconte, G.; Ergonul, O.; Ippolito, G.; Petersen, E. COVID-19, SARS and MERS:are they closely related? Clin. Microbiol. Infect. 2020, 26, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Wu, Q.; Zhang, Z. Probable pangolin origin of SARS-CoV-2 associated with the COVID-19 outbreak. Curr. Biol. 2020, 30, 1346–1351. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020, 181, 281–292. [Google Scholar] [CrossRef]
- Daly, J.L.; Simonetti, B.; Klein, K. ; Chen KE, Williamson MK, Antón-Plágaro C, Shoemark DK, Simón-Gracia L, Bauer M, Hollandi R, et al. Neuropilin-1 is a host factor for SARS-CoV-2 infection. Science 2020, 370, 861–865. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Schoggins, J.W. Interferon stimulated genes:What do they all do? Annu. Rev. Virol. 2019, 6, 567–584. [Google Scholar] [CrossRef]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K. ; Panis. M., Sachs. D. et al. Wang TT, Schwartz RE, Lim JK, et al. Imbalanced host response to SARS-CoV-2 drives development of COVID-19. Cell 2020, 181, 1036–1045. [Google Scholar] [CrossRef]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.-H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Auto-antibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef]
- Broggi, A.; Ghosh, S.; Sposito, B.; Spreafico, R.; Balzarini, F.; Cascio, A.L.; Clementi, N.; De Santis, M.; Mancini, N.; Granucci, F.; et al. Type III interferons disrupt the lung epithelial barrier upon viral recognition. Science 2020, 369, 706–712. [Google Scholar] [CrossRef]
- Boudewijns, R.; Thibaut, H.J.; Kaptein, S.J.F.; Li, R.; Vergote, V.; Seldeslachts, L.; Van Weyenbergh, J.; De Keyzer, C.; Bervoets, L. ; Sharma S, et al. STAT2 signaling restricts viral dissemination but drives severe pneumonia in SARS-CoV-2 infected hamsters. Nat. Commun. 2020, 11, 5838. [Google Scholar]
- Kuba, K.; Imai, Y.; Penninger, J.M. Multiple Functions of Angiotensin-Converting Enzyme 2 and Its Relevance in Cardiovascular Diseases. Circ. J. 2013, 77, 301–308. [Google Scholar] [CrossRef]
- Semenzato, L.; Botton, J.; Drouin, J.; Baricault, B.; Vabre, C.; Cuenot, F.; Penso, L.; Herlemont, P.; Sbidian, E.; Weill, A. , et al. Antihypertensive drugs and COVID-19 risk:A cohort study of 2 million hypertensive patients. Hypertension 2021, 77, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Kutsuna, S. Coronavirus disease 2019 (COVID-19): research progress and clinical practice. Glob. Heal. Med. 2020, 2, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, N.; Hayakawa, K.; Terada, M.; Ohtsu, H.; Asai, Y.; Tsuzuki, S.; Suzuki, S.; Toyoda, A.; Suzuki, K.; Endo, M.; et al. Clinical Epidemiology of Hospitalized Patients With Coronavirus Disease 2019 (COVID-19) in Japan: Report of the COVID-19 Registry Japan. Clin. Infect. Dis. 2020, 73, e3677–e3689. [Google Scholar] [CrossRef] [PubMed]
- Altschul, D.J.; Esenwa, C.; Haranhalli, N.; Unda, S.R.; Ramos, R.d.L.G.; Dardick, J.; Fernandez-Torres, J.; Toma, A.; Labovitz, D.; Cheng, N.; et al. Predictors of mortality for patients with COVID-19 and large vessel occlusion. Interv. Neuroradiol. 2020, 26, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Mayer, C.; Woo, M.S.; Brehm, T.T.; Heyer, A.; Fischer, M.; Fischbach, F.; Bal, L.C.; Addo, M.M.; Kluge, S.; Thomalla, G.; et al. History of cerebrovascular disease but not dementia increases the risk for secondary vascular events during SARS-CoV-2 infection with presumed Omicron variant: a retrospective observational study. Eur. J. Neurol. 2023, 30, 2297–2304. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; He, Z.; Yang, J.; Guo, Q.; Weng, H.; Luo, J.; Gong, B.; Cui, W.; Ding, B.; Guo, J. Clinical Characteristics, Outcomes, and Risk Factors of Disease Severity in Patients With COVID-19 and With a History of Cerebrovascular Disease in Wuhan, China: A Retrospective Study. Front. Neurol. 2022, 12, 706478. [Google Scholar] [CrossRef]
- Aggarwal, G.; Lippi, G.; Henry, B.M. Cerebrovascular disease is associated with an increased disease severity in patients with Coronavirus Disease 2019 (COVID-19): A pooled analysis of published literature. Int. J. Stroke 2020, 15, 385–389. [Google Scholar] [CrossRef]
- Li, Y.; Li, M.; Wang, M.; Zhou, Y.; Chang, J.; Xian, Y.; Wang, D.; Mao, L.; Jin, H.; Hu, B. Acute cerebrovascular disease following COVID-19: a single center, retrospective, observational study. Stroke Vasc. Neurol. 2020, 5, 279–284. [Google Scholar] [CrossRef]
- Zhou, Y.; Li, W.; Wang, D.; Mao, L.; Jin, H.; Li, Y.; Hong, C.; Chen, S.; Chang, J.; He, Q.; et al. Clinical time course of COVID-19, its neurological manifestation and some thoughts on its management. Stroke Vasc. Neurol. 2020, 5, 177–179. [Google Scholar] [CrossRef]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.-D.; Sacco, C.; Bertuzzi, A.; et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef]
- Annie, F.; Bates, M.C.; Nanjundappa, A.; Bhatt, D.L.; Alkhouli, M. Prevalence and Outcomes of Acute Ischemic Stroke Among Patients ≤50 Years of Age With Laboratory Confirmed COVID-19 Infection. Am. J. Cardiol. 2020, 130, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Kihira, S.; Schefflein, J.; Mahmoudi, K.; Rigney, B.; Delman, B.N.; Mocco, J.; Doshi, A.; Belani, P. Association of Coronavirus Disease (COVID-19) With Large Vessel Occlusion Strokes: A Case-Control Study. Am. J. Roentgenol. 2021, 216, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Paganini-Hill, A.; Lozano, E.; Fischberg, G.; Perez Barreto, M.; Rajamani, K.; Ameriso, S.F.; Heseltine, P.N.; Fisher, M. Infection and risk of ischemic stroke: Differences among stroke subtypes. Stroke 2003, 34, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Yaghi S, Ishida K, Torres J, et al. SARS-CoV-2 and stroke in a New York healthcare system. Stroke 2020, 51, 2002–2011.
- Rothstein, A.; Oldridge, O.; Schwennesen, H.; Do, D.; Cucchiara, B.L. Acute Cerebrovascular Events in Hospitalized COVID-19 Patients. Stroke 2020, 51, E219–E222. [Google Scholar] [CrossRef]
- Ntaios, G.; Michel, P.; Georgiopoulos, G.; Guo, Y.; Li, W.; Xiong, J.; Calleja, P.; Ostos F.; González-Ortega, G.; Fuentes, B., et al. Characteristics and outcomes in patients with COVID-19 and acute ischemic stroke: The Global COVID-19 Stroke Registry. Stroke 2020 Sep;51: e254-e258.
- Merkler, A.E.; Parikh, N.S.; Mir, S.; Gupta, A.; Kamel, H.; Lin, E.; Lantos, J.; Schenck, E.J.; Goyal, P.; Bruce, S.S.; et al. Risk of Ischemic Stroke in Patients With Coronavirus Disease 2019 (COVID-19) vs Patients With Influenza. JAMA Neurol. 2020, 77, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H. ; Schroeder, S;, Krüger, N. ; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu,N.H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280. [Google Scholar]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, S.; Sinha, A.; Banach, M.; Mittoo, S.; Weissert, R.; Kass, J.S.; Rajagopal, S.; Pai, A.R.; Kutty, S. Cytokine Storm in COVID-19-Immunopathological Mechanisms, Clinical Considerations, and Therapeutic Approaches: The REPROGRAM Consortium Position Paper. Front. Immunol. 2020, 11, 1648. [Google Scholar] [CrossRef]
- Belani P, Schefflein J, Kihira S, Rigney B, Delman BN, Mahmoudi K, Mocco J, Majidi S, Yeckley J, Aggarwal A, et al. AJNR Am. J. Neuroradiol. 2020, 41, 1361–1364.
- Harrison, S.L.; Buckley, B.J.R.; Rivera-Caravaca, J.M.; Zhang, J.; Lip, G.Y.H. Cardiovascular risk factors, cardiovascular disease, and COVID-19: an umbrella review of systematic reviews. Eur. Hear. J. - Qual. Care Clin. Outcomes 2021, 7, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Martí-Fàbregas, J.; Guisado-Alonso, D.; Delgado-Mederos, R. , Martínez-Domeño, A. ; Prats-Sánchez, L.; Guasch-Jiménez, M.; Cardona, P.; Núñez-Guillén, A.; Requena, M.; Rubiera, M.; et al. Impact of COVID-19 infection on the outcome of patients with ischemic stroke. Stroke 2021, 52, 3908–3917. [Google Scholar]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Akinosoglou, K.; Schinas, G.; Gogos, C. Oral Antiviral Treatment for COVID-19: A Comprehensive Review on Nirmatrelvir/Ritonavir. Viruses 2022, 14, 2540. [Google Scholar] [CrossRef]
- Moura, E.C.; Cortez-Escalante, J.; Cavalcante, F.V.; Barreto, I.C.H.C.; Sanchez, M.N.; Santos, L.M.P. Covid-19: Temporal Evolution and Immunization in the Three Epidemiological Waves, Brazil, 2020-2022. Rev. Saude. Publica. 2022, 56, 105. [Google Scholar] [CrossRef] [PubMed]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical severity of, and effectiveness of mRNA vaccines against, Covid-19 from Omicron, Delta, and Alpha SARS-CoV-2 variants in the United States: Prospective observational study. B.M.J. 2022, 376, e069761. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.K.; Goh, C.; Leow, A.S.; A Tambyah, P.; Ang, A.; Yap, E.S.; Tu, T.M.; Sharma, V.; Yeo, L.L.; Chan, B.P.; et al. Abstract P89: Covid-19 and Ischemic Stroke: A Systematic Review and Meta-Summary of the Literature. Stroke 2021, 52. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



