
Submitted:
06 October 2023
Posted:
10 October 2023
You are already at the latest version
Abstract
The World Health Organization has highlighted the substantial impact of viral hepatitis on individuals, healthcare systems, and economies worldwide. This study's objective is to monitor disease notifications to assess their trend. Data were analyzed from infectious disease notifications detected in the Marche Region (Italy) and entered on the Nuovo Sistema Informativo Sanitario portal between 01/01/2012 and 31/12/2021. In this period there were 399 confirmed reports, of which 47,9% were for hepatitis A, 26,8% for B, 7% for C, 18,3% for E; 67.4% were male and the average age was 43.5 years old. The year with the highest peak was 2017, with 18% of reports, while the year with the lowest number was 2020 followed by 2021, with 3.8% and 4.5% respectively. Effective surveillance systems are key to combating the spread of hepatitis and reducing its impact, although they have been affected by the Sars-CoV-2 pandemic, with many cases remaining undetected.
Keywords:
viral hepatitis
; infectious diseases
; notification system
1. Introduction
Viral hepatitis is a major global health problem, affecting an estimated 290 million people worldwide [1]. The World Health Organization (WHO) has highlighted the substantial impact of viral hepatitis on individuals, healthcare systems, and economies [2]. There are five main types of viral hepatitis: A, B, C, D, and E. Hepatitis A and E are typically transmitted through the fecal-oral route, while hepatitis B, C, and D are transmitted through blood or body fluids. Hepatitis A and E are usually acute infections that resolve on their own, but hepatitis B, C, and D can become chronic and lead to serious liver damage, including cirrhosis and liver cancer [3]. Hepatitis B (HBV) infection stands as the primary contributor to chronic liver disease on a global scale, impacting a staggering 257 million individuals worldwide. This viral infection plays a pivotal role in approximately 54% of hepatocellular carcinoma (HCC) cases [4]. The initial worldwide hepatitis report, published in 2017, revealed that in the year 2015, the consequences of viral hepatitis infection resulted in the deaths of 1.4 million individuals [2]. The overwhelming majority, over 90% of this mortality, was attributed to cirrhosis and HCC, both of which are outcomes of chronic hepatitis B (CHB) and chronic hepatitis C (CHC) infections [5]. In 2015, the United Nations passed a resolution that advocated for targeted measures to address viral hepatitis as an integral component of the Agenda for Achieving Sustainable Development Goals by 2030. Subsequently, in 2016, the World Health Organization introduced its global hepatitis strategy, endorsed by all WHO Member States, aims to reduce new hepatitis infections by 90% and deaths by 65% between 2016 and 2030 [6,7]. This study’s objective is to monitor hepatitis notifications in the Marche Region, Italy to assess their trend.
2. Materials and Methods
Data were analyzed from infectious disease notifications detected in the Marche Region (Italy) and entered on the New Health Information System (NSIS) portal between 01/01/2012 and 31/12/2021. The NSIS represents the reference tool for quality, efficiency and appropriateness measures of the National Health Service (SSN), through the availability of information that, due to its completeness, consistency and timeliness, supports the Regions and the Ministry in the exercise of their functions and, in particular, the Ministry in its role as guarantor of the uniform application of the Essential Levels of Care (Livelli Essenziali di Assistenza - LEA) throughout the country [8]. NSIS was created, therefore, with the aim of making available, at a national and regional level, a wealth of data, rules and methodologies for measuring quality, efficiency, appropriateness and cost to support the governance of the SSN, the monitoring of LEA and health expenditure, shared among the various institutional levels and centered on the citizen [8]. For each patient, gender, age, nationality, reporting province, reporting facility and type of infectious disease were recorded. Data were recorded anonymously and the identity of the patients cannot be traced. Analyses have been performed with Microsoft Excel 16.77.1.
3. Results
Our study sample included 399 confirmed reports, of which 47.9% (n= 191) were for hepatitis A, 26.8% (n= 107) for B, 7.0% (n=28) for C and 18.3% (n=73) for E (Table 1). In the case of hepatitis A infections, 61.3% (n=117) of the cases were males, 94.2% (n=180) were of Italian nationality, with a mean age of 36.7 years. For hepatitis B, 74.7% (n=81) were males, 93.5% (n=100) had Italian nationality, and the mean age was 51.1 years and for hepatitis C, 64.3% (n=18) were males, 96.4% (n=27) were of Italian nationality, and the mean age was 44.7 years. Lastly, for hepatitis E, 72.6% (n=53) were males, 98.6% (n=72) were of Italian nationality, and the mean age was 56.1 years. Table 1
For all four types of hepatitis, the origin of the alert is mainly from the hospital, 81.7% (n=156) for hepatitis A, 93.5% (n=100) for hepatitis B, 67.9% (n=19) for hepatitis C and 87.7% (n=64) for hepatitis E (Table 2).
Looking at the reporting province, there is no homogeneity of reporting either geographically or in terms of infection (Table 2).
Overall, the year with the peak of notified cases was in 2017, with 18% of the total reports, while the year with the lowest number of notifications was 2020 followed by 2021, with 3.8% and 4.5% respectively (Figure 1).
The total number of notified cases tends to follow the rise and fall of hepatitis A cases which is the most numerous and the one with the highest magnitude of change. Figure 1
4. Discussion
Our study focused on monitoring hepatitis notifications to evaluate their characteristics and trends. In alignment with national epidemiological data [9], our findings indicate a higher incidence of hepatitis among men for both total and specific infections. Notably, the number of notified cases of hepatitis A experienced peaks in 2013 and 2017, attributed to outbreaks linked to mixed frozen berries in 2013 and an outbreak among men who have sex with men (MSM) following the pride festival in 2016 [10,11]. The implementation of mandatory hepatitis B vaccination for newborns and 12-year-old children (born in 1980) in Italy in 1991 under Law 165/1991 could have contributed to the higher mean age of notified hepatitis B cases [12]. Regarding hepatitis E, an increase in cases between 2018 and 2019 was documented in central Italy by Garbuglia et al.’s study on an outbreak [13]. The sharp decline in hepatitis cases in 2020 can be attributed to the SARS-CoV-2 pandemic, resulting in underreporting of infectious diseases across the board [14]. Furthermore, the majority of notifications originated from hospital settings, underscoring that new diagnoses are more frequent in hospitals where the serological status of patients is more frequently investigated to navigate various differential diagnoses. However, it’s important to acknowledge the limitations of this study. Data completeness could be an issue, potentially leading to an underestimation of hepatitis incidence in the Marche Region. Additionally, missing information on vaccination status, comorbidities, and other medical histories of patients impedes a comprehensive understanding of infected patients. Furthermore, knowledge of patients’ residency country or travel history could aid in distinguishing between imported and locally acquired infections.
5. Conclusion
Data highlights the need for targeted prevention strategies, screening programs for at-risk populations, advancements in diagnostics and therapeutics for effective treatment options, as well as ongoing efforts towards achieving elimination targets. In 2023, the Marche Region is actively promoting a hepatitis C screening campaign for individuals born between 1969 and 1989. Data from this campaign will provide a more accurate picture of hepatitis C serological status of Marche’s population.
Author Contributions
Conceptualization, CDG.M.; investigation, CDG.M., A.M., G.M. and LC.I.; data curation, C.F. and D.MdR.; writing—original draft preparation, CDG.M., C.F. and D.MdR.; writing—review and editing, C.F., A.P. and D.MdR.; supervision, F.F.; All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Global hepatitis report 2021. WHO. 2021. Available at: https://www.who.int/publications/i/item/WHO-HIV-2016.06 (accessed on 25 September 2023).
- Global hepatitis report 2017. WHO. 2017. Available at: https://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/ (accessed on 25 September 2023).
- European Association for the Study of the Liver. EASL clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2023, 70, 167–202. [Google Scholar]
- Global Burden of Disease Liver Cancer Collaboration; Akinyemiju, T.; Abera, S.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Global health sector strategy on viral hepatitis, 2016–2021. WHO; 2016. Available at: http://apps.who.int/iris/bitstream/10665/246177/1/WHO-HIV-2016.06-eng.pdf?ua51 (accessed on 25 September 2023).
- Lanini, S.; Easterbrook, P.J.; Zumla, A.; et al. Hepatitis C: global epidemiology and strategies for control. Clin Microbiol Infect 2016, 22, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Elimination of hepatitis by 2030. WHO. 2016. Available at: https://www.who.int/health-topics/hepatitis/elimination-of-hepatitis-by-2030#tab=tab_1 (accessed on 25 September 2023).
- Nuovo sistema informativo sanitario - NSIS. Ministero della Salute. 2012. Available at: https://www.salute.gov.it/portale/temi/p2_4.jsp?area=sistemaInformativo&tema=Piani,%20finanziamenti%20e%20monitoraggio%20del%20SSN (accessed on 25 September 2023).
- Epidemiology - SEIEVA data. Istituto Superiore di Sanità. 2023; Available at: https://www.epicentro.iss.it/en/hepatitis/data-seieva (accessed on 25 September 2023).
- Outbreak of hepatitis A infection in Italy and Ireland. ECDC. 2013. Available at: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/ROA-update_HAV_Italy_Ireland-final.
- Ndumbi Patricia, Freidl Gudrun S, Williams Christopher J, Mårdh Otilia, Varela Carmen, Avellón Ana, Friesema Ingrid, Vennema Harry, Beebeejaun Kazim, Ngui Siew Lin, Edelstein Michael, Smith-Palmer Alison, Murphy Niamh, Dean Jonathan, Faber Mirko, Wenzel Jürgen, Kontio Mia, Müller Luise, Midgley Sofie Elisabeth, Sundqvist Lena, Ederth Josefine Lundberg, Roque-Afonso Anne-Marie, Couturier Elisabeth, Klamer Sofieke, Rebolledo Javiera, Suin Vanessa, Aberle Stephan W., Schmid Daniela, De Sousa Rita, Augusto Gonçalo Figueiredo, Alfonsi Valeria, Del Manso Martina, Ciccaglione Anna Rita, Mellou Kassiani, Hadjichristodoulou Christos, Donachie Alastair, Borg Maria-Louise, Sočan Maja, Poljak Mario, Severi Ettore, Members of the European Hepatitis A Outbreak Investigation Team. Hepatitis A outbreak disproportionately affecting men who have sex with men (MSM) in the European Union and European Economic Area, June 2016 to May 2017. Euro Surveill. 2018, 23, 1700641. [Google Scholar] [CrossRef]
- LEGGE 27 maggio 1991, n. 1991. Available at: https://www.gazzettaufficiale.
- Garbuglia, A.R.; Bruni, R.; Villano, U.; Vairo, F.; Lapa, D.; Madonna, E.; Picchi, G.; Binda, B.; Mariani, R.; De Paulis, F.; D’Amato, S.; Grimaldi, A.; Scognamiglio, P.; Capobianchi, M.R.; Ciccaglione, A.R.; The Other Members Of The Hev Outbreak Working Group. Hepatitis E Outbreak in the Central Part of Italy Sustained by Multiple HEV Genotype 3 Strains, June-December 2019. Viruses 2021, 13, 1159. [Google Scholar] [CrossRef] [PubMed]
- Meadows, A.J.; Oppenheim, B.; Guerrero, J.; Ash, B.; Badker, R.; Lam, C.K.; Pardee, C.; Ngoon, C.; Savage, P.T.; Sridharan, V.; Madhav, N.K.; Stephenson, N. Infectious Disease Underreporting Is Predicted by Country-Level Preparedness, Politics, and Pathogen Severity. Health Secur. 2022, 20, 331–338. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Incidence of viral hepatitis notifications in the Marche Region (Italy) from 2012 to 2021.
Figure 1.
Incidence of viral hepatitis notifications in the Marche Region (Italy) from 2012 to 2021.
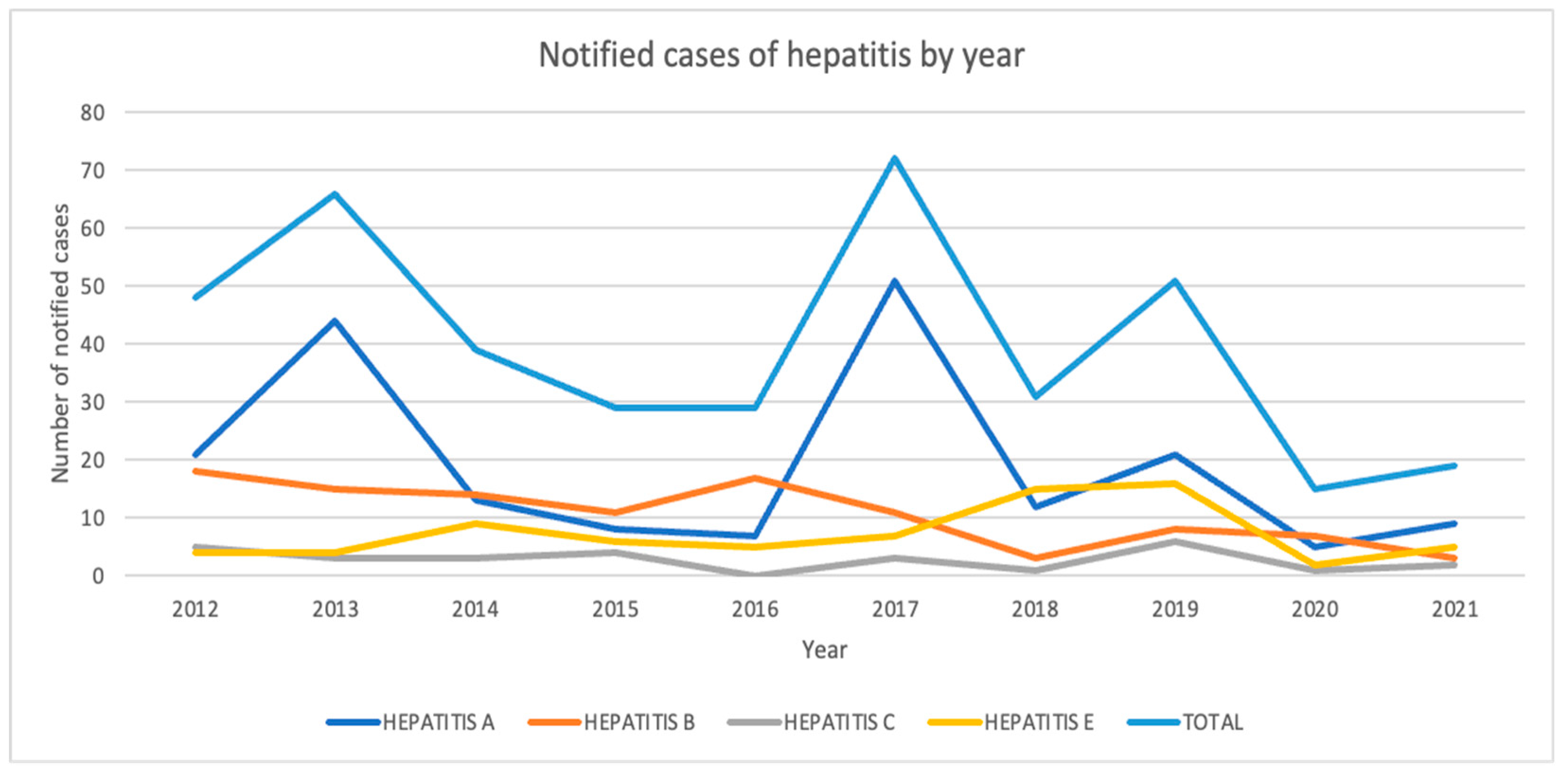

Table 1.
Descriptive analysis of patients characteristics.
| Hepatitis A | Hepatitis B | Hepatitis C | Hepatitis E | |
|---|---|---|---|---|
| Gender | n (%) | n (%) | n (%) | n (%) |
| Male | 117 (61.3) | 81 (75.7) | 18 (64.3) | 53 (72.6) |
| Female | 74 (38.7) | 26 (24.3) | 10 (35.7) | 20 (27.4) |
| Nationality | ||||
| Italian | 180 (94.2) | 100 (93.5) | 27 (96.4) | 72 (98.6) |
| Other | 11 (5.8) | 7 (6.5) | 1 (3.6) | 1 (1.4) |
| Total | 191 (47.9) | 107 (26.8) | 28( 7.0) | 73 (18.3) |
| Mean Age (years) | 36,7 | 50,1 | 44,7 | 56,1 |
Table 2.
Descriptive analysis of alert’s origin.
| Hepatitis A | Hepatitis B | Hepatitis C | Hepatitis E | |
|---|---|---|---|---|
| Facility | n (%) | n (%) | n (%) | n (%) |
| Hospital | 156 (81.7) | 100 (93.5) | 19 (67.9) | 64 (87.7) |
| Healthcare District | 35 (18.3) | 7 (6.5) | 9 (32.1) | 9 (12.3) |
| Province | ||||
| Pesaro Urbino | 45 (23.6) | 44 (41.1) | 7 (25.0) | 7 (9.6) |
| Ancona | 62 (32.5) | 28 (26.2) | 4 (14.3) | 32 (43.8) |
| Macerata | 54 (28.3) | 20 (18.7) | 11 (39.3) | 17 (23.3) |
| Fermo | 18 (9.4) | 12 (11.2) | 2 (7.1) | 10 (13.7) |
| Ascoli Piceno | 12 (6.3) | 3 (2.8) | 4 (14.3) | 7 (9.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



