
Submitted:
10 October 2023
Posted:
11 October 2023
You are already at the latest version
Abstract
The aim of this study was to evaluate the biomechanical changes of the cornea after wearing soft contact lenses (CLs) in healthy myopic patients measured with the Corvis ST® analyzer. This prospective, cross-sectional, single-center study was performed in twenty-two Caucasian patients aged between 19 and 24 years (20.64 ± 1.21 years) range). Five device-specific biomechanical parameters, central corneal thickness and intraocular pressure were measured prior to fitting and one month after CLs wear. Differences between the means of the DA Ratio and the standard deviation of the DA Ratio pre- and post-CLs wear were found to be significant (p value=0.002 in both cases). Significant differences were found between pre- and post-CLs wear values in CCT (p value=0.013). For all other biomechanical measures, no significant differences were observed before and after treatment. A significant association was found between changes in bIOP and classification according to changes in Int. Radius (p value = 0.047) and SSI (p value = 0.026) standard deviations. The corneal biomechanical indices provided by CST demonstrate that fitting of soft CLs is a safe optical compensation method for the stability of corneal stiffness. No significant differences were found pre- and post-CLs wear in the assessment of bIOP.
Keywords:
Myopia
; Soft contact lenses
; Corneal biomechanics
; Scheimpflug technology
; Corvis ST
1. Introduction
The cornea, together with the tear film, is the most anterior part of the eye, in front of the iris and the pupil [1]. It is the first optical interface of the visual system and is responsible for most of the refractive convergence power of the eye. It is the densest tissue in the body and most of the corneal nerves are sensory nerves, derived from the ophthalmic branch of the trigeminal nerve [2]. This transparent avascular tissue also acts as a barrier against trauma and microbial agents [1].
The shape of the cornea is a determining factor in ocular refraction, but is itself determined by its biomechanical properties. The cornea must be soft enough to expand into the spherical hemisphere, but rigid enough to hold its shape and resist intraocular pressure (IOP) [3]. Biological properties, such as healing responses and biomechanics, are essential in determining and maintaining corneal transparency, as well as geometric and optical properties [4].
Transparency of the corneal stroma depends mainly on the degree of spatial arrangement of the collagen fibrils, which have a narrow diameter and are closely grouped in a regular network. Collagen fibrils themselves are weak scatterers because their diameter is smaller than the wavelength of light and their refractive index is close to that of the ground substance. There is little difference in the diameter of the fibers and the distance between the anterior and posterior surfaces of the cornea. Research has shown that the cornea is a complex biomechanical complex and that intact corneal structural components are critical to overall corneal biomechanics [5].
Most biomechanical studies to date have focused on the stroma, which constitutes 90% of the total thickness of the cornea and is generally considered to be the primsry supporting layer of the cornea. Studies have demonstrated the complex nature of the stroma and the regular diameter and spacing of the collagen fibrils, as well as their influence on corneal transparency and biomechanical behavior [6].
Noteworthy, the cornea maintains a delicate and complex balance between stiffness, strength, elasticity and overall strength to withstand internal and external forces that constantly compress it, distort its shape or threaten its integrity. [7]. This is measured by corneal biomechanics, which has emerged as a research and development topic in modern ophthalmology due to its many potential applications [8]. Corneal biomechanics is the study of the structure of the cornea by defining physical and mathematical principles that can predict the dynamic response of the cornea to physiological and/or pathological conditions through behavioral patterns or model definitions of the corneal tissue. Explore. Corneal biomechanics is the science that deals with the balance and deformation of tissue subjected to any force. It studies the function and structure of the cornea and forms a basis for predicting its dynamic response in physiological and pathological conditions [2].
The capability to measure the biomechanical properties of the cornea in vivo is of great clinical importance as it helps to improve many treatment and management procedures that mechanically interact with or affect the eye. Examples include measuring IOP for effective glaucoma management [9], planning refractive surgery [10], determining keratoconus risk [11], and optimizing various protocols for collagen cross-linking treatments or evaluation [12], including preoperative evaluation for re-treatment of refractive surgery. , the mechanical interaction between the lens and the anterior segment is not currently considered in the selection of intracorneal ring implants or even in the design of soft contact lenses [13]. Additionally, corneal biomechanical analysis has been suggested as a potentially relevant factor in orthopedics, but the role of corneal biomechanical properties in predicting the correction obtained with this refractive compensation option is unclear [14].
Interest in the use of biomechanical principles in the cornea has increased significantly in recent years with the aim of better understanding corneal behavior and improving the safety and efficacy of various ocular treatments or refractive techniques [15].
In vivo evaluation of corneal parameters is essential to understand corneal behavior under physical stress. However, in clinical practice, it is not easy to accurately evaluate the behavior of the cornea under stress and use the results to estimate some mechanical properties of the cornea [15]. However, until recently, the evaluation of the biomechanical properties of the cornea was limited to ex vivo laboratory studies and mathematical models of the cornea [16].
There are still a limited number of techniques developed and tested to characterize corneal biomechanics with potential application in clinical practice. Two instruments are currently available to characterize the biomechanical properties of the cornea in clinical settings: the Ocular Response analyzer (ORA; Reichert Inc., Depew, NY) and the Corvis ST (CST, Oculus Optikgeräte GmbH, Wetzlar, Germany), based on the measurement of corneal deformation using the Scheimpflug technique. Both have unique parameters that describe corneal biomechanics, but their relationship to standard mechanical properties is unknown and is not associated with a specific biomechanical model. Therefore, there is inconsistency in the definition of some fundamental biomechanical parameters, such as viscosity or elasticity, to characterize the biomechanical properties of the cornea. As a result, comparative analysis between studies using different technologies is difficult [17].
The ORA was presented as the first equipment to assess the biomechanical behavior of the cornea in vivo at the 2005 ESCRS meeting (Lisbon, Portugal) [18]. The ORA is a modified non-contact tonometer (NCT) initially designed to provide more accurate IOP measurements through corneal biomechanical compensation. It analyzes the behavior of the cornea during bidirectional applanation induced by an air jet and generates estimates of corneal hysteresis (CH) and corneal resistance factor (CRF) along with a set of 36 waveform-derived parameters [16]. ORA combines an air puff with an infrared transmitter and receiver. This device can evaluate corneal deformation only indirectly based on infrared signals [19].
The photoelectric coherence detection system monitors the curvature of the cornea with a central diameter of 3.0 mm during a 20 ms measurement [20]. In this system, the máximum air pressure generated varies from the first stabilization event. The maximum pressure of the ORA is adjusted from test to test, so that eyes with early initial loading and typically low IOP receive a lower maximum pressure, and eyes with high IOP receive a larger maximum pressure bladder [21]. The measurement involves automatic alignment with the top of the cornea and triggers the airpuff. The measurement takes approximately 25 milliseconds (ms). The cornea deforms due to air pressure (internal phase) and the first flattening occurs when the pressure is recorded (P1). The cornea takes a concave shape, until the air pressure decreases, allowing the cornea to gradually return to its normal shape. During the exit phase, it undergoes a second delamination state, where the pressure (P2) is recorded again. Both abrasion events are recognized by peaks in the corneal reflex signal corresponding to two independent pressure values in the air puff pressure profile. These pressure measurements (P1 and P2) form the basis of the first generation variants reported from the original ORA program [18].
The average of the two applanation pressures was correlated with Goldmann tonometry results in an internal study with the aim of providing (linear) calibration coefficients for reporting intraocular pressure and CH in millimeters of mercury. The procedure has been described [20].
The CST, the analytical tool used in this study, was later introduced as NCT. This device uses an ultrahigh-speed (UHS) Scheimpflug camera to monitor the corneal response to air pressure pulses and uses the acquired image sequences to estimate IOP and strain response parameters. [16].
The CST has been commercially available since 2011 and is based on UHS dynamic Scheimpflug imaging technology. It measures IOP, central corneal thickness (CCT), and corneal biomechanical parameters by directly observing and imaging corneal deformation in response to a standard puff of air in real time [22]. The instrument is ergonomically designed with an adjustable head control and chin rest. The patient is positioned comfortably with the chin and forehead positioned appropriately. The patient is asked to focus on the central red LED (light emitting diode). A front camera with a keratometer-type projection system is installed to focus and align the corneal apex. The test is programmed to trigger automatically when synchronization with the first corneal Purkinje reflex is achieved. Manual triggering is also possible [4].
The UHS Scheimpflug camera uses more than 4,300 frames per second to monitor the corneal response to a collimated puff of air measured in a fixed profile with a symmetrical configuration and a fixed maximum internal pump pressure of 25 kPa. UHS Scheimpflug cameras are equipped with blue light LEDs (455 nm, no UV) and cover 8.5 mm horizontally with a slit. The exposure time is 30 ms and 140 digital images can be acquired. Each image has 576 pixels [4].
In addition to IOP, corrected IOP (corrected IOP based on the Dresden correction table) and CCT, the following parameters are measured: time to first (A1) and second (A2) lamination (time to reach first and second lamination, respectively), length A1 and A2 (length of the segment flatness in the Scheimflug image during first and second flattening), A1 and A2 velocities (velocity of corneal movement in inner and outer flattening), and features of the highest concavity, including time to reach maximum stress (hours), strain amplitude (DA), and distance between peaks Point of curvature (PD) and radius of curvature [22].
The development of new biomechanical principles of ocular structure is an emerging area of research in optometry and ophthalmology. This is a challenge that must be met in order to create more appropriate in vivo biomechanical models of the cornea and to define appropriate predictive models of corneal behavior. These tools will allow the clinician to predict the clinical outcomes of various ocular treatments before they are performed, thus allowing for their optimization [23].
On the other hand, adaptation of contact lenses (CLs) on the ocular surface causes a multitude of physical corneal changes, modifying its curvature and tear quality. From the first hours of wear, corneal alterations are recorded that lead to the appearance of allergic, infectious, anatomical and metabolic phenomena that result in discomfort or discomfort for the wearer, with infection being the most serious complication [24]. However, there are limited data on corneal biomechanical changes after daily wear of soft CLs. There are several reports of changes in corneal topography [25], changes in anterior corneal topography [26] and central corneal edema [27] after CLs use.
A possible mechanism for the changes in biomechanical properties has been attributed to corneal stromal edema after CLs use, which increases the distance between collagen fibrils and affects the biomechanical function of the cornea [28]. Furthermore, another possible hypothesis regarding the repolarization of corneal tissue and the resulting changes in corneal biomechanical behavior may be related to the local alteration of inflammatory cytokines and chemokines after CLs use [29].
The scientific literature contains several studies on the characterisation of corneal biomechanics in different study designs, having been evaluated with both the ORA and the CST [21]. Regarding corneal biomechanics related to the wearing of soft CLs, we found studies utilising the ORA, but to our knowledge, there are limited reports about the relationship between soft CLs use and corneal biomechanics using the CST [30].
Therefore, we consider it of utmost importance to understand the structural and biomechanical changes of the cornea after wearing CLs in our research of hydrophilic material because this may have important clinical implications, especially in patients whose properties are already altered before use, as in the case of pathological corneas, as well as in the development of new CLs with different uses or applications. Thus, the need for this project arises.
2. Materials and Methods
2.1. Design
This prospective, cross-sectional, single-center study was conducted between February 2023 and May 2023 at the facilities of the Faculty of Pharmacy (Department of Optics and Optometry) of the University of Seville, Spain. The study complied with the standards established by the Declaration of Helsinki and the Andalusian Ethics Committee Council. After explaining the nature of the study, informed consent was obtained from each subject.
2.2. Subjects
Twenty-two Caucasian patients belonging to the student community of the University of Seville were recruited. To avoid any bias, only one eye from each participant was randomly selected for inclusion in the study [31]. Inclusion criteria were as follows: (1) 18 years of age; (2) habitual CLs wearer; (3) simple or compound myopic refractive error (with astigmatism); (4) cessation of CLs wear for at least 7-21 days among hydrophilic and rigid gas permeable lens wearers, respectively, with special topography follow-up in case of corneal moulding until disappearance or topographic stabilisation; and (5) acceptance of participation in the study and ability to understand the informed consent and subsequent signature of the consent form. Exclusion criteria were as follows: (1) collagen or autoimmune diseases; (2) previous intraocular or corneal surgery; (3) ocular pathologies; (4) corneal dystrophies and degenerations; (5) dry eye syndrome; (6) persistent epithelial defects; (7) history of herpetic corneal ulcer; (8) central corneal leukoma; (9) topographic map compatible with subclinical keratoconus or other corneal ectatic disorder; and (10) current antiglaucomatous or hypotonic treatment.
2.3. Contact Lenses
The lens used by the subjects were Lens 55® UV (Ocufilcon D4 (19) [55%]. Servilens, https://www.lens55.com/documents/catalogo_Servilens_V20.pdf), a hydrogel lens with a thin rim design, performing well in terms of comfort and parameters.
CLs prescriptions were determined based on the refraction of the spectacle distance and modified, if necessary, by taking into account the vertex distance. The lenses were fitted binocularly, and the same type of lens was used in each eye. Each pair of lenses was worn for 10 minutes to settle on the eye before starting measurements and then worn for approximately half an hour during the assessment of distance visual acuity. After the settling period, the CLs fit was checked and confirmed to be acceptable (<1.0 mm of decentration, <1.0 mm of movement) before proceeding with the assessment [32]. Thus, the wearers' initial response to the CL was assessed.
2.4. Procedure
Once the informed consent form had been signed, each study subject underwent a pre-visit in which, in addition to collecting the relevant data from the clinical history, they underwent a complete ophthalmological examination with the following diagnostic tests: optically corrected visual acuity (BCVA) according to the Snellen decimal scale; subjective and objective refraction without cycloplegia; corneal topography; corneal biomechanics analysis using Scheimpflug technology via the CST analyser (Oculus Optikgeräte GmbH, Wetzlar, Germany) and slit-lamp anterior pole examination. Another visit was scheduled for CLs fitting and a final examination one month after CLs wear, at which time biomechanical parameters were remeasured.
All measurements with the CST were performed by the same technicians and recorded with automatic release to ensure the absence of examiner dependence. If the examination quality (QS) box showed any type of alteration, this was identified in the device software; to be considered an optimal image, the quality factor had to be higher than 95% (this figure may be lower due to the presence of artifacts in the image, eye blinking, or insufficient eye opening by the patient); otherwise, the necessary correction was made and the acquisition was repeated. Only Corvis ST exams with an "OK" quality rating were included in the analysis, excluding alignment errors. Flicker errors were also excluded. In all cases, 3 measurements were taken per patient and the mean was calculated.
The variables included in this study are the most reproducible parameters of the CST, as collected in the Biomechanical Comparison Display (Figure 1): (1) Deflection Amplitude Ratio (DA Ratio): this is the ratio between the central corneal deflection and the average of two points located at 1.0 mm (DAR1) or 2.0 mm (DAR2) either side of the center. Stiffer corneas would have a lower DA because the center of the cornea and the cornea at 1.0 or 2.0 mm deflect at the same time, whereas a higher DA indicates that the central cornea deflects more than the average of the other two points, corresponding to softer tissue; (2) Ambrosio Horizontal Relational Thickness (ARTh): corneal thickness is measured using the horizontal Scheimpflug image. This allows the rate of increase in corneal thickness from the apex to the nasal and temporal sides to be calculated. Characterisation of the thickness profile allows calculation of the Ambrósio Relational Thickness across the horizontal meridian, which is a relative simplification of the tomographic Relational Thickness calculations also provided by the Pentacam; (3) Stiffness Parameter-A1 (SP-A1): it is defined as the pressure at first flattening, which is the difference between the air bubble pressure at the corneal surface and the bIOP, divided by the DA. It is determined from the displacement of the apex from rest to first flattening. This value has been clinically proven to be useful in assessing KC with the highest sensitivity and specificity of any of the parameter values. Higher values indicate stiffer corneas; (4) Integrated Radius (Int. Radius): dynamic corneal deformation response parameter representing the reciprocal of the radius at the state of maximum corneal concavity. A larger concave radius is associated with greater resistance to deformation, i.e., a stiffer cornea. The larger the integrated inverse radius and the maximum inverse radius, the lower the resistance to deformation and the lower the corneal stiffness; and (5) Stress‒Strain Index (SSI): a new parameter for estimating the material stiffness of corneal tissue that is independent of IOP and corneal geometry. The stress/strain curve describes the elastic properties of the cornea. The curves are shifted to the right if the cornea is soft and to the left if it is stiff. The SSI index describes the position of the curve. A value of 1 indicates average elasticity, a value less than 1 indicates softer behaviour and a value greater than 1 indicates stiffer than average behaviour. Secondary variables were (1) Central Corneal Thickness (CCT) and (2) Biomechanically Corrected Intraocular Pressure (bIOP). None of the variables have units, and moreover, they do not have standardised values. However, the standard deviation (SD) PRE-POST is compared, and depending on the variable, the change is qualified as not significant, softer/stiffer or thinner/thicker (Table 1). All measurements with CST were taken by the same technicians and captured by automatic release to ensure no examiner dependence. To be considered an optimal image, the quality factor had to be higher than 95%. In all cases, 3 measurements were obtained per patient, and the mean value was used.
2.5. Data Analysis
The data collected were reviewed for consistency and correctness. Subsequently, statistical analysis was carried out using SPSS software for Windows version 22.0 (IBM, USA). The normality of both the variables that record the biomechanical values and those that record the standard deviations of these values was checked using the Shapiro‒Wilk test. For the variables that followed a normal distribution, the T test for related samples was employed. For those variables for which it was not possible to assume normality, non-parametric techniques were used, specifically the Wilcoxon test. For all statistical tests, a p value < 0.05 was considered statistically significant. Statistical analysis of the data collected under the guidelines of the clinical protocol allowed us to draw and establish the conclusions of the study, thus quantifying the biomechanical impact on the use of soft CLs.
3. Results
Twenty-two eyes [6 right (27.3%) and 16 left (72.7%)] of 22 patients (mean age, 20.64 ± 1.21 years, range 19-24 years) were included. There were 7 males (31.8%) and 15 females (68.2%). Descriptive data for biomechanical measurements pre- and post-CLs wear are presented in Table 2.
Differences between the means of the DA Ratio and the SD of the DA Ratio pre- and post-CLs wear (Figure 2) were found to be significant according to Student's t test for related samples (p value=0.002 in both cases). Similarly, significant differences were found between pre- and post-CLs wear values in CCT according to the Wilcoxon test (p value=0.013), indicating corneal thickening. For all other biomechanical measures, no significant differences were observed before and after treatment. Table 3 presents the summary of the changes, showing the 95% confidence intervals for the mean SD difference (pre - post) at normality assumptions and the classification value for these changes, according to which the patients are classified as shown in histograms in Figure 3. The biomechanical changes correlating significantly through Pearson's r correlation coefficient were changes in DA Ratio and ARTh (r=0.442, p=0.039), changes in Int. Radius and SP-A1 (r=0.475, p=0.025), and changes in SP-A1 and SSI (r=0.434, p=0.044), showing direct linear associations. Similarly, an inverse linear correlation was found between spherical equivalent (SE) and axial length (AXL) (r=-0.633, p=0.002). No significant associations were found for any variable according to age, sex or eye (right or left). A significant association was found according to the chi-square test between changes in bIOP and classification according to changes in Int. Radius (p value = 0.047) and SSI (p value = 0.026) standard deviations.
4. Discussion
Most studies analysing changes in biomechanical properties, especially after different corneal refractive procedures, have been performed with ORA, as it was the first to be available. Its clinical introduction was extremely important because it was the first time that the biomechanical response of the cornea to a perturbation could be measured in vivo using a puff of air to deform it. However, basic misconceptions have been perpetuated, obscuring interpretation of the results, including the desire to biomechanically characterise the cornea with a single number that may answer clinical questions about corneal stiffness or basic corneal weakness [23].
Similarly, when CST became available, there was a new wave of studies, from the first in 2014, in which Hassan et al. compared the results of PRK and LASIK techniques [33], until 2017, when the same team discussed the effects of FEMTOLASIK and PRK [34].
Interest in corneal biomechanics was spreading as the instrument evolved, providing new parameters. Thus, authors such as Yang et al. decided to compare these new parameters in healthy eyes undergoing LASIK surgery, patients with post-LASIK ectasia and patients with keratoconus [35].
Regarding CLs wear, most studies are related to orthokeratology and carried out with ORA. This is the case for Chen et al. [36], who determined an alteration in biomechanical properties such as a lower corneal resistance factor (CRF) as the duration of orthokeratology lens wear increased. On the other hand, Manuel González-Méijome et al. found a faster recovery effect in less resistant corneas, correlating corneal hysteresis (CH) with changes in keratometry and CCT during lens wear and reporting a need for further studies to determine these changes [37].
For soft CLs, most studies have also used ORA. Cankaya et al. performed analysis with the aim of comparing CH and CRF with and without wearing CLs [38], concluding that CH did not show a trend of change with the use of CLs. Conversely, Somayeh Radaie Moghadam et al. and Lau and Pye reported a decrease in CH at one month after fitting and immediately after using CLs [39,40]. On the other hand, CRF showed higher values in patients wearing CLs, with a statistically significant difference associated with corneal remodelling due to chronic use of CLs. Somayeh Radaie Moghadam et al., 2016 and Lau and Pye, 2011 found a decrease in CRF when CLs use was discontinued. In our case, corneal weakening was observed after CLs wear in a small percentage of wearers, though in the majority, there was no statistical significance.
According to studies performed with CST, there is controversy in the literature with regard to changes in CST after the use of soft CLs, as Braun and Penno indicated that this value decreased in relation to the control population [41], whereas authors such as Cemal Çavdarli and Peyman et al. observed a null impact [30, 42]. By evaluating these long-term changes, Yeniad et al. showed thickening after one month of use and thinning after 6 months. In this study, an increase in corneal thickness (p value < 0.05) was observed in the measurement after one month of wear [43].
Similar to the study by Peyman et al. [30], the present study also found no significant differences in corneal biomechanical parameters after one month of CLs use. Changes in DA Ratio and ARTh, Int. Radius and SP - A1, SP - A1 and SSI correlated directly, with SE and AXL correlating inversely.
Sapkota et al. studied the effect of soft CL on IOP, observing a reduction in both Goldmann correlated intraocular pressure (gIOP) and compensated intraocular pressure (cIOP), as measured by ORA, of approximately 1.02 mmHg during the first month. The authors concluded that these changes were significantly related to lens type, i.e., daily or monthly disposable, but not to the wearing pattern [38]. In our study, the bIOP value decreased (p value > 0.05).
5. Conclusions
The corneal biomechanical indices provided by CST demonstrate that fitting of soft CLs is a safe optical compensation method for the stability of corneal stiffness in healthy patients with myopia.
No significant differences were found pre- and post-CLs wear in the assessment of bIOP. It is confirmed that CST is an objective tool for IOP measurement.
We believe that our study would benefit from a control group either not wearing CLs or a group with newer materials lenses such as silicone hydrogel.
An advanced understanding of the biomechanical properties of the cornea would be needed for those patients with mild or subclinical forms of ectatic corneal disease who can still compensate for their refractive error by wearing soft CLs.
Author Contributions
Conceptualization, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; methodology, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; software, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; validation, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; formal analysis, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; investigation, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; resources, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; data curation, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; writing—original draft preparation, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; writing—review and editing, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; visualization, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; supervision, A.L.-M., I.L.-C., U.T.-P. and M.G.-R.; project administration, A.L.-M., I.L.-C., U.T.-P. and M.G.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Andalusian Ethics Committee.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Acknowledgments
The authors appreciate the support offered by the members of the Department of Physics of Condensed Matter, Faculty of Physics, University of Seville, with special thanks to Ángela Gallardo-López. In addition, the authors also appreciate the technical support by members and facilities of the Faculty of Pharmacy, University of Seville, with special thanks to María Álvarez-de-Sotomayor.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Dupps Jr, W.J., Wilson, S.E. (2006). Biomechanics and wound healing in the cornea. Experimental eye research, 83(4), 709-720.
- Torres R, Merayo-Lloves J, Jaramillo, M., Galvis, V. Biomecánica de la córnea. Arch Soc Esp Oftalmol. 2005;80(4):215-223. https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0365-66912005000400004&lng=es&nrm=iso&tlng=es. Accessed February 8, 2022.
- Kling, S., & Hafezi, F. (2017). Corneal biomechanics–a review. Ophthalmic and Physiological Optics, 37(3), 240-252.
- Ambrósio Jr, R., Ramos, I., Luz, A., Faria, F.C., Steinmueller, A., Krug, M., ... & Roberts, C.J. (2013). Dynamic ultra high speed Scheimpflug imaging for assessing corneal biomechanical properties. Revista Brasileira de Oftalmologia, 72, 99-102.
- Huseynova, T., Waring IV, G.O., Roberts, C., Krueger, R.R., & Tomita, M. (2014). Corneal biomechanics as a function of intraocular pressure and pachymetry by dynamic infrared signal and Scheimpflug imaging analysis in normal eyes. American journal of ophthalmology, 157(4), 885-893. 4.
- Elsheikh, A., Alhasso, D., & Rama, P. (2008). Assessment of the epithelium's contribution to corneal biomechanics. Experimental eye research, 86(2), 445-451.
- Ma, J.; Wang, Y.; Wei, P.; Jhanji, V. Biomechanics and structure of the cornea: implications and association with corneal disorders. Surv. Ophthalmol. 2018, 63, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Esporcatte, L.P.G.; Salomão, M.Q.; Lopes, B.T.; Vinciguerra, P.; Vinciguerra, R.; Roberts, C.; Elsheikh, A.; Dawson, D.G.; Ambrósio, R. Biomechanical diagnostics of the cornea. Eye Vis. 2020, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Elsheikh, A.; Alhasso, D.; Kotecha, A.; Garway-Heath, D. Assessment of the Ocular Response Analyzer as a Tool for Intraocular Pressure Measurement. J. Biomech. Eng. 2009, 131, 081010–081010. [Google Scholar] [CrossRef] [PubMed]
- Pepose, J.S.; Feigenbaum, S.K.; Qazi, M.A.; Sanderson, J.P.; Roberts, C.J. Changes in Corneal Biomechanics and Intraocular Pressure Following LASIK Using Static, Dynamic, and Noncontact Tonometry. Arch. Ophthalmol. 2007, 143, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Ambrósio Jr, R., Correia, F.F., Lopes, B., Salomão, M.Q., Luz, A., Dawson, D.G., ... & Roberts, C.J. (2017). Suppl-1, M2: Corneal biomechanics in ectatic diseases: Refractive surgery implications. The open ophthalmology journal, 11, 176.
- Goldich, Y., Marcovich, A.L., Barkana, Y., Mandel, Y., Hirsh, A., Morad, Y., ... & Zadok, D. (2012). Clinical and corneal biomechanical changes after collagen cross-linking with riboflavin and UV irradiation in patients with progressive keratoconus: Results after 2 years of follow-up. Cornea, 31(6), 609-614.
- Eliasy, A.; Chen, K.-J.; Vinciguerra, R.; Lopes, B.T.; Abass, A.; Vinciguerra, P.; Ambrósio, R., Jr.; Roberts, C.J.; Elsheikh, A. Determination of Corneal Biomechanical Behavior in-vivo for Healthy Eyes Using CorVis ST Tonometry: Stress-Strain Index. Front. Bioeng. Biotechnol. 2019, 7, 105. [Google Scholar] [CrossRef]
- Piñero, D.P.; Alcón, N. Corneal biomechanics: a review. Clin. Exp. Optom. 2015, 98, 107–116. [Google Scholar] [CrossRef]
- Garcia-Porta, N.; Fernandes, P.; Queiros, A.; Salgado-Borges, J.; Parafita-Mato, M.; González-Méijome, J.M. Corneal Biomechanical Properties in Different Ocular Conditions and New Measurement Techniques. ISRN Ophthalmol. 2014, 2014, 1–19. [Google Scholar] [CrossRef]
- Vinciguerra, R., Elsheikh, A., Roberts, C.J., Ambrósio Jr, R., Kang, D.S.Y., Lopes, B.T., ... & Vinciguerra, P. (2016). Influence of pachymetry and intraocular pressure on dynamic corneal response parameters in healthy patients. Journal of refractive surgery, 32(8), 550-561. 8.
- Roberts, C.J., & Dupps Jr, W.J. (2014). Biomechanics of corneal ectasia and biomechanical treatments. Journal of Cataract & Refractive Surgery, 40(6), 991-998.
- Ambrósio, J.R., Jr.; Correia, F.F.; Lopes, B.; Salomão, M.Q.; Luz, A.; Dawson, D.G.; Elsheikh, A.; Vinciguerra, R.; Vinciguerra, P.; Roberts, C.J. Corneal Biomechanics in Ectatic Diseases: Refractive Surgery Implications. Open Ophthalmol. J. 2017, 11, 176–193. [Google Scholar] [CrossRef]
- Lopes, B.T.; Roberts, C.J.; Elsheikh, A.; Vinciguerra, R.; Vinciguerra, P.; Reisdorf, S.; Berger, S.; Koprowski, R.; Ambrósio, R. Repeatability and Reproducibility of Intraocular Pressure and Dynamic Corneal Response Parameters Assessed by the Corvis ST. J. Ophthalmol. 2017, 2017, 1–4. [Google Scholar] [CrossRef]
- Luce, D.A. Determining in vivo biomechanical properties of the cornea with an ocular response analyzer. J. Cataract. Refract. Surg. 2005, 31, 156–162. [Google Scholar] [CrossRef]
- Piñero, D.P.; Alcón, N. In vivo characterization of corneal biomechanics. J. Cataract. Refract. Surg. 2014, 40, 870–887. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, H.; Asgari, S.; Mortazavi, M.; Ghaffari, R. Evaluation of Corneal Biomechanics After Excimer Laser Corneal Refractive Surgery in High Myopic Patients Using Dynamic Scheimpflug Technology. Eye Contact Lens: Sci. Clin. Pr. 2017, 43, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Kling, S.; Hafezi, F. Corneal biomechanics – a review. Ophthalmic Physiol. Opt. 2017, 37, 240–252. [Google Scholar] [CrossRef]
- Darlen Rodríguez Rivero D, Dra Silvia María López Hernández I, Yoanner Martín Perera, I.; et al. Corneal ulcers in contact lens wearers. Rev Cuba Oftalmol. 2015;28(2):220-227. http://scielo.sld.cu.
- Alba-Bueno, F.; Beltran-Masgoret, A.; Sanjuan, C.; Biarnés, M.; Marín, J. Corneal shape changes induced by first and second generation silicone hydrogel contact lenses in daily wear. Contact Lens Anterior Eye 2009, 32, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, G.; Collins, M.; Read, S.; Davis, B. Regional Changes in Corneal Thickness and Shape with Soft Contact Lenses. Optom. Vis. Sci. 2010, 87, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Braun, D.A.; Penno, E.E.A. Effect of contact lens wear on central corneal thickness measurements. J. Cataract. Refract. Surg. 2003, 29, 1319–1322. [Google Scholar] [CrossRef]
- Sánchez-Tena, M. .; Martinez-Perez, C.; Villa-Collar, C.; Alvarez-Peregrina, C. Long-term effect of contact lens wear: A citation network study. Contact Lens Anterior Eye 2022, 45, 101527. [Google Scholar] [CrossRef]
- Alipour, F.; Khaheshi, S.; Soleimanzadeh, M.; Heidarzadeh, S.; Heydarzadeh, S. Contact Lens-related Complications: A Review. Journal of ophthalmic vision research, 2017, 12, 193–204. [CrossRef]
- Peyman, A.; Ghoreishi, M.; Hashemi-Estabragh, S.-S.; Mirmohammadkhani, M.; Mohammadinia, M.; Pourazizi, M. Corneal biomechanical properties after soft contact lens wear measured on a dynamic Scheimpflug analyzer: A before and after study. Journal Français d’Ophtalmologie2021, 44, 391–396. [CrossRef]
- Armstrong, R.A. Statistical guidelines for the analysis of data obtained from one or both eyes. Ophthalmic Physiol. Opt. 2012, 33, 7–14. [Google Scholar] [CrossRef]
- Jaisankar D, Leube A, Gifford KL, Schmid KL, Atchison DA. Effects of eye rotation and contact lens decentration on horizontal peripheral refraction. Ophthalmic Physiol Opt. 2019;39(5):370-377.
- Hassan Z, Modis L, Szalai E, Berta, A., Nemeth, G. Author ’ s personal copy Contact Lens & Anterior Eye Examination of ocular biomechanics with a new Scheimpflug technology after corneal refractive surgery.
- Hashemi, H.; Asgari, S.; Mortazavi, M.; Ghaffari, R. Evaluation of Corneal Biomechanics After Excimer Laser Corneal Refractive Surgery in High Myopic Patients Using Dynamic Scheimpflug Technology. Eye Contact Lens: Sci. Clin. Pr. 2017, 43, 371–377. [Google Scholar] [CrossRef]
- Yang, K.; Xu, L.; Fan, Q.; Gu, Y.; Song, P.; Zhang, B.; Zhao, D.; Pang, C.; Ren, S. Evaluation of new Corvis ST parameters in normal, Post-LASIK, Post-LASIK keratectasia and keratoconus eyes. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Chen, D.; Lam, A.K.C.; Cho, P. A pilot study on the corneal biomechanical changes in short-term orthokeratology. Ophthalmic Physiol. Opt. 2009, 29, 464–471. [Google Scholar] [CrossRef] [PubMed]
- González-Méijome, J.M.; Villa-Collar, C.; Queirós, A.; Jorge, J.; A Parafita, M. Pilot Study on the Influence of Corneal Biomechanical Properties Over the Short Term in Response to Corneal Refractive Therapy for Myopia. Cornea 2008, 27, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Cankaya, A.B.; Beyazyildiz, E.; Ileri, D.; Ozturk, F. The Effect of Contact Lens Usage on Corneal Biomechanical Parameters in Myopic Patients. Cornea 2012, 31, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadehpur, E.; Radaie-Moghadam, S.; Hashemi, H.; Yekta, A.; Khabazkhoob, M. Corneal biomechanical changes following toric soft contact lens wear. 2016, 11, 131–5. [CrossRef]
- Lau, W.; Pye, D. Changes in Corneal Biomechanics and Applanation Tonometry with Induced Corneal Swelling. Investig. Opthalmology Vis. Sci. 2011, 52, 3207–3214. [Google Scholar] [CrossRef]
- Braun, D.A.; Penno, E.E.A. Effect of contact lens wear on central corneal thickness measurements. J. Cataract. Refract. Surg. 2003, 29, 1319–1322. [Google Scholar] [CrossRef]
- Çavdarlı, C.; Topçu-Yılmaz, P. Does Long-term Soft Contact Lens Wear Affect Corneal and Anterior Chamber Parameters? Turk. J. Ophthalmol. 2018, 48, 166–170. [Google Scholar] [CrossRef]
- Yeniad, Barş, M.D.ı; Yiğit, Bülent, M.D.; İşsever, Halim PH.D.; Bilgin, Lale Közer, M.D.. Effects of Contact Lenses on Corneal Thickness and Corneal Curvature During Usage. Eye & Contact Lens: Science & Clinical Practice: October 2003 - Volume 29 - Issue 4 - p 223-229. 20 October. [CrossRef]
- Sapkota, K.; Franco, S.; Lira, M. Intraocular pressure measurement with ocular response analyzer over soft contact lens. Contact Lens Anterior Eye 2014, 37, 415–419. [Google Scholar] [CrossRef]
Figure 1.
Comparison pre- and post-contact lens wear of biomechanical Corvis ST parameters.
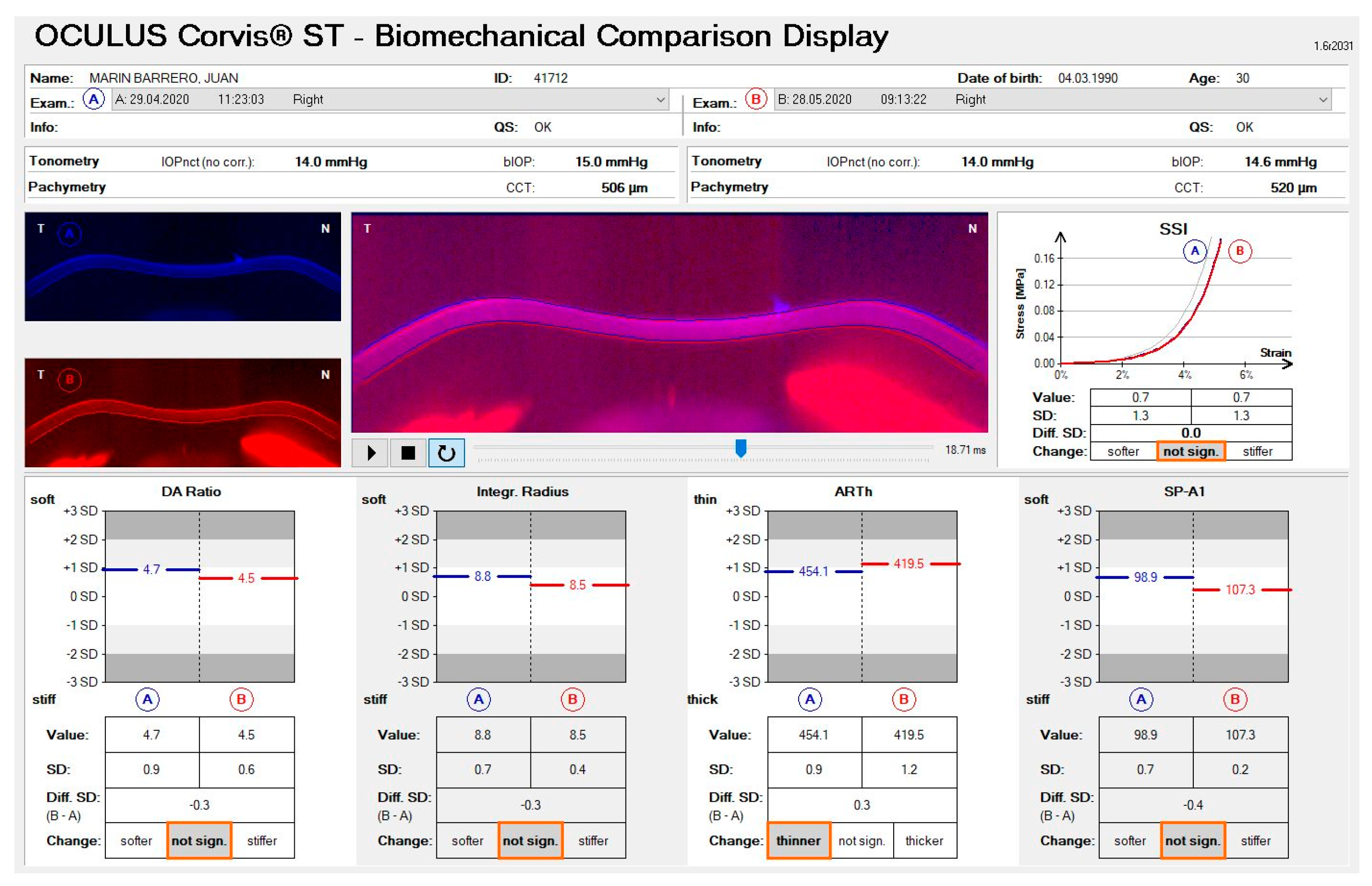
Figure 2.
(a) Differences between the mean of the DAR plot pre- and post-contact lens wear; (b) Differences between the mean of the SD_DAR plot pre- and post-contact lens wear.
Figure 2.
(a) Differences between the mean of the DAR plot pre- and post-contact lens wear; (b) Differences between the mean of the SD_DAR plot pre- and post-contact lens wear.
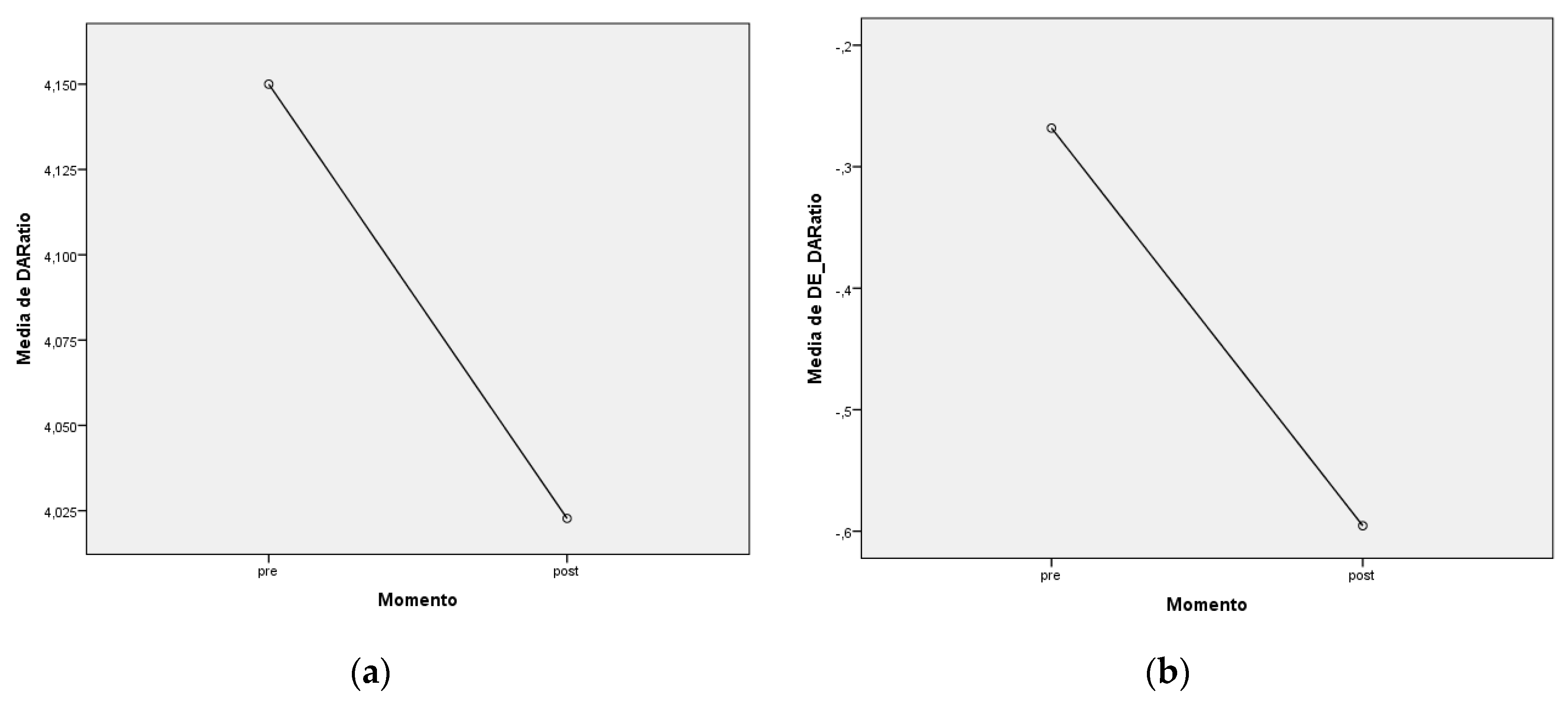
Figure 3.
Histograms of classification according to changes in different biomechanical measures pre- and post-contact lens wear: (a) SD_DARatio; (b) SD_Int_Ratius; (c) SD_SP_A1; (d) SD_ARTh; (e) SD_SSI.
Figure 3.
Histograms of classification according to changes in different biomechanical measures pre- and post-contact lens wear: (a) SD_DARatio; (b) SD_Int_Ratius; (c) SD_SP_A1; (d) SD_ARTh; (e) SD_SSI.
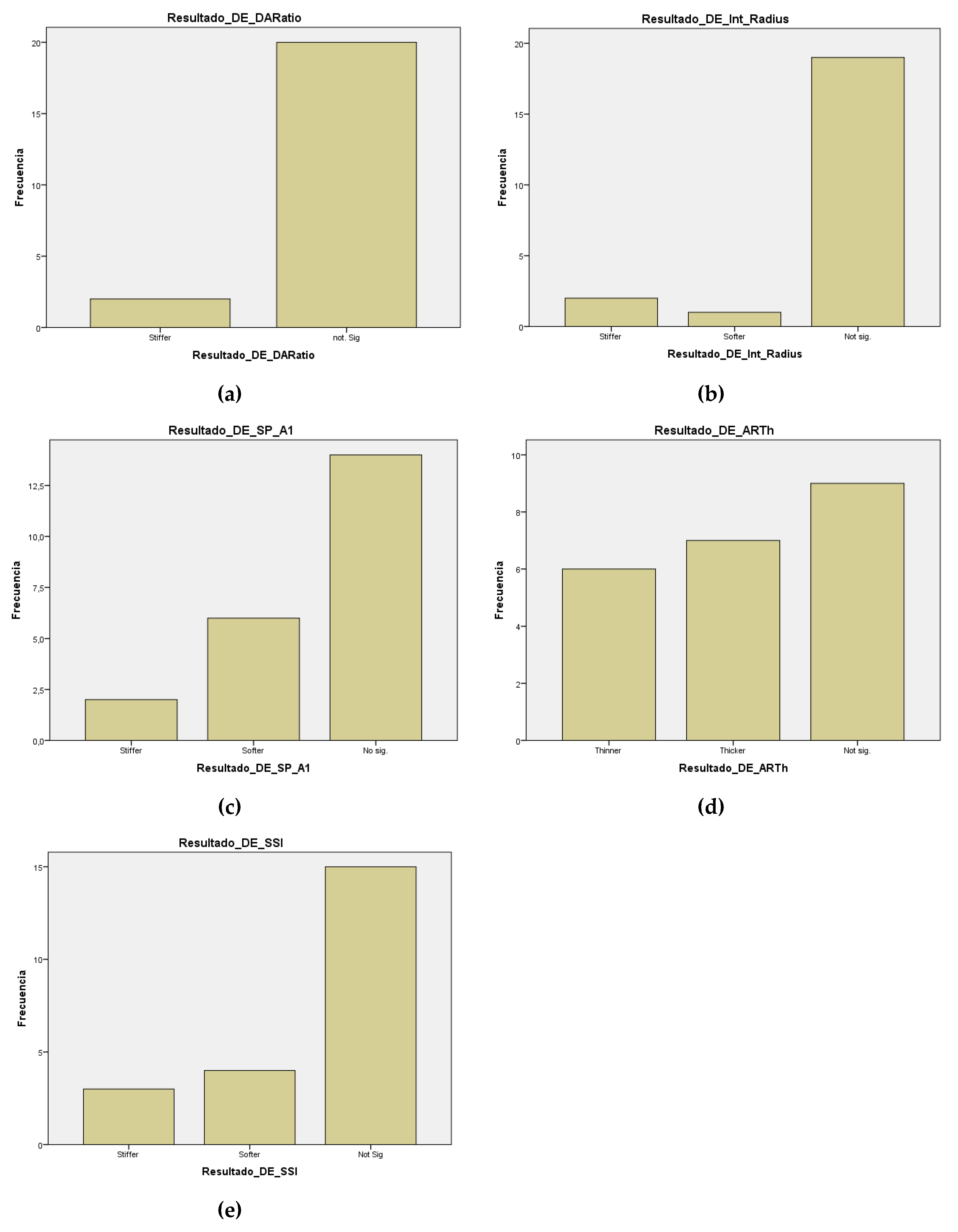

Table 1.
Classification of the change in standard deviation of biomechanical parameters post-pre (B-A) of the Biomechanical Comparison Display software.
Table 1.
Classification of the change in standard deviation of biomechanical parameters post-pre (B-A) of the Biomechanical Comparison Display software.
| B-A Not Significant | B-A Stiffer | B-A Softer | |
|---|---|---|---|
| DAR | ± 1.0 | > -1.0 | > +1.0 |
| Int. Radius | ± 0.7 | > -0.7 | > +0.7 |
| SP-A1 | ± 0.8 | > -0.8 | > +0.8 |
| SSI | ± 0.4 | > -0.4 | > +0.4 |
| B-A Not Significant | B-A Thicker | B-A Thinner | |
| ARTh | ± 0.3 | > -0.3 | > +0.3 |
DAR = Deflection Amplitude Ratio; Int. Radius = Integrated Radius; SP-A1 = Stiffness Para- meter-A1; SSI = Stress‒Strain Index ; ARTh = Ambrosio Horizontal Relational Thickness.
Table 2.
Descriptive analysis of biomechanical data, bIOP and CCT, pre- and post- contact lens wear.
Table 2.
Descriptive analysis of biomechanical data, bIOP and CCT, pre- and post- contact lens wear.
| Variables | |||
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| DAR |
Pre 4,15 ± 0,32 Post 4,02 ± 0,29 |
SD_DAR |
Pre -0,27 ± 0,78 Post -0,60 ± 0,68 |
| Int. Radius |
Pre 7,57 ± 1,05 Post 7,38 ± 0,83 |
SD_Int. Ratius |
Pre -0,43 ± 0,93 Post -0,59 ± 0,75 |
| ARTh |
Pre 521,14 ± 81,60 Post 528,77 ± 106,75 |
SD_ARTh | Pre 0,33 ± 0,66 Post 0,29 ± 0,85 |
| SP-A1 |
Pre 112,77 ± 15,50 Post 108,82 ± 12,69 |
SD_SP-A1 | Pre -0,04 ± 0,82 Post 0,16 ± 0,69 |
| SSI |
Pre 0,97 ± 0,14 Post 0,95 ± 0,14 |
SD_SSI | Pre 0,20 ± 0,58 Post 0,17 ± 0,66 |
| bIOP |
Pre 16,14 ± 2,67 Post 15,61 ± 1,85 |
CCT | Pre 556,00 ± 91,38 Post 545,23 ± 21,75 |
DAR = Deflection Amplitude Ratio; Int. Radius = Integrated Radius; ARTh = Ambrosio Horizontal Relational Thickness; SP-A1 = Stiffness Parameter-A1; SSI = Stress‒Strain Index ; bIOP = Biomecha- nically Corrected Intraocular Pressure; CCT = Central Corneal Thickness; SD = Standard Deviation.
Table 3.
Summary of changes in corneal biomechanical parameters, bIOP and CCT, before and after contact lens wear and classification.
Table 3.
Summary of changes in corneal biomechanical parameters, bIOP and CCT, before and after contact lens wear and classification.
| Variables | p-valor | IC (µpre - µpost) | Resultado | Clasificación |
|---|---|---|---|---|
| DAR (SD) | 0,002 | (0,1361;0,5184) | pre > post | |post-pre|<1 |
| Int. Radius (SD) | 0,1 | No normalidad | No sig. | |post-pre|<0,7 |
| SP-A1 (SD) | 0,129 | (-0,46355; 0,06355) | No sig. | |post-pre|<0,8 |
| SSI (SD) | 0,779 | (-0,20054; 0,26418) | No sig. | |post-pre|<0,4 |
| ARTh (SD) | 0,986 | No normalidad | No sig. | |post-pre|<0,3 |
| bIOP | 0,135 | No normalidad | No sig. | |
| CCT | 0,013 | No normalidad | Pre < post |
DAR = Deflection Amplitude Ratio; Int. Radius = Integrated Radius; SP-A1 = Stiffness Parameter -A1; SSI = Stress‒Strain Index ; ARTh = Ambrosio Horizontal Relational Thickness; bIOP = Bio- mechanically Corrected Intraocular Pressure; CCT = Central Corneal Thickness; SD = Standard Deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



