
Submitted:
10 October 2023
Posted:
11 October 2023
You are already at the latest version
Abstract
Abdominal entry is the critical initial step of laparoscopic surgery as it is associated with unexpected complications. Acceptable working space is a prerequisite for safe minimal access surgery. Direct trocar insertion (DTI) technique has been often reported to be time-consuming and capable of causing injuries. We aim to facilitate conventional DTI employing an easy-to-use self-designed abdominal wall-lifting device, OneShot-M. We tested its safety in a porcine model. 18 pigs were randomized into three groups (n=6): open laparoscopy (Group A), DTI (Group B), DTI using OneShot-M (Group C), suitable for a 5-mm trocar. Outcomes were access time, entry-related minor and major complications. Median access time was shorter in C (43 seconds; range: 35-49 seconds), followed by B (82.5; 72-90) and A (190.5; 182-240). Statistically significant differences in procedural time between techniques were detected (p-value = 0.0005). Pairwise comparisons exhibited a statistically significant difference between A and C in terms of access time. Only one difficulty in entry was seen in C; pigs experienced several occurrences in A and B. This pilot study suggests that OneShot-M appears to be a technically feasible, fast and safe method for pneumoperitoneum induction in a porcine model, as it provides sufficient exposure of the operative field without access-related complications. Further clinical studies are needed.
Keywords:
laparoscopy
; peritoneal access
; direct trocar insertion
; wall-lifting device
; access time
; complications
1. Introduction
Laparoscopy is a well-established procedure largely used to examine the contents of the abdominal or pelvic cavities for both diagnosis and treatment of different diseases and conditions. Thanks to better aesthetic outcomes, minimal tissue injury, lower complication rate, shorter hospital stay and faster recovery, this minimally invasive approach became the method of choice in the performance of numerous surgical procedures in various fields, replacing surgical interventions with open technique [1,2,3,4,5,6]. Although it is estimated that laparoscopy is 41% safer than open surgery and possible major complications arising from this technology are rare, the rate of risks ranges from 5% to 8% for all procedures [3,7,8,9,10,11,12].
Insertion of the Veress needle and primary trocar for establishing an acceptable pneumoperitoneum is the first and most hazardous step in laparoscopy, in which more than 50% of major laparoscopic complications occur before commencement of intended surgery [8,13,14]. Entry-related complications including abdominal wall bleeding, subcutaneous emphysema, wound infection, wound herniation, gastrointestinal tract perforation, and retroperitoneal vascular injury are the most serious and are uncommon, but they can result in significant morbidity and even death in 0.05% to 0.2% of cases [14,15,16,17,18,19].
Despite decades of technological development to introduce surgical procedures and instruments for a safer abdominal wall perforation, no single method, currently used for peritoneal cavity access, has been proved to avoid laparoscopic entry-associated risks [20,21,22]. Four basic techniques have been developed to enter the abdomen, such as closed technique (Veress needle), open laparoscopy (Hasson), direct trocar insertion (DTI), and visual entry method (optical trocar) [23]. One third to one half of all major intra-abdominal vascular and intestinal injuries is caused by placement of the Veress needle (39.8%) [24]. Open approach has a lower incidence of vascular complications, but a potentially higher incidence of bowel damage [15,17,25,26,27,28,29,30]. Several reasons for limiting the use of the open method exist, including greater time needed for its performance, technical difficulty, obese patients, and difficulty in pneumoperitoneum maintenance. Direct trocar insertion is slightly faster than any other system of laparoscopic access and also entails just one “blind step” (trocar), instead of three with closed method (Veress needle, insufflation, trocar), but it remains probably the least-performed technique in clinical practice due to fear of causing internal lesions as it is a blind approach. Recently, the optical trocar [23] has been developed to allow the surgeon to visualize the abdominal wall layers on the monitor as they are approached and crossed before transection, which helps avoid viscera injury [6,31]. Nevertheless, major vascular lesions seem to remain a risk associated with the visual entry system [11,32,33,34].
In light of the above, there is no optimal single form of laparoscopic access that completely eliminates entrance-related complications in the low-risk patient, hence the procedure most experienced by the surgeon should be chosen. Currently, there is still no consensus regarding how to introduce the primary trocar inside the peritoneal cavity without injuries and an increasing number of researchers have investigated the feasibility of innovative technologies and devices of port insertion for a safer trocar entry.
In a previous work we evaluated and successfully tested in an in vivo animal model the feasibility, effectiveness, and safety of OneShot-M, a suction cup device that we designed and initially proposed for making Veress needle introduction secure, simple and speed [35]. In the effort to optimize the efficacy of DTI method, the current study aimed to report our experience in a porcine model using a prototype of OneShot-M modified in order to facilitate the direct positioning of the first trocar. It may help develop a safer and quicker alternative method of pneumoperitoneum establishment as well as minimize the incidence of DTI-related injuries. We also wanted to assess the feasibility profile of DTI approach combined with the self-made wall-lifting device by comparing it to the standard open and DTI techniques.
2. Materials and Methods
2.1. Animals
The study started in January 2020 and was completed in August 2020. All procedures were performed in the operating room of the Ce.Me.Ri.T. (Centro Mediterraneo di Ricerca e Training) of the Istituto Zooprofilattico Sperimentale della Sicilia “A. Mirri”, Palermo. 18 large white female pigs weighting 30 to 35 kg were included in the experiments. Animals came from outsourced specialized facilities external to the room where the experiments were conducted; they were housed and acclimated to the facility for at least two days after arrival. Pigs were randomly divided into three groups and underwent three different techniques of laparoscopic surgery: Group A (n = 6) where the open Hasson access technique (OAT) was executed, Group B (n = 6) where direct trocar insertion (DTI) method was performed, and Group C (n = 6) where OneShot-M device was used to facilitate the DTI technique (OSM/DTI). The surgical team comprised at least 2 operating surgeons. The same equipment, including the same monitor, insufflators, light source and camera, were used for all cases. In all animals, disposable trocars were used. OneShot-M prototype configuration is described in Figure 1. Compared to the prototype used in the previous work [35], when the access hole was specially designed to allow Veress needle insertion, the suction cup device has been modified so that it could be crossed by a 5-mm trocar/cannula.
Briefly, twenty-four hours before surgery, all animals started fasting. All pigs were given pre-anesthesia using intramuscular injection of tiletamine hydrochloride and zolazepam hydrochloride (6.3 mg/kg) and medetomidine hydrochloride (1 mg/kg). General anesthesia was inducted with propofol (0.5 mg/kg) and maintained with isoflurane (2%) and oxygen (1 to 2 L) through an endotracheal tube. Animals received a post-operative antibiotic treatment with oxytetracycline (20 mg/kg/day, for 6 days). On the day of the experiment, each animal was placed in a supine position, with all limbs fixed to the operating table, then, careful shaving, cleansing, and disinfection of the operating field with 10% povidone-iodine were performed. During surgery, heart rate, blood pressure, blood oxygen saturation, and central venous pressure were monitored. Infusion of liquids and drugs was achieved through a central venous catheter positioned into the jugular vein and appropriately channeled into the subcutaneous tissue of the neck. Peritoneal cavity was entered with the technique allotted by randomization.
2.2. Surgical procedures
In Group A, the OAT was carried out as follows. Briefly, a 1.5-2.0 cm vertical skin incision was made in the lower abdomen. Dissection was continued down to the fascia while the skin was held laterally retracted. Thereafter, the fascia was incised, and the peritoneal cavity entered by the cannula of a 10-mm nondisposable Hasson trocar (Mölnlycke® Health Care S.r.l., Italia) with blunt obturator inside through the defect. Once successfully entered into the abdomen, the obturator was removed, leaving the cannula positioned correctly. The insufflation tube was connected to the trocar for the creation of the necessary CO2 pneumoperitoneum.
In Group B, the DTI entry technique was performed as follows. A 5-mm skin incision was made in the lower abdomen to accommodate the diameter of a sharp trocar system. The abdominal wall was held and adequately elevated manually and a 5-mm shielded trocar (Endopath® Xcel™ trocar, Ethicon Endo-Surgery, Inc, Cincinnati, OH) was inserted directly into the cavity at a 90° angle and then advanced by a controlled twisting movement. When the surgeon felt the resistance offered by the fascial layer, the abdominal wall was grasped and lifted by hand or using a Backhaus towel clamp to form a “tent” and then moved away from the contents. Entry into the abdominal cavity was confirmed by the audible click of the shield lock on the trocar. Afterwards, the obturator was removed and the cannula was further inserted by 2–3 cm, a laparoscope was placed in the cannula and the placement of the trocar was confirmed. Insufflation was then started.
In Group C, the method adopted for DTI facilitated by the OneShot-M device included the following steps (Figure 2). First, a 5-mm horizontal skin incision was made in the lower abdomen, followed by placement of the suction cup system on the abdominal wall, so that the trocar access hole perfectly matched the small cut below (Figure 2A). At the same time, a 5-mm disposable shielded blade trocar (Endopath® Xcel™ trocar, Ethicon Endo-Surgery, Inc, Cincinnati, OH) was introduced through the specified hole, the tip being directly perpendicular to the incision (Figure 2B). After lightly pressing the device to the abdomen, the abdominal wall was gently lifted by holding the OneShot-M handle and picking up the entire system, thus distancing the abdominal wall from the internal organs and thus creating a “safety room” (Figure 2C-D).
The trocar was then gradually advanced into the peritoneal cavity by twisting it slowly through the OneShot-M. Abdominal penetration could be easily felt by the surgeon and entry into the abdominal cavity was confirmed by the audible double click of the shield lock on the trocar. The trocar blade tip was covered after it entered the peritoneal cavity to reduce the risk of injury to internal organs. After that, the obturator was withdrawn, leaving the 5-mm cannula in place; in order to confirm the correct positioning of the trocar in the peritoneum and the absence of lesions to the viscera, a laparoscope was inserted into the cannula for direct visualization of the abdominal cavity on display. Subsequently, the insufflation tube was attached to the sleeve for pneumoperitoneum induction. After both the laparoscope and the insufflation tube were temporarily pulled from the cannula, the trocar seal was unscrewed to allow removal of OneShot-M. Once the seal was screwed back on, both instruments were reinserted to continue the pneumoinsufflation under direct vision. In all techniques, fascia and skin closure was performed with 2-0 absorbable Vicryl after removal of the access port.
The abdominal cavity was thoroughly inspected after pneumoperitoneum for complications which were classified as major and minor depending on the nature and severity of injuries. For evaluation purposes, the outcome measures were defined as 1. access time: the time interval between skin incision and introduction of the laparoscope for confirmation of access, 2. minor complications (such as difficulty in primary trocar entry, localized emphysema, leakage of gas from the port-site, abdominal bruise/small hematoma at port-site, omental injury), and 3. major complications (such as bowel perforation, mesenteric vascular injury, solid organ injury). Difficulty in inserting the trocar was defined as failure of two attempts to enter into the peritoneal cavity.
2.3. Statistical Analysis
Bodyweight and access time values for all animals were recorded and expressed as kilograms (kg) and seconds (s), respectively. The small sample size led us to choose to conduct a non-parametric analysis on both variables, animal weight and access time, despite the Shapiro-Wilk test of normality did not allow to reject the hypothesis of normality of the distribution of the weight. Therefore, the non-parametric Kruskal-Wallis (KW) test was performed to look for any significant differences in distributions of the variables in the three groups. Dunn's post hoc test, with Bonferroni method, was used to pairwise comparisons [36]. Bonferroni’s method was used because were evaluated all-possible pairs, and the Bonferroni Test value (z-value) has been adjusted for multiple tests by dividing α/2 by k(k-1)/2, making it zα/(k(k-1)), where the k(k-1)/2 is the number of possible pairs of k groups. A p-value of 0.05 was considered statistically significant for all the tests evaluated. All calculations were performed using the SAS 9.4 software (SAS Institute, Inc.).
3. Results
Statistical analysis regarding weight and access time are reported in Table 1. Boxplots relevant to access time values for each technique are represented in Figure 3. The KW test showed no statistically significant differences in body weight between groups (p-value = 0.7253). Median access time was shorter in Group C (43 s, range: 35-49 s), followed by Group B (82.5 s, range 72-90 s) and Group A (190.5 s, range 182-240 s) (Table 1). The KW test exhibited statistically significant differences in procedural time between techniques (p-value = 0.0005, Table 1). Pairwise comparisons using the Dunn's post hoc test, with Bonferroni’s method, detected a statistically significant difference between the groups A and C in terms of access time, that is the time needed for laparoscopic entry in OneShot-M/DTI group was significantly shorter than in the open Hasson group (Table 1). No other comparisons were statistically significant.
Table 2 shows the comparison of three methods of laparoscopic trocar insertion (open, DTI, and OneShot-M/DTI) in terms of complication. Overall, only one minor complication [difficulty in primary trocar entry] happened in the OneShot-M/DTI group. Number of occurrences in the other groups are described in Table 2. The small sample size did not allow to perform any statistical test to verify the association between methods and number of occurrences.
4. Discussion
Laparoscopic abdominal surgery requires the achievement of successful pneumoperitoneum. In order to establish it, the first and most critical step of all laparoscopic procedures is the insertion of surgical instruments to gain access into the peritoneal cavity. In the vast majority of patients, possible reasons of main complications include unsuitable placement of a Veress needle or primary umbilical trocar, which results in abdominal wall bleeding and intra-abdominal complications, that is bowel and major vascular injuries [37]. Furthermore, reliable evidences support a lower relative risk of trocar site-associated bleeding and overall complications with blunt-tipped laparoscopic cannulas than bladed trocars [38]. Intestinal injuries and major vessel lesions incidence are 0.07% and 0.04%, while the overall incidence of these complications at the time of access is 0.11%, although it seems that these adverse events are under-reported [28]. The mortality rate related to bowel damage ranges from 2.5% to 5% [11,16,24,39], whereas a high mortality rate of 8-17% has been described for injuries to major retroperitoneal vessels because of their severe, even life-threatening, complications [40,41,42,43,44,45]. It is clear that preventing the risk of entry-related injuries and optimizing the access technique is essential. Currently, there is still no sufficient evidence in the most respected international literature of which procedure for initial trocar entry, close or open, is the “ideal”, that is to say free of complications [11,46,47]. Moreover, no single method is appropriate for all cases and the technique may be personalized in each case, depending on suitable preoperative evaluation and surgical skills.
DTI method was first described by Dingfelder more than 40 years ago [48]: the surgeon lifts the abdominal wall to avoid injuring the abdominal aorta and directly inserts a trocar into the peritoneal cavity without prior implementing pneumoperitoneum. DTI decreases the number of “blind steps” from three with closed method (Veress needle, insufflation, trocar], to just one (trocar), but it still remains the least-preferred technique owing to the fear of producing lesions to gastrointestinal system and retroperitoneal vessels. It is correctly documented that with DTI it is possible to immediately recognize any kind of intraabdominal injury and to laparoscopically repair that lesion at once [7,20,48,49,50,51,52,53]. Nonetheless, initial trocar entry has been often reported to be time-consuming due to insufflation-related complication, such as gas embolism, as well as the need to repeat the procedure due to failure.
Our pilot study was an effort to improve the safety and effectiveness of DTI technique by facilitating its routine practical applicability for a rapid and risk-free pneumoperitoneum establishment. To address this issue, we described a procedure slightly modified from the standard DTI, since we proposed the employment of a self-designed wall-lifting device, called OneShot-M, which is a secure, quick and very easy-to-use suction cup system that uses manual force to elevate the abdominal wall over the umbilicus and thus favor initial trocar insertion. In order to demonstrate the advantages of the proposed device, we tested its efficacy in facilitating the placement of the primary trocar on animal model, and we also compared the “modified” DTI method against both open and traditional DTI laparoscopy in terms of access times and rates of unpleasant complications.
OneShot-M feasibility had already been successfully proven in 2018 in an experimental study on porcine model, for which the device was specially designed and created in order to allow the passage of a 15 cm-long Veress needle [35]. In that work, the self-made suction cup system allowed us to gain abdominal entry and pneumoperitoneum fast and securely in all procedures, without any intraoperative and postoperative complication linked to Veress needle technique.
According to the promising findings of this previous research [35], in the current study we evaluated OneShot-M performance applied to the DTI method. This goal required the necessary adjustment of the device structure from the aforementioned prototype, in order to create an access hole suitable for the introduction of a 5 mm-long trocar (Figure 1). Therefore, we believed that the gentle lift of the abdominal wall, by picking up our suction cup system, instead of grasping the skin by hand or using towel clips, provides a safer, quick and reliable trocar placement. It is noticed that many surgeons advocate elevating the lower anterior abdominal wall by hand or using Backhaus towel clamps at the time of primary trocar entry, causing aortic injuries and omental perforations as the omentum was elevated [lifted by hand], together with the anterior wall [54,55,56,57].
The idea that the proposed device may be an advisable procedure for executing a safer abdominal access with DTI method was encouraged and confirmed by the results of our pilot study. Concerning intra-abdominal complications, bowel perforation, mesenteric vessel injury and bladder injury were taken as major complications (Table 2). Our tests showed no major complications when the direct trocar insertion by using OneShot-M was performed, whereas one bowel injury (ileum) occurred in the DTI group. Several studies have been focused on comparing the safety of DTI technique to other traditional laparoscopic entry strategies [18,20,49,54,57,58,59,60,61,62,63,64,65,66]. In this regard, the scientific literature supports that DTI is not only faster but also shows trend toward lesser complications than the open method. Falahatkar et al. [62] reported one vascular injury in OAT group (n = 86) and none in DTI group (n = 62). A recent study of Kaistha et al. [18], involving 955 participants, documented two bowel injuries in OAT group and none in DTI group, further strengthening the literature on DTI being a good technique of laparoscopic access. No minor or major complications and a total (100%) feasibility rate have been observed by Agresta et al. [20], in a case-series study involving 2175 DTI procedures. In a large meta-analysis of 51 publications including DTI, open, and Veress needle procedures, Molloy et al. [28] reported that, overall, DTI was correlated with an importantly reduced incidence of major complications equal to 0.05%, when compared to both open (0.11%) and closed (0.09%) methods. Regarding abdominal wall complications, as already defined as minor complications, we did not find localized emphysema, leakage of gas, and bruise/hematoma at the port site in OneShot-M/DTI laparoscopy, whereas only one access problem [initial entry failure] was seen as a minor complication in this group, such that we had to repeat access into the peritoneal cavity in one pig (Table 2). On the other hand, as reported in Table 2, animals experienced these minor complications both in the open and in the DTI group. With regard to minor complications, our findings confirm data in literature, e.g. the aforementioned study of Kaistha et al. [18], in which minor complications occurred more frequently in the OAT, favoring the direct trocar entry technique: significant gas leakage from umbilical port occurred in 39 patients in OAT arm and 4 in DTI arm; DTI was found to be superior to OAT in terms of umbilical port-site hernia, port-site infection, port-site bleed, and port-site pain.
In light of all these scientific evidences, although the small sample size did not allow us to perform any statistical test to confirm the association between methods and number of occurrences, we believed that the absence of minor and major complications observed when the DTI was facilitated by using our wall-lifting device could further enhance the safety of DTI technique and strengthen the literature, already in favor of the advantages of the DTI approach over other entry procedures. In our modification of DTI method, after OneShot-M was applied to the pig’s umbilical region and pressed on the skin, the subsequent negative pressure allowed the abdominal wall to be simply and homogeneously raised, distancing it from the underlying viscera. Subsequent intraabdominal observations confirmed not only a significant displacement of the abdominal wall but also, and above all, the presence of the so-called “dome-effect”, that is the creation of a periumbilical dome, adherent to the suction cup, which generates an adequate “safety room” where the first trocar can be gradually introduced and advanced into the peritoneal cavity through the perforated OneShot-M handle. The increased working space gained with the initial suction dome allowed the surgeon to slightly elevate the abdomen without strong traction and traumas, preventing severe injuries to the internal organs.
Another parameter for successfully performing the laparoscopy procedure is the importance of time. Since by decreasing the time of entry, the overall time of surgery is reduced. In our study, as can be seen in Table 1, DTI with OneShot-M seems to be the fastest (43 s) access technique, compared to conventional DTI (82.5 s), and, ever more, open method (190.5 s) (p-value = 0.0005, Table 1). Furthermore, pairwise comparisons revealed that the operative time needed for laparoscopic entry in OneShot-M/DTI group was significantly shorter only than in the open Hasson group (p-value < 0.001, Table 1), but no other comparisons were statistically significant. As represented in boxplots in Figure 3, by comparing the respective medians and the lengths of the three boxes, we observed that access time values in the OneShot-M/DTI group were less dispersed than the values measured in the other two groups; after all, this minor data variability was confirmed by the range of the operative times, which was smaller in Group C than in Group B and Group A (Table 1). Since it's true that the smaller the number, the higher the repeatability, and the higher the reliability of the results, this finding suggest that the proposed experimental procedure is more reproducible and standardizable than the traditional open and DTI techniques. It’s means that a shorter entry time obtained by using OneShot-M should be achieved again with a high degree of agreement when the access is replicated with the same method by different surgeons and in patients with different features.
Finally, our experiences indicate that our wall-lifting system allowed an effective and fast laparoscopic access controlled by a single surgeon instead of two. This is a significant advantage, as we consider that open technique required the participation of at least two experienced operators. Surgical training may be useful in facilitating the development of surgeons’ skills with regard to the OneShot-M/direct trocar insertion access.
5. Conclusions
These preliminary outcomes suggest that the direct trocar insertion by the self-designed wall-lifting device is technically easy, feasible, reliable, fast and safe in a porcine model and can provide sufficient exposure of the working space. OneShot-M allowed the surgeon to raise the abdominal wall homogeneously, with no risk of internal injury, and with shorter procedural times. Although the encouraging findings, our pilot study has some limits, due to the relatively small number of pigs enrolled in the present experimental design. In the near future, we plan to perform additional animal experiments in order to strengthen scientific evidence in support of the wall-lifting system here discussed. Moreover, confirmation of these results obtained on animal model requires further evaluation in a clinical trial on humans.
Author Contributions
Conceptualization, G.C.; methodology, G.C.; software, R.A.; validation, G.C. and L.C.; formal analysis, R.A. and C.R.; investigation, L.C. and P.L.; data curation, L.C.; writing—original draft preparation, R.C.; writing—review and editing, R.C.; supervision, G.C.; project administration, G.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Council Directive 2010/63/EEC of the European Union and the Italian D. Lgs. 26/2014, and approved by the Ethics Committee of the Istituto Zooprofilattico Sperimentale della Sicilia “A. Mirri” (OpBA, Organismo preposto al Benessere degli Animali) (protocol code n°. 34/2018-PR; 15/01/2019).
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article; further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fujiwara M, Kodera Y, Misawa K, Kinoshita M, Kinoshita T, Miura S, et al. Longterm outcomes of early-stage gastric carcinoma patients treated with laparoscopy-assisted surgery. J Am Coll Surg. 2008, 206, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Ohtani H, Tamamori Y, Noguchi K, Azuma T, Fujimoto S, Oba H, et al. A meta-analysis of randomized controlled trials that compared laparoscopy-assisted and open distal gastrectomy for early gastric cancer. J Gastrointest Surg Off J Soc Surg Aliment Tract. 2010, 14, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Passerotti CC, Begg N, Penna FJ, Passerotti AMAMS, Leite KRM, Antunes AA, et al. Safety profile of trocar and insufflation needle access systems in laparoscopic surgery. J Am Coll Surg. 2009, 209, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Pickett SD, Rodewald KJ, Billow MR, Giannios NM, Hurd WW. Avoiding major vessel injury during laparoscopic instrument insertion. Obstet Gynecol Clin North Am. 2010, 37, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Simforoosh N, Basiri A, Ziaee S-A-M, Tabibi A, Nouralizadeh A, Radfar MH, et al. Major vascular injury in laparoscopic urology. JSLS. 2014, 18, e2014–00283. [Google Scholar]
- Tanaka C, Fujiwara M, Kanda M, Murotani K, Iwata N, Hayashi M, et al. Optical trocar access for initial trocar placement in laparoscopic gastrointestinal surgery: A propensity score-matching analysis. Asian J Endosc Surg. 2019, 12, 37–42. [Google Scholar] [CrossRef]
- Altun H, Banli O, Kavlakoglu B, Kücükkayikci B, Kelesoglu C, Erez N. Comparison between direct trocar and Veress needle insertion in laparoscopic cholecystectomy. J Laparoendosc Adv Surg Tech A. 2007, 17, 709–712. [Google Scholar] [CrossRef]
- Chapron C, Fauconnier A, Goffinet F, Bréart G, Dubuisson JB. Laparoscopic surgery is not inherently dangerous for patients presenting with benign gynaecologic pathology. Results of a meta-analysis. Hum Reprod Oxf Engl. 2002, 17, 1334–1342. [Google Scholar] [CrossRef]
- Tuveri M, Tuveri A. Laparoscopic cholecystectomy: complications and conversions with the 3-trocar technique: a 10-year review. Surg Laparosc Endosc Percutan Tech. 2007, 17, 380–384.
- Vilos, G.A. The ABCs of a safer laparoscopic entry. J Minim Invasive Gynecol 2006, 13, 249–251. [Google Scholar] [CrossRef]
- Vilos GA, Ternamian A, Dempster J, Laberge PY, CLINICAL PRACTICE GYNAECOLOGY COMMITTEE. Laparoscopic entry: a review of techniques, technologies, and complications. J Obstet Gynecol Can JOGC. 2007, 29, 433–447. [Google Scholar] [CrossRef] [PubMed]
- Yanke BV, Horowitz M. Safety of the Veress needle in pediatric laparoscopy. J Endourol. 2007, 21, 695–697. [Google Scholar] [CrossRef]
- Jansen FW, Kapiteyn K, Trimbos-Kemper T, Hermans J, Trimbos JB. Complications of laparoscopy: a prospective multicentre observational study. Br J Obstet Gynaecol. 1997, 104, 595–600. [Google Scholar] [CrossRef]
- Magrina, JF. Complications of laparoscopic surgery. Clin Obstet Gynecol. 2002, 45, 469–480. [Google Scholar] [CrossRef]
- Catarci M, Carlini M, Gentileschi P, Santoro E. Major and minor injuries during the creation of pneumoperitoneum. A multicenter study on 12,919 cases. Surg Endosc. 2001, 15, 566–569. [Google Scholar] [CrossRef] [PubMed]
- Fuller J, Ashar BS, Carey-Corrado J. Trocar-associated injuries and fatalities: an analysis of 1399 reports to the FDA. J Minim Invasive Gynecol. 2005, 12, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Jansen FW, Kolkman W, Bakkum EA, de Kroon CD, Trimbos-Kemper TCM, Trimbos JB. Complications of laparoscopy: an inquiry about closed- versus open-entry technique. Am J Obstet Gynecol. 2004, 190, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Kaistha S, Kumar A, Gangavatiker R, Br S, Sisodiya N. Laparoscopic Access: Direct Trocar Insertion Versus Open Technique. J Laparoendosc Adv Surg Tech A. 2019, 29, 489–494. [Google Scholar] [CrossRef]
- Munro, MG. Laparoscopic access: complications, technologies, and techniques. Curr Opin Obstet Gynecol. 2002, 14, 365–374. [Google Scholar] [CrossRef]
- Agresta F, Mazzarolo G, Bedin N. Direct trocar insertion for laparoscopy. JSLS 2012, 16, 255–259. [Google Scholar] [CrossRef]
- Shirk GJ, Johns A, Redwine DB. Complications of laparoscopic surgery: How to avoid them and how to repair them. J Minim Invasive Gynecol. 2006, 13, 352–359. [Google Scholar] [CrossRef]
- Taye MK, Fazal SA, Pegu D, Saikia D. Open Versus Closed Laparoscopy: Yet an Unresolved Controversy. J Clin Diagn Res JCDR 2016, 10, QC04–QC07.
- Neudecker J, Sauerland S, Neugebauer E, Bergamaschi R, Bonjer HJ, Cuschieri A, et al. The European Association for Endoscopic Surgery clinical practice guideline on the pneumoperitoneum for laparoscopic surgery. Surg Endosc. 2002, 16, 1121–1143. [Google Scholar] [CrossRef]
- Krishnakumar S, Tambe P. Entry complications in laparoscopic surgery. J Gynecol Endosc Surg. 2009, 1, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Bonjer HJ, Hazebroek EJ, Kazemier G, Giuffrida MC, Meijer WS, Lange JF. Open versus closed establishment of pneumoperitoneum in laparoscopic surgery. Br J Surg. 1997, 84, 599–602. [Google Scholar]
- Chapron C, Cravello L, Chopin N, Kreiker G, Blanc B, Dubuisson JB. Complications during set-up procedures for laparoscopy in gynecology: open laparoscopy does not reduce the risk of major complications. Acta Obstet Gynecol Scand. 2003, 82, 1125–1129. [Google Scholar] [CrossRef]
- Larobina M, Nottle P. Complete evidence regarding major vascular injuries during laparoscopic access. Surg Laparosc Endosc Percutan Tech. 2005, 15, 119–123. [Google Scholar] [CrossRef]
- Molloy D, Kaloo PD, Cooper M, Nguyen TV. Laparoscopic entry: a literature review and analysis of techniques and complications of primary port entry. Aust N Z J Obstet Gynaecol. 2002, 42, 246–254. [Google Scholar] [CrossRef]
- Schäfer M, Lauper M, Krähenbühl L. Trocar and Veress needle injuries during laparoscopy. Surg Endosc. 2001, 15, 275–280. [Google Scholar] [CrossRef]
- Zaraca F, Catarci M, Gossetti F, Mulieri G, Carboni M. Routine use of open laparoscopy: 1,006 consecutive cases. J Laparoendosc Adv Surg Tech A. 1999, 9, 75–80. [Google Scholar] [CrossRef]
- Kaali, S.G. Introduction of the Opti-trocar. J Am Assoc Gynecol Laparosc. 1993, 1, 50–53. [Google Scholar] [CrossRef]
- Berch BR, Torquati A, Lutfi RE, Richards WO. Experience with the optical access trocar for safe and rapid entry in the performance of laparoscopic gastric bypass. Surg Endosc. 2006, 20, 1238–1241. [Google Scholar] [CrossRef] [PubMed]
- Sharp HT, Dodson MK, Draper ML, Watts DA, Doucette RC, Hurd WW. Complications associated with optical-access laparoscopic trocars. Obstet Gynecol. 2002, 99, 553–555. [Google Scholar]
- Tinelli A, Malvasi A, Mynbaev OA, Tsin DA, Davila F, Dominguez G, et al. Bladeless direct optical trocar insertion in laparoscopic procedures on the obese patient. JSLS 2013, 17, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Cassata G, Palumbo V, Cicero L, De Luca A, Damiano G, Fazzotta S, et al. OneShot-M: A New Device for Close Laparoscopy Pneumoperitoneum. Surg Innov. 2018, 25, 570–577. [Google Scholar] [CrossRef]
- Daniel, W.W. Applied Nonparametric Statistics; PWS-KENT: Boston, MA, USA, 1990. [Google Scholar]
- Philips PA, Amaral JF. Abdominal access complications in laparoscopic surgery. J Am Coll Surg. 2001, 192, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Antoniou SA, Antoniou GA, Koch OO, Pointner R, Granderath FA. Blunt versus bladed trocars in laparoscopic surgery: a systematic review and meta-analysis of randomized trials. Surg Endosc. 2013, 27, 2312–2320. [Google Scholar] [CrossRef] [PubMed]
- Chandler JG, Corson SL, Way LW. Three spectra of laparoscopic entry access injuries. J Am Coll Surg. 2001, 192, 478–490. [Google Scholar] [CrossRef]
- Azevedo JLMC, Azevedo OC, Miyahira SA, Miguel GPS, Becker OM, Hypólito OHM, et al. Injuries caused by Veress needle insertion for creation of pneumoperitoneum: a systematic literature review. Surg Endosc. 2009, 23, 1428–1432. [Google Scholar] [CrossRef]
- Chapron C, Querleu D, Bruhat MA, Madelenat P, Fernandez H, Pierre F, et al. Surgical complications of diagnostic and operative gynaecological laparoscopy: a series of 29,966 cases. Hum Reprod Oxf Engl. 1998, 13, 867–872. [Google Scholar] [CrossRef]
- Dunne N, Booth MI, Dehn TCB. Establishing pneumoperitoneum: Verres or Hasson? The debate continues. Ann R Coll Surg Engl. 2011, 93, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Makai G, Isaacson K. Complications of gynecologic laparoscopy. Clin Obstet Gynecol. 2009, 52, 401–411. [Google Scholar] [CrossRef] [PubMed]
- McDonald PT, Rich NM, Collins GJ, Andersen CA, Kozloff L. Vascular trauma secondary to diagnostic and therapeutic procedures: laparoscopy. Am J Surg. 1978, 135, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Opitz I, Gantert W, Giger U, Kocher T, Krähenbühl L. Bleeding remains a major complication during laparoscopic surgery: analysis of the SALTS database. Langenbecks Arch Surg. 2005, 390, 128–133. [Google Scholar] [CrossRef]
- Ahmad G, Duffy JMN, Phillips K, Watson A. Laparoscopic entry techniques. Cochrane Database Syst Rev. 2008, 16, CD006583. [Google Scholar]
- Tinelli A, Malvasi A, Istre O, Keckstein J, Stark M, Mettler L. Abdominal access in gynaecological laparoscopy: a comparison between direct optical and blind closed access by Verres needle. Eur J Obstet Gynecol Reprod Biol. 2010, 148, 191–194. [Google Scholar] [CrossRef]
- Dingfelder, JR. Direct laparoscope trocar insertion without prior pneumoperitoneum. J Reprod Med. 1978, 21, 45–47. [Google Scholar]
- Günenç MZ, Yesildaglar N, Bingöl B, Onalan G, Tabak S, Gökmen B. The safety and efficacy of direct trocar insertion with elevation of the rectus sheath instead of the skin for pneumoperitoneum. Surg Laparosc Endosc Percutan Tech. 2005, 15, 80–81. [Google Scholar] [CrossRef]
- Inan A, Sen M, Dener C, Bozer M. Comparison of direct trocar and veress needle insertion in the performance of pneumoperitoneum in laparoscopic cholecystectomy. Acta Chir Belg. 2005, 105, 515–518. [Google Scholar] [CrossRef]
- Moreno DG, Pereira CAM, Sant Anna RK, de Azevedo RU, Savio LF, Duarte RJ, et al. Laparoscopic Insertion of Various Shaped Trocars in a Porcine Model. JSLS 2019, 23, e2019–00002. [Google Scholar]
- Theodoropoulou K, Lethaby DR, Bradpiece HA, Lo TL, Parihar A. Direct trocar insertion technique: an alternative for creation of pneumoperitoneum. JSLS 2008, 12, 156–158. [Google Scholar]
- Zakherah, MS. Direct trocar versus veress needle entry for laparoscopy: a randomized clinical trial. Gynecol Obstet Invest. 2010, 69, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Nezhat FR, Silfen SL, Evans D, Nezhat C. Comparison of direct insertion of disposable and standard reusable laparoscopic trocars and previous pneumoperitoneum with Veress needle. Obstet Gynecol. 1991, 148–150. [Google Scholar]
- Roy GM, Bazzurini L, Solima E, Luciano AA. Safe technique for laparoscopic entry into the abdominal cavity. J Am Assoc Gynecol Laparosc. 2001, 8, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Corson SL, Brooks PG, Soderstrom RM. Safe technique for laparoscopic entry into the abdominal cavity. J Am Assoc Gynecol Laparosc. 2002, 9, 399. [Google Scholar]
- Hill DJ, Maher PJ. Direct cannula entry for laparoscopy. J Am Assoc Gynecol Laparosc. 1996, 4, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Jacobson MT, Osias J, Bizhang R, Tsang M, Lata S, Helmy M, et al. The direct trocar technique: an alternative approach to abdominal entry for laparoscopy. JSLS. 2002, 6, 169–174. [Google Scholar]
- Copeland C, Wing R, Hulka JF. Direct trocar insertion at laparoscopy: an evaluation. Obstet Gynecol. 1983, 62, 655–659. [Google Scholar]
- Saidi, MH. Direct laparoscopy without prior pneumoperitoneum. J Reprod Med. 1986, 31, 684–686. [Google Scholar]
- Jarrett, JC. Laparoscopy: direct trocar insertion without pneumoperitoneum. Obstet Gynecol. 1990, 75, 725–727. [Google Scholar]
- Falahatkar S, Nadjafi-Semnani M, Panahandeh Z, Allahkhah A, Emadi S, Motevali S, et al. Direct Trocar Insertion Compare With Open Laparoscopy [Hasson Technique] in Patients Undergoing Urolaparoscopic Surgery. Urotoday Int J 2009, 2.
- Byron JW, Fujiyoshi CA, Miyazawa K. Evaluation of the direct trocar insertion technique at laparoscopy. Obstet Gynecol. 1989, 74 Pt 1, 423–425. [Google Scholar]
- Borgatta L, Gruss L, Barad D, Kaali SG. Direct trocar insertion vs. Verres needle use for laparoscopic sterilization. J Reprod Med. 1990, 35, 891–894.
- Angioli R, Terranova C, De Cicco Nardone C, Cafà EV, Damiani P, Portuesi R, et al. A comparison of three different entry techniques in gynecological laparoscopic surgery: a randomized prospective trial. Eur J Obstet Gynecol Reprod Biol. 2013, 171, 339–342. [Google Scholar] [CrossRef]
- Byron JW, Markenson G, Miyazawa K. A randomized comparison of Verres needle and direct trocar insertion for laparoscopy. Surg Gynecol Obstet. 1993, 177, 259–262. [Google Scholar]
Figure 1.
OneShot-M prototype modified to allow the insertion of a 5-mm trocar.
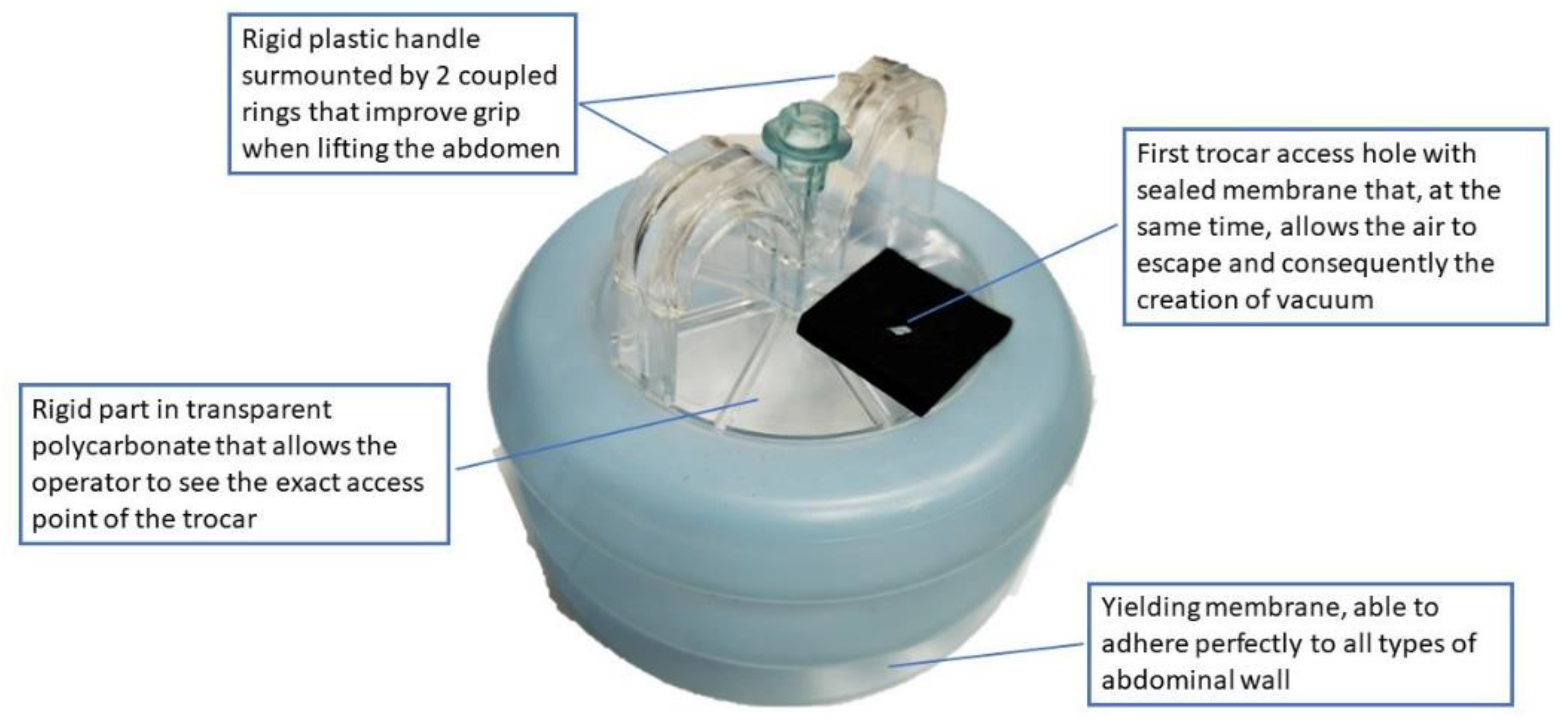
Figure 2.
Direct trocar insertion by using OneShot-M device. [A] The suction cup system is positioned on the abdominal wall so that the trocar access hole perfectly matches the 5-mm horizontal skin incision below. [B] The device is lightly pressed on the abdomen. [C] The abdominal wall is gently lifted by holding OneShot-M handle and the entire system is picked up, in order to distance the abdominal wall from the internal organs. [D] After being introduced through the specified hole and the small cut, a 5-mm single-use shielded bladed trocar is then gradually advanced into the peritoneal cavity by twisting it slowly through the OneShot-M.
Figure 2.
Direct trocar insertion by using OneShot-M device. [A] The suction cup system is positioned on the abdominal wall so that the trocar access hole perfectly matches the 5-mm horizontal skin incision below. [B] The device is lightly pressed on the abdomen. [C] The abdominal wall is gently lifted by holding OneShot-M handle and the entire system is picked up, in order to distance the abdominal wall from the internal organs. [D] After being introduced through the specified hole and the small cut, a 5-mm single-use shielded bladed trocar is then gradually advanced into the peritoneal cavity by twisting it slowly through the OneShot-M.
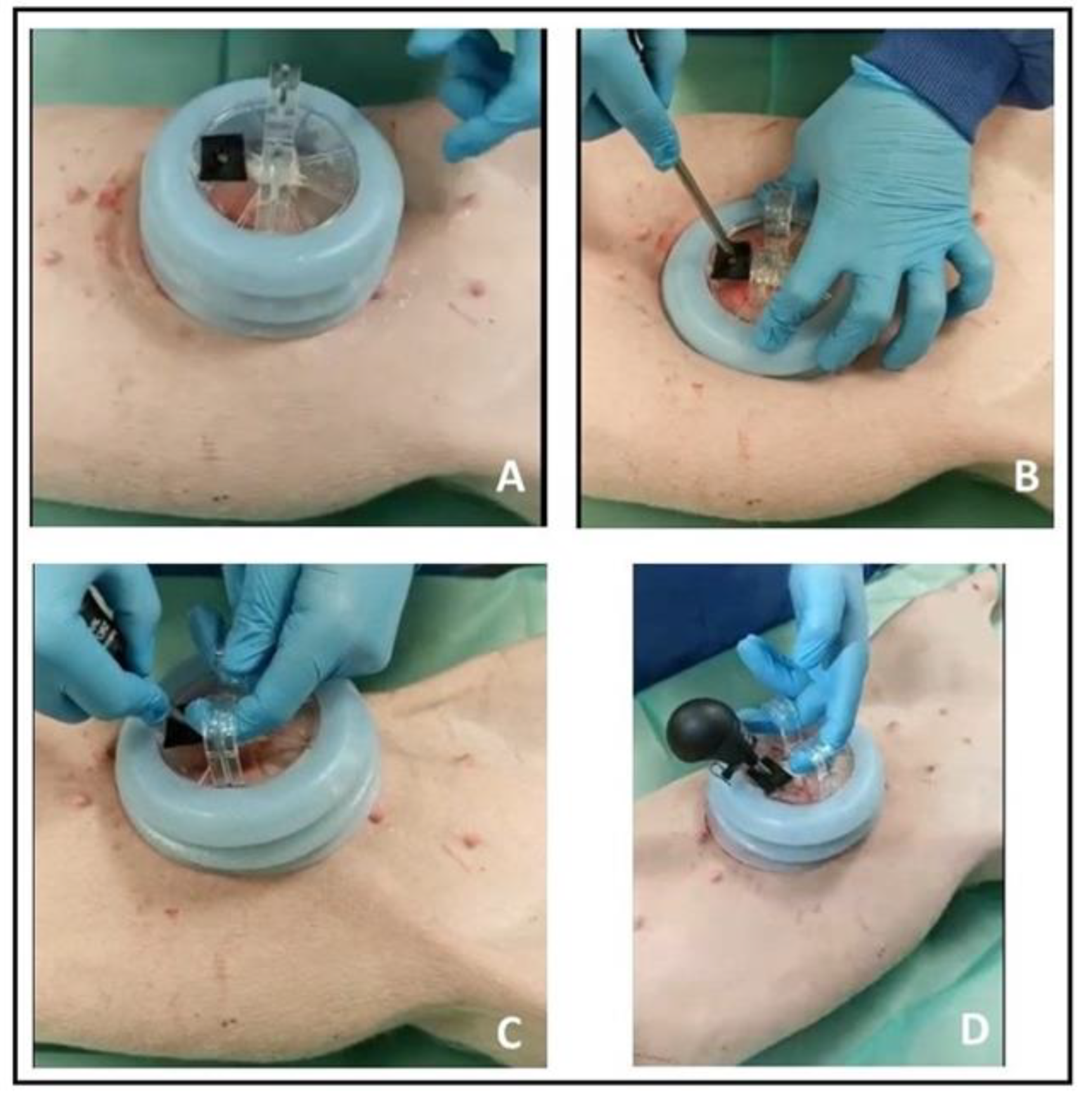
Figure 3.
Boxplots of access time (s) values of the three different laparoscopic access techniques.
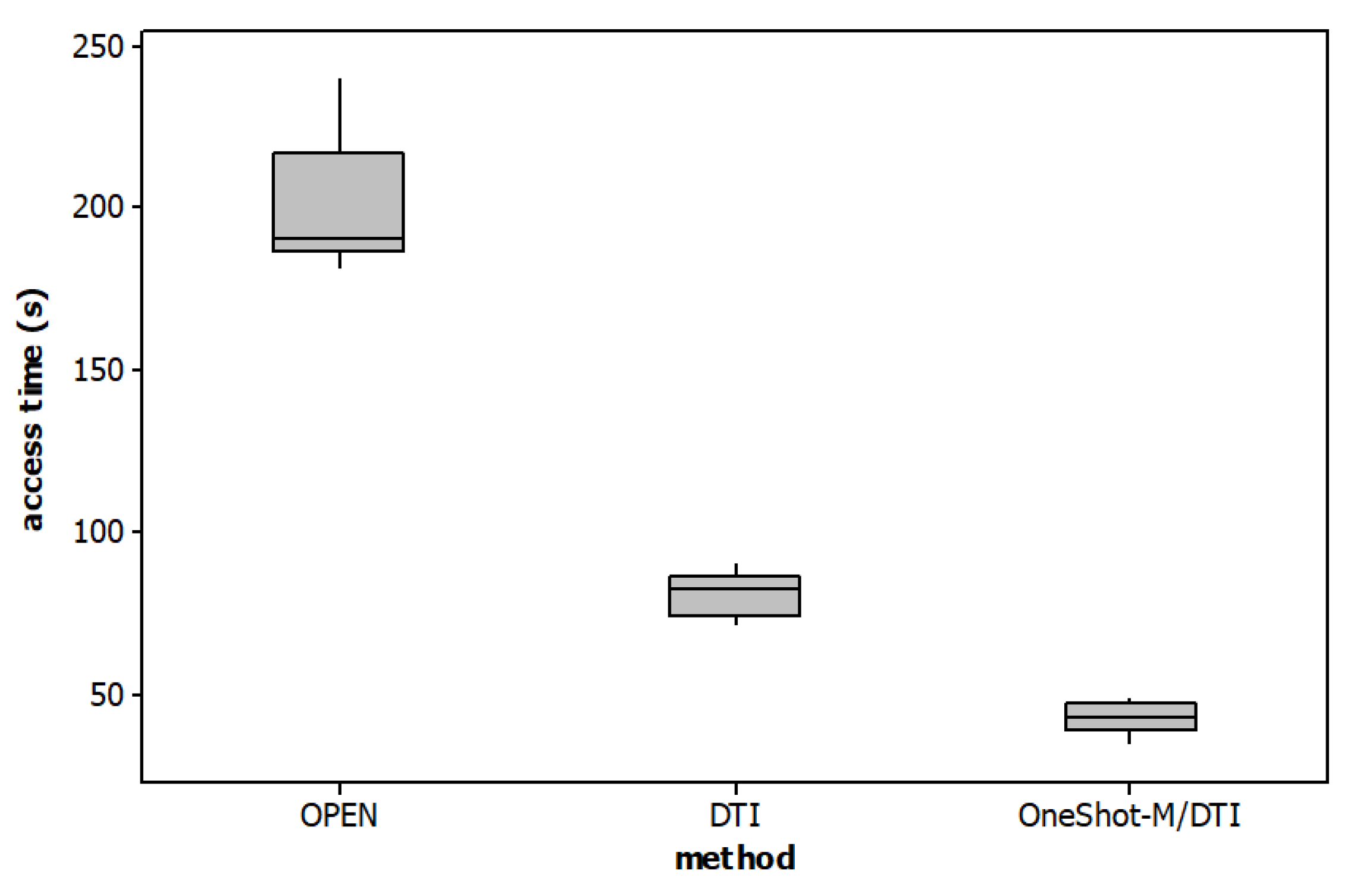

Table 1.
Comparison of three methods of laparoscopic trocar insertion; statistical analysis.
| Methods | Median (range) | Kruskal-Wallis Test (p-value) | Comparison | Dunn’s post hoc test (p-value) |
|
|---|---|---|---|---|---|
| Weight | Group A: OPEN | 33.15 (31.2 – 3) | 0.725 | ||
| Group B: DTI | 32.5 (30 – 35) | ||||
| Group C: OneShot-M/DTI | 33.25 (31.3 – 35) | ||||
| Access time | Group A: OPEN | 190.5 (182 – 240) | 0.0005 | A vs B | 0.155 |
| Group B: DTI | 82.5 (72 – 90) | A vs C | <0.001 | ||
| Group C: OneShot-M/DTI | 43 (35 – 49) | B vs C | 0. 155 |
Table 2.
Comparison of three methods of laparoscopic trocar insertion (open vs. DTI vs. OneShot-M/DTI) in terms of complication. The results are expressed as percentages and in brackets the number of occurrences.
Table 2.
Comparison of three methods of laparoscopic trocar insertion (open vs. DTI vs. OneShot-M/DTI) in terms of complication. The results are expressed as percentages and in brackets the number of occurrences.
|
Complication % (number) |
Group A OPEN(n = 6) |
Group B DTI (n = 6) |
Group C OneShot-M/DTI (n = 6) |
| Difficulty in entry | 33.33 (2) | 50 (3) | 16.67 (1) |
| Localized emphysema | 16.67 (1) | 16.67 (1) | - |
| Leakage of gas | 50.00 (3) | 16.67 (1) | - |
| Bruise/haematoma at port site | 16.67 (1) | 50.00 (3) | - |
| Omental injury | - | - | - |
| Bowel perforation | - | 16.67 (1) | - |
| Mesenteric vascular injury | - | - | - |
| Solid-organ injury | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



