
Submitted:
10 October 2023
Posted:
11 October 2023
You are already at the latest version
Abstract
In this study, we aimed to identify blood lymphocytes as a prognostic factor for survival in patients with locally advanced stage III non-small cell lung cancer (NSCLC) treated with concurrent chemoradiotherapy (CCRT). We conducted a secondary analysis of 196 patients enrolled in the Korean Radiation Oncology Group 0903 phase III clinical trial to evaluate the prognostic significance of circulating blood lymphocyte levels. The median total lymphocyte count (TLC) reduction ratio during CCRT was 0.74 (range: 0.29 – 0.97). In multivariate analysis, patient age (p = 0.014) and gross tumor volume (GTV, p = 0.031) were significant factors associated with overall survival, while TLC reduction (p = 0.018) and pretreatment neutrophil-to-lymphocyte ratio (NLR; p = 0.010) were associated with progression-free survival (PFS). In multivariate logistic regression analysis, pretreatment NLR, GTV, and heart V20 were significantly associated with TLC reduction. TLC reduction during CCRT is a significant prognostic factor for PFS, and heart V20 is significantly associated with TLC reduction. Thus, constraining the volume of the radiation dose to the whole heart must be prioritized to reduce TLC.
Keywords:
Blood lymphocytes
; CCRT
; non-small cell lung cancer
1. Introduction
Immune surveillance plays an important role in the pathogenesis and progression of non-small cell lung cancer (NSCLC). The failure of host immune surveillance mechanisms, in which lymphocytes play a pivotal role, is a key step in the early stages of tumor development [1]. The outcome of cancer-immune interactions —“cancer immunogram”— is based on a number of largely unrelated parameters, such as tumor “foreignness” and T-cell inhibitory mechanisms, and the proposed cancer immunogram assumes that T-cell activity is the ultimate effector mechanism in human tumors [2]. Among the parameters constituting a reasonable framework for building such an immunogram, targetable biomarkers for immunotherapy are the lymphocyte count, intratumoral T-cell infiltration, and the presence of T-cell checkpoints, such as cytotoxic T lymphocyte-associated protein 4 (CTLA4) and programmed cell death protein 1 (PD1) – known as immune checkpoints. Immune checkpoint inhibitors (ICIs) are approved for the treatment of advanced NSCLC [3,4].
Lymphocytes are highly sensitive to radiotherapy (RT) and a reduction in total blood lymphocyte count is a common consequence of irradiation [5]. Reduced absolute lymphocyte count (ALC) and an elevated neutrophil-to-lymphocyte ratio (NLR) are independent negative prognostic factors for survival in many malignancies [6-11]. The occurrence of radiation-associated lymphopenia (RAL) is dependent on the field size, fraction number, and treatment duration [12,13]. In particular, exposure of immune-related organs, such as the lungs and heart, is associated with immunosuppression during treatment, resulting in worse patient outcomes [8,14]. Moreover, severe lymphopenia at the onset of immunotherapy is associated with poor survival in patients treated with ICIs [15]. In clinical settings, following the concurrent administration of RT and ICIs, RAL at the onset of ICI therapy was found to be associated with increased mortality. The authors explained that the effector activity of ICIs relies on cytotoxic T lymphocytes, and that RAL might negate the activity of ICIs.
Therefore, in the present study, we aimed to identify blood lymphocytes as a prognostic factor for survival and identify any risk factors affecting clinically significant RAL.
2. Materials and Methods
2.1. Participants
The current study was a secondary analysis of 196 eligible patients enrolled in the Korean Radiation Oncology Group (KROG) 0903 phase III prospective randomized multicenter clinical trial. Details on the patient eligibility criteria and treatment are reported in the primary outcome manuscript [16]. The overall treatment scheme for the KROG 0903 trial is shown in Figure 1.
2.2. Dosimetric Analysis and Hematologic Evaluation
Treatment plans were generated with lung heterogeneity correction using Eclipse version 8.1 (Varian Medical Systems, Palo Alto, CA, USA). For treatment planning, the dosimetric constraints for normal tissues included the lungs, heart, and esophagus. The esophageal contour began at the level of the cricoid cartilage and extended to the gastroesophageal junction. The lung contours included the air-inflated lung parenchyma, excluding fluid and atelectasis on CT scans. Heart contours were reviewed and recontoured as necessary according to the RTOG 0617 secondary analysis atlas [17]. The relative percent volumes of the lung and heart receiving at least 2, 5, 10, 12.5, 15, 20, 30, 40, 50, and 60 Gy, and the mean doses were identified. There was a strong correlation between clinical factors, particularly among the dose-volume histogram parameters. To avoid multicollinearity, the variance inflation factor or Pearson’s correlation coefficient was calculated. Finally, we chose lung V2, V20, V50, and V60 and heart V2, V20, V50, and V60. None of the variables had a variance inflation factor of >10 or a Pearson correlation coefficient of ≥ 0.8.
The peripheral blood count was analyzed before, during, and after concurrent chemoradiotherapy (CCRT). Complete blood count data, including the white blood cell (WBC) count, ALC, monocyte count, and absolute neutrophil count (ANC), were collected within 2 weeks before initiating RT, weekly during CCRT, and randomly whenever patients were followed up after completing RT. The nadir blood count was the lowest during CCRT. The NLR was calculated by dividing the ANC by the ALC. Clinically significant lymphopenia was defined as an ALC nadir of < 500 cells/µL during CCRT. Total lymphocyte count (TLC) reduction was defined as the ratio of baseline TLC minus nadir TLC during CCRT to baseline TLC.
2.3. Immunohistochemistry for Programmed Death-Ligand 1 (PDL1) and CD8
Immunohistochemistry was performed using formaldehyde-fixed paraffin-embedded (FFPE) tissue specimens obtained on the first diagnostic biopsy of 84 patients. Immunohistochemical staining was performed with 5-μm entire standard tissue sections of FFPE tumor samples. To detect PDL1, a pre-diluted PDL1 rabbit monoclonal antibody (SP263; Ventana Medical Systems, Oro Valley, Arizona, USA) was used as the primary antibody, with staining performed on a Ventana Benchmark Ultra autostainer using an UltraView diaminobenzidine kit (Ventana Medical Systems, Oro Valley, AZ, USA). Immunohistochemical staining for CD8 expression on T cells was performed using an anti-CD8 mouse monoclonal antibody (clone 144 B, diluted 1:100; Abcam, Cambridge, UK) as the primary antibody, with staining performed using the BondMax Leica autostainer.
2.3.1. Assessment of PDL1 Expression
PDL1 expression in the tumor cells was quantitatively measured using an established immunohistochemical assay (Ventana SP 263). The PDL1 tumor proportion score (TPS), which is the percentage of tumor cells showing partial or complete membrane staining, was calculated. PDL1 expression in ≥ 1% of tumor cells was considered positive. We divided patients into PDL1-positive and PDL1-negative groups (Figure 2A,B).
2.3.2. Assessment of CD8 Expression on Tumor-Infiltrating Lymphocytes (TILs)
CD8 expression on lymphocytes was reported as the proportion of positive cells among all nucleated cells in the adjacent stromal compartment of the tumor nests. Scoring was recorded as the count of TILs with CD8 expression, which was classified as a low count (< 30%) or a high count (≥ 30%) (Figure 2C,D).
2.4. Follow-Up and Statistical Analyses
The patients were evaluated weekly and clinically indicated during treatment, and the protocol was continued as needed. After the completion of CCRT, patients were followed-up using CT after 1 month and then at 3–month intervals for the first 1–3 years, and then every 6 after 3 years thereafter until death. Acute and late toxicities were graded using the Common Terminology Criteria for Adverse Events (CTCAE), version 3.0. Acute toxicities were defined as those that occurred within 90 days of treatment initiation, while late toxicities were defined as those that occurred thereafter. The maximum toxicity grade was chosen to represent the final toxicity grade among the acute toxicities during radiotherapy and late toxicities at follow-up visits. Progression-free survival (PFS) was defined as the period between the start of CCRT and tumor progression or death in the absence of disease progression. Disease progression within the initial radiation field, which included the primary tumor and the involved lymph nodes, was defined as local failure; distant failure was defined as recurrence outside the radiation field; and elective nodal failure is defined as an uninvolved nodal failure outside the initial irradiation field.
Survival rates were calculated using the Kaplan–Meier method and compared using log-rank statistics. The forward conditional Cox regression model was used for the multivariate analysis. Multivariate logistic regression was used to analyze the correlation between TLC reduction and dosimetric parameters. Maxstat, the maximum chi-square method in R 2.13.0 (R Development Core Team, Vienna, Austria, http://www.R-project.org), was used to identify the optimal cutting points. Statistical analyses were performed using SPSS, version 21 (SPSS Inc., Chicago, IL, USA), and p-values < 0.05 were considered statistically significant.
3. Results
3.1. Patient Characteristics
The clinical characteristics of the 196 patients are presented in Table 1. A total of 183 patients (93.4%) were men, with an age range of 40 to 75 years (median: 66 years). Among them, 146 patients (74.5%) had squamous cell carcinoma, with stage IIIA and IIIB tumors constituting 71.9% and 28.1% of the cases, respectively. FDG-PET was performed for all patients. The median follow-up period for all patients was 23 months (range: 2–99 months). The median follow-up time was 40 months for the surviving patients.
3.2. Survival Analysis and Prognostic Factor Determination
The median overall survival (OS) of all 196 patients was 29 months, and the 2-year and 5-year OS rates were 55.9% and 29.8%, respectively. The 2-year and 5-year PFS rates were 32.3% and 25.3%, respectively, and with median PFS of 12 months. The 2-year and 5-year actuarial local control rates were 54.3% and 48.1%, respectively, and the elective nodal failure rate was 6.1% (observed in 12 of 196 patients). The factors associated with OS and PFS in univariate analysis are summarized in Table 2.
In the multivariate analysis, age and GTV were identified as significant factors associated with OS, while TLC reduction and pretreatment NLR were associated with PFS (Table 3, Figure 3). Both local recurrence-free survival (LRFS) and distant recurrence-free survival (DRFS) were significantly associated with TLC reduction during CCRT. In contrast, the GTV was significantly associated with LRFS, and the pretreatment NLR was associated with DRFS.
3.3. Association between Peripheral Blood Cells and Dosimetric Parameters
The median WBC, lymphocyte, neutrophil, and monocyte counts before CCRT were 8700 cells/μL (range: 3400–32800 cells/μL), 2130 cells/μL (range: 860–4640 cells/μL), 4985 cells/μL (range: 1039–9760 cells/μL), and 680 cells/μL (range: 150–1870 cells/μL), respectively (Table 1). Lymphocytes decreased more markedly than other blood cell counts immediately after the second week of CCRT (Figure 4). From weeks 2 to 6, the median ALC was 1520 cells/μL, 1060 cells/μL, 795 cells/μL, 675 cells/μL, and 615 cells/μL, respectively. The median ALC nadir during CCRT was 555 cells/μL (range: 50–1930 cells/μL); the difference between the ALC before CCRT and nadir was 1520 cells/μL (range: 440–3640 cells/μL); and the median TLC reduction was 0.74 (range: 0.29–0.97). Lymphopenia was the most common hematologic toxicity grade ≥ 3 during CCRT (Table 4).
In multivariate logistic regression analysis, the pretreatment NLR, GTV, and heart V20 were significantly associated with TLC reduction (Table 5). Patient age, treatment duration, and RT technique were not significant factors in the multivariate analysis. Lung V2, lung V20, and heart V2 doses were significantly associated with TLC reduction in univariate analysis, although the significance was not retained in multivariate analysis.
3.4. Toxicity Analysis
The overall incidence rates of radiation pneumonitis and esophagitis are shown in Table 4. Clinically significant radiation pneumonitis and esophagitis of grade ≥ 3 was observed in ten patients (5.1%) and seven patients (3.6%), respectively. On pretreatment CT scans, nine patients (4.6%) had interstitial lung disease. On univariate analysis, older age, lower lobe interstitial lung disease, and low diffusing capacity for carbon monoxide were significantly associated with grade ≥ 3 radiation pneumonitis (Supplementary Table S1). Dosimetric analysis showed that MLD, V5, V10, V20, and V30 of the whole lung were significantly associated with grade ≥ 3 radiation pneumonitis (Supplementary Table S2). Dosimetric parameters were not significantly associated with grade ≥ 3 radiation esophagitis, but there was a trend toward a higher radiation dose in patients with severe grade ≥ 3 radiation esophagitis (Supplementary Table S3). After CCRT, 22 patients (11.2%) developed heart disease. Eleven patients had heart problems before treatment, including nine with ischemic heart disease and two with arrhythmia. Most cardiac events occurred within 3 years of CCRT, and there was no significant association between clinical factors and cardiac events after CCRT. Maximum doses to the entire heart and left ventricle were significantly associated with cardiac toxicity after CCRT (Supplementary Table S4).
3.5. Subgroup Analysis for PD-L1 and CD8 TIL Expression
For PDL1 and CD8 analyses, adequate histological tissues containing abundant tumor cells were obtained from 84 patients. The relationship between PDL1 expression and patient characteristics is shown in Table 6.
No significant correlation was found between PDL1 expression and patient characteristics. Patients with more advanced disease stages showed a tendency toward PDL1 expression (p = 0.070). No correlation was between PDL1 and CD8 expression. CD8 expression was not significantly associated with the pretreatment lymphocyte count (p = 0.673), and PDL1 expression was not significantly associated with OS or PFS (Figure 5A,C). Univariate analysis revealed that high CD8 expression in TILs was associated with favorable OS (Figure 5B, p = 0.068) and was significantly associated with favorable PFS (Figure 5D, p = 0.032).
according to (C) PDL1 (no vs. yes) and (D) CD8+ TIL low group or high group.
4. Discussion
Platinum-based doublet concurrent chemoradiotherapy (CCRT) followed by durvalumab has been the standard treatment for eligible patients with locally advanced unresectable NSCLC, with good performance and minimal weight loss [18-20]. Suboptimal primary tumor control has led to radiation dose escalation studies aimed at achieving better treatment outcomes. RTOG 0617 was a landmark study that compared high-dose RT (74 Gy) and standard-dose RT (60 Gy) with or without cetuximab in patients with IIIA or IIIIB NSCLC [21]. The median OS was 28.7 months for patients who received standard-dose radiotherapy and 20.3 months for those who received high-dose radiotherapy (p = 0.004). Unexpectedly, there were more treatment-related deaths among patients treated with high-dose RT.
A secondary study of the RTOG 0617 trial evaluated host immune function and tumor control [22]. The effective dose to immune cells was modeled using the RT fractions and doses to the lungs, heart, and whole body. The 2-year OS of patients with a high effective dose to immune cells was poor. Immunotoxicity associated with RT has been shown to be a predictive factor for treatment outcomes. The immunosuppressive effects of RT include the inactivation of lymphocytes, recruitment of MDSCs and Treg lymphocytes, M2 polarization of macrophages, secretion of TGF-β, and induction of PDL1 expression on tumor cells [23].
Lymphocytes are highly sensitive to radiation; indeed, the LD50 of lymphocytes (lethal dose required to reduce the surviving fraction of lymphocytes by 50%) is approximately 2 Gy, and the LD90 is 3 Gy [24]. TLC remains stable during neoadjuvant chemotherapy, grade III–IV lymphocyte reduction was observed in nearly half of the patients 2 months after the initiation of radiation [6]. Treatment-related lymphopenia is more likely to be radiation-related than chemotherapy-related. Our study showed that lymphopenia was the most common grade ≥ 3 hematologic toxicity during CCRT and lymphocytes decreased more markedly than the other blood cells immediately after CCRT. The median TLC reduction ratio was 0.74, indicating severe lymphopenia.
Joseph et al. demonstrated that lymphopenia is associated with poor survival in patients with lung cancer [10]. In multivariate analysis, low post-treatment ALC, high pre-treatment ANC, and high PTV integral dose were associated with poor survival. The authors explained that a high pre-treatment ANC indicates cancer-induced inflammation and is useful for predicting aggressive tumor biology. Neutrophils promote tumor growth by inducing tumor growth and angiogenesis [25]. The current study demonstrated that TLC reduction was significantly associated with PFS, and that the pretreatment NLR was significantly associated with DRFS. In many studies, a high NLR has been recognized as a poor prognostic indicator of solid cancers [7,11].
Tang et al. sought to determine factors associated with lymphopenia in patients receiving definitive radiotherapy for NSCLC [14]. The results demonstrated that the GTV was better associated with the nadir of lymphocytes than with other WBCs, such as neutrophils and monocytes, during RT. In association with TLC reduction, pretreatment NLR, GTV, and heart V20 were significant predictive factors in the current study. To avoid multicollinearity, heart V2, V20, V50, and V60 were selected. Multivariate linear regression analysis showed that heart V20 was more significantly associated with TLC reduction than V60. A large volume of the critical lower dose could lead to more lymphocyte destruction (i.e., a greater “low-dose bath”) [14]. Contreras et al. demonstrated a relationship between lymphopenia and increased heart dose [8]. Most patients (n = 310, 77%) underwent CCRT, and male sex, RT alone, percentage of the heart receiving ≥ 50 Gy, and a higher NLR at 4 months were found to be associated with reduced OS in multivariate analysis. In subgroup analyses of patients with stage III disease treated with CCRT, heart V50 > 25% was associated with an elevated NLR at 4 months after RT on multivariable logistic regression analysis.
When lung cancer is treated with RT, the lungs, heart, great vessel, and bone marrow are affected. We confirmed that RAL during CCRT was immediately apparent within 2–3 weeks of treatment. Nadir ALC during CCRT was significantly associated with OS, LRFS, and DRFS in the current study, although the significance disappeared in the multivariate analysis. In contrast, the NLR during CCRT was significantly associated with survival outcomes only on univariate analysis, whereas the pretreatment NLR was significantly associated with PFS and DRFS on multivariate analysis. Hence, we hypothesized that the patient’s immune status before treatment might be more important than that during or after treatment in predicting treatment outcomes.
High PDL1 expression predicts response to pembrolizumab in the primary treatment of advanced NSCLC [26,27]. In a meta-analysis, PDL1 expression was associated with sex, smoking status, histology, differentiation, tumor size, lymph node metastasis, TNM stage, and EGFR mutation [28]. However, our data did not show a significant relationship between PDL1 expression and the aforementioned clinical parameters, except that patients with more advanced stage IIIB tumors tended to express PDL1. PDL1 does not appear to be a prognostic factor in patients with locally advanced NSCLC who have undergone CCRT alone [29]. Moreover, our data did not reveal a relationship between PDL1 expression and survival outcomes; however, changes in PDL1 expression after CCRT have been shown to be associated with the prognosis of patients with locally advanced NSCLC [30]. Indeed, the OS of patients with locally advanced NSCLC and increased PDL1 expression after CCRT was poorer than that of patients with decreased or unchanged PDL1 expression. Gong et al. showed that PDL1 expression increased after conventional fractionated radiation [31]. Patients with negative PDL1 expression showed significantly higher objective response and disease control rates than those with positive PDL1 expression. This study demonstrated the possibility that radiotherapy plus anti-PDL1 antibody synergistically enhances antitumor immunity.
TILs are significantly associated with treatment outcomes in NSCLC and survival after therapy [32]. Tokito et al. demonstrated that the density of CD8+ TILs was an independent and significant predictive factor for PFS and OS in patients with locally advanced NSCLC who underwent CCRT [29]. In the current study, CD8+ TILs were significantly associated with PFS and marginally associated with OS. CD8+ T cells are also significant predictors of OS and disease-free survival in early stage NSCLC [33]. However, in the present study, no relationship was observed between CD8+ TILs and peripheral circulating lymphocytes, and no correlation was noted between CD8+ expression and pretreatment lymphocyte count.
Previous studies have suggested that RAL may reduce the effectiveness of immunotherapy [15,34]. Pike et al. demonstrated the effect of radiation on lymphocyte counts and the survival of patients with metastatic cancer receiving a PD1 ICI [15]. Severe lymphopenia at the time of ICI treatment initiation was associated with decreased survival. In a retrospective study of lymphopenia in patients receiving immunotherapy for NSCLC, radiation was a significant risk factor for peri-immunotherapy lymphopenia in multivariate logistic regression analysis [34]. Peri-immunotherapy lymphopenia was a significant prognostic factor of both PFS and OS. Hence, greater efforts are needed to determine the optimal radiation technique that preserves ALC during radiotherapy in the era of standard immunotherapies, such as durvalumab, following CCRT in patients with unresectable NSCLC. Unfortunately, our data did not confirm a survival difference when the radiation techniques were considered. Patients treated with partial or full IMRT showed a trend towards better survival outcomes than those treated with 3D-CRT alone, albeit without statistical significance.
As we did not design a secondary analysis, we must consider some possible limitations of this study. First, although serial hematological parameters could be obtained faithfully, data on PDL1 and CD8+ TILs were obtained only from patients with available tissue specimens, and the post-radiation changes in these parameters could not be evaluated. Second, we did not scrutinize the effects of immunotherapy as a salvage therapy after tumor recurrence, which might affect overall survival. However, this is unlikely to have had a significant impact on the results because most patients in this study were enrolled before the era of immunotherapy.
In conclusion, TLC reduction during CCRT and pretreatment NLR are significant prognostic factors for PFS. In subgroup analysis, CD8+ TILs were significantly associated with PFS and marginally significantly associated with OS. Both LRFS and DRFS were significantly dependent on TLC reduction during CCRT, whereas DRFS was associated with pretreatment NLR. TLC reduction during CCRT is closely associated with GTV, pretreatment NLR, and heart V20. Thus, efforts are needed to reduce TLC by constraining the volume of the radiation dose to the entire heart. Further studies should focus on developing precise RT techniques to overcome RAL.
Author Contributions
Conceptualization, S.-J.A. and Y.-H.K.; methodology, S.-J.A. and Y.-H.K.; software, Y.-H.K.; validation, Y.-H.K., Y.-D.C., S.-J.A., Y.-C.K., I.-J.O., C.-K.P., T.-K.N., M.S.Y., J.-U.J., I.J.C., J.-Y.S., and S.C.; formal analysis, Y.-H.K., Y.-D.C. and S.-J.A.; investigation, Y.-H.K., Y.-D.C. and S.-J.A.; resources, S.-J.A., Y.-C.K., I.-J.O., C.-K.P., T.-K.N., M.S.Y. and J.-U.J.; data curation, Y.-H.K., Y.-D.C., S.-J.A., Y.-C.K., I.-J.O., C.-K.P., T.-K.N., M.S.Y. and J.-U.J.; writing—original draft preparation, Y.-H.K., Y.-D.C., S.-J.A., Y.-C.K., I.-J.O., C.-K.P., T.-K.N., M.S.Y., J.-U.J., I.J.C., J.-Y.S., and S.C.; writing—review and editing, Y.-H.K., Y.-D.C., S.-J.A., Y.-C.K., I.-J.O., C.-K.P., T.-K.N., M.S.Y., J.-U.J., I.J.C., J.-Y.S., and S.C.; visualization, Y.-H.K. and Y.-D.C.; supervision, Y.-H.K., Y.-D.C., S.-J.A., Y.-C.K., I.-J.O., C.-K.P., T.-K.N., M.S.Y. and J.-U.J.; project administration, S.-J.A. and Y.-H.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the institutional review board of the Chonnam National University Hwasun Hospital (CNUHH-2010-010).
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to institutional data-sharing restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- O'Callaghan, D.S.; O'Donnell, D.; O'Connell, F.; O'Byrne, K.J. The role of inflammation in the pathogenesis of non-small cell lung cancer. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2010, 5, 2024–2036. [Google Scholar] [CrossRef]
- Blank, C.U.; Haanen, J.B.; Ribas, A.; Schumacher, T.N. CANCER IMMUNOLOGY. The "cancer immunogram". Sci. (N. Y.) 2016, 352, 658–660. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Grossman, S.A.; Ellsworth, S.; Campian, J.; Wild, A.T.; Herman, J.M.; Laheru, D.; Brock, M.; Balmanoukian, A.; Ye, X. Survival in Patients With Severe Lymphopenia Following Treatment With Radiation and Chemotherapy for Newly Diagnosed Solid Tumors. J. Natl. Compr. Cancer Netw. JNCCN 2015, 13, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Campian, J.L.; Ye, X.; Brock, M.; Grossman, S.A. Treatment-related lymphopenia in patients with stage III non-small-cell lung cancer. Cancer Investig. 2013, 31, 183–188. [Google Scholar] [CrossRef]
- Choi, N.; Kim, J.H.; Chie, E.K.; Gim, J.; Kang, H.C. A meta-analysis of the impact of neutrophil-to-lymphocyte ratio on treatment outcomes after radiotherapy for solid tumors. Medicine 2019, 98, e15369. [Google Scholar] [CrossRef] [PubMed]
- Contreras, J.A.; Lin, A.J.; Weiner, A.; Speirs, C.; Samson, P.; Mullen, D.; Campian, J.; Bradley, J.; Roach, M.; Robinson, C. Cardiac dose is associated with immunosuppression and poor survival in locally advanced non-small cell lung cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2018, 128, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Ellsworth, S.G. Field size effects on the risk and severity of treatment-induced lymphopenia in patients undergoing radiation therapy for solid tumors. Adv. Radiat. Oncol. 2018, 3, 512–519. [Google Scholar] [CrossRef]
- Joseph, N.; McWilliam, A.; Kennedy, J.; Haslett, K.; Mahil, J.; Gavarraju, A.; Mistry, H.; Van Herk, M.; Faivre-Finn, C.; Choudhury, A. Post-treatment lymphocytopaenia, integral body dose and overall survival in lung cancer patients treated with radical radiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2019, 135, 115–119. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [PubMed]
- Yovino, S.; Kleinberg, L.; Grossman, S.A.; Narayanan, M.; Ford, E. The etiology of treatment-related lymphopenia in patients with malignant gliomas: Modeling radiation dose to circulating lymphocytes explains clinical observations and suggests methods of modifying the impact of radiation on immune cells. Cancer Investig. 2013, 31, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Chen, G.; Ye, L.; Shi, S.; Du, S.; Zeng, Z.; He, J. Treatment-duration is related to changes in peripheral lymphocyte counts during definitive radiotherapy for unresectable stage III NSCLC. Radiat. Oncol. (Lond. Engl.) 2019, 14, 86. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Liao, Z.; Gomez, D.; Levy, L.; Zhuang, Y.; Gebremichael, R.A.; Hong, D.S.; Komaki, R.; Welsh, J.W. Lymphopenia association with gross tumor volume and lung V5 and its effects on non-small cell lung cancer patient outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 1084–1091. [Google Scholar] [CrossRef]
- Pike, L.R.G.; Bang, A.; Mahal, B.A.; Taylor, A.; Krishnan, M.; Spektor, A.; Cagney, D.N.; Aizer, A.A.; Alexander, B.M.; Rahma, O.; et al. The Impact of Radiation Therapy on Lymphocyte Count and Survival in Metastatic Cancer Patients Receiving PD-1 Immune Checkpoint Inhibitors. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 142–151. [Google Scholar] [CrossRef]
- Kim, Y.H.; Ahn, S.J.; Moon, S.H.; Kim, J.H.; Kim, Y.C.; Oh, I.J.; Park, C.K.; Jeong, J.U.; Yoon, M.S.; Song, J.Y.; et al. Randomized, Multicenter, Phase 3 Study of Accelerated Fraction Radiation Therapy With Concomitant Boost to the Gross Tumor Volume Compared With Conventional Fractionation in Concurrent Chemoradiation in Patients With Unresectable Stage III Non-Small Cell Lung Cancer: The Korean Radiation Oncology Group 09-03 Trial. Int. J. Radiat. Oncol. Biol. Phys. 2023, 115, 873–885. [Google Scholar] [CrossRef]
- Wheatley, M.; Gore, E.; Ad, V.B.; Robinson, C.; Bradley, J.J. Defining a novel cardiac contouring atlas for NSCLC using cadaveric anatomy. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, S658. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. New Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef]
- Aupérin, A.; Le Péchoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef]
- Yoon, S.M.; Shaikh, T.; Hallman, M. Therapeutic management options for stage III non-small cell lung cancer. World J. Clin. Oncol. 2017, 8, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet. Oncol. 2015, 16, 187–199. [Google Scholar] [CrossRef]
- Jin, J.; Hu, C.; Xiao, Y.; Zhang, H.; Ellsworth, S.; Schild, S.; Bogart, J.; Dobelbower, M.; Kavadi, V.; Narayan, S.J. Higher radiation dose to immune system is correlated with poorer survival in patients with stage III non–small cell lung cancer: A secondary study of a phase 3 cooperative group trial (NRG Oncology RTOG 0617). Biol. Phys. 2017, 99, S151–S152. [Google Scholar] [CrossRef]
- Wang, S.J.; Haffty, B. Radiotherapy as a New Player in Immuno-Oncology. Cancers 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Sellins, K.S.; Cohen, J.J. Gene induction by gamma-irradiation leads to DNA fragmentation in lymphocytes. J. Immunol. 1987, 139, 3199–3206. [Google Scholar] [CrossRef] [PubMed]
- Coffelt, S.B.; Wellenstein, M.D.; de Visser, K.E. Neutrophils in cancer: Neutral no more. Nat. Rev. Cancer 2016, 16, 431–446. [Google Scholar] [CrossRef]
- Gridelli, C.; Ardizzoni, A.; Barberis, M.; Cappuzzo, F.; Casaluce, F.; Danesi, R.; Troncone, G.; De Marinis, F. Predictive biomarkers of immunotherapy for non-small cell lung cancer: Results from an Experts Panel Meeting of the Italian Association of Thoracic Oncology. Transl. Lung Cancer Res. 2017, 6, 373–386. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. New Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Li, G.; Wang, Y.; Wang, Y.; Zhao, S.; Haihong, P.; Zhao, H.; Wang, Y. PD-L1 expression in lung cancer and its correlation with driver mutations: A meta-analysis. Sci. Rep. 2017, 7, 10255. [Google Scholar] [CrossRef]
- Tokito, T.; Azuma, K.; Kawahara, A.; Ishii, H.; Yamada, K.; Matsuo, N.; Kinoshita, T.; Mizukami, N.; Ono, H.; Kage, M.; et al. Predictive relevance of PD-L1 expression combined with CD8+ TIL density in stage III non-small cell lung cancer patients receiving concurrent chemoradiotherapy. Eur. J. Cancer 2016, 55, 7–14. [Google Scholar] [CrossRef]
- Fujimoto, D.; Uehara, K.; Sato, Y.; Sakanoue, I.; Ito, M.; Teraoka, S.; Nagata, K.; Nakagawa, A.; Kosaka, Y.; Otsuka, K.; et al. Alteration of PD-L1 expression and its prognostic impact after concurrent chemoradiation therapy in non-small cell lung cancer patients. Sci. Rep. 2017, 7, 11373. [Google Scholar] [CrossRef]
- Gong, X.; Li, X.; Jiang, T.; Xie, H.; Zhu, Z.; Zhou, F.; Zhou, C. Combined Radiotherapy and Anti-PD-L1 Antibody Synergistically Enhances Antitumor Effect in Non-Small Cell Lung Cancer. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2017, 12, 1085–1097. [Google Scholar] [CrossRef] [PubMed]
- Zeng, D.Q.; Yu, Y.F.; Ou, Q.Y.; Li, X.Y.; Zhong, R.Z.; Xie, C.M.; Hu, Q.G. Prognostic and predictive value of tumor-infiltrating lymphocytes for clinical therapeutic research in patients with non-small cell lung cancer. Oncotarget 2016, 7, 13765–13781. [Google Scholar] [CrossRef]
- Teng, F.; Meng, X.; Wang, X.; Yuan, J.; Liu, S.; Mu, D.; Zhu, H.; Kong, L.; Yu, J. Expressions of CD8+TILs, PD-L1 and Foxp3+TILs in stage I NSCLC guiding adjuvant chemotherapy decisions. Oncotarget 2016, 7, 64318–64329. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Park, S.; Byun, H.K.; Lee, C.G.; Cho, J.; Hong, M.H.; Kim, H.R.; Cho, B.C.; Kim, S.; Park, J.; et al. Impact of Treatment-Related Lymphopenia on Immunotherapy for Advanced Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Overall treatment scheme for the Korean Radiation Oncology Group. Abbreviations: RT: Radiation therapy, CT: Chemotherapy, PTV: Planning target volume, Gy: Gray, TP: Paclitaxel and cisplatin, R: Radiation therapy.
Figure 1.
Overall treatment scheme for the Korean Radiation Oncology Group. Abbreviations: RT: Radiation therapy, CT: Chemotherapy, PTV: Planning target volume, Gy: Gray, TP: Paclitaxel and cisplatin, R: Radiation therapy.
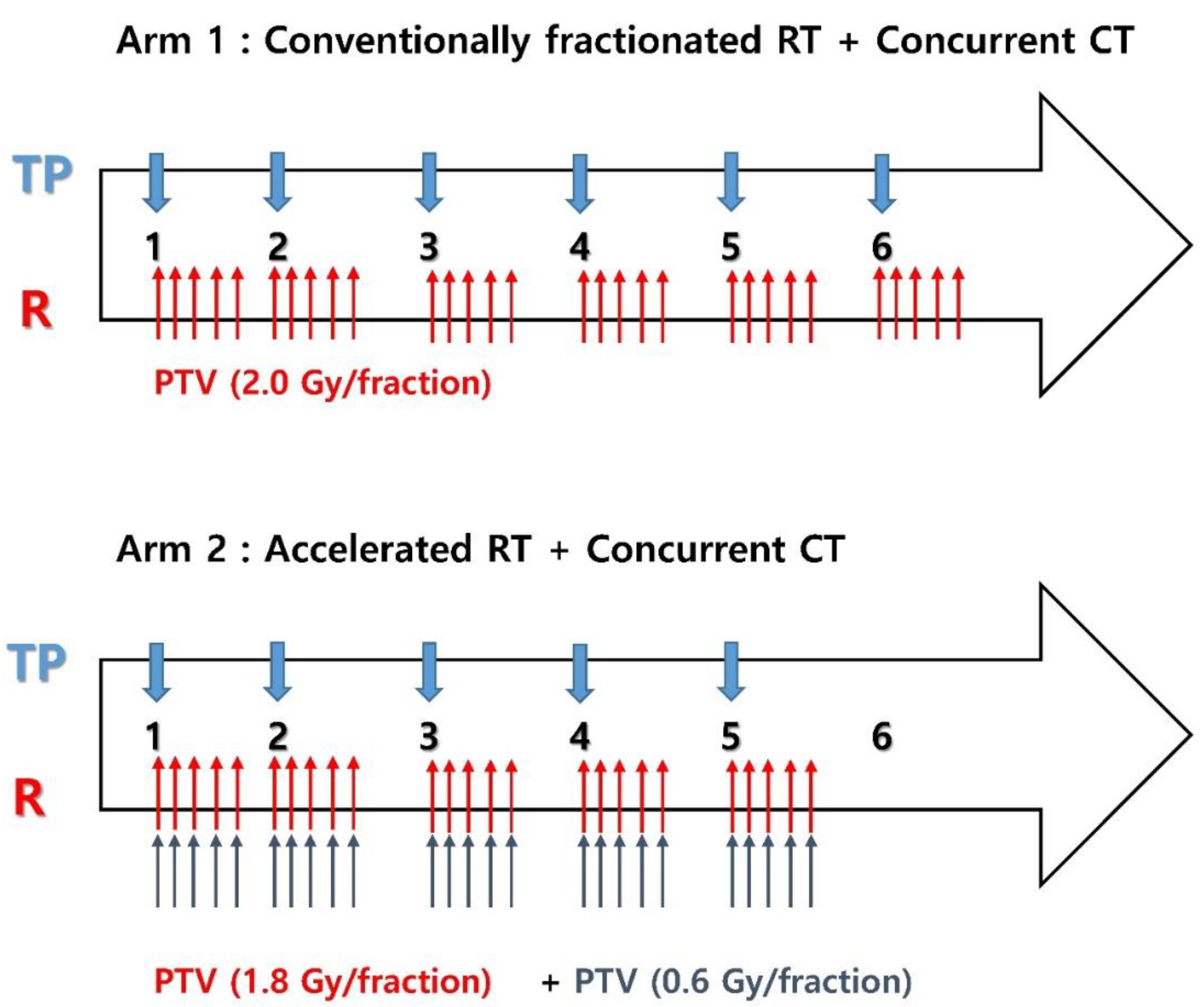
Figure 2.
Immunohistochemical (IHC) staining for programmed cell death-ligand 1 (PDL1), (A) positive and (B) negative staining. Immunohistochemical (IHC) staining for CD8+ tumor infiltrating lymphocyte (TIL), (C) high group (≥ 30%) and (D) low group (< 30%).
Figure 2.
Immunohistochemical (IHC) staining for programmed cell death-ligand 1 (PDL1), (A) positive and (B) negative staining. Immunohistochemical (IHC) staining for CD8+ tumor infiltrating lymphocyte (TIL), (C) high group (≥ 30%) and (D) low group (< 30%).
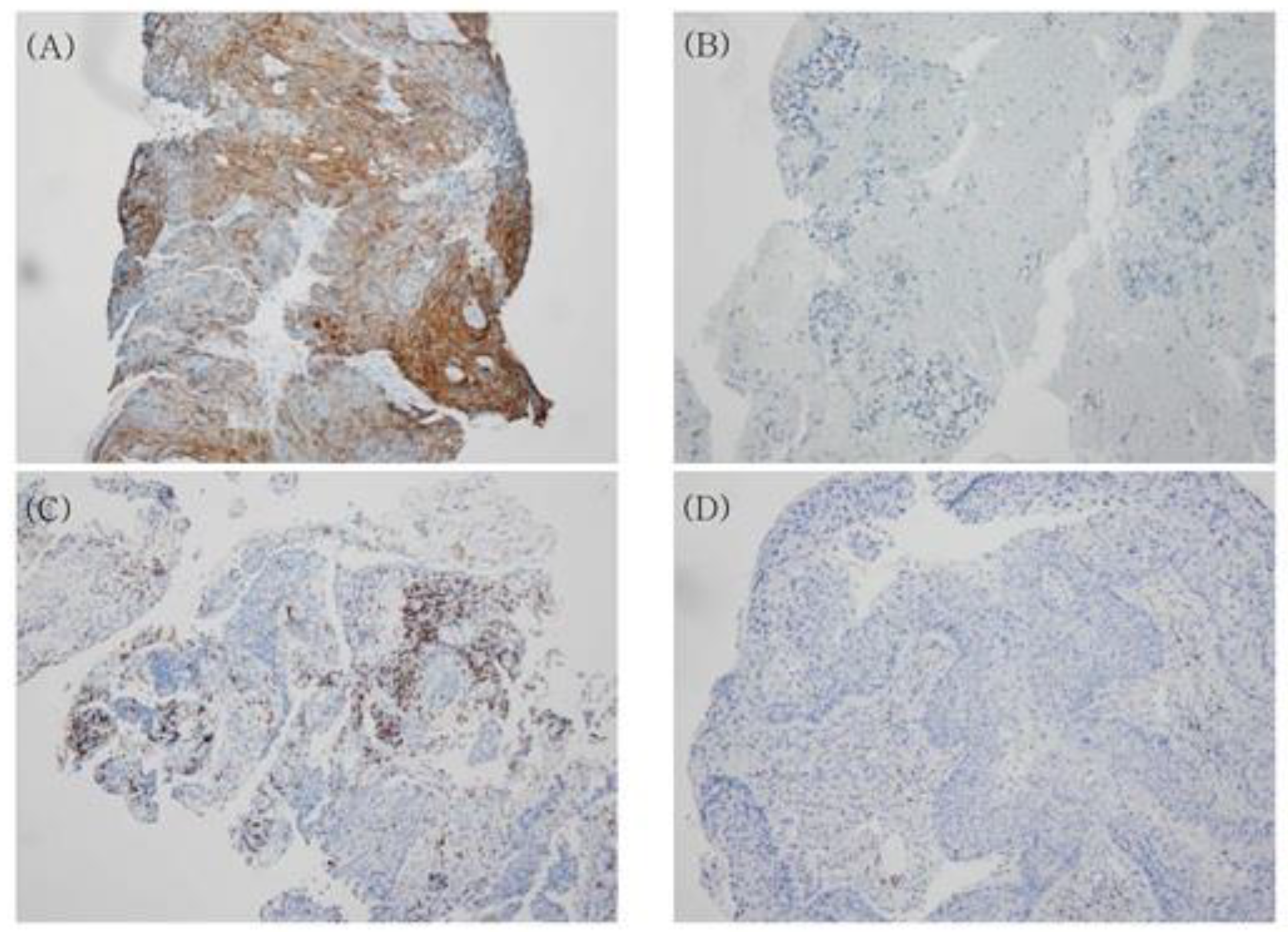
Figure 3.
Overall survival according to (A) total lymphocyte counts (TLC) reduction (≤ 0.78 vs. > 0.78) and (B) pretreatment neutrophil to lymphocyte ratio (NLR) (≤ 2.63 vs. > 2.63). Progression-free survival according to (C) TLC reduction (≤ 0.78 vs. > 0.78) and (D) pretreatment NLR (≤ 2.63 vs. > 2.63).
Figure 3.
Overall survival according to (A) total lymphocyte counts (TLC) reduction (≤ 0.78 vs. > 0.78) and (B) pretreatment neutrophil to lymphocyte ratio (NLR) (≤ 2.63 vs. > 2.63). Progression-free survival according to (C) TLC reduction (≤ 0.78 vs. > 0.78) and (D) pretreatment NLR (≤ 2.63 vs. > 2.63).
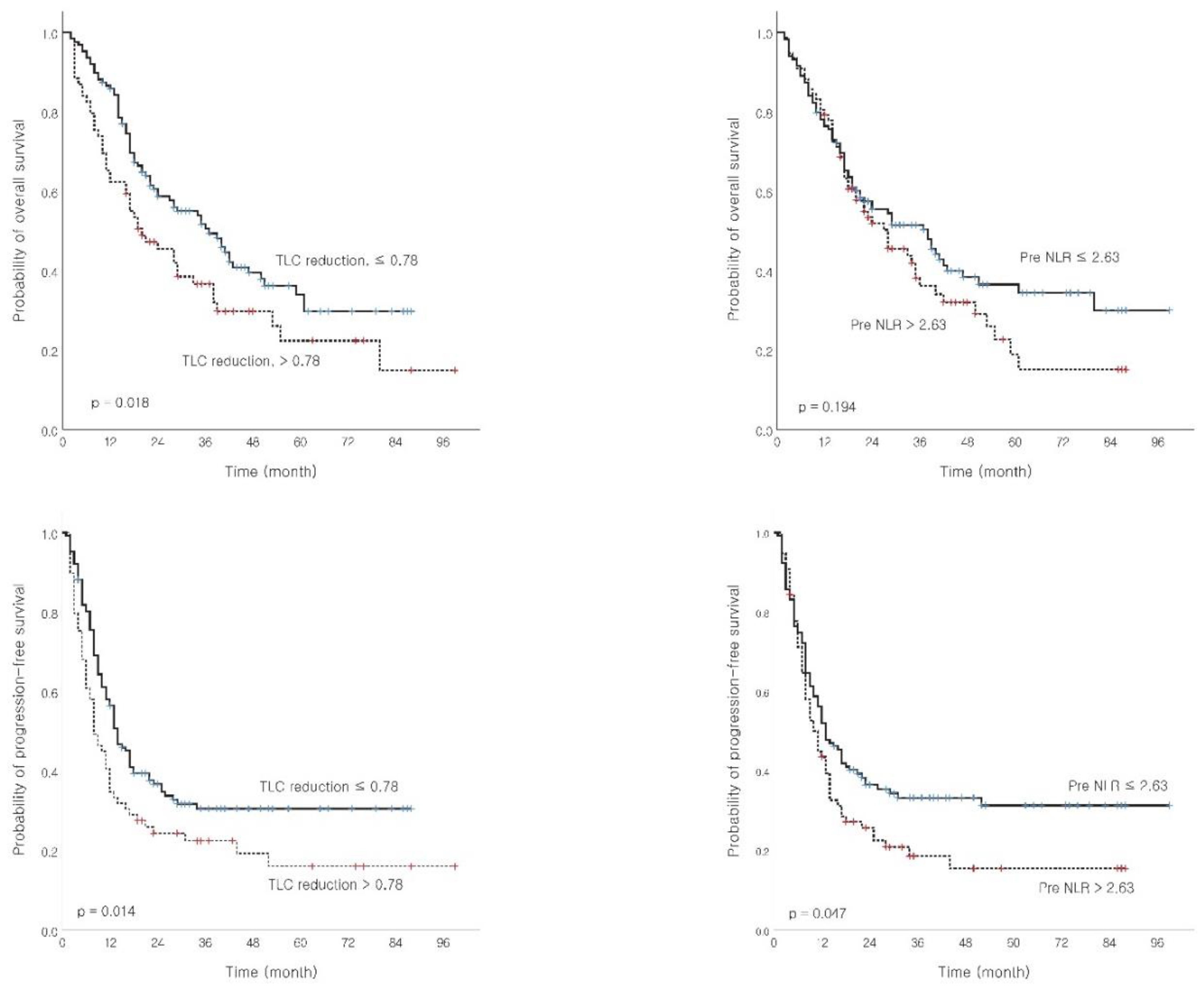
Figure 5.
Overall survival according to (A) programmed death ligand 1 (PDL1) (no vs. yes) and (B) CD8+ tumor infiltrating lymphocyte (TIL) low group (< 30%) or high group (≥ 30%). Progression-free survival.
Figure 5.
Overall survival according to (A) programmed death ligand 1 (PDL1) (no vs. yes) and (B) CD8+ tumor infiltrating lymphocyte (TIL) low group (< 30%) or high group (≥ 30%). Progression-free survival.
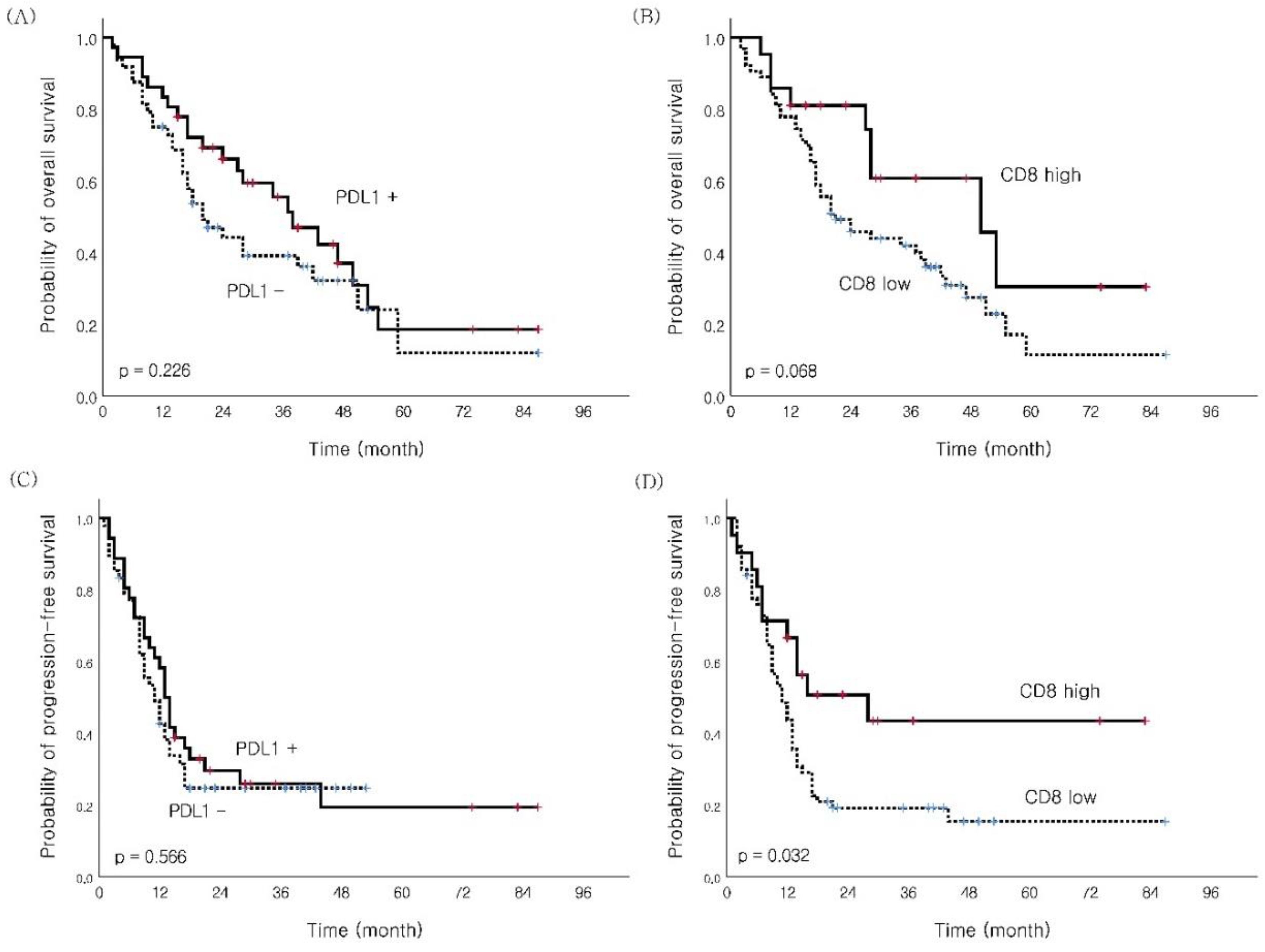

Table 1.
Patient characteristics (n = 196).
| Characteristic | All Patients (Median) |
|---|---|
| Age, years | 40–75 (66) |
| Sex | |
| Male | 183 (93.4%) |
| Female | 13 (6.6%) |
| ECOG PS | |
| 0 | 25 (12.8%) |
| 1 | 171 (87.2%) |
| Weight loss (%) | 0–19 (0) |
| Smoking history | |
| Never | 16 (8.2%) |
| Ex-smoker | 53 (27.0%) |
| Current smoker (< 1 year quit) | 127 (64.8%) |
| Histology | |
| SqCC | 146 (74.5%) |
| Non-SqCC | 50 (25.5%) |
| Clinical stage | |
| IIIA | 141 (71.9%) |
| IIIB | 55 (28.1%) |
| GTV (cm3) | 20.2–869.0 (154.65) |
| Hematologic parameters (cells/μL) | |
| Pre-treatment WBC | 3400–32800 (8700) |
| Pre-treatment ALC | 860–4640 (2130) |
| Pre-treatment ANC | 1039–9760 (4985) |
| Pre-treatment monocyte | 150–1870 (680) |
| Pre-treatment NLR | 0.22–8.95 (2.33) |
| DLCO (%) | 27–193 (89) |
| RT duration (day) | 27–56 (41) |
| Chemotherapy cycle | 4–6 (6) |
Abbreviations: ECOG PS: Eastern Cooperative Oncology Group Performance Status, SqCC: Squamous cell carcinoma, WBC: White blood cell, ALC: Absolute lymphocyte count, ANC: Absolute neutrophil count, NLR: Neutrophil-to-lymphocyte ratio, FEV1: Forced expiratory volume in one second, DLCO: Diffusing capacity for carbon monoxide.
Table 2.
Univariate analysis with treatment outcome.
| Variable | No. (%) | OS | PFS | LRFS | DRFS | ||||
|---|---|---|---|---|---|---|---|---|---|
| MS (months) | p-value | MS (months) | p-value | MS (months) | p-value | MS (months) | p-value | ||
|
Age (years) ≤65 > 65 |
91 (46.4) 105 (53.6) |
39 22 |
0.014 |
13 11 |
0.041 | 21 14 |
0.028 | 22 15 |
0.024 |
|
Clinical stage IIIA IIIB |
141 (71.9) 55 (28.1) |
33 27 |
0.592 |
13 10 |
0.473 | 15 14 |
0.625 | 17 17 |
0.527 |
|
Sex Male Female |
183 (93.4) 13 (6.6) |
29 36 |
0.532 |
12 11 |
0.233 | 15 14 |
0.950 | 17 16 |
0.489 |
|
ECOG PS 0 1 |
25 (12.8) 171 (87.2) |
43 28 |
0.124 |
13 12 |
0.336 | 14 15 |
0.364 | 14 17 |
0.341 |
|
Weight loss ≤ 5% > 5% |
140 (71.4) 56 (28.6) |
34 20 |
0.509 |
13 8 |
0.382 | 17 12 |
0.446 | 17 11 |
0.500 |
|
Current smoking No Yes (quit < 1 years) |
69 (35.2) 127 (64.8) |
29 29 |
0.813 | 12 13 |
0.595 |
18 14 |
0.997 | 18 16 |
0.740 |
|
Pre NLR ≤2.63 > 2.63 |
119 (60.7) 77 (39.3) |
38 28 |
0.194 |
13 11 |
0.047 | 16 14 |
0.346 | 18 12 |
0.013 |
|
TLC reduction ≤0.78 > 0.78 |
127 (64.8) 69 (35.2) |
37 20 |
0.018 | 14 8 |
0.014 | 18 11 |
0.008 | 19 11 |
0.018 |
|
Nadir ALC (cell/µL) ≥ 500 < 500 |
113 (57.7) 83 (42.3) |
36 24 |
0.031 |
13 10 |
0.075 | 18 12 |
0.029 | 19 12 |
0.045 |
|
NLR during CCRT ≤ 9.25 > 9.25 |
163 (83.2) 33 (16.8) |
35 17 |
0.039 |
13 8 |
0.020 | 17 8 |
0.012 | 17 9 |
0.033 |
|
GTV (cc) ≤ 165 > 165 |
104 (53.1) 92 (46.9) |
38 19 |
0.032 |
14 10 |
0.022 | 22 11 |
0.010 | 22 12 |
0.088 |
|
RT duration (days) ≤42 > 43 |
128 (65.3) 68 (34.7) |
35 21 |
0.300 |
13 11 |
0.388 |
14 14 |
0.374 |
18 14 |
0.245 |
|
RT technique 3D CRT only IMRT* |
87 (44.4) 109 (55.6) |
28 36 |
0.867 | 11 13 |
0.567 | 14 16 |
0.728 | 16 18 |
0.804 |
Abbreviations: 3D CRT: Three-dimensional conformal radiotherapy, ECOG PS: Eastern Cooperative Oncology Group Performance Status, NLR: Neutrophil-to-lymphocyte ratio, TLC: Ratio of baseline total lymphocyte count (TLC) minus nadir TLC during concurrent chemoradiation to baseline TLC, Nadir ALC: Lowest lymphocyte count, GTV: Gross tumor volume, OS: Overall survival, PFS: Progression-free survival, LRFS: Local recurrence-free survival, DRFS: Distant recurrence-free survival.*Thirty-two patients underwent hybrid 3D CRT & IMRT.
Table 3.
Multivariate analysis by prognostic factor.
| Variable | Prognostic Factor | HR (95% CI) | p-value |
|---|---|---|---|
| OS | Age (years), ≤ 65 vs. > 65 | 1.579 (1.097–2.274) | 0.014 |
| GTV (cc), ≤ 165 vs. > 165 | 1.482 (1.036–2.119) | 0.031 | |
| PFS | TLC reduction, ≤ 0.78 vs. > 0.78 | 1.510 (1.075–2.121) | 0.018 |
| Pre-treatment NLR ≤ 2.63 vs. > 2.63 | 1.561 (1.110–2.197) | 0.010 | |
| LRFS | TLC reduction, ≤ 0.78 vs. > 0.78 | 1.505 (1.060–2.136) | 0.022 |
| GTV (cc), ≤ 165 vs. > 165 | 1.467 (1.041–2.068) | 0.029 | |
| DRFS | Pre-treatment NLR ≤ 2.63 vs. > 2.63 | 1.578 (1.135–2.244) | 0.007 |
| TLC reduction, ≤ 0.78 vs. > 0.78 | 1.578 (1.118–2.228) | 0.010 |
Abbreviations: OS: Overall survival, PFS: Progression-free survival, LRFS: Local recurrence-free survival, DRFS: Distant recurrence-free survival, GTV: Gross tumor volume, TLC reduction: Ratio of baseline total lymphocyte count (TLC) minus nadir TLC during concurrent chemoradiation to baseline TLC, NLR: Neutrophil-to-lymphocyte ratio, HR: Hazard ratio.
Table 4.
Hematologic and non-hematologic toxicity during treatment.
| Adverse Event (n,%) | G0-1 | G2 | G3 | G4 | G5 |
|---|---|---|---|---|---|
| Hematologic toxicity | |||||
| Leukopenia | 152 (77.6) | 27 (13.8) | 15 (7.7) | 2 (1.0) | 0 (0.0) |
| Neutropenia | 147 (75.0) | 34 (17.3) | 11 (5.6) | 4 (2.0) | 0 (0.0) |
| Thrombocytopenia | 194 (99.0) | 2 (1.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Lymphopenia | 43 (21.9) | 70 (35.7) | 79 (40.3) | 4 (2.0) | 0 (0.0) |
| Non-hematologic toxicity | |||||
| Radiation pneumonitis | 171 (87.2) | 15 (7.7) | 4 (2.0) | 0 (0.0) | 6 (3.1) |
| Radiation esophagitis | 142 (72.5) | 47 (24.0) | 4 (2.0) | 2 (1.0) | 1 (0.5) |
Table 5.
Logistic regression analysis associating with TLC reduction.
| Variable | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| OR | p-Value | OR | p-Value | 95% CI | |
| Age (years) | 1.016 | 0.445 | |||
| Treatment duration (day) | 0.999 | 0.984 | |||
| Pre-NLR | 0.764 | 0.043 | 0.714 | 0.018 | 0.540–0.945 |
| GTV (cm3) | 1.003 | 0.003 | 1.003 | 0.010 | 1.001–1.005 |
| Lung V2 (%) | 1.026 | 0.002 | |||
| Lung V20 (%) | 1.077 | 0.006 | |||
| Lung V50 (%) | 0.999 | 0.968 | |||
| Lung V60 (%) | 0.923 | 0.184 | |||
| Heart V2 (%) | 1.018 | 0.001 | |||
| Heart V20 (%) | 1.026 | 0.001 | 1.025 | 0.002 | 1.009–1.040 |
| Heart V50 (%) | 1.023 | 0.093 | |||
| Heart V60 (%) | 1.027 | 0.374 | |||
| Smoking (others vs. never) | 1.029 | 0.927 | |||
| RT technique (3D vs. IMRT) | 1.393 | 0.276 | |||
Abbreviations: GTV: Gross tumor volume, WBC: White blood cell, ALC: Absolute lymphocyte count, ANC: Absolute neutrophil count.
Table 6.
Relationship between PD-L1 expression, CD8 and patient characteristics.
| Characteristic | n (%) | PDL1 Expression | p-Value | CD8 Expressiom | p-Value | ||
|---|---|---|---|---|---|---|---|
| No | Yes | Low | High | ||||
| Age (years) ≤ 65 > 65 |
46 (54.8) 38 (45.2) |
26 22 |
20 16 |
0.899 |
34 29 |
12 9 |
0.800 |
| Clinical stage IIIA IIIB |
60 (71.4) 24 (28.6) |
38 10 |
22 14 |
0.070 |
46 17 |
14 7 |
0.577 |
| Sex Male Female |
77 (91.7) 7 (8.3) |
44 4 |
33 3 |
1.000 |
58 5 |
19 2 |
0.820 |
| Smoking No Yes (quit < 1 year) |
28 (33.3) 56 (66.7) |
13 35 |
15 21 |
0.161 |
18 45 |
10 11 |
0.109 |
| Pathology SqCC Non-SqCC |
64 (76.2) 20 (23.8) |
37 11 |
27 9 |
0.824 |
48 15 |
16 5 |
1.000 |
| Pre NLR ≤2.63 >2.63 |
54 (64.3) 30 (35.7) |
32 16 |
22 14 |
0.599 |
40 19 |
10 11 |
0.066 |
| GTV (cc) ≤ 165 > 165 |
49 (58.3) 35 (41.7) |
27 21 |
22 14 |
0.655 |
38 25 |
11 10 |
0.523 |
| CD8 Low High |
63 (75.0) 21 (25.0) |
38 10 |
25 11 |
0.309 |
|||
Abbreviations: SqCC: Squamous cell carcinoma, NLR: Neutrophil-to-lymphocyte ratio, GTV: Gross tumor volume, PDL1: Programmed cell death ligand 1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



