
Submitted:
12 October 2023
Posted:
13 October 2023
You are already at the latest version
Abstract
A multicenter, prospective cohort study conducted in 5 physiotherapy clinics in the UAE from January 2021 to March 2023 to assess coronal lumbar spine radiographic parameters as a predictor of conservative therapy outcomes in patients suffering from low back and leg pain due to lumbar disc herniation (HNP). Ninety patients (mean age 44 yrs., 54% male) with lumbar HNP underwent conservative therapy. All participants received lumbar spine MRI and radiography to assess spine alignment. Interventions included specific exercises, diathermy, traction, education, a home-based exercise pro-gram, and medications. Detailed demographic data was collected. Follow-up was 6-months after discharge. A successful outcome was based on a minimum of the following four outcomes: (1) reduction of pain by 17.5 points (0–100 NRS); (2) fatigue reduction by 7.5 points; (3) distress reduction by 5 points; and (4) interference reduction by 9.5 points. At 6-month follow-up it was found that patient age, education, and radio-graphic determined lumbosacral angle measures significantly affected the odds of a successful outcome. Increasing age 1-year significantly decreased the odds of success of improving pain, fatigue (OR = 0.85, p = 0.016) and interference scores (OR = 0.89, p = 0.042) by 15%, 15%, and 11% respectively. Lower education significantly increased the odds of success for improving pain, fatigue, and interference by 26.18, 26.18, and 7.5 (p = 0.006, = 0.006, and = 0.029 respectively). Increasing (worsening) the radiographic lumbosacral angle by each 1° significantly reduced the odds of success for improving pain, fatigue, distress, and interference by 3.52, 3.52, 27.99, and 2.55, respectively (p < 0.001, < 0.001, = 0.003, = 0.001). Our findings indicate that younger age, less education, and better coronal radiological lumbar spine alignment all had a substantial impact on the likelihood of success of 6-month outcomes in patients suffering from chronic lower back pain and radiculopathy due to HNP.
Keywords:
low back pain
; leg pain
; disc herniation
; clinical trial
; radiography
1. Introduction
Lumbosacral radiculopathy associated with disk herniation (HNP) is a common clinical problem strongly associated with delayed recovery, persistent disability and increased healthcare utilization and costs [1]. Despite the high prevalence of this condition, its conservative treatment remains challenging for spine specialists [2,3]. Recent systematic reviews reported a lack of clearly effective conservative treatments for lumbar radicular pain, particularly for long-term management [4,5]. Most important, the literature provides scant information about the relevant biopsychosocial patient variables that may be the explanatory reasons for those patients who will have suboptimal outcomes at long-term assessment after rehabilitation programs [6]. The prognosis for conservative treatment needs to be determined in a timely and efficient manner to allow health professionals to decide whether the lumbar HNP patient requires surgery or continues non-surgical management [7].
Accordingly, investigations identifying patient specific outcomes that predict the odds of successful conservative treatment for lumbar HNP are crucial. Specific predictors can help target and improve treatment options to the patients as well as having the potential to enhance clinical care and improve prognosis for long-term care plans. Some predictors such as magnetic resonance imaging (MRI) classification, pain intensity, duration of complaints, response to the straight-leg raising test (SLRT), and grade of motor power have been reported previously [8,9]. Despite the fact that many studies have described the important role of abnormal spine / posture alignment, which is considered by some to be an important etiological factor for low back pain and many other pathological changes [10,11], there is little agreement as to what constitutes an 'acceptable' coronal lumbo-pelvic spinal alignment and / or which specific spine measurement variables should be used to define and predict patient outcomes in the majority of cases. It is important to note that the literature on spinal alignment has established that a better spine alignment including coronal and sagittal balance is essential for optimal biomechanical function [12,13,14,15] and many clinical trials [16,17,18,19] have demonstrated that corrections in patient posture and sagittal plane curvatures have resulted in relief of neurological symptoms.
However, reviewing the literature on this topic suggests that most rehabilitation programs do not typically consider spinal alignment variables, in particular the coronal alignment factors. Certainly, achieving spinal sagittal balance has emerged as one of the most important clinical outcomes and has been shown to have a significant effect on patient-related outcomes [16,17,18,19]. More recently, imbalance in the coronal plane has been shown to negatively affect patient satisfaction and is associated with increased pain, increased loss of function, and decreased quality of life [20,21,22,23]. Specifically, the fractional lumbo-sacral curve (FLSC), which is the coronal curvature from L4-S1 and is generally in the opposite direction relative to the primary Cobb angle curvature in the lumbar spine, has been detailed and found to be a predictor of poor patient outcomes in conservative and surgical interventions in adult patient populations suffering from scoliotic deformities [24,25,26,27]. However, we could not locate any investigations looking at the FLSC in chronic low back pain patients with radiculopathy due to disc herniations; it may be relevant to identify if the FLSC is a predictor of patient responsive to conservative based interventions for this unique population. Accordingly, our study sought to investigate the coronal lumbar spinal alignment as predictor of conservative treatment outcomes in patients with chronic low back pain and radiculopathy due to HNP using a multi-center conservative care prospective observational trial with a 6-month follow up. We hypothesize that the magnitude of FLSC and other AP lumbar radiographic coronal displacements would be a predictor of success or failure of conservative care outcomes in patients suffering from low back pain and radicular pain due to HNP.
2. Materials and Methods
2.1. Study design and population.
This is multicenter, prospective cohort study conducted across 5 physiotherapy clinics in the UAE and Egypt from January 2021 to March 2023 to assess the coronal lumbar radiographic spinal parameters as potential predictors of conservative therapy outcomes in HNP patients suffering from lower back pain and radiculopathy. The protocol of the study was approved by Ethical Review Boards of the UOS [REC-21-03-11-03-S]. Written informed consent was obtained from all participants. Patients with lumbar HNP who underwent conservative therapy as a first line of treatment were included in this prospective study. Conservative therapy included back rest, physical therapy (back exercise, diathermy therapy and traction, education with instructions for home-based exercise), and medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) analgesics, muscle relaxants, or oral narcotics.
Lumbar HNP was defined as disc herniation that occurred at any mid-lower lumbar levels (L2-S1) and was diagnosed using magnetic resonance imaging. All types of protrusions (central, paramedian or foraminal) and all protrusion magnitudes (bulge, protrusion, or extrusion) were included. Figure 1 shows the qualitative types of HNP included in our investigation. The Michigan State University (MSU) classification for lumbar disc herniation was used as it is a simple and reliable method to objectively measure herniated lumbar discs [28]. All lumbar HNP with unilateral or bilateral radicular pain and patients aged between 18 and 65 years old were considered eligible. Demographical data such as age, sex, educational level, marital status, body mass index (BMI), and smoking status were collected. Clinical follow up was scheduled for the sixth month after discharge from active conservative care treatment. Exclusion criteria were patients with cauda equina syndrome, pregnancy, who had received spine surgery around the lumbar region, and had significant lumbar deformity. Additionally, anatomical leg discrepancy greater than 12mm was excluded from our study population and was verified both by radiography clinical examination by an Orthopedic surgeon.
2.2. Outcome variables.
The primary outcome variable used in this study was the conservative treatment outcome after 6 months follow-up after completion of active interventions (defined as success or failure). In the current study, we defined the success criteria from the spine pain patient’s perspective across multiple, relevant domains using patient centered outcome questionnaires. The following four end points were considered because previous research has shown them to be clinically relevant [29]. The rehabilitation program will be considered success if the 4 domain outcomes were decreased at discharge time by the Optimal cutoff points according to Brown et al. [30], and this improvement was maintained or further improved at the 6-month follow up otherwise it was considered as a failure. The optimal cutoff points were: (1) reduction of pain of 17.5 points or more (0–100 numerical rating scale); (2) fatigue reduction of 7.5 points or more; (3) reduction for distress by 5 points or more; and (4) reduction of interference by 9.5 points or more. The criteria for the 6-month follow-up failure were: (1) increase of pain or reduction less than 17.5 points; (2) increase of fatigue or reduction less than 7.5 points; (3) increase of distress or reduction less than 5 points; and (4) increase in the inference with daily activities or reduction less 9.5 points.
- Radiological Explanatory variables
The AP lumbo-pelvic radiographs were analyzed with a modified Risser-Ferguson method, which includes a lateral translation distance of T12 compared with the S2 tubercle (Tx), an angle of coronal bending at mid-lumbar spine (LD), an angle of the sacral base tilt angle relative to horizontal (HB), and an angle of lateral bending of the lower lumbar vertebra compared with the sacral base (LS); note the LS angle here is similar in concept to the FLSC in lumbar scoliotic deformity analysis. This AP radiographic method used herein has been reported to have inter-class and intra-class correlation coefficients in the high ranges with low standard errors of measurement (SEM < 2° for angles and SEM < 2 mm for distances) [31]. Figure 2 demonstrates this method of AP lumbar radiographic assessment. And these measurements are described in further detail here:
- T12-S1 centroid horizontal displacement for trunk lateral translation is measured using a vertical line drawn up from mid-S1 or S2 tubercle. The amount of trunk shift (lateral translation) is measured as the displacement of the centroid (Risser-Ferguson method) of T12 vertebra from this vertical line in millimeters (Tx). Figure 2.
- Sacral unleveling is measured relative to a line drawn across the sacral base and compared with a true horizontal line (HB angle). Figure 2.
- Lumbo Sacral angle is the lower lumbar vertebra centroid line relative to the sacral base line and is the LS angle; this is similar to the FLSC in lumbar scoliotic deformity analysis. Figure 2.
- Lumbo-dorsal angle or mid lumbar scoliosis angle is similar in concept to a Cobb angle but it uses all the vertebrae to create the angle and thus is more representative of actual lumbar coronal bending alignment. Figure 2.
2.3. Data analysis
The descriptive statistics utilized in our investigation included count and percentages and these were used to describe categorical data. The Shapiro-walk test was used to test the normality of the numerical variables. Based on this, we report the median and interquartile ranges (IQR) to describe numerical data since all the numerical data such as age, exploratory radiological data, and the scores of the 4 study outcomes were not normally distributed. Multiple logistic regression models were used to assess the predictors of the success of each of the 4 outcomes as well as the 4 outcomes combined in one variable. Generalized estimation equations were developed and this is a type of regression used to assess the effect of time on pain, fatigue, distress, and interference scores as well as the effect of other potential predictors. SPSS version 25.0 for Windows (IBM, Armonk, NY, USA).
3. Results
Participant demographics and characteristics
Ninety patients participated in this investigation. The median age of the participants is 44 years with an IQR of 38-49, 73.3% of them have a normal weight, 54.4% are males, 75.6% had bachelor’s or master’s degrees, 54.4% are smokers, 92.2% are married, 70% have unilateral pain, the MSU location in 75.6 % of the participants is AB, however, the MSU magnitude in 92.2% of the participants is 2. Turning to the radiological exploratory variables, the median of T12 S1 Centroid horizontal displacement measures is 7 mm with an IQR 5 to 10 mm, the median of sacral un-leveling measures is 3 degrees with an IQR of 2 to 5.38 degrees, the median of lumbo-sacral angle measures is 87 degrees with an IQR 86-89 degrees, and finally the median of lumbo-dorsal measures is 7.5 degrees with an IQR of 5-10 degrees. The 4 study outcomes are pain, fatigue, distress, and interference, the percentage of success in these 4 outcomes are 53.3%, 53.3%, 11.1%, and 45.6% respectively, after considering the success in the 4 outcomes together, the main study outcome showed 10% success. Table 1 and Figure 3.
The results of Demographic characters distributed across gender are presented in Table 2. There were no statistically significant differences between males and females in any of the study variables.
As shown in Table 3, all the radiological variables are strongly correlated with each other (r > 0.7 and p < 0.001), for this reason, only one of these variables was used in the logistic regression models to prevent the potential multi-collinearity. The lumbosacral angle was the most suitable variable that was selected in all the models as the assumptions of the models were perfectly met by adding this variable. All the potential predictors were put in the models and the assumptions of each model were tested to make sure that each model can fit the data perfectly, regarding the model showing the predictors of distress, the variables education level, marital status, and MSU magnitude were removed as they showed infinite 95% CI due to the low sample size (only 10 people from 90 showed success in reducing distress scores).
As shown in Table 4, the same people who showed success in decreasing pain scores also showed success in decreasing fatigue scores and interference, so the models showing the predictors of pain, fatigue, and interference are the same. Age, educational level, and the lumbosacral angle measures significantly affected the odds of success. Increasing age 1 year has significantly decreased the odds of success of decreasing pain, fatigue, and interference scores by 15%, 15%, and 11% respectively (Pain and fatigue OR = 0.85, p = 0.016, while interference OR = 0.89, p = 0.042). High school or lower education has significantly increased the odds of success of lowering the scores of pain, fatigue, and interference by 26.18, 26.18, and 7.5 the odds when compared with bachelor or master education (p = 0.006, 0.006, and 0.029 respectively). Increasing the lumbosacral angle measures 1 degree has significantly increased the odds of success of lowering the scores of pain, fatigue, distress, and interference by 3.52, 3.52, 27.99, and 2.55 the odds respectively (p < 0.001, < 0.001, = 0.003, = 0.001 respectively).
The backward selection method was used to build this model, whereas the variables of education level, marital status, type of pain, and MSU magnitude were removed as they caused infinite confidence intervals due to the small sample size (only 9 people from 90 showed success of the combined outcomes). Both the crude and adjusted odds ratios of the lumbosacral angle measures showed significance, when the lumbosacral angle increases 1 degree, the odds of success of the combined outcome will significantly increase by 13.24 crude odds and 29.89 adjusted odds (p = 0.002 and 0.003 significantly). Table 5.
As shown in the above GEE model in Table 6, pain scores have significantly decreased by 47 points at discharge and decreased by 38 points after the 6 months of follow-up compared to the scores at baseline (p < 0.001, < 0.001 respectively). When the lumbosacral angle increases 1 degree, the pain scores significantly decrease by 4.4 points (p < 0.001).
As shown in the above GEE model in Table 7, fatigue scores have significantly decreased by 48 points at discharge and decreased by 31 points after the 6 months of follow-up compared to the scores at baseline (p < 0.001, < 0.001 respectively). When age increased 1 year, fatigue scores significantly increase by 0.38 points (p = 0.012). Those who are graduated from High school or have lower education have significantly decreased fatigue scores by 7.6 points compared to those with bachelor’s or master’s degree (p = 0.005). When the lumbosacral angle increases 1 degree, the fatigue scores significantly decrease by 2.2 points (p < 0.001).
As shown in Table 8, distress scores have significantly decreased by 42 points at discharge and decreased by 19 points after the 6 months of follow-up compared to the scores at baseline (p < 0.001, < 0.001 respectively). If age increased 1 year, distress scores significantly increase by 0.39 points (p = 0.013). When the lumbosacral angle increases 1 degree, the distress scores significantly decrease by 2.5 points (p < 0.001).
Interference scores have significantly decreased by 49 points at discharge and decreased by 28 points after the 6 months of follow-up compared to the scores at baseline (p < 0.001, < 0.001 respectively). When the lumbosacral angle increases 1 degree, the interference scores significantly decrease by 5.1 points (p < 0.001). Table 9.
4. Discussion
The current study was conducted to investigate if coronal radiological parameters and demographic variables might predict the successful outcome of physiotherapeutic interventions in clinical practice. We found that age, educational level, and coronal radiological markers all had a substantial impact on the likelihood of success. This finding is consistent with previous investigations that found age to be a significant predictor of HNP treatment success [32,33]. In contrast to previous studies [34,35], however, the current study findings indicate that lower education has significantly increased the odds of success of improving the scores of pain, fatigue, and interference (by 26.18, 26.18, and 7.5) when compared to patients with a bachelors or masters education. The cause of this discrepancy is not fully understood, where possible mechanisms include a direct effect of educational level on occupation; the majority of more educated people might be office workers with less physical activity which is a potential risk factor for low back pain.
4.1. Radiological parameters.
We found that the lumbosacral angle significantly affected the odds of success. We found multicollinearity between the potential radiological predictors, i.e. that the potential predictors were interrelated. A statistical consequence of this is that a multivariate regression model may give non-significant results even if several of the factors are important and significant in bivariate analyses. For instance, T12-S1 centroid horizontal displacement, sacral unleveling, lumbodorsal angle, and the lumbosacral angle may all be important predictors, but since these variables are correlated a regression model may give non-significant results for these predictors. As a matter of fact, the predictor lumbosacral angle is related to several of the other radiological variables. In several of the stepwise regression models, the lumbosacral angle was selected first. The fact that other predictors were not selected does not mean that they are unimportant, but they could be omitted just because part of the information they contain already is accounted for by the lumbosacral angle already included in the model.
The current study is among the first to look at lumbar coronal radiological parameters as predictors of the success of physiotherapeutic interventions in clinical practice for treatment of low back pain and radiculopathy due to HNP. Though, herein, we excluded patients from our population with LLD > 12mm, there is evidence to support mild to moderate leg length discrepancy (LLD < 12mm) and subsequent lumbosacral coronal imbalance as a cause of persistent biomechanical changes in the lumbar spine, and those biomechanical abnormalities may result in permanent degenerative changes to the lumbar spine. Previously, researchers have clarified the observed link between low back pain and coronal alignment and LLD [36,37,38]. The prevailing theory appears to be that pelvic tilt and compensatory, or functional, scoliosis resulted in unbalanced stress of the lumbar spine's intervertebral discs and facet joints in the short and long-term. This irregularity, in turn, causes mechanical low back pain and sciatica due to foraminal stenosis caused by disc bulging or herniation [38]. Additionally, it was considered that long-term aberrant spinal biomechanics caused degenerative disc degeneration and irreversible abnormalities in the lumbar spine [39].
One of the important factors that might contribute to long-term failure of rehabilitation programs is that biomechanical alterations influence the spine during gait and everyday activities. In a comprehensive study on this issue, Khamis and Carmeli found that a LLD of 10 mm can cause significant alterations in gait, and that these changes linearly correlate with the degree of discrepancy [40]. Gurney et al. [41] found that patients had increased oxygen consumption and felt exertion when they walked with a 20mm LLD as opposed to no discrepancy in an investigation of gait in 44 healthy men and women exposed to artificial LLD (in the form of shoe lifts). In a study of 653 Finnish military patients with persistent low back pain and 359 asymptomatic controls, Friberg noted that symptomatic individuals were 5.32 times more likely than asymptomatic patients to have an LLD of 15 mm. In support of this positive association, the author found that 91% of symptomatic patients treated conservatively with a shoe lift and monitored for at least 6 months had either diminished or resolved symptoms.[38] Friberg hypothesized that functional scoliosis caused by LLD compresses the concave side of the disc, causing it to expand posterolaterally toward the nerve root on the side of the longer leg. This notion was supported by his observation that the majority of patients experienced symptoms on the longer side [38].
More recent investigations have identified that imbalance in the coronal plane negatively affects patient satisfaction and is associated with increased pain, increased loss of function, and decreased quality of life [20,21,22,23]. For example, the fractional lumbo-sacral curve (FLSC), defined as the coronal curvature from L4-S1 that is generally in the opposite direction relative to the primary Cobb angle curvature in the lumbar spine, has been found to be a predictor of poor patient outcomes in conservative and surgical interventions in adult patient populations suffering from scoliotic deformities [24,25,26,27]. However, we could not locate any investigations looking at the FLSC in chronic low back pain patients with radiculopathy due to disc herniations and thus ours appears to the first conservative trial looking into this as an outcome affecting success of conservative care. The lumbo-sacral angle used in the current investigation is a type of measurement of the FLSC for the distal lumbo-pelvic spine and this measurement was reported two decades earlier [42]. In a population of chronic low back pain patients, Harrison and colleagues reported the reduction of lateral trunk translation following a program of reverse postural training and this trunk translation was shown to improve the lumbo-sacral angles as well as other coronal radiographic measures. It may be that both trunk lateral translation and mild-moderate LLD can contribute to increasing the lumbo-sacral angle and that these mechanical spine displacements may be relevant to identify as a predictor of patient responsive to conservative based interventions for this unique population.
4.2. Limitations and future investigations.
As with all investigations, our study has limitations. Primarily, this was not a randomized controlled trial looking at the success or failure of specific treatment interventions. Thus, it is not known whether the exact type of treatment provided was optimum as it was a compilation of interventions known to aid patients suffering from HNP. Furthermore, because we did not specifically look at interventions that are known to improve the lumbo-sacral angle and other coronal radiological measures, we cannot say whether improving these coronal lumbar alignment variables would result in better success for patients with this condition. Future randomized trials are needed to investigate these limitations in order to determine more effective clinical intervention strategies for patients with coronal lumbar radiographic imbalances in combination with HNP and lower back pain with radiculopathy.
4.3. Conclusions.
Our findings indicate that younger age, less education, and better coronal radiological lumbar spine alignment all had a substantial impact on the likelihood of success of 6-month outcomes in patients suffering from chronic lower back pain and radiculopathy due to HNP. Similar to the fractional lumbo-sacral curve in lumbar scoliotic deformities, the coronal lumbo-sacral angle as reported herein, warrants further investigation as to the effects of this radiographic spine displacement angle on patient pain, disability, and conservative care outcomes.
Author Contributions
YA: IM, MB, NH, PO, DH all participated in the research idea and participated in its design. YA, IM, MB, and DH contributed to the statistical analysis methods. YA, IM, MB, NH participated in data collection and study supervision. YA, IM, MB, NH, PO, DH all contributed to the interpretation of the results and wrote the drafts. All authors have read and agreed to the published version of the manuscript.
Funding
CBP Nonprofit (Eagle, ID, USA) approved possible funding of this manuscript for publication fees in the JCM. Deed Harrison’s role as a senior author and conflicts of interest are outlined below.
Institutional Review Board Statement
The research was conducted in accordance with international guidelines. The protocol of the study was approved by Ethical Review Boards of the UOS [REC-21-03-11-03-S].
Informed Consent Statement
All participants received informed consent prior to inclusion and participating in this investigation.
Data Availability Statement
The datasets analyzed in the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
PAO is a paid consultant for CBP NonProfit, Inc. DEH teaches rehabilitation methods and is the CEO of a company that distributes products to physicians in the U.S.A. used for the rehabilitation of postural abnormalities. All the other authors declare that they have no competing interests.
References
- Alexander, C.; Varacallo, M. Lumbosacral radiculopathy. StatPearls 2022, 1–8.
- Hahne, Andrew J. BPhysio*; Ford, Jon J. PhD*; McMeeken, Joan M. MSc†. Conservative management of lumbar disc herniation with associated radiculopathy: A systematic review. Spine 35(11):p E488-E504, May 15, 2010. [CrossRef]
- Lewis RA, Williams NH, Sutton AJ, et al. Comparative clinical effectiveness of management strategies for sciatica: systematic review and network meta-analyses. Spine J. 2015;15(6):1461 1477.
- Yang S, Kim W, Kong HH, Do KH, Choi KH. Epidural steroid injection versus conservative treatment for patients with lumbosacral radicular pain: A meta-analysis of randomized controlled trials. Medicine (Baltimore). 2020;99(30):e21283. [CrossRef]
- Vanti C, Saccardo K, Panizzolo A, Turone L, Guccione AA, Pillastrini P. The effects of the addition of mechanical traction to physical therapy on low back pain? A systematic review with meta-analysis. Acta Orthop Traumatol Turc. 2023;57(1):3-16. [CrossRef]
- Azharuddin, A.; Aryandono, T.; Magetsari, R.; Dwiprahasto, I. Predictors of the conservative management outcomes in patients with lumbar herniated nucleus pulposus: A prospective study in Indonesia. Asian J. Surg. 2022, 45, 277–283. [CrossRef]
- Parker, S.L.; Godil, S.S.; Mendenhall, S.K.; Zuckerman, S.L.; Shau, D.N.; Mcgirt, M.J. Two-year comprehensive medical management of degenerative lumbar spine disease (lumbar spondylolisthesis, stenosis, or disc Herniation): A value analysis of cost, pain, disability, and quality of life: clinical article. J. Neurosurg. Spine 2014, 21, 143–149. [CrossRef]
- Suri, P.; Rainville, J.; Gellhorn, A. Predictors of patient-reported recovery from motor or sensory deficits two years after acute symptomatic lumbar disk herniation. PM R 2012, 4. [CrossRef]
- Varlotta, C.G.; Ge, D.H.; Stekas, N.; Frangella, N.J.; Manning, J.H.; Steinmetz, L.; Vasquez-Montes, D.; Errico, T.J.; Bendo, J.A.; Kim, Y.H.; et al. MRI radiological predictors of requiring microscopic lumbar discectomy after lumbar disc herniation. Glob. spine J. 2020, 10, 63–68. [CrossRef]
- Chun, S.W.; Lim, C.Y.; Kim, K.; Hwang, J.; Chung, S.G. The relationship between low back pain and lumbar lordosis: A systematic review and meta-analysis. Spine J. 2017, 17, 1180–1191.
- Sadler, S.G.; Spink, M.J.; Ho, A.; De Jonge, X.J.; Chuter, V.H. Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: A systematic review of prospective cohort studies. BMC Musculoskelet. Disord. 2017, 18, 179.
- Mekhael, E.; El Rachkidi, R.; Saliby, R.M.; Nassim, N.; Semaan, K.; Massaad, A.; Karam, M.; Saade, M.; Ayoub, E.; Rteil, A.; et al. Functional assessment using 3D movement analysis can better predict health-related quality of life outcomes in patients with adult spinal deformity: A machine learning approach. Front. Surg. 2023, 10, 1166734. [Google Scholar] [CrossRef] [PubMed]
- Terran, J.; Schwab, F.; Shaffrey, C.I.; Smith, J.S.; Devos, P.; Ames, C.P.; Fu, K.M.; Burton, D.; Hostin, R.; Klineberg, E.; et al. The SRS-Schwab adult spinal deformity classification: Assessment and clinical correlations based on a prospective operative and nonoperative cohort. Neurosurgery 2013, 73, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Pellisé, F.; Vila-Casademunt, A.; Ferrer, M.; Domingo-Sàbat, M.; Bagó, J.; Pérez-Grueso, F.J.; Alanay, A.; Mannion, A.F.; Acaroglu, E.; European Spine Study Group (ESSG). Impact on health related quality of life of adult spinal deformity (ASD) compared with other chronic conditions. Eur. Spine J. 2015, 24, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Kyrölä, K.; Repo, J.; Mecklin, J.P.; Ylinen, J.; Kautiainen, H.; Häkkinen, A. Spinopelvic changes based on the simplified SRS-Schwab adult spinal deformity classification: relationships with disability and health-related quality of life in adult patients with prolonged degenerative spinal disorders. Spine 2018, 43, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A. Extension traction treatment for patients with discogenic lumbosacral radiculopathy: A randomized controlled trial. Clin. Rehabil. 2013, 27, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Moustafa IM, Diab AA. The effect of adding forward head posture corrective exercises in the management of lumbosacral radiculopathy: a randomized controlled study. J Manipulative Physiol Ther. 2015;38(3):167-178. [CrossRef]
- Moustafa IM, Diab AA, Harrison DE. The efficacy of cervical lordosis rehabilitation for nerve root function and pain in cervical spondylotic radiculopathy: A randomized trial with 2-year follow-up. J Clin Med. 2022;11(21):6515. Published 2022 Nov 2. [CrossRef]
- Moustafa IM, Diab AAM, Harrison DE. Does improvement towards a normal cervical sagittal configuration aid in the management of lumbosacral radiculopathy: A randomized controlled trial. J Clin Med. 2022;11(19):5768. Published 2022 Sep 29. [CrossRef]
- Acaroglu, E.; Guler, U.O.; Olgun, Z.D.; Yavuz, Y.; Pellise, F.; Domingo-Sabat, M.; Yakici, S.; Alanay, A.; Perez-Grueso, F.S.; Yavuz, Y. Multiple regression analysis of factors affecting health-related quality of life in adult spinal deformity. Spine Deform. 2015, 3, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Daubs, M.D.; Lenke, L.G.; Bridwell, K.H.; Kim, Y.J.; Hung, M.; Cheh, G.; Koester, L.A. Does correction of preoperative coronal imbalance make a difference in outcomes of adult patients with deformity? Spine (Phila. Pa. 1976). 2013, 38, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Koller, H.; Pfanz, C.; Meier, O.; Hitzl, W.; Mayer, M.; Bullmann, V.; Schulte, T.L. Factors influencing radiographic and clinical outcomes in adult scoliosis surgery: A study of 448 European patients. Eur. Spine J. 2016, 25, 532–548. [Google Scholar] [CrossRef] [PubMed]
- Ploumis, A.; Liu, H.; Mehbod, A.A.; Transfeldt, E.E.; Winter, R.B. A correlation of radiographic and functional measurements in adult degenerative scoliosis. Spine (Phila. Pa. 1976). 2009, 34, 1581–1584. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman SL, Chanbour H, Hassan FM, et al. The lumbosacral fractional curve vs maximum coronal Cobb angle in adult spinal deformity patients with coronal malalignment: Which matters more? [published online ahead of print, 2023 Mar 29]. Global Spine J. 2023;21925682231161564. [CrossRef]
- Zhang Z, Liu T, Wang Y, Wang Z, Zheng G. Factors related to preoperative coronal malalignment in degenerative lumbar scoliosis: An analysis on coronal parameters. Orthop Surg. 2022;14(8):1846-1852.
- Zhang J, Wang Z, Chi P, Chi C. Directionality of lumbosacral fractional curve relative to C7 plumb line, a novel index associated with postoperative coronal imbalance in patients with degenerative lumbar scoliosis. Spine (Phila Pa 1976). 2021;46(6):366-373. [CrossRef]
- Zhang J, Wang Z, Chi P, Chi C. Orientation of L4 coronal tilt relative to C7 plumb line as a predictor for postoperative coronal imbalance in patients with degenerative lumbar scoliosis. Sci Rep. 2020;10(1):16148. Published 2020 Sep 30. [CrossRef]
- Mysliwiec LW, Cholewicki J, Winkelpleck MD, Eis GP. MSU classification for herniated lumbar discs on MRI: toward developing objective criteria for surgical selection. Eur Spine J. 2010;19:1087–93. [CrossRef]
- Zeppieri, G.; George, S.Z. Patient-defined desired outcome, success criteria, and expectation in outpatient physical therapy: A longitudinal assessment. Health Qual. Life Outcomes 2017, 15. [Google Scholar] [CrossRef] [PubMed]
- Brown JL, Edwards PS, Atchison JW, Lafayette-Lucey A, Wittmer VT, Robinson ME. Affiliations expand. Defining patient-centered, multidimensional success criteria for treatment of chronic spine pain. Pain Med. 2008 ;9(7):851-62. [CrossRef]
- Harrison, D.E.; Holland, B.; Harrison, D.D.; Janik, T.J. Further reliability analysis of the harrison radiographic line-drawing methods: crossed ICCs for lateral posterior tangents and modified Risser-Ferguson method on AP views. J. Manipulative Physiol. Ther. 2002, 25, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, A.; Bolm-Audorff, U.; Ditchen, D.; Ellegast, R.; Grifka, J.; Haerting, J.; Hofmann, F.; Jäger, M.; Linhardt, O.; Luttmann, A.; et al. Do occupational risks for low back pain differ from risks for specific lumbar disc diseases? Results of the German lumbar spine study (EPILIFT). Spine (Phila. Pa. 1976). 2017, 42, E1204–E1211. [Google Scholar] [CrossRef] [PubMed]
- Silverplats, K.; Lind, B.; Zoëga, B.; Halldin, K.; Gellerstedt, M.; Brisby, H.; Rutberg, L. Clinical factors of importance for outcome after lumbar disc herniation surgery: Long-term follow-up. Eur. Spine J. 2010, 19, 1459–1467. [Google Scholar] [CrossRef] [PubMed]
- Dionne, C.E.; Von Korff, M.; Koepsell, T.D.; Deyo, R.A.; Barlow, W.E.; Checkoway, H. Formal education and back pain: A review. J. Epidemiol. Community Heal. 2001, 55, 455–468. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Hendrick, P.; Blake, H. Predictors of self-management in patients with chronic low back pain: A longitudinal study. BMC Musculoskelet. Disord. 2022, 23, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Giles, L.G.F.; Taylor, J.R. Low-back pain associated with leg length inequality. Spine (Phila. Pa. 1976). 1981, 6, 510–521. [Google Scholar] [CrossRef] [PubMed]
- Sheha, E.D.; Steinhaus, M.E.; Kim, H.J.; Cunningham, M.E.; Fragomen, A.T.; Rozbruch, S.R. Leg-length discrepancy, functional scoliosis, and low back pain. JBJS Rev. 2018, 6, e6. [Google Scholar] [CrossRef] [PubMed]
- Friberg, O. Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality. Spine (Phila. Pa. 1976). 1983, 8, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Wiltse LL. The effect of the common anomalies of the lumbar spine upon disc degeneration and low back pain. Orthop Clin North Am. 1971;2(2):569-582.
- Khamis, S.; Carmeli, E. Relationship and significance of gait deviations associated with limb length discrepancy: A systematic review. Gait Posture 2017, 57, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Gurney, B.; Mermier, C.; Robergs, R.; Gibson, A.; Rivero, D. Effects of limb-length discrepancy on gait economy and lower-extremity muscle activity in older adults. J. Bone Jt. Surg. 2001, 83, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Harrison DE, Cailliet R, Betz JW, et al. A non-randomized clinical control trial of Harrison mirror image methods for correcting trunk list (lateral translations of the thoracic cage) in patients with chronic low back pain. Eur Spine J. 2005;14(2):155-162. [CrossRef]
Figure 1.
Lumbar HNP was defined was diagnosed using magnetic resonance imaging. All types of protrusions (central, paramedian or foraminal) and all protrusion sizes (bulge, protrusion or extrusion) were included. The Michigan State University (MSU) classification for lumbar disc herniation was used as it is a simple and reliable method to objectively measure herniated lumbar discs [28].
Figure 1.
Lumbar HNP was defined was diagnosed using magnetic resonance imaging. All types of protrusions (central, paramedian or foraminal) and all protrusion sizes (bulge, protrusion or extrusion) were included. The Michigan State University (MSU) classification for lumbar disc herniation was used as it is a simple and reliable method to objectively measure herniated lumbar discs [28].

Figure 2.
Spine radiographs were analyzed for: (1) a lateral translation of T12 compared to S2 tubercle (TxT12-S1), (2) a mid-lumbar angle (LD), (3) the sacral base to horizontal (HB), and (4) lateral bending of the lower lumbar vertebra compared with the sacral base (LS). This method has excellent reliability [31].
Figure 2.
Spine radiographs were analyzed for: (1) a lateral translation of T12 compared to S2 tubercle (TxT12-S1), (2) a mid-lumbar angle (LD), (3) the sacral base to horizontal (HB), and (4) lateral bending of the lower lumbar vertebra compared with the sacral base (LS). This method has excellent reliability [31].
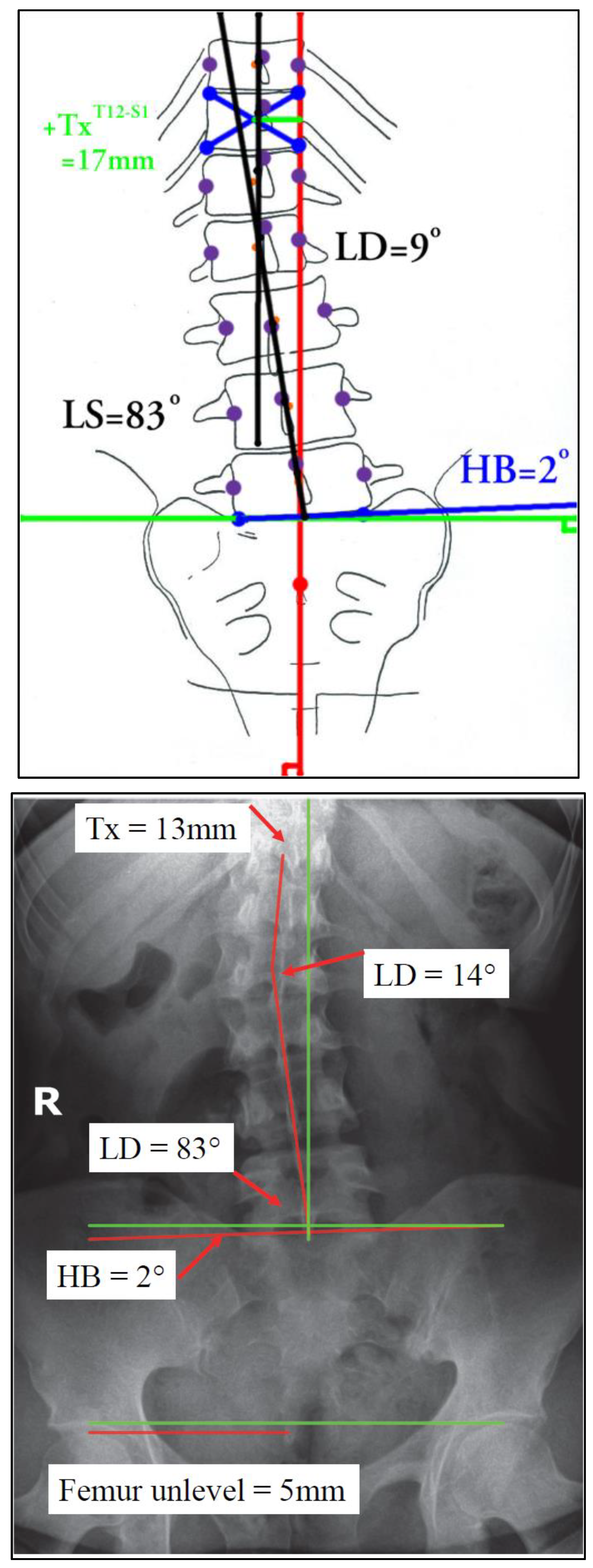
Figure 3.
Bar charts showing the percentage of success and failure of the 4 primary study patient relevant outcomes [29,30].
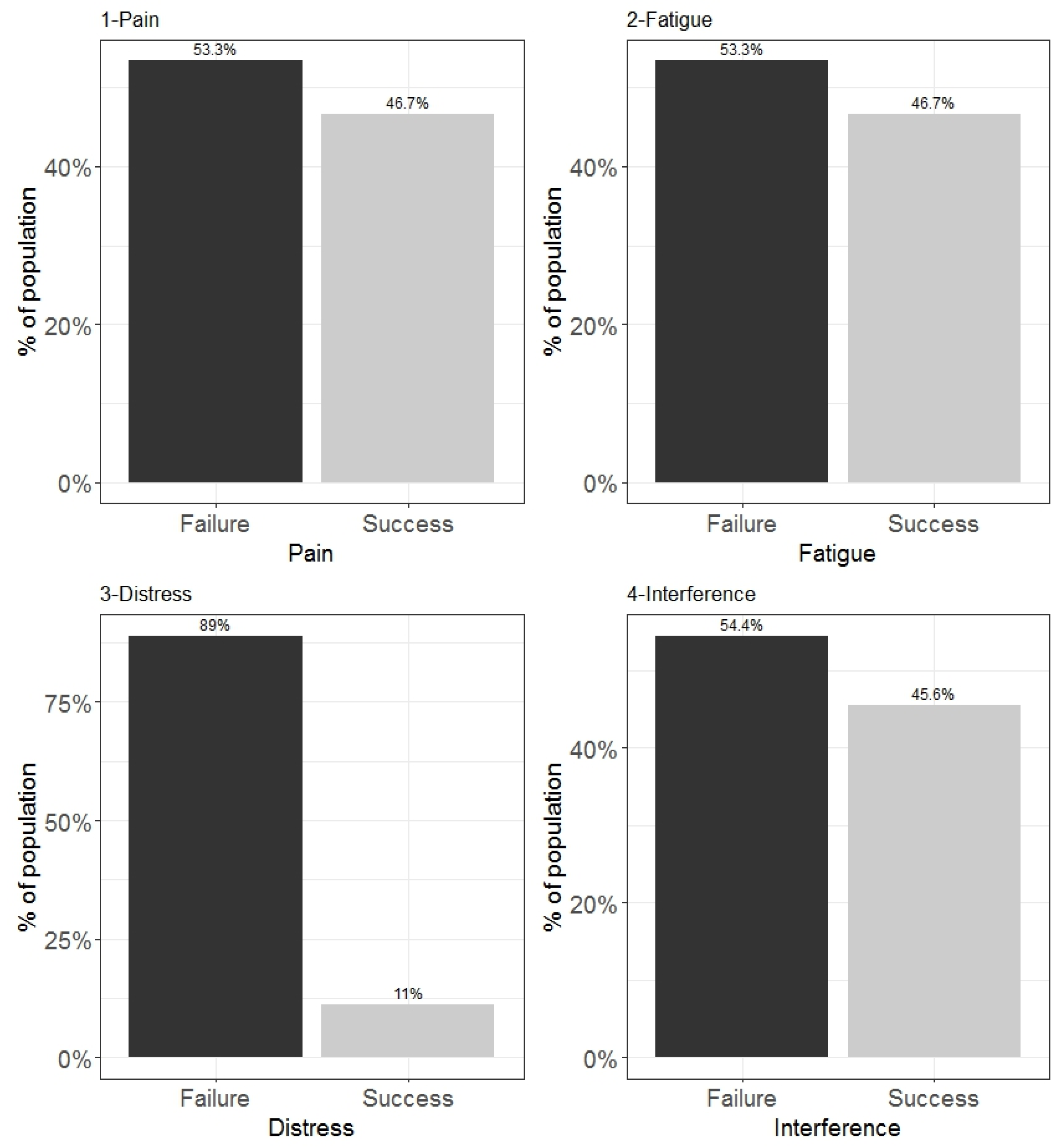

Table 1.
Demographic characteristics of the participants.
| Demographic characteristics of the study participants | N = 901 |
|---|---|
| Age | 44 (38, 49) |
| BMI | |
| Normal | 66 (73.3%) |
| Obese | 24 (26.7%) |
| Gender | |
| Female | 41 (45.6%) |
| Male | 49 (54.4%) |
| Educational level | |
| Bachelor or Master | 68 (75.6%) |
| High school or less | 22 (24.4%) |
| Smoking | |
| Yes | 49 (54.4%) |
| No | 41 (45.6%) |
| Marital status | |
| Married | 83 (92.2%) |
| Not married | 7 (7.8%) |
| Type of dominant pain | |
| Bilateral | 27 (30.0%) |
| Unilateral | 63 (70.0%) |
| MSU Location | |
| AB | 68 (75.6%) |
| B or C | 22 (24.4%) |
| MSU Magnitude | |
| 3 | 7 (7.8%) |
| 2 | 83 (92.2%) |
| T12 S1 Centroid horizontal displacement | 7 (5, 10) |
| Sacral un-leveling | 3.00 (2.00, 5.38) |
| Lumbo-Sacral angle | 87 (86, 89) |
| Lumbo-dorsal angle | 7.5 (5.0, 10.0) |
| Pain | |
| Failure | 48 (53.3%) |
| Success | 42 (46.7%) |
| Fatigue | |
| Failure | 48 (53.3%) |
| Success | 42 (46.7%) |
| Distress | |
| Failure | 80 (88.9%) |
| Success | 10 (11.1%) |
| Interference | |
| Failure | 49 (54.4%) |
| Success | 41 (45.6%) |
| Combined outcome (Pain, Fatigue, Distress, and Interference) | |
| Failure | 81 (90.0%) |
| Success | 9 (10.0%) |
| 1 Median (IQR); n (%) | |
Table 2.
Demographic characters distributed across gender.
| Demographic characteristics of the study participants | Gender | p-value2 | |
| Female, N = 411 |
Male, N = 491 |
||
| Age | 45 (42, 49) | 44 (37, 49) | 0.455 |
| BMI | 0.639 | ||
| Normal | 29 (70.7%) | 37 (75.5%) | |
| Obese | 12 (29.3%) | 12 (24.5%) | |
| Educational level | 0.615 | ||
| Bachelor or Master | 32 (78.0%) | 36 (73.5%) | |
| High school or less | 9 (22.0%) | 13 (26.5%) | |
| Smoking | 0.773 | ||
| Yes | 23 (56.1%) | 26 (53.1%) | |
| No | 18 (43.9%) | 23 (46.9%) | |
| Marital status | 0.121 | ||
| Married | 40 (97.6%) | 43 (87.8%) | |
| Not married | 1 (2.4%) | 6 (12.2%) | |
| Type of dominant pain | 0.890 | ||
| bilateral | 12 (29.3%) | 15 (30.6%) | |
| unilateral | 29 (70.7%) | 34 (69.4%) | |
| MSU Location | 0.615 | ||
| AB | 32 (78.0%) | 36 (73.5%) | |
| B or C | 9 (22.0%) | 13 (26.5%) | |
| MSU Magnitude | > 0.999 | ||
| 3 | 3 (7.3%) | 4 (8.2%) | |
| 2 | 38 (92.7%) | 45 (91.8%) | |
| T12 S1 Centroid horizontal displacement | 7 (5, 10) | 6 (4, 10) | 0.418 |
| Sacral un-leveling | 4.00 (2.00, 5.00) | 3.00 (2.00, 5.50) | 0.533 |
| Lumbo Sacral angle | 88.00 (87.00, 89.00) | 87.00 (86.00, 89.00) | 0.918 |
| Lumbo dorsal angle | 8.0 (6.0, 10.0) | 7.0 (5.0, 10.0) | 0.418 |
| Pain | 0.184 | ||
| Failure | 25 (61.0%) | 23 (46.9%) | |
| Success | 16 (39.0%) | 26 (53.1%) | |
| Fatigue | 0.184 | ||
| Failure | 25 (61.0%) | 23 (46.9%) | |
| Success | 16 (39.0%) | 26 (53.1%) | |
| Distress | 0.750 | ||
| Failure | 37 (90.2%) | 43 (87.8%) | |
| Success | 4 (9.8%) | 6 (12.2%) | |
| Interference | 0.255 | ||
| Failure | 25 (61.0%) | 24 (49.0%) | |
| Success | 16 (39.0%) | 25 (51.0%) | |
| Combined outcome | > 0.999 | ||
| Failure | 37 (90.2%) | 44 (89.8%) | |
| Success | 4 (9.8%) | 5 (10.2%) | |
| 1 Median (IQR); n (%) | |||
| 2 Wilcoxon rank sum test; Fisher's exact test; Pearson's Chi-squared test | |||
Table 3.
Correlation matrix between the radiographic variables.
| T12 S1 Centroid horizontal displacement | Sacral unleveling | Lumbo Sacral angle | Lumbo dorsal angle | |
| T12 S1 Centroid horizontal displacement | 1 | |||
| Sacral unleveling | 0.994 (< .001) |
1 | ||
| Lumbosacral angle | -0.796 (< .001) |
-0.791 (< .001) |
1 | |
| Lumbodorsal angle | 0.995 (< .001) |
0.993 ( < .001) |
-0.794 (< .001) |
1 |
| Computed correlation used spearman-method with listwise-deletion. | ||||
Table 4.
Logistic regression models showing the predictors of the 4 outcomes of the study.
| Pain | Fatigue | Distress | Interference | |||||
| Predictors of success | Odds Ratios (95% CI) | p | Odds Ratios (95% CI) |
p | Odds Ratios (95% CI) |
p | Odds Ratios (95% CI) |
P |
| Age | 0.85 (0.73 – 0.96) |
0.016 | 0.85 (0.73 – 0.96) |
0.016 | 0.88 (0.73 – 1.03) |
0.138 | 0.89 (0.79 – 0.99) |
0.042 |
| BMI [Obese] | 0.26 (0.03 – 1.78) |
0.187 | 0.26 (0.03 – 1.78) |
0.187 | 0.72 (0.01 – 26.33) |
0.866 | 0.16 (0.02 – 0.99) |
0.067 |
| Educational [High school or less] | 26.18 (3.36 – 365.34) |
0.006 | 26.18 (3.36 – 365.34) |
0.006 |
1.2 (0.98 - 46.45) |
0.8 | 7.50 (1.40 – 56.53) |
0.029 |
| Type of dominantpain [unilateral] | 1.33 (0.16 – 10.72) |
0.781 | 1.33 (0.16 – 10.72) |
0.781 | 1.35 (0.08 – 38.89) |
0.834 | 4.12 (0.61 – 31.65) |
0.150 |
| Smoking [No] | 1.40 (0.34 – 6.20) |
0.642 | 1.40 (0.34 – 6.20) |
0.642 | 0.33 (0.03 – 2.77) |
0.329 | 1.81 (0.47 – 7.64) |
0.393 |
| Marital status[Not married] | 1.54 (0.00 – 1487.04) |
0.943 | 1.54 (0.00 – 1487.04) |
0.943 | 2.31 (0.01 – 909.88) |
0.846 | ||
| MSU Location [B or C] | 2.58 (0.41 – 20.50) |
0.325 | 2.58 (0.41 – 20.50) |
0.325 | 0.07 (0.00 – 0.80) |
0.067 | 2.45 (0.44 – 16.65) |
0.320 |
| MSU Magnitude [2] | 0.06 (0.00 – 2.53) |
0.157 | 0.06 (0.00 – 2.53) |
0.157 | 0.10 (0.00 – 4.00) |
0.266 | ||
| Lumbo Sacral angle | 3.52 (1.94 – 8.03) |
<0.001 | 3.52 (1.94 – 8.03) |
<0.001 | 27.99 (4.99 – 473.94) |
0.003 | 2.55 (1.54 – 4.91) |
0.001 |
| Observations | 90 | 90 | 90 | 90 | ||||
Table 5.
Logistic regression model showing the predictors of the combined main study outcome.
| Dependent: | Crude OR | Adjusted OR | |
|---|---|---|---|
| Combined Outcome | |||
| Age | - | 1.01 (0.92 - 1.12, p = 0.836) | 0.92 (0.76 - 1.07, p = 0.296) |
| BMI | Normal | - | - |
| Obese | 0.32 (0.02 - 1.86, p = 0.289) | 0.85 (0.02 - 26.16, p = 0.926) | |
| Smoking | Yes | - | - |
| No | 0.57 (0.11 - 2.30, p = 0.442) | 0.62 (0.06 - 5.49, p = 0.665) | |
| MSU Location | AB | - | - |
| B or C | 0.87 (0.12 - 3.96, p = 0.870) | 0.12 (0.01 - 1.25, p = 0.115) | |
| Lumbo -sacral angle | - | 13.24 (3.52 - 98.70, p = 0.002) | 29.89 (4.95-504.31, p = 0.003) |
Table 6.
Generalized estimation equation table showing the predictors of pain score.
| Dependent= pain scores | Beta | 95% CI1 | p-value |
|---|---|---|---|
| Time | |||
| Baseline | — | — | |
| After completion of treatment | -47 | -51, -44 | < 0.001 |
| After 6 months | -38 | -42, -34 | < 0.001 |
| Age | 0.01 | -0.24, 0.25 | 0.960 |
| BMI | |||
| Normal | — | — | |
| Obese | 1.2 | -2.6, 4.9 | 0.540 |
| Gender | |||
| Female | — | — | |
| Male | -1.7 | -5.0, 1.6 | 0.303 |
| Educational level | |||
| Bachelor or Master | — | — | |
| High school or less | 3.0 | -1.6, 7.6 | 0.202 |
| Smoking | |||
| Yes | — | — | |
| No | -0.02 | -3.2, 3.1 | 0.991 |
| Marital status | |||
| Married | — | — | |
| Not married | -2.6 | -9.0, 3.9 | 0.437 |
| Type of dominant pain | |||
| Bilateral | — | — | |
| Unilateral | -2.7 | -7.3, 1.8 | 0.237 |
| MSU Location | |||
| AB | — | — | |
| B or C | 1.2 | -3.4, 5.8 | 0.614 |
| MSU Magnitude | |||
| 3 | — | — | |
| 2 | 0.61 | -7.6, 8.8 | 0.884 |
| Lumbo Sacral angle | -4.4 | -5.7, -3.2 | < 0.001 |
| 1 CI = Confidence Interval | |||
Table 7.
Generalized estimation equation table showing the predictors of fatigue scores.
| Dependent= Fatigue scores | Beta | 95% CI1 | p-value |
|---|---|---|---|
| Time | |||
| Baseline | — | — | |
| After disposal | -48 | -51, -45 | < 0.001 |
| After 6 months | -31 | -36, -26 | < 0.001 |
| Age | 0.38 | 0.08, 0.67 | 0.012 |
| BMI | |||
| Normal | — | — | |
| Obese | 1.8 | -2.4, 6.1 | 0.399 |
| Gender | |||
| Female | — | — | |
| Male | -2.3 | -6.0, 1.4 | 0.232 |
| Educational level | |||
| Bachelor or Master | — | — | |
| High school or less | -7.6 | -13, -2.3 | 0.005 |
| Smoking | |||
| Yes | — | — | |
| No | -0.36 | -4.0, 3.2 | 0.842 |
| Marital status | |||
| Married | — | — | |
| Not married | 1.5 | -4.6, 7.7 | 0.626 |
| Type of dominant pain | |||
| Bilateral | — | — | |
| Unilateral | 1.3 | -3.7, 6.3 | 0.603 |
| MSU Location | |||
| AB | — | — | |
| B or C | 0.83 | -4.5, 6.1 | 0.759 |
| MSU Magnitude | |||
| 3 | — | — | |
| 2 | 7.3 | -0.88, 15 | 0.080 |
| Lumbo Sacral angle | -2.2 | -3.5, -0.92 | < 0.001 |
| 1 CI = Confidence Interval | |||
Table 8.
Generalized estimation equation table showing the predictors of distress scores.
| Dependent= Distress scores | Beta | 95% CI1 | p-value |
|---|---|---|---|
| Time | |||
| Baseline | — | — | |
| After disposal | -42 | -46, -39 | < 0.001 |
| After 6 months | -19 | -24, -14 | < 0.001 |
| Age | 0.39 | 0.08, 0.69 | 0.013 |
| BMI | |||
| Normal | — | — | |
| Obese | -1.1 | -6.0, 3.7 | 0.645 |
| Gender | |||
| Female | — | — | |
| Male | -2.0 | -5.9, 1.8 | 0.300 |
| Educational level | |||
| Bachelor or Master | — | — | |
| High school or less | 1.1 | -3.7, 6.0 | 0.652 |
| Smoking | |||
| Yes | — | — | |
| No | 0.77 | -3.0, 4.6 | 0.690 |
| Marital status | |||
| Married | — | — | |
| Not married | -1.5 | -8.1, 5.2 | 0.667 |
| Type of dominant pain | |||
| Bilateral | — | — | |
| Unilateral | 0.04 | -5.9, 6.0 | 0.988 |
| MSU Location | |||
| AB | — | — | |
| B or C | -4.2 | -9.7, 1.4 | 0.142 |
| MSU Magnitude | |||
| 3 | — | — | |
| 2 | -4.8 | -13, 3.6 | 0.262 |
| Lumbosacral angle | -2.5 | -4.0, -1.0 | < 0.001 |
| 1 CI = Confidence Interval | |||
Table 9.
Generalized estimation equation table showing the predictors of interference scores.
| Dependent=Interference scores | Beta | 95% CI1 | p-value |
|---|---|---|---|
| Time | |||
| Baseline | — | — | |
| After disposal | -49 | -52, -46 | < 0.001 |
| After 6 months | -28 | -32, -23 | < 0.001 |
| Age | 0.24 | -0.03, 0.52 | 0.086 |
| BMI | |||
| Normal | — | — | |
| Obese | 3.2 | -0.66, 7.2 | 0.104 |
| Gender | |||
| Female | — | — | |
| Male | -2.2 | -5.8, 1.4 | 0.225 |
| Educational level | |||
| Bachelor or Master | — | — | |
| High school or less | 1.6 | -3.7, 6.8 | 0.553 |
| Smoking | |||
| Yes | — | — | |
| No | 1.1 | -2.5, 4.6 | 0.554 |
| Marital status | |||
| Married | — | — | |
| Not married | 0.27 | -6.3, 6.9 | 0.936 |
| Type of dominant pain | |||
| Bilateral | — | — | |
| Unilateral | -3.8 | -8.7, 1.1 | 0.125 |
| MSU Location | |||
| AB | — | — | |
| B or C | 0.20 | -4.3, 4.7 | 0.932 |
| MSU Magnitude | |||
| 3 | — | — | |
| 2 | 6.0 | -2.9, 15 | 0.185 |
| Lumbo Sacral angle | -5.1 | -6.4, -3.9 | < 0.001 |
| 1 CI = Confidence Interval | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



