
Submitted:
12 October 2023
Posted:
13 October 2023
You are already at the latest version
Abstract
Background. This study aimed to establish a prognostic nomogram for predicting overall survival (OS) and cancer-specific survival (CSS) of patients with early-onset endometrial cancer (EOEC). Methods. Patients diagnosed with EOEC during 2004-2015 were extracted from the Surveillance, Epidemiology, and End Results (SEER) database. Univariate and multivariate Cox regression analyses were performed to ascertain the independent factors impacting the prognosis of EOEC patients, while a prognostic nomogram was established. Its performance was verified by the receiver operating characteristic (ROC) curves, and calibration plots. The prediction accuracy and clinical net benefit between the model, TNM stage and SEER stage were further compared by the concordance index (C-index) and decision curve analysis (DCA). Results. A total of 4415 eligible patients with EOEC were identified and enrolled in this study. Independent prognostic factors for OS and CSS were confirmed by multivariate Cox regression, which were further incorporated to constructed a nomogram. ROC curves and calibration curves indicated an optimal accuracy of the nomogram. Meanwhile, the C-index and DCA showed the predictive capability and the clinical applicability of the nomogram was superior over the TNM stage and SEER stage. Conclusions. Nomogram based on risk factors was developed as an individualized tool to predict OS and CSS for EOEC patients. The novel tool will assist in patient counseling and selection of appropriate therapeutic regimens.
Keywords:
early-onset endometrial cancer
; prognostic nomogram
; overall survival
; cancer-specific survival
; SEER
1. Introduction
Endometrial cancer (EC) is the most common gynaecological malignancies, and the sixth most common cancer in women, with an estimated 65620 newly diagnosed cases and over 12590 deaths in 2021, seriously threatening women’s health [1,2]. The overall incidence of EC is slowly increasing, while the number of young women with EC is doubled [3]. This may be due to the prevalence of EC screening, as well as the influence of obesity [4], metabolic syndrome [5], insulin resistance [6], and reproductive factors [7,8]. A woman’s lifetime risk of developing EC is about 3%, with a median age at diagnosis of 61 years old [9]. Patients with EC usually have classical clinical manifestations of postmenopausal bleeding, which facilitates early diagnosis. However, the pre-operative diagnosis of EC in premenopausal young women is a clinical challenge.
There is no consensus on explicit definition of early-onset endometrial cancer (EOEC). According to previous literature and clinical studies, EOEC denotes that EC patients are diagnosed at an age < 50 years old [10,11,12]. EOEC patients have a more favorable prognosis than elderly patients with more frequent well-differentiated tumor and better tumor stage [13]. However, recurrence can still occur even in early-stage patients with EOEC, which is the primary cause of cancer death.
Clinically, TNM staging system has been widely implemented in cancer management. However, this prognostic scoring system only considers tumor invasion, regional lymph node, and distant metastasis as predictors, and does not incorporate demographic and clinical characteristics, making it limited and not an accurate predictor of prognosis [14]. Therefore, it is necessary to develop nomogram models based on multiple risk factors to analyze the prognosis of cancer patients.
Currently, some nomograms have been constructed to predict the prognosis of EC patients, but these models are not suitable for assessing the survival of EOEC [15,16]. To fill this research gap, we conducted this study based on SEER database to explore the prognostic variables and construct specific nomograms for EOEC. Then, the predictive performance and application value of nomograms were validated and further compared with TNM stage and SEER stage. Effective prediction of prognosis in EOEC can inform evidence-based interventions for the individual and reduce the healthcare burden of this disease.
2. Materials and Methods
2.1. Patients Population
EC patients who were diagnosed during 2004-2015 were obtained from the SEER database using SEER*Stat program (v8.4.0.1). Patients with EOEC were identified by the histological code (ICD-O-3) and the cancer staging scheme (v0204) [17]. The exclusion criteria were (1) age ≥ 50 years old; (2) multiple primary tumors; (3) incomplete clinicopathological data (race, tumor size, grade, and TNM stage); (4) survival information or surgical records missing. The flow diagram of the screened EOEC patients was depicted in Figure 1. Since the data were derived from the publicly available SEER database, institutional review board approval and informed consent were not required.
2.2. Variables
Variables encompassed age, race, grade, tumor size, TNM 7th stage, SEER stage, surgery, lymphadenectomy, radiotherapy, and chemotherapy. OS was defined as the period from diagnosis to death or last follow-up. CSS was defined as the period from diagnosis to death caused by endometrial cancer or censoring. X-tile program was utilized to evaluate the optimal thresholds for variables (tumor size and patients age) (Figure 2) [18].
2.3. Statistical Analysis
EOEC patients were randomly separated into either a training cohort or a verification cohort. The training cohort was employed to develop the nomograms, then accuracy of the prediction models were assessed by the verification cohort. SPSS (v25.0) and R (v4.2.1) software were utilized for statistical analysis. Detailed R code was provided in Supplementary Materials R. Categorical data were expressed as frequencies with percentages, and further analyzed by Chi-square test or Fisher’s exact test. Kaplan-Meier analyses were utilized to generate and describe OS and CSS curves. Multivariate Cox regression was utilized to verify the predictors. Meanwhile, hazard ratio (HR) were calculated, which were displayed with 95% CI. P-value <0.05 were considered as statistically significant.
3. Results
3.1. Demographic and Clinical Characteristics
Demographic information and clinical data of EC patients were selected from SEER database during 2004-2015. A total of 4415 younger and 36267 elderly patients were screened and enrolled. Detailed information about clinical pathological features were demonstrated in Table 1. In the whole study cohort, elderly patients accounted for the majority of the cases (89.1%), whereas younger patients accounted for only 10.9%. In terms of race, the proportion of other races, such as Asian/Pacific Islanders, in younger patients is higher than that in elderly patients. With regard to the grade and TNM stage, younger patients have a higher proportion of grade I (55.9%), T1 stage (81.5%), N0 stage (91.1%), and M0 stage (95.9%). Concerning treatment, more elderly patients received lymphadenectomy (68.2%), radiotherapy (31.1%), and chemotherapy (23.9%). Moreover, survival analysis illustrated that younger patients had higher OS and CSS than elderly patients (P < 0.0001) (Figure 3).
Among EOEC patients, 3092 patients were separated into a training cohort and the rest into a validation cohort (n = 1323). There were not statistically different between the datasets and their baseline characteristics were summarized in Table S1.
3.2. Establishment of the Nomogram
Univariate and multivariate Cox regression analyses were performed to identify independent prognostic factors (Table 2 and Table 3). Then, six predictors identified by multivariate regression models were further recruited and used for developing OS and CSS nomogram models, including age, race, grade, T stage, tumor size, and surgery (Figure 4). According to the degree of contribution of each predictor to the resulting events (OS and CSS), the corresponding points (the first axis) were obtained. Then, the points of each predictor were summed to predict the survival probability of EOEC patients.
3.3. Validation of the Nomogram
The established nomogram models were further verified with C-index and AUC values. In the OS and CSS prediction models, the C-index values for the training cohort were 0.828 (95% CI: 0.801-0.855) and 0.827 (95% CI: 0.800-0.854). While for validation cohort, the C-index values were 0.844 (95% CI: 0.809-0.879) and 0.889 (95% CI: 0.854-0.924). AUC values of the models were above 0.8, demonstrating that the models had good discriminatory (Figure 5). The calibration curves demonstrated that only minor deviations from perfect consistency between the predicted and observed values, implying that the models fit well (Figure 6).
In addition, we evaluated the merits and demerits of the newly constructed nomograms by comparing with TNM stage and SEER stage. First, we used C-index to verify the prediction models for OS and CSS, which were better than TNM stage and SEER stage (Table 4 and Table 5). Moreover, the DCA results also implied that the clinical applicability of the models were superior over TNM stage and SEER stage (Figure 7).
3.4. Survival Analysis
The Kaplan-Meier method was used to evaluate the OS and CSS among EOEC patients (Figure 8 and Figure S1). Age had an impact on survival, with patients aged > 47 years seeming to have a worse prognosis. Black patients had the shorter survival time than other race, and the prognosis of patients with tumors > 7.8 cm seems to have a worse survival. In terms of tumor characteristics, T stage and tumor grade were respectively related to the outcome of EOEC patients. Patients with T4 stage or grade IV had worse OS and CSS significantly. Meanwhile, OS and CSS improved significantly with surgery compared to untreated patients.
4. Discussion
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
The overall incidence of EC has increased in recent years, especially among younger patients. EOEC has gradually become a unique subset due to the significant differences in clinical manifestations, clinicopathological features, and survival prognosis [19]. In our present study, although young patients with EC accounted for only 10.9%, due to the large population base of patients, this number is still large and increasing. Thus, it’s of great significance to accurately predict the survival time of EOEC patients by comprehensively considering multiple clinical features. Here, we first constructed and validated specialized survival nomograms for EOEC to predict individual OS and CSS.
In this study, twelve factors of demographic and clinical characteristics were analyzed, and six factors were determined as predictors for constructing nomograms, which consisted of age, tumor size, race, grade, T stage, and surgery. These variables have been reported to be associated with the prognosis of EOEC patients [20]. In our study, age was an independent prognostic factor for EOEC patients. Elderly patients with EC are often accompanied by some basic diseases, such as diabetes, hypertension, neurological diseases, etc., which cause deterioration of patients’ condition. For young patients, their physical fitness, immunity, and tolerance are relatively good, allowing for earlier diagnosis and a better prognosis. More interestingly, we observed a higher risk of death in patients > 47 years; similarly with multivariate analysis results, survival analysis also indicated a worse prognosis for patients > 47 years. It is speculated that some premenopausal women aged > 47 years mostly presented clinically with menstrual disorders that cover up EOEC and delay the diagnosis, which may be a potential cause of adverse prognosis. Therefore, clinicians should be alert to these women with risk factors and treat them aggressively; conversely, patients younger than 47 years should be evaluated thoroughly to avoid overtreatment.
A number of studies have demonstrated race was associated with the prognosis of EC, which were consistent with our findings [21]. Our present study suggested that Black women with EOEC had a worse prognosis compared to White women. Moreover, we also found that survival rates for other races were between Blacks and Whites, which may be related to changes in people’s living style and eating habits in recent years. An epidemiological report indicated that although the incidence of endometrial cancer in Black women is similar to that of Whites, the death rate is 97% higher than that in White women [22]. The difference in cancer prognosis can be attributed in part to genetics differences, the majority of race disparity is driven by variations in socioeconomic status and access to quality medical care [23,24]. By measuring the weights of variables on the nomogram scale, we found that tumor grade was the most important prognostic factor for EOEC, with a higher grade frequently indicating a worse prognosis. Despite the overall survival rate of patients is relatively high, high-grade EC tend to recur, which is one of the main causes of death [25,26]. Our present study demonstrated tumor size and T stage were closely related to the survival status of patients with EOEC, especially when tumor size larger than 7.8 cm as well as deep tumor invasion (T3 and T4), presenting a worse OS. This result was in agreement with previous reports [27]. Additionally, our study also confirmed the importance of surgical treatment for EOEC patients, which can prolong the OS and CSS. In the study by Son J et al. [28], 96.1% young patients with EC underwent hysterectomy, whereas patients who opted for fertility-sparing treatment with progestin therapy were associated with higher recurrence rates. Therefore, surgical treatment is of great significance in improving the prognosis and survival of patients with EOEC.
Noteworthy, N stage, M stage, radiotherapy, and chemotherapy were not candidate predictors for EOEC in the present study. Actually, N and M stages were considered as essential risk factors for EC patients, we considered that these disagreements arose from our focus on EOEC patients rather than all EC patients, and some high-risk clinical features, including high N and M stages, were infrequently found in EOEC. Hence, using these factors to predict the survival of EOEC may not be reliable. More intriguingly, younger patients were less likely to receive adjuvant therapy than the older groups, making radiotherapy and chemotherapy not significant in multivariate analysis [28].
In recent years, many predict models and molecular scoring systems have been established to predict the survival status of EC patients. But the high cost of testing and the cumbersome inspections make it difficult to carry out in many regions. The nomogram we established was based on six readily available clinical characteristics, which was more beneficial to clinicians in assessing patients’ prognosis and make appropriate clinical decisions. Meanwhile, our model was based on a representative large population-based dataset from SEER, which enhances its generalizability. Moreover, the analysis of only EOEC cases provided an opportunity to comprehensively consider the variables incorporated into the model. The nomogram that integrated multiple clinical variables outperformed than TNM stage and SEER stage, and showed good prognostic discrimination in patients with EOEC.
However, there remains some limitation in our study. First, detailed treatment records were not adequately provided in the SEER database, including surgical procedures and chemotherapy regimens, which hinders further exploration of EOEC. Second, other known prognostic factors, such as lymphovascular space invasion, histological type, estrogen receptor, and progesterone receptor, were not contained in the present study. Finally, our study was derived from a retrospective analysis of public data, which may cause selection bias; and the predictive accuracy of the model should be further confirmed by a multicenter prospective study.
5. Conclusions
In summary, the nomograms were available for predicting the survival prognosis of patients with EOEC to assist clinicians in making treatment decisions and scientific management of patients.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary Materials R: Related computerized programs for nomogram with R; Table S1: Baseline characteristics of the training set and the validation set; Figure S1: Survival analysis of different variables affecting CSS in patients with early-onset endometrial cancer.
Author Contributions
Y.Z. and P.J. are co-first authors. Y.Z. and Y.T. contributed to the acquisition of the data and data analysis, and Y.Z. drafted the manuscript. Y.H., J.W., C.T. and S.G. contributed to the literature search. R.Y. and Q.C. contributed to the major concept of this study and provided funding support. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the Natural Science Foundation of Chongqing (grant number: CSTB2022NSCQ-MSX0071).
Institutional Review Board Statement
Since this study used de-identified data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results program, ethical review and approval were not required.
Informed Consent Statement
This study used de-identified data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results program, and informed consent was not required.
Data Availability Statement
Publicly available datasets were analysed in this study. This data can be found in the SEER database (https://seer.cancer.gov/).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel RL, Miller KD and Jemal A. Cancer statistics, 2020. CA Cancer J Clin, 2020, 70(1): 7-30.
- Liu J, Cui G, Ye J, et al. Comprehensive Analysis of the Prognostic Signature of Mutation-Derived Genome Instability-Related lncRNAs for Patients With Endometrial Cancer. Front Cell Dev Biol, 2022, 10: 753957.
- Yao K, Zheng H and Li T. Association Between Metformin Use and the Risk, Prognosis of Gynecologic Cancer. Front Oncol, 2022, 12: 942380. [CrossRef]
- Reeves KW, Carter GC, Rodabough RJ, et al. Obesity in relation to endometrial cancer risk and disease characteristics in the Women's Health Initiative. Gynecol Oncol, 2011, 121(2): 376-382. [CrossRef]
- Yao X and Wang X. Bioinformatics searching of diagnostic markers and immune infiltration in polycystic ovary syndrome. Front Genet, 2022, 13: 937309. [CrossRef]
- Esposito G, Bravi F, Serraino D, et al. Diabetes Risk Reduction Diet and Endometrial Cancer Risk. Nutrients, 2021, 13(8): 2630. [CrossRef]
- Wu QJ, Li YY, Tu C, et al. Parity and endometrial cancer risk: a meta-analysis of epidemiological studies. Sci Rep, 2015, 5: 14243. [CrossRef]
- Wernli KJ, Ray RM, Gao DL, et al. Menstrual and reproductive factors in relation to risk of endometrial cancer in Chinese women. Cancer Causes Control, 2006, 17(7): 949-955. [CrossRef]
- Crosbie EJ, Kitson SJ, McAlpine JN, et al. Endometrial cancer. Lancet, 2022, 399(10333): 1412-1428. [CrossRef]
- Choi J, Holowatyj AN, Du M, et al. Distinct Genomic Landscapes in Early-Onset and Late-Onset Endometrial Cancer. JCO Precis Oncol, 2022, 6: e2100401. [CrossRef]
- Walsh MD, Cummings MC, Buchanan DD, et al. Molecular, pathologic, and clinical features of early-onset endometrial cancer: identifying presumptive Lynch syndrome patients. Clin Cancer Res, 2008, 14(6): 1692-1700. [CrossRef]
- Parslov M, Lidegaard O, Klintorp S, et al. Risk factors among young women with endometrial cancer: a Danish case-control study. Am J Obstet Gynecol, 2000, 182(1 Pt 1): 23-29. [CrossRef]
- Crissman JD, Azoury RS, Barnes AE, et al. Endometrial carcinoma in women 40 years of age or younger. Obstet Gynecol, 1981, 57(6): 699-704. [PubMed]
- Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J Clin, 2017, 67(2): 93-99. [CrossRef]
- Wang Z, Zhang S, Ma Y, et al. A nomogram prediction model for lymph node metastasis in endometrial cancer patients. BMC Cancer, 2021, 21(1): 748. [CrossRef]
- Celli V, Guerreri M, Pernazza A, et al. MRI- and Histologic-Molecular-Based Radio-Genomics Nomogram for Preoperative Assessment of Risk Classes in Endometrial Cancer. Cancers (Basel), 2022, 14(23): 5881. [CrossRef]
- Doll KM and Winn AN. Assessing endometrial cancer risk among US women: long-term trends using hysterectomy-adjusted analysis. Am J Obstet Gynecol, 2019, 221(4): 318.e311-318.e319. [CrossRef]
- Camp RL, Dolled-Filhart M and Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res, 2004, 10(21): 7252-7259. [CrossRef]
- Abdol Manap N, Ng BK, Phon SE, et al. Endometrial Cancer in Pre-Menopausal Women and Younger: Risk Factors and Outcome. Int J Environ Res Public Health, 2022, 19(15): 9059. [CrossRef]
- Yamagami W, Susumu N, Banno K, et al. Clinicopathologic manifestations of early-onset endometrial cancer in Japanese women with a familial predisposition to cancer. J Obstet Gynaecol Res, 2005, 31(5): 444-451. [CrossRef]
- Tarney CM, Tian C, Wang G, et al. Impact of age at diagnosis on racial disparities in endometrial cancer patients. Gynecol Oncol, 2018, 149(1): 12-21. [CrossRef]
- Giaquinto AN, Miller KD, Tossas KY, et al. Cancer statistics for African American/Black People 2022. CA Cancer J Clin, 2022, 72(3): 202-229. [CrossRef]
- Bailey ZD, Feldman JM and Bassett MT. How Structural Racism Works - Racist Policies as a Root Cause of U.S. Racial Health Inequities. N Engl J Med, 2021, 384(8): 768-773. [CrossRef]
- Williams DR, Lawrence JA and Davis BA. Racism and Health: Evidence and Needed Research. Annu Rev Public Health, 2019, 40: 105-125. [PubMed]
- Jiang P, Huang J, Deng Y, et al. Predicting Recurrence in Endometrial Cancer Based on a Combination of Classical Parameters and Immunohistochemical Markers. Cancer Manag Res, 2020, 12: 7395-7403. [CrossRef]
- Jiang P, Wang J, Gong C, et al. A Nomogram Model for Predicting Recurrence of Stage I-III Endometrial Cancer Based on Inflammation-Immunity-Nutrition Score (IINS) and Traditional Classical Predictors. J Inflamm Res, 2022, 15: 3021-3037. [CrossRef]
- Saha S, Shaik M, Johnston G, et al. Tumor size predicts long-term survival in colon cancer: an analysis of the National Cancer Data Base. Am J Surg, 2015, 209(3): 570-574. [CrossRef]
- Son J, Carr C, Yao M, et al. Endometrial cancer in young women: prognostic factors and treatment outcomes in women aged ≤40 years. Int J Gynecol Cancer, 2020, 30(5): 631-639. [CrossRef]
Figure 1.
Flowchart of selection of EOEC.
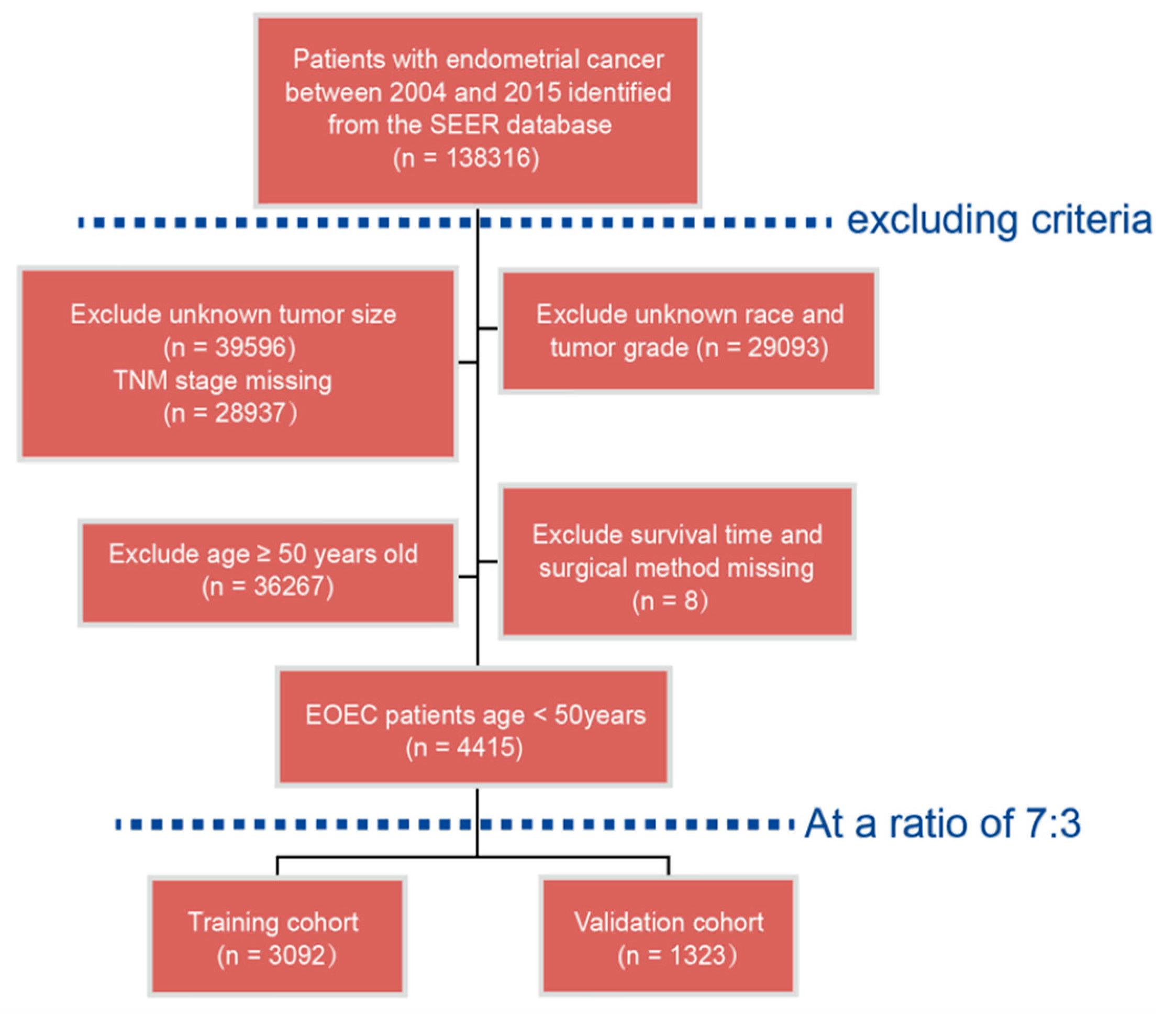
Figure 2.
The optimal thresholds for variables were evaluated using X-tile. (a-c) The optimal thresholds for patients age in the entire cohort were assessed by X-tile; (d-f) The optimal thresholds for tumor size in the entire cohort were assessed by X-tile.
Figure 2.
The optimal thresholds for variables were evaluated using X-tile. (a-c) The optimal thresholds for patients age in the entire cohort were assessed by X-tile; (d-f) The optimal thresholds for tumor size in the entire cohort were assessed by X-tile.
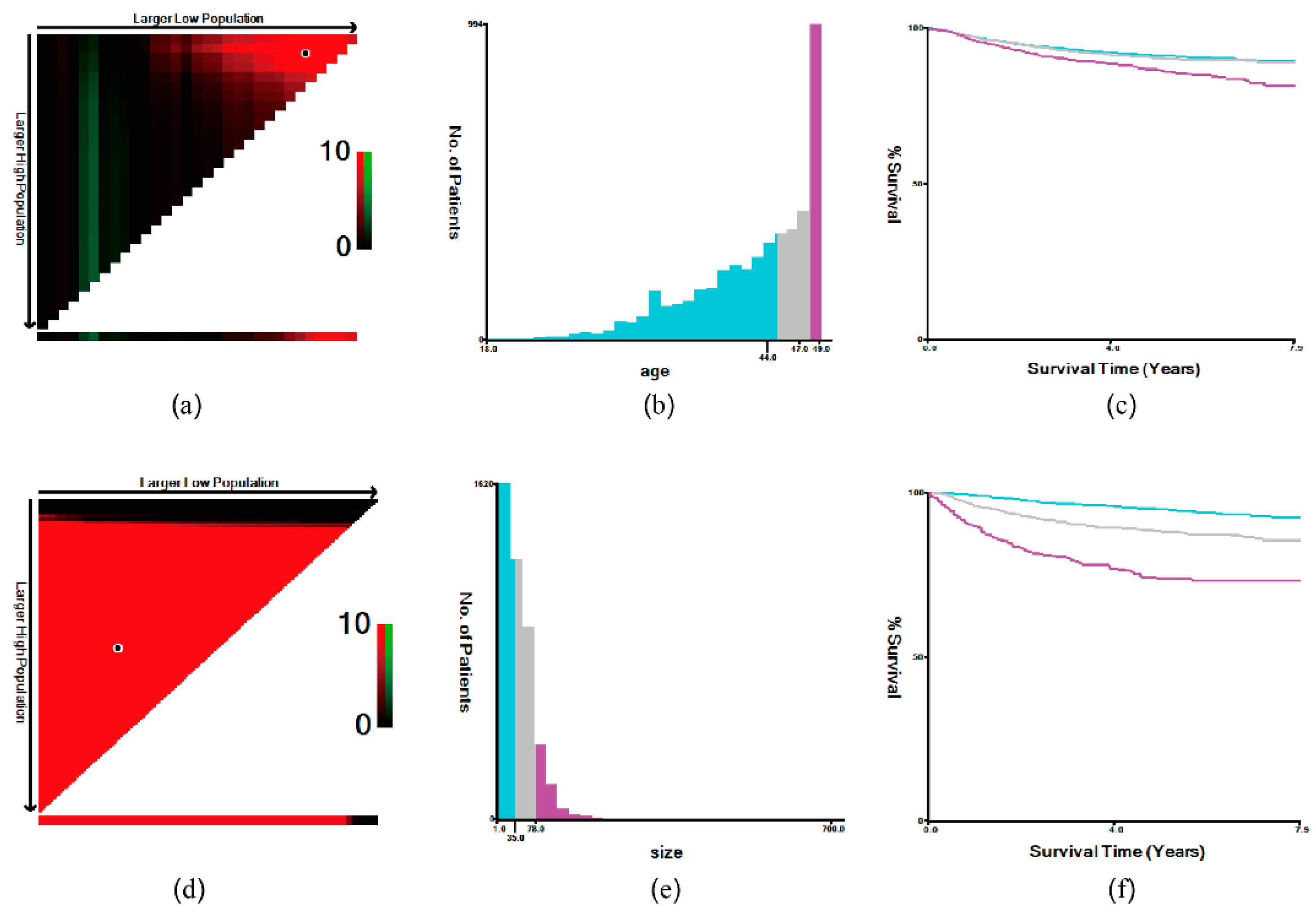
Figure 3.
Kaplan-Meier plots of (a) OS and (b) CSS in younger and elderly patients with EC.
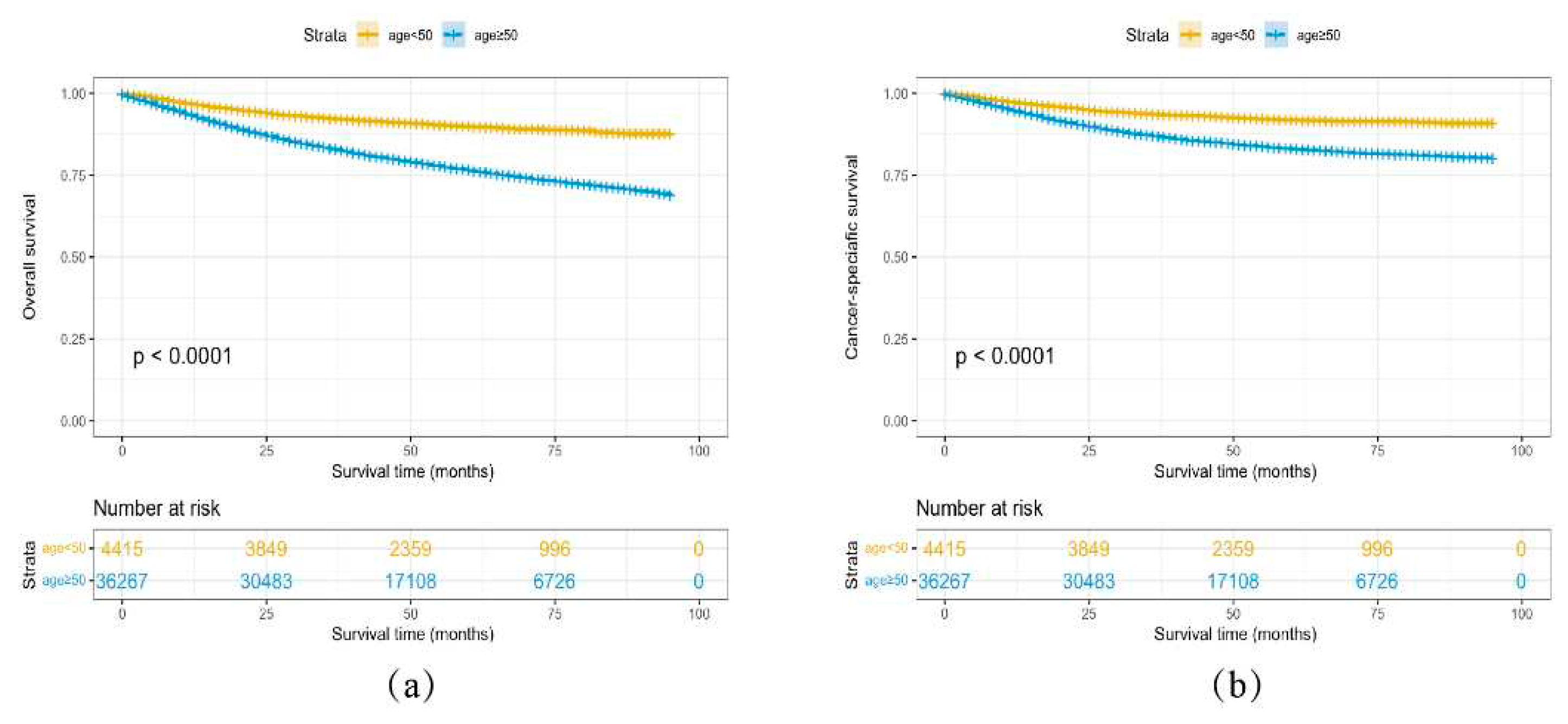
Figure 4.
Nomograms for early-onset endometrial cancer patients predicting 3- and 5-year (a) OS and (b) CSS.
Figure 4.
Nomograms for early-onset endometrial cancer patients predicting 3- and 5-year (a) OS and (b) CSS.
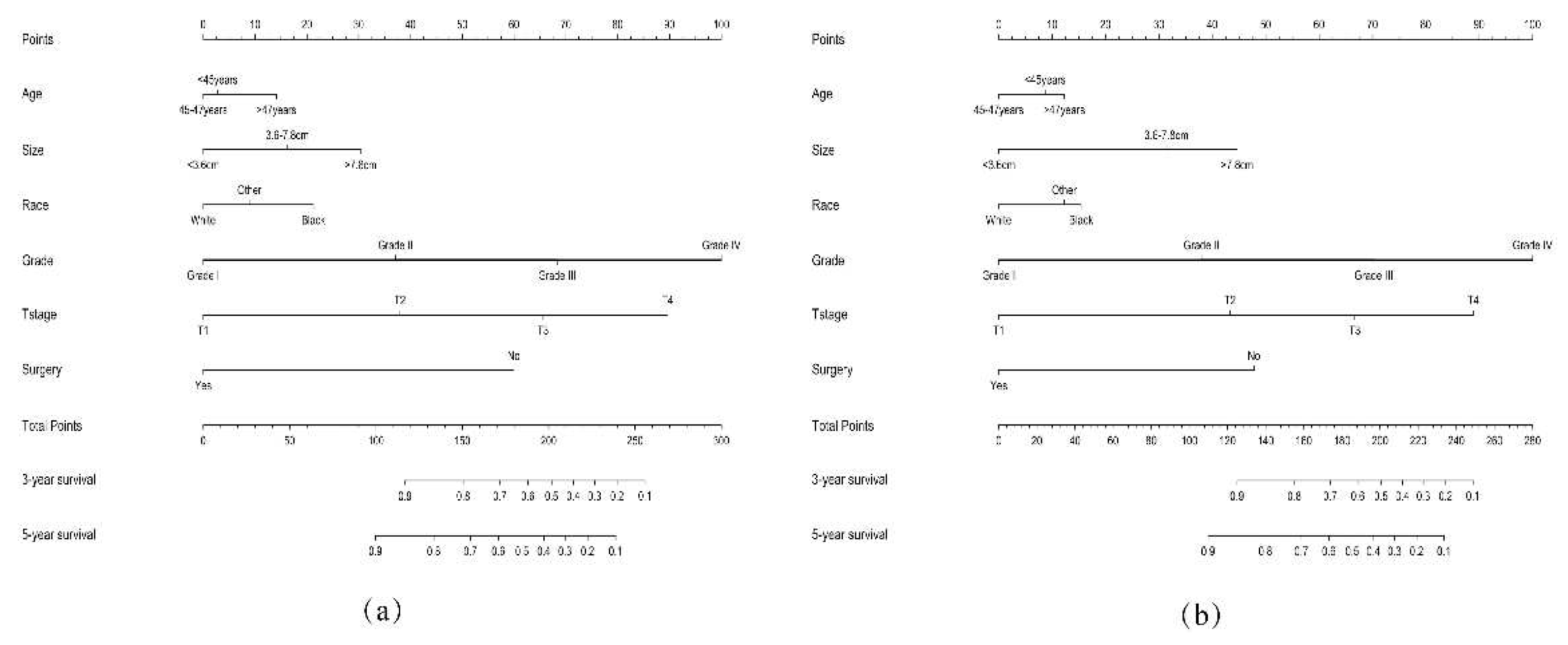
Figure 5.
ROC analysis of models for 3- and 5-year OS in (a) the training cohort; (b) the validation cohort; for 3- and 5-year CSS in (c) the training cohort; (d) the validation cohort.
Figure 5.
ROC analysis of models for 3- and 5-year OS in (a) the training cohort; (b) the validation cohort; for 3- and 5-year CSS in (c) the training cohort; (d) the validation cohort.
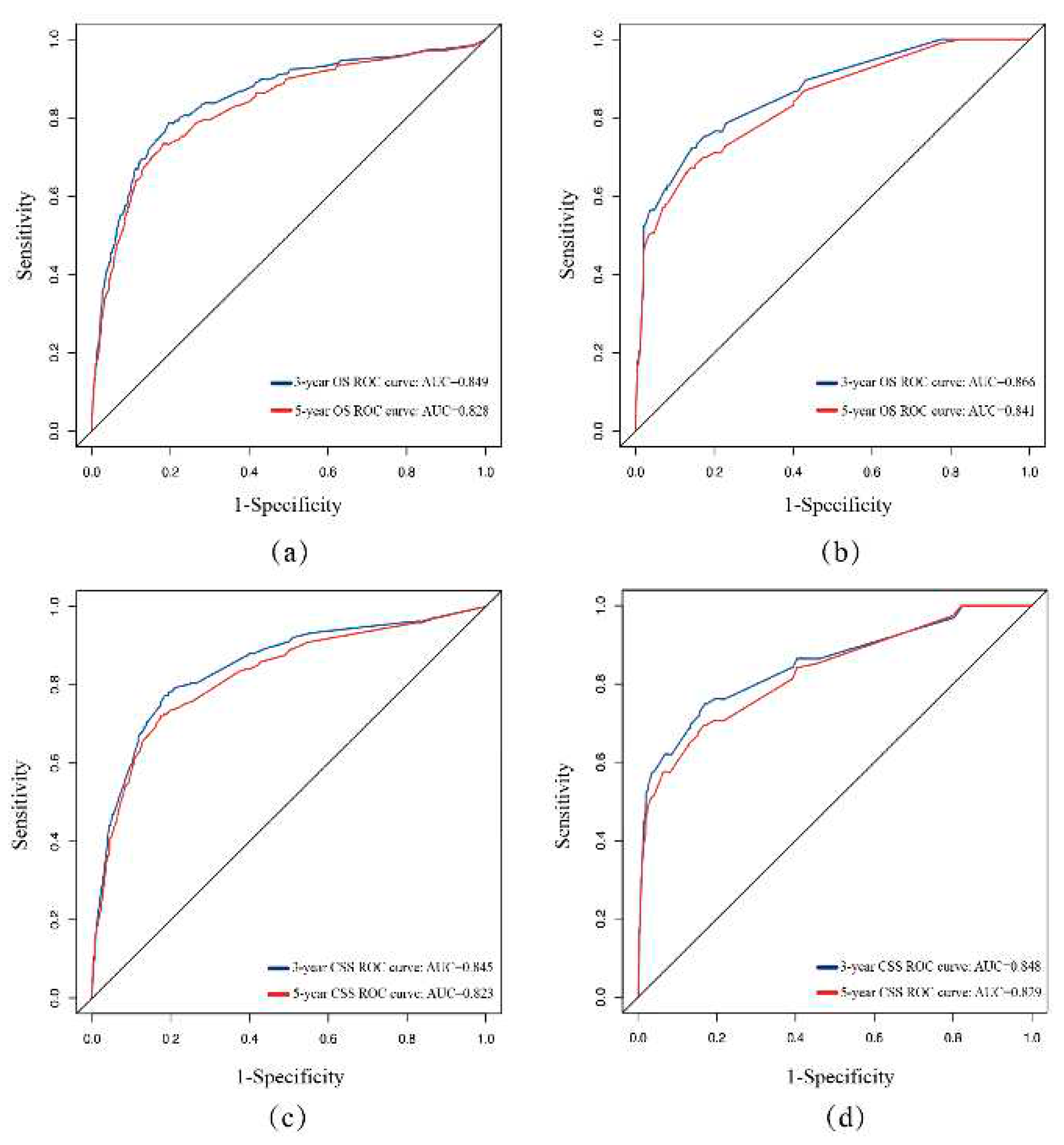
Figure 6.
Calibration plots of nomograms for 3- and 5-year OS in (a, b) the training cohort; (c, d) the validation cohort; for 3- and 5-year CSS in (e, f) the training cohort; (g, h) the validation cohort.
Figure 6.
Calibration plots of nomograms for 3- and 5-year OS in (a, b) the training cohort; (c, d) the validation cohort; for 3- and 5-year CSS in (e, f) the training cohort; (g, h) the validation cohort.
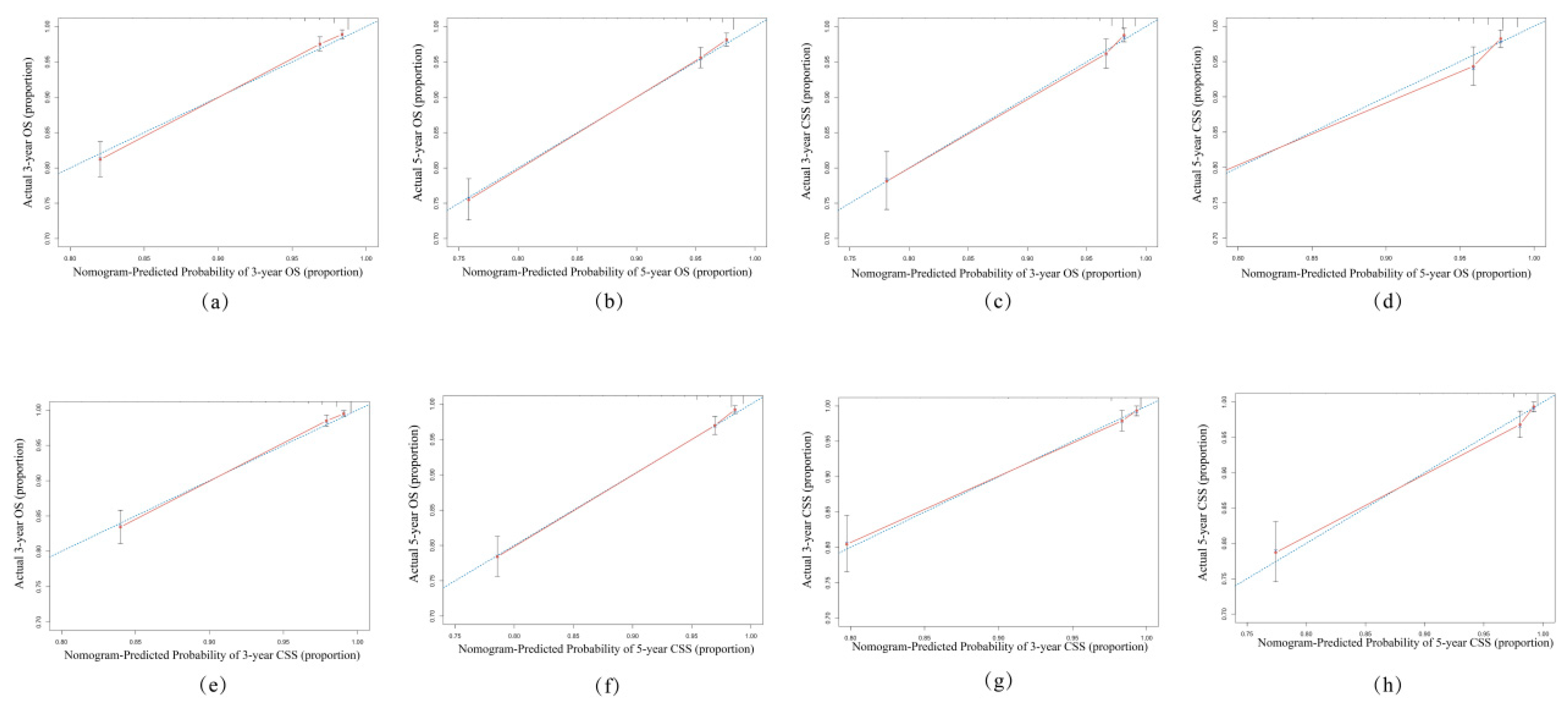
Figure 7.
DCA for different risk stratification systems for 3- and 5-year OS in (a, b) the training cohort; (c, d) the validation cohort; for 3- and 5-year CSS in (e, f) the training cohort; (g, h) the validation cohort.
Figure 7.
DCA for different risk stratification systems for 3- and 5-year OS in (a, b) the training cohort; (c, d) the validation cohort; for 3- and 5-year CSS in (e, f) the training cohort; (g, h) the validation cohort.
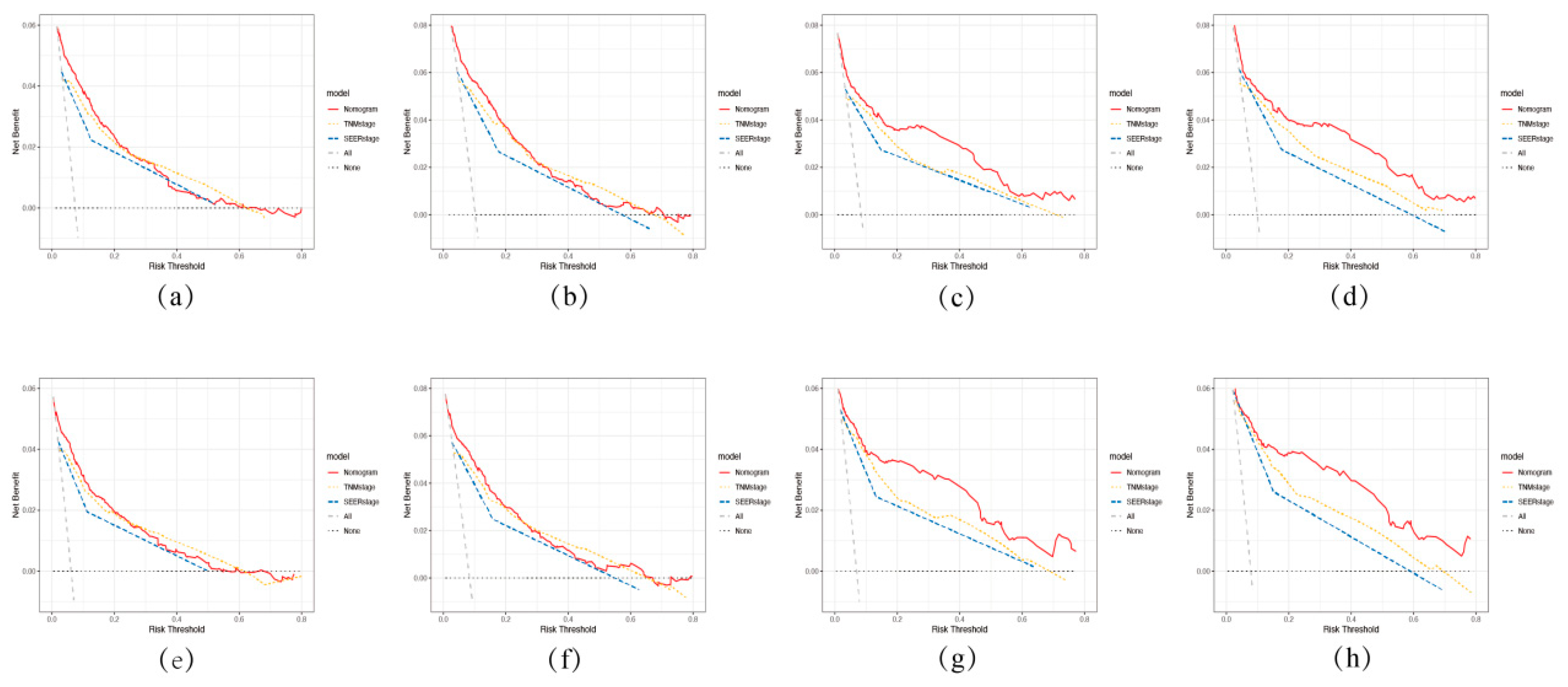
Figure 8.
Survival analysis to determine the impact of (a) age; (b) tumor size; (c) race; (d)T stage; (e) grade; (f) surgery on OS.
Figure 8.
Survival analysis to determine the impact of (a) age; (b) tumor size; (c) race; (d)T stage; (e) grade; (f) surgery on OS.
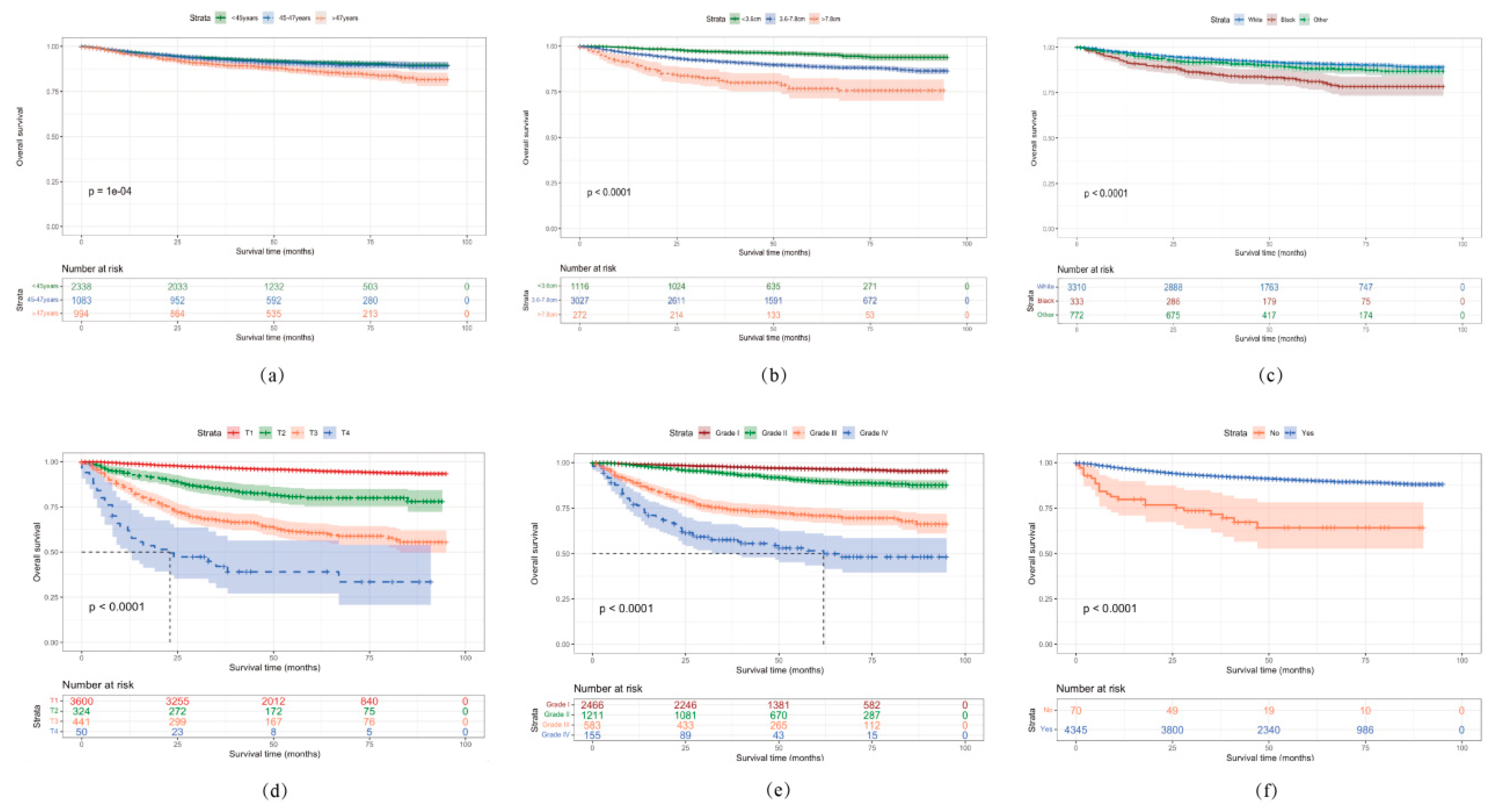

Table 1.
Baseline demographic and clinicopathologic characteristics of younger and elderly patients with EC.
Table 1.
Baseline demographic and clinicopathologic characteristics of younger and elderly patients with EC.
| Variables | Age < 50 years old (n = 4415) |
Age ≥ 50 years old (n = 36267) |
P value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Race | <0.001* | ||||
| White | 3310 | 75.0 | 29535 | 81.5 | |
| Black | 333 | 7.5 | 3451 | 9.5 | |
| Other | 772 | 17.5 | 3281 | 9.0 | |
| Grade | <0.001* | ||||
| I | 2466 | 55.9 | 14351 | 39.6 | |
| II | 1211 | 27.4 | 9980 | 27.5 | |
| III | 583 | 13.2 | 8436 | 23.3 | |
| IV | 155 | 3.5 | 3500 | 9.6 | |
| T stage | 0.018* | ||||
| T1 | 3600 | 81.5 | 29081 | 80.2 | |
| T2 | 324 | 7.3 | 2580 | 7.1 | |
| T3 | 441 | 10.1 | 4093 | 11.3 | |
| T4 | 50 | 1.1 | 513 | 1.4 | |
| N stage | <0.001* | ||||
| N0 | 4023 | 91.1 | 31958 | 88.1 | |
| N1 | 237 | 5.4 | 2526 | 7.0 | |
| N2 | 155 | 3.5 | 1783 | 4.9 | |
| M stage | 0.002* | ||||
| M0 | 4232 | 95.9 | 34359 | 94.7 | |
| M1 | 183 | 4.1 | 1908 | 5.3 | |
| Tumor size (cm) | <0.001* | ||||
| <3.6 | 1116 | 25.3 | 7815 | 21.5 | |
| 3.6-7.8 | 3027 | 68.5 | 25998 | 71.7 | |
| >7.8 | 272 | 6.2 | 2454 | 6.8 | |
| SEER stage | <0.001* | ||||
| Localized | 3232 | 73.2 | 25104 | 69.2 | |
| Regional | 978 | 22.2 | 9027 | 24.9 | |
| Distant | 205 | 4.6 | 2136 | 5.9 | |
| Surgery | 0.746 | ||||
| No | 70 | 1.6 | 552 | 1.5 | |
| Yes | 4345 | 98.4 | 35715 | 98.5 | |
| Lymphadenectomy | <0.001* | ||||
| No | 1879 | 42.6 | 11541 | 31.8 | |
| Yes | 2536 | 57.4 | 24726 | 68.2 | |
| Radiotherapy | <0.001* | ||||
| No/Unknown | 3509 | 79.5 | 25000 | 68.9 | |
| Yes | 906 | 20.5 | 11267 | 31.1 | |
| Chemotherapy | <0.001* | ||||
| No/Unknown | 3546 | 80.3 | 27602 | 76.1 | |
| Yes | 869 | 19.7 | 8665 | 23.9 | |
*, P <0.05.
Table 2.
Univariate and multivariate analyses for OS in the training cohort (n=3092).
| Variables | No. of patients | Univariate analysis | Multivariate analysis | |
|---|---|---|---|---|
| P value | HR (95% CI) | P value | ||
| Age | <0.001* | |||
| <45 | 1624 | Ref | ||
| 45-47 | 760 | 0.99 (0.73-1.3) | 0.95 | |
| >47 | 708 | 1.4 (1.1-1.9) | 0.011* | |
| Race | <0.001* | |||
| White | 2323 | Ref | ||
| Black | 241 | 1.7 (1.2-2.4) | 0.002* | |
| Other | 528 | 1.2 (0.9-1.7) | 0.19 | |
| Grade | <0.001* | |||
| I | 1735 | Ref | ||
| II | 836 | 2.2 (1.6-3.2) | <0.001* | |
| III | 411 | 3.9 (2.6-5.7) | <0.001* | |
| IV | 110 | 7.5 (4.7-12) | <0.001* | |
| T stage | <0.001* | |||
| T1 | 2510 | Ref | ||
| T2 | 248 | 2.2 (1.3-3.6) | 0.002* | |
| T3 | 296 | 2.6 (1.6-4) | <0.001* | |
| T4 | 38 | 2.8 (1.4-5.7) | 0.004* | |
| N stage | <0.001* | |||
| N0 | 2812 | Ref | ||
| N1 | 170 | 1.2 (0.83-1.7) | 0.35 | |
| N2 | 110 | 1.3 (0.88-1.9) | 0.19 | |
| M stage | <0.001* | |||
| M0 | 2962 | Ref | ||
| M1 | 130 | 2.4 (0.86-6.6) | 0.096 | |
| Tumor size (cm) | <0.001* | |||
| <3.6 | 778 | Ref | ||
| 3.6-7.8 | 2124 | 1.4 (0.98-2.1) | 0.06 | |
| >7.8 | 190 | 1.8 (1.1-2.9) | 0.017* | |
| SEER stage | <0.001* | |||
| Localized | 2259 | Ref | ||
| Regional | 687 | 1.2 (0.74-1.9) | 0.47 | |
| Distant | 146 | 1.6 (0.5-5) | 0.44 | |
| Surgery | <0.001* | |||
| No | 47 | Ref | ||
| Yes | 3045 | 0.29 (0.17-0.49) | <0.001* | |
| Lymphadenectomy | 0.36 | – | – | |
| No | 1322 | – | – | |
| Yes | 1770 | – | – | |
| Radiotherapy | <0.001* | |||
| No/Unknown | 2451 | Ref | ||
| Yes | 641 | 0.77 (0.59-1) | 0.06 | |
| Chemotherapy | <0.001* | |||
| No/Unknown | 2489 | Ref | ||
| Yes | 603 | 1.1 (0.76-1.5) | 0.66 | |
HR, hazard ratio; CI, confidence intervals; *, P <0.05.
Table 3.
Univariate and multivariate analyses for CSS in the training cohort (n=3092).
| Variables | No. Of patients | Univariate analysis | Multivariate analysis | |
|---|---|---|---|---|
| P value | HR (95% CI) | P value | ||
| Age | 0.005* | |||
| <45 | 1624 | Ref | ||
| 45-47 | 760 | 1 (0.74-1.4) | 0.95 | |
| >47 | 708 | 1.5 (1.1-1.9) | 0.008* | |
| Race | <0.001* | |||
| White | 2323 | Ref | ||
| Black | 241 | 1.7 (1.2-2.4) | 0.001* | |
| Other | 528 | 1.2 (0.9-1.7) | 0.21 | |
| Grade | <0.001* | |||
| I | 1735 | Ref | ||
| II | 836 | 2.2 (1.6-3.2) | <0.001* | |
| III | 411 | 3.9 (2.6-5.7) | <0.001* | |
| IV | 110 | 7.6 (4.8-12) | <0.001* | |
| T stage | <0.001* | |||
| T1 | 2510 | Ref | ||
| T2 | 248 | 2.2 (1.3-3.6) | 0.002* | |
| T3 | 296 | 2.5 (1.6-4) | <0.001* | |
| T4 | 38 | 2.6 (1.3-5.4) | 0.008* | |
| N stage | <0.001* | |||
| N0 | 2812 | Ref | ||
| N1 | 170 | 1.2 (0.84-1.7) | 0.33 | |
| N2 | 110 | 1.3 (0.9-2) | 0.15 | |
| M stage | <0.001* | |||
| M0 | 2962 | Ref | ||
| M1 | 130 | 2.2 (0.79-6.3) | 0.13 | |
| Tumor size (cm) | <0.001* | |||
| <3.6 | 778 | Ref | ||
| 3.6-7.8 | 2124 | 1.5 (1-2.1) | 0.048* | |
| >7.8 | 190 | 1.8 (1.1-3) | 0.017 | |
| SEER stage | <0.001* | |||
| Localized | 2259 | Ref | ||
| Regional | 687 | 1.2 (0.73-1.9) | 0.49 | |
| Distant | 146 | 1.7 (0.53-5.4) | 0.38 | |
| Surgery | <0.001* | |||
| No | 47 | Ref | ||
| Yes | 3045 | 0.28 (0.17-0.48) | <0.001* | |
| Lymphadenectomy | 0.23 | – | ||
| No | 1322 | – | ||
| Yes | 1770 | – | ||
| Radiotherapy | <0.001* | |||
| No/Unknown | 2451 | Ref | ||
| Yes | 641 | 0.78 (0.59-1) | 0.071 | |
| Chemotherapy | <0.001* | |||
| No/Unknown | 2489 | Ref | ||
| Yes | 603 | 1.1 (0.75-1.5) | 0.73 | |
HR, hazard ratio; CI, confidence intervals; *, P <0.05.
Table 4.
C-index of different risk stratification systems for OS in the training and validation set.
Table 4.
C-index of different risk stratification systems for OS in the training and validation set.
| Risk stratification systems | Training set | Validation set | ||
|---|---|---|---|---|
| C-index | 95% CI | C-index | 95% CI | |
| AJCC TNM stage | 0.772 | (0.743-0.801) | 0.766 | (0.720-0.813) |
| SEER stage | 0.758 | (0.729-0.787) | 0.773 | (0.730- 0.816) |
| Nomogram model | 0.828 | (0.801-0.855) | 0.844 | (0.809-0.879) |
index, concordance index; CI, confidence interval; OS, overall survival.
Table 5.
C-index of different risk stratification systems for CSS in the training and validation set.
Table 5.
C-index of different risk stratification systems for CSS in the training and validation set.
| Risk stratification systems | Training set | Validation set | ||
|---|---|---|---|---|
| C-index | 95% CI | C-index | 95% CI | |
| AJCC TNM stage | 0.770 | (0.741- 0.799) | 0.837 | (0.792-0.882) |
| SEER stage | 0.756 | (0.727-0.785) | 0.826 | (0.783-0.869) |
| Nomogram model | 0.827 | (0.800-0.854) | 0.889 | (0.854-0.924) |
index, concordance index; CI, confidence interval; CSS, cancer-specific survival.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



