
Submitted:
12 October 2023
Posted:
13 October 2023
You are already at the latest version
Abstract
Liver transplantation is currently the only curative therapy for patients with liver cirrhosis. Not all patients in the natural course of the disease will undergo transplantation, but the majority of them will experience portal hypertension and its complications. In addition to medical and endoscopic therapy, a key role in managing these complications is played by the placement of a transjugular intrahepatic portosystemic shunt (TIPS). Some indications for TIPS placement are well-established and they are expanding and broadening over time. This review aims to describe the role of TIPS in managing patients with liver cirrhosis, considering them as potential candidates for liver transplantation. As far as is known TIPS placement seems not to affect the surgical aspects of liver transplantation, in terms of intra operative bleeding rates, postoperative complications or length of stay in the Intensive Care Unit. However, the placement of a TIPS “towards transplant" can offer advantages in terms of enhancing the patient's clinical condition at the time of transplantation and improving patient survival. Additionally, the TIPS procedure can help preserve the technical feasibility of the transplant itself. In this context, indications for TIPS placement may be expanded and considered at an earlier stage. TIPS insertion can also lead to serious adverse events and there are no evidence-based recommendations on this topic to date. For these reasons further studies are needed to make reliable recommendations for TIPS in the pre-transplant setting.
Keywords:
Transjugular Intrahepatic Portosystemic Shunt
; TIPS
; liver transplantation
; bridge to transplant
; timing
1. Introduction
Cirrhosis represents an advanced stage of chronic liver disease, characterized by an unfavorable prognosis and associated with 2,4% of global deaths in 2019 (1) due to liver decompensation.
Complications of liver cirrhosis arise from liver failure and from the development of portal hypertension leading to a progressive worsening of the disease. Mortality rate ranges from less than 1% per year in patients with compensated cirrhosis to more than 20% per year after the first ascitic decompensation (2) (3).
To treat complications of portal hypertension chronic medical treatment is needed, with diuretics and nonselective beta-blocker (NSBB) (4) (5) or endoscopic band ligation. However, during the natural history of cirrhosis, some patients may develop difficult to treat/refractory ascites or high risk of recurrent gastrointestinal (GI) bleeding, requiring a Transjugular intrahepatic portosystemic shunt (TIPS) procedure (6). Following TIPS placement, the pressure in the portal venous system drops, reducing the risk of variceal bleeding and improving refractory ascites. Due to the treatment of Portal Hypertension (PH) TIPS may even improve patients’ survival (7) but the progression of liver failure and its consequences, frequently leave liver transplant as the only definitive treatment in these patients. (Figure 1). For these reasons (8) during the clinical course of advanced liver disease, TIPS may also be an opportunity to allow more patients to reach the time of liver transplant more safely.
2. TIPS towards Liver Transplant: Role and Timing
Liver transplant represents the only curative treatment for patients with liver cirrhosis.
Bridges to transplantation are used to manage patients who are listed for an organ transplant, acting to temporize whilst on the waiting list. Various approaches can be chosen depending on the patient's underlying medical condition and individual characteristics.
In patients awaiting liver transplant, TIPS placement can be an option to manage complications associated with portal hypertension, in order to reduce morbidity and mortality.
Ascites, hydrothorax, and GI bleeding represent frequent and widely-recognized indications for TIPS placement, based on well-established literature data assessing complications management and mortality as outcomes (9) (10). However, from a transplant perspective, these indications may be expanded and can be considered at an earlier stage. In this scenario, a "TIPS towards transplant" can provide advantages in terms of improving the patient's clinical condition at the time of transplantation and patient’s survival. Furthermore, TIPS procedure can preserve the technical feasibility of the transplant itself.
To better understand this concept, in this review, we aim to explore some liver transplantation settings in which an early evaluation and discussion of TIPS placement can lead to a significant positive clinical outcome (Figure 2).
As known, TIPS can be placed in a bridge-to-transplant setting for patients with end-stage liver disease at high risk of decompensation and, consequently, mortality. A recent meta-analysis based on individual data has shown that, compared to standard therapy, the use of TIPS reduces the incidence of further decompensation events, regardless of the indication, and so, it increases survival in highly selected patients with variceal bleeding and refractory ascites (7). Patients on the liver transplant waiting list are typically individuals with end-stage liver disease, who, frequently, have already experienced multiple episodes of liver decompensation. In the absence of a transplant, the disease tends to progress. Patients may experience further decompensation and lastly death. The concept of “further decompensation” is lately gaining ground as a critical moment in the natural history of cirrhosis, being associated with a worse prognosis compared to the first decompensation (9). As recently demonstrated in a meta-analysis based on individual data evaluating carvedilol in compensated cirrhosis (11) and in a previous study on the clinical course of cirrhosis (12), most deaths occur when episodes of decompensation become recurrent. (Figure 1).
In this context, removing the primary etiological factor of liver disease (e.g., viral infection, alcohol abuse, metabolic alterations) represents the main determinant in reducing the risk of hepatic decompensation (9).
According to a French study published in 2022 (13), the dropout rate due to death or disease worsening in a list of 15,584 patients waiting for liver transplantation, during a 10-year observation time, is approximately 22%. 46,6 % of these patients were listed for HCC. Similar results were obtained from a study on portal vein thrombosis (PVT) (14), showing dropout rates even greater than 20% considering that PVT may also compromise technical feasibility of liver transplantation.
Indeed, PVT is a common event in cirrhosis, with a prevalence ranging from 2% to 26% in liver transplant candidates (15) and is associated with a 62% increase in the risk of mortality compared to cirrhotic patients without PVT (16). PVT is associated with increased mortality also in the post-transplant period (17). A large study conducted in a single center, involving over 3,200 liver transplant candidates, found that those undergoing transplantation with an occlusive PVT had a sevenfold higher risk of mortality at 30 days compared to those without PVT (18). One retrospective study using the Organ Procurement and Transplant Network (OPTN) database, reported that the prevalence of PVT at candidate registration was increased between 2002 and 2014, and that the presence of PVT was associated with an increased waitlist dropout due to illness severity (14).
TIPS placement can be difficult in the setting of PVT or cavernomatosis, even if recent studies suggest that the success rate of the procedure is improving due to new technical approaches (19) (20). In a recent randomized controlled study, the success rate of TIPS placement was very high and, in addition to excellent rebleeding control, TIPS also improved recanalization of the portal vein (21). In a recent systematic review involving 399 patients (92% of whom had cirrhosis), the success rate was approximately 95% (95% confidence interval, CI: 89%–98%), even though there was significant heterogeneity in the group, primarily attributable to the proportion of patients with cavernomatosis (22). To face technical difficulties caused by a complete portal thrombosis or a portal cavernomatosis, alternative techniques have been described, such as transhepatic and trans splenic approach, which achieve almost 100% technical feasibility, allowing many patients who are excluded from transplantation to access it (19) (20).
For these reasons, TIPS, in addition to enabling transplant-listed patients to maintain surgical feasibility at the time of transplantation, would prevent many patients from experiencing rapid clinical deterioration after PVT or death before transplantation. Moreover, TIPS procedure would allow cirrhotic patients who are not on the transplant list yet, to preserve their vascular axis for a potential future need of transplant.
Variceal bleeding represents one of the worst decompensations of liver cirrhosis, with a high rate of mortality after the event. Endoscopic band ligation (EBL) and non-selective beta blockers (NSBB) represent the first step in the management of variceal bleeding, both in primary and secondary prophylaxis. However, there is an estimated 15–21% risk of treatment failure or rebleeding in these patients, causing a rate of mortality as high as 80% (23). In this perspective, TIPS placement in high-risk variceal bleeding patients (pre-emptive TIPS) has been clearly demonstrated superior to the standard medical treatment in improving survival (24) (25) (26) (27). The placement of TIPS on time, reducing mortality and rapid deterioration of liver disease, allows more patients to access liver transplantation opportunities.
Refractory ascites is a common complication of advanced cirrhosis, involving 5-10% of patients (28). Diuretics and repeated large volume paracentesis (LVP) are the first line strategy to manage ascites decompensation. However, as time passes, patients may experience a range of related complications, such as hypotension, acute kidney injury, hepatorenal syndrome, spontaneous bacterial peritonitis.
TIPS placement is an effective therapy for refractory ascites and has been recently proposed also for recurrent ascites, even if results for survival benefits are controversial (29) (30) (31). One meta-analysis analyzed aggregated individual patient data from four randomized controlled trials, revealing that TIPS led to a significant improvement in liver transplant-free (LTF) survival (32). In another study the proportions of liver disease-related deaths were 30% and 40% in the TIPS and in the paracentesis groups, respectively (33) and no significant difference was observed in the numbers of patients who underwent liver transplantation. In a retrospective study, cirrhotic patients who underwent TIPS for refractory ascites were compared to similar patients who underwent serial paracentesis. After adjusting for patient characteristics, TIPS patients showed a trend towards improved survival compared to those who underwent paracentesis, with significant differences in survival rates at 1, 2, and 3 years (34). However, the patient eligible for TIPS should be carefully selected, taking into account the stage of liver disease, which serves as a warning for the high rate of decompensation and death after the procedure, although a retrospective study from 2019 has shown that mortality in these kind of patients (MELD > 18) appears to be independent of the therapeutic strategy (LVP vs. TIPS) (35).
Malnutrition is a common feature of liver cirrhosis and significantly impacts the disease’s prognosis (36) (37) (38) (39). The rate of sarcopenia is directly related to the stage of liver disease (40); for this reason, alterations of nutritional status can significantly impact the prognosis in patients waiting for liver transplantation (41); sarcopenia can sometimes represent a relative contraindication for surgery due to the higher rate of death or complication during and after liver transplantation (40) (42).
A strong interrelation has been reported between TIPS placement and the patient’s nutritional status. From one side, patients with advanced sarcopenia have a worse prognosis after TIPS in terms of hepatic decompensation, acute on-chronic liver failure and survival (43) (44) (45), on the other hand, TIPS placement may improve nutritional status and sometimes can even reverse the condition of sarcopenia (46). Montomoli et al., in a prospective observational study, have investigated the effect of TIPS on malnutrition in portal hypertensive cirrhotic patients and they observed that dry lean mass increased in low or normal weight patients after TIPS placement but did not in overweight patients (47). It is still under debate whether TIPS placement could be anticipated in some patients with complications of portal hypertension, also to prevent advanced malnutrition and sarcopenia (46).
In this context, the placement of a TIPS within a “therapeutic window” may lead to improved nutritional status for the patient and prevent advanced malnutrition from becoming also a risk factor for liver transplant surgery.
Lastly, it’s important to note that liver cirrhosis is a chronic condition characterized by persistent and recurring complications, which significantly contribute to the overall burden of healthcare costs. In this context, TIPS, allowing a reduction in the rate of liver decompensations, a decrease in portal hypertension related complications and by limiting frequent hospitalizations may lead to cost reduction, better management and improvement of the economic impact (48). This consideration could be particularly true if we consider patients with refractory/recurrent ascites who require frequent LVP, access to day hospital or hospitalizations and treatment for further decompensations. This savings would allow a larger amount of resources available for diagnostic and therapeutic needs for patients awaiting liver transplantation.
The choice of the best timing for TIPS placement during the natural history of liver cirrhosis is at present an important topic with no definitive answers. In some patients a multidisciplinary discussion and a team decision could be helpful to take care, accurately, of the complete patient's individual context. It is well known that TIPS placement can also give rise to several adverse effects, including an acceleration of liver failure due to decreased blood supply (49) (50), exacerbation of cardiomyopathy (51) (52), and the occurrence of HE (53) (54), which stands out as the most prevalent clinical complication during the early period following TIPS placement.
Nonetheless, recent evidence indicates that HE is preventable (55) and treatable in the majority of patients and does not impact the patient's long-term prognosis. (56).
A retrospective, single-center study investigated the role of TIPS as a bridge therapy in liver transplant-eligible patients (57). Ninety-eight patients were enrolled, 73 had the TIPS placed before being listed and 25 underwent TIPS procedure while on the waiting list. Both groups were compared to a control group of 60 patients without TIPS. The timing of TIPS placement, before or after being listed, did not impact the survival rate before transplantation. The mortality rate of the patients on the waiting list was reported to have decreased, after TIPS placement was introduced as an option according to clinical indications, compared to historical data reported in the same center. Some patients were even delisted due to clinical improvement after TIPS placement; they showed a similar 5-year overall survival rate compared to those who underwent liver transplantation.
In older times, TIPS was investigated as a potential technique to mitigate intraoperative blood loss during transplantation, thereby positively influencing short-term outcomes. (58) (59) (60) (61). Moreno et al. conducted an extensive comparative longitudinal retrospective study of 875 patients aimed at assessing the short- and long-term outcomes of liver transplantation by comparing individuals with TIPS and those without. The study evaluated various endpoints, including the duration of surgery, cold ischemia time, warm ischemia time, blood product need, postoperative complications (both vascular and non-vascular), length of stay in the Intensive Care Unit (ICU), total hospital stay, retransplantation rates, and 1- and 3-year survival rates. Remarkably, no statistically significant differences were observed between the two groups in any of these parameters (62). Similar conclusions were reported by Dell'Era et al. who found no significant differences between patients with prior TIPS placement and the control group with regard to transfusion requirements, operative time, overall length of hospital stay, ICU length of stay, and complication rates (63).
A subsequent prospective study conducted on a large sample of 591 patients confirmed that the presence of a TIPS had no influence in intra-operative parameters or post-transplant survival up to 5 years (64). Comparing the largest studies on the subject, Barbieri et al. concluded that placement of TIPS before transplantation, had no significant impact on either perioperative parameters or survival at 1 month and 1, 3 and 5 years after liver transplant (65).
In conclusion, TIPS placement is effective in managing complications associated with portal hypertension in cirrhotic patients, and may serve as an excellent tool to potentially prevent deaths while on the waiting list for liver transplantation. TIPS procedure could also play a specific role in restoring portal vein patency in patients under consideration for liver transplant in whom portal thrombosis occurs. Due to the complexity of the decision and the need of taking into account a number of relevant issues when positioning a TIPS in a patient with advanced liver disease waiting for liver transplantation, a multidisciplinary team decision is recommended. There is no impact of having a prior TIPS during the surgical procedure of liver transplantation for duration of surgery, blood product need, postoperative complications, length of stay in the Intensive Care Unit, total hospital stay and re-transplantation rates.
3. TIPS in “Special” Liver Transplant Settings
3.1. Hepatocellular Carcinoma (HCC)
TIPS placement in patients with clinically significant portal hypertension and HCC has proven to be feasible and effective in selected cases (66) (67).
The major safety issues relate to the size of the tumor, the possibility that the nodule location interferes with the trajectory of the stent, and the eventual risk of distant metastasis caused by the procedure (68). Definite answers about these issues are lacking and in the majority of cases the decision will need a team discussion among the radiologist, the hepatologist and the surgeon.
In older times, some studies suggested that TIPS procedure could somehow increase the risk of HCC in cirrhotic patients (69) (70). This finding was supported thanks to the hypothesis that TIPS could lead to vascular alterations, resulting in hypoxia triggers and therefore the development of hepatocellular carcinoma. Further studies, also included in a recent meta-analysis, failed to demonstrate any association between the presence of TIPS and the onset of an HCC (risk ratio: 1.37, (CI): 0.96-1.97; p = 0.08) (71).
Other studies have investigated the safety of transarterial chemoembolization (TACE), radiofrequency ablation (RFTA) and radioembolization in patients with TIPS (72) (73) (74) (75) (76). While these locoregional treatments were feasible, they were utilized in selected patients to provide adequate liver function. Indeed, other studies evidenced an increased risk of hepatotoxicity and hepatic encephalopathy (77) with this combined approach. In addition, Kuo et al.l demonstrated that, although feasible, TACE in patients bearing a TIPS is associated with worse outcomes than in no-TIPS patients, both in terms of safety and efficacy (78). Nevertheless, the 3 years overall survival did not reveal significant differences when uncensored for liver transplant.
In conclusion, locoregional treatment for hepatocellular carcinoma, which is a frequent need in patients in the waiting list for liver transplant, is feasible in patients with TIPS but may further deteriorate liver function. Multidisciplinary decisions with the radiologist, the hepatologist and liver transplant surgeons are recommended.
3.2. Acute-on-Chronic Liver Failure (ACLF)
Acute-on-chronic liver failure (ACLF) is a subtype of acutely decompensated cirrhosis, which is associated with a significantly higher 28-day mortality rate when compared to acutely decompensated cirrhosis without ACLF (more than 20% versus less than 5%) as reported in a study published in Gastroenterology (79). Currently, there is a dearth of studies assessing the impact of TIPS insertion on the disease course when ACLF itself is the indication for TIPS placement. It's worth noting that, despite having a plausible pathophysiological rationale (acting upstream on the pathophysiological pathway - portal hypertension), TIPS insertion is often infeasible in most ACLF patients due to kidney and brain dysfunction. Due to the lack of conclusive evidence supporting TIPS placement in ACLF patients alone, it cannot be recommended as a bridge-to-transplant therapy.
Additionally, two distinct scenarios arise concerning ACLF and variceal bleeding. The first scenario is variceal bleeding as a precipitating factor of ACLF, and the second is variceal bleeding as a complication of ACLF. The management of variceal bleeding outside the context of ACLF is generally accepted and includes consideration of pre-emptive or salvage TIPS procedures (80) (9). The management of patients with variceal bleeding as a complication of ACLF is similar to that of patients without ACLF.
While no studies have specifically examined ACLF patients undergoing elective TIPS procedures to date, numerous studies have explored both preemptive and salvage TIPS placements. Gu et al. have recently published a comprehensive narrative review, highlighting that preemptive TIPS benefits ACLF patients when compared to non-ACLF patients and that salvage TIPS improves one-year mortality rates in patients with ACLF grade 1, albeit not in grades 2 or 3 (81). Based on this emerging evidence, preemptive TIPS may be taken into consideration as a bridge-to-transplant option in cirrhotic patients with ACLF and variceal bleeding.
3.3. Hepatorenal Syndrome
Hepatorenal syndrome (HRS) is a condition characterized by kidney dysfunction in cirrhotic patients, primarily attributed to a reduction in renal blood flow despite the kidneys being histologically normal. HRS can be further classified into two categories: "acute kidney injury" (HRS-AKI) and "non-acute kidney injury" (HRS-NAKI). The conventional approach to managing HRS-AKI involves discontinuing diuretic use and administering albumin infusions in conjunction with vasoactive agents, such as terlipressin. Patients who do not respond to this treatment should be considered for liver transplantation, similar to HRS-NAKI patients.
Numerous retrospective observational studies have indicated that TIPS can ameliorate kidney function. Wong et al. reported that in HRS-AKI patients, TIPS not only initially improved kidney function but also led to the normalization of plasma renin and aldosterone levels, glomerular filtration rate, and urinary sodium excretion 12 months after the procedure (82). Similarly, Testino et al. demonstrated significant improvements in serum creatinine and blood urea nitrogen at 30 days after TIPS insertion in patients with alcoholic hepatitis and HRS-1 (historically known as HRS-AKI) (83). However, both studies may be affected by small sample sizes and lack comparisons to cohorts receiving a standard treatment.
Brensing et al. observed improved kidney function, as evidenced by increased creatinine clearance and sodium excretion, within two weeks following TIPS in patients with HRS (both type I and II) compared to a control group. They also noted enhanced three, six, 12, and 18-month survival rates in TIPS patients (84). Nevertheless, a recent meta-analysis revealed a favorable trend in short-term and one-year survival among HRS patients treated with TIPS. However, the authors acknowledged limitations, including small sample sizes and potential patient selection bias in the underlying studies (85). Consequently, further investigation is needed before recommending TIPS as a bridge-to-transplant option for any type of HRS patient.
In light of this need for additional research, it's worth noting that ongoing work is already underway. Ripoll et al. recently published a study protocol investigating whether TIPS is superior to the standard of care in patients with HRS-AKI (86) (87).
3.4. Cirrhotic Cardiomyopathy
Cirrhotic cardiomyopathy (CCM) is a distinct clinical syndrome in patients with liver cirrhosis, regardless of the underlying etiology. CCM is characterized by systolic and/or diastolic dysfunction resulting from peripheral vasodilation, complicated by hemodynamic derangement and prolonged activation of compensatory mechanisms. However, the pathophysiology is far more complex and beyond the scope of this article; a comprehensive review is reported/can be found in (88). CCM has been reported in 30-70% of patients with liver cirrhosis (89) and may become clinically evident in conditions of rapid and significant hearth overload such as in the first weeks after TIPS placement (90).
Some studies evaluated the short- and medium-term occurrence of cardiac decompensation and mortality following TIPS in patients with previously documented cirrhotic cardiomyopathy. Radunski et al. observed a significant increase in cardiac chamber volumes following TIPS; however, after a median follow-up time of 207 days, no patients experienced cardiac decompensation or heart-related death (91). Fili et al. followed 15 patients with decompensated cirrhosis (33% with diastolic dysfunction) and did not observe any change in cardiac function or any episode of cardiac decompensation one month after TIPS placement (92). On the other hand, Meucci et al., following a mixed cohort of patients (with and without CCM) for a median of 36 months after TIPS , found a higher all-cause mortality rate in patients with higher grades of diastolic dysfunction before the TIPS procedure (93). Similarly, diastolic dysfunction, indicated by a reduced E/A ratio, is associated with reduced ascites clearance and increased mortality post TIPS (94).
Following these observations, also due to the scarcity of data in the setting of TIPS as a bridge-to-transplant, careful caution should be taken with regard to TIPS positioning shortly before liver transplant. In patients with otherwise compensated CCM, TIPS procedure may trigger symptoms of cardiac overload in the short term, therefore suggesting a time lag for cardiac monitoring before surgery takes place. Indeed, current evidence suggests an initial risk of cardiac decompensation following liver transplantation although cardiac function improvement, resulting from a reversal of hyperdynamic circulation during 6–12 months after liver transplantation has been reported (89).
4. Conclusion
TIPS placement in patients with liver cirrhosis is becoming increasingly common in addressing both acute and chronic complications of portal hypertension. The decision of placing a TIPS in a patient in the waiting list for liver transplant should be carefully taken. This procedure may be life-saving in some conditions (GI bleeding) or may even relieve some complications (refractory ascites) facilitating “the patient's journey” to liver transplantation. At the same time these patients due to advanced liver disease may manifest more severe consequences. Therefore, the timing of TIPS placement within a 'therapeutic window' is crucial to maximize benefits without causing adverse events. In the context of liver transplantation, TIPS could potentially prevent certain liver complications that serve as contraindications to transplantation itself, such as advanced malnutrition or complete portal vein thrombosis.
There are currently insufficient studies assessing the impact of TIPS on waitlist mortality and post-transplant survival, and such studies will be necessary in the near future to reach evidence-based recommendations.
However, what we can state regarding the management of portal hypertension complications is that TIPS plays a crucial role with indications that are increasing and expanding. Therefore, patients should be evaluated from this point of view, especially if they are young and have a transplant perspective, with a case by case and multidisciplinary approach.
Author Contributions
Simone Di Cola & Lucia Lapenna: conceptualization, investigation, writing-review & editing. Jakub Gazda, Giulia Cusi, Stefano Fonte, Marco Mattana, investigation, writing original draft. Manuela Merli: supervision and project administration. All authors have read and agreed to the published version of the manuscript.
Funding
All the authors declare that they have not received any funding for this study.
Conflicts of Interest
All authors have none to declare.
References
- https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death.
- D'Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006 Jan;44(1):217-31. [CrossRef]
- D'Amico G, Morabito A, D'Amico M, Pasta L, Malizia G, Rebora P, Valsecchi MG. Clinical states of cirrhosis and competing risks. J Hepatol. 2018 Mar;68(3):563-576. [CrossRef]
- Rudler M, Mallet M, Sultanik P, Bouzbib C, Thabut D. Optimal management of ascites. Liver Int. 2020 Feb;40 Suppl 1:128-135. Erratum in: Liver Int. 2020 May;40(5):1247. [CrossRef]
- Jakab SS, Garcia-Tsao G. Evaluation and Management of Esophageal and Gastric Varices in Patients with Cirrhosis. Clin Liver Dis. 2020 Aug;24(3):335-350. [CrossRef]
- Smith M, Durham J. Evolving Indications for Tips. Tech Vasc Interv Radiol. 2016 Mar;19(1):36-41. [CrossRef]
- Larrue H, D'Amico G, Olivas P, Lv Y, Bucsics T, Rudler M, Sauerbruch T, Hernandez-Gea V, Han G, Reiberger T, Thabut D, Vinel JP, Péron JM, García-Pagán JC, Bureau C. TIPS prevents further decompensation and improves survival in patients with cirrhosis and portal hypertension in an individual patient data meta-analysis. J Hepatol. 2023 Sep;79(3):692-703. [CrossRef]
- Bodzin AS, Baker TB. Liver Transplantation Today: Where We Are Now and Where We Are Going. Liver Transpl. 2018 Oct;24(10):1470-1475. [CrossRef]
- de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C; Baveno VII Faculty. Baveno VII - Renewing consensus in portal hypertension. J Hepatol. 2022 Apr;76(4):959-974. [CrossRef]
- Tripathi D, Stanley AJ, Hayes PC, Travis S, Armstrong MJ, Tsochatzis EA, Rowe IA, Roslund N, Ireland H, Lomax M, Leithead JA, Mehrzad H, Aspinall RJ, McDonagh J, Patch D. Transjugular intrahepatic portosystemic stent-shunt in the management of portal hypertension. Gut. 2020 Jul;69(7):1173-1192. [CrossRef]
- Villanueva C, Torres F, Sarin SK, Shah HA, Tripathi D, Brujats A, Rodrigues SG, Bhardwaj A, Azam Z, Hayes PC, Jindal A, Abid S, Alvarado E, Bosch J; Carvedilol-IPD-MA-group and the Baveno Cooperation: an EASL Consortium. Carvedilol reduces the risk of decompensation and mortality in patients with compensated cirrhosis in a competing-risk meta-analysis. J Hepatol. 2022 Oct;77(4):1014-1025. [CrossRef]
- Sinagra E, Perricone G, D'Amico M, Tinè F, D'Amico G. Systematic review with meta-analysis: the haemodynamic effects of carvedilol compared with propranolol for portal hypertension in cirrhosis. Aliment Pharmacol Ther. 2014 Mar;39(6):557-68. [CrossRef]
- Delacôte C, Favre M, El Amrani M, Ningarhari M, Lemaitre E, Ntandja-Wandji LC, Bauvin P, Boleslawski E, Millet G, Truant S, Mathurin P, Louvet A, Canva V, Lebuffe G, Pruvot FR, Dharancy S, Lassailly G; French ABM study group. Morbid obesity increases death and dropout from the liver transplantation waiting list: A prospective cohort study. United European Gastroenterol J. 2022 May;10(4):396-408. [CrossRef]
- Montenovo M, Rahnemai-Azar A, Reyes J, Perkins J. Clinical Impact and Risk Factors of Portal Vein Thrombosis for Patients on Wait List for Liver Transplant. Exp Clin Transplant. 2018 Apr;16(2):166-171. [CrossRef]
- Ponziani FR, Zocco MA, Senzolo M, Pompili M, Gasbarrini A, Avolio AW. Portal vein thrombosis and liver transplantation: implications for waiting list period, surgical approach, early and late follow-up. Transplant Rev (Orlando). 2014 Apr;28(2):92-101. [CrossRef]
- Stine JG, Shah PM, Cornella SL, Rudnick SR, Ghabril MS, Stukenborg GJ, Northup PG. Portal vein thrombosis, mortality and hepatic decompensation in patients with cirrhosis: A meta-analysis. World J Hepatol. 2015 Nov 28;7(27):2774-80. [CrossRef]
- Ghabril M, Agarwal S, Lacerda M, Chalasani N, Kwo P, Tector AJ. Portal Vein Thrombosis Is a Risk Factor for Poor Early Outcomes After Liver Transplantation: Analysis of Risk Factors and Outcomes for Portal Vein Thrombosis in Waitlisted Patients. Transplantation. 2016 Jan;100(1):126-33. [CrossRef]
- Englesbe MJ, Kubus J, Muhammad W, Sonnenday CJ, Welling T, Punch JD, Lynch RJ, Marrero JA, Pelletier SJ. Portal vein thrombosis and survival in patients with cirrhosis. Liver Transpl. 2010 Jan;16(1):83-90. [CrossRef]
- Thornburg B, Desai K, Hickey R, Kulik L, Ganger D, Baker T, Abecassis M, Lewandowski RJ, Salem R. Portal Vein Recanalization and Transjugular Intrahepatic Portosystemic Shunt Creation for Chronic Portal Vein Thrombosis: Technical Considerations. Tech Vasc Interv Radiol. 2016 Mar;19(1):52-60. [CrossRef]
- Salem R, Vouche M, Baker T, Herrero JI, Caicedo JC, Fryer J, Hickey R, Habib A, Abecassis M, Koller F, Vogelzang R, Desai K, Thornburg B, Hohlastos E, Resnick S, Lewandowski RJ, Sato K, Ryu RK, Ganger D, Kulik L. Pretransplant Portal Vein Recanalization-Transjugular Intrahepatic Portosystemic Shunt in Patients With Complete Obliterative Portal Vein Thrombosis. Transplantation. 2015 Nov;99(11):2347-55. [CrossRef]
- Lapenna L, Di Cola S, Gazda J, De Felice I, Gioia S, Merli M. New Indications for TIPSs: What Do We Know So Far? J Clin Exp Hepatol. 2023 Sep-Oct;13(5):794-803. [CrossRef]
- Rodrigues SG, Sixt S, Abraldes JG, De Gottardi A, Klinger C, Bosch J, Baumgartner I, Berzigotti A. Systematic review with meta-analysis: portal vein recanalisation and transjugular intrahepatic portosystemic shunt for portal vein thrombosis. Aliment Pharmacol Ther. 2019 Jan;49(1):20-30. [CrossRef]
- Asrani SK, Kamath PS. Natural history of cirrhosis. Curr Gastroenterol Rep. 2013 Feb;15(2):308. [CrossRef]
- Monescillo A, Martínez-Lagares F, Ruiz-del-Arbol L, Sierra A, Guevara C, Jiménez E, Marrero JM, Buceta E, Sánchez J, Castellot A, Peñate M, Cruz A, Peña E. Influence of portal hypertension and its early decompression by TIPS placement on the outcome of variceal bleeding. Hepatology. 2004 Oct;40(4):793-801. [CrossRef]
- García-Pagán JC, Caca K, Bureau C, Laleman W, Appenrodt B, Luca A, Abraldes JG, Nevens F, Vinel JP, Mössner J, Bosch J; Early TIPS (Transjugular Intrahepatic Portosystemic Shunt) Cooperative Study Group. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010 Jun 24;362(25):2370-9. [CrossRef]
- Manning C, Elzubeir A, Alam S. The role of pre-emptive Transjugular Intrahepatic Portosystemic Shunt in acute variceal bleeding: a literature review. Ther Adv Chronic Dis. 2021 Mar 5;12:2040622321995771. [CrossRef]
- Hussain I, Wong YJ, Lohan R, Lin S, Kumar R. Does preemptive transjugular intrahepatic portosystemic shunt improve survival after acute variceal bleeding? Systematic review, meta-analysis, and trial sequential analysis of randomized trials. J Gastroenterol Hepatol. 2022 Mar;37(3):455-463. [CrossRef]
- Arroyo V, Colmenero J. Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management. J Hepatol. 2003;38 Suppl 1:S69-89. [CrossRef]
- Ginès P, Uriz J, Calahorra B, Garcia-Tsao G, Kamath PS, Del Arbol LR, Planas R, Bosch J, Arroyo V, Rodés J. Transjugular intrahepatic portosystemic shunting versus paracentesis plus albumin for refractory ascites in cirrhosis. Gastroenterology. 2002 Dec;123(6):1839-47. [CrossRef]
- Narahara Y, Kanazawa H, Fukuda T, Matsushita Y, Harimoto H, Kidokoro H, Katakura T, Atsukawa M, Taki Y, Kimura Y, Nakatsuka K, Sakamoto C. Transjugular intrahepatic portosystemic shunt versus paracentesis plus albumin in patients with refractory ascites who have good hepatic and renal function: a prospective randomized trial. J Gastroenterol. 2011 Jan;46(1):78-85. [CrossRef]
- D'Amico G, Luca A, Morabito A, Miraglia R, D'Amico M. Uncovered transjugular intrahepatic portosystemic shunt for refractory ascites: a meta-analysis. Gastroenterology. 2005 Oct;129(4):1282-93. [CrossRef]
- Salerno F, Cammà C, Enea M, Rössle M, Wong F. Transjugular intrahepatic portosystemic shunt for refractory ascites: a meta-analysis of individual patient data. Gastroenterology. 2007 Sep;133(3):825-34. Erratum in: Gastroenterology. 2007 Nov;133(5):1746. [CrossRef]
- Bai M, Qi XS, Yang ZP, Yang M, Fan DM, Han GH. TIPS improves liver transplantation-free survival in cirrhotic patients with refractory ascites: an updated meta-analysis. World J Gastroenterol. 2014 Mar 14;20(10):2704-14. [CrossRef]
- Gaba RC, Parvinian A, Casadaban LC, Couture PM, Zivin SP, Lakhoo J, Minocha J, Ray CE Jr, Knuttinen MG, Bui JT. Survival benefit of TIPS versus serial paracentesis in patients with refractory ascites: a single institution case-control propensity score analysis. Clin Radiol. 2015 May;70(5):e51-7. [CrossRef]
- Ronald J, Rao R, Choi SS, Kappus M, Martin JG, Sag AA, Pabon-Ramos WM, Suhocki PV, Smith TP, Kim CY. No Increased Mortality After TIPS Compared with Serial Large Volume Paracenteses in Patients with Higher Model for End-Stage Liver Disease Score and Refractory Ascites. Cardiovasc Intervent Radiol. 2019 May;42(5):720-728. [CrossRef]
- Bischoff SC, Bernal W, Dasarathy S, Merli M, Plank LD, Schütz T, Plauth M. ESPEN practical guideline: Clinical nutrition in liver disease. Clin Nutr. 2020 Dec;39(12):3533-3562. [CrossRef]
- European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J Hepatol. 2019 Jan;70(1):172-193. [CrossRef]
- Amodio P, Bemeur C, Butterworth R, Cordoba J, Kato A, Montagnese S, Uribe M, Vilstrup H, Morgan MY. The nutritional management of hepatic encephalopathy in patients with cirrhosis: International Society for Hepatic Encephalopathy and Nitrogen Metabolism Consensus. Hepatology. 2013 Jul;58(1):325-36. [CrossRef]
- Merli M, Giusto M, Molfino A, Bonetto A, Rossi M, Ginanni Corradini S, Baccino FM, Rossi Fanelli F, Costelli P, Muscaritoli M. MuRF-1 and p-GSK3β expression in muscle atrophy of cirrhosis. Liver Int. 2013 May;33(5):714-21. [CrossRef]
- Kim G, Kang SH, Kim MY, Baik SK. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PLoS One. 2017 Oct 24;12(10):e0186990. [CrossRef]
- Lattanzi B, Nardelli S, Pigliacelli A, Di Cola S, Farcomeni A, D'Ambrosio D, Gioia S, Ginanni Corradini S, Lucidi C, Mennini G, Rossi M, Merli M, Riggio O. The additive value of sarcopenia, myosteatosis and hepatic encephalopathy in the predictivity of model for end-stage liver disease. Dig Liver Dis. 2019 Nov;51(11):1508-1512. [CrossRef]
- Merli M, Giusto M, Giannelli V, Lucidi C, Riggio O. Nutritional status and liver transplantation. J Clin Exp Hepatol. 2011 Dec;1(3):190-8. [CrossRef]
- Mangana Del Rio T, Sacleux SC, Vionnet J, Ichaï P, Denys A, Schneider A, Coilly A, Fraga M, Wetzel A, Koerfer J, Chiche JD, Saliba F, Moradpour D, Becce F, Artru F. Body composition and short-term mortality in patients critically ill with acute-on-chronic liver failure. JHEP Rep. 2023 Apr 7;5(8):100758. [CrossRef]
- Nardelli S, Lattanzi B, Torrisi S, Greco F, Farcomeni A, Gioia S, Merli M, Riggio O. Sarcopenia Is Risk Factor for Development of Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt Placement. Clin Gastroenterol Hepatol. 2017 Jun;15(6):934-936. [CrossRef]
- Praktiknjo M, Clees C, Pigliacelli A, Fischer S, Jansen C, Lehmann J, Pohlmann A, Lattanzi B, Krabbe VK, Strassburg CP, Arroyo V, Merli M, Meyer C, Trebicka J. Sarcopenia Is Associated With Development of Acute-on-Chronic Liver Failure in Decompensated Liver Cirrhosis Receiving Transjugular Intrahepatic Portosystemic Shunt. Clin Transl Gastroenterol. 2019 Apr;10(4):e00025. [CrossRef]
- Gazda J, Di Cola S, Lapenna L, Khan S, Merli M. The Impact of Transjugular Intrahepatic Portosystemic Shunt on Nutrition in Liver Cirrhosis Patients: A Systematic Review. Nutrients. 2023 Mar 27;15(7):1617. [CrossRef]
- Montomoli J, Holland-Fischer P, Bianchi G, Grønbaek H, Vilstrup H, Marchesini G, Zoli M. Body composition changes after transjugular intrahepatic portosystemic shunt in patients with cirrhosis. World J Gastroenterol. 2010 Jan 21;16(3):348-53. [CrossRef]
- Bañares R, Albillos A, Nakum M, Gea S, Varghese A, Green W. An Economic Analysis of Transjugular Intrahepatic Portosystemic Covered Stent Shunt for Variceal Bleeding and Refractory Ascites in a Spanish Setting. Adv Ther. 2023 Jul;40(7):3006-3020. [CrossRef]
- Casadaban LC, Parvinian A, Couture PM, Minocha J, Knuttinen MG, Bui JT, Gaba RC. Characterization of liver function parameter alterations after transjugular intrahepatic portosystemic shunt creation and association with early mortality. AJR Am J Roentgenol. 2014 Dec;203(6):1363-70. [CrossRef]
- Vizzutti F, Arena U, Rega L, Zipoli M, Abraldes JG, Romanelli RG, Tarquini R, Laffi G, Pinzani M. Liver failure complicating segmental hepatic ischaemia induced by a PTFE-coated TIPS stent. Gut. 2009 Apr;58(4):582-4. [CrossRef]
- 51. Cazzaniga M, Salerno F, Pagnozzi G, et al. Diastolic dysfunction is associated with poor survival in patients with cirrhosis with transjugular intrahepatic portosystemic shunt. Gut.
- 52. Billey C, Billet S, Robic MA, et al. A prospective study identifying predictive factors of cardiac decompensation after TIPS: the Toulouse algorithm. Hepatology.
- Riggio O, Angeloni S, Salvatori FM, De Santis A, Cerini F, Farcomeni A, Attili AF, Merli M. Incidence, natural history, and risk factors of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt with polytetrafluoroethylene-covered stent grafts. Am J Gastroenterol. 2008 Nov;103(11):2738-46. [CrossRef]
- Riggio O, Nardelli S, Moscucci F, Pasquale C, Ridola L, Merli M. Hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. Clin Liver Dis. 2012 Feb;16(1):133-46. [CrossRef]
- Bureau C, Thabut D, Jezequel C, Archambeaud I, D'Alteroche L, Dharancy S, Borentain P, Oberti F, Plessier A, De Ledinghen V, Ganne-Carrié N, Carbonell N, Rousseau V, Sommet A, Péron JM, Vinel JP. The Use of Rifaximin in the Prevention of Overt Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt : A Randomized Controlled Trial. Ann Intern Med. 2021 May;174(5):633-640. [CrossRef]
- 2023.
- Unger LW, Stork T, Bucsics T, Rasoul-Rockenschaub S, Staufer K, Trauner M, Maschke S, Pawloff M, Soliman T, Reiberger T, Berlakovich GA. The role of TIPS in the management of liver transplant candidates. United European Gastroenterol J. 2017 Dec;5(8):1100-1107. [CrossRef]
- Freeman RB Jr, FitzMaurice SE, Greenfield AE, Halin N, Haug CE, Rohrer RJ. Is the transjugular intrahepatic portocaval shunt procedure beneficial for liver transplant recipients? Transplantation. 1994 Aug 15;58(3):297-300. Erratum in: Transplantation 1994 Nov 27;58(10):1144.
- Menegaux F, Baker E, Keeffe EB, Monge H, Egawa H, Esquivel CO. Impact of transjugular intrahepatic portosystemic shunt on orthotopic liver transplantation. World J Surg. 1994 Nov-Dec;18(6):866-70; discussion 870-1. [CrossRef]
- Martin M, Zajko AB, Orons PD, Dodd G, Wright H, Colangelo J, Tartar R. Transjugular intrahepatic portosystemic shunt in the management of variceal bleeding: indications and clinical results. Surgery. 1993 Oct;114(4):719-26; discussion 726-7.
- Woodle ES, Darcy M, White HM, Perdrizet GA, Vesely TM, Picus D, Hicks M, So SK, Jendrisak MD, McCullough CS, et al. Intrahepatic portosystemic vascular stents: a bridge to hepatic transplantation. Surgery. 1993 Mar;113(3):344-51.
- Moreno A, Meneu JC, Moreno E, Fraile M, García I, Loinaz C, Abradelo M, Jiménez C, Gomez R, García-Sesma A, Manrique A, Gimeno A. Liver transplantation and transjugular intrahepatic portosystemic shunt. Transplant Proc. 2003 Aug;35(5):1869-70. [CrossRef]
- Dell'Era A, Grande L, Barros-Schelotto P, Turnes J, Fuster J, Charco R, García-Valdecasas JC, Bosch J, García-Pagán JC. Impact of prior portosystemic shunt procedures on outcome of liver transplantation. Surgery. 2005 Jun;137(6):620-5. [CrossRef]
- Guerrini GP, Pleguezuelo M, Maimone S, Calvaruso V, Xirouchakis E, Patch D, Rolando N, Davidson B, Rolles K, Burroughs A. Impact of tips preliver transplantation for the outcome posttransplantation. Am J Transplant. 2009 Jan;9(1):192-200. [CrossRef]
- Barbier L, Hardwigsen J, Borentain P, Biance N, Daghfous A, Louis G, Botta-Fridlund D, Le Treut YP. Impact of transjugular intrahepatic portosystemic shunting on liver transplantation: 12-year single-center experience. Clin Res Hepatol Gastroenterol. 2014 Apr;38(2):155-63. [CrossRef]
- Sellers CM, Nezami N, Schilsky ML, Kim HS. Transjugular intrahepatic portosystemic shunt as a bridge to liver transplant: Current state and future directions. Transplant Rev (Orlando). 2019 Apr;33(2):64-71. [CrossRef]
- Balducci D, Montori M, De Blasio F, Di Bucchianico A, Argenziano ME, Baroni GS, Scarpellini E. The Role of Transjugular Intrahepatic Portosystemic Shunt (TIPS) in Treating Portal Hypertension in Patients with Hepatocellular Carcinoma. Medicina (Kaunas). 2023 Jun 15;59(6):1150. [CrossRef]
- Chen, Z.X. , Qiu Z.K., Wang G.B., Wang G.S., Jiang W.W., Gao F. Safety and effectiveness of transjugular intrahepatic portosystemic shunt in hepatocellular carcinoma patients with portal hypertension: A systematic review and meta-analysis. Clin. Radiol. [CrossRef]
- Bjørneboe M, Andersen JR, Christensen U, Skinhøj P, Jensen OM. Does a portal-systemic shunt increase the risk of primary hepatic carcinoma in cirrhosis of the liver? Scand J Gastroenterol. 1985 Jan;20(1):59-64. [CrossRef]
- Bañares R, Núñez O, Escudero M, Fernández C, Vaquero J, Beceiro I, Echenagusía A, Clemente G, Santos L. Patients with cirrhosis and bare-stent TIPS may have increased risk of hepatocellular carcinoma. Hepatology. 2005 Mar;41(3):566-71. [CrossRef]
- Chen, B. , Pang L., Chen HBin Wu D.B., Wang Y.H., Chen E.Q. TIPS Is Not Associated with a Higher Risk of Developing HCC in Cirrhotic Patients: A Systematic Review and Meta-analysis. J. Clin. Transl. Hepatol. [CrossRef]
- Kang, J.W. , Kim J.H., Ko G.Y., Gwon DIl Yoon H.K., Sung K.B. Transarterial chemoembolization for hepatocellular carcinoma after transjugular intrahepatic portosystemic shunt. Acta Radiol. [CrossRef]
- Tesdal IK, Wikström M, Flechtenmacher C, Filser T, Dueber C. Percutaneous treatment of hepatocellular carcinoma in patients with transjugular intrahepatic portosystemic shunts. Cardiovasc Intervent Radiol. 2006 Sep-Oct;29(5):778-84. [CrossRef]
- Wang, Z. , Zhang H., Zhao H., Wang X., Tsauo J., Luo X., Li X. Repeated transcatheter arterial chemoembolization is safe for hepatocellular carcinoma in cirrhotic patients with transjugular intrahepatic portosystemic shunt. Diagn. Interv. Radiol. [CrossRef]
- Donahue LA, Kulik L, Baker T, Ganger DR, Gupta R, Memon K, Abecassis MM, Salem R, Lewandowski RJ. Yttrium-90 radioembolization for the treatment of unresectable hepatocellular carcinoma in patients with transjugular intrahepatic portosystemic shunts. J Vasc Interv Radiol. 2013 Jan;24(1):74-80. [CrossRef]
- Park JK, Al-Tariq QZ, Zaw TM, Raman SS, Lu DS. Radiofrequency Ablation for the Treatment of Hepatocellular Carcinoma in Patients with Transjugular Intrahepatic Portosystemic Shunts. Cardiovasc Intervent Radiol. 2015 Oct;38(5):1211-7. [CrossRef]
- Kohi MP, Fidelman N, Naeger DM, LaBerge JM, Gordon RL, Kerlan RK Jr. Hepatotoxicity after transarterial chemoembolization and transjugular intrahepatic portosystemic shunt: do two rights make a wrong? J Vasc Interv Radiol. 2013 Jan;24(1):68-73. [CrossRef]
- Kuo YC, Kohi MP, Naeger DM, Tong RT, Kolli KP, Taylor AG, Laberge JM, Kerlan RK Jr, Fidelman N. Efficacy of TACE in TIPS patients: comparison of treatment response to chemoembolization for hepatocellular carcinoma in patients with and without a transjugular intrahepatic portosystemic shunt. Cardiovasc Intervent Radiol. 2013 Oct;36(5):1336-43. [CrossRef]
- Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, Durand F, Gustot T, Saliba F, Domenicali M, Gerbes A, Wendon J, Alessandria C, Laleman W, Zeuzem S, Trebicka J, Bernardi M, Arroyo V; CANONIC Study Investigators of the EASL–CLIF Consortium. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013 Jun; 144(7): 1426-37, 1437. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018 Aug;69(2):406-460. Erratum in: J Hepatol. 2018 Nov;69(5):1207. [CrossRef]
- Gu W, Kimmann M, Laleman W, Praktiknjo M, Trebicka J. To TIPS or Not to TIPS in High Risk of Variceal Rebleeding and Acute-on-Chronic Liver Failure. Semin Liver Dis. 2023 May;43(2):189-205. [CrossRef]
- Wong F, Pantea L, Sniderman K. Midodrine, octreotide, albumin, and TIPS in selected patients with cirrhosis and type 1 hepatorenal syndrome. Hepatology. 2004 Jul;40(1):55-64. [CrossRef]
- Testino G, Leone S, Ferro C, Borro P. Severe acute alcoholic hepatitis and hepatorenal syndrome: role of transjugular intrahepatic portosystemic stent shunt. J Med Life. 2012 Jun 12;5(2):203-5. Epub 2012 Jun 18.
- Brensing KA, Textor J, Perz J, Schiedermaier P, Raab P, Strunk H, Klehr HU, Kramer HJ, Spengler U, Schild H, Sauerbruch T. Long term outcome after transjugular intrahepatic portosystemic stent-shunt in non-transplant cirrhotics with hepatorenal syndrome: a phase II study. Gut. 2000 Aug;47(2):288-95. [CrossRef]
- Song T, Rössle M, He F, Liu F, Guo X, Qi X. Transjugular intrahepatic portosystemic shunt for hepatorenal syndrome: A systematic review and meta-analysis. Dig Liver Dis. 2018 Apr;50(4):323-330. [CrossRef]
- Ripoll C, Platzer S, Franken P, Aschenbach R, Wienke A, Schuhmacher U, Teichgräber U, Stallmach A, Steighardt J, Zipprich A; Liver-HERO Study Group. Liver-HERO: hepatorenal syndrome-acute kidney injury (HRS-AKI) treatment with transjugular intrahepatic portosystemic shunt in patients with cirrhosis-a randomized controlled trial. Trials. 2023 Apr 5;24(1):258. [CrossRef]
- Ripoll C, Platzer S, Franken P, Aschenbach R, Wienke A, Schuhmacher U, Teichgräber U, Stallmach A, Steighardt J, Zipprich A; Liver-HERO Study Group. Liver-HERO: hepatorenal syndrome-acute kidney injury (HRS-AKI) treatment with transjugular intrahepatic portosystemic shunt in patients with cirrhosis-a randomized controlled trial. Trials. 2023 Apr 5;24(1):258. [CrossRef]
- Kaur H, Premkumar M. Diagnosis and Management of Cirrhotic Cardiomyopathy. J Clin Exp Hepatol. 2022 Jan-Feb;12(1):186-199. [CrossRef]
- Premkumar M, Devurgowda D, Vyas T, Shasthry SM, Khumuckham JS, Goyal R, Thomas SS, Kumar G. Left Ventricular Diastolic Dysfunction is Associated with Renal Dysfunction, Poor Survival and Low Health Related Quality of Life in Cirrhosis. J Clin Exp Hepatol. 2019 May-Jun;9(3):324-333. [CrossRef]
- Merli M, Valeriano V, Funaro S, Attili AF, Masini A, Efrati C, De CS, Riggio O. Modifications of cardiac function in cirrhotic patients treated with transjugular intrahepatic portosystemic shunt (TIPS). Am J Gastroenterol. 2002 Jan;97(1):142-8. [CrossRef]
- Radunski UK, Kluwe J, Klein M, Galante A, Lund GK, Sinning C, Bohnen S, Tahir E, Starekova J, Bannas P, Stehning C, Adam G, Lohse AW, Blankenberg S, Muellerleile K, Benten D. Cardiovascular magnetic resonance demonstrates structural cardiac changes following transjugular intrahepatic portosystemic shunt. Sci Rep. 2021 Jun 16;11(1):12719. [CrossRef]
- Filì D, Falletta C, Luca A, Hernandez Baravoglia C, Clemenza F, Miraglia R, Scardulla C, Tuzzolino F, Vizzini G, Gridelli B, Bosch J. Circulatory response to volume expansion and transjugular intrahepatic portosystemic shunt in refractory ascites: Relationship with diastolic dysfunction. Dig Liver Dis. 2015 Dec;47(12):1052-8. [CrossRef]
- Meucci MC, Hoogerduijn Strating MM, Butcher SC, van Rijswijk CSP, Van Hoek B, Delgado V, Bax JJ, Tushuizen ME, Marsan NA. Left atrial dysfunction is an independent predictor of mortality in patients with cirrhosis treated by transjugular intrahepatic portosystemic shunt. Hepatol Commun. 2022 Nov;6(11):3163-3174. [CrossRef]
- Rabie RN, Cazzaniga M, Salerno F, Wong F. The use of E/A ratio as a predictor of outcome in cirrhotic patients treated with transjugular intrahepatic portosystemic shunt. Am J Gastroenterol. 2009 Oct;104(10):2458-66. Erratum in: Am J Gastroenterol. 2009 Aug;104(8):2128. [CrossRef]
Figure 1.
Possible scenarios after second decompensation in patients with liver cirrhosis treated with medical therapy versus TIPS placement with a view to transplantation. Red arrows indicate possible causes of dropout. Patients with decompensated liver cirrhosis who undergo medical or endoscopic therapy may experience clinical improvement, but the natural history of the disease may progress to further deterioration and need transplantation. Patients with TIPS can often develop hepatic encephalopathy, which is frequently transient, and seldom ACLF or cardiac deterioration. Some patients after TIPS may correct portal thrombosis making liver transplant more feasible. TIPS by improving portal hypertension-related complications may increase transplant free survival. HE, Hepatic encephalopathy; TIPS, Transjugular intrahepatic portosystemic shunt, PH, Portal Hypertension; ACLF, Acute on Chronic Liver Failure; PV, Portal Vein.
Figure 1.
Possible scenarios after second decompensation in patients with liver cirrhosis treated with medical therapy versus TIPS placement with a view to transplantation. Red arrows indicate possible causes of dropout. Patients with decompensated liver cirrhosis who undergo medical or endoscopic therapy may experience clinical improvement, but the natural history of the disease may progress to further deterioration and need transplantation. Patients with TIPS can often develop hepatic encephalopathy, which is frequently transient, and seldom ACLF or cardiac deterioration. Some patients after TIPS may correct portal thrombosis making liver transplant more feasible. TIPS by improving portal hypertension-related complications may increase transplant free survival. HE, Hepatic encephalopathy; TIPS, Transjugular intrahepatic portosystemic shunt, PH, Portal Hypertension; ACLF, Acute on Chronic Liver Failure; PV, Portal Vein.
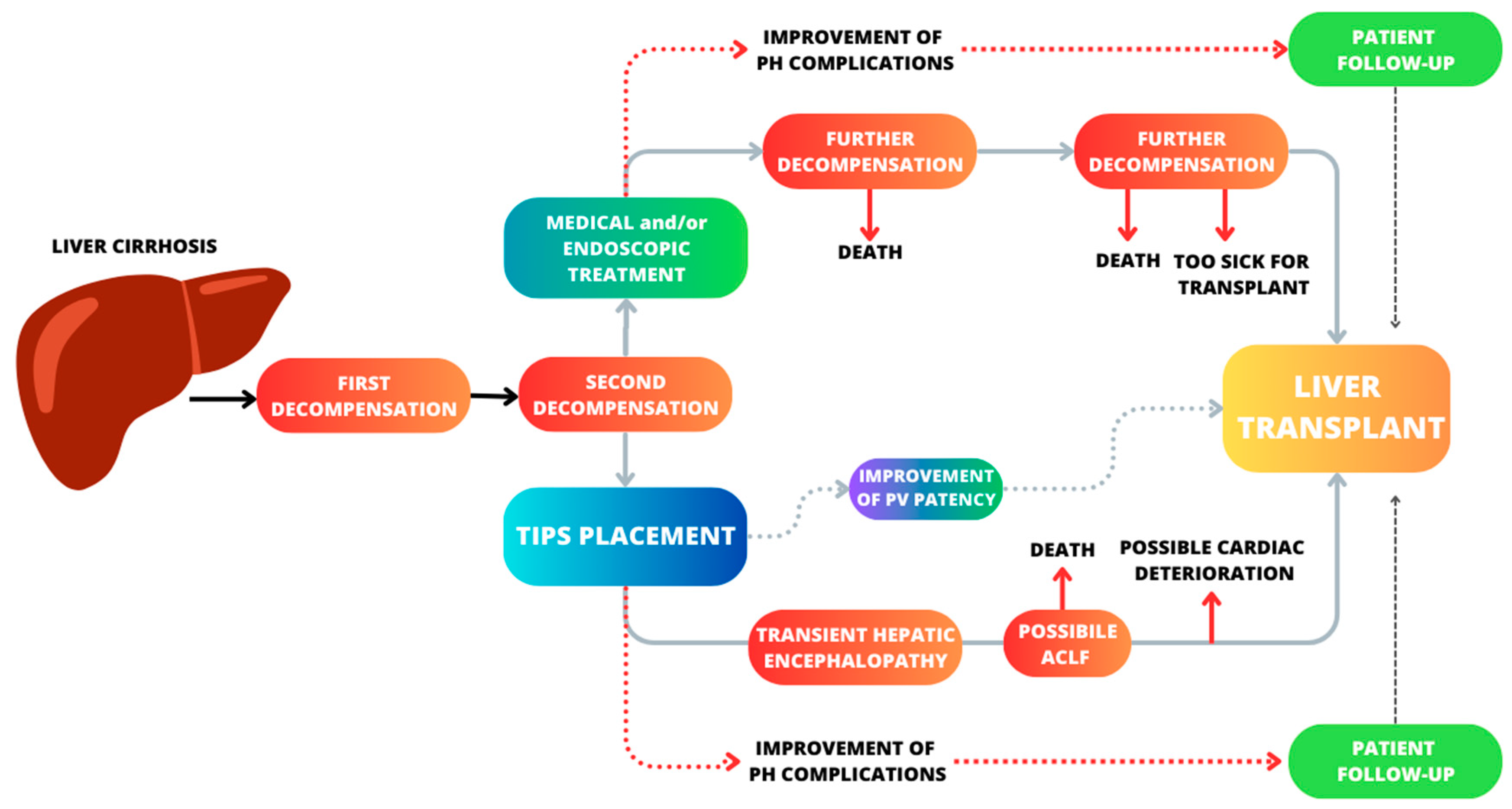
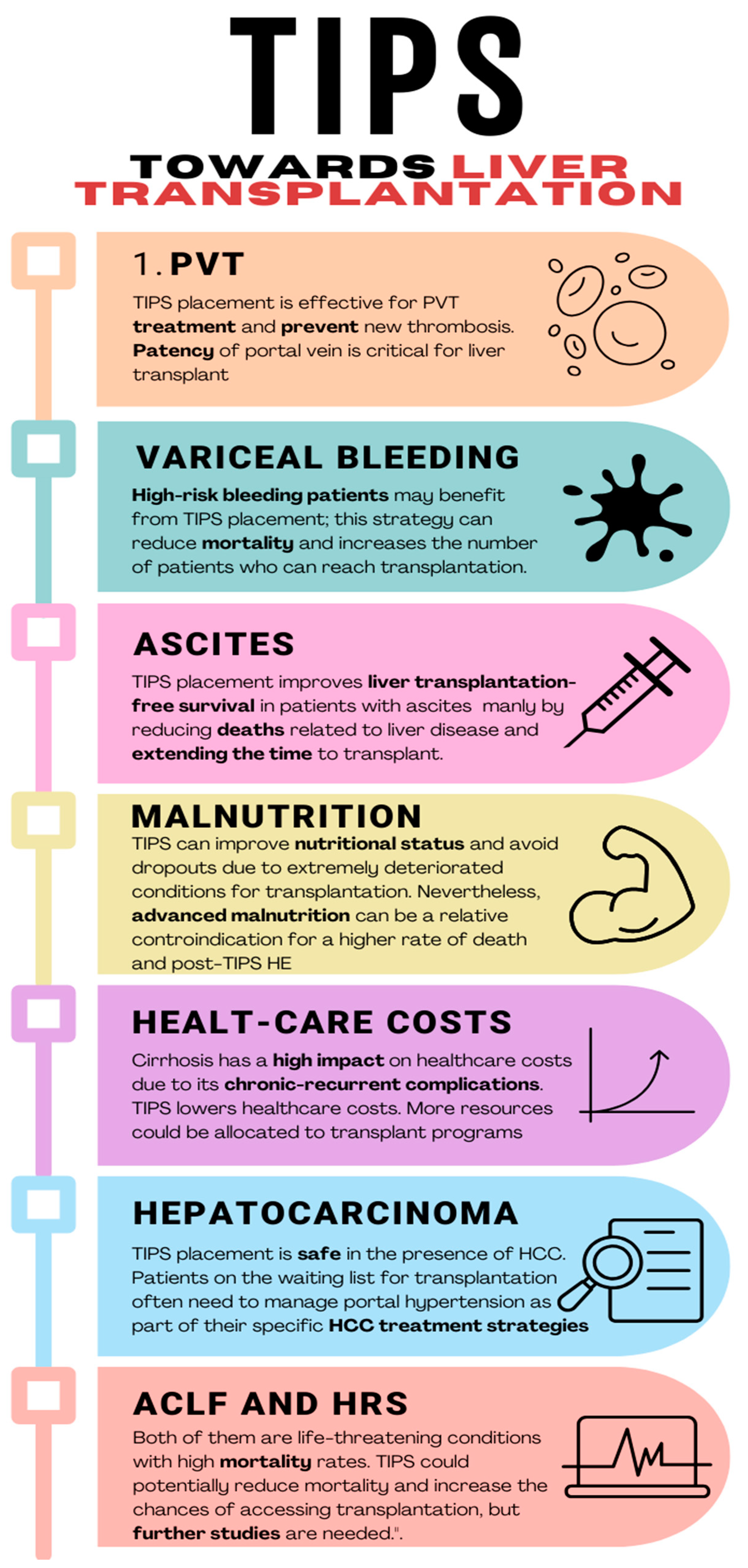
Figure 2.
Different settings in which TIPS placement plays a fundamental role in the route to transplantation. PVT, Portal Vein Thrombosis; HCC, Hepatocarcinoma; ACLF, Acute on Chronic Liver Failure; HRS, HepatoRenal Syndrome; HE, Hepatic Encephalopathy.
Figure 2.
Different settings in which TIPS placement plays a fundamental role in the route to transplantation. PVT, Portal Vein Thrombosis; HCC, Hepatocarcinoma; ACLF, Acute on Chronic Liver Failure; HRS, HepatoRenal Syndrome; HE, Hepatic Encephalopathy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



