
Submitted:
12 October 2023
Posted:
13 October 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction and Aims: COVID-19-associated invasive pulmonary aspergillosis (CAPA) is common and is associated with poor outcomes in critically ill patients. This prospective observational study aimed to explore the association between CAPA development and the incidence and prognosis of cytomegalovirus (CMV) reactivation in critically ill COVID-19 patients.
Materials and Methods: We included all consecutive critically ill adult patients with confirmed COVID-19 infection who were admitted to three COVID-19 intensive care units (ICUs) in an Italian hospital from February 25, 2020, to May 8, 2022. A standardized procedure was employed for early detection of CAPA. Risk factors associated with CAPA and CMV reactivation and the association between CMV recurrence and mortality were estimated using adjusted Cox proportional hazard regression models.
Results: CAPA occurred in 96 patients (16,6%) of the 579 patients analyzed. Among the CAPA population 40 (41,7%) patients developed CMV blood reactivation with a median time of 18 days (IQR 7-27). The CAPA+CMV group did not exhibit a significantly higher 90-day mortality rate (62.5% vs. 48.2%) than the CAPA alone group (p=0.166). The CAPA+CMV group had a longer ICU stay, fewer ventilation-free days, and a higher rate of secondary bacterial infections than the control group of CAPA alone. In the CAPA population, prior immunosuppression was the only independent risk factor for CMV reactivation (HR 2.33, 95% C.I. 1.21-4.48, p=0.011).
Conclusions: In critically ill COVID-19 patients, CMV reactivation is common in those with a previous CAPA diagnosis. Basal immunosuppression before COVID-19 appeared to be the primary independent variable affecting CMV reactivation in patients with CAPA. Furthermore, the association of CAPA+CMV versus CAPA alone appears to impact ICU length of stay and secondary bacterial infections but not mortality.
Keywords:
COVID-19
; invasive pulmonary aspergillosis
; critically ill
; cytomegalovirus
; ards
1. Introduction
Invasive pulmonary aspergillosis (IPA) primarily affects immunocompromised patients, including those with severe and prolonged neutropenia, hematological malignancies, organ transplant recipients, and individuals with structural lung damage receiving systemic corticosteroids [1]. In the last few decades, several cases of IPA have been described in ICU patients hospitalized for influenza pneumonia among critically ill patients without immunosuppression, and severe influenza is now recognized as a risk factor for IPA [2]. Recently, severe COVID-19 pneumonia has emerged as a risk factor, leading to the recognition of COVID-19-associated pulmonary aspergillosis (CAPA) as a significant complication among critically ill COVID-19 patients [3]. Approximately 10–20% of ICU-admitted COVID-19 patients eventually develop CAPA [4,5], which is associated with high mortality rates [5].
The relationship between cytomegalovirus (CMV) and IPA is well established in immunocompromised individuals [6] but has been less explored in critically ill patients [7], especially those with COVID-19 [8].
This observational study aimed to describe the link between CMV replication and CAPA occurrence in COVID-19 patients admitted to our ICUs.
2. Materials and Methods
This observational study analysed prospectively collected data from all consecutive adult patients admitted to the three COVID-19 ICUs at the University Hospital of Modena with confirmed SARS-CoV-2 infection and moderate to severe acute respiratory distress syndrome (ARDS) from February 25th, 2020, to May 08th, 2022 [9]. Patients who were aged < 18 years, had an ICU length of stay (LOS) < 24 h, limitation of care, or lack of resuscitate order were excluded from the analysis. This study was approved by the Institutional Ethics Committee of Area Vasta Emilia Nord (approval number:396/2020/OSS/AOUMO—CoV-2 MO-Study). Owing to the observational nature of this study, written informed consent was not required.
2.1. Treatment protocol
All patients received standard ICU and supportive care, as recommended by the World Health Organization (WHO) guidelines [10], specific therapies according to national guidelines [11], and local protocols for COVID-19 treatment, including dexamethasone and low-molecular weight heparin for prophylaxis of deep vein thrombosis according to individual body weight and renal function. In addition, the local protocol allowed the use of steroids (methylprednisolone 2 mg/kg/day) to prevent the onset of pulmonary fibrosis in patients who maintained a PaO2/FiO2 ratio < 150 mmHg for at least 7 days of mechanical ventilation [12]. Since March 2020, the local management protocol has included tocilizumab for patients with moderate or severe ARDS and the need for mechanical ventilation (noninvasive or invasive). From the end of March 2020, all patients who received tocilizumab or high-dose steroids received standard acyclovir prophylaxis. Starting in late April 2021, remdesivir was administered to ICU patients with a disease history or onset of symptoms of less than seven days, based on the dosage of SARS-CoV2 viremia. Selective digestive decontamination (SDD) has been introduced in the structured protocol for VAP prevention since the end of April 2021. SDD consisted of tobramycin sulfate, colistin sulfate, and amphotericin B suspension applied to the patient’s oropharynx and stomach via a nasogastric tube. Standard supportive management in the ICU did not significantly change during the study period.
2.2. Data collection
Patient demographics, Sequential Organ Failure Assessment (SOFA) score, Simplified Acute Physiology Score II (SAPS II), and standard laboratory results, including coagulation and inflammatory variables, were collected at ICU admission. In addition, the need for invasive mechanical ventilation, therapy with steroids, tocilizumab (also before ICU admission), Ganciclovir, the CMV blood reactivation, and the occurrence of new bacterial infections were collected during ICU stay. Regarding the ICU protocol, patients were screened on ICU admission and twice (in invasive mechanically ventilated patients) or once per week for bacterial colonization in the rectum, respiratory tract (if tracheal intubation was performed), urinary tract, and quantitative CMV DNAemia in the blood.
2.3. CAPA definition
Criteria for “Probable CAPA” were as follows: patient admitted to the ICU with laboratory confirmed SARS-CoV-2 infection presenting a positive Aspergillus culture in bronchoalveolar lavage (BAL) or serum galactomannan (GM) Optical Density Index (ODI) > 0.5 or BAL GM ODI >=1 [13,14,15,16]. These findings were considered alongside concomitant clinical and radiological signs, consistent with the definition of probable CAPA. Each patient included in the study underwent IPA screening using various methods. This screening involved monitoring serum and BAL GM, assessing Aspergillus growth in BAL cultures, measuring serum beta-d-glucan levels, and reviewing radiological images (chest CT). GM testing was performed on the serum and BAL samples obtained by deep tracheal aspiration using a closed aspiration system from the lower respiratory tract. Polymerase chain reaction (PCR) testing for Aspergillus spp. in the serum or BAL was conducted only in cases where there was significant doubt regarding IPA or when BAL GM was positive. Biomarkers were typically measured at ICU admission and then every 4-5 days. BAL-GM testing was primarily performed in the intubated patients. For each patient, the most relevant values of respiratory or serum GM and serum β-d-glucan were identified and reported, and a positive Aspergillus spp. culture in BAL or tracheal aspirate and a positive PCR test for Aspergillus spp. in serum or BAL were assessed. Patients undergoing treatment for IPA were identified, and the type of treatment was defined according to CAPA recommendations [15]. The first-line treatment was voriconazole at a loading dose of 6 mg/kg twice daily for two doses, followed by 4 mg/kg twice daily. As recommended, patients with CAPA underwent therapeutic monitoring of the drug once or twice weekly in cases of fully sensitive Aspergillus spp., specifically voriconazole [15]. Secondary infections were defined in line with international guidelines [17,18] and categorized as hospital-acquired pneumonia (HAP), including ventilator-associated pneumonia (VAP) and bloodstream infection (BSI). All microbiological samples were analyzed at the local microbiological and virology laboratory.
2.4. Data analysis
After initially describing the entire population, we focused on the subpopulation that developed CAPA and divided these patients into two groups: those who developed CMV blood reactivation during their ICU stay and those who did not. Categorical variables are expressed as absolute numbers and percentages, and continuous variables are expressed as medians and interquartile ranges (IQR). For comparison, the Chi-squared or Fisher’s exact test was performed for categorical variables, and the Mann-Whitney U-test was used for continuous variables. The independent association between different variables and in-hospital mortality censored at day 90 was estimated using a multivariable Cox proportional hazards regression model, including all variables associated with a p-value <0.2 in the unadjusted analysis, and forcing the variable considered relevant in the model. Patients discharged from the hospital before day 90 were considered to have survived. Kaplan Meier curves were performed to estimate the crude association between CMV blood reactivation and 90-day mortality in subpopulation of patients developing CAPA. SPSS (version 22.0; SPSS Inc., Chicago, IL, USA) was used to perform statistical analyses.
3. Results
In total, 579 patients were included in the analysis. Of these, 96 (16.6%) patients developed CAPA, whereas the remaining 483 did not. Demographic and baseline characteristics of the included patients, as well as comparisons between those who developed CAPA and those who did not, are presented in Table 1. Patients who developed CAPA exhibited significantly higher severity scores and lower lymphocyte counts at ICU admission than controls. The use of steroid therapy and tocilizumab was similar between the two groups. A significantly higher proportion of patients who developed CAPA underwent SDD during their ICU stay. Furthermore, 87.5% of patients with CAPA required invasive mechanical ventilation (IMV) (p<0.001).
We then conducted an analysis comparing patients with CMV blood reactivation during the ICU stay to those without CMV reactivation in the CAPA population (n=96). Of the 96 patients with CAPA, 40 (41,7%) developed CMV reactivation. The median time from ICU admission to CMV reactivation was 18 days (IQR 7-27), with higher peaks of CMV DNA load in the CAPA population than in patients without CAPA (Table S1). The baseline characteristics and main interventions in the comparison of patients with and without CMV blood reactivation were similar and are shown in Table 2. Notably, patients with CAPA who developed CMV blood reactivation had a significantly higher rate (97.5%) of IMV (p=0.012).
The 90-day mortality rates were 62,5% in the CAPA+CMV group and 48,2% in the CAPA and no CMV group (p=0,166) (Table 3). A longer ICU LOS was observed in the CAPA+CMV group (p<0.001). In the CAPA+CMV group 77.5% of patients developed secondary bacterial infection during their ICU stay, compared to 53.6% of patients in the CAPA and no CMV group (p=0.016) (Table 3). The median time to secondary infection occurrence in CAPA population was 11 days (IQR 6-17). The CAPA+CMV group had lower ventilation-free days compared to CAPA and no CMV group (p=0.020). Moreover, CMV reactivation occurred more frequently in patients who developed CAPA later during ICU stay (median 9,5 days vs 2 days, p<0,001). Kaplan Meier curves demonstrated no difference in cumulative survival between CAPA population with or without CMV reactivation (Long Rank=0,335) (Figure 1).
The Cox regression multivariate analysis for the comparison of CAPA patients with or without CMV blood reactivation at day 90 indicated that only a previous history of immunosuppression increased the risk of CMV blood reactivation, censored at day 90 (HR 2.33, 95% C.I. 1,21-4,48, p=0.011). The use of immunotherapy did not correlate with the adjusted risk of CMV reactivation in the CAPA population (p=0.951) (Table 4).
4. Discussion
Our large, single-center observational study investigated the incidence of CAPA in critically ill patients admitted to the ICU during a four-wave period of COVID-19 and established an association between this condition and CMV reactivation. In the initial analysis, critically ill patients who developed CAPA tended to be older and presented with more severe illness upon ICU admission. SDD was administered more frequently to patients with CAPA, although it was used in less than 15% of the entire cohort. Within the CAPA population, we conducted a sub-study to compare patients with and without CMV reactivation. To date, this is the largest study investigating this association, and it adds to the understanding of the relationship between CAPA and CMV reactivation in critically ill COVID-19 patients.
CMV and IPA in immunocompromised hosts have been well-described [19,20]. However, there is limited knowledge about how these infections interact in critically ill patients, and even less is known about their association with COVID-19 [8]. Similarly, in a retrospective case-control study by Calderón-Parra et al. [8], CMV reactivation was much more frequent in patients with CAPA than in those without CAPA, with an incidence difference of >25%. However, a discordant point with respect to the aforementioned study [8] is the onset time of CMV replication. In the Calderón-Parra study [8], 9 out of 11 patients developed viral replication before the onset of CAPA; in contrast, our data revealed that CMV typically reactivated later, with a median time from ICU admission of 18 days compared to a median of 5.5 days for the onset of CAPA (as shown in Table S1). This difference in timing raises questions regarding the chronological relationship between CMV and CAPA in COVID-19 patients. The exact pathophysiological mechanisms underlying the interplay between CMV and CAPA in COVID-19 patients remain unclear. Although our data suggest that CAPA tends to occur before CMV reactivation in our cohort, further research is needed to understand the temporal and causal relationships between these two infections. Additionally, it is important to consider that the dynamics of infections can vary among individuals and that the timing of infection events may not be consistent across all patients.
In terms of ICU and 90-days mortality, no differences were detected between patients with CAPA+CMV and CAPA-noCMV, as highlighted by Calderon et al. [8] (Table 3). The role of CMV reactivation in critically ill patients is highly debated, and we have already discussed this argument in COVID-19 patients [21].
The main finding of this study is the multivariate Cox regression analysis of the factors independently associated with the development of CMV blood replication in patients with CAPA. Pre-COVID immunosuppression appeared to be independently associated with CMV reactivation in the blood (HR 2.33 [1.21-4.48] ). Therefore, neither anti-cytokine immunological therapies nor the severity of COVID-19, as expressed by IMV and secondary bacterial infections, seem to play a role. During the COVID-19 waves, a discussion arose about whether the therapies to counteract the cytokine storm, when added to the immune dysfunction probably induced by SARS-CoV-2 infection, could further deteriorate the immunocompetence of COVID-19 patients [22,23]. This is particularly relevant for patients who develop CAPA, which promotes viral reactivation. However, our data does not support this hypothesis. Our data underscore once again that basal immunosuppression is the key point that plays a major role [6], this finding argues for the chance of performing prophylaxis against the development of CMV in patients with basal immunosuppression.
The strengths of our study are as follows: (a) the systematic protocol implemented to identify CAPA and CMV in patients with COVID-19 admitted to the ICU, and (b) the large number of patients analyzed and the prospective methodology of the observations. However, there are several weaknesses and concerns to consider: (a) the data from three different ICUs still come from a single hospital, so we do not know if the results can be applied to other clinical settings; and (b) the protocol for CAPA detection did not include systematic PCR testing for Aspergillus spp. in serum or BAL, which was performed only in cases of strong doubt regarding IPA, which may have underestimated the sample of CAPA.
5. Conclusions
In critically ill COVID-19 patients, CMV reactivation is common in those with a previous CAPA diagnosis. Basal immunosuppression before COVID-19 appeared to be the primary independent variable affecting CMV reactivation in patients with CAPA. Furthermore, the association of CAPA+CMV versus CAPA alone appears to impact ICU length of stay and secondary bacterial infections but not mortality.
Funding
No funds.
Availability of data and material
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The members of Modena COVID-19 Working Group (MoCo19) are: Stefano Busani, Massimo Girardis, Alberto Andreotti, Emanuela Biagioni, Filippo Bondi, Giovanni Chierego, Marzia Scotti, Lucia Serio, Annamaria Ghirardini, Marco Sita, Stefano De Julis, Lara Donno, Lorenzo Dall’Ara, Fabrizio Di Salvo, Carlotta Farinelli, Laura Rinaldi, Ilaria Cavazzuti, Andrea Ghidoni, Antonio Buono, Elena Ferrari, Daniela Iseppi, Anna Maria Ardito, Irene Coloretti, Sophie Venturelli, Elena Munari, Martina Tosi, Erika Roat, Ilenia Gatto, Marco Sarti, Andrea Cossarizza, Caterina Bellinazzi, Rebecca Borella, Sara De Biasi, Anna De Gaetano, Lucia Fidanza, Lara Gibellini, Anna Iannone, Domenico Lo Tartaro, Marco Mattioli, Milena Nasi, Annamaria Paolini, Marcello Pinti, Cristina Mussini, Giovanni Guaraldi, Marianna Meschiari, Alessandro Cozzi-Lepri, Jovana Milic, Marianna Menozzi, Erica Franceschini, Gianluca Cuomo, Gabriella Orlando, Vanni Borghi, Antonella Santoro, Margherita Di Gaetano, Cinzia Puzzolante, Federica Carli, Andrea Bedini, Luca Corradi, Enrico Clini, Roberto Tonelli, Riccardo Fantini, Alessandro Marchioni, Ivana Castaniere, Luca Tabbì, Giulia Bruzzi, Chiara Nani, Fabiana Trentacosti, Pierluigi Donatelli, Maria Rosaria Pellegrino, Linda Manicardi, Antonio Moretti, Morgana Vermi, Caterina Cerbone, Monica Pecorari, William Gennari, Antonella Grottola, Giulia Fregni Serpini.
Declaration of Competing Interests
The authors declare no conflicts of interest.
References
- Brown, G.D.; Denning, D.W.; Gow, N.A.R.; Levitz, S.M.; Netea, M.G.; White, T.C. Hidden Killers: Human Fungal Infections. Sci. Transl. Med. 2012, 4, 165rv13. [Google Scholar] [CrossRef]
- Schauwvlieghe, A.F.A.D.; Rijnders, B.J.A.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van De Veerdonk, F.L.; Gommers, D.; et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: A retrospective cohort study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. COVID-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef]
- Dimopoulos, G.; Almyroudi, M.-P.; Myrianthefs, P.; Rello, J. COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Intensiv. Med. 2021, 1, 71–80. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Mikulska, M.; Raiola, A.M.; Bruno, B.; Furfaro, E.; Van Lint, M.T.; Bregante, S.; Ibatici, A.; Del Bono, V.; Bacigalupo, A.; Viscoli, C. Risk factors for invasive aspergillosis and related mortality in recipients of allogeneic SCT from alternative donors: An analysis of 306 patients. Bone Marrow Transplant. 2009, 44, 361–370. [Google Scholar] [CrossRef]
- Verweij, P.E.; Rijnders, B.J.A.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.J.; Cornely, O.A.; Chiller, T.; et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: An expert opinion. Intensive Care Med. 2020, 46, 1524–1535. [Google Scholar] [CrossRef]
- Calderón-Parra, J.; Moreno-Torres, V.; Mills-Sanchez, P.; Tejado-Bravo, S.; Romero-Sánchez, I.; Balandin-Moreno, B.; Calvo-Salvador, M.; Portero-Azorín, F.; García-Masedo, S.; Muñez-Rubio, E.; et al. Association of COVID-19-Associated Pulmonary Aspergillosis with Cytomegalovirus Replication: A Case–Control Study. J. Fungi 2022, 8, 161. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- World Health Organization. COVID-19 Clinical Management: Living Guidance. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 14 June 2021).
- Mussini, C.; Falcone, M.; Nozza, S.; Sagnelli, C.; Parrella, R.; Meschiari, M.; Petrosillo, N.; Mastroianni, C.; Cascio, A.; Iaria, C.; et al. Therapeutic strategies for severe COVID-19: A position paper from the Italian Society of Infectious and Tropical Diseases (SIMIT). Clin. Microbiol. Infect. 2020, 27, 389–395. [Google Scholar] [CrossRef]
- Steinberg, K.P.; Hudson, L.D.; Goodman, R.B.; Lee Hough, C.; Lanken, P.N.; Hyzy, R.; Thompson, B.T.; Ancukiewicz, M. Efficacy and Safety of Corticosteroids for Persistent Acute Respiratory Distress Syndrome. New Engl. J. Med. 2006, 354, 1671–1684. [Google Scholar] [PubMed]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. A National Strategy to Diagnose Coronavirus Disease 2019–Associated Invasive Fungal Disease in the Intensive Care Unit. Clin. Infect. Dis. 2020, 73, e1634–e1644. [Google Scholar] [CrossRef] [PubMed]
- Van Biesen, S.; Kwa, D.; Bosman, R.J.; Juffermans, N.P. Detection of Invasive Pulmonary Aspergillosis in COVID-19 with Nondirected BAL. Am. J. Respir. Crit. Care Med. 2020, 208, 1171–1173. [Google Scholar] [CrossRef]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of invasive pulmonary aspergillosis among COVID-19 intubated patients: A prospective study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, E3606–14. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef]
- Manian, F.A. IDSA Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Bloodstream Infection. Clin. Infect. Dis. 2009, 49, 1770–1771. [Google Scholar] [CrossRef] [PubMed]
- Chuleerarux, N.; Thongkam, A.; Manothummetha, K.; Nematollahi, S.; Dioverti-Prono, V.; Torvorapanit, P.; Langsiri, N.; Worasilchai, N.; Plongla, R.; Chindamporn, A.; et al. Does Post-Transplant Cytomegalovirus Increase the Risk of Invasive Aspergillosis in Solid Organ Transplant Recipients? A Systematic Review and Meta-Analysis. J. Fungi 2021, 7, 327. [Google Scholar] [CrossRef]
- Kuo, C.-W.; Wang, S.-Y.; Tsai, H.-P.; Su, P.-L.; Cia, C.-T.; Lai, C.-H.; Chen, C.-W.; Shieh, C.-C.; Lin, S.-H. Invasive pulmonary aspergillosis is associated with cytomegalovirus viremia in critically ill patients—A retrospective cohort study. J. Microbiol. Immunol. Infect. 2021, 55, 291–299. [Google Scholar] [CrossRef]
- Gatto, I.; Biagioni, E.; Coloretti, I.; Farinelli, C.; Avoni, C.; Caciagli, V.; Busani, S.; Pecorari, M.; Gennari, W.; Guaraldi, G.; et al. Cytomegalovirus blood reactivation in COVID-19 critically ill patients: Risk factors and impact on mortality. Intensiv. Care Med. 2022, 48, 706–713. [Google Scholar] [CrossRef]
- Moore, J.; Stroever, S.; Rondain, P.; Scatena, R. Incidence of secondary bacterial infections following utilization of tocilizumab for the treatment of COVID-19—A matched retrospective cohort study. J. Glob. Infect. Dis. 2021, 13, 67–71. [Google Scholar] [CrossRef]
- Karakike, E.; Dalekos, G.N.; Koutsodimitropoulos, I.; Saridaki, M.; Pourzitaki, C.; Papathanakos, G.; Kotsaki, A.; Chalvatzis, S.; Dimakopoulou, V.; Vechlidis, N.; et al. ESCAPE: An Open-Label Trial of Personalized Immunotherapy in Critically lll COVID-19 Patients. J. Innate Immun. 2021, 14, 218–228. [Google Scholar] [CrossRef]
Figure 1.
Kaplan Meier curve for cumulative 90-day survival in CAPA population developing CMV blood reactivation or not.
Figure 1.
Kaplan Meier curve for cumulative 90-day survival in CAPA population developing CMV blood reactivation or not.
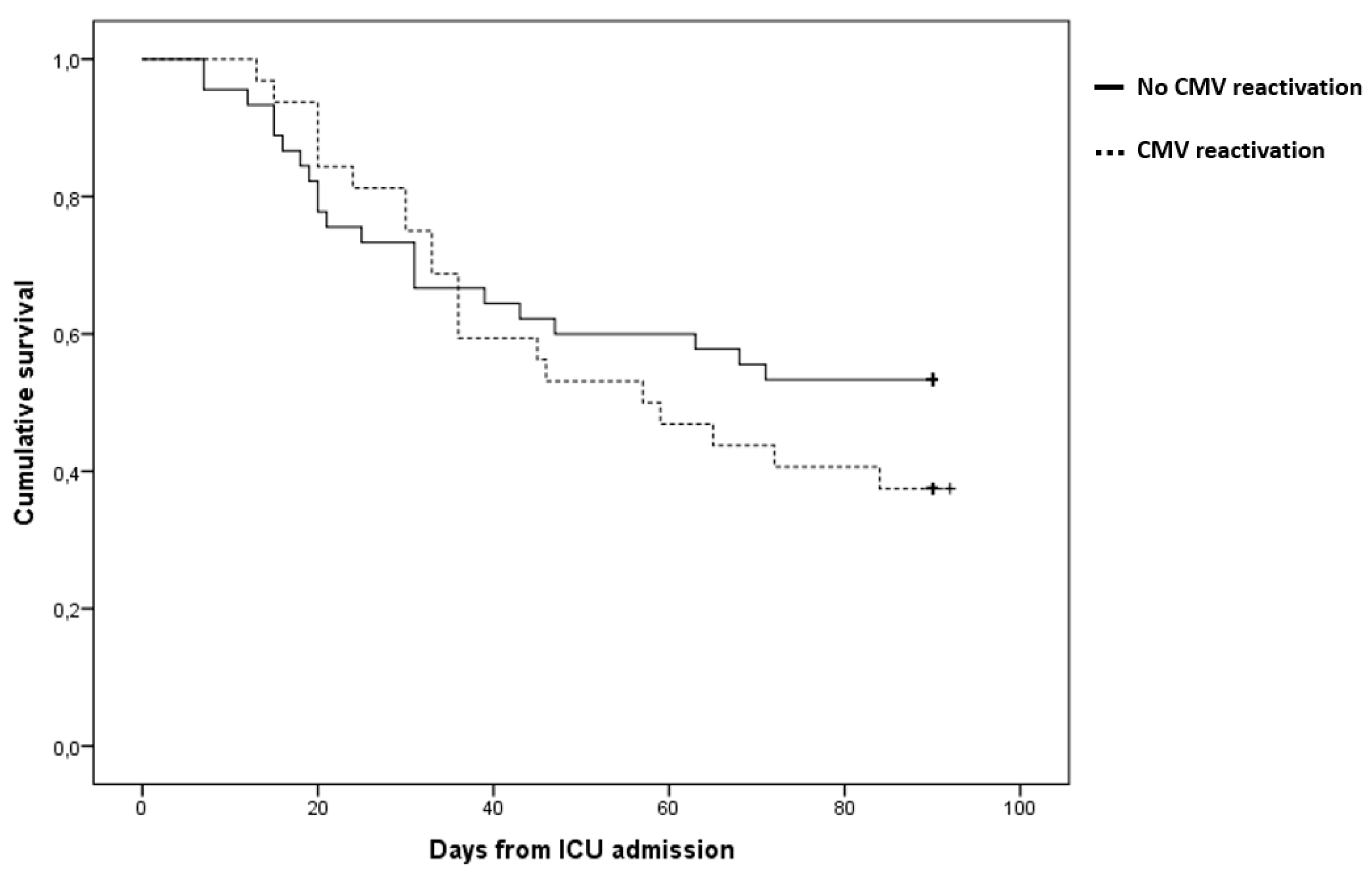

Table 1.
Demographics, comorbidities, severity scores, and laboratory results at ICU admission in all patients and in patients with or without CAPA. The use of steroids during ICU stay and tocilizumab before and during ICU stay has also been reported.
Table 1.
Demographics, comorbidities, severity scores, and laboratory results at ICU admission in all patients and in patients with or without CAPA. The use of steroids during ICU stay and tocilizumab before and during ICU stay has also been reported.
| BASELINE | All population (n=579) |
No CAPA (n=483) |
CAPA (n=96) |
p-value |
|---|---|---|---|---|
| Sex (Male; n, %) | 419 (72,4%) | 348 (72) | 71 (74) | 0,702 |
| Age (median, IQR) | 65 (56-72) | 63 (55-72) | 70 (63-75) | <0,001 |
| BMI (median, IQR) | 29 (26-33) | 29 (26-33) | 29 (26-33) | 0,761 |
| SAPSII score (median, IQR) |
34 (28-39) | 33 (28-38) | 36 (33-43) | <0,001 |
| D-dimer (mcg/l; median, IQR) |
1470 (820-3020) | 1510 (820-2850) | 1325 (780-3660) | 0,992 |
| LDH (U/l; median, IQR) |
823 (634-1104) | 815 (635-1096) | 916 (624-1239) | 0,341 |
| Leukocyte count (cells/mcl; median, IQR) | 8,3 (5,9-11,2) | 8,2 (5,9-10,9) | 8,5 (5,5-11,7) | 0,829 |
| Lymphocyte count (cells/mcl; median, IQR) | 0,7 (0,5-1,0) | 0,7 (0,5-1,0) | 0,6 (0,4-0,9) | 0,008 |
| Platelet count (1000/mmᶾ; median, IQR) | 219 (170-288) | 222 (171-288) | 205 (155-269) | 0,182 |
| CRP (mg/l; median, IQR) |
6,3 (2,2-17,1) | 6,6 (2,6-17,4) | 5,6 (1,2-16,1) | 0,069 |
| PCT (ng/ml; median, IQR) |
0,2 (0,1-0,5) | 0,2 (0,1-0,5) | 0,2 (0,1-0,6) | 0,772 |
| PaO2/FiO2 (mmHg; median, IQR) |
102 (82-135) | 102 (81-136) | 103 (91-135) | 0,347 |
| IL-6 (pg/ml; median, IQR) |
276,6 (93,3-834) | 259,5 (80,0-770,3) | 295,3 (114,9-1177,6) | 0,170 |
| Steroid (n, %) | 533 (92,2) | 441 (91,3) | 92 (96,8) | 0,066 |
| Immunotherapy (n,%) | 477 (82,4) | 398 (82,4) | 79 (82,3) | 0,979 |
| SDD (n,%) | 83 (14,3) | 60 (12,4) | 23 (24,0) | 0,003 |
| Invasive mechanical ventilation (n,%) | 347 (59,9) | 263 (54,5) | 84 (87,5) | < 0,001 |
| Waves | ||||
|
1st wave February 25th, 2020- July 6th, 2020 |
102 | 88 (86,3) | 14 (13,7) | |
|
2nd wave September 20th, 2020-February 13th, 2021 |
166 | 142 (85,5) | 24 (14,5) | |
|
3rd wave February 14th, 2021-April 30th, 2021 |
172 | 136 (79,1) | 36 (20,9) | |
|
4th wave April 30th, 2021-May 8th, 2022 |
139 | 117 (84,2) | 22 (15,8) | |
Table 2.
CMV replication-associated factors among CAPA patients with available serum CMV-DNA.
| Variable |
Total (n=96) |
No CMV Reactivation (n=56) |
CMV Reactivation (n=40) |
P value |
|---|---|---|---|---|
| Sex (Male; n, %) | 71 (74) | 39 (69,9) | 32 (80,0) | 0,254 |
| Age (median-, QR) |
70 (63-75) | 70 (63-75) | 71 (63-76) | 0,663 |
| SOFA (median, IQR) |
4 (3-6) | 4 (3-6) | 5 (4-6) | 0,158 |
| SAPSII score (median, IQR) | 36 (33-43) | 36 (33-42) | 37 (32-44) | 0,519 |
| D-dimer (mcg/l; median, IQR) | 1325 (780-3660) | 1360 (760-3355) | 1305 (800-4866) | 0,994 |
| LDH (U/l; median, IQR) | 916 (624-1239) | 991 (697-1264) | 788 (532-1104) | 0,065 |
| Leukocyte count (cells/mcl; median, IQR) | 8,5 (5,5-11,7) | 8,7 (5,6-11,6) | 8,3 (5,4-15,8) | 0,749 |
| Lymphocyte count (cells/mcl; median, IQR) | 0,6 (0,4-0,9) | 0,6 (0,4-0,8) | 0,6 (0,4-0,9) | 0,624 |
| Platelet count (1000/mmᶾ; median, IQR) | 205 (155-269) | 219 (155-289) | 198 (153-255) | 0,205 |
| CRP (mg/l; median, IQR) | 5,6 (1,2-16,1) | 4,6 (1,4-16,9) | 6,0 (1,1-14,7) | 0,649 |
| PCT T0 (ng/ml; median, IQR) | 0,2 (0,1-0,6) | 0,2 (0,1-0,5) | 0,2 (0,1-0,6) | 0,777 |
| PaO2/FiO2 (mmHg; median, IQR) | 103 (91-135) | 107 (92-142) | 101 (91-129) | 0,483 |
| IL6 (pg/ml; median, IQR) | 295,3 (114,9-1177,6) | 385,6 (194,1-1491,0) | 165,2 (95,9-875,0) | 0,069 |
| BMI (median, IQR) | 29 (26-33) | 29 (26-33) | 29 (27-33) | 0,642 |
| Steroid (n, %) | 92 (96,8) | 52 (94,5) | 40 (100) | 0,133 |
| Immunotherapy (n,%) | 79 (82,3) | 47 (83,9) | 32 (80,0) | 0,619 |
| SDD (n,%) | 23 (24,0) | 14 (25,0) | 9 (22,5) | 0,777 |
| Invasive mechanical ventilation (n,%) | 84 (87,5) | 45 (80,4) | 39 (97,5) | 0,012 |
| Waves | ||||
|
1st wave February 25th, 2020- July 6th, 2020 |
14 (13,7) | 8 (14,3) | 6 (15,0) | 0,969 |
|
2nd wave September 20th, 2020-February 13th, 2021 |
24 (14,5) | 14 (25,0) | 10 (25,0) | |
|
3rd wave February 14th, 2021-April 30th, 2021 |
36 (20,9) | 22 (39,3) | 14 (35,0) | |
|
4th wave April 30th, 2021-May 8th,2022 |
22 (15,8) | 12 (21,4) | 10 (25,0) | |
Table 3.
Main outcomes among CAPA patients with available serum CMV DNA compared to those with CMV blood reactivation.
Table 3.
Main outcomes among CAPA patients with available serum CMV DNA compared to those with CMV blood reactivation.
| OUTCOME |
Total (n=96) |
No CMV Reactivation (n=56) |
CMV Reactivation (n=40) |
P value |
|---|---|---|---|---|
| 90-day mortality (n, %) | 52 (54,2%) | 27 (48,2) | 25 (62,5) | 0,166 |
| ICU mortality (n, %) | 48 (50%) | 24 (42,9) | 24 (60,0) | 0,098 |
| ICU length of stay (days; median, IQR) | 19 (8-39) | 12 (6-23) | 35 (20-59) | <0,001 |
| Invasive mechanical ventilation-free days at day 60 (days; median, IQR) | 9 (1-48) | 13 (1-56) | 7 (0-15) | 0,020 |
| Mechanical ventilation-free days at day 60 (days; median, IQR) | 0 (0-35) | 0 (0-53) | 0 (0-0) | 0,001 |
| Secondary bacterial infection (n, %) | 61 (63.5%) | 30 (53,6) | 31 (77,5) | 0,016 |
| Bacteremia (n, %) | 24 (25%) | 12 (21,4) | 12 (30) | 0,339 |
| Pneumonia (n, %) | 49 (51%) | 25 (44,6) | 24 (60) | 0,914 |
| Time to CAPA occurrence (days; median, IQR) | 5,5 (1,0-12,0) | 2 (1-7,5) | 9,5 (5-20,5) | <0,001 |
| Time to secondary bacterial infection (days; median, IQR) | 11 (6-17) | 10 (10-10) | 19 (6-29) | 0,667 |
Table 4.
Cox regression analysis of factors independently associated with CMV blood reactivation in the population of patients who developed CAPA censored at day 90.
Table 4.
Cox regression analysis of factors independently associated with CMV blood reactivation in the population of patients who developed CAPA censored at day 90.
| CMV blood reactivation at day 90 (n= 40) |
No CMV blood reactivation at at day 90 (n =56) |
Unadjusted HR (95% CI); |
p value | Adjusted HR (95% CI); |
p value | |
|---|---|---|---|---|---|---|
| Invasive Mechanical Ventilation (n,%) | 39 (97,5) | 45 (80,4) | 7,02 (0,96-51,14) | 0,094 | 6,00 (0,74-48,75) | 0,094 |
| Secondary bacterial infection (n,%) | 31 (77,55) | 30 (53,6) | 2,20 (1,04-4,62) | 0,038 | 1,32 (0,60-2,93) | 0,491 |
| Immunotherapy (n,%) | 32 (80,0) | 47 (83,9) | 0,74 (0,34-1,60) | 0,438 | 0,98 (0,44-2,16) | 0,951 |
| Previous immune-suppression (n,%) | 16 (40,0) | 10 (17,9) | 2,33 (1,24-4,40) | 0,009 | 2,33 (1,21-4,48) | 0,011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



