
Submitted:
12 October 2023
Posted:
13 October 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Postural orthostatic tachycardia syndrome (POTS) and its related symptoms have been identified as a possible complication of COVID-19 infection and vaccination and have recently gained attention. The diagnosis and management of POTS require great care and attention, even under normal circumstances, due to its complex nature. However, the COVID-19 pandemic and its complications have further complicated the diagnosis and management of this syndrome in COVID-19-related settings. The objective of this study is to enhance our comprehension of POTS and POTS-like symptoms in the context of COVID-19. To achieve this, we provide a concise overview of the POTS concept, its potential underlying mechanisms, available clinical reports of POTS following COVID-19 infection and vaccination, as well as the clinical manifestations of this syndrome in COVID-19-related scenarios with a brief overview of its management.
Keywords:
Postural Orthostatic Tachycardia Syndrome (POTS)
; COVID-19
; SARS-CoV-2
; Vaccination
1. Introduction
The Coronavirus disease 2019 (COVID-19) pandemic has revealed several strange features of a viral infection. At the beginning of the pandemic, it had been believed that COVID-19 is predominantly a respiratory disease with occasional gastrointestinal involvement. Nevertheless, the vast range of neurological, cardiovascular, dermatological, and metabolic complications occurring during the pandemic was later discovered to be attributable to the virus[1,2]. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has led to many serious cardiac consequences, including myocardial infarction in individuals with no cardiovascular risk factors, which has subsequently been demonstrated to be the result of this viral infection. Later, the introduction of SARS-CoV-2 vaccines further complicated the condition. Despite being an essential health issue, vaccines are sometimes followed by adverse events (AEs). Some vaccine-associated AEs, like thromboembolic events, are life-threatening, while others are only bothersome without risk of death[3,4,5].
As time progresses since the onset of the ARDS-like condition caused by COVID-19, it has become increasingly apparent that individuals may experience long-term effects. One such effect is POTS, which has now been referred to as a component of "Long-COVID." This condition impacts COVID-19 survivors and can be challenging to diagnose and treat due to its clinical similarities with other post-COVID symptoms. The syndrome can significantly impact an individual's life, affecting their physical, functional, social, and psychological well-being[6]. Additionally, it also causes financial difficulties for the person affected[7].
Diagnosis of POTS has always been challenging, even without considering the Covid pandemic and its complications. As a result of the pandemic and, its consequences have made it much more complicated than before to distinguish between POTS-not related to Covid and POTS as complications of post-COVID-19 infection or its vaccination. Although this syndrome is often undiagnosed, it is diagnosed as an anxiety disorder due to hyperadrenergic symptoms and other similarities[8]; Moreover, this debilitating condition has not only been reported its relation to COVID-19 infection but also to post-Covid vaccination[9].
Thus, in the current study, we not only examined the concept of POTS, its possible underlying mechanism, and its relationship with COVID-19 infection and how to manage them, but we also compared the manifestations and characteristics of POTS after COVID-19 infection with POTS after the Covid-19 vaccine, based on the existing literature.
2. POTS
2.1. What is POTS?
POTS is a complex medical condition characterized by hemodynamic and clinical criteria; this syndrome is a persistent chronic condition and should last at least three months. Hemodynamic changes comprise a sustained increasing heart rate of 30 beats per minute in individuals older than 19 or an increase of 40bpm in patients younger than 19 years; these hemodynamic changes should occur transitioning from a supine to an upright position within 10 minutes in the vertical position without orthostatic hypotension or definite underlying etiologies. Clinical manifestations can be categorized into positional-related symptoms and unrelated positional symptoms. Positional-related symptoms include lightheadedness, tremor, palpitation, and atypical chest discomfort. On the other hand, unrelated positional symptoms include headaches, chronic fatigue, exercise intolerance, deconditioning, perceived mental impairment (commonly known as "brain fog"), peripheral acrocyanosis (also called "POTS feet"), frequent nausea, mild diarrhea, constipation, bloating, and unspecific abdominal discomfort (such as "irritable bowel syndrome")[10].
2.2. What is the pathophysiology of POTS?
While several possible underlying pathophysiologies of POTS have been postulated, the following explanations comprise "autonomic denervation"(e.g.,.post ganglionic autonomic fiber restriction, Sympathetic tone impairment)[11], "hypovolemia"(blood volume and renin-angiotensin-aldosterone activity reduction)[12], "hyperadrenergic stimulation"(Norepinephrine transporter deficiency)[13], and "deconditioning"( Stroke volume reduction)[14] have been more widely accepted. Despite the semi-acceptance of most of these mentioned mechanisms, it should be noted that POTS is not necessarily dependent on these mechanisms; This suggests that these mechanisms may be linked to POTS rather than being the direct cause.
Although some studies have reported upper respiratory and digestive tract infections with viral agents such as influenza, EBV, and Borrelia burgdorferi as the responsible agents prior to the initiation of POTS[15,16], the relationship of this syndrome with collagen vascular and autoimmune diseases have also been reported[17,18]. Moreover, some exacerbating factors, such as trauma, pregnancy, and heightened psychological or social stress, can potentially trigger or exacerbate the condition [11,19].
2.3. POTS diagnosis and management
Diagnosing POTS is quite tricky and necessitates careful attention and effort. It has been found that a significant proportion of patients, four out of five to be precise, are initially diagnosed with psychological disorders before receiving a POTS diagnosis, according to a recent study[20]. The lack of clarity of manifestations and the widespread nature of tachycardia, which exists in a broad spectrum of diseases, add to the difficulty of diagnosis. The diagnosis of POTS requires a comprehensive assessment of clinical signs and symptoms, as well as a hemodynamic status examination. It is essential to conduct both evaluations simultaneously to obtain an accurate diagnosis. In other words, misdiagnosis might occur if attention is paid solely to clinical manifestation or hemodynamic orthostatic changes[21].
Chronic orthostatic intolerance syndromes include a group of diseases with similar clinical manifestations and hemodynamic instability, one of which is POTS; the others include "POTS plus, "postural symptoms without tachycardia(PSWT), "PSWT plus," and "postural tachycardia of other causes(PTOC)[10]." Consequently, the complicated nature of POTS, besides differential diagnoses, underlying diseases, drug complications, and existing in the chronic orthostatic intolerance syndromes category, makes the POTS diagnosis more challenging and requires clinical expertise and careful observation.
The diagnosis of POTS is usually delayed due to the nonspecific presentations of this condition. The most sensitive method to detect POTS is a detailed medical history, physical examination with vital orthostatic signs or brief tilt table test, and a resting 12-lead electrocardiogram. When managing patients with POTS, it is imperative to carefully monitor their diet, particularly their salt and water intake, and thoroughly assess their autonomic system. Furthermore, a detailed assessment of medications and substance use is crucial, which can exacerbate or imitate POTS, despite often being neglected in the clinical history. These measures are essential for effective POTS management and should be considered in the patient's care plan[22,23,24].
POTS and inappropriate sinus tachycardia overlap several manifestations. A 24-hour Holter monitoring may assist in distinguishing between the two scenarios. Several patients with suspected POTS may not exhibit the classic 30-point rise in their heart rate during their medical visit; Rather, they may tend towards increased heart rate in an upright position[25]. A monitoring device that can differentiate these patterns from other arrhythmias may be advantageous for these patients. Morning evaluations are typically more sensitive since the heart rate fluctuates throughout the day [26]. The head-up tilt and active upright position tests are additional diagnostic tools that could be helpful. POTS is diagnosed when a patient experiences a heart rate increase of 30 beats per minute or more within the first 10 minutes of a head-up tilt or active upright standing position test; Increasing heart rate should not be accompanied by a corresponding decrease in blood pressure[23].
Although autonomic examinations such as Valsalva maneuvers, deep breathing tests, tilt table testing, and plasma norepinephrine levels are not routinely performed, in such cases, highly suspicious for autonomic neuropathy can be done besides referring them to the specialist. It is unclear whether neuroimaging or antibody testing has any medical value for these patients and is not a standard part of clinical practice[10,27].
Additional diagnostic testing may be warranted in selected patients based on clinical signs. Diagnosing postural orthostatic tachycardia requires that orthostatic hypotension (a fall in blood pressure of more than 20 mm Hg systolic or 10 mm Hg diastolic within three minutes of standing) and other probable causes of tachycardia (e.g., anemia, dehydration, fever, sepsis, endocrinological conditions such as hyperthyroidism or Addison’s disease, respiratory conditions such as pulmonary embolism, and cardiac conditions) be excluded.
Hence, through laboratory workup including measurement of blood glucose, serum cortisol, complete blood count, renal and thyroid function tests, inflammatory biomarkers like erythrocyte sedimentation rate (ESR) and C reactive protein (CRP), ferritin, vitamin B12, folate, and calcium, In addition, chest x-ray imaging is required if clinically indicated. However, it should be noted that cardiac ischemia, myocarditis, and pulmonary embolism must be considered in any patient presenting with possible acute cardiac symptoms, as acute conditions need to be urgently detected and managed[22,24,28].
Current management of POTS is predominantly dependent upon symptom therapy and lifestyle modification. The management of POTS consists of non-pharmacologic(as the first line) and pharmacologic therapies. Non-pharmacologic treatment includes increasing fluid and salt intake, increasing isometric and aerobic exercise, lower-limbs strengthening, the gradual elevation of intensity and duration of physical activity- Exercises should be initiated in a lying-down position if standing exercise and physical activity exacerbate symptoms-., psychological support and training to control pain and anxiety, rehabilitation, reassurance, and family education, and avoiding triggers like alcohol, caffeine, heavy meals, prolonged standing or upright position, warm places, and discontinuation of antihypertensive drugs including hypotensive medications like diuretics, opiates, a-receptor blockers, angiotensin-converting enzyme inhibitors, nitrates, tricyclic antidepressants, monoamine oxidase inhibitors, phenothiazines, and sildenafil citrate if possible[29,30].
Pharmacologic treatment includes heart rate control, peripheral vasoconstriction, and intravascular volume increase. Medical therapy is usually individualized but generally consists of β-blockers (Propranolol), channel blockers (Ivabradine), α-agonists (Clonidine), antihistamines (Diphenhydramine), mineralocorticoids (Fludrocortisone), vasopressin analogs (Desmopressin), anticholinesterase inhibitors (Pyridostigmine), CNS stimulants (Modafinil), and selective serotonin reuptake inhibitors (Sertraline). POTS may interfere with even the most minor energy-requiring daily activities like bathing or housework, significantly decreasing functional capacity. Nevertheless, it is not associated with mortality; many patients improve after diagnosis and proper treatment [31,32,33,34,35].
3. POTS following SARS-CoV-2 infection
The COVID-19 pandemic has caused patients to experience prolonged symptoms that can be highly debilitating. These symptoms are commonly referred to as "long COVID," "long-haul COVID," Post-Covid syndrome," or "chronic COVID"[36].
Widely known terms "Long-COVID" and "Post-COVID Syndrome" also refer to post-acute sequelae of SARS-CoV-2, a combination of signs and symptoms that continue for weeks or months after the SARS-COV-2 infection initiation. According to the current broadest definition, LONG-COVID refers to the continued presence of symptoms or the new onset of malaise that persists for a minimum of four weeks following a laboratory-confirmed case of COVID-19 despite the receipt of appropriate medical attempts[37].
Long-Covid symptoms comprise shortness of breath, palpitation, chest discomfort, orthostatic intolerance, fatigue, joint and muscle aches, headache, tinnitus, sleep trouble, and gastrointestinal-like symptoms(e.g., Nausea, diarrhea, abdominal discomfort), and also neuropsychiatric symptoms such as cognitive impairment, peripheral neuropathy, anxiety, or depression[38].
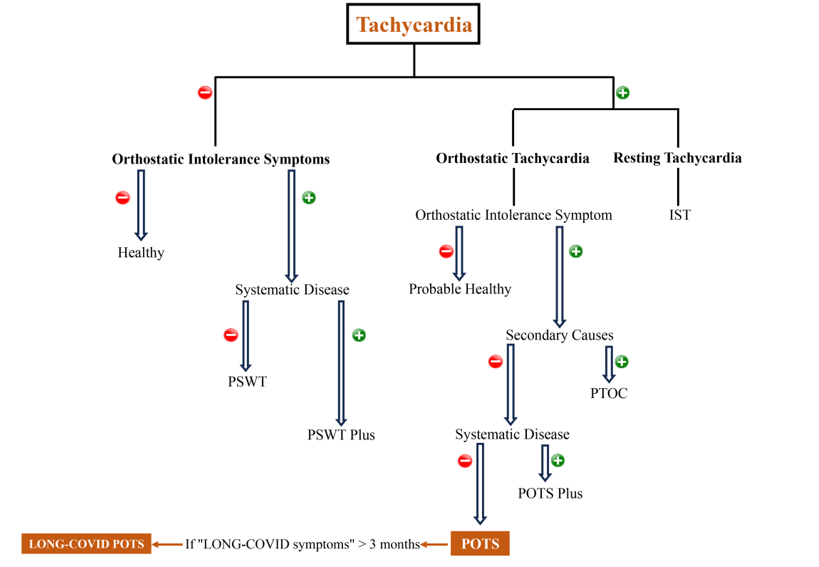
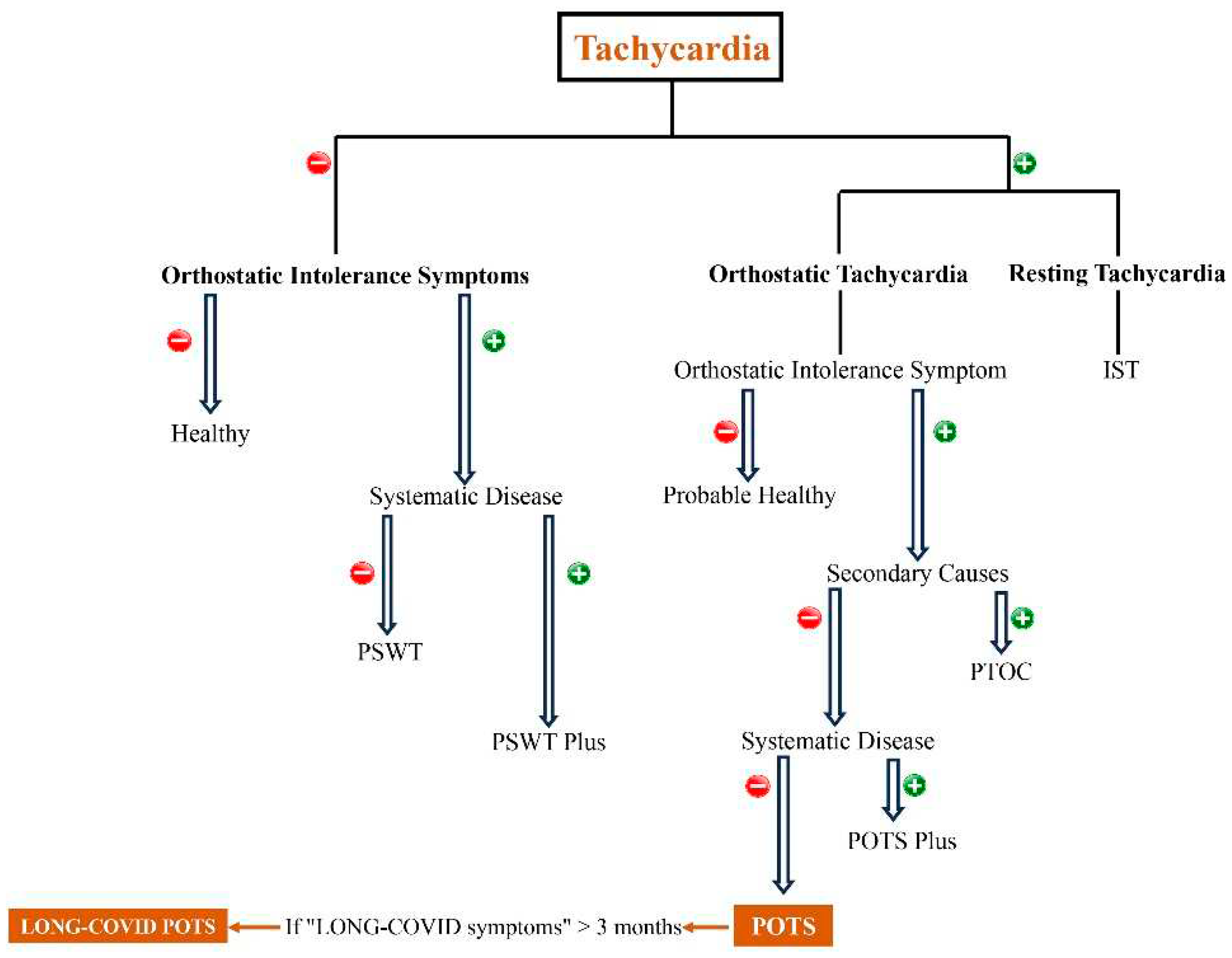
Along with other complications known for LONG-COVID, a new member called post-COVID POTS has recently been added to this family. Post-Covid-19 POTS(Long-Covid-POTS) is diagnosed when the post-COVID (LONG-COVID) symptoms combine with excessive orthostatic tachycardia for over three months in a Sars-Cov-2 infected patient[39](Figure 1).
3.1. Pathogenesis of LONG-Covid POTS
Understanding the primary mechanism behind Long-Covid can provide insight into its symptoms and complications, including Post-Covid-POTS. However, despite numerous efforts and speculations, the exact pathogenesis and pathophysiology of Long-Covid remains unknown. Although the exact mechanism of long-Covid is still unclear, some studies have suggested different possible mechanisms for long-Covid.
According to recent studies, some possible broad classifications of mechanisms have been reported for the LONG-covid pathogenesis, such as the following:
The number of studies supporting the evidence of the persistence of the virus itself or its components in various body organs, even after a time interval from the initial entry, has increased[36]; A study that examined the autopsies of 44 patients who died due to Covid-19 in 2022 showed that the virus or its components were present in the pulmonary and extrapulmonary organ autopsies, including the brain, heart, and lymphatic organs [41].
Although the respiratory organ was the most common site, RNA of Sars-Cov-2 was detected in more than half of the patient's extrapulmonary sites. Interestingly, all the samples taken from the brain sites, except Dura, showed the presence of the virus or its components. Also, this study showed that viral RNA could be detectable up to 230 days after the onset of initial manifestations[41].
Another study that examined the biopsies of asymptomatic COVID-19 patients revealed that five of fourteen patients with long-COVID had detectable viral RNA in their gastrointestinal tracts months after the initial entry[47].
At this time, there is a lack of understanding regarding the mechanisms of the persistence of the virus in body cells and the interactions of the virus with intracellular systems. Further research is necessary to gain insight into these critical areas of exploration.
However, some believe that, unlike acute infection, the virus and the host cell reach a concurrence or interactive stage in the chronic and prolonged phase, probably due to cellular-molecular and immunological events[48,49]; Scilicet, opposite to the acute phase – acute phase: the virus uses the tools of the host cell for its maximum reproduction and leads to host cell death [50,51]- in the chronic phase, these interactions let the host cell to survive and the virus to invade the immune responses. All of these create a viral reservoir from the host cell that this viral reservoir not only disrupts the immune system functionality but also causes a continuous defective inflammatory cycle, which ultimately causes cell damage and tissue death[52,53].
In summary, it can be stated that all the mentioned mechanisms, including the "persistence of the virus in different body organs," "the reactivation of viruses such as EBV," "immune responses against the virus," "the mechanisms of autoimmunity induced by the virus," and the "micro clot formation due to the coagulatory mechanisms disturbance and endothelial damage" cause a series of cytokines, chemokines and different factors including interferons and pentraxin 3(PTX3); As a result, the body enters into a defective persistent inflammatory phase that causes damage to the pulmonary, cerebral, cardiovascular and other organs.
More specifically, for POTS related to Covid-19 should be noted that Although the precise pathophysiological mechanisms behind the context of post-covid POTS are still being investigated, several hypotheses have been suggested:
(1)Autonomic dysfunction in POTS patients due to sympathetic overactivity, parasympathetic impairment, and/or small fibers neuropathy caused by sars-cov-2 infection[25,28].
(2)Endothelial dysfunction and increased vascular permeability due to excessive inflammation and persistent inflammatory responses to the virus or its particles, which are seen in COVID-19 patients, may contribute to the pathogenesis of post-covid POTS[25].
(3) Ongoing inflammatory responses due to the persistence of the virus itself or its components in certain tissues, including the autonomic ganglia and nerve endings, leading to autonomic nerve dysfunction[54].
Also, based on recent studies, it seems that autoantibodies play a role in the development of Long-Covid POTS, though these auto-antibodies have not been confirmed as a cause; One of these recently received attention is autoantibody against alpha-1-adrenergic receptors.
A study found high levels of autoantibodies against alpha-1 adrenergic receptors in patients with COVID-19 and considered it responsible for complications, including POTS; Therefore, this study stated that the high level of this autoantibody is the cause of increased alpha receptor-mediated vasoconstriction and beta receptor-mediated tachycardia as a compensatory mechanism[11]. On the other hand, Gunning et al. discovered that antibodies against alpha-2, beta-1, and beta-2 receptors are only present in the serum of POTS patients if alpha-1-adrenergic receptor autoantibodies are present[55].
However, the most probable mechanism of post-COVID-19 POTS is SARS-CoV-2-associated induction of autoimmunity through producing cross-reacting antibodies with autonomic ganglia and nerve fibers and neuronal or cardiovascular receptors. In addition, sympathetic overactivation induced by SARS-CoV-2 infection may lead to post-COVID POTS[55,56].
3.2. Prevalence
In accordance with a recent investigation, the prevalence of postural orthostatic tachycardia syndrome (POTS) among COVID-19-infected or vaccinated individuals in the United States has been estimated to be 300,000[57]. Numerous investigations have endeavored to assess the prevalence and the potential number of persons who experience POTS subsequent to being infected with SARS-CoV-2 or being vaccinated against COVID-19. However, extant reports do not furnish adequate evidence to establish the precise figure of patients who are affected by POTS as a complication of SARS-CoV-2 infection or a consequence of COVID-19 vaccination.
Several have identified POTS as a subset of long-term complications of Sars-Cov-2 infection. However, some of these reports are inconsistent with the definition of POTS, which needs some degree of chronicity; Some studies that reported POTS after COVID-19 proposed this diagnosis shortly after the onset of symptoms, even though POTS demands at least three months to be diagnosed[58,59]. Due to the intricate nature of diagnosing this syndrome, it is exceedingly challenging to determine the precise prevalence of individuals experiencing it as a complication following a COVID-19 infection based on the currently available literature.
3.3. Overview of clinical reports on suspicious post-Covid-POTS
Observations and potential associations between postural orthostatic tachycardia syndrome (POTS) and the Sars-Cov-2 infection, as well as the COVID-19 vaccination, have increased in recent years. Nonetheless, the first likely association between POTS and COVID-19 infection was reported in early 2020[30]. The clinical reports on POTS following SARS infection are presented in Table 1. This table accounts for all articles containing information on POTS following Sars-Cov-2 infection from the initiation of this topic to January 2023.
The data presented in Table 1 indicate that the manifestations observed in patients with POTS who contracted SARS-Cov-2 are remarkably similar to those observed in patients with POTS who did not contract the infection. Studies indicate that the aforementioned medical ailment exhibits a higher incidence rate amongst females and individuals affected by dysautonomia, as well as those harboring underlying autoimmune disorders. Although some studies believe that a mild primary infection is associated with a higher prevalence of POTS[39,60], the severity of the primary infection does not seem to be related to the prevalence, severity of POTS, and treatment response.
According to a study, patients who underwent Enhanced External Counterpulsation treatment experienced a remarkable improvement in their health condition[61]; However, in order to fully comprehend the exact relationship between the severity of the initial infection and the POTS incidence, its severity, and response rate to the treatment, as well as the efficacy of response to the treatments such as Enhanced external counterpulsation, necessitates extensive research conducted with systematic methodology (Table 1).

Table 1.
Overview of clinical reports on POTS after Covid-19.
| Author | Region | Number of diagnosed patients | Gender | Time to diagnosis | Manifestations | hospitalization | Management | Outcome | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | ≥ 3 months | < 3 months | Yes | No | ||||||
| Umapathi et al,[62] |
Asia | 4 | 1 | 3 | 0 | 4 | Sweating, constipation, nausea, after-meal abdominal discomfort, tachycardia on standing and during passive 60-degree tilt without blood pressure decreasing | 4 | 0 | Fludrocortisone, sodium tablets, Pyridostigmine | Good (Recovered and symptoms improvement) |
| Rudofker et al,[63] |
America | 3 | 1 | 2 | 2 | 1 | fatigue, lightheadedness, brain fog, and palpitations, syncope, breathlessness, paroxysmal coughing ,increasing resting heart rate of 10 to 15 Beats per minute | 1 | 2 | exercise (rowing/biking) for 2 months |
Good (Recovered) |
| Shouman et al,[64] |
America | 27 | 11 | 16 | some | some | Common symptoms : Lightheadedness, orthostatic headache, syncope, hyperhidrosis, and pain n=11 →Orthostatic intolerance without tachycardia/n=6 →Orthostatic intolerance with orthostatic tachycardia/n= 3 → Overlapping symptoms |
N/A | N/A | Rehabilitation, low dose beta blockers, Anxiolytics Gabapentin and topical lidocaine for neuropathic symptoms in the autonomic neuropathy cases |
Good (Improvement, except for anxyiolytic) |
| Desai et al,[65] |
America | 11 | 2 | 9 | Some | Most (Mean ≈ 40 day) | Palpitations, fatigue, chest discomfort | N/A | N/A | Beta blockers (5), midodrine (1), colchicine (1), ibuprofen (2), lifestyle modifications (2) | Good (all improved except for colchicine) |
| Agnihotri et al,[66] |
America | 1 | 0 | 1 | 1 | 0 | Lightheadedness, palpitations, tingling, hyperhidrosis, tremor, and red discoloration of feet on upright position | 0 | 1 | metoprolol, midodrine, lifestyle change | Good (symptoms improved) |
| Ocher et al,[67] |
America | 1 | 0 | 1 | 0 | 1 | IST | 1 | 0 | Metoprolol,Ivabradine | Poor |
| Parker et al,[68] |
America | 7 | 1 | 6 | 0 | 7 | Palpitations, chest discomfort and tachypnea, GI symptoms | N/A | N/A | supportive therapy; ivabradine, midodrine metoprolol;intravenous immunoglobulin | Not clearly mentioned (2 out of 3 severe patients responded to IV immunoglubolin) |
| O’Sullivan et al,[59] |
Europe | 1 | 0 | 1 | 0 | 1 | Chest tightness, palpitations, breathlessness, fatigue | 0 | 1 | lifestyle change ,ivabradine |
Good (Best symptoms improvement with ivabradine) |
| Blitshteyn et al,[15] |
America | 20 | 6 | 14 | 20 | 0 | Fatigue, postural tachycardia, brain fog, and exercise intolerance | N/A | N/A | All prescribed lifestyle modifications, 16 needed pharmacological drug including beta blockers, fludrocortisone midodrine, ivabradine | Good ( all fully recovered, except three of them which near complete recovered) |
| Jamal et al,[69] |
America | 24 | 4 | 20 | 24 | 0 | tachycardia with subordinary physical activity or positional change, palpitations |
2 | 22 | N/A | N/A |
| Kitsou et al,[70] |
Europe | 1 | 0 | 1 | 1 | 0 | Chest discomfort, exertional dyspnea, palpitations, syncope | 0 | 1 | Metoprolol | Good ( improved after six months) |
| Johansson et al,[71] |
Europe | 3 | 1 | 2 | 1 | 2 | sinus tachycardia; chest discomfort, fatigue, dizziness, headache, fatigue, muscle weakness, sleep disturbance, palpitations, and “brain fog”, concentration issue | 2 | 1 | (A)Lifestyle change, ivabradine (B) lifestyle changes ,propranolol,antihistamines(C) lifestyle changes, pyridostigmine, propranolol antihistamines |
Acceptable(A) Poor(B,C) (A) →Partial recovery (B)→ symptoms remained (C)→ Symptoms Remained |
| Varanasi et al,[61] |
America | 1 | 0 | 1 | 1 | 0 | Fatigue, “brain fog”, breathlessness, exertional dyspnea | 1 | 0 | External counterpulsation | Good |
| Kanjwal et al,[58] |
America | 1 | 0 | 1 | 0 | 1 | headache, dizziness, chest discomfort, and palpitations, fatigue | 0 | 1 | Ivabradine, salt water intake | Acceptable (improved but tachycardia remained) |
| Miglis et al,[30] |
America | 1 | 0 | 1 | 1 | 0 | Tachycardia, chest discomfort, breathlessness, fatigue and exercise intolerance, fever, sleep disturbance | 1 | 0 | Propranolol | Acceptable (partially recovered) |
| Ishibashi et al,[72] |
Asia | 1 | 0 | 1 | 0 | 1 | Fatigue, palpitation, chest discomfort | N/A | N/A | Bisoprolol | Good (marked recovery) |
| Kalia et al,[73] |
America | 1 | 0 | 1 | 1 | 0 | Tachycardia, headaches, pre-syncope | N/A | N/A | Metoprolol | Acceptable (partially recovered) |
| Bosco et al,[74] |
Asia | 1 | 0 | 1 | 1 | 0 | exertional fatigue, memory and concentration impairement, headaches, blurred vision, malaise, | 0 | 1 | Lifestyle changes, exercise therapy | Acceptable (partially recovered) |
4. POTS following COVID-19 vaccination
Postural orthostatic tachycardia syndrome(POTS) has not only possibly occurred as a part of the “long COVID” syndrome following SARS-CoV-2 infection but has also been reported after COVID-19 vaccination. However, the incidence rate is multiple times higher after infection than after vaccination[57,75]. Postural Orthostatic Tachycardia Syndrome (POTS) has been previously observed as a potential adverse effect following some vaccines, including the Human Papillomavirus (HPV) vaccine[76,77]. However, in light of the ongoing pandemic and heightened sensitivities surrounding COVID-19 vaccinations, reports of POTS following the COVID-19 vaccine administration have garnered significant attention and concern. Although POTS can occur after the covid-vaccine, the occurrence after Sars-Cov-2 infection is five-fold higher, according to a recent study[57].
4.1. Overview of the clinical reports on suspected POTS after Covid-vaccine
When analyzing the timing of POTS-like symptoms, it is noteworthy that they tend to manifest sooner following the Covid vaccination than a Covid infection; According to the available reports, it has been observed that the onset of POTS-like symptoms has manifested within a variable timeframe ranging from several hours to a few weeks following the Covid-vaccine, on the other hand, POTS symptoms after Sars-cov-2 infection tend to manifest several months later often (Table1 and Table 2). While POTS-like symptoms, unlike the COVID infection, manifest earlier after the COVID-19 vaccine, they are reported to be more common in the female gender, similar to the post-COVID infection. Although POTS-like symptoms are more frequently reported after the mRNA vaccines of COVID-19, a clear cause-and-effect relationship cannot be established for the occurrence of these symptoms after the mRNA vaccines; Since, in addition to the fact that these manifestations have been reported after non-mRNA COVID vaccines, including Oxford-AstraZeneca[78], they have also been reported after HPV and influenza vaccines[79,80].
The most common manifestations were dizziness, palpitation, fatigue, nausea, headache, abnormal sensations like tingling and numbness, and syncopal events, which aggravate in an upright position. Although the different treatment approaches, including lifestyle modifications and medical agents used in the studies, aimed to relieve the symptoms and manifestations, except for one patient whose symptoms continued, most patients improved.
Several reported the beneficial and improving effects of IVIG and plasma exchange in managing and treating some patients who did not respond to conventional treatments[81,82]. However, we need studies with a higher sample size and a transparent methodology to draw conclusions about the use of IVIG or plasma exchange in this patient category (Table 2).
Table 2.
Overview of clinical report on POTS-like symptoms after Covid-19 vaccination.
| Patient | Gender | Age | PMH | Drug history | Type of vaccine | Vaccine dose | POTS Symptoms onset after vaccination | Manifestations | Management | Outcome | Reference Author |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient 1 |
Female | 37 | seasonal allergy and depression | Vortioxetine | Moderna | First dose | 1 week | lightheadedness, heart racing, weakness, difficulty concentrating, blurry vision, shakiness, vertigo, and clamminess when assuming upright posture, improving symptoms in the supine position, dry eyes and mouth unrelated to medications, heat sensitivity, constipation, numbness and tingling of the feet, legs hands, and occasionally the face. | 5 mg of ivabradine twice a day | "Good" (Improve) |
Eldokla et al., [83] |
| Patient 2 |
Female | 21 | No | No | BioNTech-Pfizer | First dose | 12 days | headache, palpitation, weakness, difficulty thinking, improving symptoms in the supine position, heat sensitivity, sweating, face and extremities numbness and tingling | metoprolol 25 mg, and fludrocortisone 0.2 mg daily | "Good" (Improve) |
Eldokla et al., [83] |
| Patient 3 |
Female | 46 | No | No | BioNTech-Pfizer | First dose | 2 weeks | lightheadedness, nausea, fatigue, poor concentration, palpitations, and brain fog, increase sympathetic activity after the head-up position in spectral Fourier analysis | fludrocortisone and propranolol | "Good" (Improve) |
Eldokla et al., [83] |
| Patient 4 |
Female | 19 | No | No | BioNTech-Pfizer | Second dose | 18 days | dizziness, headache ,nausea, sweating, and fatigue, increase in sympathetic tone after the head-up position in spectral Fourier analysis | salt tablets and propranolol | "Good" (Improve) |
Eldokla et al., [83] |
| Patient 5 |
Female | 17 | No | No | BioNTech–Pfizer | Second dose | 3 weeks | syncope, fatigue, chest tightness, nausea, and heat intolerance, increased sympathetic activity with occasional spikes of vagal tone after the head-up position in spectral Fourier analysis | scopolamine patches for nausea, salt tablets and propranolol | "Good" (Improve) |
Eldokla et al., [83] |
| Patient 6 |
Male | 40 | No | No | Moderna | First dose | one week | Orthostatic palpitation, intermittent headache, fatigue, dyspnea, increasing HR from 72 to 110 in Head-up tilt test | propranolol 20 mg, three times daily for 2 months | "Good" (Improve) |
Park et al., [84] |
| Patient 7 |
Male | 42 | Hypothyroidism, vitamin B-12 deficiency, Left-sided orchiectomy for cryptorchidism | Levothyroxine 125 mg, vitamin B-12 shots | BioNTech–Pfizer | First dose | six days | syncopal episode, sinus tachycardia, intermittent palpitations, anxiety, sleep disturbances, occasional numbness in the lower extremities | lifestyle modifications, such as wearing compression socks and increased sodium intake | "Unchanged" (Existing symptom) |
Reddy et al., [85] |
| Patient 8 |
Male | 13 | No | No | BioNTech–Pfizer | Second dose | Fourteen days | fatigue, headache, and orthostatic intolerance symptoms including lightheadedness and palpitations | salt and fluid intake and exercise,propranolol, midodrine (2 mg, twice daily),droxidopa, (IVIG) 2 g/kg was administered for the myocarditis | "Acceptable" (almost improved) |
Sanada et al.,[82] |
| Patient 9 |
Male | 15 | No | No | BioNTech–Pfizer | Third dose | Two weeks | Presyncope and syncopal episodes, and lightheadedness | fludrocortisone 0.1 mg every eight hours, Ivabradine 2.5 mg every 12 hours, lifestyle modification with respect to increasing sodium and fluid intake, moderate exercise | "Good" (Improve) |
Maharaj et al., [9] |
| Patient 10 | Female | 46 | allergic rhinitis, history of COVID-19 infection | No | BioNTech-Pfizer | First dose | four weeks | lightheadedness, tremors, increasing heart rate, Raynaud’s Phenomenon, fatigue, brain fog, headache, chest discomfort, exercise intolerance, profound fatigue, dizziness, and paresthesia | salt consumption, fluid intake, and 20 mmHG compression stockings, ivabradine 5 mg BID, dietary supplement, | "Acceptable" (all improved except Raynaud’s Phenomenon) |
Hermel et al., [86] |
| Patient 11 | Male | 29 | No | No | Oxford-AstraZeneca | First dose | 4 days | Intermittent paresthesia, palpitations, dizziness, , heart beat racing |
Steroid for 5 weeks without effect, lifestyle modifications |
"Acceptable"(some symptoms improved) | Karimi et al.,[78] |
| Patient 12 | Male | 43 | Sleep disturbance | Naproxen, Lansoprazole, Dihydrocodeine, Melatonin |
Oxford-AstraZeneca | First dose | 6 hours | Dizziness, nausea, weakness, bradykinesia, brain fog, early waking, fatigue, “jelly-legs”, changes to walking gait, |
Hydroxocobalamin IM |
"Good" (Improve) |
Carroll et al.,[87] |
| Patient 13 | Male | 52 | No | No | BioNTech-Pfizer | Second dose | Not specifically mentioned | Feeling stabbing, orthostatic intolerance, syncope, supraventricular tachycardia, tinnitus |
Nadolol, Gabapentin, Amitriptyline, and trazodone (no effect) / plasma exchange for Five time |
"Good" (Improve) |
Schelke et al., [81] |
| Patient 14 | Female | N/M | History of COVID-19 and family history of Sjrogen’s disease |
No | Oxford-AstraZeneca | First dose | 2 hour | Limbs paresthesia, tachycardia, blood pressure fluctuation, intermittent internal tremor, cognitive complaints |
N/A | N/A | Safavi et al., [88] |
| Patient 15 | Female | N/M | Family history of psoriasis |
No | Moderna | Second dose | 2 days | Orthostasis, heart rate and blood pressure fluctuation, nausea, diarrhea, face and limbs paresthesia, internal tremor |
N/A | N/A | Safavi et al., [88] |
| Patient 16 | Female | N/M | Family history of rheumatoid arthritis |
No | BioNTech-Pfizer | Second dose | 10 days | Severe orthostatic Tachycardia, diarrhea, blood pressure fluctuation | N/A | N/A | Safavi et al., [88] |
| Patient 17 | Female | N/M | No | No | Moderna | First dose | 2 days | Intermittent paresthesia, face and limbs numbness, Mild right-hand weakness, episodic positional palpitation |
N/A | N/A | Safavi et al., [88] |
| Patient 18 | Female | N/M | No | No | Moderna | First dose | 6 days | Exercise intolerance, Limbs fasciculation, internal tremor, facial paresthesia, chest discomfort; cognitive disturbance, episodic positional palpitations | N/A | N/A | Safavi et al., [88] |
| Patient 19 | Female | N/M | No | No | Moderna | Second dose | 5 days | Facial Paresthesia and burning sensation, positional Palpitation,dizziness | N/A | N/A | Safavi et al., [88] |
PMH, Past medical history; N/A, Not applicable; N/M, Not mentioned; IM, Intramuscular; IV, Intravenous.
4.2. COVID-19 vaccination-induced autoimmunity
In accordance with the currently available evidence, it appears that autoimmune pathways may play a substantial role in the development of POTS-like symptoms following a COVID-19 vaccine. Recently, studies have increasingly highlighted the emergence of Postural Orthostatic Tachycardia Syndrome (POTS)-like symptoms following COVID-19 vaccination. This emergence has brought increased attention to the possibility that POTS is a potential complication of the COVID-19 vaccine, in addition to being a long-term COVID-19 infection complication. Researchers have postulated that similar to the cross-reactivity observed between antibodies targeting the COVID-19 infection and different aspects of the autonomic system, including nerve fibers, a comparable cross-reactivity may manifest following COVID-19 vaccination[15,88].
Researchers have proposed the following possible mechanisms according to the hypothesis of cross-reactivity between components of the autonomic system and antibodies produced in response to the vaccine : (1)Cross-reactivity between vaccine-induced antibodies with alpha-1 adrenergic receptors can disrupt the vasoconstriction response; However, it results in autonomic system hyperactivity compensatory response and following compensatory tachycardia[85]. (2)Research suggests that angiotensin-converting enzyme-2 receptor dysfunction not only plays a causative role in postural orthostatic tachycardia syndrome (POTS) but also interferes with the pathogenesis of SAR-CoV-2 infection; Cross-reactivity between vaccine-induced antibodies and angiotensin-converting enzyme-2 receptors may disrupt these receptors, resulting in compensatory hyperadrenergic symptoms[62,89]. Immunotherapy may be a viable treatment for the side effects of the COVID-19 vaccination, adding weight to the concept that autoimmune mechanisms may be at play[88].
4.2. Common Covid-vaccination side effects and POTS-like symptoms
To ensure a proper diagnosis of postural orthostatic tachycardia syndrome (POTS) in individuals who have received the COVID-19 vaccination, suspected patients must meet the essential diagnostic criteria for POTS, which includes orthostatic intolerance symptoms and hemodynamic criteria, as well as document the specific duration of these symptoms; orthostatic hypotension and underlying secondary causes also need to be excluded for accurate diagnosis. As with the diagnosis of POTS in non-Covid settings, detailed history and clinical examination are the primary and crucial elements of diagnosing this syndrome.
In addition to the history taking and detailed clinical examination and cardiac and neurological evaluation to rule out underlying etiologies, routine workups, including blood tests, electrolytes, electrocardiography, Thyroid function testing, and other procedures described in previous sections, are performed on patients with suspected symptoms of POTS[10,90].
As delineated in Table 2, certain reports of symptoms following a Covid-vaccine injection, which is labeled as Postural Orthostatic Tachycardia Syndrome (POTS), do not meet the established criteria for this condition, as it requires the presence of sustained symptoms over a minimum of three months. Due to the fact that POTS diagnosis necessitates the persistence of symptoms for a prolonged period ranging from 3 to 6 months, it is impossible to classify immediate symptoms occurring post-vaccination as POTS. A more appropriate term for these symptoms could be "POTS-like[91]."
It is crucial to note that the general side effects that may occur after receiving a COVID vaccination, such as fatigue and headache, may resemble the symptoms of Postural Orthostatic Tachycardia Syndrome-like symptoms; Therefore, it is essential to distinguish between general vaccination-related adverse effects and symptoms similar to POTS-like symptoms. Taking into account the following points may aid clinicians in distinguishing between these two conditions.
While a few studies have noted POTS-like symptoms within a few hours to three days after receiving the COVID-19 vaccine, the majority of cases have been reported one week after the injection, particularly in those without preexisting medical conditions. A possible explanation for symptoms similar to POTS syndrome shortly after the vaccine injection is a history of prior Sars-Cov-2 infection, which prone the immune system react quickly to the vaccine. Another notice that could be helpful to consider is that adverse events such as presyncope and syncopal episodes in postural orthostatic tachycardia syndrome (POTS) are improbable following COVID-19 vaccination[92,93].
5. Conclusions
Given that POTS and POTS-like symptoms are potential complications of COVID-19 infection or vaccination and the complex diagnostic nature of this syndrome, which can lead to misdiagnosis or undiagnosed in numerous cases, it is imperative that clinicians remain aware of this condition and consider it along with other possible diagnoses. To ensure an accurate diagnosis of the syndrome in COVID-related settings, such as following COVID infection or vaccination, it is paramount that in addition to keeping in mind this possible diagnosis in suspicious individuals, a comprehensive history-taking and clinical examination as the most crucial diagnostic element along with other additional diagnostic workups should be considered.
Based on the available evidence, the following points can be mentioned in comparing POTS and POTS-like symptoms after the COVID-19 infection with post-covid-vaccine: POTS and related symptoms may manifest with a more extended latency following a Sars-Cov-2 infection than Covid vaccination. Notably, the incidence of this syndrome and its related symptoms is frequently observed in females gender, regardless of whether it follows a Covid infection or its vaccination; However, it does not seem that the occurrence of POTS is linked to the severity of the initial infection or the specific vaccine type used, as it has been reported in individuals with both mild and severe infections as well as after various types of vaccines.
Based on the currently available reports, it appears that the symptoms of POTS related to COVID-19, whether consequent to infection or vaccination, are not notably distinct from those of POTS unrelated to COVID-19 settings. Therefore, the diagnosis of COVID-19-related POTS does not differ significantly from that unrelated to COVID-19 and is based on the fulfillment of established diagnostic criteria. Even though some studies used interventions like EECP and plasma exchange for mitigating symptoms in POTS after COVID-19 infection or vaccination, the preponderance of reports revealed that conventional approaches commonly employed in non-COVID scenarios—including Lifestyle modifications and pharmacological therapies like beta-blockers—are potentially efficacious in ameliorating patients' symptoms.
While multiple studies have identified cases of POTS in COVID-related settings, some of these cases do not fully align with the classic criteria for diagnosing POTS in terms of symptom duration, hemodynamic or clinical criteria. To accurately determine the prevalence of POTS in COVID settings, clinicians must comprehensively understand the exact definition of POTS along with paying close attention to the points outlined in this study.
Author Contributions
Conceptualization, Z.M.A and E.H.; methodology, H.M and M.B.; validation, H.N.R and M.B.; formal analysis, A.B.; investigation, H.N.R and E.H.; resources, E.H.; data curation, H.M and M.B; writing—original draft preparation, Z.M.A and E.H.; writing—review and editing, H.M. and S.E; visualization, A.B.; supervision, E.H and S.E.; project administration, E.H and S.E.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Acknowledgments
The authors wish to thank the Clinical Research Development Center of Imam Reza Hospital of Kermanshah University of Medical Sciences and Infectious Diseases and Tropical Medicine Research Center of Babol University of Medical Sciences.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mohseni Afshar Z, Babazadeh A, Alizadeh Khatir A, Mohammadnia-Afrouzi M, Javanian M, Vasigala V, et al. Neurological manifestations in COVID-19: an overview. Minerva Pneumologica. 2021:52-8. [CrossRef]
- Afshar ZM, Babazadeh A, Javanian M, Ramezani E, Shemshadi R, Ebrahimpour S. A review of cardiac involvement in COVID-19 infection. Cor et Vasa. 2020;62(6):610-5. [CrossRef]
- Mohseni Afshar Z, Tavakoli Pirzaman A, Liang JJ, Sharma A, Pirzadeh M, Babazadeh A, et al. Do we miss rare adverse events induced by COVID-19 vaccination? Frontiers in medicine. 2022;9:933914.
- Mohseni Afshar Z, Babazadeh A, Janbakhsh A, Afsharian M, Saleki K, Barary M, et al. Vaccine-induced immune thrombotic thrombocytopenia after vaccination against Covid-19: a clinical dilemma for clinicians and patients. Reviews in medical virology. 2022;32(2):e2273. [CrossRef]
- Afshar ZM, Barary M, Babazadeh A, Hosseinzadeh R, Alijanpour A, Miri SR, et al. SARS-CoV-2-related and Covid-19 vaccine-induced thromboembolic events: A comparative review. Reviews in medical virology. 2022;32(4):e2327.
- Benrud-Larson LM, Dewar MS, Sandroni P, Rummans TA, Haythornthwaite JA, Low PA, editors. Quality of life in patients with postural tachycardia syndrome. Mayo Clinic Proceedings; 2002: Elsevier. [CrossRef]
- Bourne KM, Chew DS, Stiles LE, Shaw BH, Shibao CA, Okamoto LE, et al. Postural orthostatic tachycardia syndrome is associated with significant employment and economic loss. Journal of internal medicine. 2021;290(1):203-12. [CrossRef]
- Kesserwani H, Kesserwani HN. Postural orthostatic tachycardia syndrome misdiagnosed as anxiety: A case report with a review of therapy and pathophysiology. Cureus. 2020;12(10). [CrossRef]
- Maharaj N, Swarath S, Seecheran R, Seecheran V, Panday A, Seecheran N, et al. Suspected COVID-19 mRNA Vaccine-Induced Postural Orthostatic Tachycardia Syndrome. Cureus. 2023;15(1). [CrossRef]
- Raj SR, Guzman JC, Harvey P, Richer L, Schondorf R, Seifer C, et al. Canadian Cardiovascular Society position statement on postural orthostatic tachycardia syndrome (POTS) and related disorders of chronic orthostatic intolerance. Canadian Journal of Cardiology. 2020;36(3):357-72.
- Li H, Yu X, Liles C, Khan M, Vanderlinde-Wood M, Galloway A, et al. Autoimmune basis for postural tachycardia syndrome. Journal of the American Heart Association. 2014;3(1):e000755. [CrossRef]
- Raj SR, Biaggioni I, Yamhure PC, Black BK, Paranjape SY, Byrne DW, et al. Renin-aldosterone paradox and perturbed blood volume regulation underlying postural tachycardia syndrome. Circulation. 2005;111(13):1574-82.
- Garland E, Raj S, Black B, Harris P, Robertson D. The hemodynamic and neurohumoral phenotype of postural tachycardia syndrome. Neurology. 2007;69(8):790-8. [CrossRef]
- Fu Q, VanGundy TB, Galbreath MM, Shibata S, Jain M, Hastings JL, et al. Cardiac origins of the postural orthostatic tachycardia syndrome. Journal of the American College of Cardiology. 2010;55(25):2858-68. [CrossRef]
- Blitshteyn S, Whitelaw S. Postural orthostatic tachycardia syndrome (POTS) and other autonomic disorders after COVID-19 infection: a case series of 20 patients. Immunologic research. 2021;69(2):205-11.
- Watari M, Nakane S, Mukaino A, Nakajima M, Mori Y, Maeda Y, et al. Autoimmune postural orthostatic tachycardia syndrome. Annals of Clinical and Translational Neurology. 2018;5(4):486-92. [CrossRef]
- Celletti C, Camerota F, Castori M, Censi F, Gioffrè L, Calcagnini G, et al. Orthostatic intolerance and postural orthostatic tachycardia syndrome in joint hypermobility syndrome/Ehlers-Danlos syndrome, hypermobility type: neurovegetative dysregulation or autonomic failure? BioMed research international. 2017;2017. [CrossRef]
- Mannan H, Pain CM. Sex adjusted standardized prevalence ratios for celiac disease and other autoimmune diseases in patients with postural orthostatic tachycardia syndrome (POTS): A systematic review and meta-analysis. Heliyon. 2023. [CrossRef]
- Lei LY, Chew DS, Sheldon RS, Raj SR. Evaluating and managing postural tachycardia syndrome. Cleve Clin J Med. 2019;86(5):333-44. [CrossRef]
- Shaw B, Stiles L, Bourne K, Green E, Shibao C, Okamoto L, et al. The face of postural tachycardia syndrome–insights from a large cross-sectional online community-based survey. Journal of internal medicine. 2019;286(4):438-48.
- van Halteren AG, Tysma OM, van Etten E, Mathieu C, Roep BO. 1α, 25-Dihydroxyvitamin D3 or analogue treated dendritic cells modulate human autoreactive T cells via the selective induction of apoptosis. Journal of autoimmunity. 2004;23(3):233-9. [CrossRef]
- Arnold AC, Ng J, Raj SR. Postural tachycardia syndrome–diagnosis, physiology, and prognosis. Autonomic Neuroscience. 2018;215:3-11.
- Raj, SR. The postural tachycardia syndrome (POTS): pathophysiology, diagnosis & management. Indian pacing and electrophysiology journal. 2006;6(2):84.
- Vance H, Maslach A, Stoneman E, Harmes K, Ransom A, Seagly K, et al. Addressing post-COVID symptoms: a guide for primary care physicians. The Journal of the American Board of Family Medicine. 2021;34(6):1229-42. [CrossRef]
- Savytskyi IV, Pruc M, Malysz M, Maslyukov A, Szarpak L. Post-COVID-19 postural orthostatic tachycardia syndrome. Cardiology Journal. 2022;29(3):531-2.
- Raj SR, Fedorowski A, Sheldon RS. Diagnosis and management of postural orthostatic tachycardia syndrome. Cmaj. 2022;194(10):E378-E85.
- Grubb, BP. Autonomic Dysfunction as a Consequence of COVID-19 Infection: A New Twist on an Old Problem. American College of Cardiology Foundation Washington DC; 2022. p. 2331-2.
- Fedorowski A, Sutton R. Autonomic dysfunction and postural orthostatic tachycardia syndrome in post-acute COVID-19 syndrome. Nature Reviews Cardiology. 2023;20(5):281-2. [CrossRef]
- Kavi, L. Postural tachycardia syndrome and long COVID: an update. British Journal of General Practice; 2022. p. 8-9. [CrossRef]
- Miglis MG, Prieto T, Shaik R, Muppidi S, Sinn D-I, Jaradeh S. A case report of postural tachycardia syndrome after COVID-19. Clinical Autonomic Research. 2020;30(5):449-51. [CrossRef]
- Johnson JN, Mack KJ, Kuntz NL, Brands CK, Porter CJ, Fischer PR. Postural orthostatic tachycardia syndrome: a clinical review. Pediatric neurology. 2010;42(2):77-85. [CrossRef]
- Junghans-Rutelonis AN, Craner JR, Ale CM, Harbeck-Weber C, Fischer PR, Weiss KE. Youth with chronic pain and postural orthostatic tachycardia syndrome (POTS): treatment mediators of improvement in functional disability. Journal of clinical psychology in medical settings. 2018;25:471-84.
- Kanjwal K, Karabin B, Sheikh M, Elmer L, Kanjwal Y, Saeed B, et al. Pyridostigmine in the treatment of postural orthostatic tachycardia: A single-center experience. Pacing and clinical electrophysiology. 2011;34(6):750-5. [CrossRef]
- Gee ME, Watkins AK, Brown JN, Young EJ. Ivabradine for the treatment of postural orthostatic tachycardia syndrome: a systematic review. American Journal of Cardiovascular Drugs. 2018;18:195-204. [CrossRef]
- Schmidt LL, Karabin BL, Malone AC. Postural orthostatic tachycardia syndrome (POTS): assess, diagnose, and evaluate for POTS treatment (ADEPT). Integrative Medicine International. 2019;4(3-4):142-53. [CrossRef]
- Mehandru S, Merad M. Pathological sequelae of long-haul COVID. Nature immunology. 2022;23(2):194-202. [CrossRef]
- Szabo S, Zayachkivska O, Hussain A, Muller V. What is really ‘Long COVID’? Inflammopharmacology. 2023;31(2):551-7.
- Fernández-de-Las-Peñas, C. Long COVID: current definition. Infection. 2022;50(1):285-6. [CrossRef]
- Raj SR, Arnold AC, Barboi A, Claydon VE, Limberg JK, Lucci V-EM, et al. Long-COVID postural tachycardia syndrome: an American Autonomic Society statement. Clinical Autonomic Research. 2021;31(3):365-8.
- Ramakrishnan RK, Kashour T, Hamid Q, Halwani R, Tleyjeh IM. Unraveling the mystery surrounding post-acute sequelae of COVID-19. Frontiers in immunology. 2021;12:686029. [CrossRef]
- Chertow D, Stein S, Ramelli S, Grazioli A, Chung J, Singh M, et al. SARS-CoV-2 infection and persistence throughout the human body and brain. 2021.
- Parasa S, Desai M, Chandrasekar VT, Patel HK, Kennedy KF, Roesch T, et al. Prevalence of gastrointestinal symptoms and fecal viral shedding in patients with coronavirus disease 2019: a systematic review and meta-analysis. JAMA network open. 2020;3(6):e2011335-e.
- Su Y, Yuan D, Chen DG, Ng RH, Wang K, Choi J, et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell. 2022;185(5):881-95.e20. [CrossRef]
- Getts DR, Getts MT, King NJ, Miller SD. Infectious triggers of T cell autoimmunity. The autoimmune diseases: Elsevier; 2014. p. 263-74.
- Cervia C, Zurbuchen Y, Taeschler P, Ballouz T, Menges D, Hasler S, et al. Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome. Nature Communications. 2022;13(1):1-12. [CrossRef]
- Kell DB, Laubscher GJ, Pretorius E. A central role for amyloid fibrin microclots in long COVID/PASC: origins and therapeutic implications. Biochemical Journal. 2022;479(4):537-59. [CrossRef]
- Gaebler C, Wang Z, Lorenzi JC, Muecksch F, Finkin S, Tokuyama M, et al. Evolution of antibody immunity to SARS-CoV-2. Nature. 2021;591(7851):639-44.
- Lee S, Yoon GY, Myoung J, Kim S-J, Ahn D-G. Robust and persistent SARS-CoV-2 infection in the human intestinal brush border expressing cells. Emerging Microbes & Infections. 2020;9(1):2169-79.
- Gamage AM, Tan KS, Chan WO, Lew ZZR, Liu J, Tan CW, et al. Human nasal epithelial cells sustain persistent SARS-CoV-2 infection in vitro, despite eliciting a prolonged antiviral response. Mbio. 2022;13(1):e03436-21.
- Thoms M, Buschauer R, Ameismeier M, Koepke L, Denk T, Hirschenberger M, et al. Structural basis for translational shutdown and immune evasion by the Nsp1 protein of SARS-CoV-2. Science. 2020;369(6508):1249-55.
- Stukalov A, Girault V, Grass V, Karayel O, Bergant V, Urban C, et al. Multilevel proteomics reveals host perturbations by SARS-CoV-2 and SARS-CoV. Nature. 2021;594(7862):246-52.
- Yang B, Fan J, Huang J, Guo E, Fu Y, Liu S, et al. Clinical and molecular characteristics of COVID-19 patients with persistent SARS-CoV-2 infection. Nature Communications. 2021;12(1):3501.
- Moran E, Cook T, Goodman AL, Gupta RK, Jolles S, Menon DK, et al. Persistent SARS-CoV-2 infection: the urgent need for access to treatment and trials. The Lancet Infectious Diseases. 2021;21(10):1345-7.
- Espinosa-Gonzalez AB, Master H, Gall N, Halpin S, Rogers N, Greenhalgh T. Orthostatic tachycardia after COVID-19. Bmj. 2023;380. [CrossRef]
- Gunning III WT, Kvale H, Kramer PM, Karabin BL, Grubb BP. Postural orthostatic tachycardia syndrome is associated with elevated G-protein coupled receptor autoantibodies. Journal of the American Heart Association. 2019;8(18):e013602.
- Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nature medicine. 2021;27(4):601-15.
- Kwan AC, Ebinger JE, Wei J, Le CN, Oft JR, Zabner R, et al. Apparent risks of postural orthostatic tachycardia syndrome diagnoses after COVID-19 vaccination and SARS-Cov-2 Infection. Nature cardiovascular research. 2022;1(12):1187-94. [CrossRef]
- Kanjwal K, Jamal S, Kichloo A, Grubb BP. New-onset postural orthostatic tachycardia syndrome following coronavirus disease 2019 infection. The Journal of innovations in cardiac rhythm management. 2020;11(11):4302. [CrossRef]
- O'Sullivan JS, Lyne A, Vaughan CJ. COVID-19-induced postural orthostatic tachycardia syndrome treated with ivabradine. BMJ Case Reports CP. 2021;14(6):e243585. [CrossRef]
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nature Reviews Microbiology. 2023;21(3):133-46.
- Varanasi S, Sathyamoorthy M, Chamakura S, Shah SA. Management of long-COVID postural orthostatic tachycardia syndrome with enhanced external counterpulsation. Cureus. 2021;13(9). [CrossRef]
- Umapathi T, Poh MQ, Fan BE, Li KFC, George J, Tan JY. Acute hyperhidrosis and postural tachycardia in a COVID-19 patient. Clinical Autonomic Research. 2020;30:571-3. [CrossRef]
- Rudofker EW, Parker H, Cornwell III WK. An exercise prescription as a novel management strategy for treatment of long COVID. Case Reports. 2022;4(20):1344-7.
- Shouman K, Vanichkachorn G, Cheshire WP, Suarez MD, Shelly S, Lamotte GJ, et al. Autonomic dysfunction following COVID-19 infection: an early experience. Clinical Autonomic Research. 2021;31:385-94. [CrossRef]
- Desai AD, Boursiquot BC, Moore CJ, Gopinathannair R, Waase MP, Rubin GA, et al. Autonomic dysfunction post–acute COVID-19 infection. HeartRhythm Case Reports. 2022;8(3):143-6. [CrossRef]
- Agnihotri SP, Luis CVS, Kazamel M. Autonomic neuropathy as post-acute sequela of SARS-CoV-2 infection: a case report. Journal of NeuroVirology. 2022;28(1):158-61.
- Ocher RA, Padilla E, Hsu JC, Taub PR. Clinical and laboratory improvement in hyperadrenergic postural orthostatic tachycardia syndrome (POTS) after COVID-19 infection. Case Reports in Cardiology. 2021;2021. [CrossRef]
- Parker WH, Moudgil R, Wilson RG, Tonelli AR, Mayuga KA, Singh TK. COVID-19 and postural tachycardia syndrome: a case series. European Heart Journal-Case Reports. 2021;5(12):ytab325. [CrossRef]
- Jamal SM, Landers DB, Hollenberg SM, Turi ZG, Glotzer TV, Tancredi J, et al. Prospective evaluation of autonomic dysfunction in post-acute sequela of COVID-19. Journal of the American College of Cardiology. 2022;79(23):2325-30. [CrossRef]
- Kitsou V, Blomberg B, Lunde T, Saeed S. Intermittent left bundle branch block with septal flash and postural orthostatic tachycardia syndrome in a young woman with long COVID-19. BMJ Case Reports CP. 2022;15(6):e249608. [CrossRef]
- Johansson M, Ståhlberg M, Runold M, Nygren-Bonnier M, Nilsson J, Olshansky B, et al. Long-haul post–COVID-19 symptoms presenting as a variant of postural orthostatic tachycardia syndrome: the Swedish experience. Case Reports. 2021;3(4):573-80.
- Ishibashi Y, Yoneyama K, Tsuchida T, Akashi YJ. Post-COVID-19 postural orthostatic tachycardia syndrome. Internal Medicine. 2021;60(14):2345-. [CrossRef]
- Kalia R, Kalia R, Musih J, Cubelo M, Popat J. Post-COVID-19 syndrome: a novel diagnosis. Cureus. 2022;14(8).
- Bosco J, Titano R. Severe Post-COVID-19 dysautonomia: a case report. BMC Infectious Diseases. 2022;22(1):1-4. [CrossRef]
- Blitshteyn S, Fedorowski A. The risks of POTS after COVID-19 vaccination and SARS-CoV-2 infection: it’s worth a shot. Nature Cardiovascular Research. 2022;1(12):1119-20.
- Brinth LS, Pors K, Theibel AC, Mehlsen J. Orthostatic intolerance and postural tachycardia syndrome as suspected adverse effects of vaccination against human papilloma virus. Vaccine. 2015;33(22):2602-5. [CrossRef]
- Blitshteyn, S. Postural tachycardia syndrome after vaccination with Gardasil. European Journal Of Neurology:. 2010;17(7):e52. [CrossRef]
- Karimi Galougahi, K. Autonomic dysfunction post-inoculation with ChAdOx1 nCoV-19 vaccine. European Heart Journal-Case Reports. 2021;5(12):ytab472.
- Tsai C-K, Chu H, Cheng C-A. Novel H1N1 influenza vaccine the cause of postural orthostatic tachycardia syndrome followed by cerebral hypoperfusion. Journal of Medical Sciences. 2011;31(2):91-3.
- Blitshteyn S, Brook J. Postural tachycardia syndrome (POTS) with anti-NMDA receptor antibodies after human papillomavirus vaccination. Immunologic research. 2017;65:282-4. [CrossRef]
- Schelke MW, Barcavage S, Lampshire E, Brannagan III TH. Post–COVID-19 vaccine small-fiber neuropathy and tinnitus treated with plasma exchange. Muscle & Nerve. 2022;66(4):E21.
- Sanada Y, Azuma J, Hirano Y, Hasegawa Y, Yamamoto T, Hirano Sr Y. Overlapping myocarditis and postural orthostatic tachycardia syndrome after COVID-19 messenger RNA vaccination: a case report. Cureus. 2022;14(11).
- Eldokla AM, Numan MT. Postural orthostatic tachycardia syndrome after mRNA COVID-19 vaccine. Clinical Autonomic Research. 2022;32(4):307-11. [CrossRef]
- Park J, Kim S, Lee J, An JY. A case of transient POTS following COVID-19 vaccine. Acta Neurologica Belgica. 2022;122(4):1081-3. [CrossRef]
- Reddy S, Reddy S, Arora M. A case of postural orthostatic tachycardia syndrome secondary to the messenger RNA COVID-19 vaccine. Cureus. 2021;13(5).
- Hermel M, Sweeney M, Abud E, Luskin K, Criado JP, Bonakdar R, et al. COVID-19 vaccination might induce postural orthostatic tachycardia syndrome: a case report. Vaccines. 2022;10(7):991. [CrossRef]
- Carroll HA, Millar E, Deans KA. Vitamin B12 and D deficiency as cofactors of COVID-19 vaccine-induced chronic neurological adverse reactions: Two cases and a hypothesis. 2022.
- Safavi F, Gustafson L, Walitt B, Lehky T, Dehbashi S, Wiebold A, et al. Neuropathic symptoms with SARS-CoV-2 vaccination. MedRxiv. 2022.
- Mustafa HI, Garland EM, Biaggioni I, Black BK, Dupont WD, Robertson D, et al. Abnormalities of angiotensin regulation in postural tachycardia syndrome. Heart Rhythm. 2011;8(3):422-8. [CrossRef]
- Rubin, R. Large cohort study finds possible association between postural orthostatic tachycardia syndrome and COVID-19 vaccination but far stronger link with SARS-CoV-2 infection. JAMA. 2023;329(6):454-6.
- Tv P, Tran TT, Hao HT, Hau NTH, Jain N, Reinis A. Postural orthostatic tachycardia syndrome-like symptoms following COVID-19 vaccination: An overview of clinical literature. Human Antibodies. 2023(Preprint):1-9. [CrossRef]
- Im JH, Kim E, Lee E, Seo Y, Lee Y, Jang Y, et al. Adverse events with the Pfizer-BioNTech COVID-19 vaccine among Korean healthcare workers. Yonsei Medical Journal. 2021;62(12):1162.
- Dighriri IM, Alhusayni KM, Mobarki AY, Aljerary IS, Alqurashi KA, Aljuaid FA, et al. Pfizer-BioNTech COVID-19 vaccine (BNT162b2) side effects: a systematic review. Cureus. 2022;14(3).
Figure 1.
Schematic suggested approach to POTS diagnosis following COVID-19 infection. It was adapted from the Canadian Cardiovascular Society Position Statement on Postural Orthostatic Tachycardia Syndrome 2020 [10]. Abbreviations: POTS, postural orthostatic tachycardia syndrome; PSWT, postural symptoms without tachycardia; IST, Inappropriate sinus tachycardia; PTOC, postural tachycardia of other cause; POTS plus, postural orthostatic tachycardia syndrome with associated comorbidities; PSWT plus, postural symptoms without tachycardia with associated comorbidities.
Figure 1.
Schematic suggested approach to POTS diagnosis following COVID-19 infection. It was adapted from the Canadian Cardiovascular Society Position Statement on Postural Orthostatic Tachycardia Syndrome 2020 [10]. Abbreviations: POTS, postural orthostatic tachycardia syndrome; PSWT, postural symptoms without tachycardia; IST, Inappropriate sinus tachycardia; PTOC, postural tachycardia of other cause; POTS plus, postural orthostatic tachycardia syndrome with associated comorbidities; PSWT plus, postural symptoms without tachycardia with associated comorbidities.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



