Submitted:
13 October 2023
Posted:
13 October 2023
You are already at the latest version
Abstract
Background: Lung cancer is still the most lethal malignancy in the world from the report of Cancer Statistics in 2021. Platinum-based chemotherapy combined immunotherapy is the first-line treatment in lung cancer patients. However, the 5-year survival rate always affected by the adverse reaction and drug resistance caused by platinum-based chemotherapy. DNA damage and repair system is one of the important mechanisms which can affect the response to chemotherapy and clinical outcome in lung cancer patients.
Objective: The objective of this study is to find the relationship between the polymorphisms of DNA repair genes with the prognosis in platinum-based chemotherapy in lung cancer patients.
Patients and Methods: We performed genotyping in 17 single nucleotide polymorphisms (SNPs) of Excision Repair Cross-Complementation group (ERCC) genes and X-ray Repair Cross-Complementing (XRCC) genes of 345 lung cancer patients by Sequenom MassARRAY. We used Cox proportional hazard models, state and plink to analyze the associations between SNPs and the prognosis of lung cancer patients.
Results: We found that the ERCC5 rs873601 was associated with the overall survival time in lung cancer patients treat by platinum-based chemotherapy (p=0.031*). We also discovered that the polymorphisms in rs873601 was significantly associated with the prognosis in age more than 55 years, Small Cell Lung Cancer (SCLC) and smoking patients, Long Intergenic Non-protein Coding RNA (PNKY) rs2444933 in age less than 55 years, SCLC, metastasis and stage III/IV/ED patients, Short Tau Inversion Recovery (STIR1) rs3740051 in SCLC and metastasis patients, PNKY rs1869641 in SCLC patients, XRCC5 rs1051685 in non-metastasis patients, respectively.
Conclusion: The ERCC5 rs873601(G>A) maybe a valuable biomarker for predicting the prognosis in lung cancer patients treated with platinum-based chemotherapy.
Statements and Declarations: The authors declare that they have no conflict of interest.
Keywords:
lung cancer
; platinum-based chemotherapy
; ERCC5
; Genetic polymorphism
; prognosis
Introduction
Lung cancer is one of the leading cancer types and the highest lethal malignancies in the world [1]. It consists of Small Cell Lung Cancer (SCLC) and Non-Small Cell Lung Cancer (NSCLC), NSCLC account for almost 80% for the lung cancer cases, including adenocarcinoma, squamous cell cancer and large cell lung cancer [2]. The treatment strategy of lung cancer consists of surgery, radiation oncology, chemotherapy, immunotherapy and targeted therapy [3]. Despite the progress of immunotherapy and targeted therapy in the past years, platinum-based chemotherapy combined immunotherapy is still the first-line treatment for lung cancer patients [4]. The 5-year survival is a crucial indicator for the treatment efficacy [5]. The occurrence of drug-resistance and treatment toxicity creates substantial barriers to disease control, such as gastrointestinal toxicity and hematological toxicity, which result in a poor 5-year survival [6]. It’s remarkable that the chemotherapy outcomes differ from individuals, which means the genetic polymorphisms may play an important role in the efficacy of chemotherapy treatment [7]. Until now, more and more genetic polymorphisms have been found to be associated with the outcomes of chemotherapy, such as Eukaryotic translation Initiation Factor 3 subunit A (eIF3A), Rac family small GTPase 1 (RAC1), WNT1 Inducible Signaling Pathway protein 1 (WISP1) and so on [8,9,10]. The specific mechanisms are still discovering on the way.
As we all know, DNA damage and repair pathway is of great importance in heath and disease [11]. DNA damage can be classified into two main categories based on its origin: endogenous and exogenous [12]. DNA damage and repair pathway can prevent DNA damage from causing mutations and cytotoxicity, but the unbalanced repair of DNA damage always leads to the development of tumors [13,14]. It has been reported that the genetic polymorphisms of DNA repair pathways can significantly affect the response to cisplatin treatment in lung cancer patients [15,16]. The DNA damage and repair pathway are consist of mismatch repair (MMR), base excision repair (BER), nucleotide excision repair (NER) and double-strand break (DSB) repair systems [17].
The Excision Repair Cross-Complementation 5 (ERCC5), also called as Xeroderma Pigmentosum Group (XPG), is a gene performing its function in nucleotide excision repair (NER), and it can also protect replication forks by promoting homologous recombination [18]. ERCC5 contains 17 exons, spans 32 kb with a location of chromosome 13q33.1 [19]. It plays an essential role in the occurrences and clinical outcomes of lung cancer. The ERCC5 rs4771436 and rs1047768 genotypes have been found to be associate with the risk of lung cancer [20]. The ERCC5 His46His genomic polymorphisms can significantly affect the response to chemotherapy in advanced NSCLC patients [21].
The Xeroderma Pigmentosum group A (XPA) is another key member of NER, it can catch the damage site of the DNA substrate through binding the NER core repair factors [22]. It is also reported to be connected with the development and efficacy of lung cancer. XPA rs1800975 polymorphisms has been found to be associated with the susceptibility in lung cancer patients [23]. The genomic variabilities of XPA rs2808668 is also considered to jointly contribute to lung cancer risk [24]. The mutation of XPA rs3176658 is significantly associate with the progress free survival in NSCLC patients [25].
The other genes of NER are also reported to play vital roles in lung cancer occurrences and clinical outcomes. The single nucleotide polymorphisms of XRCC3 rs861539 is related to the prognosis of NSCLC patients [26]. The variables of XRCC5 (rs1051685, rs6941) were associated with hematologic toxicity in lung cancer patients treat with platinum-based chemotherapy, which means it can predict the platinum-based chemotherapy toxicity in lung cancer patients [27]. The expression of ERCC1 may be a useful prognostic marker in lung adenocarcinoma, the lower expression had a longer overall survival [28]. And patients with the C/C genotype in rs3212986 of the ERCC1 gene had longer median progress free survival in NSCLC patients [29].
In this study, we selected 17 SNPs from ERCC5, PNKY, ERCC1, SIRT1, XPA, XRCC3 and XRCC5, such as rs873601, rs2444933, rs3740051, rs1869641, rs1051685 and so on. The rs873601 has been reported to be associated with cancer susceptibility [30]. The rs3740051 plays an important role in the development of pituitary adenoma [31]. The transporter genes polymorphisms of rs1869641 have been reported to show significant relation to chemotherapy response [32]. The rs1051685 was reported to associated with the response and survival in relapsed or refractory multiple myeloma patients [33]. Based on the previous study, we aim to find the new biomarkers to predict the efficacy in lung cancer patients, which can make forward to a more intensive guidance in the clinical diagnosis and treatment.
Material and Methods
Research Objects and Treatment Procedures
All the subjects enrolled were selected by the following conditions: (1) Patients who were in diagnosed of lung cancer for the first time at Xiangya Hospital of Central South University or Hunan province of Cancer Hospital (Changsha, Hunan, China) between August 2009 and January 2013; (2) Patients didn’t receive surgery treatment before palatinum-based chemotherapy. (3) All the patients should receive at least 2 periods of platinum-based chemotherapy. The clinical characteristics of the enrolled subjects are listed in Table 1. All the patients should write the approved informed consent before they participated in this study. The investigation protocol was approved by the Ethics Committee of Xiangya School of Medicine, Central South University, with a registration number of CTXY-110008-1.
Data Collection
The deadline for patients recruited was July 15, 2019. Their survival data were collected by telephone follow-up or residence registration. The endpoint criteria were progress-free survival (PFS) and overall survival (OS). The progress-free survival (PFS) was according to the date diagnosed of lung cancer and the date of the first local recurrence or metastases in the last follow-up. The overall survival (OS) time was calculated form the time between diagnosed of lung cancer and the date of the last follow-up or death. Patients without progression will be defined as censor when analyzed. As researchers, the polymorphisms of the patients were unknown before the sequencing analysis.
SNP Selecting, DNA Extraction and Genotyping
There were 17 common SNPs of DNA damage and repair genes selected in our study (Table 2). The candidate SNPs were located from 5 kb upstream of the first exon to the downstream of the last exon respectively. We used Haploview version 4.2 to choose the Haplotype tagging SNPs. And all the selected SNPs must satisfy the condition that the minor allele frequency (MAF)>0.05 in the HapMap CHB population. The DNA we used for genotyping was separated from a 5ml external blood sample using FlexiGene DNA Kit (Qiagen, Hilden, Germany). And all the samples were stored at 4°C before using. Genotyping was conducted by Sequenom’s MassARRAY system (Sequenom, San Diego, California, USA).
Statistical Analysis
We used Cox proportional hazard models to analyze the differences in the variables, as histology, age, clinical stage, smoking status, gender and metastasis between the PFS and OS. We used forward stepwise method of Cox proportional hazard models to find the covariates. Variables which were significantly associated with OS or PFS were considered as the covariates in the specific subgroup. And then, we fit the covariates into multivariate logistic regression model to adjust the covariates, through the command of --covar in PLINK. The p value was 2-sided and p<0.05 will be considered as statistically significant. All association analyses were conducted by three models including additive, dominant, and recessive. The additive model is for the additive effects of SNPs. It means that, if D is a minor allele and d is the major allele, the additive model means DD versus Dd versus dd. Dominant and recessive models are tests for the minor allele with two of the classes pooled. The dominant model means (DD, Dd) versus dd, and the recessive model means DD versus (Dd, dd). The aforementioned statistical analyses were performed using PLINK (ver 1.07, http://pngu.mgh.harvard.edu/purcell/plink/) and SPSS 18.0 (SPSS Inc, Chicago, Illinois, USA)
Results
Distribution of Characteristics in Lung Cancer Patients and Prognosis Analysis
The demographic characteristics and prognosis consequences for the 345 lung cancer patients were provided in Table 3. The majority of these patients were NSCLC (67.5%), compared with SCLC (28.7%). The median age was 56 years old. Most of them were diagnosed at advanced time, III/IV/ED (86.4%), contrast to I/II/LD (11.9%). More than half of the patients were smokers (64.6%) with a non-smoking proportion (35.4%). Most patients were male (82.6%) versus female (17.4%). The patients with metastasis were 43.2%, and without metastasis were 17.7%. The median survival time of overall survival (MST-OS) is 4.42 year, and the median survival time of progression free survival (MST-PFS) is 3.16 year. The other statistics of the clinical outcomes in the above subgroups were also summarized in Table 3.
Association between the Polymorphisms and Prognosis in the Lung Cancer Patients
As we analyzed, the genomic polymorphisms ERCC5 rs873601 (G>A) was significantly associated with the overall survival (OS) of lung cancer patients in recessive model (p=0.031). Which means patients carry the ERCC5 rs873601 GG genotype had a shorter MST-OS than the patients who have the ERCC5 rs873601 GA or AA genotypes (MST-OS: 3.28, 4.88, 4.02 years, respectively) (Table 4). In conclusion, patients who carry the allele A of ERCC5 rs873601 are the protective allele in the prognosis of lung cancer treated with platinum-based chemotherapy (Figure 1).
Stratification Analyses of Association between Polymorphisms and Prognosis in Lung Cancer Patients
To further elucidate the association between these SNPs and the prognosis in lung cancer patients, we also performed subgroup analysis based on age, gender, smoking status, histology, clinical stage and metastasis. As shown in Table 5, the ERCC5 rs873601 was related to overall survival in additive and recessive model in age>56 years lung cancer patients (Additive model: p=0.032; Recessive model: p=0.004) and smoker patients in additive and recessive model (Additive model: p=0.048; Recessive model: p=0.018). The PNKY rs2444933 was significantly associated with the overall survival in age≤56 (Additive model: p=0.043; Recessive model: p=0.036), metastasis (Additive model: p=0.019; Recessive model: p=0.035), non-smoking (Recessive model: p=0.042) and III/IV/ED (Additive model: p=0.040) patients. What’s more, the STIR1 rs3740051 polymorphisms in SCLC (Additive model: p=0.018; Dominant model: p=0.023) and metastasis (Additive model: p=0.048) patients was significantly associated with the overall survival (Figure 2).
We also analyzed the association between the genomic polymorphisms with progress free survival (PFS) in subgroups. The polymorphisms of ERCC5 rs873601 (Additive model: p=0.031; Dominant model: p=0.027), PNKY rs2444933 (Recessive model: p=0.007) and PNKY rs1869641 (Recessive model: p=0.028) were significantly associated with the PFS in SCLC patients. The XRCC5 rs1051685 were significantly associated with the PFS in non-metastasis patients in additive and dominant models (Additive model: p=0.037; Dominant model: p=0.037) (Figure 3).
As we showed in Figure 4, the main finding of our study was the polymorphisms of ERCC5 rs873601 play an important role in the prognosis of lung cancer patients treated with platinum-based chemotherapy. The mechanism of which is also valuable to be discussed. The rs873601 is a 3_prime_UTR_variant in ERCC5, it may affect the translation of mRNA of ERCC5, the RNA-binding protein (RBP) and the protein-to-protein interaction. ERCC5 can regulate the NER pathway of DNA damage and repair, which have been reported to be significantly associated with the prognosis of lung cancer patients treated with platinum-based chemotherapy. ERCC5 may be a potential therapeutic target in the treatment of lung cancer patients, which is valuable to be further investigated.
Discussion
As a crucial member of DNA damage and repair system, there are plenty of reports about ERCC5 and lung cancer. The ERCC5 polymorphisms of rs2016073, rs4771436, rs11069498 and rs4150330 were significantly associated with NSCLC risk, the ERCC5 rs4771436 was also significantly correlated with the reduced risk of toxicity in Chineses NSCLC patients [34]. In the other investigation, ERCC5 rs4771436 and rs1047768 genotypes were reported to be associated with an increased risk of lung cancer patients [20]. What’s more, there was a study in North Indians found that the ERCC5 rs751402 polymorphisms was significantly related to the risk in NSCLC patients [35]. In other population of coal-mining region, the genomic variants of ERCC5 rs17655 was associated with lung cancer risk significantly [36]. There were also investigations about ERCC5 and lung cancer prognosis, ERCC5 (rs2094258 and rs2296147) was reported to be related with progression-free survival (PFS) in NSCLC patients treated with platinum-based chemotherapy [37]. It has been also found that the ERCC5 rs751402 genotype was associated with the treatment response in patients with advanced non-small-cell lung cancer treated with platinum-based chemotherapy [38]. The SNPs of ERCC5 in Nucleotide Excision Repair (NER) pathway genes were correlated with toxicity treated with double chemotherapy in advanced NSCLC patients [39]. These all mean that the polymorphisms in DNA repair genes are significantly related to the risk of lung cancer, and play an important role in the occurrence of lung cancer.
As we all know, Human Epidermal growth factor Receptor 2 (HER2/ERBB2) and Epidermal Growth Factor Receptor (EGFR) are two crucial biomarkers in the prognosis of lung cancer [40,41]. These biomarkers are often used for screening, detection, diagnosis, prognosis, prediction and monitoring of cancer development [42]. It has been reported that the adverse drug reaction (ADR) in HER2 (+) patients with Grade 3 or 4 was significantly higher than that in the control group in NSCLC patients [43]. EGFR tyrosine kinase inhibitors (TKI) is an important treatment regimen for lung cancer patients, however, up to 50% of patients treated with first- and second-generation TKIs develop an EGFR exon 20 T790M mutation at the time of progression, which may lead to a treatment failure in these patients [44]. To find the new biomarkers for lung cancer patients is of great importance. ERCC5 as an important component in the repair pathway of platinum-induced damage, plays an important role in the prognosis of lung cancer patients [45]. The polymorphisms of ERCC5 have been reported to be associated with the risk of NSCLC [46]. ERCC5 may become a potential therapeutic target for the treatment in lung cancer patients, as important as HER2 and EGFR.
We also found the PNKY rs2444933 and rs1869641 were associated with the prognosis in lung cancer patients through the stratified analysis. Most report of PNKY was about its function in brain, there are several investigations about its role in cancer. It has been found that PNKY can inhibit the binding of miR124 to Polypyrimidine Tract-Binding Protein 1 (PTBP1) and maintained the homeostasis of choroidal vascular function [47]. PNKY may control the resistance of platinum-based chemotherapy through the regulation of the maintain of choroidal vascular. STIR1 rs3740051 and XRCC5 rs1051685 polymorphisms were associated with the prognosis significantly in lung cancer patients treated with platinum-based chemotherapy. STIR1 was reported to be related with immune evasion, which may be essential to maintain their stability [48]. STIR1 may play an important role in lung cancer survival through its regulation in immune evasion. XRCC5 was overexpressed in lung adenocarcinoma, it may be a risk factor and it can also predict a poor prognosis in lung adenocarcinoma patients [49]. The other investigation also found that XRCC5 was independent risk factors affecting the prognosis of lung adenocarcinoma patients [50]. It was also reported that the transcriptional overexpression of XRCC5 showed significant correlation with a shorter patients' outcome in advanced lung cancer patients [51].
Our study investigated the association between the polymorphisms of DNA repair gene, PNKY and STIR1 with the prognosis in Chinese lung cancer patients treated with platinum-based chemotherapy. And we also stratified these polymorphisms in age, gender, smoking, histology, clinical stage and metastasis. However, there were several limitations in our study. First, the simple size of our study was not large enough, we just enrolled 345 patients in our project. Second, the biological function mechanisms of these SNPs need further study in vitro. Finally, the validation of our results needs replication studies with other independent subjects.
In conclusion, the variants of ERCC5 rs873601 was significantly associated with the prognosis in lung cancer patients treated with platinum-based chemotherapy. Patients carry the ERCC5 rs873601 A allele may have a longer overall survival (OS) than G allele. The genotypes of ERCC5 rs873601 may be an attractive biomarker used to predict the prognosis of lung cancer patients treated with platinum-based chemotherapy.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (82173901), Major Project of Natural Science Foundation of Hunan Province (Open competition, 2021 JC0002), and Major Science and Technology Program of Changsha(kh2003010).
Disclosure Statement
The authors declare that they have no conflict of interest.
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J Clin 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Roy-Chowdhuri, S. Molecular Pathology of Lung Cancer. Surg Pathol Clin 2021, 14, 369–377. [Google Scholar] [CrossRef]
- Vrana, D. Advances in the therapy of small cell lung cancer. Klin Onkol 2021, 34, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.; Hanna, N. Advances in systemic therapy for non-small cell lung cancer. BMJ 2021, 375, n2363. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C. [Advances in Lung Cancer Treatment]. Dtsch Med Wochenschr 2021, 146, 1283–1286. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, H.; Lee, B.; Lee, S.H.; Sun, J.M.; Park, W.Y.; Ahn, J.S.; Ahn, M.J.; Park, K. DNA Damage Response and Repair Pathway Alteration and Its Association With Tumor Mutation Burden and Platinum-Based Chemotherapy in SCLC. J Thorac Oncol 2019, 14, 1640–1650. [Google Scholar] [CrossRef] [PubMed]
- Ge, F.; Huo, Z.; Li, C.; Wang, R.; Wang, R.; Liu, Y.; Chen, J.; Lu, Y.; Wen, Y.; Jiang, Y.; et al. Lung cancer risk in patients with multiple sclerosis: A Mendelian randomization analysis. Mult Scler Relat Disord 2021, 51, 102927. [Google Scholar] [CrossRef]
- Yin, J.Y.; Zhang, J.T.; Zhang, W.; Zhou, H.H.; Liu, Z.Q. eIF3a: A new anticancer drug target in the eIF family. Cancer Lett 2018, 412, 81–87. [Google Scholar] [CrossRef]
- Zou, T.; Yin, J.; Zheng, W.; Xiao, L.; Tan, L.; Chen, J.; Wang, Y.; Li, X.; Qian, C.; Cui, J.; et al. Rho GTPases: RAC1 polymorphisms affected platinum-based chemotherapy toxicity in lung cancer patients. Cancer Chemother Pharmacol 2016, 78, 249–258. [Google Scholar] [CrossRef]
- He, J.; Wang, Z.; Wang, Y.; Zou, T.; Li, X.P.; Cao, L.; Chen, J. The Effects of WISP1 Polymorphisms on the Prognosis of Lung Cancer Patients with Platinum-Based Chemotherapy. Pharmgenomics Pers Med 2021, 14, 1193–1203. [Google Scholar] [CrossRef]
- Schumacher, B.; Pothof, J.; Vijg, J.; Hoeijmakers, J.H.J. The central role of DNA damage in the ageing process. Nature 2021, 592, 695–703. [Google Scholar] [CrossRef]
- Ashour, M.E.; Mosammaparast, N. Mechanisms of damage tolerance and repair during DNA replication. Nucleic Acids Res 2021, 49, 3033–3047. [Google Scholar] [CrossRef] [PubMed]
- Kay, J.; Thadhani, E.; Samson, L.; Engelward, B. Inflammation-induced DNA damage, mutations and cancer. DNA Repair (Amst) 2019, 83, 102673. [Google Scholar] [CrossRef] [PubMed]
- Paull, T.T. DNA damage and regulation of protein homeostasis. DNA Repair (Amst) 2021, 105, 103155. [Google Scholar] [CrossRef]
- Pilger, D.; Seymour, L.W.; Jackson, S.P. Interfaces between cellular responses to DNA damage and cancer immunotherapy. Genes Dev 2021, 35, 602–618. [Google Scholar] [CrossRef]
- Dai, C.H.; Li, J.; Chen, P.; Jiang, H.G.; Wu, M.; Chen, Y.C. RNA interferences targeting the Fanconi anemia/BRCA pathway upstream genes reverse cisplatin resistance in drug-resistant lung cancer cells. J Biomed Sci 2015, 22, 77. [Google Scholar] [CrossRef]
- Gorbunova, V.; Seluanov, A.; Mao, Z.; Hine, C. Changes in DNA repair during aging. Nucleic Acids Res 2007, 35, 7466–7474. [Google Scholar] [CrossRef]
- Muniesa-Vargas, A.; Theil, A.F.; Ribeiro-Silva, C.; Vermeulen, W.; Lans, H. XPG: A multitasking genome caretaker. Cell Mol Life Sci 2022, 79, 166. [Google Scholar] [CrossRef]
- Kiyohara, C.; Yoshimasu, K. Genetic polymorphisms in the nucleotide excision repair pathway and lung cancer risk: A meta-analysis. Int J Med Sci 2007, 4, 59–71. [Google Scholar] [CrossRef]
- Lan, X.; Li, Y.; Wu, Y.; Li, X.; Xu, L. The Association of ERCC1 and ERCC5 Polymorphisms with Lung Cancer Risk in Han Chinese. J Cancer 2022, 13, 517–526. [Google Scholar] [CrossRef]
- Liu, D.; Wu, J.; Shi, G.Y.; Zhou, H.F.; Yu, Y. Role of XRCC1 and ERCC5 polymorphisms on clinical outcomes in advanced non-small cell lung cancer. Genet Mol Res 2014, 13, 3100–3107. [Google Scholar] [CrossRef]
- Pradhan, S.; Sarma, H.; Mattaparthi, V.S.K. Investigation of the probable homo-dimer model of the Xeroderma pigmentosum complementation group A (XPA) protein to represent the DNA-binding core. J Biomol Struct Dyn 2019, 37, 3322–3336. [Google Scholar] [CrossRef]
- Yuan, M.; Yu, C.; Yu, K. Association of human XPA rs1800975 polymorphism and cancer susceptibility: An integrative analysis of 71 case-control studies. Cancer Cell Int 2020, 20, 164. [Google Scholar] [CrossRef]
- Mei, C.; Hou, M.; Guo, S.; Hua, F.; Zheng, D.; Xu, F.; Jiang, Y.; Li, L.; Qiao, Y.; Fan, Y.; et al. Polymorphisms in DNA repair genes of XRCC1, XPA, XPC, XPD and associations with lung cancer risk in Chinese people. Thorac Cancer 2014, 5, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Wang, S.; Hong, X.; Li, X.; Zhao, X.; Huai, C.; Chen, H.; Gao, Z.; Qian, J.; Wang, J.; et al. Single nucleotide polymorphisms of nucleotide excision repair pathway are significantly associated with outcomes of platinum-based chemotherapy in lung cancer. Sci Rep 2017, 7, 11785. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Zhang, H.; Xu, F.; Kong, J.; Yu, H.; Qian, B. DNA Repair Gene Polymorphisms in Relation to Non-Small Cell Lung Cancer Survival. Cell Physiol Biochem 2015, 36, 1419–1429. [Google Scholar] [CrossRef]
- Chen, J.; Wu, L.; Wang, Y.; Yin, J.; Li, X.; Wang, Z.; Li, H.; Zou, T.; Qian, C.; Li, C.; et al. Effect of transporter and DNA repair gene polymorphisms to lung cancer chemotherapy toxicity. Tumour Biol 2016, 37, 2275–2284. [Google Scholar] [CrossRef]
- Piljic Burazer, M.; Mladinov, S.; Matana, A.; Kuret, S.; Bezic, J.; Glavina Durdov, M. Low ERCC1 expression is a good predictive marker in lung adenocarcinoma patients receiving chemotherapy based on platinum in all TNM stages—A single-center study. Diagn Pathol 2019, 14, 105. [Google Scholar] [CrossRef]
- Grenda, A.; Blach, J.; Szczyrek, M.; Krawczyk, P.; Nicos, M.; Kuznar Kaminska, B.; Jakimiec, M.; Balicka, G.; Chmielewska, I.; Batura-Gabryel, H.; et al. Promoter polymorphisms of TOP2A and ERCC1 genes as predictive factors for chemotherapy in non-small cell lung cancer patients. Cancer Med 2020, 9, 605–614. [Google Scholar] [CrossRef]
- Huang, J.; Liu, X.; Tang, L.L.; Long, J.T.; Zhu, J.; Hua, R.X.; Li, J. XPG gene polymorphisms and cancer susceptibility: Evidence from 47 studies. Oncotarget 2017, 8, 37263–37277. [Google Scholar] [CrossRef] [PubMed]
- Liutkeviciene, R.; Vilkeviciute, A.; Morkunaite, G.; Glebauskiene, B.; Kriauciuniene, L. SIRT1 (rs3740051) role in pituitary adenoma development. BMC Med Genet 2019, 20, 185. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yin, J.Y.; Li, X.P.; Chen, J.; Qian, C.Y.; Zheng, Y.; Fu, Y.L.; Chen, Z.Y.; Zhou, H.H.; Liu, Z.Q. The association of transporter genes polymorphisms and lung cancer chemotherapy response. PLoS ONE 2014, 9, e91967. [Google Scholar] [CrossRef] [PubMed]
- Cibeira, M.T.; de Larrea, C.F.; Navarro, A.; Diaz, T.; Fuster, D.; Tovar, N.; Rosinol, L.; Monzo, M.; Blade, J. Impact on response and survival of DNA repair single nucleotide polymorphisms in relapsed or refractory multiple myeloma patients treated with thalidomide. Leuk Res 2011, 35, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Xu, B.; Lin, D.; Tan, W.; Leaw, S.; Hong, X.; Hu, X. XRCC1 polymorphisms and severe toxicity in lung cancer patients treated with cisplatin-based chemotherapy in Chinese population. Lung Cancer 2008, 62, 99–104. [Google Scholar] [CrossRef]
- Bhat, G.R.; Sethi, I.; Bhat, A.; Verma, S.; Bakshi, D.; Sharma, B.; Nazir, M.; Dar, K.A.; Abrol, D.; Shah, R.; et al. Genetic evaluation of the variants using MassARRAY in non-small cell lung cancer among North Indians. Sci Rep 2021, 11, 11291. [Google Scholar] [CrossRef]
- Minina, V.I.; Bakanova, M.L.; Soboleva, O.A.; Ryzhkova, A.V.; Titov, R.A.; Savchenko, Y.A.; Sinitsky, M.Y.; Voronina, E.N.; Titov, V.A.; Glushkov, A.N. Polymorphisms in DNA repair genes in lung cancer patients living in a coal-mining region. Eur J Cancer Prev 2019, 28, 522–528. [Google Scholar] [CrossRef]
- Perez-Ramirez, C.; Canadas-Garre, M.; Molina, M.A.; Robles, A.I.; Faus-Dader, M.J.; Calleja-Hernandez, M.A. Contribution of genetic factors to platinum-based chemotherapy sensitivity and prognosis of non-small cell lung cancer. Mutat Res Rev Mutat Res 2017, 771, 32–58. [Google Scholar] [CrossRef]
- He, C.; Duan, Z.; Li, P.; Xu, Q.; Yuan, Y. Role of ERCC5 promoter polymorphisms in response to platinum-based chemotherapy in patients with advanced non-small-cell lung cancer. Anticancer Drugs 2013, 24, 300–305. [Google Scholar] [CrossRef]
- Zhang, L.; Gao, G.; Li, X.; Ren, S.; Li, A.; Xu, J.; Zhang, J.; Zhou, C. Association between single nucleotide polymorphisms (SNPs) and toxicity of advanced non-small-cell lung cancer patients treated with chemotherapy. PLoS ONE 2012, 7, e48350. [Google Scholar] [CrossRef]
- Landi, L.; Cappuzzo, F. HER2 and lung cancer. Expert Rev Anticancer Ther 2013, 13, 1219–1228. [Google Scholar] [CrossRef]
- Leonetti, A.; Sharma, S.; Minari, R.; Perego, P.; Giovannetti, E.; Tiseo, M. Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer. Br J Cancer 2019, 121, 725–737. [Google Scholar] [CrossRef]
- Sharma, B.; Kanwar, S.S. Phosphatidylserine: A cancer cell targeting biomarker. Semin Cancer Biol 2018, 52, 17–25. [Google Scholar] [CrossRef]
- Diao, W.Y.; Ding, C.L.; Yuan, B.Y.; Li, Z.; Sun, N.; Huang, J.B. Clinical Characteristics and Prognosis of HER2 Gene Phenotype in Patients with Non-Small Cell Lung Cancer. Int J Gen Med 2021, 14, 9153–9161. [Google Scholar] [CrossRef] [PubMed]
- Baraibar, I.; Mezquita, L.; Gil-Bazo, I.; Planchard, D. Novel drugs targeting EGFR and HER2 exon 20 mutations in metastatic NSCLC. Crit Rev Oncol Hematol 2020, 148, 102906. [Google Scholar] [CrossRef] [PubMed]
- Abdalkhalek, E.S.; Wakeel, L.M.E.; Nagy, A.A.; Sabri, N.A. Variants of ERCC5 and the outcome of platinum-based regimens in non-small cell lung cancer: A prospective cohort study. Med Oncol 2022, 39, 152. [Google Scholar] [CrossRef] [PubMed]
- Zienolddiny, S.; Campa, D.; Lind, H.; Ryberg, D.; Skaug, V.; Stangeland, L.; Phillips, D.H.; Canzian, F.; Haugen, A. Polymorphisms of DNA repair genes and risk of non-small cell lung cancer. Carcinogenesis 2006, 27, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Han, X.; Liu, C.; Li, X.; Lu, S.; Jiang, Q.; Yao, J. Long Non-Coding RNA PNKY Modulates the Development of Choroidal Neovascularization. Front Cell Dev Biol 2022, 10, 836031. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Yang, Q.; Wei, W.; Wang, K.; Wang, E. Toll/IL-1 receptor-containing proteins STIR-1, STIR-2 and STIR-3 synergistically assist Yersinia ruckeri SC09 immune escape. Fish Shellfish Immunol 2020, 103, 357–365. [Google Scholar] [CrossRef]
- Fan, Y.; Gao, Z.; Li, X.; Wei, S.; Yuan, K. Gene expression and prognosis of x-ray repair cross-complementing family members in non-small cell lung cancer. Bioengineered 2021, 12, 6210–6228. [Google Scholar] [CrossRef]
- Zhang, Q.X.; Yang, Y.; Yang, H.; Guo, Q.; Guo, J.L.; Liu, H.S.; Zhang, J.; Li, D. The roles of risk model based on the 3-XRCC genes in lung adenocarcinoma progression. Transl Cancer Res 2021, 10, 4413–4431. [Google Scholar] [CrossRef]
- Saviozzi, S.; Ceppi, P.; Novello, S.; Ghio, P.; Lo Iacono, M.; Borasio, P.; Cambieri, A.; Volante, M.; Papotti, M.; Calogero, R.A.; et al. Non-small cell lung cancer exhibits transcript overexpression of genes associated with homologous recombination and DNA replication pathways. Cancer Res 2009, 69, 3390–3396. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The ERCC5 rs873601 polymorphisms are significantly associcated with the prognosis in lung cancer patients treated with platinum-based chemotherapy, and the A variant allele of ERCC5 rs873601 are protective alleles. Patients carry the AA or GA genotypes have a longer MST-OS than GG (p=0.031*).
Figure 1.
The ERCC5 rs873601 polymorphisms are significantly associcated with the prognosis in lung cancer patients treated with platinum-based chemotherapy, and the A variant allele of ERCC5 rs873601 are protective alleles. Patients carry the AA or GA genotypes have a longer MST-OS than GG (p=0.031*).

Figure 2.
The polymorphisms of ERCC5 rs873601, PNKY rs2444933 and STIR1 rs1051685 were related with the overall survival (OS) significantly. The ERCC5 rs873601 polymorphisms were significantly associated with the overall survival (OS) in age>56 and smoking patients. The variants of PNKY rs2444933 were related with the prognosis significantly in age≤56, metastasis, non-smoker and clinical in III/IV/ED patients. The polymorphisms of STIR1 rs3740051 were significantly associated with the overall survival in SCLC and metastasis patients.
Figure 2.
The polymorphisms of ERCC5 rs873601, PNKY rs2444933 and STIR1 rs1051685 were related with the overall survival (OS) significantly. The ERCC5 rs873601 polymorphisms were significantly associated with the overall survival (OS) in age>56 and smoking patients. The variants of PNKY rs2444933 were related with the prognosis significantly in age≤56, metastasis, non-smoker and clinical in III/IV/ED patients. The polymorphisms of STIR1 rs3740051 were significantly associated with the overall survival in SCLC and metastasis patients.
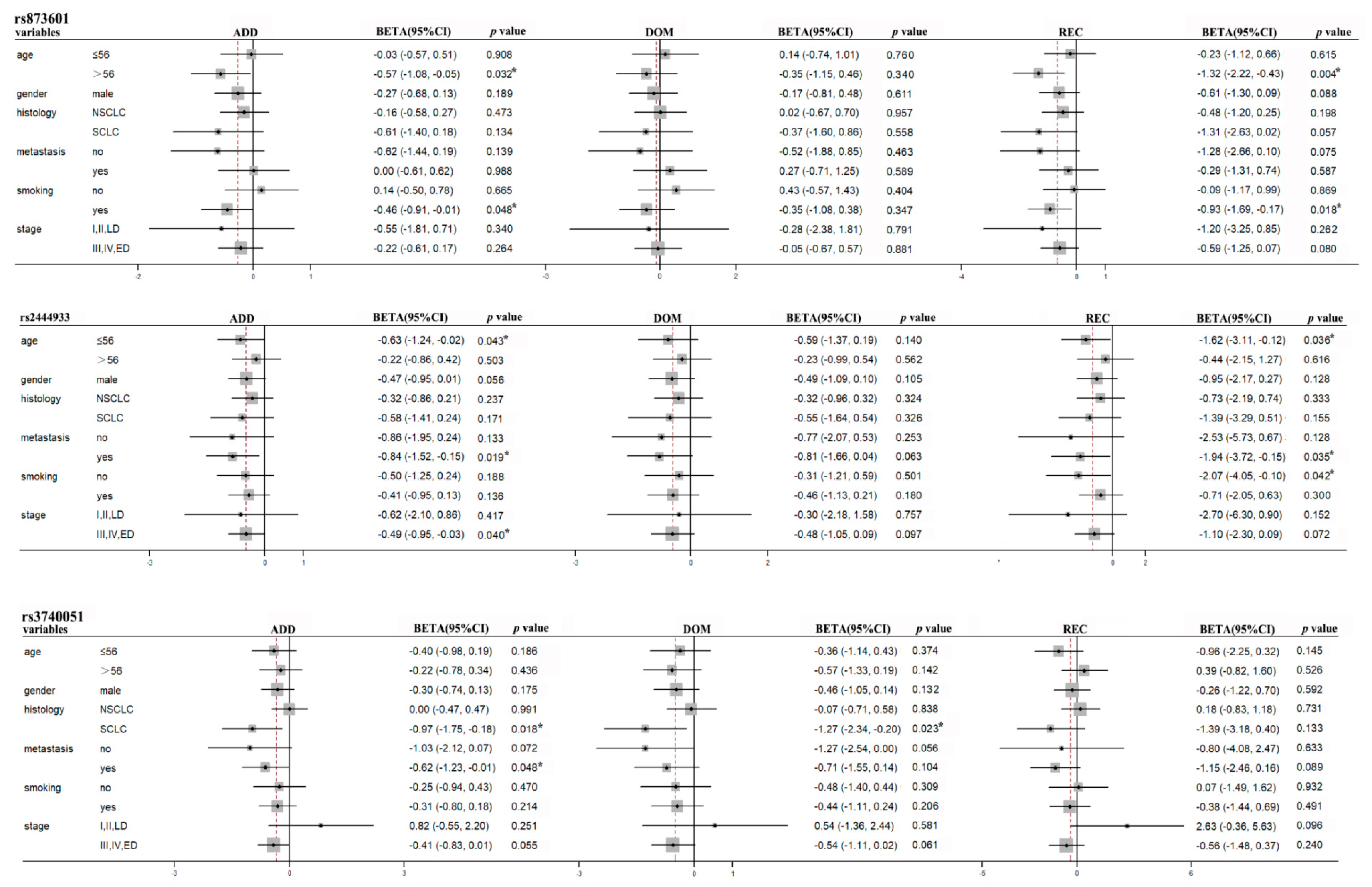
Figure 3.
The polymorphisms of ERCC5 rs873601, PNKY rs2444933, rs1849641 and XRCC5 rs1051685 were significantly with the progress free survival (PFS) significantly. The ERCC5 rs873601, PNKY rs2444933 and rs1869641 polymorphisms were significantly associated with the progress free survival (PFS) in SCLC patients. The variants of XRCC5 rs1051685 were related with the prognosis significantly in non-metastasis patients.
Figure 3.
The polymorphisms of ERCC5 rs873601, PNKY rs2444933, rs1849641 and XRCC5 rs1051685 were significantly with the progress free survival (PFS) significantly. The ERCC5 rs873601, PNKY rs2444933 and rs1869641 polymorphisms were significantly associated with the progress free survival (PFS) in SCLC patients. The variants of XRCC5 rs1051685 were related with the prognosis significantly in non-metastasis patients.
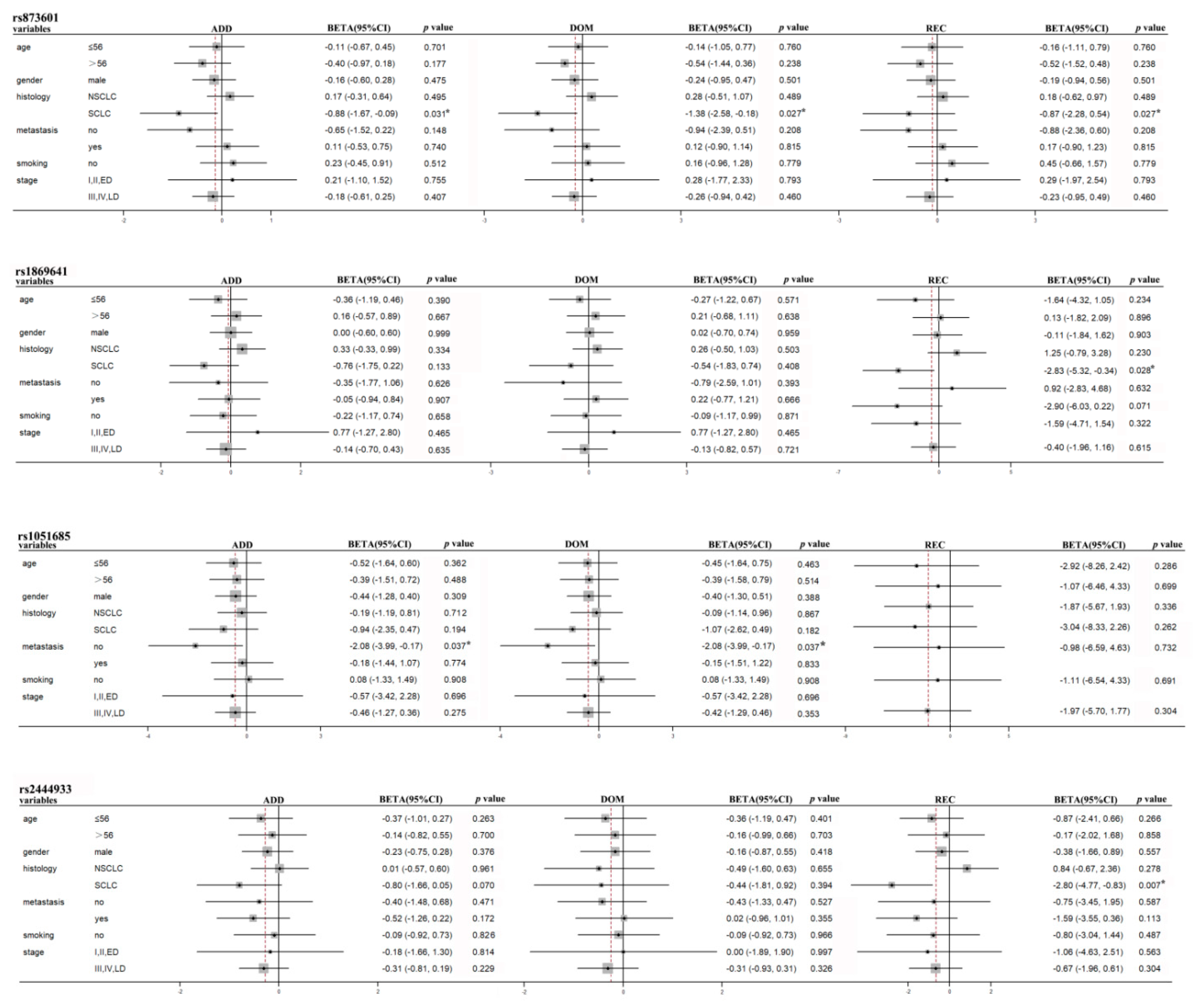
Figure 4.
The polymorphisms of ERCC5 rs873601 can affect the prognosis of lung cancer patients. Rs873601 is a mutation located in the 3’UTR of ERCC5, it can affect the mRNA of ERCC5 to translation protein. It can also regulate the RNA-binding protein and the protein-to-protein interaction of ERCC5. These may have an influence in the DNA damage and repair in NER pathway, which is a vital regulator in the prognosis of lung cancer patients treated with platinum-based chemotherapy.
Figure 4.
The polymorphisms of ERCC5 rs873601 can affect the prognosis of lung cancer patients. Rs873601 is a mutation located in the 3’UTR of ERCC5, it can affect the mRNA of ERCC5 to translation protein. It can also regulate the RNA-binding protein and the protein-to-protein interaction of ERCC5. These may have an influence in the DNA damage and repair in NER pathway, which is a vital regulator in the prognosis of lung cancer patients treated with platinum-based chemotherapy.
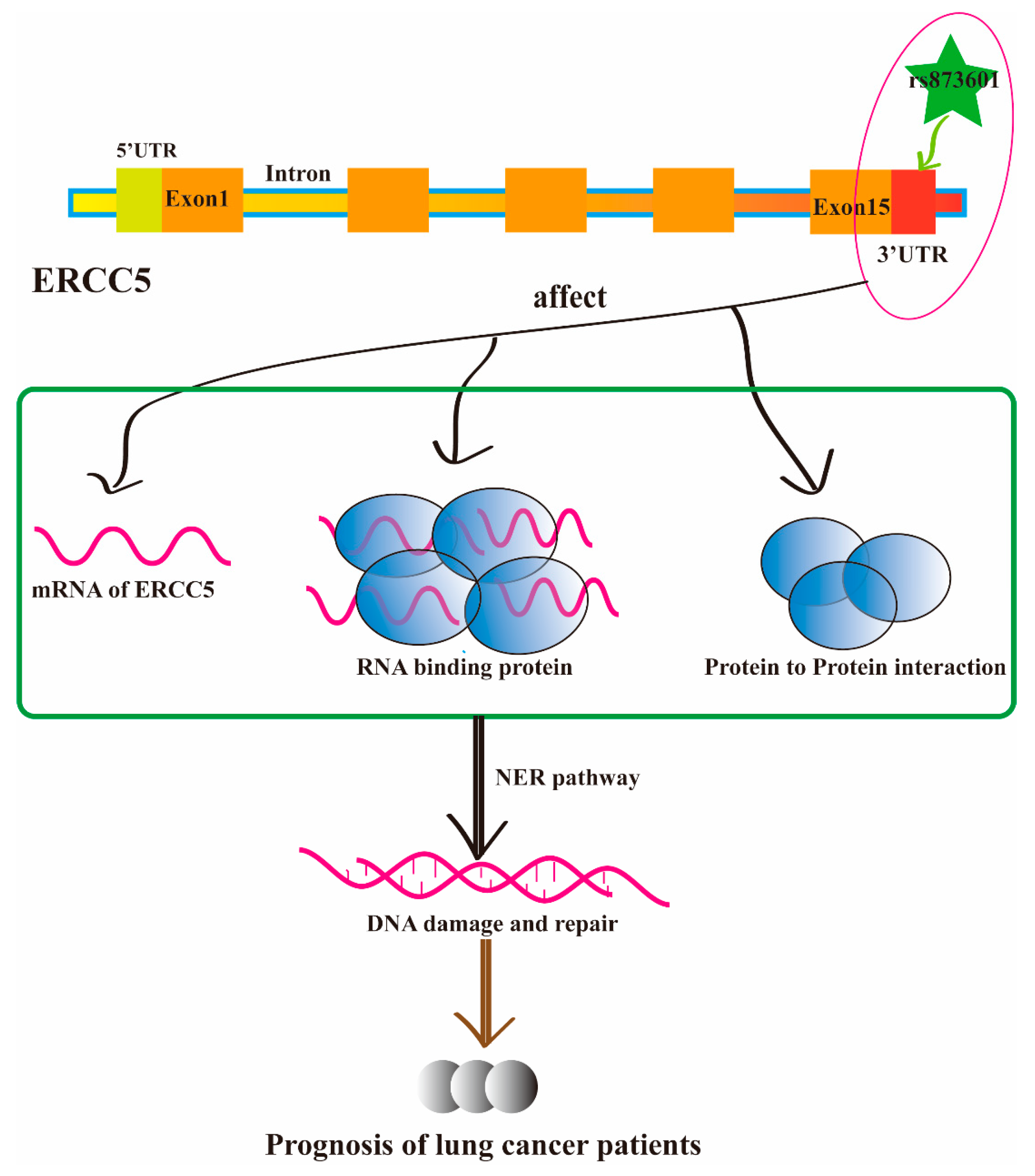

Table 1.
Clinical characteristic of lung cancer patients.
| Patient characteristics | N (%) |
|---|---|
| Total no. of patients | 345 |
| Histology | |
| Adenocarcinoma | 112(32.5) |
| Squamous cell Small cell |
111(32.2) 99(28.7) |
| Age | |
| ≤56 | 172(49.9) |
| >56 | 173(50.1) |
| Clinical stage | |
| I/II/LD | 41(11.9) |
| III/IV/ED | 298(86.4) |
| Smoking status | |
| Non-smoker | 122(35.4) |
| Smoker | 223(64.6) |
| Gender | |
| Male | 285(82.6) |
| Female | 60(17.4) |
| Metastasis | |
| No Yes |
61(17.7) 149(34.2) |
| Chemotherapy regimens | |
| Platinum/gemcitabine | 109(31.6) |
| Platinum/paclitaxel | 59(17.1) |
| Platinum/navelbine | 8(2.3) |
| Platinum/etoposide | 77(22.3) |
| Platinum/irinotecan | 8(2.3) |
Table 2.
The 17 polymorphisms examined in this study.
| Gene | Locus | dbSNP | Call Rate(%) | Polymorphism | MAF |
|---|---|---|---|---|---|
| ERCC1 | 19q13.32 | rs12984195 | 97.97 | T>C | 3.70 |
| rs117128015 | 100.00 | C>T | 8.00 | ||
| ERCC5 | 13q33.1 | rs873601 | 99.13 | G>A | 49.11 |
| PNKY | 6q16.1 | rs1869641 | 98.84 | G>A | 22.22 |
| rs1883306 | 93.91 | T>G | 38.53 | ||
| rs2444933 | 99.13 | A>G | 31.62 | ||
| SIRT1 | 10q21.3 | rs3758391 | 97.39 | T>C | 24.46 |
| rs3740051 | 96.52 | A>G | 33.41 | ||
| rs4746720 | 99.13 | T>C | 46.67 | ||
| rs12778366 | 95.65 | T>C | 22.09 | ||
| XPA | 9q22.33 | rs3176751 | 98.84 | G>C | 20.61 |
| rs3176752 | 98.84 | C>A | 21.44 | ||
| XRCC3 | 14q32.33 | rs3212117 | 98.84 | C>A | 5.28 |
| rs3212121 | 98.55 | A>G | 4.24 | ||
| XRCC5 | 2q35 | rs1051677 | 98.84 | T>C | 22.43 |
| rs2440 | 98.55 | C>T | 34.03 | ||
| rs1051685 | 99.13 | A>G | 12.14 |
Table 3.
Distribution of characteristics in lung cancer patients and prognosis analysis.
| Variables | Patients N(%) | Death N(%) | MST-OS (year) | MST-PFS (year) |
|---|---|---|---|---|
| Lung cancer | 345 | 279 | 4.42 | 3.16 |
| NSCLC | 233(67.5) | 188(67.4) | 4.56 | 3.25 |
| SCLC | 99(28.7) | 80(28.7) | 4.17 | 3.10 |
| Age | ||||
| ≤56 | 172(49.9) | 142(50.9) | 4.48 | 2.95 |
| >56 | 173(50.1) | 137(49.1) | 4.36 | 3.80 |
| Clinical stage | ||||
| I/II/LD | 41(11.9) | 31(11.1) | 3.14 | 4.05 |
| III/IV/ED | 298(86.4) | 243(87.1) | 4.55 | 3.21 |
| Smoking status | ||||
| Non-smoker | 122(35.4) | 97(34.8) | 4.77 | 4.60 |
| Smoker | 223(64.6) | 182(65.2) | 4.26 | 2.61 |
| Gender | ||||
| male | 285(82.6) | 229(82.1) | 4.39 | 2.93 |
| female | 60(17.4) | 50(17.9) | 4.57 | 4.47 |
| Metastasis | ||||
| No | 61(17.7) | 51(18.3) | 3.84 | 2.28 |
| Yes | 149(43.2) | 121(43.4) | 4.53 | 3.94 |
MST, median survival time; OS, overall survival; PFS, progression free survival; NSCLC, non-small lung cancer; SCLC, small cell lung cancer; LD, Limitation Period; ED, Extensive period.
Table 4.
Association of the ERCC5 rs873601 polymorphisms and OS in lung cancer patients.
| Gene | Polymorphisms | Genotype | MST(year) | Additive | Dominant | Recessive | |||
|---|---|---|---|---|---|---|---|---|---|
| BETA (95%CI) | p value | BETA (95%CI) | p value | BETA (95%CI) | p value | ||||
| ERCC5 | rs873601 | G G | 3.28 | -0.37(-0.75,0.01) | 0.061 | -0.30(-0.91,0.32) | 0.348 | -0.70(-1.34,-0.07) | 0.031* |
| G A A A |
4.88 4.02 |
Table 5.
Stratification analyses of Association between polymorphisms and OS or PFS in lung cancer patients.
Table 5.
Stratification analyses of Association between polymorphisms and OS or PFS in lung cancer patients.
| OS/PFS |
Gene |
Polymorphisms | Subgroup | Additive | Dominant | Recessive | |||
|---|---|---|---|---|---|---|---|---|---|
| BETA (95%CI) | p value | BETA (95%CI) | p value | BETA (95%CI) | p value | ||||
| OS | ERCC5 | rs873601 | age>56 | -0.57(-1.08,-0.05) | 0.032* | -0.35(-1.15,0.46) | 0.399 | -1.32(-2.22,-0.43) | 0.004* |
|
PFS |
PNKY STIR1 ERCC5 PNKY XRCC5 |
rs2444933 rs3740051 rs873601 rs2444933 rs1869641 rs1051685 |
smokers age≤56 metastasis non-smoker III/IV/ED SCLC metastasis SCLC SCLC SCLC Non-metastasis |
-0.46(-0.91,-0.01) -0.63(-1.24,-0.02) -0.84(-1.53,-0.15) -0.51(-1.25,0.24) -0.49(-0.95,-0.03) -0.97(-1.75,-0.18) -0.62(-1.23,-0.01) -0.88(-1.67,-0.09) -0.80(-1.66,0.05) -0.76(-1.75,0.22) -2.08(-3.99,-0.17) |
0.048* 0.043* 0.019* 0.188 0.040* 0.018* 0.048* 0.031* 0.070 0.133 0.037* |
-0.35(-1.08,0.38) -0.59(-1.37,0.19) -0.81(-1.66,0.04) -0.31(-1.21,0.59) -0.48(-1.05,0.09) -1.27(-2.34,-0.20) -0.71(-1.55,0.14) -1.38(-2.58,-0.18) -0.49(-1.60,0.63) -0.54(-1.83,0.74) -2.08(-3.99,-0.17) |
0.347 0.140 0.063 0.501 0.097 0.023* 0.104 0.027* 0.394 0.408 0.037* |
-0.93(-1.69,-0.17) -1.62(-3.11,-0.12) -1.94(-3.72,-0.15) -2.07(-4.05,-0.10) -1.10(-2.30,0.09) -1.39(-3.18,0.40) -1.15(-2.46,0.16) -0.87(-2.28,0.54) -2.80(-4.77,-0.83) -2.83(-5.32,-0.34) |
0.018* 0.036* 0.035* 0.042* 0.072 0.133 0.089 0.230 0.007* 0.028* |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



