
Submitted:
17 October 2023
Posted:
17 October 2023
You are already at the latest version
Abstract
Hepatocellular carcinoma (HCC) is a non-AIDS-defining cancer closely tied to the chronic HIV infection and associated with the release of inflammatory cytokines, immune system dysfunction, and genetic alterations within mitochondria. However, our understanding of how these factors contribute to HCC risk in PLWH is limited. The objective of the study was to ascertain the differential secretion of cytokines and mitochondria DNA (mtDNA) deletion in PLWH, and individuals diagnosed with HCC without HIV. A cross-sectional study was conducted with PLWH and HCC participants from the Korle-Bu Teaching Hospital. Plasma and peripheral blood mononuclear cells (PBMCs) were isolated from whole blood. The plasma samples were used to measure cytokines using ELISA and Luminex techniques. We determined mtDNA deletions from PBMCs. We found that the secretion of the cytokines TGF-β, FGF-2, IL-8, TNF-α, VEGF, and RANTES implicated in the pre-cancer, initiation, and early stages of HCC were similar in PLWH compared to HCC participants without HIV. PBMCs of PLWH exhibited high mtDNA deletion (60%) comparable to HCC participants without HIV (64%). These findings underscore the underlying risks associated with HCC development in PLWH. There is a need for HCC surveillance among PLWH and these cytokines could be used as biomarkers.
Keywords:
Hepatocellular carcinoma (HCC)
; Human immunodeficiency virus (HIV)
; hepatitis
; inflammatory cytokines
; mitochondria DNA deletion
1. Introduction
People living with HIV (PLWH) are at high risk of developing acquired immunodeficiency syndrome (AIDS)-defining cancers such as Kaposi's sarcoma, non-Hodgkin lymphoma, and cervical cancer. Antiretroviral therapy (ART) has reduced the incidence of AIDS-defining cancers and reduced morbidity and mortality, leading to longer life expectancy 1,2. Despite the benefits of ART, the incidence of non-AIDS-defining cancers in PLWH such as hepatocellular carcinoma (HCC), Hodgkin’s lymphoma, skin melanoma, oral, lung, and anal cancers is increasing 1. The mortality from non-AIDS-defining cancers between 2001 and 2015 was estimated at 9.2% compared to 5% of AIDS-defining cancers in a study conducted in the United States of America 3. Furthermore, published data from a multicenter study in Europe on PLWH showed 15% mortality associated with non-AIDS-defining cancers 4.
HCC or liver cancer is the sixth most common cancer and the third leading cause of cancer deaths globally. In 2020, over 900,000 new cases were reported worldwide, with the highest burden in Asia and Africa 5,6. HCC is on the rise among PLWH with an estimated 72% increase in incidence rate and a higher risk among PLWH aged 50 years or older 7. A recent retrospective study in the USA and Canada estimated the prevalence of HCC between 0.1 to 0.5% in PLWH 7,8. However, other studies conducted within HIV endemic regions in South Africa, Uganda, and Kenya estimated a prevalence of 18 to 22% showing the enormous burden of HCC cases in PLWH in Sub-Saharan Africa 9–11. PLWH with chronic hepatitis B or C virus (HBV or HCV respectively) coinfection are at a higher risk of developing HCC 12. HBV and HCV infections are more predominant in PLWH 13. Moreover, PLWH with HBV and/or HCV coinfections have a rapid progression to end-stage liver disease compared to individuals with HBV and HCV monoinfections 8,14. These viruses establish chronic infections and the host immune response to curtail the infection leads to the persistent production of cytokines 15.
Cytokines, which are modulated by the host immune system are secreted to regulate cellular stresses such as infection, inflammation, and carcinogen-induced injury 16,17. Cytokines are classified as pro- and anti-inflammatory. The imbalance between pro- and anti-inflammatory cytokines in chronic infections results in chronic inflammation. The state of chronic inflammation is critical in the formation, development, progression, and metastasis of cancers 16,18,19. Although cytokines are linked to the development of several cancers, certain cytokines are markers for specific cancers. For instance, IL-6, TGF-β, FGF-2, MCP-1, and VEGF have been linked to the pre-cancer or initiation (formation) of HCC. The developmental or early stage HCC has been associated with VEGF, GDF-15, RANTES, and OPN, while interleukin-10 (IL-10), MIP-3, and IL-37b are makers for the advanced stage of HCC 16,20. Other studies have reported tumor necrosis factor-alpha (TNF-α) as a key marker in cirrhosis and HCC development correlating with the secretion of IL-6 20. In addition, the secretion of TNF-α is implicated in the production of reactive oxygen species (ROS) by the mitochondria which results in oxidative stress and nucleotide damage leading to mitochondrial DNA (mtDNA) mutagenesis 21. Interestingly, there are several inflammatory cytokines produced in PLWH resulting in chronic immune activation and inflammation. Furthermore, there is preponderance of data to suggest that HIV increases the risk of cancer, though the underlying mechanisms are not well-understood. Could pro-inflammatory cytokines play a role in the increased incidence of non-AIDS-defining cancers in PLWH?
The purpose of this study was to investigate the differential secretion of cytokines and mitochondria deletion in PLWH and individuals with HCC without HIV infection. We hypothesize that PLWH secrete cytokines that result in chronic systemic inflammation and immune dysregulation responsible for the increased risk of HCC. Delineating the cytokines differentially secreted between PLWH and individuals with HCC could be crucial in screening HCC in PLWH and facilitating appropriate care and treatment.
2. Methods
2.1. Study design and study population
This was a cross-sectional study of individuals diagnosed with HCC (HCC+) without HIV infection and PLWH (HIV+) receiving care at the Section of Gastroenterology and the Fever’s Unit, respectively at the Korle-Bu Teaching Hospital (KBTH), Accra, Ghana. Study participants were recruited on convenience during their routine clinic visits between June and September 2022. HCC participants with fatty or alcohol-associated liver disease were excluded. The study protocol was reviewed and approved by the Institutional Review Boards of the KBTH and Noguchi Memorial Institute for Medical Research (NMIMR).
2.2. Data collection and sample collection
Participants 18 years and above were consented and recruited. Each participant gave a written informed consent. At enrollment, 50 ml of blood was collected from each participant. Participant’s medical records and treatment including history of infection, years on ART treatment, HIV viral load, HIV CD4 count, and liver function tests were reviewed and recorded. A study questionnaire administered by the study research assistants was used to obtain demographic and socio-economic data including age, sex, educational background, history of cancer in the family, and history on smoking and alcohol intake. Data was entered and managed using the Research Electronic Data Capture (REDCap) software 22.
2.3. Blood separation
Plasma and peripheral mononuclear blood cells (PBMCs) were separated from whole blood through density gradient centrifugation using Ficoll® as previously described 23. The plasma was stored at a -20°C while the PBMCs were cryopreserved in freezing medium and stored in liquid nitrogen.
2.4. Serological testing of HBV and HCV
All Participants were screened for HBV (Acro Biotech, California, USA) and HCV (Acro Biotech, California, USA).
2.5. Cytokine profile
Plasma from each participant was assayed for cytokines using ELISA and Luminex assays according to manufacturer’s instructions 24,25. Macrophage inflammatory protein 3 (MIP-3), osteopontin (OPN), growth differentiation factor 15 (GDF-15), and transforming growth factor beta (TGF-β) were measured using ELISA (Sigma, Darmstadt, Germany). Luminex assay (MILLIPLEX MAP, Millipore, Darmstadt, Germany) was used to measure the expression levels of the following cytokines—Fibroblast growth factor 2 (FGF-2), Interferon gamma (IFN- γ), interleukin (IL)-2, IL-6, IL-8, IL-10, IL-12p70, IL-12p40, IL-18, interferon-gamma induced protein 10 (IP-10/CXCL10), monocyte chemoattractant protein 1 (MCP-1), tumor necrosis factor (TNF) - alpha (TNF-α), vascular endothelial growth factor (VEGF), and regulated upon activation, normal T cell expressed and secreted (RANTES/CCL5). The runs were performed in duplicates.
2.6. Mitochondrial mutations
To assess the mtDNA common deletion (4977 deletion), nested PCR was performed using primers and protocols as previously described 26. In brief, genomic DNA was extracted from PBMCs using the DNeasy blood and tissue kit (QIAgen, Hilden, Germany). Two pairs of primers were used for the detection of the 4,977-bp deletion: The round 1 primers were 1F: AACCACAGTTTCATGCCCATC; and 1R: TGTTAGTAAGGGTGGGGAAGC; and the round 2 primers were 2F: ACCCTATTGCACCCCCTCTAC; and 2R: CTTGTCAGGGAGGTAGCGATG. The PCR condition set used for the nested PCR was pre-denaturation at 94°C for 5 min; then 30 cycles at 94°C for 10 s, 58°C for 45 s and 72°C for 50 s; and a final extension at 72°C for 10 min. The PCR products were then electrophoresed on 2% agarose gel and the 4,977-bp deletion was indicated by the presence of a 358-bp band.
2.7. Data analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS; IBM Corporation, Armonk, NY) and GraphPad Prism 9 (Dotmatics, Boston, USA). Categorical variables were presented as frequency and percentage, while continuous variables were expressed as median and interquartile range (IQR) with confidence interval (CI). Chi-square and/or regression analysis were used in determining risk-associated factors. Statistical significance was considered p < 0.05.
3. Results
3.1. Demographic and disease characteristics of study participants
We enrolled a total of 93 participants — 33 had HCC without HIV (HCC+) and 60 were PLWH without HCC (HIV+) as shown in Table 1. Females made up 63%, and the mean age of study participants was 50 ± 13 years. About 54% were aged 50 years and above. The highest level of education was junior high school for two-thirds of participants (65%). Nearly half of the participants had a history of alcohol usage. The prevalence of hypertension was higher in HIV+ participants compared to HCC+ participants. All the HCC+ participants were hepatitis B or C positive, whereas 16 out of the 60 (26.7%) PLWH were co-infected with either hepatitis B or C virus. Study participants with HIV only were 44 (73.3%) of the 60 PLWH.
As shown in Table 2, 31 (54%) of the HIV+ participants had been diagnosed of HIV for at least 10 years while 28 (50%) had been on ART for 10 years. Of the HIV+ participants, most of them were categorized as HIV stage 1 (43.6%), had viral loads below 50 copies/ml (78.2%), and had CD4 cell counts above 200 cells (89.4%).
3.2. Liver function of study participants
Liver function tests including alanine transaminase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), albumin, and bilirubin were extracted from participant’s medical records. The records showed that the HCC+ participants had higher levels of liver enzymes ALT, AST, and ALP as well as bilirubin compared to the HIV+ participants. However, the albumin level was lower in the HCC+ participants compared to the HIV+ participants (Table 3).
3.3. Cytokine profile of study participants
We determined the cytokine profile of HCC+ participants compared to HIV+ participants. We screened for 18 cytokines that were either pro-inflammatory or anti-inflammatory. Next, we grouped them into cytokines associated with pre-cancer or the initiation stage of HCC (IL-6, TGF-β, MCP-1, FGF-2, IL-2, IL-8, IL-12p40, IL-12p70, IL-18, IP-10, TNF-α, and IFN-γ), early stage of HCC (OPN, GDF-15, RANTES, and VEGF), and advanced stage of HCC (IL-10, and MIP-3) . As shown in Figure 1, the cytokines associated with the pre-cancer or the initiation stage of HCC, TGF-β, FGF-2, IL-8, and TNF-α were expressed at similar levels in the HIV+ participants compared to the HCC+ participants. However, IL-6, MCP-1, and IP-10 had significantly higher expression in HCC+ participants than in HIV+ participants. Comparison of cytokines implicated in the early stage of HCC showed that OPN was significantly expressed in the HCC+ participants but VEGF, GDF-15 and RANTES were secreted to similar levels compared to that of the HIV+ participants (Figure 2A). More importantly, among the PLWH, the pre-cancer, initiation, and early-stage cytokines were expressed at similar levels between hepatitis positive and negative patients (Figure 1 and Figure 2A). The advanced stage cytokines IL-10 and MIP-3 were significantly expressed in HCC+ participants than the HIV+ participants (Figure 2B).
3.4. Correlation of cytokine levels in HIV+ participants
We next investigated the correlation among the 19 cytokines screened. As presented in Table 4, the notable pairwise correlations with the HIV+ cohort were 0.89 for IL-12p70 and IL-12p40, 0.87 for RANTES and TGF-β, and 0.85 for TNF-α and TGF-β. There was high correlation of the cytokines implicated in the pre-cancer, the initiation stage of HCC, and the early stage of HCC. Notably, the cytokines including IL-6, TGF-β, FGF-2, VEGF, IL-8, TNF-α, and RANTES exhibited positive correlations with each other. Interestingly, GDF-15 negatively correlated with IL-8, TGF-β, VEGF, OPN, and RANTES in the HIV+ participants.
3.5. Mitochondrial mutations among the cohorts
Mitochondrial mutagenesis has been associated with the development of cancers 27. Mitochondrial deletion mutations are more prevalent than point mutations 28. We therefore investigated mitochondrial deletion mutations in the PBMCs of HCC+ and HIV+ participants. We observed a high rate of mtDNA deletion in both cohorts; 60% and 64% in HIV+ and HCC+ participants, respectively. Overall, we observed that mtDNA deletion was associated with increase in age, and male gender. There was no association between mtDNA deletion and history of alcohol usage (Table 5). Risks analysis showed that age above 50 (OR 3.3; CI 1.1 - 9.8), males (OR 4.5; CI 1.1 - 17.8), diagnosed with HIV over 10 years (OR 3.3; CI 1.1 - 10.0), use of ART over 10 years (OR 2.1; CI 0.7 - 6.2), and viral loads more than 50 copies (OR 2.2; CI 0.5 - 9.1) were associated with mtDNA deletions in the HIV+ cohort. HIV-hepatitis coinfected participants (69%) had a 1.7 times likelihood for mtDNA mutagenesis compared to their HIV-monoinfected participants (57%).
4. Discussion
The chronic inflammation state of HBV or HCV stimulates the continuous secretion of cytokines that contributes to HCC development. Moreover, HIV infection leads to chronic inflammation with the secretion of several cytokines (proinflammatory or anti-inflammatory) that could initiate the development of cancers 29. Consequently, with the increased incidence of non-AIDS-defining including hepatocellular carcinoma, we raised the question: Could pro-inflammatory cytokines play a role in the increased incidence of non-AIDS-defining cancers such as HCC in PLWH? We found high levels of inflammatory cytokines TGF-β, FGF-2, IL-8, TNF-α, VEGF, and RANTES, and mutagenesis of mtDNA in PLWH. These are cytokines implicated in the pre-cancerous, initiation and early stages of HCC. Importantly, the study offered preliminary evidence indicating a resemblance between the secretion patterns of these inflammatory cytokines in PLWH and those observed in HCC patients, thereby underscoring the potential risks of HCC development among PLWH.
Comparison of the levels of cytokines implicated in liver fibrosis, cirrhosis, or the initiation of HCC in HIV+ participants were similar to those in HCC+ participants with the exception of IL-6 and MCP-1. The cytokines TGF-β, FGF-2, IL-8, and TNF-α as observed in the HCC patients and PLWH were consistent with studies implicating these cytokines in hepatic injury and the initiation of HCC in PLWH 30–33. Moreover, studies have further shown that HIV-infected PBMCs stimulates the expression of pro-inflammatory, pro-fibrogenic, angiogenic, and proliferative cytokines including IL-6, VEGF, and TGF-β in hepatic stellate cells 34. The secretion of these cytokines exhibited a positive correlation among the HIV participants, which aligns with findings from other studies indicating a correlation between the cytokines TNF-α, IL-6, and IL-8 in PLWH coinfected with hepatitis, as well as in individuals with chronic hepatitis. 32,35. TGF-β is anti-inflammatory and involved in inhibiting apoptosis, while TNF-α, IL-8, FGF-2, and VEGF are involved in hepatic injury or cirrhosis through cell proliferative and angiogenic activities 16,36. High levels of IL-6 and MCP-1 correlate with worse prognosis for cirrhotic and HCC patients hence suggested as biomarkers to track the development of HCC 37–39. This implies that the low levels of IL-6 and MCP-1 in the HIV+ participants compared to the HCC individuals, could be monitored for liver prognosis. Additional studies are necessary to determine if IL-6 together with cytokines such as MCP-1 could be used to monitor the initiation and progression of HCC in PLWH.
The observed expression of VEGF and RANTES, both linked to the early stages of HCC development, is consistent with previous findings 40,41. Studies have suggested that VEGF and RANTES could predict the presence of HCC and high levels of these cytokines could be important as prognostic factor in determining the survival of HCC patients 42,43. Notably, VEGF is closely tied to angiogenesis, while RANTES has been implicated in facilitating metastasis 42,43. These preliminary findings underscore the potential role of VEGF and RANTES as critical players in the early progression of HCC, thereby warranting further investigation into their mechanistic contributions and potential clinical implications.
Furthermore, consistent with other studies, our findings showed that MIP-3 and IL-10 secretions are associated with the advanced stage of HCC 44. The study findings showed low secretion of MIP-3 and IL-10 among PLWH compared to HCC patients. This finding is consistent with other studies showing high levels of MIP-3 and IL-10 in HCC patients compared to their cirrhotic or non-HCC counterparts 44–46. The secretion and expression of MIP-3 is further associated with the developmental stages or grades of the liver tumors 47. This suggests that the study’s HIV+ participants were likely not having any advanced HCC. MIP-3 and IL-10 are associated with chronic infections with anti-inflammatory effects in immune regulatory, angiogenesis and tumorigenesis 46,48.
Consistent with other studies, our findings revealed a high rate of mtDNA mutations (deletions) in PBMCs from both HIV+ and HCC+ participants 49–51. In addition, the study results suggest that hepatitis infection contributes to high mtDNA deletions in HIV-hepatitis coinfected participants compared to HIV-monoinfected participants as demonstrated in another study 51. Mitochondrium is the chief powerhouse of the cell with its function designed to meet the energy and metabolic needs of the cell 27. However, several environmental conditions including chronic infections as established in our study participants by the HIV and hepatitis viruses, could disrupt the functions of the mitochondria 51,52. The most common causes of disruption of mitochondrial functions are mtDNA mutations, deletions, and impaired DNA replication. The accumulation of mtDNA mutagenesis is a hallmark of mitochondrial dysfunction which is implicated in carcinogenesis including HCC 52. Subsequently, mitochondrial dysfunction results in the generation of mitochondrial reactive oxygen species (ROS). The mitochondrial ROS can result in further damage to the structure and functions of the mitochondria, other organelles, cells, tissues, and organs contributing to carcinogenesis. Furthermore, chronic infections with the HIV and hepatitis B and C viruses as observed in the HIV and HCC participants stimulate the secretion of cytokines such as TNF-α. The secretion of TNF-α stimulates the production of ROS resulting in oxidative stress. These ROS-generated oxidative stress results in nucleotide damage leading to mtDNA deletions and subsequently affecting the genome integrity, apoptosis, and promoting the outgrowth of cancerous cells 53,54. The biology and the interactions of HIV and hepatitis B and C viruses on mtDNA mutations and their implications in the development of HCC is not well understood. Therefore, further studies would be important to determine the role of chronic hepatitis infection in the initiation and progression of HCC in HIV-hepatitis coinfected patients compared the HIV-monoinfected patients.
The study sought to determine factors contributing to the increased incidence of HCC among PLWH in the Sub-Saharan African region. Despite the study determining the differential secretion of cytokines between PLWH and HCC individuals, as well as mitochondria mutagenesis, it is important to acknowledge the inherent limitations within this study. Firstly, the research was conducted as an exploratory study, resulting in a relatively small sample size. The cross-sectional study design, though informative, would benefit from the establishment of a larger cohort for longitudinal observation to thoroughly examine the dynamic relationship between inflammatory cytokines and HCC development in PLWH. Secondly, inclusion of a well-matched healthy control group, factoring in gender and age, would establish baseline levels of cytokine secretion within PLWH. Thirdly, the absence of ultrasound screening to assess liver conditions in HIV-positive participants, including potential factors like fibrosis and cirrhosis, is a noteworthy limitation. Correlating such factors with cytokine secretion patterns could provide valuable insights. Finally, the study did not assess the correlation between cytokine levels and mtDNA mutagenesis with the viral load of HBV or HCV.
5. Conclusion
In essence, HIV infection, regardless of hepatitis coinfection, appears to trigger the release of cytokines associated with fibrogenesis, cirrhosis, liver tissue tumorigenesis, and mutagenesis of mtDNA, potentially initiating HCC among PLWH. The study presents initial evidence that the profile of these inflammatory cytokines released in PLWH resembles that found in HCC patients, implying an elevated risk of HCC development in PLWH. These findings shed light on the underlying risks of HCC in PLWH and underscore the importance of HCC surveillance within this population. Additional research is imperative to comprehensively investigate and elucidate the roles of cytokines and mtDNA mutations in HCC development, as well as their implications for other cancers within the context of HIV infection and concurrent coinfections with opportunistic viruses.
Author Contributions
Conceptualization: J.O.A., G.B.K., and E.P.; Method: J.O.A., R.A-T., L.Z., P.W., V.G., K.T., B.N.A.A., M.M, and T.K.; Validation: J.O.A, R.A-T, P.W., B.N.A.A, M.M. and T.K.; Analysis: J.O.A.; Writing: J.O.A.; Review: G.B.K., E.P., R.A-T., L.Z., V.G., and K.T.; Supervision: G.B.K. and E.P. All authors have read and agreed to the published version of the manuscript.
Funding
The study was supported by the UG/Yale HIV Comorbidities Research Training (HIVComRT) in Ghana through the NIH Fogarty International Centre (D43 5D43TW011526).
Institutional Review Board Statement
The study was performed in accordance with the Declaration of Helsinki and approved by the Institutional Review Boards of the Noguchi Memorial Institute for Medical Research (038/21-22), and the Korle Bu Teaching Hospital (KBTH-IRB 000185/2021).
Informed Consent Statement
The study has obtained informed consent from all study participants.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to ethical restrictions and information that could compromise the privacy of the study participants.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Franceschi, S.; Lise, M.; Clifford, G. M.; Rickenbach, M.; Levi, F.; Maspoli, M.; Bouchardy, C.; Dehler, S.; Jundt, G.; Ess, S.; Bordoni, A.; Konzelmann, I.; Frick, H.; Dal Maso, L.; Elzi, L.; Furrer, H.; Calmy, A.; Cavassini, M.; Ledergerber, B.; Keiser, O. Changing Patterns of Cancer Incidence in the Early- and Late-HAART Periods: The Swiss HIV Cohort Study. Br J Cancer 2010, 103 (3), 416–422. [CrossRef]
- Yuan, T.; Hu, Y.; Zhou, X.; Yang, L.; Wang, H.; Li, L.; Wang, J.; Qian, H.-Z.; Clifford, G. M.; Zou, H. Incidence and Mortality of Non-AIDS-Defining Cancers among People Living with HIV: A Systematic Review and Meta-Analysis. eClinicalMedicine 2022, 52, 101613. [CrossRef]
- Horner, M.-J.; Shiels, M. S.; Pfeiffer, R. M.; Engels, E. A. Deaths Attributable to Cancer in the US Human Immunodeficiency Virus Population During 2001–2015. Clin Infect Dis 2020, 72 (9), e224–e231. [CrossRef]
- Smith, C. J.; Ryom, L.; Weber, R.; Morlat, P.; Pradier, C.; Reiss, P.; Kowalska, J. D.; de Wit, S.; Law, M.; el Sadr, W.; Kirk, O.; Friis-Moller, N.; Monforte, A. d’Arminio; Phillips, A. N.; Sabin, C. A.; Lundgren, J. D. Trends in Underlying Causes of Death in People with HIV from 1999 to 2011 (D:A:D): A Multicohort Collaboration. The Lancet 2014, 384 (9939), 241–248. [CrossRef]
- Rumgay, H.; Ferlay, J.; de Martel, C.; Georges, D.; Ibrahim, A. S.; Zheng, R.; Wei, W.; Lemmens, V. E. P. P.; Soerjomataram, I. Global, Regional and National Burden of Primary Liver Cancer by Subtype. European Journal of Cancer 2022, 161, 108–118. [CrossRef]
- Liver cancer statistics | World Cancer Research Fund International. WCRF International. https://www.wcrf.org/cancer-trends/liver-cancer-statistics/ (accessed 2023-01-30).
- Sun, J.; Althoff, K. N.; Jing, Y.; Horberg, M. A.; Buchacz, K.; Gill, M. J.; Justice, A. C.; Rabkin, C. S.; Goedert, J. J.; Sigel, K.; Cachay, E.; Park, L.; Lim, J. K.; Kim, H. N.; Vincent Lo Re, I. I. I.; Moore, R.; Sterling, T.; Peters, M. G.; Achenbach, C. J.; Silverberg, M.; Thorne, J. E.; Mayor, A. M.; Crane, H. M.; Kitahata, M. M.; Klein, M.; Kirk, G. D. Trends in Hepatocellular Carcinoma Incidence and Risk Among Persons With HIV in the US and Canada, 1996-2015. JAMA Network Open 2021, 4 (2). [CrossRef]
- Mehershanhi, S.; Haider, A.; Kandhi, S.; Sun, H.; Patel, H. Prevalence of Hepatocellular Carcinoma in HIV Patients Co-Infected or Triple Infected With Hepatitis B and Hepatitis C in a Community Hospital in South Bronx. Cureus 14 (6), e26089. [CrossRef]
- Otedo, A.; Simbiri, K. O.; Were, V.; Ongati, O.; Estambale, B. A. Risk Factors for Liver Cancer in HIV Endemic Areas of Western Kenya. Infect Agent Cancer 2018, 13, 41. [CrossRef]
- Mak, D.; Villiers, C. B. de; Chasela, C.; Urban, M. I.; Kramvis, A. Analysis of Risk Factors Associated with Hepatocellular Carcinoma in Black South Africans: 2000–2012. PLoS ONE 2018, 13 (5). [CrossRef]
- Nsibirwa, S. K.; Aizire, J.; Thomas, D. L.; Ocama, P.; Kirk, G. D. Rapid Progression to Death after Hepatocellular Carcinoma Diagnosis Particularly among Persons with Advanced HIV Disease in Kampala, Uganda. medRxiv June 30, 2022, p 2022.06.24.22276850. [CrossRef]
- El-Shenawy, R.; Farouk, S.; Helmy, N.; Din, N. B. E.; El-Shenawy, R.; Farouk, S.; Helmy, N.; Din, N. B. E. Risk Factors Associated with Development of Hepatocellular Carcinoma in Hepatitis C Virus Patients. In Hepatitis C - Recent Advances; IntechOpen, 2023. [CrossRef]
- Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. https://www.who.int/publications-detail-redirect/9789240027077 (accessed 2023-04-01).
- Cheng, Z.; Lin, P.; Cheng, N. HBV/HIV Coinfection: Impact on the Development and Clinical Treatment of Liver Diseases. Front Med (Lausanne) 2021, 8, 713981. [CrossRef]
- Ngcobo, S.; Molatlhegi, R. P.; Osman, F.; Ngcapu, S.; Samsunder, N.; Garrett, N. J.; Abdool Karim, S. S.; Abdool Karim, Q.; McKinnon, L. R.; Sivro, A. Pre-Infection Plasma Cytokines and Chemokines as Predictors of HIV Disease Progression. Sci Rep 2022, 12 (1), 2437. [CrossRef]
- Montanari, N. R.; Anugwom, C. M.; Boonstra, A.; Debes, J. D. The Role of Cytokines in the Different Stages of Hepatocellular Carcinoma. Cancers 2021, 13 (19). [CrossRef]
- Kany, S.; Vollrath, J. T.; Relja, B. Cytokines in Inflammatory Disease. Int J Mol Sci 2019, 20 (23), 6008. [CrossRef]
- Zamarron, B. F.; Chen, W. Dual Roles of Immune Cells and Their Factors in Cancer Development and Progression. International Journal of Biological Sciences 2011, 7 (5), 651. [CrossRef]
- Budhu, A.; Wang, X. W. The Role of Cytokines in Hepatocellular Carcinoma. Journal of Leukocyte Biology 2006, 80 (6), 1197–1213. [CrossRef]
- Lan, T.; Chen, L.; Wei, X. Inflammatory Cytokines in Cancer: Comprehensive Understanding and Clinical Progress in Gene Therapy. Cells 2021, 10 (1), 100. [CrossRef]
- Yan, B.; Wang, H.; Rabbani, Z. N.; Zhao, Y.; Li, W.; Yuan, Y.; Li, F.; Dewhirst, M. W.; Li, C.-Y. Tumor Necrosis Factor-α Is a Potent Endogenous Mutagen That Promotes Cellular Transformation. Cancer Res 2006, 66 (24), 11565–11570. [CrossRef]
- Patridge, E. F.; Bardyn, T. P. Research Electronic Data Capture (REDCap). J Med Libr Assoc 2018, 106 (1), 142–144. [CrossRef]
- Lu, Y.; Ahmed, S.; Harari, F.; Vahter, M. Impact of Ficoll Density Gradient Centrifugation on Major and Trace Element Concentrations in Erythrocytes and Blood Plasma. Journal of Trace Elements in Medicine and Biology 2015, 29, 249–254. [CrossRef]
- Skrzypkowska, M.; Stasiak, M.; Sakowska, J.; Chmiel, J.; Maciejewska, A.; Buciński, A.; Słomiński, B.; Trzonkowski, P.; Łuczkiewicz, P. Cytokines and Chemokines Multiplex Analysis in Patients with Low Disease Activity Rheumatoid Arthritis. Rheumatol Int 2022, 42 (4), 609–619. [CrossRef]
- Aztatzi-Aguilar, O. G.; Sierra-Vargas, M. P.; Ortega-Romero, M.; Jiménez-Corona, A. E. Osteopontin’s Relationship with Malnutrition and Oxidative Stress in Adolescents. A Pilot Study. PLoS ONE 2021, 16 (3), e0249057. [CrossRef]
- Chen, T.; He, J.; Shen, L.; Fang, H.; Nie, H.; Jin, T.; Wei, X.; Xin, Y.; Jiang, Y.; Li, H.; Chen, G.; Lu, J.; Bai, Y. The Mitochondrial DNA 4,977-Bp Deletion and Its Implication in Copy Number Alteration in Colorectal Cancer. BMC Med Genet 2011, 12, 8. [CrossRef]
- Srinivasan, S.; Guha, M.; Kashina, A.; Avadhani, N. G. Mitochondrial Dysfunction and Mitochondrial Dynamics-The Cancer Connection. Biochim Biophys Acta 2017, 1858 (8), 602–614. [CrossRef]
- Kowald, A.; Kirkwood, T. B. L. Transcription Could Be the Key to the Selection Advantage of Mitochondrial Deletion Mutants in Aging. Proceedings of the National Academy of Sciences 2014, 111 (8), 2972–2977. [CrossRef]
- Borges, Á. H.; Silverberg, M. J.; Wentworth, D.; Grulich, A. E.; Fätkenheuer, G.; Mitsuyasu, R.; Tambussi, G.; Sabin, C. A.; Neaton, J. D.; Lundgren, J. D. Predicting Risk of Cancer during HIV Infection: The Role of Inflammatory and Coagulation Biomarkers. AIDS 2013, 27 (9), 1433–1441. [CrossRef]
- Chen, X.; Liu, X.; Duan, S.; Tang, R.; Zhou, S.; Ye, R.; Yang, Y.; Wang, J.; Yao, S.; He, N. Plasma Inflammatory Biomarkers Associated with Advanced Liver Fibrosis in HIV–HCV-Coinfected Individuals. International Journal of Environmental Research and Public Health 2020, 17 (24), 9474. [CrossRef]
- Hu, S.; Ghabril, M.; Amet, T.; Hu, N.; Byrd, D.; Yang, K.; Vuppalanchi, R.; Saxena, R.; Desai, M.; Lan, J.; Johnson, R.; Gupta, S.; Chalasani, N.; Yu, Q. HIV-1 Coinfection Profoundly Alters Intrahepatic Chemokine but Not Inflammatory Cytokine Profiles in HCV-Infected Subjects. PLoS ONE 2014, 9 (2), e86964. [CrossRef]
- Shata, M. T. M.; Abdel-hameed, E. A.; Rouster, S. D.; Yu, L.; Liang, M.; Song, E.; Esser, M. T.; Shire, N.; Sherman, K. E. HBV and HIV/HBV Infected Patients Have Distinct Immune Exhaustion and Apoptotic Serum Biomarker Profiles. Pathogens and Immunity 2019, 4 (1), 39–65. [CrossRef]
- Falasca, K.; Ucciferri, C.; Dalessandro, M.; Zingariello, P.; Mancino, P.; Petrarca, C.; Pizzigallo, E.; Conti, P.; Vecchiet, J. Cytokine Patterns Correlate with Liver Damage in Patients with Chronic Hepatitis B and C. Ann Clin Lab Sci 2006, 36 (2), 144–150.
- Gupta, D.; Rani, M.; Khan, N.; Jameel, S. HIV-1 Infected Peripheral Blood Mononuclear Cells Modulate the Fibrogenic Activity of Hepatic Stellate Cells through Secreted TGF-β and JNK Signaling. PLoS ONE 2014, 9 (3), e91569. [CrossRef]
- Ribeiro, C. R. de A.; Beghini, D. G.; Lemos, A. S.; Martinelli, K. G.; de Mello, V. da M.; de Almeida, N. A. A.; Lewis-Ximenez, L. L.; de Paula, V. S. Cytokines Profile in Patients with Acute and Chronic Hepatitis B Infection. Microbiology and Immunology 2022, 66 (1), 31–39. [CrossRef]
- Zajkowska, M.; Mroczko, B. Chemokines in Primary Liver Cancer. Int J Mol Sci 2022, 23 (16), 8846. [CrossRef]
- da Cruz, N. S.; Pasquarelli-do-Nascimento, G.; e Oliveira, A. C. P.; Magalhães, K. G. Inflammasome-Mediated Cytokines: A Key Connection between Obesity-Associated NASH and Liver Cancer Progression. Biomedicines 2022, 10 (10), 2344. [CrossRef]
- Naseem, S.; Hussain, T.; Manzoor, S. Interleukin-6: A Promising Cytokine to Support Liver Regeneration and Adaptive Immunity in Liver Pathologies. Cytokine & Growth Factor Reviews 2018, 39, 36–45. [CrossRef]
- You, R.; Jiang, H.; Xu, Q.; Yin, G. Preintervention MCP-1 Serum Levels as an Early Predictive Marker of Tumor Response in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization. Transl Cancer Res 2021, 10 (2), 966–976. [CrossRef]
- Matsui, D.; Nagai, H.; Mukozu, T.; Ogino, Y.; Sumino, Y. VEGF in Patients with Advanced Hepatocellular Carcinoma Receiving Intra-Arterial Chemotherapy. Anticancer Research 2015, 35 (4), 2205–2210.
- Sadeghi, M.; Lahdou, I.; Oweira, H.; Daniel, V.; Terness, P.; Schmidt, J.; Weiss, K.-H.; Longerich, T.; Schemmer, P.; Opelz, G.; Mehrabi, A. Serum Levels of Chemokines CCL4 and CCL5 in Cirrhotic Patients Indicate the Presence of Hepatocellular Carcinoma. Br J Cancer 2015, 113 (5), 756–762. [CrossRef]
- Choi, S. B.; Han, H. J.; Kim, W. B.; Song, T. J.; Choi, S. Y. VEGF Overexpression Predicts Poor Survival in Hepatocellular Carcinoma. Open Medicine 2017, 12 (1), 430–439. [CrossRef]
- Dong, G.; Fan, F.; He, Y.; Luo, Y.; Yu, J.; Liang, P. T-Lymphocyte Gene-Regulated CCL5 and Its Association with Extrahepatic Metastasis in Hepatocellular Carcinoma. JHC 2023, 10, 1267–1279. [CrossRef]
- Soliman, H. H.; Nagy, H.; Kotb, N.; El-Din, M. A. A. The Role of Chemokine CC Ligand 20 in Patients with Liver Cirrhosis and Hepatocellular Carcinoma. Int J Biol Markers 2012, 27 (2), 125–131. [CrossRef]
- Beckebaum, S.; Zhang, X.; Chen, X.; Yu, Z.; Frilling, A.; Dworacki, G.; Grosse-Wilde, H.; Broelsch, C. E.; Gerken, G.; Cicinnati, V. R. Increased Levels of Interleukin-10 in Serum from Patients with Hepatocellular Carcinoma Correlate with Profound Numerical Deficiencies and Immature Phenotype of Circulating Dendritic Cell Subsets. Clinical Cancer Research 2004, 10 (21), 7260–7269. [CrossRef]
- Qian, Q.; Wu, C.; Chen, J.; Wang, W. Relationship between IL10 and PD-L1 in Liver Hepatocellular Carcinoma Tissue and Cell Lines. BioMed Research International 2020, 2020, e8910183. [CrossRef]
- Rubie, C.; Frick, V. O.; Wagner, M.; Rau, B.; Weber, C.; Kruse, B.; Kempf, K.; Tilton, B.; König, J.; Schilling, M. Enhanced Expression and Clinical Significance of CC-Chemokine MIP-3α in Hepatocellular Carcinoma. Scandinavian Journal of Immunology 2006, 63 (6), 468–477. [CrossRef]
- Zhang, S.; Gan, X.; Qiu, J.; Ju, Z.; Gao, J.; Zhou, J.; Shi, C.; Zhu, Y.; Li, Z. IL-10 Derived from Hepatocarcinoma Cells Improves Human Induced Regulatory T Cells Function via JAK1/STAT5 Pathway in Tumor Microenvironment. Molecular Immunology 2021, 133, 163–172. [CrossRef]
- Ji, X.; Guo, W.; Gu, X.; Guo, S.; Zhou, K.; Su, L.; Yuan, Q.; Liu, Y.; Guo, X.; Huang, Q.; Xing, J. Mutational Profiling of MtDNA Control Region Reveals Tumor-Specific Evolutionary Selection Involved in Mitochondrial Dysfunction. eBioMedicine 2022, 80. [CrossRef]
- Li, M.; Foli, Y.; Liu, Z.; Wang, G.; Hu, Y.; Lu, Q.; Selvaraj, S.; Lam, W.; Paintsil, E. High Frequency of Mitochondrial DNA Mutations in HIV-infected Treatment-experienced Individuals. HIV Med 2017, 18 (1), 45–55. [CrossRef]
- de Mendoza, C.; Sánchez-Conde, M.; Timmermans, E.; Buitelaar, M.; de Baar, M. P.; Gonzalez-Lahoz, J.; Soriano, V. Mitochondrial Dna Depletion in HIV-Infected Patients Is More Pronounced with Chronic Hepatitis C and Enhanced Following Treatment with Pegylated Interferon plus Ribavirin. Antiviral Therapy 2005, 10 (4), 557–561. [CrossRef]
- Yu, C.; Wang, X.; Huang, L.; Tong, Y.; Chen, L.; Wu, H.; Xia, Q.; Kong, X. Deciphering the Spectrum of Mitochondrial DNA Mutations in Hepatocellular Carcinoma Using High-Throughput Sequencing. Gene Expr 2018, 18 (2), 125–134. [CrossRef]
- Vadrot, N.; Ghanem, S.; Braut, F.; Gavrilescu, L.; Pilard, N.; Mansouri, A.; Moreau, R.; Reyl-Desmars, F. Mitochondrial DNA Maintenance Is Regulated in Human Hepatoma Cells by Glycogen Synthase Kinase 3β and P53 in Response to Tumor Necrosis Factor α. PLoS ONE 2012, 7 (7), e40879. [CrossRef]
- Giampazolias, E.; Tait, S. W. G. Mitochondria and the Hallmarks of Cancer. The FEBS Journal 2016, 283 (5), 803–814. [CrossRef]
Figure 1.
Expression of inflammatory cytokines associated with pre-cancer and initiation of HCC in HCC+ compared to HIV+ participants coinfected with or without hepatitis B and C viruses. The grey bar denotes HIV/Hep+ participants, white bar denotes HIV/Hep- participants, and black bar denotes the HCC+ participants. The sample were run in duplicates, the bar graphs with error bars were represented as median and 95% CI respectively. Differences between groups were tested by Mann-Whitney U test and significance was considered at p (p-value) < 0.05.
Figure 1.
Expression of inflammatory cytokines associated with pre-cancer and initiation of HCC in HCC+ compared to HIV+ participants coinfected with or without hepatitis B and C viruses. The grey bar denotes HIV/Hep+ participants, white bar denotes HIV/Hep- participants, and black bar denotes the HCC+ participants. The sample were run in duplicates, the bar graphs with error bars were represented as median and 95% CI respectively. Differences between groups were tested by Mann-Whitney U test and significance was considered at p (p-value) < 0.05.
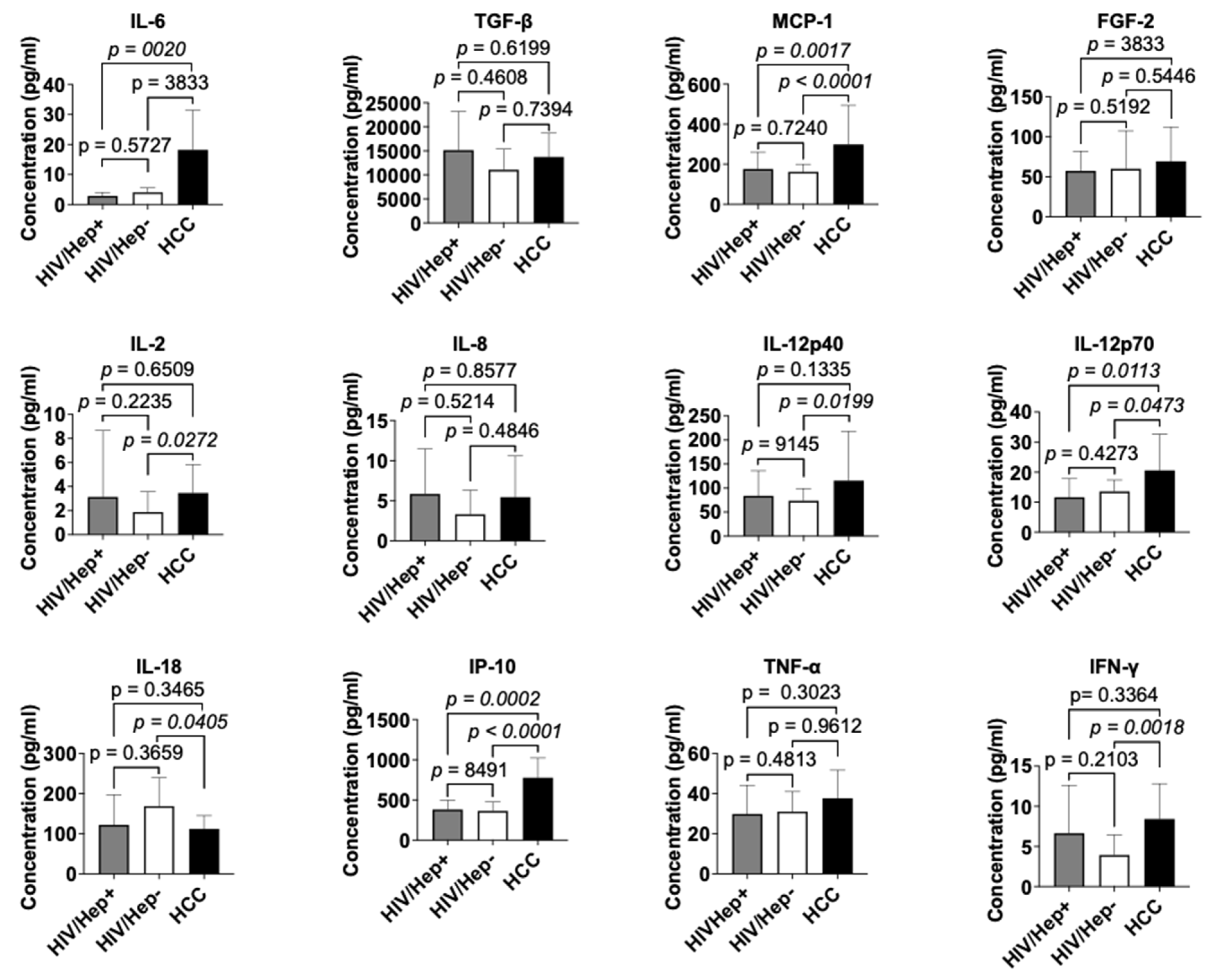
Figure 2.
Expression of cytokines implicated in the early and advanced stages of HCC in HCC+ compared to HIV+ participants coinfected with or without hepatitis B and C viruses. (A) Cytokines implicated in the early or developmental stage of HCC. (B) Cytokines implicated in the advanced stage of HCC. The grey bar denotes HIV/Hep+ participants, white bar denotes HIV/Hep- participants, and black bar denotes the HCC+ participants. The sample were run in duplicates, the bar graphs with error bars were represented as median and 95% CI respectively. Differences between groups were tested by Mann-Whitney U test and significance was considered at p (p-value) < 0.05.
Figure 2.
Expression of cytokines implicated in the early and advanced stages of HCC in HCC+ compared to HIV+ participants coinfected with or without hepatitis B and C viruses. (A) Cytokines implicated in the early or developmental stage of HCC. (B) Cytokines implicated in the advanced stage of HCC. The grey bar denotes HIV/Hep+ participants, white bar denotes HIV/Hep- participants, and black bar denotes the HCC+ participants. The sample were run in duplicates, the bar graphs with error bars were represented as median and 95% CI respectively. Differences between groups were tested by Mann-Whitney U test and significance was considered at p (p-value) < 0.05.
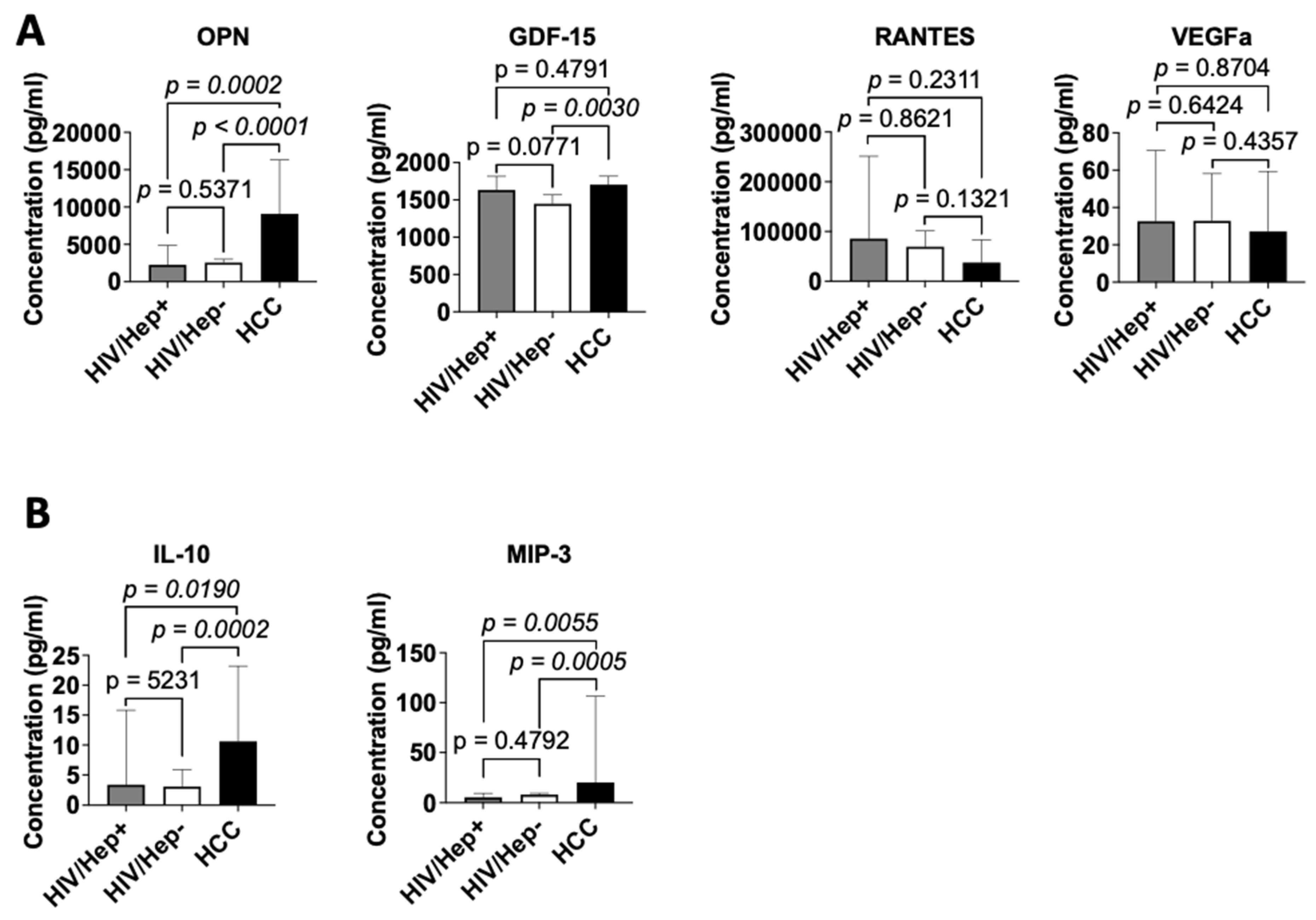

Table 1.
Demographic and exposure characteristics of study participants.
| HIV+ N (%) 60 (64.5) |
HCC+ N (%) 33 (35.5) |
Total N (%) 93 (100.0%) |
P value | |
|---|---|---|---|---|
| Gender | ||||
| Female | 43 (71.7) | 15 (45.5) | 58 (62.8) | < 0.01 |
| Male | 17 (28.3) | 18 (54.5) | 35 (27.2) | |
| Age | ||||
| < 50 | 27 (45.0) | 16 (48.5) | 43 (46.2) | 0.31 |
| ≥ 50 | 33 (55.0) | 17 (51.5) | 50 (53.8) | |
| Mean ± SD | 51 ± 11 | 50 ± 15 | 50 ± 13 | |
| Educational Level | ||||
| ≤ Junior High School | 45 (75.0) | 15 (45.5) | 60 (64.5) | < 0.01 |
| > Junior High School | 15 (25.0) | 18 (54.5) | 33 (35.5) | |
| History/Exposure | ||||
| Family history of cancer | 2 (3.3) | 5 (15.2) | 7 (13.2) | 0.04 |
| Hypertension | 33 (55.0) | 13 (39.4) | 46 (49.5) | 0.15 |
| Smoking | 1 (1.7) | 2 (6.1) | 3 (3.2) | 0.26 |
| Alcohol | 30 (50.0) | 19 (57.6) | 49 (52.7) | 0.48 |
| Virus Infection | ||||
| HCV | 6 (10.0) | 7 (21.2) | 13 (14.0) | 0.14 |
| HBV | 10 (16.7) | 31 (93.9) | 41 (44.1) | < 0.01 |
| Hepatitis B and C coinfection | 0 (0.0) | 5 (15.2) | 5 (5.4) | < 0.01 |
Table 2.
HIV-associated characteristic in the HIV+ participants.
| Variable | HIV+ | |
|---|---|---|
| N (%) | P-value | |
| Years Diagnosed | ||
| < 10 | 26 (43.3) | 0.35 |
| ≥ 10 | 31 (51.7) | |
| Missing | 3 (5.0) | |
| Years on ART | ||
| < 10 | 28 (46.7) | 1.00 |
| ≥ 10 | 28 (46.7) | |
| Missing | 4 (6.7) | |
| HIV Stage | ||
| 1 | 24 (40.0) | < 0.01 |
| 2 | 10 (16.7) | |
| 3 | 13 (21.7) | |
| 4 | 8 (13.3) | |
| Missing | 5 (8.3) | |
| Viral Load | ||
|
≤ 50 Median (Range) |
43 (71.7) < 20 (< 20 - 30) |
< 0.01 |
| > 50 Median (Range) |
12 (20.0) 5731.5 (52 - 2.5e5) |
|
| Missing | 5 (8.3) | |
| CD4 count | ||
| < 200 Median (Range) |
5 (8.3) 159 (21 - 183) |
< 0.01 |
| 200 – 499 Median (Range) |
17 (28.3) 383 (202 - 495) |
|
| > 500 Median (Range) |
25 (41.7) 721 (502 - 1353) |
|
| Missing | 5 (100.0) | |
Table 3.
Liver function tests (liver enzymes and proteins) in the HIV+ and HCC+ cohorts.
| Variable | Study Cohort | P value | |
|---|---|---|---|
| HIV+ | HCC+ | ||
| ALT (IU/L) | |||
| Median (Range) | 22 (7 - 123) | 62 (17 - 553) | < 0.01 |
| Normal Range | 7 to 55 | ||
| AST (IU/L) | |||
| Median (Range) | 32 (17 - 106) | 91 (19 - 870) | < 0.01 |
| Normal Range | 8 to 48 | ||
| ALP (IU/L) | |||
| Median (Range) | 99.5 (0 - 323) | 207 (91 - 1581) | < 0.01 |
| Normal Range | 44 to 147 | ||
| Albumin (g/L) | |||
| Median (Range) | 41 (4.3 - 267) | 35 (21 - 46) | 0.04 |
| Normal Range | 34 to 55 | ||
| Bilirubin (µmol/L) | |||
| Median (Range) | 7.9 (0 - 73) | 23.1 (4 - 680) | < 0.01 |
| Normal Range | 1.7 to 20.5 | ||
Table 4.
Correlation of cytokines in PLWH. Values in red denote significant correlations of the level of cytokines among individuals living with HIV.
Table 4.
Correlation of cytokines in PLWH. Values in red denote significant correlations of the level of cytokines among individuals living with HIV.
| HIV+ | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IL-6 | TGFb | MCP1 | FGF-2 | VEGF | OPN | GDF-15 | RANTES | IL-10 | MIP-3 | IP-10 | IL-2 | IL-8 | IL-12p70 | IL-12p40 | IL-18 | TNF-α | IFN-γ | ||
| HIV+ | IL-6 | 1 | |||||||||||||||||
| TGF-β | 0.52 | 1 | |||||||||||||||||
| MCP1 | 0.27 | -0.06 | 1 | ||||||||||||||||
| FGF-2 | 0.56 | 0.69 | 0.05 | 1 | |||||||||||||||
| VEGF | 0.37 | 0.60 | 0.06 | 0.46 | 1 | ||||||||||||||
| OPN | 0.41 | 0.29 | -0.02 | 0.11 | 0.23 | 1 | |||||||||||||
| GDF-15 | -0.13 | -0.33 | 0.17 | -0.18 | -0.29 | -0.26 | 1 | ||||||||||||
| RANTES | 0.37 | 0.87 | 0.00 | 0.55 | 0.66 | 0.30 | -0.35 | 1 | |||||||||||
| IL-10 | 0.22 | 0.01 | 0.17 | -0.03 | 0.02 | 0.42 | 0.16 | -0.03 | 1 | ||||||||||
| MIP-3 | 0.22 | 0.09 | 0.00 | 0.02 | 0.11 | 0.09 | -0.12 | 0.02 | -0.07 | 1 | |||||||||
| IP-10 | 0.08 | -0.03 | 0.38 | 0.01 | 0.00 | 0.03 | 0.13 | -0.03 | 0.31 | 0.02 | 1 | ||||||||
| IL-2 | 0.57 | 0.20 | 0.43 | 0.42 | 0.29 | 0.21 | 0.00 | 0.22 | 0.24 | -0.06 | 0.21 | 1 | |||||||
| IL-8 | 0.43 | 0.64 | -0.28 | 0.63 | 0.32 | 0.20 | -0.28 | 0.49 | -0.14 | 0.09 | -0.07 | -0.12 | 1 | ||||||
| IL-12p70 | 0.56 | 0.24 | 0.52 | 0.25 | 0.33 | 0.29 | 0.02 | 0.26 | 0.47 | -0.10 | 0.32 | 0.76 | -0.10 | 1 | |||||
| IL-12p40 | 0.59 | 0.26 | 0.52 | 0.22 | 0.25 | 0.34 | -0.04 | 0.23 | 0.40 | -0.08 | 0.29 | 0.72 | -0.12 | 0.89 | 1 | ||||
| IL-18 | 0.24 | 0.22 | 0.05 | 0.11 | 0.07 | -0.12 | 0.06 | 0.17 | -0.01 | -0.11 | 0.13 | 0.03 | 0.35 | 0.11 | 0.02 | 1 | |||
| TNF-α | 0.52 | 0.85 | -0.08 | 0.65 | 0.56 | 0.23 | -0.19 | 0.68 | -0.01 | 0.06 | 0.08 | 0.08 | 0.68 | 0.12 | 0.16 | 0.27 | 1 | ||
| IFN-γ | 0.38 | 0.06 | 0.04 | 0.46 | 0.22 | 0.05 | 0.06 | 0.07 | 0.06 | -0.04 | 0.10 | 0.73 | 0.00 | 0.38 | 0.26 | 0.12 | 0.00 | 1 | |
Table 5.
Frequency of mtDNA deletion among the HIV+ and HCC+ cohort.
| Variable | Study Cohort | |||
|---|---|---|---|---|
| HIV+ | HCC+ | Total | P value | |
| mtDNA mutation | ||||
| Present | 36 (60.0) | 21 (63.6) | 57 (61.3) | 0.730 |
| Absent | 24 (40.0) | 12 (36.4) | 36 (38.7) | |
| P value | 0.03 | 0.03 | < 0.01 | |
| Age | ||||
| 18-39 | 3/7 (42.9) | 4/7 (57.1) | 7/14 (50.0) | 0.59 |
| 40-49 | 9/20 (45.0) | 5/9 (55.6) | 14/29 (48.3) | 0.60 |
| ≥ 50 | 24/33 (72.7) | 12/17 (70.5) | 36/50 (72.0) | 0.87 |
| P value | 0.13 | 0.42 | 0.07 | |
| Sex | ||||
| Female | 22/43 (51.2) | 9/15 (60.0) | 31/58 (53.4) | 0.55 |
| Male | 14/17 (82.4) | 12/18 (66.7) | 26/35 (74.3) | 0.29 |
| P value | 0.03 | 0.69 | 0.05 | |
| Alcohol history | ||||
| Yes | 18/30 (60.0) | 10/19 (52.6) | 28/49 (57.1) | 0.61 |
| No | 18/30 (60.0) | 11/14 (78.5) | 29/44 (65.9) | 0.23 |
| P value | 1.00 | 0.13 | 0.39 | |
Table 6.
Risks associated with mtDNA deletions in PLWH.
| Variable | mtDNA deletion | OR (CI) | P value | |
|---|---|---|---|---|
| Yes (%) | No (%) | |||
| Age | ||||
| < 50 | 12 (44.4) | 15 (55.6) | 1 | |
| ≥ 50 | 24 (72.7) | 9 (27.3) | 3.3 (1.1 – 9.8) | 0.03 |
| Sex | ||||
| Female | 22 (51.2) | 21 (48.8) | 1 | |
| Male | 14 (82.4) | 3 (17.6) | 4.5 (1.1 – 17.8) | 0.03 |
| Years Diagnosed | ||||
| < 10 | 11 (42.3) | 15 (57.7) | 1 | |
| ≥ 10 | 22 (71.0) | 9 (29.0) | 3.3 (1.1 – 10.0) | 0.03 |
| Years on ART | ||||
| < 10 | 14 (50.0) | 14 (50.0) | 1 | |
| ≥ 10 | 19 (67.9) | 9 (32.1) | 2.1 (0.7 – 6.2) | 0.18 |
| Viral Load | ||||
| ≤ 50 | 25 (58.1) | 18 (41.9) | 1 | |
| > 50 | 9 (75.0) | 3 (25.0) | 2.2 (0.5 – 9.1) | 0.29 |
| CD4 count | ||||
| < 200 | 1 (20.0) | 4 (80.0) | 0.1 (0.0 – 1.5) | 0.10 |
| 200 – 499 | 13 (76.5) | 4 (23.5) | 1.8 (0.5 – 7.3) | 0.39 |
| > 500 | 16 (64.0) | 9 (36.0) | 1 | |
| Hepatitis status | ||||
| Positive | 11 (68.8) | 5 (21.2) | 1.7 (0.5 -5.6) | 0.47 |
| Negative | 25 (56.8) | 19 (43.2) | 1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



