
Submitted:
18 October 2023
Posted:
19 October 2023
You are already at the latest version
Abstract
Delayed discharge for non-clinical reasons is defined as a period of stay that continues after a patient has been deemed medically fit to leave the hospital but is unable to do so for non-medical reasons. This circumstance overburdens the healthcare system and constitutes a major problem for healthcare systems and the patients themselves in this situation.The aim of this study was to evaluate the delay in effective discharge for non-medical reasons in patients admitted to acute care hospitals in Spain. A scoping review was conducted in order to revise and obtain an up-to-date review. The initial search strategy identified a total of 123 references, which were successively screened to a final selection of 13 studies. To conclude, delayed discharge from hospital for non-clinical reasons is a multifactorial problem. It may be due to factors internal or external to the hospital, as well as personal factors. The main causes of the delay are similar among the studies found, as are the clinical characteristics of the patients, most of whom are elderly, frail, and more dependent due to declining functional capacities. Further studies addressing the socio-familial characteristics of the patients and the perspective of the patient and families would be necessary.
Keywords:
Delayed discharges
; Discharge delays
; Bed-blocking
; Timely discharge
; Unnecessary days
; Inappropriate stays
1. Introduction
Delayed hospital discharge is a quality-of-care issue shared by many healthcare systems worldwide [1]. It is defined as “a period of stay that continues after a patient has been deemed medically fit to leave the hospital but is unable to do so for non-medical reasons” [2].
This circumstance overburdens the healthcare system and constitutes a major problem for healthcare systems and the patients themselves in this situation, as care normally diminishes or stops completely while they are waiting to be discharged, putting patients at risk of functional impairment [3], falls [4], and infections [5]. Delayed discharges are not simply a product of increasingly complex patients’ needs but the result of inefficiencies within and between health sectors and organizations [6].
Progressive ageing of the population and increased number of dependent people, together with social changes experienced in the last decades have modified socio-familial structures. According to projections from the National Institute of Statistics (INE, by its acronym in Spanish), people aged 65 and over will account for 26.5% of the whole Spanish population by 2035 [7]. Moreover, high prevalence of loneliness among the elderly has proven to be linked to health and satisfaction with formal and informal care [8]. According to these data, delayed discharges are expected to be an emerging issue in Spain. However, the incidence of this problem and its clinical and socio-familial characteristics have been scarcely evaluated to date in the country.
Spain has a national health service that provides tax-funded universal care, each Autonomous Community being responsible for managing their own health services. In 2006, the «Law to promote personal autonomy and care for dependent people» was passed: a project to finance the needs of dependent people [9].
Delayed discharges are known to be strongly affected by the level of coordination between the health and social care systems on the long term. Thus, the ongoing expansion of care to dependent people since the passing of the law has proven to help reduce inefficiencies in hospital care, as well as the number and frequency of hospitalisations [8].
A study carried out in Spain in 2009 on patients admitted to Internal Medicine (IM) units found 3.5% incidence of discharge delays [10], while another performed between 2007 and 2015 studying all cases of delayed discharges in the hospitalisation units of a General University Hospital of Cantabria identified 3015 cases of delayed discharges during the study period. This amounts to a proportion of 0.93% of all discharges [11]. Both studies share the limitations of identifying the characteristics of the patient and his/her environment, and functional dependency, which can lead to endogeneity when explaining discharge delays.
Furthermore, the issue of delayed discharges is influenced by local social and health resources, thus limiting results and their comparability. The findings can help identify the necessary realistic measures to improve this situation in Spain.
In view of the above, the study of delayed discharge for non-clinical reasons is relevant mainly because demographic evolution can worsen the issue. The study aims at analysing delayed effective discharges for non-medical reasons of patients admitted to acute care hospitals in Spain.
2. Materials and Methods
A Scoping Review was carried out of the studies analysing delayed effective discharge for non-medical reasons of patients admitted to acute care hospitals in Spain.
It was performed following the Joanna Briggs Institute manual, Arksey and O´Malley protocol [12], and Prisma criteria for Scoping reviews [13].
2.1. Search Strategy
The review was carried out according to JBI methodology [14], and a five-step methodological framework was used for additional support following Arksey H and al. criteria [12]:
- Stage 1: Identification of the research question.
- Stage 2: Identification of pertinent or relevant studies.
- Stage 3: Studies selection according to inclusion criteria.
- Stage 4: Data registration and report.
- Stage 5: Collection, summary, and communication of results.
Firstly, a search was carried out to contextualize and update the research topic using databases such as PubMed and resources like ScienceDirect. Besides allowing to analyse the current scenario of the research topic, it also permitted to identify descriptors («delayed discharges», «discharge delays», «bed-blocking», «timely discharge», «unnecessary days» and «inappropriate stays») later used for literature searching.
Table 1 shows the search strategy applied on 28 March 2023 for each database used in the search process.
2.2. Study Selection Criteria
Quantitative or qualitative studies published in scientific journals on delayed effective discharge for non-medical reasons of patients admitted to hospital for any health issue of medical and/or surgical origin were selected. Only studies published in English or Spanish were considered. The search period was from January to March 2023.
Studies analysing the impact and experiences of delayed discharge were included if they fulfilled one or more of the following inclusion criteria:
- Quantitative data on the impact of delayed discharge on health outcomes (e.g., care quality, satisfaction, number of infections, mental health, mortality, morbidity, readmissions, and functionality)
- Qualitative data on delayed discharge experiences from the perspective of patients (e.g., perceived impact on health or patient’s experience), health professionals and hospitals
- Information on delayed discharge costs due to unnecessary hospitalisation days
Summaries, editorials, comments, and book reviews were excluded.
The search started with a selection of papers according to tittle, summary, and key words by two reviewers acting in parallel and independently and including them in the study once the paper was entirely reviewed. Doubts about the inclusion or exclusion of a paper were solved by consensus of two authors. References of all papers selected were then revised in search of another paper suitable to be included.
2.3. Data Analysis
Information collection of the documents was performed using a structured datasheet specifically developed by the authors following JBI recommendations for data collection [14]. From each paper included the following information was collected: i) Author, publication year. ii) Tittle. iii) Geographical location of the study. iv) Design and aim of the study. v) Summary of results.
3. Results
The initial search strategy identified a total of 123 references which were subsequently screened according to the aim of this review. A total of 13 studies were finally selected (Figure 1).
Table 2 shows the characteristics of all 13 studies included in this review. They were classified by author and publication year, context, design and aim, participants, and main findings.
4. Discussion
Literature on delayed effective discharge for non-medical reasons of patients admitted to acute hospitals in Spain is limited.
To enable comparison over time between different studies a consistent definition of the concept of discharge delay, delayed discharge or bed-blocking is needed. Considering it is a subjective decision taken by a physician, the question of when and why different patients are qualified as “Bed-blocking” should be carefully studied. Other expressions used as synonyms are long stays, discharge delay, transfer delay, inadequate hospitalisation days, alternative level of care, barrier days [16].
The most common definition in the selected papers was that delayed discharge for non-clinical reasons or bed-blocking is an extended period of stay starting when the patient is considered clinically stable for discharge but remains at hospital for non-medical reasons [2].
Another term found is inappropriate hospital use. It is defined as a hospital admission to provide care that could have been given in a less complex healthcare environment at a lower cost [23].
Two tools used to assess the need of admission and the causes of inadequacy were identified. On the one hand, the Appropriateness Evaluation Protocol (AEP) which is best known and most frequently used and consists of explicit criteria on medical care, nursing care, and patients’ clinical condition. Fulfilment of these criteria justifies days of stay; inversely, not meeting any criterium is considered an inadequate situation [15,21,22,23].
The other tool is by adeQhos®. It is an easy to use, quick questionnaire filled in by the clinicians themselves incorporating a subjective clinical criterium [24].
The definition is also relevant to assess the selection of study subjects. Studies were found whose patients’ samples were patients who had already been given a discharge date by the hospital but were still occupying hospital beds for non-clinical reasons. Namely, patients deemed fit to be discharged by the admissions unit of the hospital but whose actual discharge was delayed for over 24 hours [11,17,20].
Another study included patients who remained in the hospital despite having been declared clinically fit to be discharged by their attending physician without specifying minimum delay time [10].
Hence, there is no consensus as to when a case ought to be considered delayed discharge for non-clinical reasons. Although most authors agree that the patient remains in the hospital despite having been deemed clinically fit for discharge, there is a lack of objective criteria to define such fitness.
As to prevalence data, the proportion was found to vary widely depending on whether the study focused on total number of hospital beds or specific units, such as those of geriatric patients with a chronic disease. Thus, these findings should be taken with caution. The study by Pellico-López et al. during the period between 2007 and 2015 [11] found a prevalence of 0.93% of inadequate stays among the total number of discharges despite the HUMV being authorised to transfer patients to a private long-stay centre having an agreement with the national health service to provide functional recovery care and rehabilitation or palliative care as an intermediate care step between hospitalisation and community during the study period.
Mean admission stays after being discharged vary widely between studies, ranging from 5 days (range: 3-12 days) [10] in a study only including IM patients to 7.34 days in the studies carried out in the HUMV between 2007 and 2015 [11]; with slight variations depending on the cause for admission: from 7.12 days in hip processes [16] to 7.61 days in admissions for pneumonia [17]. Data from three public hospitals in Cantabria from 2010 to 2014 revealed a mean delayed stay of 13.56 days [20].
Causes of delayed discharge can be divided into clinical and care-related characteristics.
As to demographic characteristics, it was found that in the studies developed in the HUMV during the period from 2007 to 2015 mean age of patients was 77.28 years and 65.97% of patients were over 75 [11]. In stroke cases, mean age increased to 79.7 years [18].
A previous study with IM patients showed lower mean age: 75.74 years. Still, mean age of patients with delayed discharge was higher than that of the total number of patients admitted to IM units [10].
Overall, the studies consulted agreed that patients over 75 have longer stays and are more likely to endure delayed discharges.
As far as sex, an even distribution was found.
Older age and diseases causing an abrupt functionality decline and dependency are the most common characteristics in frail elderly people. Mendoza et al. study found higher prevalence of discharge delays in patients with acute cerebrovascular disease and problems related to the consumption of alcohol or benzodiazepines [10]
The complexity of patients’ processes has also been connected to delayed discharges, using Diagnosis Related Groups (DRG) to measure it. The most frequent DRGs were those linked to stroke (6.1%) and other nervous system disorders (5.6 %), pneumonia (4.1 %) and hip procedures (3.3 %) [11].
However, not all cases of delayed discharge were more complex. It was found that 10.0% of apparently simple DRGs had had delayed discharges, probably for having been admitted to hospital due to overload or lack or carer and having to resort to hospitalisation pending social care [11]. This study provides data from various units, finding links between delayed discharges and units in charge, and obtaining the longest stays in surgical units [11].
As to the effects of this problem, it was found that discharge delays for non-clinical reasons has negative repercussions beside inefficient or inappropriate use of beds in acute hospitals. A review was found by Rojas-García et al. connecting delayed stays with an increased risk of healthcare-related infections, surgical intervention delays, death, loss of functional capacity, and negative emotional impact on the patient who presented symptoms of anxiety and depression [2].
One of the causes analysed in the selected studies was death. In the study by Mendoza et al. , 15.7% of patients whose discharge was delayed died pending the resource they had applied for due to nosocomial infection in 18% of the cases [10]. Lower numbers were obtained in the HUMV study where 6.57% of delayed discharge cases died during the study period. It was found that the cases of delayed discharge admitted to medical units were more likely to die and over a third were oncology patients [19].
The study by Mendoza et al. shows that in 98.8% of delayed discharge cases the reason was some kind of socio-familial-related problem whereas the remaining 1.17% were due to problems with the department in charge of patients’ transfers. The main reasons given for discharge delays were family overload and/or inability to care for the patient for being unable to balance the care needed by the patient and work life (51.8%), and lack of family or social support network (21.8%) [10].
Family refusal to home-based care and lack of alternative care centres accounted for 6.2% of cases each [23].
Despite the extent of the problem in Spain, only two papers analysing interventions to deal with the issue were found.
A pre- and post-intervention study was carried out in 2007 in 10 acute care hospitals of Catalonia including 2 intervention groups and their corresponding control groups. Intervention was performed using adeQhos® questionnaire in the patients’ visitor pass. The same reviewers evaluated adequacy using the Appropriateness Evaluation Protocol (AEP) prior and post intervention. No significant decrease in hospital inadequacy was observed after a low intensity intervention [24].
A later study by Soria-Aledo et al. using the same protocol did a retrospective audit on a first stage (pre) to analyse a random sample of the medical records from patients admitted to hospital using AEP (control group). Then, an improvement cycle was performed implementing measures to reduce admissions and inappropriate stays, and, finally, a second evaluation was carried out re-measuring admissions and inappropriate stays using a retrospective random sample of medical records (intervention group). The measures implemented were educational sessions with all clinical units to inform about outcomes and discuss potential measures to reduce inadequacy of admissions and stays; spreading the use of the preliminary discharge report; and creation of specific circuits to perform radiology studies to priority emergency patients and those newly diagnosed with cancer. Inadequate admissions decreased by 4.2% in the intervention group. Inappropriate stays also diminished significantly from 24.6% to 10.4%. Inadequacy cost in the study sample dropped from 147,044 euros to 66,642 euros [23].
This review comes with several limitations. Firstly, literature available in Spain is scarce. Secondly, most works included are cross-sectional observational studies that do not allow causality inferences, and samples lack representativity. Thirdly, not all authors have used the same measuring tools because outcomes may not be homogeneous. More research is needed on the topic to determine the reason of the problem of delayed discharge for non-clinical reasons. Moreover, the definition of the concept focuses only on acute hospital care for adults from the organisation’s perspective. Besides, identified studies are quantitative. No primary qualitative studies focusing on personal experience of patients and families were found to allow a global overview of the problem.
In conclusion, discharge delays are confirmed to be a multifactorial issue. They can be caused by factors internal or external to hospitals, as well as personal factors. The main reasons of the delay are similar among the studies found, and so are the medical characteristics of the patients, most of whom are elderly, frail, and more dependent due to declining functional capacities. Little is mentioned about the socio-familial characteristics of the patients. Further research is thus needed on these variables to know the causes of the issue and potential interventions for improvement from the perspective of patients and families.
Author Contributions
N.L.L.: literature search, research draft, data collection, analysis and discussion, and editing. C.R.-Á.: discussion, conclusions and editing. Á.A.: discussion, conclusions and editing. L.C.-P.: literature review. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Public Involvement Statement
There was no public involvement in any aspect of this research.
Guidelines and Standards Statement
This manuscript was drafted against the Joanna Briggs Institute methodology for scoping reviews research.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Bai, A. D.; Dai, C.; Srivastava, S.; Smith, C. A.; Gill, S. S. Risk factors, costs and complications of delayed hospital discharge from internal medicine wards at a Canadian academic medical centre: retrospective cohort study. BMC Health Serv Res 2019, 19, 935. [Google Scholar] [CrossRef] [PubMed]
- Rojas-García, A.; Turner, S.; Pizzo, E.; Hudson, E.; Thomas, J.; Raine, R. Impact and experiences of delayed discharge: A mixed-studies systematic review. Health Expectations 2018, 21, 41–56. [Google Scholar] [CrossRef] [PubMed]
- Barnable, A.; Welsh, D.; Lundrigan, E.; Davis, C. Analysis of the Influencing Factors Associated With Being Designated Alternate Level of Care. Home Health Care Manag Pract 2015, 27, 3–12. [Google Scholar] [CrossRef]
- Walker, D.; Lead, P. A. L. C. Caring for our aging population and addressing alternate level of care; Ontario Ministry of Health and Long-Term Care Toronto, 2011.
- Jasinarachchi, K. H.; Ibrahim, I. R.; Keegan, B. C.; Mathialagan, R.; McGourty, J. C.; Phillips, J. R.; Myint, P. K. Delayed transfer of care from NHS secondary care to primary care in England: its determinants, effect on hospital bed days, prevalence of acute medical conditions and deaths during delay, in older adults aged 65 years and over. BMC Geriatr 2009, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Micallef, A.; Buttigieg, S. C.; Tomaselli, G.; Garg, L. Defining Delayed Discharges of Inpatients and Their Impact in Acute Hospital Care: A Scoping Review. Int J Health Policy Manag 2020. [Google Scholar] [CrossRef] [PubMed]
- INE Proyecciones de Población 2020-2070; 2020. Available online: https://www.ine.es/prensa/pp_2020_2070.pdf (accessed on 11 October 2023).
- Gallardo Peralta, L. P.; Sánchez Moreno, E.; Rodríguez Rodríguez, V.; García Martín, M. La investigación sobre soledad y redes de apoyo social en las personas mayores: una revisión sistemática en Europa. Rev Esp Salud Pública. 2023, 97. [Google Scholar]
- Boletin Oficial del Estado Ley 39/2006, de 14 de diciembre, de Promoción de la Autonomía Personal y Atención a las personas en situación de dependencia; 2006; Vol. 299, p. 15. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-2006-21990 (accessed on 11 October 2023).
- Mendoza Giraldo, D.; Navarro, A.; Sánchez-Quijano, A.; Villegas, A.; Asencio, R.; Lissen, E. Impact of delayed discharge for nonmedical reasons in a tertiary hospital internal medicine department. Rev Clin Esp 2012, 212, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Pellico-López, A.; Cantarero, D.; Fernández-Feito, A.; Parás-Bravo, P.; De Las Cuevas, J. C.; Paz-Zulueta, M. Factors associated with bed-blocking at a university hospital (Cantabria, Spain) between 2007 and 2015: A retrospective observational study. Int J Environ Res Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology: Theory and Practice 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Page, M. J.; Moher, D. Evaluations of the uptake and impact of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Statement and extensions: A scoping review. Syst Rev 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.; Godfrey, C. M.; Mcinerney, P.; Soares, C. B. Methodology for JBI Scoping Reviews Chronic Diseases Management View project Tonsillectomy View project; 2015.
- Rodríguez-Vera, F. J.; Marín Fernández, Y.; Sánchez, A.; Borrachero, C.; Pujol de la Llave, E. Adecuación de los ingresos y estancias en un Servicio de Medicina Interna de un hospital de segundo nivel utilizando la versión concurrente del AEP (Appropriateness Evaluation Protocol). Anales de Medicina Interna 2003, 20, 27–30. [Google Scholar] [CrossRef]
- Pellico-López, A.; Fernández-Feito, A.; Cantarero, D.; Herrero-Montes, M.; Cuevas, J. C. D. Las; Parás-Bravo, P.; Paz-Zulueta, M. Delayed discharge for non-clinical reasons in hip procedures: Differential characteristics and opportunity cost. Int J Environ Res Public Health 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- Pellico-López, A.; Fernández-Feito, A.; Parás-Bravo, P.; Herrero-Montes, M.; Cayón-De las Cuevas, J.; Cantarero, D.; Paz-Zulueta, M. Differential characteristics of cases of patients diagnosed with pneumonia and delayed discharge for non-clinical reasons in Northern Spain. Int J Clin Pract 2021, 75. [Google Scholar] [CrossRef] [PubMed]
- Pellico-López, A.; Fernández-Feito, A.; Cantarero, D.; Herrero-Montes, M.; Cayón-de las Cuevas, J.; Parás-Bravo, P.; Paz-Zulueta, M. Cost of stay and characteristics of patients with stroke and delayed discharge for non-clinical reasons. Sci Rep 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Pellico-López, A.; Herrero-Montes, M.; Cantarero Prieto, D.; Fernández-Feito, A.; Cayon-De las Cuevas, J.; Parás-Bravo, P.; Paz-Zulueta, M. Patient deaths during the period of prolonged stay in cases of delayed discharge for nonclinical reasons at a university hospital: a cross sectional study. PeerJ 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Pellico López, A.; Paz-Zulueta, M.; Fernández-Feito, A.; Parás-Bravo, P.; Santibañez, M.; Cantarero Prieto, D. Cases of bed blockage in Northern Spain during 2010–2014: Delayed discharge from acute hospitalization to long-term care. Rev Epidemiol Sante Publique 2018, 66, S403. [Google Scholar] [CrossRef]
- Soria-Aledo, V.; Carrillo-Alcaraz, A.; Campillo-Soto, Á.; Flores-Pastor, B.; Leal-Llopis, J.; Fernández-Martín, M. P.; Carrasco-Prats, M.; Aguayo-Albasini, J. L. Associated factors and cost of inappropriate hospital admissions and stays in a second-level hospital. American Journal of Medical Quality 2009, 24, 321–332. [Google Scholar] [CrossRef]
- Zambrana García, J. L.; Delgado Fernández, M.; Cruz Caparrós, G.; Escalante, M. D. M.; Díez García, F.; Ruiz Bailén, M. Predictive factors for inappropriate hospital stays in an internal medicine department. Med Clin (Barc) 2001, 117, 90–92. [Google Scholar]
- Soria-Aledo, V.; Carrillo-Alcaraz, A.; Flores-Pastor, B.; Moreno-Egea, A.; Carrasco-Prats, M.; Aguayo-Albasini, J. L. Reduction in inappropriate hospital use based on analysis of the causes, 2012.
- Monteis Catot, J.; Martín-Baranera, M.; Soler, N.; Vilaró, J.; Moya, C.; Francesc Martínez, N.; Riu, M.; Puig, C.; Riba, A.; Navarro, G.; et al. Impacto de una intervención de autoevaluación clínica sobre la adecuación de la estancia hospitalaria, 2007; Vol. 21.
Figure 1.
Search results (Flow chart—PRISMA [13]).
Figure 1.
Search results (Flow chart—PRISMA [13]).
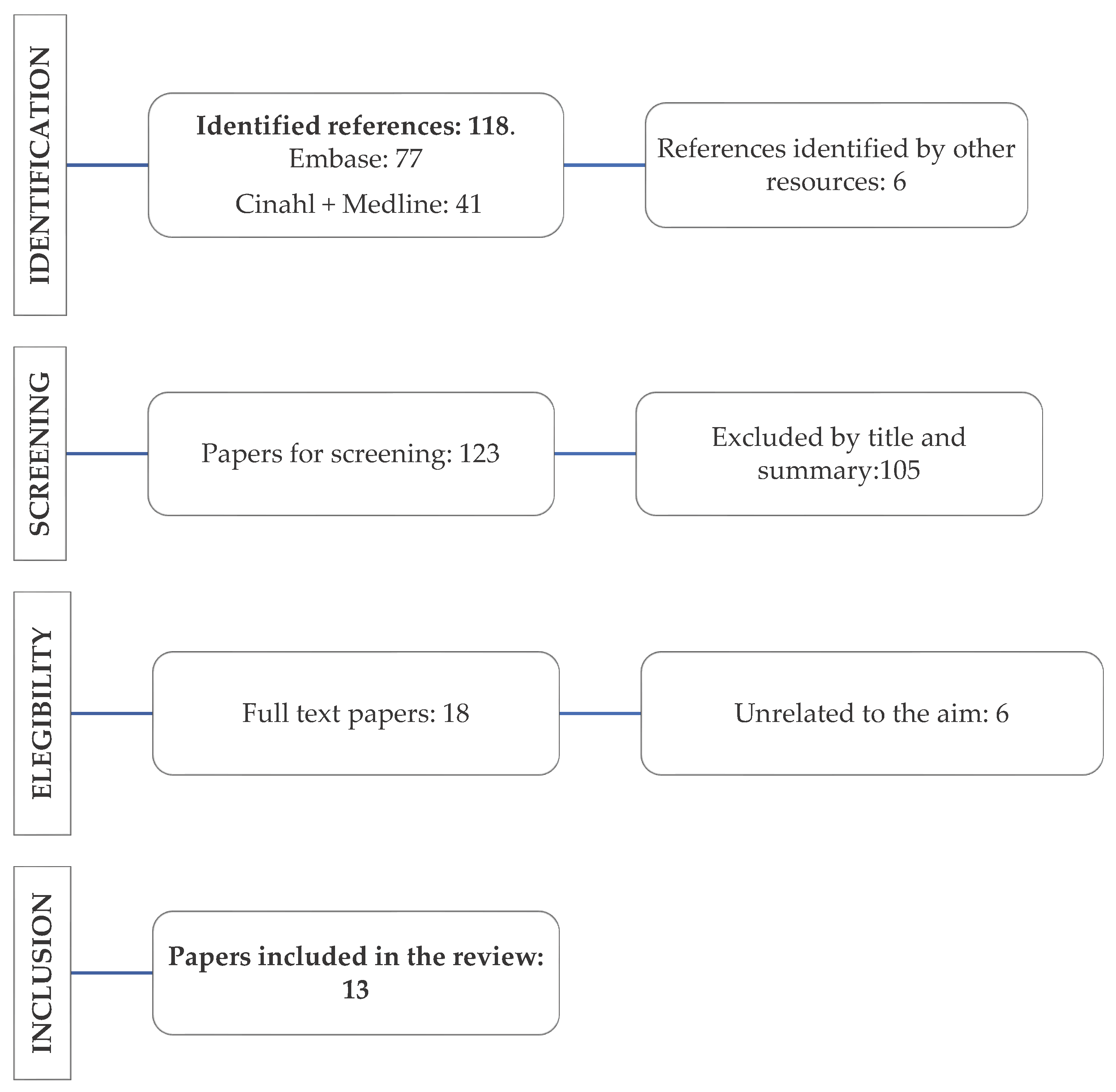

Table 1.
Search strategy used depending on database.
| Database | Search Strategy | Search Date | Results | Selected |
|---|---|---|---|---|
| Embase | ((’delayed discharges’ or ’discharge delays’ or ’bed blocking’ or ’timely discharge’ or ’unnecessary days’ or ’inappropriate stays’) and (’spain’ or ’spanish’)).mp. [mp=title, abstract, full text, caption text] |
28/03/2023 | 77 | 3 |
| CINAHL+ Medline | AB (delayed discharge or delayed discharge from hospital or bed-blocking or delayed transfer of care) AND TX (spain or spanish or españa) |
28/03/2023 | 41 | 10 |
Table 3.
Participants design and main results of the studies included in the review.
| Author and Year | Study Type | Aim | Participants and Context | Main Findings |
|---|---|---|---|---|
| Pellico-López, Fernández-Feito et al., (2022) [18] | Descriptive, observational, cross-sectional, and retrospective study | Describing the costs and characteristics of patients diagnosed with stroke and discharged late for non-clinical reasons, and evaluating the connection between total stay duration and patient’s characteristics and care context | 443 patients diagnosed with stroke and discharged late for non-clinical reasons in the University Hospital “Marqués de Valdecilla” (HUMV, by its Spanish acronym) (2007-2015) | Delayed discharges increase the total duration of stay by approximately a week. These patients with stroke have longer hospital stays, more complex care, and higher costs than other cases of delayed discharges. |
| Pellico-López, Herrero-Montes, (2022) [19] | Descriptive, observational, cross-sectional, and retrospective study | Describing the characteristics of patients deceased during delayed stays in terms of duration of hospital stay, patient’s characteristics, and care context | 198 patients deceased during their hospital stay after being discharged from the HUMV (2007-2015) | 6.57% of patients with delayed discharges for non-clinical reasons died during their hospital stay. The most common diagnosis among the deceased was simple pneumonia, likely caused by factors such as old age, comorbidity, fragility, or complications arising from hospital infections. |
| Pellico-López, Fernández-Feito, Cantarero et al., (2021)[16] | Descriptive, observational, cross-sectional, and retrospective study | Quantifying the connexion between stay and its costs in hip processes with delayed discharge for non-clinical reasons | 306 patients admitted to the HUMV (2007-2015) for hip processes with delayed discharges for non-clinical reasons | Average delayed stay was 7.12 days. The cost of delayed stay amounted to €641,002.09. Up to 85.29% of patients lived in urban areas near the hospital and 3.33% had been transferred to a long-stay centre for recovery. The percentage of patients with hip procedures and delayed discharge was lower to prior reports; however, their duration of stay was longer. |
| Pellico -López, Fernández-Feito et al., (2021)[17] | Descriptive, observational, cross-sectional, and retrospective study | Understanding which characteristics are common in pneumonia patients, compared to other cases of delayed discharge. | 170 patients diagnosed with pneumonia who were discharged late in the HUMV (2007-2015) | Pneumonia patients were older, less complex, and had higher death rates than the rest of the patients. |
| Pellico -López et al., (2019) [11] | Descriptive, observational, cross-sectional, and retrospective study | Quantifying the number of delayed discharge cases and inappropriate hospitalisation days and identifying the use of health services linked to bed-blocking | 3015 patients with delayed discharges in the HUMV (2007-2015) | The characteristics most frequently associated with longer stays were the following: increased complexity, diagnosis implying lack of functional capacity, surgical treatment, having to wait for a destination when discharged or getting back home. Multiple-component interventions linked to discharge planning may favour inefficiency reduction minimising unnecessary stays. |
| Pellico-López et al., (2018) [20] | Descriptive, retrospective study | Identifying which characteristics may influence the issue and quantifying inappropriate hospitalisation days. | This study included three public hospitals of a northern Spanish region (Cantabria), during 2010–2014. | In the period from 2010 to 2014, 1415 bed-blocking cases were found in Cantabria hospitals waiting to be admitted to long-stay hospitals. |
| Rojas-García et al., (2018) [2] | Systematic review | Systematically reviewing delayed discharge experiences from the perspective of patients, health professionals and hospitals, and their impact on patients’ outcomes and costs. | 37 papers were included of which 2 were developed in Spain | Most of the research was conducted poorly which asks for precaution when considering its practical implications. The results suggest that the adverse effects of delayed discharges are both direct, due to the potential health problems they may cause to patients, and indirect owing to increased pressure on healthcare workers. |
| Soria-Aledo et al., (2012) [23] | Descriptive, pre- and post-intervention, retrospective study | Reducing inappropriate admission and stays, as well as analysing the hospital costs saved by inadequate stay reduction. | 1350 stays at J. M. Morales Meseguer Hospital | Inappropriate stays considerably decreased from 24.6% to 10.4%. Inadequacy cost in the study sample dropped from 147,044 euros to 66,642 euros. |
| Mendoza Giraldo et al., (2012) [10] | Unicentric, observational, open, and prospective study | Analysing discharge delays for non-medical reasons at the IM Unit of a third level hospital and establishing the clinical and socio-familial factors linked to this situation. | 164 patients admitted to the IM unit of the Virgen del Rocío University Hospital (HUVR, by its Spanish acronym) whose discharges were delayed for non-medical reasons (between 1 February 2008 and 31 January 2009). | 3.5% of discharges were delayed for non-medical reasons. Patients whose discharges were delayed were older and presented higher prevalence of acute cerebrovascular disease and problems related to alcohol or benzodiazepine consumption.The main reasons given for not being discharged were family overload and/or inability to provide care, and lack of family or social support network. |
| Soria-Aledo et al., (2009) [21] | Retrospective, descriptive study | Analysing variables linked to inappropriate admissions and hospital stays, and their economic repercussions. | A total of 725 medical records and 1355 stays at J. M. Morales Meseguer Hospital were selected. | The study found 7.4% of admissions and 24.6% of stays to be inappropriate. Most common causes of inappropriate stays were diagnosis or therapeutical procedures that can be performed on an outpatient basis, waiting for test results or consultations, physician conservative attitude, bank holidays, and lack of a diagnostic or treatment plan |
| Monteis-Catot et al., (2007)[24] | Pre- and post-intervention study using«adeQhos®» questionnaire | Evaluating the impact of an intervention on the percentage of inappropriate stays (IS) to verify the hypothesis that a simple information and participation intervention (adeQhos®) allows to reduce IS percentage. | Design consisting of 2 intervention groups and their corresponding control groups in acute hospitals in Catalonia (708 patients per group) | No significant reduction of hospital inadequacy was observed after a low intensity intervention. |
| Rodríguez-Vera, (2003) [15] | Observational, descriptive study | Determining admissions and stays inadequacy at an IM unit using AEP (Appropriateness Evaluation Protocol) concurrent version. | 59 patients admitted to Juan Ramón Jiménez Hospital | 33% of stays was found to be inadequate. Waiting for complementary test results and interconsultations was the most common reason for inadequate stay. |
| Zambrana-García et al., (2001) [22] | Observational, descriptive, and prospective study | Knowing the factors that may influence inadequate stays in an IM unit. | 1,046 of the 13,384 stays generated during 1998 in the IM unit of the Poniente Hospital. | A total of 176 stays were considered inadequate (16.8%). A logistic regression analysis revealed the main factors of stay inadequacy to be days of stay, day of the week, and diagnosis on admission. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



