
Submitted:
21 October 2023
Posted:
24 October 2023
You are already at the latest version
Abstract
Foot lesions are among the most frequent causes of morbidity and disability in the diabetic population. Thus, exploration of means of preventive control are vital for detecting early signs and symptoms of this disease, Infrared thermography has been proven effective in the control of diabetic foot is among the complementary diagnostic tools available for this disease. The last review on this topic was published in 2015 and so, here we conducted a bibliographic review of the main databases (PubMed, the Web of Science, Cochrane library, and Scopus) during the third quarter of 2023. We aimed to identify the effectiveness of infrared thermography as a diagnostic element in pre-ulcerous states in diabetic patients and to detect diabetic foot ulcer complications. We obtained a total of 200 articles, 22 of which were included in this present review; 17 articles had been published after 2017. After analysing the use of infrared Thermography in diabetic patients both with and without ulcers, as well as in healthy individuals, we concluded that is an effective tool for detecting early-stage ulcers in diabetic foot patients.
Keywords:
temperature
; skin temperature
; wounds
; risk foot
1. Introduction
Foot lesions are among the most frequent causes of morbidity and disability in the population with diabetes and are the most common reason for hospital admission and decreased patient quality of life. Indeed, there is a 40–70% probability of patients with this disease requiring a lower limb amputation [1]. Exploration and preventive control of this pathology are vital to detect early signs and symptoms that, in the long term, can promote the appearance of ulcers. This exploration must be performed at least once in the absence of risk factors and once every six months if there is any risk of ulcers [2]. Therefore, it is especially important to follow a protocol for these patients, in which the anamnesis and clinical history play a substantial role. Different complementary telemedical methods are available to aid the diagnosis of diabetic foot, of which infrared thermography is one of the most important [3]. This technique was first used for military applications at the beginning of the 20th century. However, infrared thermography soon transferred to biomedical fields and started being used for the non-invasive diagnosis of vascular disease, fever, breast cancer, and in the analysis of inflammatory arthritis, osteoarthritis, and other pathologies [4].
Infrared thermography is a safe, repeatable, contactless, and non-invasive procedure that measures and maps the temperature distribution radiating from body surfaces [5]. An infrared camera identifies and monitors the amount of radiation emitted and translates this value into a temperature. These projections allow identification of the heat radiating away from the body [3,6] and produce images with specific physiological thermal patterns that can be collected according to specific standards, thereby allowing the quality of this technique to increase in the future [6].
2. Materials and Methods
Following the preferred reporting items for systematic review and meta-analysis descripts (PRISMA) guidelines, we conducted a systematic review of the academic literature on infrared thermography as a tool for diagnosing diabetic foot. We followed the population, intervention, control, and outcomes (PICO) format (Table 1) to formulate the basis of this research.
We consulted the Descriptors in Health Science (DeCS) and Medical Subject Headings (MeSH) terms to devise the following PubMed search strategy: ((((“Diabetic Foot”[Title/Abstract]) OR (diabetic foot[MeSH Terms])) OR ((“Diabetic Neuropathies”[Title/Abstract]) OR (diabetic neuropathies[MeSH Terms])))) AND (((“thermal imaging”[Title/Abstract]) OR (differential thermal analysis[MeSH Terms])) OR (analyses, differential thermal[MeSH Terms])). The results were subsequently summarised in databases, as shown in Table 2.
We searched the main health sciences databases including PubMed, the Web of Science (WoS), Scopus, and the Cochrane library during the third quarter of 2023. The inclusion criteria were articles about infrared thermography conducted in humans with and without diabetes and ulcers, published from 2013 to 2023 in English or Spanish. Some publications such as editor’s letters, reviews, systematic reviews, meta-analyses, and conference reports were excluded. Of note, no Cochrane reviews were included because none met the inclusion criteria. Once the screened publications were obtained, we read the publications and reviewed their quality by employing the PEDro scale [7].
3. Results
Our search strategy obtained a total of 200 publications (28 in PubMed, 56 in the WoS, 16in the Cochrane library, and 100 in Scopus). After applying the inclusion criteria, 22 valid citations were reviewed, as reflected in the PRISMA flowchart (Figure 1).
All the articles included were quantitative and were assessed according to the PEDRo scale which assigned a score of 0 if the criterion is absent and 1 if it is present in the article [8]. The first criterion on this scale was not recorded because it considered the external validity of the articles [9].
| Inclusion and source | Random assign | Hidden assign | Baseline comparability | Blinded subjects | Blinded therapists | Blinded raters | Results above 85% | Analysis by “intention to treat” | Statiscal comparisons between groups | Measurement and variability data | SCORE | |
| Machin G et al. (2019) | ✓ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 5 |
| Petrova NL el al. (2018) | ✓ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 5 |
| Mory T et al. (2013) | ✓ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 4 |
| Petrova NL et al. (2020) | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 8 |
| Van Netten JJ et al. (2013) | ✓ | ✕ | ✓ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 6 |
| Van Dorelamen RFM et al. (2019) | ✓ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 5 |
| Aliahmad B et al. (2019) | ✓ | ✓ | ✕ | ✓ | ✕ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | 7 |
| Kanazawa T et al. (2016) | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | 9 |
| McDonald A et al. (2019) | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 8 |
| Gatt A et al. (2018) | ✓ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 4 |
| Astasio-Picado A et al. (2018) | ✓ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 5 |
| Liu C et al. (2015) | ✓ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 4 |
| Zhou Q et al. (2021) | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 8 |
| Ashok BH et al. (2020) | ✓ | ✕ | ✕ | ✓ | ✓ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 6 |
| Rai M et al. (2022) | ✓ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 4 |
| Arteaga-Marrero N et al. (2021) | ✓ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | 3 |
| Hernandez-Contreras DA et al. (2019) | ✓ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | 3 |
| Carabott M et al. (2021) | ✓ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | 3 |
| Van Dorelamen RFM et al. (2020) | ✓ | ✕ | ✓ | ✕ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | 5 |
| Ilo et al. (2019) | ✓ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 5 |
| Astasio-picado A (2019) | ✓ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | 4 |
| McDonald A et al. (2017) | ✓ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | 5 |
4. Discussion
To assess if infrared thermography was a useful tool for diagnosing pre-ulcerous states and detecting the complications of ulcers in diabetic patients, we performed an exhaustive review of the relevant available literature. We found elements that made this comparison difficult such as the differences in the samples used in each study, including the infrared camera used and protocol followed to capture the images.
Our search highlighted articles that had analysed and compared foot temperature using infrared thermography in healthy [10,11,12,13] and diabetic patients [14,15,16,20,21,22,23,24,25], although other studies had directly analyzed both types of patients with other methods [5,14,24,25,26,27,28,29]. This type of comparison had confirmed the difference between the temperature of both groups, registering lower temperatures in the healthy group as compared with the diabetic one [3,5,23,24,25,26]. However, it is important to consider that this technique has the drawback of its high variability. Indeed, studies such as those by Machin et al. [10] and Ray et al. [25] observed an increase in plantar temperature in healthy patients that could be indicative of the presence of inflammation.
The previous publication benchmark values in healthy people [10,11,12,13] allowed us to define standardized results that could be used to refine the methodology to achieve satisfactory results when taking samples.
Studies in diabetic patients have highlighted the fact that thermography can be used to control temperature (which is approximately 2 °C higher in infected wounds) to help patients to avoid pressure zones, thereby favoring the prevention of lesions and their complications [15]. However, as Petrova et al. [14] explained, no temperature differences were observed between patients assessed with or without thermography. Therefore, there is insufficient evidence to support the use of thermography to prevent complications because the values it detects do not always significantly differ from normality.
Although studies with larger sample sizes are still required, databases such as the one published by Hernández-Contreras et al. [27] which contain both healthy and diabetic patient thermograms could be created. This database contains 167 patients and so could serve as a useful baseline for the comparison of results with those of future studies. Although different types of voluntary subjects were included in the different studies considered in this review, these results could be addressed together because they all suggest that thermography is a suitable tool to detect foot temperature changes. If they are sufficiently early detected, this technology may help to prevent the appearance of pre-ulcerous complications and could favour ulcer healing and to avoid infections through early treatment [14,24].
Even though one of the exclusion criteria for this current work was not being exposed to other pathologies that could result in temperature changes, it was very difficult to isolate diabetic foot from other pathologies such as peripheral vascular disease because many of these coexist [24,27,28]. Indeed, some authors observed that temperatures in the fifth metatarsal and hallux were lower in patients with associated pathologies [5,21].
Furthermore, Mori et al. [13] suggest that temperature distribution patterns must be identified by collecting and classifying these images according to maps of heat distribution so that they can be compared without relying on the angiosome divisions proposed by other authors [5,13]. An other authors suggest that patients with diabetic foot present a significantly higher temperature in the fifth metatarsal area and hallux compared to healthy individuals [20,22,26]. These variations represent different pattern distributions of temperature. For example, diabetic patients have notably higher temperature asymmetry and hot spots on the sole of the foot that indicate a heat increase [10,25]. Regardless, the lack of consensus in the use of angiosomes and for temperature distribution patterns makes it difficult to generalise the results published up to date.
Moreover, it is important to highlight the differences in thermographic images from studies comparing the affected and contralateral limbs in diseased or healthy patients. According to Van Netten et al. [15] there was no difference between the limbs of the same patient, while Macdonald et al. [19] or Mori et al. [13] suggested that intra-patient variability is comparable with that of other patients, with a difference of up to 2 °C between both feet. Nonetheless, infrared thermography is the most common method used to compare contralateral limbs in these patients [12,14,15,19,22]. The work by Gatt et al. [20] indicated that there were differences between patients with or without lesions. This increased temperature may be altered in pre-ulcerous states, although once the wound is present it is difficult to predict the development of complications using thermography alone, because no difference between ulcered and healthy toes of the same foot can be detected.
Of note, a wide range of different infrared cameras are used for these types of study. In average it can be assumed that standard spatial resolution of 320 × 240 pixels [14,20,21,22,25] conferees a thermal resolution up to 0.1 °C [15,19,20,24] to with a temperature range of 0–100 °C [18]. Although the use of standard infrared cameras is quite common, some studies have proposed using infrared smartphone cameras [18,29] to make this technique even more accessible. Indeed, some studies have even proposed merging 3D and thermography images to obtain more realistic results [16].
However, phone cameras have a lower (160 × 120 pixels) resolution [16,29] and these devices cannot obtain specific data like absolute temperature. Despite this limitation, Kanazawa et al. [18] suggest that images are obtained much faster and are sufficient for data comparison. In fact, Van Doremalen et al. [29] stated that cameras connected to smartphones showed excellent validity for studying diabetic foot and therefore, such studies with smartphone cameras should be increased. Of note, although working at room temperature, some studies use a black background to dampen the influence of light [3,22,24,25,29] because environmental variations can alter the results, as shown by Ashok et al. [24].
As it has been observed during the development of this current study, there are some limitations to compare the use of infrared thermography in patients with diabetic foot. First, very few studies have individually tackled this technique comparing it with other techniques or in other pathologies associated with diabetic foot. Second, a wide range of cameras can be used to record sample images, leading to the misconception that accuracy is unreliable, but actually images are not necessarily comparable depending on many factors, especially its spatial resolution. Furthermore, the decision to use a black background in the images can significantly alter the results and no algorithms have yet been developed that can unify all these criteria.
In addition, it is to be highlighted that working with healthy or diabetic individuals with or without an ulcer or underlying pathologies can result in very disparate sample images. Thus, it has been proposed by other authors, the generation of a large thermographic image database could help to create thermographic standards and to make comparison of results to be more feasible. Consensuated criteria that can help to unify results must be developed so that this technique can be used to help prevent complications or promote ulcer healing in diabetic patients.
5. Conclusions
Infrared thermography represents a potentially effective tool for detecting pre-ulcerous states in diabetic foot patients. However, further research is still required to investigate its applications for preventing diabetic foot ulcer complications. It is very important to highlight these thermographic studies must consider the sample type (healthy or diabetic patients, with or without an ulcer), protocol used to obtain the images (e.g., with or without a black background), and results analysis (software used). It is essential to continue research into infrared thermography because it is a cheap, non-invasive, and painless technique that can provide useful data for the development of new methods to further prevent and palliate diabetic foot complications.
Author Contributions
Marina Faus Camarena participed in the conception and design of the study, do the literature research, was involved in the analysis and interpretation of the results and drafted the article. Ivan Julián-Rochina and Marta Izquierdo-Renau participated in the conception and the design of the study, were involved in the analysis and interpretation of the results and reviewed the article critically for important intellectual content. Manuel Miralles and Manel Arrébola reviewed the article critically for important intellectual content and gave final approval of the version to be published.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Enciso Rojas ÁD. Risk factors associated with diabetic foot. Rev Virtual la Soc Paraguaya Med Interna 2016, 3(2):58–70. [CrossRef]
- Rincón, Y.; Gil, V.; Pacheco, J.; Benítez, I.; Sánchez, M. Evaluación y tratamiento del pie diabético. Rev Venez Endocrinol y Metab 2012, 10, 176–87. [Google Scholar]
- Liu C, van Netten JJ, van Baal JG, Bus SA, van der Heijden F. Automatic detection of diabetic foot complications with infrared thermography by asymmetric analysis. J Biomed Opt 2015, Feb 11;20(2):026003. [CrossRef]
- Ramírez-Arbeláez, L.M.; Jiménez-Díaz, K.T.; Correa-Castañeda, A.C.; Giraldo-Restrepo, J.A.; Fandiño-Toro, H.A. Protocolo de adquisición de imágenes diagnósticas por termografía infrarroja. Med y Lab 2015, 21, 161–78. [Google Scholar] [CrossRef]
- Ilo A, Romsi P, Mäkelä J. Infrared Thermography and Vascular Disorders in Diabetic Feet. J Diabetes Sci Technol 2019, 14(1):28–36. [CrossRef]
- Hidalgo Salvador, E.; Álvarez González, F.; Salvador Luna, A. Application of Infrared thermography in legal medicine. Is it a valid test for an objective assessm. Cuad Med Forense 2014, 20, 77–84. [Google Scholar] [CrossRef]
- Franciele C da S, Beatriz Angélica VA, Rodrigo da RI, Paulo Jose BGF, Rudney da S. Escalas y listas de evaluación de la calidad de estudios científicos. Rev Cuba Inf en Ciencias la Salud [Internet] 2013, 295–312. Available from: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S2307-21132013000300007&lang=pt. /.
- Albanese E, Bütikofer L, Armijo-Olivo S, Ha C, Egger M. Construct validity of the Physiotherapy Evidence Database (PEDro) quality scale for randomized trials: Item response theory and factor analyses. Res Synth Methods 2020, 11(2):227–36. [CrossRef]
- Escala PEDro - PEDro [Internet]. Available from: https://pedro.org.au/spanish/resources/pedro-scale/.
- Machin, G., Whittam, A., Ainarkar, S., Allen, J., Bevans, J., Edmonds, M., Kluwe, B. M, A., Petrova, N., Plassmann, P., Ring, F., Rogers, L., Simpson R. A medical thermal imaging device for the prevention of diabetic foot ulceration. iopscience 2019, 6(12):125337. [CrossRef]
- Petrova NL, Whittam A, MacDonald A, Ainarkar S, Donaldson AN, Bevans J, et al. Reliability of a novel thermal imaging system for temperature assessment of healthy feet. J Foot Ankle Res 2018, 11. [CrossRef]
- Macdonald A, Petrova N, Ainarkar S, Allen J, Plassmann P, Whittam A, et al. Reproducibility of Thermal Images: Some Healthy Examples. In: Ng EYK, Etehadtavakol M, editors. APPLICATION OF INFRARED TO BIOMEDICAL SCIENCES. 2017. p. 265–76.
- Mori, Taketoshi., Nagase, Takashi., Takehara, K., Oe, Makoto., Ohashi, Y., Amemiya, Ayumi., Noguchi, Hiroshi., Ueki, Kohijiro., Kadowaki, Takashi., Sanada H. Morphological pattern classification system for plantar thermography of patients with diabetes. J Diabetes Sci Technol 2013, 7(5):1102–12. [CrossRef]
- Petrova NL, Donaldson NK, Tang W, MacDonald A, Allen J, Lomas C, et al. Infrared thermography and ulcer prevention in the high-risk diabetic foot: data from a single-blind multicentre controlled clinical trial. Diabet Med 2020, 37(1):95–104. [CrossRef]
- Van Netten JJ, Van Baal JG, Liu C, Van Der Heijden F, Bus SA. Infrared thermal imaging for automated detection of diabetic foot complications. J Diabetes Sci Technol 2013, 7(5):1122–9. [CrossRef]
- Van Doremalen RFM, van Netten JJ, van Baal JG, Vollenbroek-Hutten MMR, van der Heijden F. Infrared 3D Thermography for Inflammation Detection in Diabetic Foot Disease: A Proof of Concept. J Diabetes Sci Technol 2020, 14(1):46–54. [CrossRef]
- Aliahmad B, Tint AN, Poosapadi Arjunan S, Rani P, Kumar DK, Miller J, et al. Is Thermal Imaging a Useful Predictor of the Healing Status of Diabetes-Related Foot Ulcers? A Pilot Study. J Diabetes Sci Technol 2019, 13(3):561–7. [CrossRef]
- Kanazawa, T., Nakagami, G., Goto, T., Noguchi, H., Oe, M., Miyagaki, T., Hayashi, A., Sasaki, S., & Sanada H. Use of smartphone attached mobile thermography assessing subclinical inflammation: a pilot study. J Wound Care [Internet] 2016, 25(4):177–82. [CrossRef]
- Macdonald, A., Petrova, N., Ainarker, S., Allen, John., Lomas, C., Tang, W., Plassmann, P., Ehittam, A., Bevans, J., Ring, F., Kluwe, B., Simpson, R., Rogers, L., Machin, G., & Edmonds M. Between visit variability of thermal imaging of feet in people attending podiatric clinics with diabetic neuropathy at high risk of developing foot ulcers. Physiol Meas 2019, 40(8): 0–68. [CrossRef]
- Gatt A, Falzon O, Cassar K, Camilleri KP, Gauci J, Ellul C, et al. The Application of Medical Thermography to Discriminate Neuroischemic Toe Ulceration in the Diabetic Foot. Int J Low Extrem Wounds 2018, 17(2):102–5. [CrossRef]
- Astasio-Picado Á, Martínez EE, Gómez-Martín B. Comparison of Thermal Foot Maps between Diabetic Patients with Neuropathic, Vascular, Neurovascular, and No Complications. Curr Diabetes Rev 2019, 15(6):503–9. [CrossRef]
- Astasio-Picado A, Martinez EE, Nova AM, Rodriguez RS, Gomez-Martin B. Thermal map of the diabetic foot using infrared thermography. INFRARED Phys Technol 2018, 93:59–62. [CrossRef]
- Zhou Q, Qian Z, Wu J, Liu J, Ren L, Ren L. Early diagnosis of diabetic peripheral neuropathy based on infrared thermal imaging technology. Diabetes Metab Res Rev 2021, Oct 1;37(7). [CrossRef]
- Ashok BH, Karnam Anantha S, Janarthan K. Plantar temperature and vibration perception in patients with diabetes: A cross-sectional study. Biocybern Biomed Eng 2020, 40(4):1600–10. [CrossRef]
- Rai M, Maity T, Sharma R, Yadav RK. Early detection of foot ulceration in type II diabetic patient using registration method in infrared images and descriptive comparison with deep learning methods. J Supercomput [Internet] 2022, (0123456789). [CrossRef]
- Arteaga-Marrero N, Bodson LC, Hernandez A, Villa E, Ruiz-Alzola J. Morphological Foot Model for Temperature Pattern Analysis Proposed for Diabetic Foot Disorders. Appl Sci 2021, 11(16). [CrossRef]
- Hernandez-Contreras DA, Peregrina-Barreto H, Rangel-Magdaleno JD, Renero-Carrillo FJ. Plantar Thermogram Database for the Study of Diabetic Foot Complications. IEEE ACCESS 2019, 7:161296–307. [CrossRef]
- Carabott M, Formosa C, Mizzi A, Papanas N, Gatt A. Thermographic Characteristics of the Diabetic Foot with Peripheral Arterial Disease Using the Angiosome Concept. Exp Clin Endocrinol Diabetes 2021, Feb 1;129(2):93–8. [CrossRef]
- Van Doremalen RFM, van Netten JJ, van Baal JG, Vollenbroek-Hutten MMR, van der Heijden F. Validation of low-cost smartphone-based thermal camera for diabetic foot assessment. Diabetes Res Clin Pract 2019, Mar 1;149:132–9. [CrossRef]
Figure 1.
PRISMA study selection flowchart.
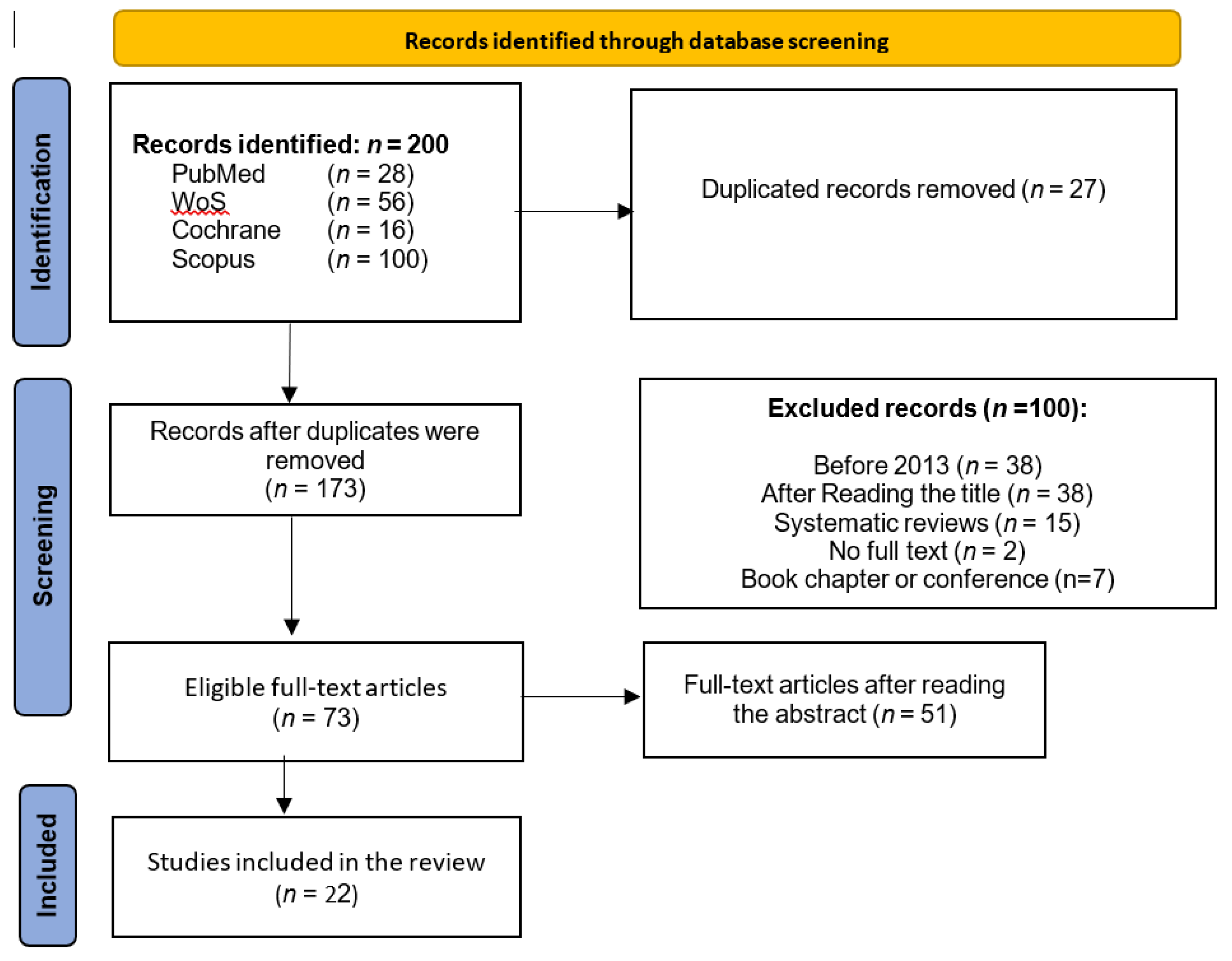

Table 1.
PICO research questions.
| P | Patient | Healthy or diabetic patients with or without ulcers. |
| I | Intervention | Diagnosis of diabetic foot complications. |
| C | Comparison | Use of thermography as a diagnostic tool for complications versus not using this technology. |
| O | Outcomes | Early detection of complications. |
Table 2.
Bibliographical database search strategy.
| Database | Search strategies | Data | Results | Selected |
|---|---|---|---|---|
| PubMed | ((((“Diabetic Foot”[Title/Abstract]) OR (diabetic foot[MeSH Terms])) OR ((“Diabetic Neuropathies”[Title/Abstract]) OR (diabetic neuropathies[MeSH Terms])))) AND (((“thermal imaging”[Title/Abstract]) OR (differential thermal analysis[MeSH Terms])) OR (analyses, differential thermal[MeSH Terms])) | Sept 2023 | 29 | 11 |
| WoS | (“Diabetic Foot” OR “Diabetic Neuropathies”) AND (“thermal imaging” OR “differential thermal analysis”) | Sept 2023 | 58 | 73 |
| Cochrane | ((diabetic foot) OR (neuropathy)) and ((thermal imaging) OR (infrared thermography) OR (temperature monitoring) or (infrared image) OR (skin temperature) OR (thermal imaging) OR (infrared sensor technology)) | Sept 2023 | 19 | 0 |
| SCOPUS | (((diabetic AND foot) OR (neuropathy)) AND ((“thermal imaging”) OR (“infrared thermography”) OR (“temperature monitoring”) OR (“infrared image”) OR (“skin temperature”) OR (“thermal imaging”) OR (“infrared sensor technology”))) | Sept 2023 | 165 | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



