
Submitted:
23 October 2023
Posted:
25 October 2023
You are already at the latest version
Abstract
Atopic dermatitis (AD), a T2 inflammatory skin condition, is widely recognized as one of the most prevalent chronic and recurrent skin disorders. One of the most effective therapy for treating moderate-to-severe AD is Dupilumab, a monoclonal antibody that blocks both IL-4 and IL-13 signaling. At the same time, no comprehensive analysis of cytokines profile was made in AD patients undergoing Dupilumab therapy. The primary objective of our research was to examine the levels of main cytokines to better understanding systemic immune response in AD and to identify potential biomarkers of the effectiveness of Dupilumab treatment. AD patients demonstrated significant clinical improvements one year after initializing of Dupilumab therapy. We identified 16 cytokines that showed major difference between Dupilumab-treated patients and patients without Dupilumab therapy. Six cytokines showed correlation with AD severity and the efficacy of Dupilumab therapy. Jointly revealed cytokines could potentially predict the effectiveness of Dupilumab treatment and help to choose the precision target therapy in AD patients as well.
Keywords:
Atopic dermatitis
; cytokines profiling
; Dupilumab
; T2 immune response
1. Introduction
Atopic dermatitis (AD) is one of the most common chronic relapsing Type 2 inflammatory skin diseases [1,2]. Epidemiological studies reveal a significant prevalence of the disease: AD affects from 17 to 24% of children and from 2 to 10% of adults worldwide [3,4,5]. AD deeply influences the life quality of patients and their families, leading to numerous adverse social and economic challenges.
AD is a heterogeneous disease, and numerous attempts have been made to define subsets of patients based on clinical and immunological features. It depends on a combination of factors including genetic characteristics (genotype), observable characteristics (clinical phenotype), and disease subtype determined by specific biomarkers (endotype).
The Type 2-response in AD is well understood, IL-4 and IL-13 considered as the key proinflammatory cytokines, but in different AD phenotypes other factors may also play a crucial role in inflammation [6].
IgE-specific sensitization is one of the main AD pathogenetic mechanisms [7,8]. Patients with AD tend to become sensitized not only to food allergens (eggs, cow’s milk, peanut, fruits, vegetables etc.) but also to environmental allergens, such as house dust mites (HDM), animal dander and pollen [9,10].
Birch pollen is one of the main allergens in Northern Europe. Sensitization to this allergen could cause various allergic diseases, including allergic rhinitis, asthma, and AD. Earlier, an AD phenotype associated with IgE sensitization to airborne allergens, including birch pollen, has been described [11,12,13].
More detailed study of the immune response in AD seems to be promising in terms of identifying immunological biomarkers in different clinical disease phenotypes, which can be considered as the targets for individual selection of the personalized immunotherapy.
Recently, targeted biological therapy has been successfully implemented across various fields of medicine. Dupilumabis a fully human monoclonal antibody that inhibits the binding of IL-4 and IL-13 to their shared receptor component, IL-4Rα, identified as key drivers of AD and other allergic diseases, serves as an instance of successful targeted therapy.
Dupilumab was the first monoclonal antibody approved for the treatment of AD in 2017, with regulatory approval granted in Europe, the USA, and other countries. Real-world studies are currently being conducted to better understand the safety and effectiveness of Dupilumab in treating of moderate-to-severe AD [14,15,16,17,18,19]. However, so far, no detailed analysis of cytokine profile in Dupilumab-treated subjects with AD has been performed. Obviously the efficacy and safety of AD targeted immunotherapy depends on the AD severity and phenotype as well. Thorough studies are required to identify reliable biomarkers that correspond to the predominant immune response mechanisms related to AD, to allow pre-selection of targeted immunotherapy.
The main aim of our study was to assess the level of key cytokines to evaluate the features of the immune response in AD patients with birch pollen sensitization with and without Dupilumab therapy in comparison with healthy subjects and to identify possible predictors of the efficacy of Dupilumab therapy.
2. Results
2.1. The Patients with Atopic Dermatitis Demonstrated Significant Clinical Improvements one Year after Initiation of Dupilumab Therapy During Birch Pollen Season
The study enrolled 29 adult participants, who were divided into three groups according to clinical data: AD natural course and severity (SCORAD, itch PP-NRS, DLQI), allergic comorbidities, sensibilization profile, treatment were enrolled in the study (Table 1, Table S1). Group 1 (Dupilumab-treated, DT) included 9 patients with moderate-to-severe AD and birch pollen allergy, who started Dupilumab treatment for 12 – 14 months before samples collection, 6 males and 3 females, average age 32.0 y.o. (IQR: 23.0 – 39.0). Group 2 (Dupilumab untreated, DUT) comprised of 10 patients with moderate-to-severe AD and birch pollen allergy who received standard therapy for AD without any biologicals, 3 males and 7 females, whose average age was 26.5 y.o. [IQR: 22.3 - 29.5]. Group 3 (Healthy subjects, HS) consisted of healthy donors, including 3 males and 3 females, with an average age of 25.5 y.o.[IQR: 24.3-28.5].
All AD patients included in the study were sensitized to the major birch pollen allergen, Bet v 1. Despite their different group designations, there were no disparities in the specific IgE levels to rBet v 1 between DT and DUT patients. A positive history of allergic rhinoconjunctivitis, as a primary clinical manifestation of birch pollen allergy, was common to all AD patients. Within DT group five out of nine patients, equating to 55.6%, were diagnosed with perennial asthma. Comparatively, within DUT group, four out of ten patients (40.0%), had perennial asthma, with one patient (10.0%), had seasonal asthma. Table 1 and Table S1 present a thorough breakdown of the clinical and demographic data of the study participants.
All patients in this study had been under the observation in the inpatient Skin Allergy Department for at least two years prior to the study initiation. Retrospectively obtained SCORAD (baseline SCORAD) indexes were measured during previous birch pollination seasons and before Dupilumab treatment commenced, from the patients' clinical documentation.
Clinical data and plasma samples had been collected during the peak of birch pollination period one year after the beginning of the study (Figure 1A).
AD patients received Dupilumab treatment demonstrated significant improvement during the birch pollen season based on the SCORAD index (Figure 1B, Table 1). On average, the SCORAD index decreased by 23.8 percent for the DT group, while the SCORAD for the DUT group remained unchanged or worsened over the year.
2.2. The Level of Bet v 1-Specific IgE was Lower in Dupilumab-Treated Patients in Comparison with Dupilumab-Untreated Group
Patients’ sera were tested with Bet v 1-specific IgE and IgG4 ELISA. Serum of DT patients showed the decrease of Bet v 1-specific IgE in comparison with DUT group (p = 0.005, Figure 1C). However, the level of Bet v 1-specific IgE in the Dupilumab-treated patients did not significantly differ from that of the Healthy subjects (p > 0.9999, Figure 1C). Conversely, the level of Bet v 1-specific IgG4 antibodies did not exhibit any difference between the DT group and DUT group (p = 0.7480, Figure S1)
2.3. The Cytokine Profile in AD Patients Without Dupilumab Treatment Significantly Differs from Those Treated with Dupilumab, as Well as from Healthy Individuals
Next we evaluated the level of 41 cytokines in serum of Dupilumab-treated and untreated patients. The concentration of cytokines in the healthy cohort ranged from 100,000 to 10 pg/ml (Figure 1D). In comparison to the HS group we found cytokines, that showed dramatically higher or lower concentrations in the DUT or DT groups. Thus, PDGF-AA, EGF, CCL22, CX3CL1, CCL4, IL-5, and IL-10 had higher level in the DUT group. In opposite, TNF-β, IL-6, CCL7, CXCL8, and CCL11 showed lower concentrations in the DT group (Figure 1D, Table S2).
2.4. The Concentrations of AD Key Cytokines were Diminished in the Group of Patients Treated with Dupilumab Compared to Those in the Group That Did Not Receive Dupilumab Treatment
The cytokines that are a part of the Type 2 immune response play crucial role in AD pathogenesis and are the primary targets of Dupilumab therapy. Indeed, IL-5 cytokine level was 2.6 times lower in the DT group compared to the DUT ( Figure 2A, Me (DT) = 3.1, Me (DUT) = 7.9, Me (HS) = 4.5; p = 0.0317 for DT vs DUT, p = 0.0381 DUT vs HS). The concentration of another Type 2 immune response IL-9 cytokine was also lower in the group of patients after Dupilumab therapy compared with the DUT group (IL-9: Me (DT) = 25.3, Me (DUT) = 41.3; p = 0.0203 for DT vs DUT). Simultaneously, no noticeable difference was observed in serum levels of IL-4 and IL-13 between HS, DT and DUT groups (Figure S3).
The role of Th17 cells in the development of atopic dermatitis is widely known. We compared serum concentrations of IL-7 and IL-17A, that take part in Th17 cell differentiation and maintenance. The level of IL-7 and IL-17A were significantly lower in Dupilumab-treated patients compared with DUT group (Figure 2B). At the same time, no discernible difference was observed between DT group and HS (IL-7: Me (DT) = 29.9, Me (DUT) = 39.9, Me (HS) = 32.1; p = 0.0050 for DT vs DUT, p = 0.0318 DUT vs HS; IL-17A: Me (DT) = 13.9, Me (DUT) = 23.3, Me (HS) = 16.2; p = 0.0017 for DT vs DUT, p = 0.0367 DUT vs HS).
Same tendency was observed for the levels of key Th1 cytokines. The highest concentrations of IL-1a, IL-1b, IL-6, IL-12 and IFN-γ cytokines were detected in DUT group in comparison to HS, still DT group showed diminished concentration of these cytokines over against the DUT group (Figure S2).
Dupilumab-untreated patients were characterized by a high concentration of some growth factors. The concentration of PDGF-AA in the DUT group was 9 times higher than in the DT group, and 15 times higher than in the HS group (Figure 2C; Me (DT) = 1492.0, Me (DUT) = 13918.0, Me (HS) = 950.2; p = 0.0408 for DT vs DUT, p = 0.0003 DUT vs HS). Additionally, the level of epidermal growth factor (EGF), which is directly involved in AD lesion progression, as well as GM-CSF level, was lower in DT group in comparison with those in DUT and HS groups (EGF: Me (DT) = 166.6, Me (DUT) = 313.8, Me (HS) = 209.8; p = 0.0132 for DT vs DUT, p = 0.0324 DUT vs HS; GM-CSF: Me (DT) = 88.1, Me (DUT) = 167.4, Me (HS) = 104.0; p = 0.0063 for DT vs DUT, p = 0.0416 DUT vs HS).
Surprisingly, Dupilumab-treated patients demonstrated a lower concentration of the level of IL-10 cytokine comparing with both DUT and HS groups (Me (DT) = 3.9, Me (DUT) = 8.0, Me (HS) = 3.9; p = 0.0286 for DT vs DUT, p = 0.0213 DUT vs HS). Lower concentration of another anti-inflammatory cytokine IL-1Ra was also noted in the DT group compared with DUT (Me (DT) = 74.2, Me (DUT) = 171.4, Me (HS) = 99.1; p = 0.0250 for DT vs DUT). This could potentially indicate a regulation in the levels of proinflammatory and anti-inflammatory cytokines at systemic level (Figure 2D).
A crucial part of researching AD involves analyzing the migration of key cells in peripheral tissues, especially skin. The level of CCL4 chemokine was 2.1 times higher in the DUT group compared to healthy subjects, whereas CCL4 concentration had no significant difference in the DT group comparing with the HS (Me (DT) = 32.2, Me (DUT) = 57.4, Me (HS) = 26.7; p = 0.0159 for DT vs DUT, p = 0.0001 DUT vs HS).
The same trend was noticed for two additional chemokines, CCL22 and CX3CL1 (Figure 2E, bottom panel). CCL22, which can mediate the local activation of keratinocytes, demonstrated a difference between the groups of HS and DUT as well as between the DT and DUT groups (CCL22: Me (DT) = 2025.0, Me (DUT) = 4357.0, Me (HS) = 1826.0; p = 0.0058 for DT vs HS). Also, the concentration of CX3CL1 was 1.8 times lower in DT group compared with DUT group (p = 0.0035, Me = 2090.0, and 1110.0, respectively) and 1.8 times higher in the DUT group in comparison with HS (p = 0.0237, Me = 1176.0 for HS).
A unique trend was demonstrated by three chemokines: CCL7, CCL11, and CXCL8. Surprisingly, the concentration of these chemokines in Dupilumab-treated patients was not only lower than in the DUT group, but even lower than in the HS group (CCL7: p = 0.0098 for DT vs DUT and p = 0.0293 for DT vs HS; CCL11: p = 0.0111 for DT vs DUT and p = 0.0466 for DT vs HS; CXCL8: p = 0.0438 for DT vs DUT and p = 0.0470 for DT vs HS).
2.5. Specific Cytokine Pattern Aid in Assessing Atopic Dermatitis Patients’ Condition
Next we proceeded with identifying a range of cytokines associated with the severity of AD. We observed a significant decrease in the levels of numerous cytokines within the Dupilumab-treated patient group, as indicated in Figures 1D and 2. Using the measured cytokine levels, we found correlations between the severity of patients' conditions and the levels of cytokines in their serum (Figure 3A). The SCORAD index exhibited an association with the cytokine levels of TNF-β, IL-15, IL-7, and IL-17A (Figure 3A). Despite the fact that the differences between DT and DUT groups for VEGF and MIP-1a were statistically insignificant, their concentrations were correlated with the SCORAD index (Figure 3A). Principal Component Analysis (PCA) was performed using cytokines, that show some differences between both DUT and DT group over against the HS group (Table S2, Figure 3B, upper panel). PCA analysis based on 28 cytokine concentrations, separated HS and DT groups from the DUT group (PC1 = 56.6%, PC2 = 9.3%). Then, we tried to decrease the number of cytokines in analysis to establish the key cytokines and reveal possible markers. Thus, 16 cytokines (Table S2), that showed difference between DUT and DT groups or had correlation with SCORAD index (IL-5, IL-7, IL-15, IL-17A, EGF, PDGF-AA, GM-CSF, VEGF, CCL11, CCL22, CCL3, CCL4, CXCL8, CX3CL1, IL1-Ra, and IL-10) were included in futher analysis. The result of PCA analysis made possible to identify Dupilumab-untreated patients (Figure 3C, bottom panel, PC1 = 62.1%, PC2 = 13.6%). For these revealed 16 cytokines, cluster analysis was performed. Cluster analysis effectively distinguished DUT patients from DT and HS groups (Figure 3C), that allowed us to indicate these group of cytokines as a potential predictors of AD remission.
3. Discussion
We have assessed the level of key cytokines to evaluate the features of the immune response in AD patients with birch pollen sensitization with and without Dupilumab treatment in our study. We selected the patients with clinical phenotype of AD based on sensibilization to birch pollen as one of the most important allergen sources in countries of the Northern hemisphere, in particular in Middle and Northern Europe and Russia and responsible for different allergic symptoms as well as manifestations of food and skin allergy [20,21,22].
We are convinced that the patients with AD demonstrated significant clinical improvements one year after initiation of Dupilumab therapy during birch pollen season which is connected with the effect of Dupilumab on Type 2 inflammation that has been confirmed in other studies [14,18,19].
Recently, meta-analysis of the Dupilumab-administering AD patients’ database has demonstrated that Dupilumab treatment can reduce new and worsening allergy events versus placebo [23].The apparent benefit of Dupilumab treatment is its ability to change the level of specific IgE and IgG4 to various allergens, including food and respiratory allergens [24,25]. In our study we have established that the level of Bet v 1-specific IgE in Dupilumab-treated patients was less than in patients in Dupilumab-untreated group, that could show Type 2 inflammation intensity decrease, but the exact mechanisms of the effect of such treatment on the IgE production remain unclear [26].
We found that the level of some pro-inflammatory cytokines is higher in AD patients with exacerbations without Dupilumab treatment compared with patients who received such therapy for a long time and healthy subjects. The revealed changes can be attributed to different pathways of immune response: Th2-, Th17- Th1-related markers, regulatory T-cell-related mediators, cellular markers of epidermal hyperplasia, chemokines and even cardiovascular mediators. We observed significantly higher levels of 28 cytokines in DUT group in comparison with HS and DT groups. Then we revealed 16 key cytokines that can potentially assess disease severity and treatment response: IL-5, IL-7, IL-15, IL-17A, EGF, PDGF-AA, GM-CSF, VEGF, CCL11, CCL22, CCL3, CCL4, CXCL8, CX3CL1, IL1-Ra, and IL-10.
Despite of numerous immune signaling pathways involved in the pathogenesis of AD which could be potentially responsible for the different disease subtypes, a dominant mechanism emerges - the activation of Type 2-mediated immune response through type 2 innate lymphoid cells (ILC) and type 2 T-helper cells producing IL-4, IL-5, and IL-13 resulting in reduction of Type 2-response cytokines in remission of AD. For instance, it has been shown that local reduction of cytokine levels in skin such as IL-4, IL-5, and IL-13 associated with improvement of the quality of life of AD patients [27]. At the same time, our results showed that the level of many important cytokines, including IL-4, IL-13 does not differ in AD patients who received and who did not receive Dupilumab compared with healthy donors. Serum cytokines levels may be variable and do not fully reflect local immune response in the skin [28]. Despite Type 2 cytokines key role in the initiating of the immune response in Type 2 diseases, many other cytokines can also be involved in chronic AD mechanisms. For instance, the level of serum IL-5 and IL-9 was significantly lower in the DT than in the DUT group.
It is well known that IL-7 is required for T cell development and survival, for instance for Th2 and Th17 cells. Besides, IL-7 plays important role in some diseases such as fungal asthma [29], where an IL-7 increase affects the production of eosinophils and inhibits their survival. Furthermore, IL-7 deficiency negatively affects the number and functionality of eosinophils [30,31]. In our study the concentration of IL-7 significantly differed between the DT and DUT groups, while the levels of IL-7 in the HS and DT groups were the same. Another cytokine that plays important role in AD development is IL-17A, that is secreted by Th17 cells. It was revealed that the combination of IL-17 and IL-22 showed a significant synergistic effect on the production of CXCL8 [32]. However, no additive or synergetic influence was demonstrated on other AD cytokines such as GM-CSF and VEGF, although IL-17 can promote their secretion. Likewise, we found lower concentration of IL-17 in the Dupilumab-treated group in comparison with Dupilumab-untreated patients.
Growth factors play important role in angiogenesis as the part of AD pathogenesis. We observed higher levels of PDGF-A, GM-CSF, EGF and FGF-2 in the group of patients without Dupilumab treatment in comparison of those who underwent the therapy. However, it's important to note that the concentration of PDGF-AB-BB was not significantly lower in DT group compared to HS and DUT group. PDGF is one of numerous growth factors that regulate cell growth and division. PDGF-A, a specific ligand for PDGFRα, promotes fibroblast and keratinocytes proliferation during wound healing of the skin [33]. Recently it was shown that the PDGFRα pathway, which is known for transducing proliferation signals in the primary cilium, promoted dendritic cells proliferation in a intraflagellar transport (IFT) system-dependent manner [34].
Another important cytokine, that plays crucial role in growth of new blood vessels from preexisting vessels, VEGF is associated with inflammation in various chronic inflammatory skin diseases. It was demonstrated that VEGF, angiopoietins, TNF-β, CXCL8, and IL-17 can induce angiogenesis in psoriasis [35].The finding that VEGF is expressed in inflammatory skin lesions indicates that angiogenesis progression is the important part of AD pathogenesis and its inhibition could be perspective strategy for a targeted AD treatment. Moreover we found a strong correlation between SCORAD index in Dupilumab-treated and Dupilumab-untreated patients and the serum concentrations of VEGF, TNF-β, IL-17A and IL-15.
One of the positive predictors of Dupilumab treatment effectiveness is an increase in the amount of anti-inflammatory cytokines in the skin [36], however, we observed the opposite systemic effect. In the group of AD without Dupilumab therapy, the highest levels of cytokines IL-10 and IL-1Ra were observed, which is also confirmed by other studies [37]. However, considering positive reverse regulation, similar levels of IL-10 in DT and healthy subjects groups can be regarded as a positive therapeutic effect of Dupilumab treatment. This could potentially indicate a balance in the pro- and anti-inflammatory blood cytokines level.
It is not easy to understand relationship between cytokines and the cells secreted them as well as the cells that they act upon. In the recently published study AD patients who underwent short-term or long-term treatment with Dupilumab were investigated. Using multi-omics profiling with single-cell RNA sequencing and multiplex proteomics, researchers found significant decreases in overall skin immune cell counts and normalization of transcriptomic dysregulation in keratinocytes consistent with clearance of disease. Disease-linked immune cell populations in resolved AD indicative of a persisting disease memory, facilitating a rapid response system of epidermal-dermal cross-talk between keratinocytes, dendritic cells, and T cells were identified [37]. This observation may help to explain the disease recurrence upon termination of immunosuppressive treatments in AD, and it identifies potential disease memory-linked cell types that may be targeted to achieve a more sustained therapeutic response [38]. In the study we evaluated concentrations of the key chemoattractants that are connected with cell migration.
CCL4 is known as macrophage inflammatory protein (MIP-1B) and it is produced during inflammation, damage or other important processes. as an angiogenesis, to attract immune cells as leukocytes to transgress the vascular endothelium and to migrate into peripheral tissues, such as skin. According to the results, the CCL4 (MIP-1b) level was 2 times more higher in the Dupilumab-untreated group in comparison to healthy controls and Dupilumab-treated patients. Furthermore, lower concentrations of CCL7 were observed in the DT than in the DUT. Additionally, the level of the chemokine CCL11, which is involved in the recruitment and chemotaxis of eosinophils, was also lower in patients receiving Dupilumab treatment. Dysregulation of CCL7 is associated with cardiovascular disease, diabetes mellitus, and kidney disease [39,40]. Elderly patients with AD (>60 years old) exhibited striking upregulation of key proinflammatory proteins, including CCL4, CCL7, SORT1 [41,42]. At the same time, the role of CCL7 in the development of psoriasis is well known. Under the influence of Th1 pro-inflammatory cytokines, keratinocytes produce CCL7, which affects dendritic cells, as well as Th1 and Th17 lymphocytes, thereby regulating the production of Th17 and Th1 cytokines [39]. Two cytokines CCL22 and TGF- which mediate the local activation of keratinocytes [43,44], demonstrated a difference between the groups of healthy subjects and patients without Dupilumab treatment.
Recent works show that there is an increased expression of fractalkine/CX3CL1 and its unique receptor CX3CR1 in allergic diseases. In allergic asthma, CX3CR1 expression regulates Th2 and Th1 cell survival in the inflamed lung tissues, while in atopic dermatitis it regulates Th2 and Th1 cell retention into the inflammation site [45,46]. Increased levels of CX3CL1 and its unique receptor CX3CR1 have been observed in AD patients, but not in psoriasis patients. CX3CL1 and CX3CR1 regulate the pathology by controlling effector CD4+ T cell survival within inflamed tissues, adoptive transfer experiments established CX3CR1 as a key regulator of CD4+ T cell retention in inflamed skin, indicating a new function for this chemokine receptor [47]. According to our data, the concentration of CX3CL1 in Dupilumab-treated group was approximately 2 times lower than in Dupilumab-untreated group. It was previously shown that CX3CL1 concentration correlates with clinical severity in pediatric AD cohort [48].
The role of memory dendritic cells and memory T cells in the development of AD explains cases of AD relapse upon discontinuation of the Dupilumab therapy or its inefficacy. Consequently, it is essential to identify a group of cytokines that serve as exacerbation predictors for the selection of a precisional therapy. Unfortunately, it is not always possible to detect changes in the levels of target cytokines IL-4 and IL-13, as well as general IgE, in a patient's serum. Our systemic-level study identified 10 cytokines and chemokines that could not only predict the effectiveness of Dupilumab treatment but might become a promising target for AD therapy.
Our study has some limitations. One of the limitations of the study is the absence of cytokine levels prior to the initiation of Dupilumab treatment. Therefore, the study design included comparison groups of patients without Dupilumab treatment and healthy volunteers. Obtained data let us to narrow down the spectrum of cytokines for a long-term investigation on a large sample of patients.
4. Materials and Methods
4.1. Patients
The cross-sectional case control study was performed in 2022 at the National Research Center Institute of Immunology of The Federal Medical Biological Agency of Russia (in Moscow, Russia).
For this pilot study we enrolled adult patients with moderate-to-severe atopic dermatitis and birch pollen sensitization which have been being observed for several years at inpatient Skin allergy and immunopathology department and were experiencing exacerbation od AD during the birch pollination season for at least three years. Twelve to thirteen months before this study part of these patients began receiving Dupilumab treatment (initial dose of 600 mg once, then 300 mg once every 2 weeks subcutaneously, a total of 28 to 30 injections).
The subjects were recruited from March, 2022 until May, when the birch pollen concentration in the air decreased but was still present at significant levels according to the pollen monitoring, so the contact with the causing allergen was prolonged enough to elicit an immune response in sensitized individuals. Healthy subjects were recruited at the same time from the outpatient department. Over this period prescreenings were performed, including checking all inclusion and exclusion criteria (provided in supplementary), except for interventional investigations, such as blood sampling. Successfully prescreened patients were directly divided into 3 study groups and provided with the screening dates. Screening visits were performed at 5 appointments within the first week of May, with 5 patients each time. This was done for the organizational reasons to obtain the blood from the Dupilumab-treated patients just before the subsequent injection without any intervention into treatment schedule.
During the screening visit, the patients were clinically examined and the severity was determined using the Scoring Atopic Dermatitis (SCORAD) scale. In addition, skin itch was recorded using numerous rating scale, and patients completed a Dermatological Life Quality questionnaire.
The subjects were allowed to use a stable topical therapy of mild-to-moderate glucocorticoids or calcineurin inhibitors throughout the study ant to use antihistamines since no significant impact on the eczema was expected. Also the patients were allowed to use medications for allergic rhinoconjunctivitis and asthma treatment, except systemic corticosteroids.
The study had been approved by the Ethics Committee of the NRC Institute of Immunology FMBA of Russia (Ethics number: #3, 16 February 2018). Written informed consent had been obtained from each participant.
Questionnaires
SCORAD
The SCORAD index established by the European Task Force on Atopic Clinical, Cosmetic and Investigational Dermatology was used to determine AD severity. This index includes assessment of both objective parameters (extent and intensity) and subjective parameters (pruritus and sleeplessness). The SCORAD is calculated using a formula reflecting the individual parameters with their specific weight. The SCORAD was calculated for each patient.
Dermatological Life Quality questionnaire
The Dermatological Life Quality Index (DLQI) includes ten questions reflecting the patient’s quality of life. The answers were summarized into a final score (scale of 0–30 scores): 0–1, not impaired; 2–5, slightly impaired; 6–10, moderately impaired; 11–20, strongly impaired; and 21–30, extremely impaired.
Itch numerous rating scale
The subjects rated their skin itch on a numerous rating scale. The numerous rating scale is a marked from 0 to 10 line. The left end of the line was labeled ‘‘no itch,’’ and the right end was labeled ‘‘worst itch imaginable.’’ During the assessment the subjects had to circle the number that reflected in the best way their feeling of itch over the past 24 hours, in relation to the descriptions at either end of the line.
4.2. Blood Sample Collection and Cytokine Analysis
Whole-blood samples were collected into S-Monovette® Lithium heparin tubes (Sarstedt, Cat. No. 02.1065.001) in May after the peak of birch pollen concentration in the air (Figure 1). Plasma samples were stored at -80°C. Prior the cytokine analysis plasma samples were diluted 10 times with sample buffer. A multiplex analysis was conducted using the Luminex kit (MILLIPLEX MAP Human Cytokine/Chemokine Magnetic Bead Panel - Premixed 41 Plex, "Millipore", USA) which included cytokines: PDGF-AB-BB, MCP-1, Eotoxin, CCL5, IL-1Ra, IL-1β, INF-gamma, IL-10, IL-3, G-CSF, TGF-α, EGF, IL-4, TNF-β, IL-5, IL-13, IL-6, IL-1a, MCP-3, IL-9, VEGF, INF-α2, IL-12(p70), IL-15, IL-7, IL-2, CCL11, Il-12(p40), GM-CSF, IL-17A, FGF-2, Fit-3L, CCL3, TNF-α, CXCL8, CCL4, CXCL10, PDGF-AA, CCL22, sCD40, CXCL1. According to the manufacturer's instructions (Millipore, USA), antibody-coupled beads were incubated with diluted sera samples for one hour. Subsequently, the beads were washed and incubated with biotinylated secondary antibodies. The reaction was developed by staining the beads with streptavidin-conjugated phycoerythrin. All incubations were carried out at room temperature on a shaker according to the kit manufacturer's instructions. Measurements were performed using the MagPix equipment (Luminex, USA). After each sample analysis, the bead array was calibrated and regularly checked according to the kit manufacturer's instructions. Sample concentrations were determined by comparing the mean fluorescence intensity with a standard curve obtained from standards with known concentrations provided by the manufacturer. The results of the multiplex analysis are presented as a concentrations (pg/mL).
4.3. ELISA
The level of Bet v 1-specific antibodies was measured using ELISA Quantitation Kit (Xema Co., Cat. No. K153G). Plasma samples were 10-fold diluted in blocking buffer. Plates were incubated with samples for 4 hours at room temperature. After washing, the plates were additionally incubated for 1 hour with anti-human IgG4 or IgE secondary antibody conjugates with horseradish peroxidase (Invitrogen, Cat. No. SA5-10261 and A-10663) diluted 1:3,000 in blocking buffer. ELISA plates were washed 7 times and developed for 10 min with 100 mL of TMB solution. The reaction was stopped by adding 50 ml 1 M H2SO4 and optical density at 450 nm was measured by using the iMark microplate absorbance reader (Bio-Rad, Cat. No. 1681130). All plasma samples were measured in triplicate. To determine the levels of IgG4 and IgE, we used high-titer serum as a standard and antibody levels were expressed as relative units (RU).
4.4. Statistical Analysis
Statistical analysis was performed using Graph Pad Prism (version 10.0.1 GraphPad Software, La Jolla California). The Kruskal–Wallis H test was used for comparison between multiple groups. Significant differences between two groups was determined by Wilcoxon test or Mann-Whitney test. The correlation between two groups was determined by Spearman rank test. P < 0.05 was considered statistically significant. CorreThe principal component analysis and Heatmap generation was performed with Clustvis using normalized data.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table S1: Clinical and demographical characteristic of AD patients. Table S2: Analysis of the quantity of cytokines in groups. The values provided in the table are ratios of the DUT or DT cytokine level median to HS median. Increased values are colored in red, decreased values are colored in blue. Figure S1: Serum Bet v 1-specific IgG4 levels for the DT, DUT and HS groups, measured by ELISA. IgG4 level is shown as a relative units (RU) against a standard serum. Figure S2. Evaluation of the levels of multiple cytokines with difference between DT, DUT and HS groups. Figure S3. Evaluation of the levels of multiple cytokines that do not contribute in differentiating the DT, DUT and HS groups.
Author Contributions
Conceptualization, O.E., E.F. and A.F.; methodology, M.B., A.L, M.S. and A.M.; validation, A.L. and E.S.; formal analysis, M.B. and A.L; investigation, M.B., A.L. E.S and D.C.; resources, M.K..; data curation, M.B. and A.L.; writing—original draft preparation, O.E., M.B. and A.L.; writing—review and editing, E.F., D.K, N.I., A.F. and M.K.; visualization, M.B.; supervision, O.E.; project administration, O.E.; funding acquisition, O.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Russian Science Foundation, grant number 23-15-00432
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Medical Ethical Committee of the Institute of Immunology (protocol code: #3, 16 February 2018).
Informed Consent Statement
Written informed consent was obtained from each of the study participants before performing any study procedures.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sroka-Tomaszewska, J.; Trzeciak, M. Molecular Mechanisms of Atopic Dermatitis Pathogenesis. International Journal of Molecular Sciences 2021, 22, 4130. [Google Scholar] [CrossRef]
- Ali, F.; Vyas, J.; Finlay, A. Counting the Burden: Atopic Dermatitis and Health-Related Quality of Life. Acta Dermato Venereologica 2020, 100, adv00161. [Google Scholar] [CrossRef]
- Nutten, S. Atopic Dermatitis: Global Epidemiology and Risk Factors. Annals of Nutrition and Metabolism 2015, 66, 8–16. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Stripling, S.; Fung, S.; Cha, A.; O’Brien, A.; Schachner, L.A. Recent Developments and Advances in Atopic Dermatitis: A Focus on Epidemiology, Pathophysiology, and Treatment in the Pediatric Setting. Pediatric Drugs 2022, 24, 293–305. [Google Scholar] [CrossRef]
- Sacotte, R.; Silverberg, J.I. Epidemiology of Adult Atopic Dermatitis. Clinics in Dermatology 2018, 36, 595–605. [Google Scholar] [CrossRef]
- Cabanillas, B.; Brehler, A.-C.; Novak, N. Atopic Dermatitis Phenotypes and the Need for Personalized Medicine. Current Opinion in Allergy & Clinical Immunology 2017, 17, 309–315. [Google Scholar] [CrossRef]
- Han, H.; Roan, F.; Ziegler, S.F. The Atopic March: Current Insights into Skin Barrier Dysfunction and Epithelial Cell-derived Cytokines. Immunological Reviews 2017, 278, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Elhaji, Y.; Sasseville, D.; Pratt, M.; Asai, Y.; Matheson, K.; McLean, W.H.I.; Hull, P.R. Filaggrin Gene Loss-of-function Mutations Constitute a Factor in Patients with Multiple Contact Allergies. Contact Dermatitis 2019, 80, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Campana, R.; Dzoro, S.; Mittermann, I.; Fedenko, E.; Elisyutina, O.; Khaitov, M.; Karaulov, A.; Valenta, R. Molecular Aspects of Allergens in Atopic Dermatitis. Current Opinion in Allergy & Clinical Immunology 2017, 17, 269–277. [Google Scholar] [CrossRef]
- Tamagawa-Mineoka, R.; Katoh, N. Atopic Dermatitis: Identification and Management of Complicating Factors. International Journal of Molecular Sciences 2020, 21, 2671. [Google Scholar] [CrossRef]
- Kihlström, A.; Lilja, G.; Pershagen, G.; Hedlin, G. Exposure to Birch Pollen in Infancy and Development of Atopic Disease in Childhood. Journal of Allergy and Clinical Immunology 2002, 110, 78–84. [Google Scholar] [CrossRef]
- Meinke, M.; Fölster-Holst, R.; Galecka, J.; Weißmantel, S.; Dickschat, U.; Rippke, F.; Bohnsack, K.; Werfel, T.; Wichmann, K.; Buchner, M.; et al. Birch Pollen Influence the Severity of Atopic Eczema &Ndash; Prospective Clinical Cohort Pilot Study and Ex Vivo Penetration Study. Clinical, Cosmetic and Investigational Dermatology 2015, 539. [Google Scholar] [CrossRef] [PubMed]
- Wassmann-Otto, A.; Heratizadeh, A.; Wichmann, K.; Werfel, T. Birch Pollen-related Foods Can Cause Late Eczematous Reactions in Patients with Atopic Dermatitis. Allergy 2018, 73, 2046–2054. [Google Scholar] [CrossRef] [PubMed]
- Blauvelt, A.; Bruin-Weller, M. de; Gooderham, M.; Cather, J.C.; Weisman, J.; Pariser, D.; Simpson, E.L.; Papp, K.A.; Hong, H.C.-H.; Rubel, D.; et al. Long-Term Management of Moderate-to-Severe Atopic Dermatitis with Dupilumab and Concomitant Topical Corticosteroids (LIBERTY AD CHRONOS): A 1-Year, Randomised, Double-Blinded, Placebo-Controlled, Phase 3 Trial. The Lancet 2017, 389, 2287–2303. [Google Scholar] [CrossRef] [PubMed]
- Bruin-Weller, M. de; Thaçi, D.; Smith, C.H.; Reich, K.; Cork, M.J.; Radin, A.; Zhang, Q.; Akinlade, B.; Gadkari, A.; Eckert, L.; et al. Dupilumab with Concomitant Topical Corticosteroid Treatment in Adults with Atopic Dermatitis with an Inadequate Response or Intolerance to Ciclosporin A or When This Treatment Is Medically Inadvisable: A Placebo-Controlled, Randomized Phase III Clinical t. British Journal of Dermatology 2018, 178, 1083–1101. [Google Scholar] [CrossRef]
- Simpson, E.L.; Bieber, T.; Guttman-Yassky, E.; Beck, L.A.; Blauvelt, A.; Cork, M.J.; Silverberg, J.I.; Deleuran, M.; Kataoka, Y.; Lacour, J.-P.; et al. Two Phase 3 Trials of Dupilumab versus Placebo in Atopic Dermatitis. New England Journal of Medicine 2016, 375, 2335–2348. [Google Scholar] [CrossRef] [PubMed]
- Snast, I.; Reiter, O.; Hodak, E.; Friedland, R.; Mimouni, D.; Leshem, Y.A. Are Biologics Efficacious in Atopic Dermatitis? A Systematic Review and Meta-Analysis. American Journal of Clinical Dermatology 2018, 19, 145–165. [Google Scholar] [CrossRef]
- Thaçi, D.; Simpson, E.L.; Deleuran, M.; Kataoka, Y.; Chen, Z.; Gadkari, A.; Eckert, L.; Akinlade, B.; Graham, N.M.H.; Pirozzi, G.; et al. Efficacy and Safety of Dupilumab Monotherapy in Adults with Moderate-to-Severe Atopic Dermatitis: A Pooled Analysis of Two Phase 3 Randomized Trials (LIBERTY AD SOLO 1 and LIBERTY AD SOLO 2). Journal of Dermatological Science 2019, 94, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.-P.; Tang, X.-J.; Wei, C.-Q.; Xu, L.-R.; Mao, H.; Luo, F.-M. Dupilumab Treatment in Moderate-to-Severe Atopic Dermatitis: A Systematic Review and Meta-Analysis. Journal of Dermatological Science 2018, 90, 190–198. [Google Scholar] [CrossRef]
- Elisyutina, O.; Lupinek, C.; Fedenko, E.; Litovkina, A.; Smolnikov, E.; Ilina, N.; Kudlay, D.; Shilovskiy, I.; Valenta, R.; Khaitov, M. IgE-reactivity Profiles to Allergen Molecules in Russian Children with and without Symptoms of Allergy Revealed by Micro-array Analysis. Pediatric Allergy and Immunology 2021, 32, 251–263. [Google Scholar] [CrossRef]
- Movérare, R.; Petäys, T.; Vartiainen, E.; Haahtela, T. IgE Reactivity Pattern to Timothy and Birch Pollen Allergens in Finnish and Russian Karelia. International Archives of Allergy and Immunology 2005, 136, 33–38. [Google Scholar] [CrossRef]
- Westman, M.; Lupinek, C.; Bousquet, J.; Andersson, N.; Pahr, S.; Baar, A.; Bergström, A.; Holmström, M.; Stjärne, P.; Carlsen, K.C.L.; et al. Early Childhood IgE Reactivity to Pathogenesis-Related Class 10 Proteins Predicts Allergic Rhinitis in Adolescence. Journal of Allergy and Clinical Immunology 2015, 135, 1199–1206e11. [Google Scholar] [CrossRef]
- Geba, G.P.; Li, D.; Xu, M.; Mohammadi, K.; Attre, R.; Ardeleanu, M.; Musser, B. Attenuating the Atopic March: Meta-Analysis of the Dupilumab Atopic Dermatitis Database for Incident Allergic Events. Journal of Allergy and Clinical Immunology 2023, 151, 756–766. [Google Scholar] [CrossRef]
- Ogawa-Momohara, M.; Muro, Y.; Murase, C.; Taki, T.; Tanahashi, K.; Yamashita, Y.; Koizumi, H.; Fukaura, R.; Takeichi, T.; Akiyama, M. Allergen-Specific IgG4 Increase in Atopic Dermatitis with Long-Term Dupilumab Use. British Journal of Dermatology 2023, 189, 472–474. [Google Scholar] [CrossRef]
- Spekhorst, L.S.; Rijst, L.P. van der; Graaf, M. de; Megen, M. van; Zuithoff, N.P.A.; Knulst, A.C.; Bruin-Weller, M.S. de; Le, T.-M. Dupilumab Has a Profound Effect on <scp>specific-IgE</Scp> Levels of Several Food Allergens in Atopic Dermatitis Patients. Allergy 2023, 78, 875–878. [Google Scholar] [CrossRef]
- Cabanillas, B. Dupilumab for Atopic Dermatitis—From Clinical Trials to Molecular and Cellular Mechanisms. Dermatitis® 2023, 34, 21–28. [Google Scholar] [CrossRef]
- Kim, K.; Kim, H.; Sung, G.Y. An Interleukin-4 and Interleukin-13 Induced Atopic Dermatitis Human Skin Equivalent Model by a Skin-On-A-Chip. IJMS 2022, 23, 2116. [Google Scholar] [CrossRef]
- Fedenko, E.S.; Elisyutina, O.G.; Filimonova, T.M.; Boldyreva, M.N.; Burmenskaya, O.V.; Rebrova, O.Y.; Yarilin, A.A.; Khaitov, R.M. Cytokine Gene Expression in the Skin and Peripheral Blood of Atopic Dermatitis Patients and Healthy Individuals. Self/Nonself 2011, 2, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Reeder, K.M.; Dunaway, C.W.; Blackburn, J.P.; Yu, Z.; Matalon, S.; Hastie, A.T.; Ampleford, E.J.; Meyers, D.A.; Steele, C. The Common γ-Chain Cytokine IL-7 Promotes Immunopathogenesis during Fungal Asthma. Mucosal Immunology 2018, 11, 1352–1362. [Google Scholar] [CrossRef] [PubMed]
- Von Freeden-Jeffry, U.; Davidson, N.; Wiler, R.; Fort, M.; Burdach, S.; Murray, R. IL-7 Deficiency Prevents Development of a Non-T Cell Non-B Cell-Mediated Colitis. The Journal of Immunology 1998, 161, 5673–5680. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Tang, T.-X.; Deng, H.; Yang, X.-P.; Tang, Z.-H. Interleukin-7 Biology and Its Effects on Immune Cells: Mediator of Generation, Differentiation, Survival, and Homeostasis. Front. Immunol. 2021, 12, 747324. [Google Scholar] [CrossRef]
- Koga, C.; Kabashima, K.; Shiraishi, N.; Kobayashi, M.; Tokura, Y. Possible Pathogenic Role of Th17 Cells for Atopic Dermatitis. Journal of Investigative Dermatology 2008, 128, 2625–2630. [Google Scholar] [CrossRef]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. PERSPECTIVE ARTICLE: Growth Factors and Cytokines in Wound Healing. Wound Repair and Regeneration 2008, 16, 585–601. [Google Scholar] [CrossRef]
- Toriyama, M.; Rizaldy, D.; Nakamura, M.; Atsumi, Y.; Toriyama, M.; Fujita, F.; Okada, F.; Morita, A.; Itoh, H.; Ishii, K.J. Dendritic Cell Proliferation by Primary Cilium in Atopic Dermatitis. Frontiers in Molecular Biosciences 2023, 10. [Google Scholar] [CrossRef]
- Lee, H.J.; Hong, Y.J.; Kim, M. Angiogenesis in Chronic Inflammatory Skin Disorders. International Journal of Molecular Sciences 2021, 22, 12035. [Google Scholar] [CrossRef]
- Biedermann, T.; Skabytska, Y.; Kaesler, S.; Volz, T. Regulation of T Cell Immunity in Atopic Dermatitis by Microbes: The Yin and Yang of Cutaneous Inflammation. Front. Immunol. 2015, 6. [Google Scholar] [CrossRef]
- Zhang, L.; Wen, X.; Hou, Y.; Yang, Y.; Song, W.; Zeng, Y.; Sun, J. Integrated Metabolomics and Lipidomics Study of Patients with Atopic Dermatitis in Response to Dupilumab. Front. Immunol. 2022, 13, 1002536. [Google Scholar] [CrossRef] [PubMed]
- Bangert, C.; Rindler, K.; Krausgruber, T.; Alkon, N.; Thaler, F.M.; Kurz, H.; Ayub, T.; Demirtas, D.; Fortelny, N.; Vorstandlechner, V.; et al. Persistence of Mature Dendritic Cells, T H 2A, and Tc2 Cells Characterize Clinically Resolved Atopic Dermatitis under IL-4Rα Blockade. Science Immunology 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Bachelez, H. Chemokine Ligand 7 ( CCL 7) and Innate Immune Cells in Psoriasis: Beyond Redundancy. Experimental Dermatology 2016, 25, 265–266. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.-T.; Chen, C.; Chen, J.-W. CCL7 as a Novel Inflammatory Mediator in Cardiovascular Disease, Diabetes Mellitus, and Kidney Disease. Cardiovasc Diabetol 2022, 21, 185. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Duca, E.D.; Diaz, A.; Kim, H.J.; Gay-Mimbrera, J.; Zhang, N.; Wu, J.; Beaziz, J.; Estrada, Y.; Krueger, J.G.; et al. Mild Atopic Dermatitis Lacks Systemic Inflammation and Shows Reduced Nonlesional Skin Abnormalities. Journal of Allergy and Clinical Immunology 2021, 147, 1369–1380. [Google Scholar] [CrossRef] [PubMed]
- Del Duca, E.; Renert-Yuval, Y.; Pavel, A.B.; Mikhaylov, D.; Wu, J.; Lefferdink, R.; Fang, M.; Sheth, A.; Blumstein, A.; Facheris, P.; et al. Proteomic Characterization of Atopic Dermatitis Blood from Infancy to Adulthood. Journal of the American Academy of Dermatology 2023, 88, 1083–1093. [Google Scholar] [CrossRef] [PubMed]
- Hirai, T.; Zenke, Y.; Yang, Y.; Bartholin, L.; Beura, L.K.; Masopust, D.; Kaplan, D.H. Keratinocyte-Mediated Activation of the Cytokine TGF-β Maintains Skin Recirculating Memory CD8+ T Cells. Immunity 2019, 50, 1249–1261e5. [Google Scholar] [CrossRef] [PubMed]
- Humeau, M.; Boniface, K.; Bodet, C. Cytokine-Mediated Crosstalk Between Keratinocytes and T Cells in Atopic Dermatitis. Front. Immunol. 2022, 13, 801579. [Google Scholar] [CrossRef]
- Julia, V.; Staumont-Salle, D.; Dombrowicz, D. Rôle de La Fractalkine/CX3CL1 et de Son Récepteur CX3CR1 Dans Les Pathologies Allergiques. médecine/sciences 2016, 32, 260–266. [Google Scholar] [CrossRef]
- Julia, V. CX3CL1 in Allergic Diseases: Not Just a Chemotactic Molecule. Allergy 2012, 67, 1106–1110. [Google Scholar] [CrossRef]
- Staumont-Sallé, D.; Fleury, S.; Lazzari, A.; Molendi-Coste, O.; Hornez, N.; Lavogiez, C.; Kanda, A.; Wartelle, J.; Fries, A.; Pennino, D.; et al. CX3CL1 (Fractalkine) and Its Receptor CX3CR1 Regulate Atopic Dermatitis by Controlling Effector T Cell Retention in Inflamed Skin. Journal of Experimental Medicine 2014, 211, 1185–1196. [Google Scholar] [CrossRef]
- Chong, S.; Lan, H.; Zeng, K.; Zhao, X. Serum Fractalkine (CX3CL1) Concentration Correlates with Clinical Severity in Pediatric Atopic Dermatitis Patients. Ann Clin Lab Sci 2016, 46, 168–173. [Google Scholar]
Figure 1.
Key characteristics of Dupilumab-treated and Dupilumab-untreated AD patients. (A) Study design. Patients with Atopic dermatitis (n = 19) were examined. Out of them 9 patients underwent Dupilumab therapy (DT) and 10 patients were treatment (DUT). Ten healthy subjects were enrolled in the study (HS). Plasma samples were obtained during the birch pollen season (day 380-385 after the initiation of Dupilumab treatment for DT). (B) SCORAD values during the birch pollen season and at the baseline for the DT and DUT groups. (C) Bet v 1-specific IgE antibody levels in DT, DUT and healthy subjects (HS). (D) The cytokines profile for the Dupilumab-treated (DT, blue) and Dupilumab-untreated (DUT, red) patients and healthy subjects (HS, violet). Lines connect the median values of each cytokine. Significant differences between the groups as determined by Wilcoxon test, Mann-Whitney test, and by Kruskal-Wallis test with Dunn’s test indicated: *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001, ns – not significant. Data are presented as median ± IQR.
Figure 1.
Key characteristics of Dupilumab-treated and Dupilumab-untreated AD patients. (A) Study design. Patients with Atopic dermatitis (n = 19) were examined. Out of them 9 patients underwent Dupilumab therapy (DT) and 10 patients were treatment (DUT). Ten healthy subjects were enrolled in the study (HS). Plasma samples were obtained during the birch pollen season (day 380-385 after the initiation of Dupilumab treatment for DT). (B) SCORAD values during the birch pollen season and at the baseline for the DT and DUT groups. (C) Bet v 1-specific IgE antibody levels in DT, DUT and healthy subjects (HS). (D) The cytokines profile for the Dupilumab-treated (DT, blue) and Dupilumab-untreated (DUT, red) patients and healthy subjects (HS, violet). Lines connect the median values of each cytokine. Significant differences between the groups as determined by Wilcoxon test, Mann-Whitney test, and by Kruskal-Wallis test with Dunn’s test indicated: *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001, ns – not significant. Data are presented as median ± IQR.
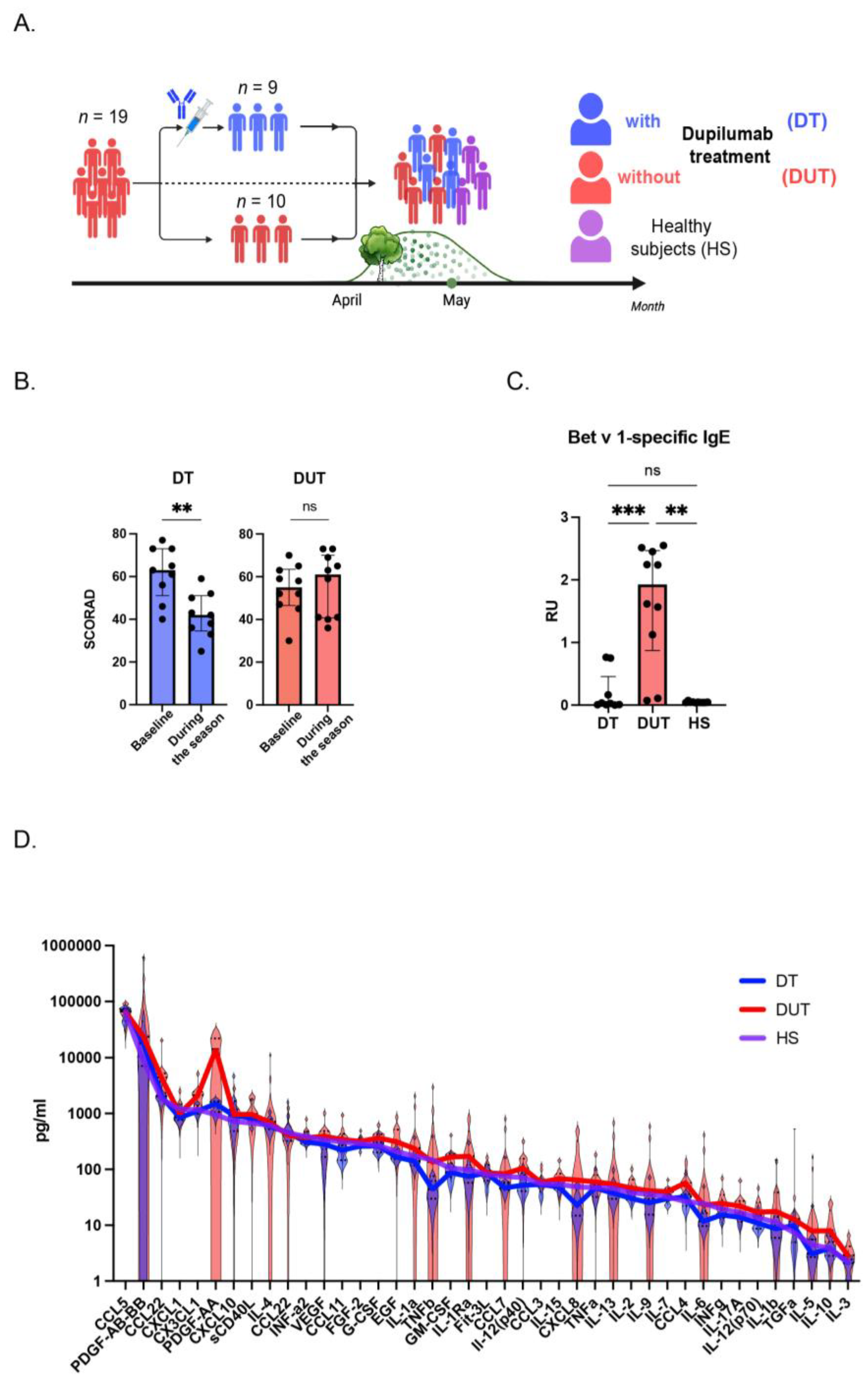
Figure 2.
Comprehensive analysis of cytokines in Dupilumab-treated and Dupilumab-untreated groups. Comparison of cytokine levels for Type 2 inflammatory cytokines (A), Th17-cytokines (B), growth factors (C), anti-inflammatory cytokines (D), and chemokines (E). DT patients are colored in blue, DUT – in red, and HS – in violet. Significant differences between groups as determined by Kruskal-Wallis test with Dunn’s test indicated: *P < 0.05, **P < 0.01, ns – not significant. Data are presented as median ± IQR.
Figure 2.
Comprehensive analysis of cytokines in Dupilumab-treated and Dupilumab-untreated groups. Comparison of cytokine levels for Type 2 inflammatory cytokines (A), Th17-cytokines (B), growth factors (C), anti-inflammatory cytokines (D), and chemokines (E). DT patients are colored in blue, DUT – in red, and HS – in violet. Significant differences between groups as determined by Kruskal-Wallis test with Dunn’s test indicated: *P < 0.05, **P < 0.01, ns – not significant. Data are presented as median ± IQR.
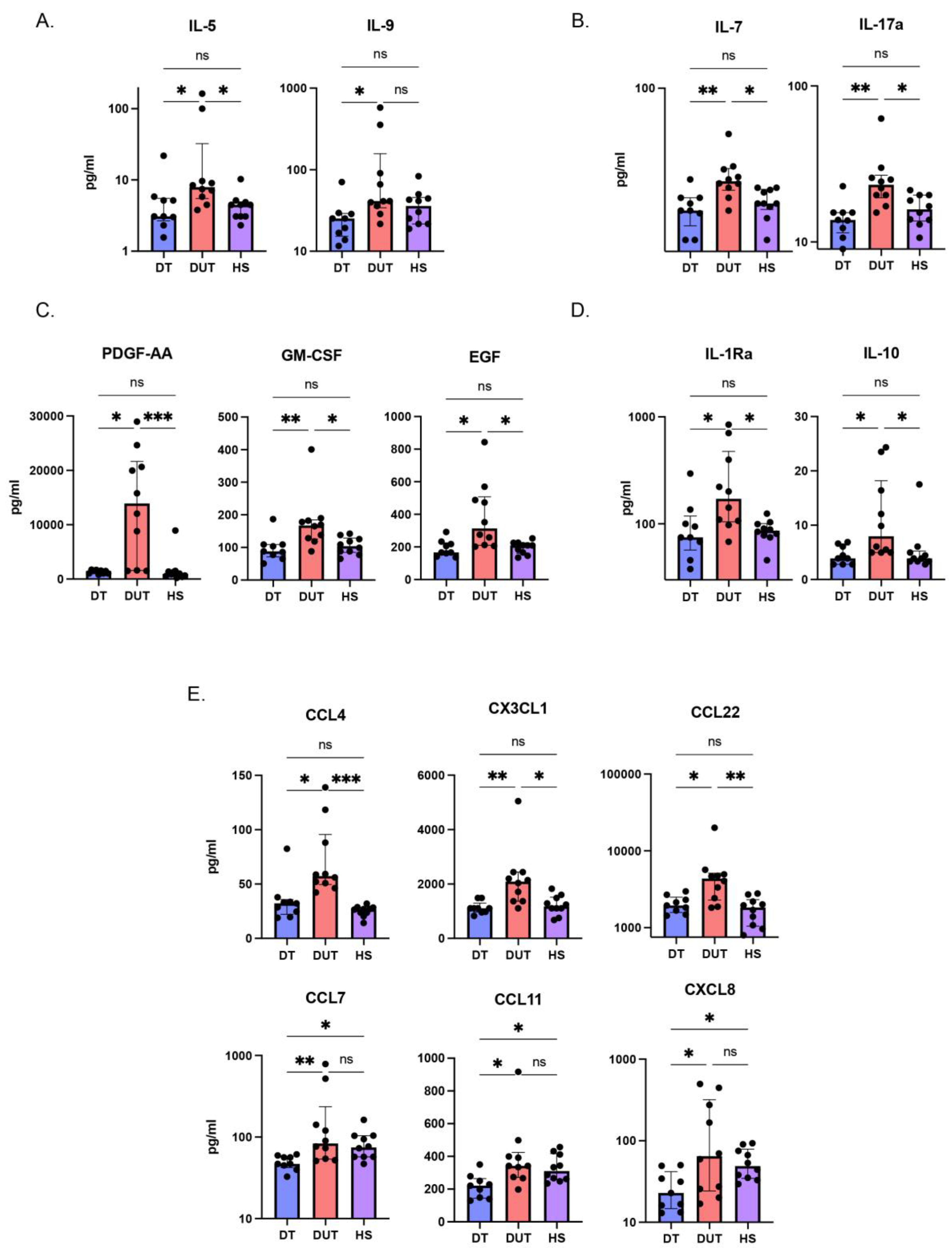
Figure 3.
Identification of the key cytokines in Dupilumab-treated, Dupilumab-untreated groups. (A) Correlations between SCORAD indexes and cytokine levels. Blue and red symbols indicate Dupilumab-treated and Dupilumab-untreated patients, respectively. Asterisks indicate significant correlations according to nonparametric Spearman test, *P < 0.05, **P < 0.01. (B) Principal component analysis (PCA) of Dupilumab-treated, Dupilumab-untreated patients and healthy subjects. Three distinct clusters are indicated by the ovals. (C) Heatmap and hierarchical clustering of DT, DUT patients and HS. Columns denote patients and healthy subjects. Rows correspond to major cytokines. Dupilumab-treated patients are colored in blue, Dupilumab-untreated patients – in red, and healthy subjects – in violet.
Figure 3.
Identification of the key cytokines in Dupilumab-treated, Dupilumab-untreated groups. (A) Correlations between SCORAD indexes and cytokine levels. Blue and red symbols indicate Dupilumab-treated and Dupilumab-untreated patients, respectively. Asterisks indicate significant correlations according to nonparametric Spearman test, *P < 0.05, **P < 0.01. (B) Principal component analysis (PCA) of Dupilumab-treated, Dupilumab-untreated patients and healthy subjects. Three distinct clusters are indicated by the ovals. (C) Heatmap and hierarchical clustering of DT, DUT patients and HS. Columns denote patients and healthy subjects. Rows correspond to major cytokines. Dupilumab-treated patients are colored in blue, Dupilumab-untreated patients – in red, and healthy subjects – in violet.
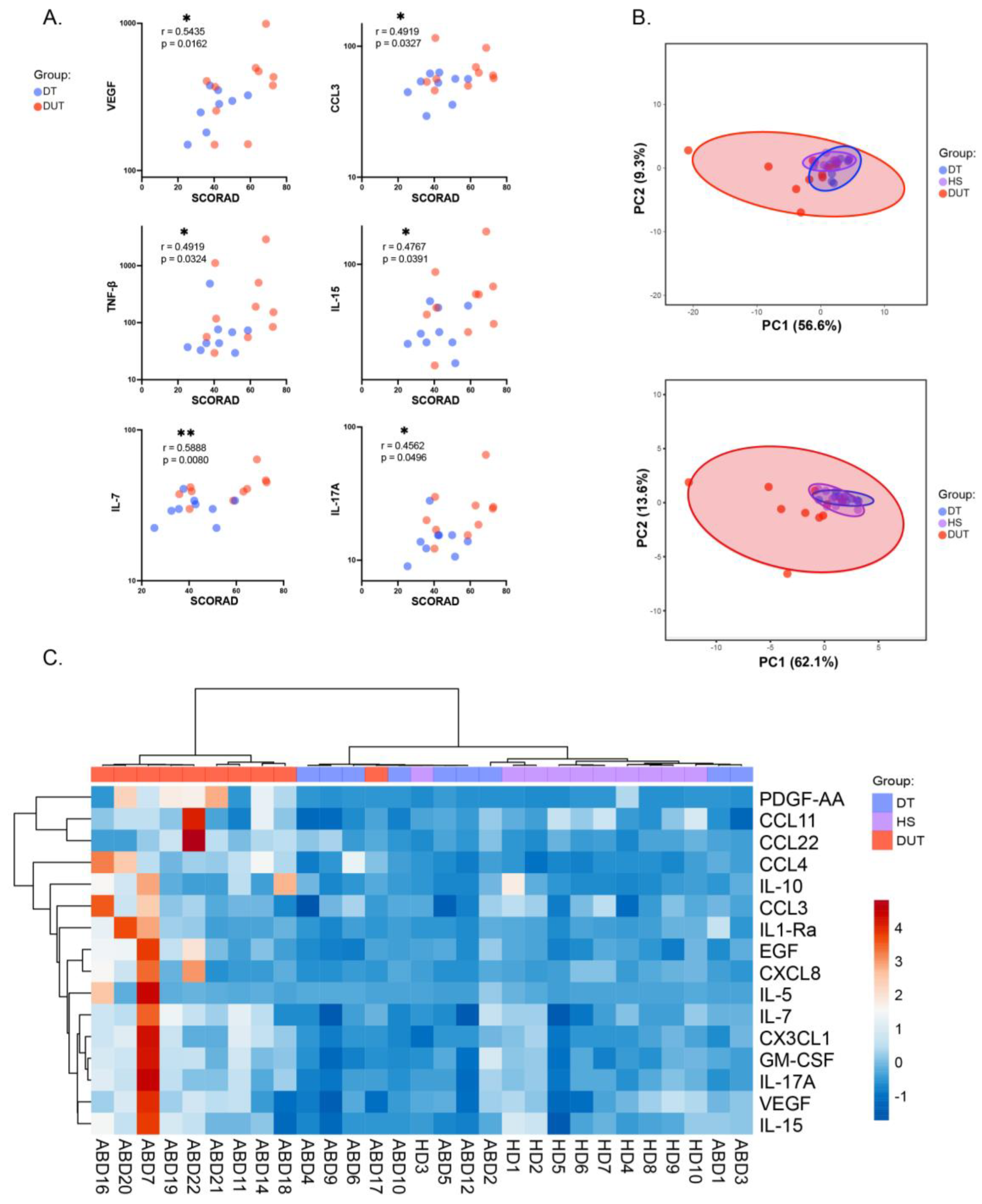

Table 1.
Clinical characteristics of AD patients and Healthy volunteers.
| Dupilumab-treated patients (DT) | Dupilumab-untreated patients (DUT) | Healthy subjects (HS) | |
|---|---|---|---|
| demographical data | Number of subjects | ||
| 9 | 10 | 10 | |
| Age, Me [Q1;Q3] years | |||
| 32.0 [23.0; 39.0] | 26.5 [22.3; 29.5] | 25.5 [24.3; 28.5] | |
| Sex(%) | |||
| m: 6 (66.7%) | m: 3 (30.0%) | m: 5 (50.0%) | |
| f: 3 (33.3%) | f: 7 (70.0%) | F: 5 (50.0%) | |
| AD characterization | AD duration (years), Me | ||
| 12 | 10 | 0 | |
| SCORAD at baseline, Me [Q1;Q3] | |||
| 63 [56.2; 72.5] | 54,65 [48.5; 61.9] | n/a | |
| SCORAD , Me [Q1;Q3] | |||
| 42,2 [35.7; 50.0] | 60,85 [40.7; 67.7] | 0 [0;0] | |
| DLQI, Me[Q1;Q3] | |||
| 5 [5.0; 12.0] | 12 [7.5; 20.0] | 0 [0;0] | |
| Itch intensity, NRS score, Me [Q1;Q3] | |||
| 4 [3.0; 6.0] | 6 [4.3; 8.8] | 0 [0;0] | |
| Allergic comorbidities | Allergic rhinitis, n(%) | ||
| 9 (100%) | 10 (100.0%) | 0 (0.0%) | |
| Asthma, n(%) | |||
| 5 (55.6%) | 5 (50.0%) | 0 (0.0%) | |
| Food allergy,n(%) | |||
| 5 (55.6%) | 8 (80.0%) | 0 (0.0%) | |
| IgE sensitization profile | House dust mites, n(%) | ||
| 8 (88.9%) | 10 (100.0%) | 0 (0.0%) | |
| Epidermal allergens, n(%) | |||
| 7 (77.8%) | 10 (100.0%) | 0 (0.0%) | |
| Trees pollen, n(%) | |||
| 9 (100%) | 10 (100.0%) | 0 (0.0%) | |
| Grass pollen, n(%) | |||
| 6 (66.7%) | 5 (50.0%) | 0 (0.0%) | |
| Weeds pollen, n(%) | |||
| 5 (55.6%) | 6 (60.0%) | 0 (0.0%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



