
Submitted:
26 October 2023
Posted:
27 October 2023
You are already at the latest version
Abstract
Renal cell carcinoma (RCC), alternative term for kidney cancer, is becoming more common worldwide each year, and there are many different contributing factors. Among all cancers, RCC is the 14th most prevalent; and it ranks as the 14th and 9th most prevalent cancer overall for women and men respectively. RCC cases increased by more than 430,000 in 2020. While disease burdens are highest in Eastern Europe (Belarus and Russia) and North America (Canada and the United States), Africa, Asia, and Latin America are predicted to report increase in prevalence as these regions embrace change in lifestyle. The majority of RCC cases are accidentally found on imaging, and survival is greatly impacted by the disease stage at diagnosis, with a metastatic cancer having a 5-year survival rate of 12%. As a consequence of early discovery and more improved treatments, RCC mortality has declined. The key epidemiologic variables of RCC include vast regional and geographical heterogeneity in prevalence rates, and the cause is largely unclear. Recognized risk factors include smoking, being overweight, having previous episodes of hypertension, and suffering chronic renal illness. Unexpectedly swift, RCC diagnosis and therapy have advanced. RCC prevalence continues to rise although survival rates have sharply improved. Cancer survival and treatment have improved, and more gains are projected as a result of clinical and translational research. In this review, kidney cancer statistics and recent literatures are examined on a global scale. It covered aspects of kidney cancer, including its epidemiology, causes, risk factors, current immunotherapy, chances for prevention, and future planning.
Keywords:
Renal cell carcinoma
; Epidemiology
; Immunotherapy
; Prevalence rate
; Mortality rate
INTRODUCTION
Renal Cell Carcinoma (RCC), is a condition in which cancerous cells develop in the kidney's tubules [1,2]. Clear cell (75% of renal cell carcinomas), papillary (15% to 20%), and chromophobe (5%) are the three main histological subtypes of RCC [3,4]. Nephroblastoma (5–6%), transitional cell carcinoma (8%), renal medullary carcinomas (1%) and renal sarcomas (1%), which complete the remaining 15% of kidney tumors, are also present [5]. RCC incidence varies greatly over the world, with Czech Republic and the North America having the highest incidence rates [6,7]. Each year, there are 14,000 RCC-related mortalities and 64,000 incidence rate of RCC in the US [8].
Due to its propensity to be found at a later stage, clear cell RCC has the worst disease-specific survival rates [3]. The risk of RCC can be impacted by smoking and the overuse of some painkillers [9]. This condition is influenced by factors like gender, race, and age. RCC is increasingly prevalent in males over the age of 60, and ages between 60-80 years have the highest proportion [5]. Compared to Asian-Americans or Pacific Islanders in the US, RCC is increasingly prevalent among Caucasians, African-Americans, Hispanics, and Native Americans [7,10].
In the last ten years, significant progress has been achieved in the management of RCC. Secondary to a better awareness of the biological mechanisms underlying the progression of cancer are advancements in treatment [11]. A number of novel immuno-oncology medications have demonstrated excellent performance in treating advanced kidney cancer, and they are now being investigated in conjunction with targeted therapy [12]. One of the primary components of the advancements has been the development of targeted therapy as the cornerstone of management in RCC [13]. In this narrative review, kidney cancer statistics and recent literature are examined on a global scale. It covered aspects of kidney cancer, including its epidemiology, causes, risk factors, current management, chances for prevention, and future planning.
1. Epidemiology of renal cell carcinoma
A crucial tool for addressing many issues about the cause of cancer is epidemiology. Numerous clinical variables linked to the progression of RCC have been identified, and differences in gender, age, and regional distribution have been described [14,15,16,17,18]. In vitro research and experimental models have both provided in-depth demonstrations of several of them, however, publications with a special attention on comparing RCC in the world are hard to find.
1.1.1. Global Epidemiology of renal cell carcinoma
Among all cancers, RCC is the 14th most prevalent. It ranks as the 14th and 9th most prevalent cancer overall for women and men respectively [17,19]. The World Cancer Research Fund International reported that there were more than 430,000 new cases of RCC in 2020 [20].
Providing periodical estimates of the global burden of cancer is one of the duties of the CSU of the IARC. The 2018 estimates of cancer incidence and death from GLOBOCAN 2020 are updated from previously published estimates. The United Nations’ 20 world regions are used as the base units for estimation as before, along with results that have been combined internationally [21]. Estimates were created for 18 of age and above and 38 cancer locations, including gender and unidentified malignancies. Using on the GLOBOCAN estimations of cancer prevalence and mortality provided by the IARC, we mentioned the burden of RCC globally in 2020 in this review. The IARC describes the sources and procedures used in creating the GLOBOCAN estimates for 2020 online ( http://gco.iarc.fr/today).
The projected number of prevalent cases over a one-year period are distributed as a proportion in Figure 1. in 2020, kidney cancer only, both sexes, ages 15-74 years in the 195 countries. Most prevalent cases (Proportion ≥ 7.9 per 100,000) occurred in Russia, Belarus, Ukraine, Kazakhstan, Poland, Romania, Argentina and Venezuela. In the second place ranking in terms of prevalent cases (Proportion, 3.4-7.9 per 100,000) occurred in United State, Canada, China, Mongolia, Australia, Brazil, Peru, Nigeria, Namibia among others. Least deaths (Proportion < 0.65 per 100, 000) occurred in Congo, Democratic Republic of Congo, Uganda, Zambia, Madagascar, Mozambique among others.
The prevalence pattern is followed by variations in mortality globally, with the highest rates found in the Baltic nations and the Czech Republic (9.1/100,000 males) [21]. Since the 1990s, the worldwide mortality rate has been steady [6]. The majority of nations have seen a decline in death rates in recent years, with noteworthy exceptions being Croatia, Brazil, Greece, Portugal, Ireland, and Slovenia, where rates have remained on the rise. In general, women appear to be experiencing a faster decline in mortality than males. Black patients in the US have had a greater drop in mortality, and since the 1970s, their mortality rates have remained less compared to those of white patients [21,22,23]. This variation might be explained by racial differences in kidney cancer biology and aggressiveness, but there may be other factors at play as well, such as competitive mortality [24].
Figure 2 shows the distribution of estimated age-standardized mortality rates (ASR) in 2020, kidney cancer only, both sexes, ages 15-74 years in the 195 countries. Most deaths (ASR ≥ 2.8 per 100,000) occurred in Russia, Belarus, Ukraine, Kazakhstan, Poland, Romania, Argentina and Venezuela. In the second place ranking in terms of number of deaths (ASR, 1.8-2.8 per 100,000) occurred in United State, Canada, China, Mongolia, Australia, Brazil, Peru, Nigeria, Namibia among others. Least deaths (ASR< 0.8 per 100, 000) occurred in Congo, Democratic Republic of Congo, Uganda, Zambia, Madagascar, Mozambique among others.
1.1.2. Epidemiology of Kidney Cancer in Europe
Incidence of RCC has been gradually rising, especially in North America [25] and Eastern Europe [6], A number of Eastern and Central European nations have among of the highest prevalence and fatality rates for kidney cancer worldwide [6], and there are no known causes for this occurrence. The estimated number of prevalent cases (1-year) and estimated number of deaths in 2020 of kidney cancer, both sexes, ages 15-74, were deduced from data used to produce a descriptive graph (Figure 3 and Figure 4). The Russian Federation was shown to have the highest prevalent cases (1 year) and deaths when compared to other Eastern and Central Europe countries.
Figure 3 shows the projected number of prevalent cases over a one-year period in 2020, kidney cancer, both sexes, ages 15-74 years in Central and Eastern Europe countries. Most prevalent cases in the order of ranking occurred as follows: Russian Federation (16.496, 20.2 %), Germany (9397, 11.5 %), France (8489, 10.4 %), United Kingdom (7722, 9.4 %), Italy (6738, 8.2 %), Spain (5044, 6.2 %), Ukraine (3681, 4.5 %) and others (24210, 29.6 %).
Figure 4 shows the projected number of deaths in 2020, kidney, both sexes, ages 15-74 years in Eastern and Central Europe countries. Central and Eastern Europe countries variations in mortality due to Kidney cancer show the trend of prevalence, with the highest deaths observed in the order of ranking, as follows: Russian Federation (6.952, 23.6 %), Germany (3110, 10.6 %), France (2295, 7.8 %), United Kingdom (2125, 7.2 %), Ukraine (2112, 7.2 %), Poland (1904, 6.5 %), Italy (1896, 6.4 %) and others (9053, 30.7 %).
2. Causes and risk factors of kidney cancer
Obesity, smoking, high blood pressure and ACKD when there is ESRD are all risk factors for RCC [26,27,28]. RCC may develop as a result of work-related exposure to trichloroethylene, and this situation may also result in higher mortality rates [25]. Trichloroethylene is being categorised as a human carcinogen by the IARC, which links it specifically to renal cancer [3]. Most often, mechanics, oil processors, dry cleaners, producers of polyvinyl chloride, and those who make low-nicotine cigarettes are exposed to trichloroethylene during work [25]. There are 10 hereditary disorders that increase the chance of RCC development [29]. The most prevalent of them is von Hippel-Lindau disease, which causes clear cell RCC by causing VEGF to be activated [29]. The similar etiology is followed by around 60% of sporadic clear cell RCC. New medicines that block VEGF receptors have been created as a result of this discovery and are being utilized to treat heritable and sporadic cases of clear cell RCC [30,31]. A complete elucidation of the risk factors of kidney cancer is shown on Table 1.
3. Current treatment of renal cell carcinoma
The clinical approach to treating individuals with RCC is constantly changing due to new drugs and drug combinations. The highlight and overview of current standards of care for advanced RCC, as well as the most recent therapy advancements are thus:
3.1. Lenvatinib plus pembrolizumab
ICIs and TKIs have transformed first-line therapy for clear cell Renal Cell Carcinoma (ccRCC). The most recent trial, together with Axitinib combined with pembrolizumab, cabozantinib combined with nivolumab and Avelumab combined with Axitinib was Lenvatinib in addition to pembrolizumab. The CLEAR study evaluated pembrolizumab 200mg three times each week in combination with lenvatinib 20 mg each day in comparison to the previous standard of treatment, sunitinib [44,47,48].
Patients showed clear cell histology and were treatment novices. Only about 10% of the 1069 randomized patients presented poor risk disease, with the majority of patients being categorized as good or intermediate risk by the IMDC score. Approximately 7% of patients had sarcomatoid characteristics, a bad prognostic indicator. In comparison to sunitinib, which had a median PFS of 9.2 months and a 2-year overall survival (OS) rate of 70.4%, Having a median PFS of 23.9 months, Lenvatinib combined with pembrolizumab showed outstanding efficacy and an OS rate of 79.2%. As remarkable in the Lenvatinib combined with pembrolizumab arm, 71% of patients experienced an objective response (OR), with 16% achieving complete remission (CR). In all analysed subgroups (CPS), the combination was preferred despite IMDC risk category or PD-L1combined positive score. Except for those who have an IMDC good risk illness, the advantage of the combination for OS was similar across all subgroups. This was only an exploratory discovery, as the study lacked the necessary power to identify variations in OS by IMDC risk group. The combination's greater efficacy is offset by its increased toxicities. In patients taking lenvatinib-pembrolizumab, gastrointestinal issues, fatigue, hypertension, and hypothyroidism were the most frequent adverse events (AE). A grade ≥3 event was experienced by 82% of participants overall versus 71.8% in the sunitinib arm. In 68.8% of patients, the lenvatinib dosage needed to be decreased. Patients in the third treatment arm of the study were administered lenvatinib 18 mg and everolimus 5 mg per day. PFS vs sunitinib was significantly increased by the treatment (14.7 vs. 9.2 months), whereas OS was the same (hazard ratio 1.15). It is not advisable to use this combination as the first-line therapy. because it does not provide an OS benefit. However, the research highlights the effectiveness of Lenvatinib combined with everolimus, and the combination is still an effective treatment choice in later-stage therapy [45]. It seems reasonable to conclude that regardless of IMDC risk category or PD-L1 status, For patients with advanced ccRCC, Lenvatinib combined with pembrolizumab constitutes a new first- line therapy standard of care.
3.2. Belzutifan
Belzutifan, an oral HIF-2 inhibitor, was the subject of two studies that were presented at the genitourinary symposium of ASCO in 2021. If cells are below hypoxic stress, HIF proteins become activated. They enhance neoangiogenesis, proliferation, and tumor growth via its function as transcription factor. Due of the widespread absence of the Von Hippel-Lindau tumor suppressor gene, HIF proteins build up in RCC. Belzutifan prevents HIF-2 and HIF-1 from heterodimerizing, reducing their ability to cause cancer. Belzutifan was administered as a single drug to 55 patients with advanced ccRCC daily at a dose of 120 mg in the first in human phase I/II research [46]. According to the IMDC score, 76% of the patients were categorized as moderate or poor risk and had already had check point and VEGF suppression medication. With a median PFS median of 14.5 months, a DCR of 80% and an ORR of 25%, belzutifan demonstrated good anticancer efficacy. Further research in a randomized phase 3 trial is in progress in light of these exceptional outcomes in a patient population that had previously received treatment. In accordance with a successful trial in phase 2 in this uncommon patient category, the US FDA has previously approved belzutifan for these patients [49]. Belzutifan and cabozantinib were investigated in another trial for their effectiveness and safety in treating patients with metastatic ccRCC [50]. Belzutifan and cabozantinib were taken daily in doses of 120 mg and 60 mg, respectively. 53 individuals who had had up to two prior therapies were included in the preliminary results. The ORR and DCR were confirmed to be 22% and 92.7%, respectively. The combination had a 6-month OS rate of 95% and a median PFS of 16.8 months. Belzutifan and cabozantinib were both discontinued by 11.3% and 15.1% of patients, respectively, of patients due to adverse events, respectively. The results of the study are consistent with the effectiveness of cabozantinib as a single agent as shown in its pivotal trial. Further research into this novel combination is justified by the encouraging results obtained in conjunction with a tolerable safety profile.
3.3. Cabozantinib
A number of small trials were presented that examined cutting-edge therapies for non-ccRCC. The most prevalent non-ccRCC is papillary carcinoma, for which sunitinib was formerly the standard of therapy due to less conclusive data [51]. Patients with non-clear cell histology were not included in studies examining the use of ICIs in conjunction with TKIs or double ICI as the first-line treatment for advanced illness. In addition to VEGF overexpression [52]. According to Mayrhofer and Niedersüß-Beke [53], papillary RCC has a high prevalence of mesenchymal epithelial transition (MET) gene changes. Advanced papillary RCC patients, participated in a randomised phase 2 trial, were compared to sunitinib and other MET kinase inhibitors. Cabozantinib inhibits multiple tyrosine kinases, such as the VEGF receptor, AXL receptor, and the MET tyrosine kinase [54]. Savolitinib and crizotinib's trial arms were prematurely discontinued for ineffectiveness. Sunitinib was given to 46 individuals, while cabozantinib was given to 44 patients. When compared to sunitinib, cabozantinib significantly raised median PFS. (9.0 months). Comparing sunitinib, which had an ORR of 4% and no CR, to cabotinib, which had a 23% ORR with 2 patients even obtaining CR, cabotinib performed much better. The investigation lacked the necessary power to identify variations in overall survival. In comparison to the sunitinib arm (39% of patients), cabozantinib arm (74% of patients) had significantly more grade 3 or 4 incidents, which is in line with the medications' known side effect profile. Therefore, the ESMO recommendation of cabotinib as the best therapy option for these patients can be regarded the new standard of care [53]. Another recent trial that evaluated the effectiveness of cabozantinib in conjunction with nivolumab further supports the drug's action in non-ccRCC [55]. A well-known standard treatment for clear cell RCC is cabozantinib combined with nivolumab [56]. Forty-seven (47) individuals were divided into two cohorts for treatment in a single-arm phase 2 trial based on the histology of their tumors. (cohort 1: papillary, unclassified RCC, cohort 2: chromophobe RCC). It was permitted to get prior therapy, however in cohort 1, which had 40 patients, 65% of them had never received any. The median OS and PFS were 28 and 12.5 months, respectively. In cohort 1, the DCR was 97%, and 48% of patients experienced a partial response. No reactions were seen in patients (cohort 2, 7 individuals) with chromophobe histology. The safety profile of this combination was consistent with its known toxicity profile. For the drugs cabozantinib and nivolumab, respectively, therapy was stopped in 17% and 19% of patients. In contrast to chromophobe RCC, which appears to be resistant to cabozantinib even when used in conjunction with immunotherapy, the study emphasizes the drug's activity in papillary RCC [56].
3.4. Current standard of care
For fit patients with metastatic ccRCC, the first-line conventional treatment consists of either double checkpoint inhibition or a TKI [53]. Pembrolizumab + axitinib [57], nivolumab + cabozantinib [56] and pembrolizumab + lenvatinib [58], when Compared to sunitinib, revealed there is a survival advantage regardless of PD-L1 status or IMDC risk category. Nivolumab + ipilimumab has an OS advantage over sunitinib in IMDC moderate or poor risk illness; as a result, it is also a recommended therapy standard in this patient population [59,60].
4. Area of prevention opportunities and future direction
Although the causes of kidney cancer are believed to be multiple, the etiology is mostly unclear (Table 1). A variety of risk variables have been researched up to this point, some of which are changeable and so present a chance for primary prevention. Abstaining from or quitting smoking, avoiding being overweight or obese, and managing hypertension are likely to play a significant role in lowering the risk of kidney cancer. To this purpose, the promotion and uptake of healthy behaviors are greatly assisted by primary care physicians and public health organizations. On a larger scale, geographic and environmental exposures at the national level, such as trichloroethylene and unidentified others, would necessitate system-level measures to affect not only the risk of kidney cancer but also the general health of the community. Nevertheless, kidney cancer is not typically seen as an occupational cancer. There hasn't been any concrete proof of a link between kidney cancer and environmental exposures in general. Additionally, renal cell carcinoma alters the tumor microenvironment to trigger an immune response, just like all other malignancies do. This alteration influences the cytokine signalling patterns of circulating immune cells, which may also be useful as cancer biomarkers or therapeutic targets.
5. Conclusion
While 2% of all cancer diagnoses and mortality worldwide are RCC, its prevalence has significantly increased in the developed world, becoming the 14th most prevalent; and it ranks as the 14th and 9th most prevalent cancer overall for women and men respectively. Clear cell histological subtype is the most prevalent, then papillary and chromophobe, and it has the strongest connections with several modifiable and unmodifiable risk factors. RCC can be prevented by avoiding modifiable risk factors. Accurate imaging analysis is essential for its early detection, and physicians need to be educated in RCC imaging diagnosis and early care. RCC therapy has evolved, and several combinations of therapies are currently being proposed. These medicines have increased patient overall survival, which has resulted in a rise in the prevalence of RCC. All of this emphasizes the need to expand research, particularly on proven beneficial combined therapy approaches.
Author Contributions
Each author reviewed this paper for intellectual content and is responsible for its accuracy. All writers also contributed to the conceptualisation or interpretation of the work. The final version was submitted with unanimous approval from all authors.
Funding
No funding.
Acknowledgments
Ministry of Science and Higher Education of the Russian Federation within the framework of state support for the creation and development of World-Class Research Centers "Digital biodesign and personalized healthcare" №075-15-2022-304.
Conflict of interest
The authors declare no conflicts of interest.
AVAILABILITY OF DATA AND MATERIALS
The datasets created and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Abbreviations
RCC= Renal cell carcinoma
ccRCC= Clear cell RCC
ACKD= Acquired cystic kidney disease
ESRD= End-stage renal disease
VEGF= Vascular endothelial growth factor
CSU= Cancer Surveillance Branch (CSU)
IARC= International Agency for Research on Cancer.
GLOBOCAN= Global Cancer Observatory
IMDC= International metastatic renal cell carcinoma database consortium
CLEAR study= A type of clinical trial in which participants are randomly assigned to groups that receive one or more interventions/treatments (or no intervention).
PFS= Progression-free survival
PD-L1= Programmed death-ligand 1
ICIs= Immune checkpoint inhibitors
TKIs= Tyrosine kinase inhibitors
HIF-2= Hypoxia inducible factor 2
NSAIDs= Nonsteroidal anti-inflammatory drugs
ASCO= American Society of Clinical Oncology (ASCO)
ORR= Objective response rate
DCR= Disease control rate
FDA= Food and Drug Administration
ESMO= European Society for Medical Oncology
References
- Sharma R, Kadife E, Myers M, Kannourakis G, Prithviraj P, Ahmed N. Determinants of resistance to VEGF-TKI and immune checkpoint inhibitors in metastatic renal cell carcinoma. J. Exp Clin Cancer Res 2021, 40(1), 1-27. [CrossRef]
- Shah A, Lal P, Toorens E, Palmer MB, Schwartz L, Vergara N, et al. Acquired cystic kidney disease–associated renal cell carcinoma (ACKD-RCC) harbor recurrent mutations in KMT2C and TSC2 genes. Am J Surg Pathol. 2020, 44(11), 1479-1486. [CrossRef]
- Gray RE, Harris GT. Renal cell carcinoma: diagnosis and management. Am. Fam. Physician. 2019, 99(3), 179-184. https://www.aafp.org/pubs/afp/issues/2019/0201/p179.html.
- Ricketts CJ, De Cubas AA, Fan H, Smith CC, Lang M, Reznik E, et al. The cancer genome atlas comprehensive molecular characterization of renal cell carcinoma. Cell Rep. 2018, 23(1), 313-326. [CrossRef]
- Nabi S, Kessler ER, Bernard B, Flaig TW, Lam ET. Renal cell carcinoma: a review of biology and pathophysiology. F1000Research. 2018, 7, 307. [CrossRef]
- Znaor A, Lortet-Tieulent J, Laversanne M, Jemal A, Bray F. International variations and trends in renal cell carcinoma incidence and mortality. Eur. Urol. 2015, 67(3), 519-530. [CrossRef]
- Chow WH, Dong LM, Devesa SS. Epidemiology and risk factors for kidney cancer. Nat Rev Urol. 2010, 7(5), 245-257. [CrossRef]
- Singh D. Current updates and future perspectives on the management of renal cell carcinoma. Life Sci. 2021, 264, 118632. [CrossRef]
- Tahbaz R, Schmid M, Merseburger AS. Prevention of kidney cancer incidence and recurrence: lifestyle, medication and nutrition. Curr Opin Urol. 2018, 28(1), 62-79. [CrossRef]
- Dizman N, Salgia NJ, Bergerot PG, Hsu J, Ruel N, Pal SK. Race/Ethnicity and Survival in Metastatic Renal Cell Carcinoma: Outcomes for Patients Receiving First Line Targeted Therapies. Kidney Cancer. 2020, 4(3), 159-166. [CrossRef]
- Elmore LW, Greer SF, Daniels EC, Saxe CC, Melner MH, Krawiec GM, et al. Blueprint for cancer research: Critical gaps and opportunities. CA: Cancer J. Clin. 2021, 71(2), 107-139. [CrossRef]
- Graham J, Heng DY, Brugarolas J, Vaishampayan U. Personalized management of advanced kidney cancer. Am Soc Clin Oncol Edu Book. 2018, 38, 330-341. https://ascopubs.org/doi/pdf/10.1200/EDBK_201215?role=tab.
- Choueiri TK, Kaelin Jr. WG. Targeting the HIF2–VEGF axis in renal cell carcinoma. Nat Med. 2020, 26(10), 1519-1530. [CrossRef]
- Nocera L, Karakiewicz PI, Wenzel M, Tian Z, Shariat SF, Saad F, et al. Clinical outcomes and adverse events after first-line treatment in metastatic renal cell carcinoma: a systematic review and network meta-analysis. J. Urol, 2022, 207(1), 16-24. [CrossRef]
- Ma X, Long L, Moon S, Adamson BH, Baxi SS. Comparison of population characteristics in real-world clinical oncology databases in the US: Flatiron Health, SEER, and NPCR. MedRxiv, 2020, 2020-03. [CrossRef]
- Fukushima H, Saito K, Yasuda Y, Tanaka H, Patil D, Cotta BH, et al. Female gender predicts favorable prognosis in patients with non-metastatic clear cell renal cell carcinoma undergoing curative surgery: results from the International Marker Consortium for Renal Cancer (INMARC). Clin Genitourin Cancer. 2020, 18(2), 111-116. [CrossRef]
- Usher-Smith J, Simmons RK, Rossi SH, Stewart GD. Current evidence on screening for renal cancer. Nat Rev Urol. 17(11), (2020), 637-642. https://www.nature.com/articles/s41585-020-0363-3.
- Mancini M, Righetto M, Baggio G. Gender-related approach to kidney cancer management: Moving forward. Int J Mol Sci. 2020, 21(9), 3378. [CrossRef]
- Rossi SH, Klatte T, Usher-Smith J, Stewart GD. Epidemiology and screening for renal cancer. World J. Urol. 2018, 36, 1341-1353. [CrossRef]
- Lalani AKA, Heng DY, Basappa NS, Wood L, Iqbal N, McLeod D, et al. Evolving landscape of first-line combination therapy in advanced renal cancer: a systematic review. Ther Adv Med Oncol. 2022, 14. [CrossRef]
- Scelo G, Larose TL. Epidemiology and risk factors for kidney cancer. J. Clin Oncol. 2018, 36(36), 3574. [CrossRef]
- Singh GK, Jemal A. Socioeconomic and racial/ethnic disparities in cancer mortality, incidence, and survival in the United States, 1950–2014: over six decades of changing patterns and widening inequalities. J. Environ Public Health. 2017, (2017), ID: 2819372. [CrossRef]
- Lipworth L, Tarone RE, McLaughlin JK. Renal cell cancer among African Americans: an epidemiologic review. BMC cancer. 2011, 11, 1-10. [CrossRef]
- Al-Husseini MJ, Kunbaz A, Saad AM, Santos JV, Salahia S, Iqbal M, et al. Trends in the incidence and mortality of transitional cell carcinoma of the bladder for the last four decades in the USA: a SEER-based analysis. BMC cancer. 2019, 19(1), 1-12. [CrossRef]
- Padala SA, Barsouk A, Thandra KC, Saginala K, Mohammed A, Vakiti A, et al. Epidemiology of renal cell carcinoma. World J. Oncol. 2020, 11(3), 79-87. https://wjon.org/index.php/wjon/article/view/1279/989.
- Saly DL, Eswarappa MS, Street SE, Deshpande P. Renal Cell Cancer and Chronic Kidney Disease. Adv Chronic Kidney Dis. 2021, 28(5), 460-468. [CrossRef]
- Escudier B, Porta C, Schmidinger M, Rioux-Leclercq N, Bex A, Khoo V, Grünwald V, et al. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann.Oncol. 2019, 30(5), 706-720. [CrossRef]
- Capitanio U, Bensalah K, Bex A, Boorjian SA, Bray F, Coleman J, et al. Epidemiology of renal cell carcinoma. Eur Urol, 2019, 75(1), 74-84. [CrossRef]
- Haas NB, Nathanson KL. Hereditary kidney cancer syndromes. Adv chronic kidney Dis. 2014, 21(1), 81-90. [CrossRef]
- Albiñana V, Gallardo-Vara E, de Rojas-P I, Recio-Poveda L, Aguado T, Canto-Cano A, et al. Targeting β2-adrenergic receptors shows therapeutical benefits in clear cell renal cell carcinoma from Von Hippel–Lindau Disease. J. Clin Med. 2020, 9(9), 2740. [CrossRef]
- Nandagopal L, Sonpavde GP, Agarwal N. Investigational MET inhibitors to treat Renal cell carcinoma. Expert Opin Investig Drugs. 2019. 28(10), 851-860. [CrossRef]
- Boi SK, Orlandella RM, Gibson JT, Turbitt WJ, Wald G, Thomas L, et al. Obesity diminishes response to PD-1-based immunotherapies in renal cancer. J. immunother Cancer. 2020, 8(2), e000725. [CrossRef]
- Aurilio G, Piva F, Santoni M, Cimadamore A, Sorgentoni G, Lopez-Beltran A, et al. The role of obesity in renal cell carcinoma patients: clinical-pathological implications. Int J. Mol Sci. 2019, 20(22), 5683. [CrossRef]
- Cohen JB, Geara AS, Hogan JJ, Townsend RR. Hypertension in cancer patients and survivors: epidemiology, diagnosis, and management. Cardio Oncol. 2019, 1(2), 238-251. [CrossRef]
- Berkenblit R, Ricci Z, Kanmaniraja D, Sarungbam J. CT features of acquired cystic kidney disease-associated renal cell carcinoma. Clin Imaging. 2022, 83, 83-86. [CrossRef]
- Kondo T, Sassa N, Yamada H, Takagi T, Iizuka J, Kobayashi H, et al. Comparable survival outcome between acquired cystic disease associated renal cell carcinoma and clear cell carcinoma in patients with end-stage renal disease: a multi-institutional central pathology study. Pathol. 2021, 53(6), 720-727. [CrossRef]
- Wozniak MB, Brennan P, Brenner DR, Overvad K, Olsen A, Tjønneland A, et al. Alcohol consumption and the risk of renal cancers in the E uropean prospective investigation into cancer and nutrition (EPIC). Int J. Cancer. 2015, 137(8), 1953-1966. [CrossRef]
- Singh S, Chaurasia A, Gopal N, Malayeri A, Ball MW. Treatment Strategies for Hereditary Kidney Cancer: Current Recommendations and Updates. Discovery Med. 2022, 34(173), 205-220. https://pubmed.ncbi.nlm.nih.gov/36602871/.
- Linehan LM, Pinto PA, Bratslavsky G, Pfaffenroth E, Merino M, Vocke CD, et al. Toro, J.R.; Bottaro, D.; Neckers, L.; Schmidt, L.S.; Srinivasan, R. Hereditary kidney cancer: unique opportunity for disease-based therapy. Cancer, 2009, 115(S10), 2252-2261. [CrossRef]
- Behrens G, Leitzmann MF. The association between physical activity and renal cancer: systematic review and meta-analysis. Br J. Cancer. 2013, 108(4), 798-811. [CrossRef]
- Tseng CH. Type 2 diabetes mellitus and kidney cancer risk: a retrospective cohort analysis of the National Health Insurance. PloS one, 2015, 10(11), e0142480. [CrossRef]
- Buhagen M, Grønskag A, Ragde SF, Hilt B. Association between kidney cancer and occupational exposure to trichloroethylene. J. Occup Environ Med. 2016, 58(9), 957-959. [CrossRef]
- Zunarelli C, Godono A, Visci G. Violante FS, Boffetta P. Occupational exposure to asbestos and risk of kidney cancer: an updated meta-analysis. Eur J Epidemiol. 2021, 36(9), 927-936. [CrossRef]
- Nayan M, Juurlink DN, Austin PC. Macdonald, E.M.; Finelli, A.; Kulkarni, G.S.; Hamilton, R.J. Canadian Drug Safety and Effectiveness Research Network (CDSERN). Medication use and kidney cancer risk: A population-based study. Eur J Cancer, 2017, 83, 203-210. [CrossRef]
- Nayan M, Macdonald EM, Juurlink DN, Austin PC, Finelli A, Kulkarni GS, et al. Medication use and survival in diabetic patients with kidney cancer: A population-based cohort study. Pharmacological research, 2016, 113, 468-474. [CrossRef]
- Choueiri TK, Je Y, Cho E. Analgesic use and the risk of kidney cancer: A meta-analysis of epidemiologic studies. International journal of cancer. 2014, 134(2):384-96. [CrossRef]
- Rini BI, Plimack ER, Stus V, Gafanov R, Hawkins R, Nosov D, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. 2019 Mar 21;380(12):1116–27. Available from: http://www.nejm.org/doi/10.1056/NEJMoa1816714.
- Ged Y, Lee CH. Lenvatinib plus pembrolizumab combination therapy for adult patients with advanced renal cell carcinoma. Expert Review of Anticancer Therapy. 2022 Oct 3;22(10):1049–59. Available from: https://www.tandfonline.com/doi/full/10.1080/14737140.2022.2128336.
- Motzer R, Alekseev B, Rha SY, Porta C, Eto M, Powles T, et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021 Apr 8;384(14):1289–300. Available from: http://www.nejm.org/doi/10.1056/NEJMoa2035716.
- Motzer RJ, Hutson TE, Glen H, Michaelson MD, Molina A, Eisen T, et al., Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: a randomised, phase 2, open-label, multicentre trial. Lancet Oncol. 2015, 16(15), 1473-1482. [CrossRef]
- Bauer TM, Choueiri TK, Papadopoulos KP, Plimack ER, Merchan JR, McDermott DF, et al. The oral HIF-2 α inhibitor MK-6482 in patients with advanced clear cell renal cell carcinoma (RCC): Updated follow-up of a phase I/II study. J. Clin Oncol. 2021, 39(6), 273-273. [CrossRef]
- Srinivasan R, Donskov F, Iliopoulos O, Rathmell WK, Narayan V, Maughan BL, et al. Phase 2 study of belzutifan (MK-6482), an oral hypoxia-inducible factor 2α (HIF-2α) inhibitor, for Von Hippel-Lindau (VHL) disease-associated clear cell renal cell carcinoma (ccRCC). J. Clin Oncol. 2021, 39(15), 4555-4555. [CrossRef]
- Choueiri TK, Bauer TM, McDermott DF, Arrowsmith E, Roy A, Perini RF, et al. Tykodi, S.S.. Phase 2 study of the oral hypoxia-inducible factor 2α (HIF-2α) inhibitor MK-6482 in combination with cabozantinib in patients with advanced clear cell renal cell carcinoma (ccRCC). J. Clin Oncol. 2021, 39(6), 272-272. [CrossRef]
- Armstrong AJ, Halabi S, Eisen T, Broderick S, Stadler WM, Jones RJ, et al. Everolimus versus sunitinib for patients with metastatic non-clear cell renal cell carcinoma (ASPEN): a multicentre, open-label, randomised phase 2 trial. Lancet Oncol. 2016, 17(3), 378-388. [CrossRef]
- Song SH. Jeong IG, You D, Hong JH, Hong BS, Song C, et al. 609 VEGF/VEGFR2 or PDGF-β/PDGFR-β expression in non-metastatic, renal cell carcinoma: a prospective study with 1,091 consecutive cases. J. Urol. 2013, 189(4S), e249-e249. [CrossRef]
- Mayrhofer K, Niedersüß-Beke D. New targeted therapies in kidney cancer. Memo-Mag Eur Med Oncol. 2022, 15(2), 133-136. [CrossRef]
- Pal SK, Tangen C, Thompson IM, Balzer-Haas N, George DJ, Heng DY, et al.A comparison of sunitinib with cabozantinib, crizotinib, and savolitinib for treatment of advanced papillary renal cell carcinoma: a randomised, open-label, phase 2 trial. Lancet, 2021, 397(10275), 695-703. [CrossRef]
- Lee CH, Voss MH, Carlo MI Chen YB, Reznik E, Knezevic A, et al. Nivolumab plus cabozantinib in patients with non-clear cell renal cell carcinoma: results of a phase 2 trial. J. Clin Oncol. 2021, 39(15_suppl), 4509. [CrossRef]
- Choueiri TK, Powles T, Burotto M, Escudier B, Bourlon MT, Zurawski B, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J. Med. 2021, 384(9), 829-841. [CrossRef]
- Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N. Engl J.. Med. 378(14), (2018), 1277-1290. [CrossRef]
Figure 1.
Estimated number of prevalent cases (1-year) as a proportion in 2020, Renal cell carcinoma, both genders, ages 15-74. Data source: GLOBOCAN 2020 Map production: IARC (http://gco.iarc.fr/today) World Health Organization.
Figure 1.
Estimated number of prevalent cases (1-year) as a proportion in 2020, Renal cell carcinoma, both genders, ages 15-74. Data source: GLOBOCAN 2020 Map production: IARC (http://gco.iarc.fr/today) World Health Organization.
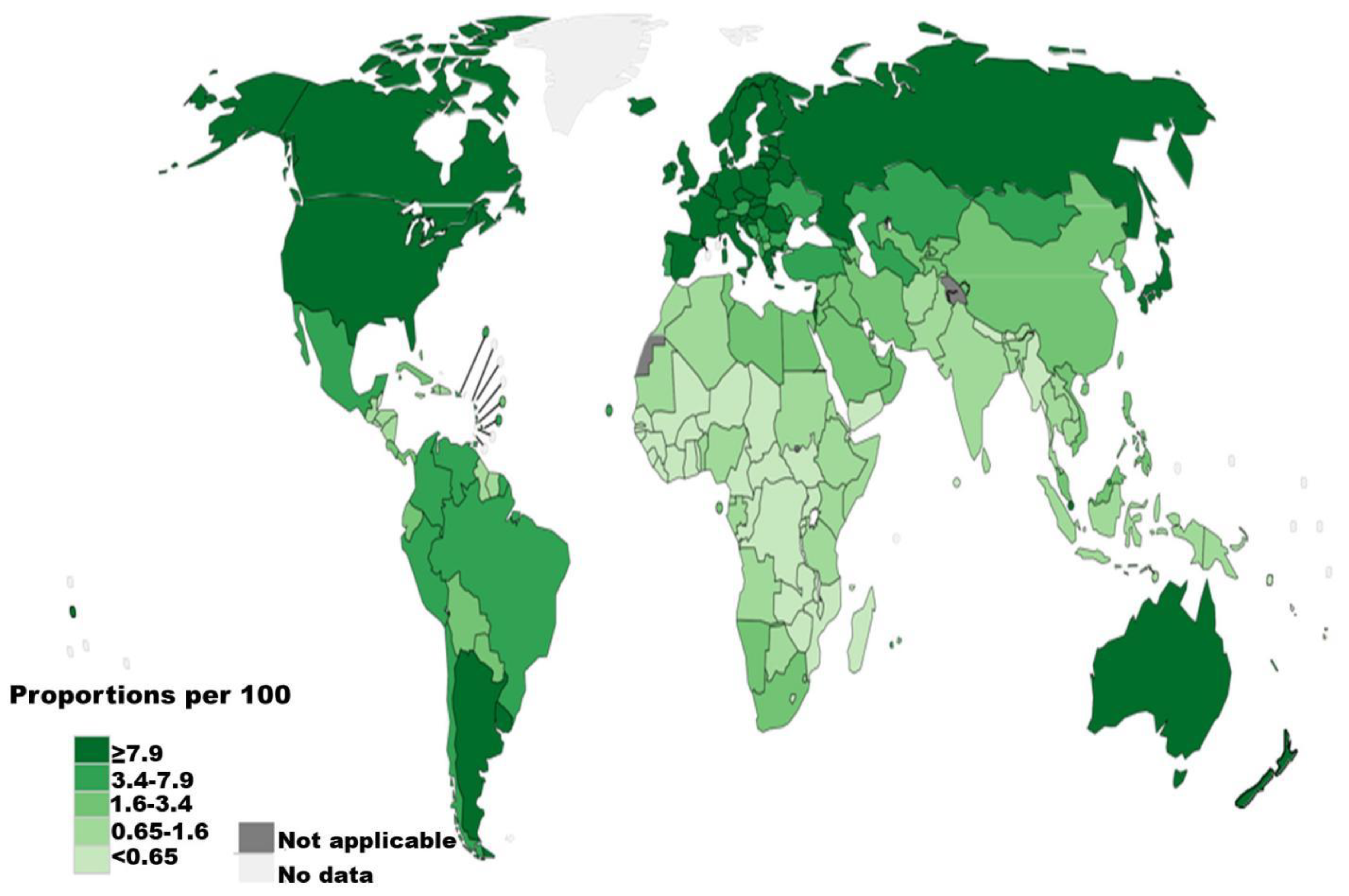
Figure 2.
Estimated age-standardized mortality rates (World) in 2020, Renal cell carcinoma, both gender, ages 15-74. Data source: GLOBOCAN 2020 Map production: IARC (http://gco.iarc.fr/today) World Health Organization.
Figure 2.
Estimated age-standardized mortality rates (World) in 2020, Renal cell carcinoma, both gender, ages 15-74. Data source: GLOBOCAN 2020 Map production: IARC (http://gco.iarc.fr/today) World Health Organization.
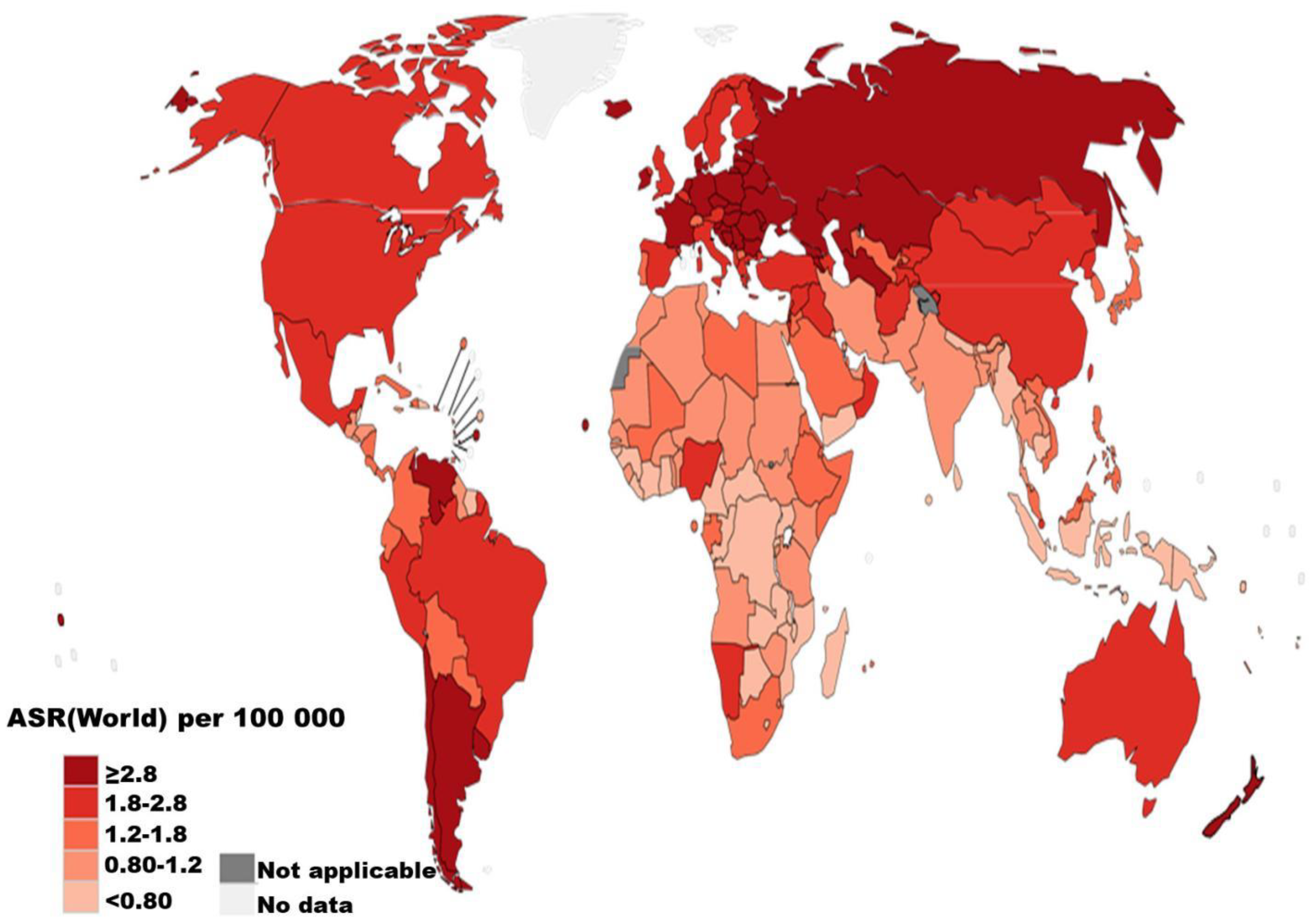
Figure 3.
Estimated number of prevalent cases (1-year) in 2020, Renal cell carcinoma, both genders, ages 15-74 in Eastern and Central Europe countries. Data source: GLOBOCAN 2020 Graph production: Global Cancer Observatory (http://gco.iarc.fr).
Figure 3.
Estimated number of prevalent cases (1-year) in 2020, Renal cell carcinoma, both genders, ages 15-74 in Eastern and Central Europe countries. Data source: GLOBOCAN 2020 Graph production: Global Cancer Observatory (http://gco.iarc.fr).
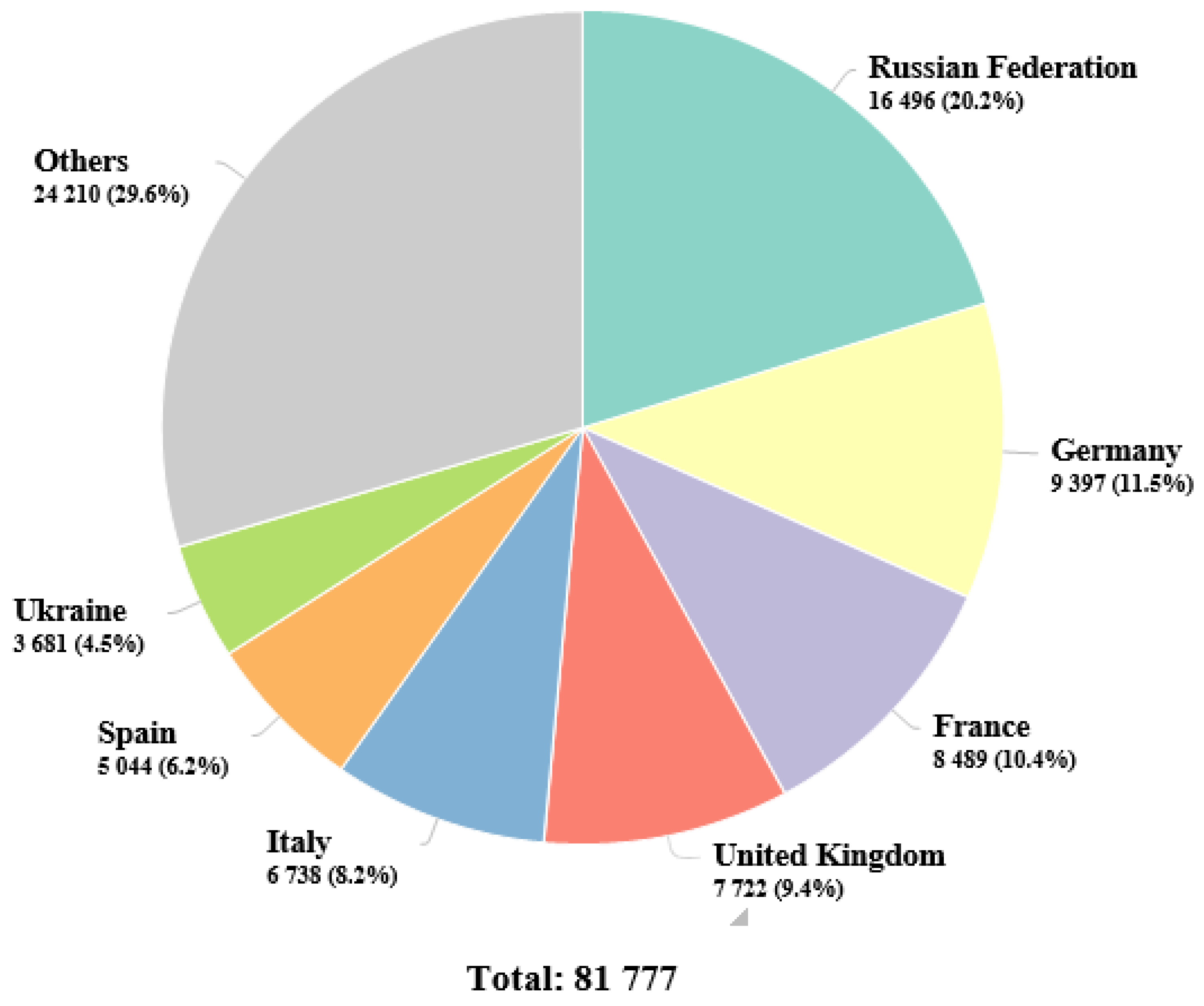
Figure 4.
Estimated number of deaths in 2020,Renal cell carcinoma, both genders, ages 15-74 in Eastern and Central Europe countries. Data source: GLOBOCAN 2020 Graph production: Global Cancer Observatory (http://gco.iarc.fr).
Figure 4.
Estimated number of deaths in 2020,Renal cell carcinoma, both genders, ages 15-74 in Eastern and Central Europe countries. Data source: GLOBOCAN 2020 Graph production: Global Cancer Observatory (http://gco.iarc.fr).
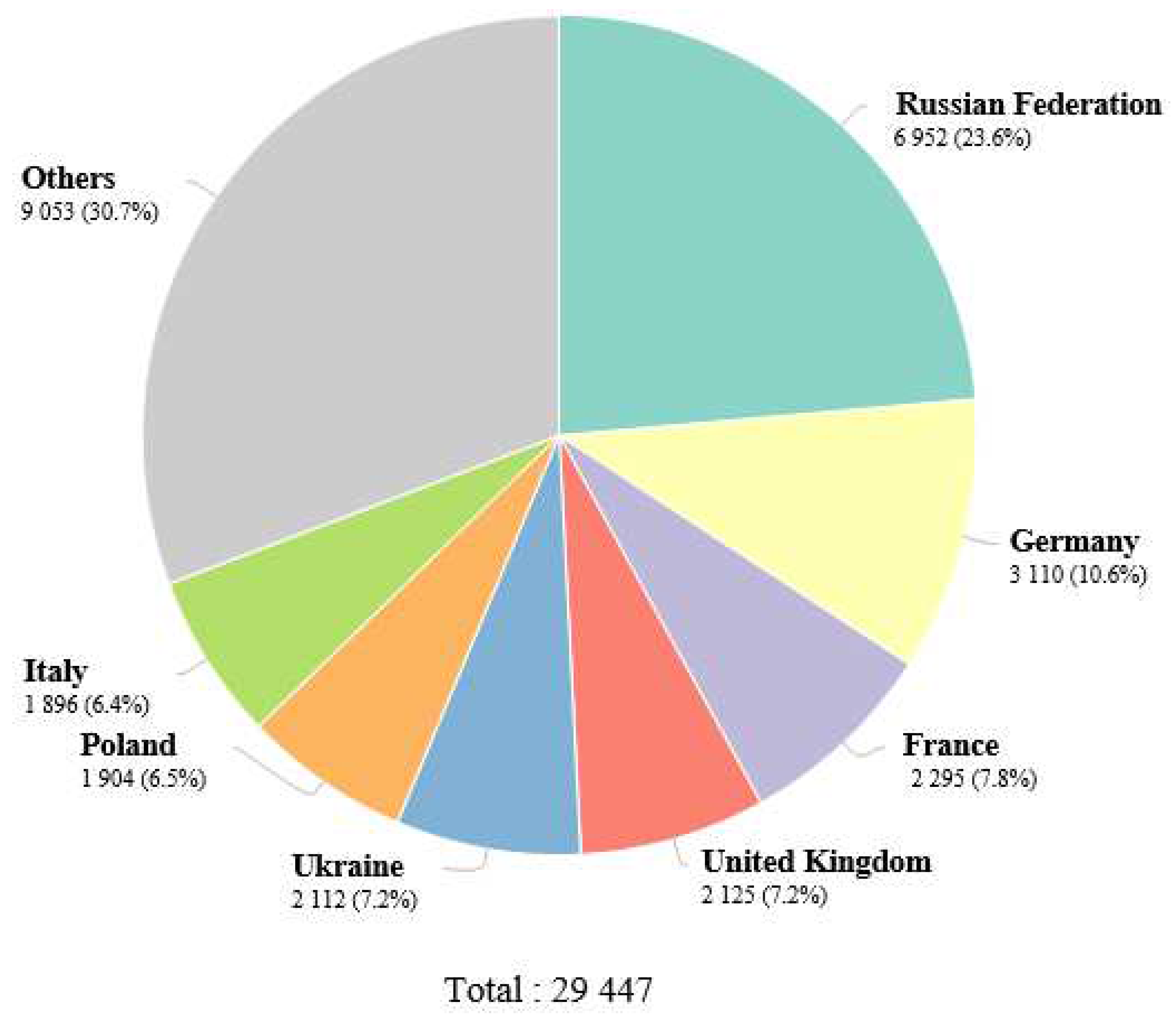

Table 1.
Risk factors kidney cancer.
| Risk factor | Inference | References |
|---|---|---|
| Established risk factor | ||
| Male gender | Positive correlation | [16,18] |
| Age | Positive correlation | [17] |
| Obesity | Positive correlation | [32,33] |
| Smoking | Positive correlation with a dosage response | [17] |
| Hypertension | Positive correlated to a dosage response. Uncertainty exists over how hypertensive drugs affect the risk of kidney cancer. | [34] |
| Renal disease | Renal cancer risk is increased in cases of ACKD, ESRD, and renal transplant. | [35,36] |
| Alcohol | Compared to abstinence, moderate alcohol use has a protective impact. Higher consumption has no added benefits | [37] |
| Family history | Renal cancer risk is increased by having an affected first-degree relative. Renal cancer is also predisposed by a number of rare inherited genetic diseases, such as von Hippel-Lindau, hereditary papillary renal carcinoma, Birt-Hogg-Dubé syndrome, hereditary leiomyomatosis RCC, succinate dehydrogenase RCC, and tuberous sclerosis. |
[38,39] |
| Unestablished risk factor | ||
| Physical activity | Greater exercise is beneficial. | [40] |
| Diabetes | Positive correlation | [41] |
| Occupational exposure | ♦ The IARC believes that there is enough evidence to classify trichloroethylene as a carcinogenic substance that can cause kidney cancer. | [42] |
| ♦ Arsenic and its inorganic compounds, cadmium and its compounds, perfluorooctanoic acid from printing operations, and welding fumes, according to the IARC, have little evidence. | [43] | |
| Analgesic use | Positive correlation with NSAIDs | [44,45,46] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



