
Submitted:
26 October 2023
Posted:
27 October 2023
You are already at the latest version
Abstract
There is no well-defined threshold for intra-operative blood transfusion (BT) in advanced epithelial ovarian cancer (EOC) surgery. We developed a Machine Learning (ML)-driven prediction algorithm to trigger and explain a communication alert for BT based on anticipated peri-operative events irrespective of BT policies. We analysed prospectively collected data from 403 EOC patients who underwent cytoreductive surgery between 2014 and 2019. We calculated the estimated blood volume (EBV) using the formula EBV = weight x 80 and set off 10%EBV as threshold for individual intervention. Based on the known estimated blood loss (EBL) we identified two groups. We employed Receiver operating characteristic (ROC) curves for performance metrics. The model performance for the above threshold prediction was satisfactory (AUC 0.823, 95% CI 0.76-0.88). The top feature commonly shared between interrogators was operative time (OT). Intra-operative blood loss of at least 10%EBV was associated with OT>250 minutes, primary surgery, serous histology, performance status 0, R2 resection and surgical complexity score >4. Large bowel resection, stoma formation, ileocecal resection/right hemicolectomy, mesenteric resection, bladder and upper abdominal peritonectomy were amongst sub-procedures clearly associated with increased intervention risk. Precise prediction of blood requirements is not possible unless a rough estimate of OT is known in advance.
Keywords:
epithelial ovarian cancer
; complete cytoreduction
; estimated blood loss
; estimated blood volume
; blood transfusion
; intra-operative mapping
; machine learning
; explainable artificial intelligence
1. Introduction
Institutional transfusion protocols are not universal, and a variety of transfusion policies may exist across participating institutions. The recently published European Society of Gynaecological Oncology (ESGO) guidelines for the peri-operative management of advanced epithelial ovarian cancer (EOC) patients clearly stated the absence of a well-defined threshold for BT in cytoreductive surgery [1]. Indeed, since many patients will require adjuvant chemotherapy, more liberal transfusion thresholds may be considered. Equally, the BT requirements have long been debated because they are not without risk [2]. Intra-operative decisions are critical in the surgical management of advanced EOC. In such a dynamic theatre environment, harmonic coordination amongst team members including surgeons, anaesthetists and theatre staff can lead to procedural success. Surgical decision- making is layered upon situational awareness and the impact of human factors [3]. While clinical judgments are enhanced over years of training, risk prediction tools still provide the opportunity to augment decision-making. Nevertheless, traditional models fall short to address the complex interactions amongst discrete prediction variables. Machine Learning- based prediction tools can potentially rise above the peak of inflated expectations [4]. Identifying the optimal BT threshold for patients undergoing cytoreduction for advanced EOC becomes crucial, considering the potential risks associated with the surgery.
We hypothesized that pre-operative and intra-operative risk factors for planned cytoreductive procedures can help predict anticipated blood requirements, use of haemostatic sealants and, subsequently anaesthetic interventions in the peri-operative period. We aimed to devise an ML-driven algorithm for transfusion prediction that could trigger a BT communication alert based on anticipated intra-operative events.
2. Methods
We analyzed prospectively collected data from 560 patients with advanced epithelial ovarian cancer (EOC) who underwent cytoreductive surgery at a UK tertiary center between January 2014 and December 2019. The internally developed database was integrated with the Electronic Health Records (EHRs). Institutional research ethics board approval was obtained through the Leeds Teaching Hospitals Trust (MO20/133163/18.06.20), and informed written consent was obtained. The study was added to the UMIN/CTR Trial Registry (UMIN000049480). Surgical management was agreed at the weekly central MDT meeting prior to patient pre-operative review. The cohort has been previously described [5]. Exclusion criteria included patients aged < 18 years; those with non-epithelial histology; synchronous primary malignancy; those undergoing secondary cytoreduction for recurrent disease. We also excluded those with pre-operative anaemia (defined as a haemoglobin level < 120 g/dl) and confirmed coagulopathy (by reviewing medical history or routinely requested coagulation results). The intra-operative fluid protocol consisted of both maintenance therapy (1 mL/kg/h of crystalloid) and replacement of blood loss (1 mL of crystalloid for each mL of directly measured blood loss). If necessary, vasoactive agents were titrated to obtain a mean blood pressure >65 mmHg. The EBL was estimated by subtracting the intra-operative fluid losses suctioned through suctioned drains into the surgical canister from the total blood volume contained in the surgical canister at the end of the procedure and empirically adding the blood loss on the required surgical gauzes. The dataset included the following features: Pre-operative features: age, Eastern Co-operative Oncology Group (ECOG) performance status (PS), histology type (serous and non-serous), grade (low and high), stage (FIGO 3 or 4), and pre-treatment and pre-surgery CA-125. Operative/tumor factors: timing of surgery (PDS or IDS, operative time (OT), estimated blood loss (EBL), site and size of main disease bulk, Peritoneal Carcinomatosis Index (PCI) [6], intra-operative mapping of ovarian cancer (IMO) [7], Surgical Complexity Score (SCS) [8], and residual disease. Residual disease was documented by a comprehensive visual assessment of all the abdominopelvic regions. Human factors: Age of consultant surgeon, and years of experience. Surgical sub-procedures: We employed an adaptation of the structured ESGO Ovarian Cancer Operative Report following the publication of quality indicators for ovarian cancer surgery [9]. This provided detailed information on the patterns of tumor dissemination (https://guidelines.esgo.org/, accessed on 10 Jun 2023). Descriptive statistics were displayed by frequency and percentages for binary and categorical variables and by means and standard deviation (SD) or medians (with lower or upper quartiles for continuous variables). The t test for continuous variables and the Chi- square test for categorical variables were performed. The Fischer’s exact tests were used for binary variables. Statistical significance was set at p < 0.05. Overall survival was analyzed using the Kaplan–Meier and the Mantel–Cox log-rank tests for comparison.
We employed the eXtreme Gradient Boosting (XGBoost) algorithm to model the features [10]. This boosts the performance of weak learning algorithms by combining all the generated hypotheses into a single hypothesis. We investigated the combined effect of eight parameters to maximize model performance by evaluating a grid of 7680 combinations of values using Scikit-learn’s GridSearchCV function. In the absence of standardized definitions for intra-operative bleeding, the study consisted of a concept phase, in which we calculated the estimated blood volume (EBV) using the formula EBV= weight x 80 and set off 10%EBV as threshold for individual intervention [11]. The 10% EBV threshold was used to formulate a binary prediction classification problem. Based on the known EBL, we identified two subgroups. The dataset was split into training and test cohorts (70%:30% ratio). There was no significant difference (p > 0.20) between the two cohorts, with respect to all variables. A five-fold stratified cross-validation (CV) was performed and imbalance was overcome by creating stratified folds to ensure equal distribution between both above and below threshold groups. The CV was iterated 100 times to decrease both variance and bias, hence creating and evaluating 500 models with each round. Model performance was assessed by measuring the total area under the receiver-operating curve (AUC). Receiver operating characteristic (ROC) and Precision-Recall curves and state-of-art scores were used for performance metrics. We used the artificial intelligence SHapley Additive exPlanations (SHAP) framework to explain the cohort-level risk estimates to define novel surgical risk phenotypes. This methodology enhances interpretability by explaining how much the presence of a feature contributes to the model’s overall prediction [12]. To demonstrate the value of the model prediction, we produced (a) SHAP summary plots for the global (cohort) explanation of the results; (b) SHAP dependence plots of the critical risk features pertinent to the prediction. The Python’s SciPy library (version 2.7) (Python Software Foundation) Python Language Reference, version 2.7. available at http://www.python.org) was used for the analyses.
3. Results
Initially, 560 EOC patients were enrolled in the study. One hundred seventeen patients and 26 patients were excluded due to pre-operative anaemia and abnormal coagulation system, respectively. Four patients were further excluded: one patient with a synchronous primary malignancy and three patients who underwent emergency cytoreduction with no intention to treat. Ten patient cases were omitted due to incomplete data. Finally, 403 EOC patients participated in the final analysis (Table 1). The patients were followed-up until April 2022. The mean age of patients in the entire cohort was 65.31 + 11.2 years. This was comparable between the train and test sets; 63.2 ± 11, 64,6 ± 12, respectively (p:NS). Histology, PS, tumour grade and stage, timing of surgery, residual disease, SCS, IMO score, PCI, pre-surgery Ca 125 and occurrence of ascites were similar in the training and test sets (P:NS). All but pre-treatment Ca 125 and age were statistically significant between the < and > 10%EBV groups. The descriptive of surgical sub-procedures has been previously published [13].
The model performance for the above threshold prediction was moderate-to-high (AUC 0.82, 95% CI 0.78-0.86; AP 0.72, 95% CI 0.67-0.76) (Figure 1). To promote reproducibility, the optimal set of model parameters are available upon reasonable request.
The importance of features in this model based on SHAP values is shown in Figure 2. The order of the features reflects their weighted importance, i.e., the sum of the SHAP value magnitudes across all the samples. Each point on the summary plot is a Shapley value for a feature. The position on the y-axis is determined by the feature and on the x-axis by the Shapley value. The color represents the value of the feature from low (blue =< 10% EBV) to high (red => 10% EBV). The top feature commonly shared between both interrogators was operative time (OT). The top-5 list of important features included pre-treatment CA125, logCa125/PCI, a marker of biological tumor aggressiveness, followed by the SCS and the size of the largest disease bulk. Long tails were observed mainly for operative time and size of the largest tumor bulk, which suggests these features can be equally important for specific if not all patients (local explainability).
The SHAP dependence plots reveal the impact of each feature on the prediction by plotting the value of the feature on the x-axis and the SHAP feature value on the y-axis. While Figure 3A fails to show a clear inflection point, inflection points are demonstrated for high grade (Figure 3B), PS > 1 (Figure 3C) and serous histology (Figure 3D). When overall SHAP values are positive, the likelihood for BT intervention is higher. For OT < 150 min, the overall SHAP values are negative, which makes BT intervention unlikely (Figure 4A). Then, there is no clear inflection point for OT ranging between 150 min and 250 min. Subsequently, for OT > 250 min, it becomes more likely to administer BT. If PCI is selected as a feature to determine its impact, an increasing PCI up to eight results in a lower likelihood for BT (Figure 4D). Similarly, the inflection points for IMO score and SCS are four and three, respectively. Clearly, delayed surgery and R0 resection do not favor BT intervention (Figure 4B and 4F). From the list of surgical sub-procedures clearly reflecting radical or ultra-radical cytoreductive efforts, an intra-operative blood loss of at least 10%EBV was associated with the performance of (A) stoma formation (Figure 5A), bladder peritonectomy (Figure 5B), para-aortic lymphadenectomy (Figure 5C), ileo-caecal resection/right hemicolectomy (Figure 5D), mesenteric resection (Figure 5E), upper abdominal peritonectomy (Figure 5F), and large bowel resection (Figure 5G).
The 5-year OS for the entire cohort was 61 months (95% CI 58-63). The median OS was 60 months for the <10%EBV group (95% CI 58–61) and 61 months (95% CI 60–63) for the >10%EBV group (p:NS). In the predicted >10%EBV group, only 10% (n= 23) received BT (Figure 6).
4. Discussion
We developed and explained an ensemble ML algorithm to predict intra-operative interventional risk for advanced EOC cytoreduction (Figure 7). Equally, we quantified the contribution of independent patient- disease- and operation-specific features to intra- operative blood loss to understand its impact on surgery. While we urge for standardized definitions of intra-operative bleeding in surgical practice, we conceptually identified a threshold for potential personalized intervention, irrespective of BT policies. This EBV- and EBL-based simple tool could improve the language and communication surrounding blood loss. Including percentage EBV triggers at the surgical safety list can potentially minimize the requirement for further interventions. Such mental preparation can be an important factor for surgical success [14]. To our knowledge, this is the first attempt to identify an objective threshold that could proactively result in interventions inclusive of BT or usage of haemostatic agents at EOC cytoreductive surgery. The study explains how EBL can be divided into a single contributing component, which is the surgical time. As such, the main study finding is that precise prediction of blood requirements or strategies to address haemostasis is not possible unless a rough estimate of OT is known in advance. An inflection point was not identified but OT >250 min clearly increases the risk for BT administration. Blood transfusion and OT are inter-related events prompting for quality assurance of all intra-operative events to be the focus of quality assurance in the future [15]. Interestingly, the top-5 list of important features included not just markers of surgical aggressiveness but also inherent tumor biology, such as the pre-treatment Ca125 or the Ca125/PCI ratio. This information is clinically relevant to be used in studies investigating haemostatic agents [11]. Previous studies identified age and low baseline hemoglobin level as risk factors for transfusion in this population [16,17]. Malignant ascites >500 mL can be a risk factor as it implies increased fluid demands and substantial alterations in circulatory blood flow during cancer surgery [2], but this was not shown in our study. Lately, we read with interest the development of a new tool that can predict the need for BT during or after primary debulking surgery in EOC patients. The tool, called the “BLOODS score” was developed to help identify patients who may benefit from pre-operative planning and blood-saving techniques [18]. The score was created using data from a similar practice setting. In a cohort totaling 1289 patients, and for a median estimated blood loss of 650 cc, the seven features associated with BT included: the American Society of Anesthesiologists physical score of 3 or higher, the pre-operative serum albumin level of 3.5 g/dL or lower, presence of ascites, pre-operative CA-125 level of 600 U/mL or higher, carcinomatosis, moderate or high SCS compared to low SCS, (h), pre-operative creatinine level greater than 0.90 mg/dL , and upper abdominal disease of 1 cm or greater. The features were assigned a score of 1 if present. The sum of the BLOODS score corresponded to the need for BT. The authors claim that a BLOODS score of 3 or higher is estimated to identify 80% of patients who require a BT, including 85% of patients who need a transfusion intra-operatively and 78% who need one post-operatively. Notably, the rate of full clearance was just above 50%. In our study, we clearly demonstrated that the risk for BT is associated with primary surgery- owing to a complete cytoreduction rate of 67.3%- too. It is likely that with expansion of our surgical cohort, we may encounter similar results in the future. At our tertiary center, consideration of patients for cytoreductive surgery is based on pre- operative evaluation with contrast-enhanced cross-sectional imaging but, more importantly stringent selection through MDT discussion. Surgeons are requested to estimate the likelihood of extensive cytoreduction and pre-operatively anticipate the input values for several intra-operative variables. We are not surprised why OT was the single most important contributor to the threshold risk for potential intervention. In theory, the duration of surgery can vary depending on the extent of disease spread, the surgical effort, the experience of the surgical team in addition to the patient’s overall health. Pre-operative prediction of the duration of the procedure is one of the critical elements of theatre scheduling, and one needs to know what surgical effort needs exerting at the beginning of surgery; this can then facilitate scheduling or anticipate needs for resources. Maximizing operating room utilization relies on accurate estimates of surgical control time. As the number of EOC diagnoses is rapidly increasing, effective management of theatre time is required. Anecdotal evidence suggests that surgeons grossly underestimate predicted surgical time [19]. Herein, we provided clear evidence of several surgical sub-procedures, indirectly linked to procedural time, which are associated with higher risk for intra-operative intervention. Nevertheless, extensive surgical approach is associated with increased blood loss and potentially higher peri-operative complications [20]. As studies continue to share knowledge about the optimal duration of surgical procedures [21], another study is currently underway to assign optimal procedural times from knowledge retrieved from operative notes using natural language processing (data not shown). This niche may have potential implications: to improve information delivery to surgeons so that careful planning is considered in reducing complications; secondly, it will improve patient counseling or discussion about extent of surgery or alternative therapeutic options. To date, most relevant studies have devised models to identify those patients who are at lowest risk and may need less pre-operative BT preparation [22,23]. This information can be used to develop EOC-specific institutional guidelines to predict crossmatch and transfusion needs, and promote the sensible use of blood products and cost savings. Owing to the high prevalence of BT in this population, this information can be of added value for accurate surgical planning and pre-operative optimization of potentially modifiable factors. We acknowledge that initial intra-operative anaesthetic interventions do not always involve transfusions of blood products. Goal-directed haemodynamic algorithms are routinely used to optimize stroke volume and provide better systemic stability and reduced need for fresh- frozen plasma [24]. Efforts to promote sensible use of intra-operative BT also include acute normovolemic haemodilution without increasing peri-operative complications [25]. Other strategies for “bloodless” surgery have been recently described [26,27]. There is insufficient evidence to recommend the routine use of tranexamic acid for reducing blood loss in women undergoing cytoreductive surgery for advanced EOC, as only limited data are available from a single, low quality RCT [28]. Optimizing intra-operative fluid management may improve short-term patient outcomes [29]. Notably, the intra-operative BT requirements are significantly lower in prehabilitation groups of EOC candidates to cytoreductive surgery [28]. The impact of BT on EOC survival has been uncertain until the ancillary analysis of the EORTC 55971 phase III trial, which concluded that BT does not negatively impact progression-free survival or overall survival. Nevertheless, it was associated with increased peri-operative morbidity without improvements in quality of life [30]. The case for overall survival was presented in our study albeit only 10% of patients in the >10%EBV group (rule of thumb) received BT peri-operatively. Intra-operative bleeding is the most relevant finding to surgical complications. Surgical time may not be related to complications, which are significantly related to delayed chemotherapy [31]. The strengths of this study included a large, population-based database inclusive of patient- and cancer-specific, but also surgical features. We cannot infer causality in variables that predicted the primary outcome. The use of an ML-based algorithm reliably predicted the risk for potential intervention. We used explainability AI to unveil the “black box” of ML, which is critical to overcome any resilience for clinical implementation. In gynaecological oncology, translatability of models is important when it comes to endpoint selections, due to the significant variability in model development [32]. Should another threshold be used, the results would have been different. Indeed, we tested the 20%EBV cut off, but the results were poor due to group imbalance. Despite the rigorous 5-fold internal validation, this single-center study design cannot provide real-world risk estimation for experienced centers. The top predictor could only be extracted from the operative details, which limits pre-operative counseling. Prospective evaluation may allow for model integration into EHR.
5. Conclusion
Our study identified the sole risk factor of weighted importance for intra-operative bleeding in EOC patients undergoing cytoreductive surgery that would require BT or use of surgical adjuncts. Provided that patients are not anaemic and have an intact anticoagulation system, the occurrence of intra-operative blood loss of at least 10%EBV was mainly associated with operative time followed by pre-treatment CA125, and a poor surgical outcome. The ROC curves indicated that by integrating these features into a single ML-based prediction system, the XGBoost reliably predicted intra-operative blood loss and anticipated requirements.
Such information will not only prevent serious post-operative mortality and morbidity but also avoid unnecessary waste of precious blood resources.
Author Contributions
Conceptualization, A.L.; Data curation, A.L., R.J., Y.T. and D.D.J.; Software, A.L., E.K. and M.E.M.; Supervision, A.T., D.N. and D.D.J.; Writing—original draft, A.L.; Writing and editing, E.K., R.J., S.M., T.B., R.H. and G.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the LTHT Institutional Review Board (MO20/133163/ 18.06.20).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | Linear dichroism |
References
- Fotopoulou, C.; Planchamp, F.; Aytulu, T.; Chiva, L.; Cina, A.; Ergönül, Ö.; Fagotti, A.; Haidopoulos, D.; Hasenburg, A.; Hughes, C.; others. European Society of Gynaecological Oncology guidelines for the peri-operative management of advanced ovarian cancer patients undergoing debulking surgery. International Journal of Gynecologic Cancer 2021, 31. [Google Scholar] [CrossRef] [PubMed]
- Manning-Geist, B.L.; Alimena, S.; Del Carmen, M.G.; Goodman, A.; Clark, R.M.; Growdon, W.B.; Horowitz, N.S.; Berkowitz, R.S.; Muto, M.G.; Worley Jr, M.J. Infection, thrombosis, and oncologic outcome after interval debulking surgery: does perioperative blood transfusion matter? Gynecologic Oncology 2019, 153, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Laios, A.; Kalampokis, E.; Johnson, R.; Munot, S.; Thangavelu, A.; Hutson, R.; Broadhead, T.; Theophilou, G.; Leach, C.; Nugent, D.; others. Factors predicting surgical effort using explainable artificial intelligence in advanced stage epithelial ovarian cancer. Cancers 2022, 14, 3447. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Asch, S.M. Machine learning and prediction in medicine—beyond the peak of inflated expectations. The New England journal of medicine 2017, 376, 2507. [Google Scholar] [CrossRef] [PubMed]
- Laios, A.; Kalampokis, E.; Johnson, R.; Thangavelu, A.; Tarabanis, C.; Nugent, D.; De Jong, D. Explainable artificial intelligence for prediction of complete surgical cytoreduction in advanced-stage epithelial ovarian cancer. Journal of personalized medicine 2022, 12, 607. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Peritoneal carcinomatosis: principles of management, 1996; pp. 359–374. [Google Scholar]
- Sehouli, J.; Könsgen, D.; Mustea, A.; Oskay-Özcelik, G.; Katsares, I.; Weidemann, H.; Lichtenegger, W. „IMO”-Intraoperatives Mapping des Ovarialkarzinoms. Zentralblatt für Gynäkologie 2003, 125, 129–135. [Google Scholar] [PubMed]
- Aletti, G.D.; Dowdy, S.C.; Podratz, K.C.; Cliby, W.A. Relationship among surgical complexity, short-term morbidity, and overall survival in primary surgery for advanced ovarian cancer. American journal of obstetrics and gynecology 2007, 197, 676–e1. [Google Scholar] [CrossRef]
- Querleu, D.; Planchamp, F.; Chiva, L.; Fotopoulou, C.; Barton, D.; Cibula, D.; Aletti, G.; Carinelli, S.; Creutzberg, C.; Davidson, B.; others. European Society of Gynaecologic Oncology quality indicators for advanced ovarian cancer surgery. International Journal of Gynecologic Cancer 2016, 26. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.H. Greedy function approximation: a gradient boosting machine. Annals of statistics, 2001; pp. 1189–1232. [Google Scholar]
- Lewis, K.M.; Li, Q.; Jones, D.S.; Corrales, J.D.; Du, H.; Spiess, P.E.; Menzo, E.L.; DeAnda Jr, A. Development and validation of an intraoperative bleeding severity scale for use in clinical studies of hemostatic agents. Surgery 2017, 161, 771–781. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Erion, G.; Chen, H.; DeGrave, A.; Prutkin, J.M.; Nair, B.; Katz, R.; Himmelfarb, J.; Bansal, N.; Lee, S.I. From local explanations to global understanding with explainable AI for trees. Nature machine intelligence 2020, 2, 56–67. [Google Scholar] [CrossRef]
- Laios, A.; Kalampokis, E.; Johnson, R.; Munot, S.; Thangavelu, A.; Hutson, R.; Broadhead, T.; Theophilou, G.; Nugent, D.; De Jong, D. Development of a Novel Intra-Operative Score to Record Diseases’ Anatomic Fingerprints (ANAFI Score) for the Prediction of Complete Cytoreduction in Advanced-Stage Ovarian Cancer by Using Machine Learning and Explainable Artificial Intelligence. Cancers 2023, 15, 966. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.; Orlick, T.; Letts, M. Mental readiness in surgeons and its links to performance excellence in surgery. Journal of Pediatric Orthopaedics 1995, 15, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.; Spooner, S.; Horne, J.; Chainrai, M.; Runau, F.; Bourne, T.; Moss, E.L.; Davies, Q.; Chattopadhyay, S.; Bharathan, R. Peri-operative variables associated with prolonged intensive care stay following cytoreductive surgery for ovarian cancer. Anticancer Research 2021, 41, 3059–3065. [Google Scholar] [CrossRef] [PubMed]
- Heddens, D.; Alberts, D.S.; Hannigan, E.V.; Williams, S.D.; Garcia, D.; Roe, D.J.; Bell, J.; Alvarez, R.D. Prediction of the need for red cell transfusion in newly diagnosed ovarian cancer patients undergoing platinum-based treatment. Gynecologic oncology 2002, 86, 239–243. [Google Scholar] [CrossRef]
- Pinheiro de Almeida, J.; Vincent, J.L.; Barbosa Gomes Galas, F.R.; Pinto Marinho de Almeida, E.; Fukushima, J.T.; Osawa, E.A.; Bergamin, F.; Lee Park, C.; Nakamura, R.E.; Fonseca, S.M.; others. Transfusion requirements in surgical oncology patients: a prospective, randomized controlled trial. Anesthesiology 2015, 122, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Kahn, R.; Boerner, T.; An, A.; Gardner, G.; Roche, K.L.; Sonoda, Y.; Zivanovic, O.; Grisham, R.; Abu-Rustum, N.; Chi, D. A preoperative tool for estimating the risk of blood transfusion over an ovarian cancer debulking surgery (113). Gynecologic Oncology 2022, 166, S74. [Google Scholar] [CrossRef]
- Goel, R.; Kanhere, H.; Trochsler, M. The ‘Surgical Time’: a myth or reality? Surgeons’ prediction of operating time and its effect on theatre scheduling. Australian Health Review 2020, 44, 772–777. [Google Scholar] [CrossRef]
- Eisenkop, S.M.; Friedman, R.L.; Wang, H.J. Complete cytoreductive surgery is feasible and maximizes survival in patients with advanced epithelial ovarian cancer: a prospective study. Gynecologic oncology 1998, 69, 103–108. [Google Scholar] [CrossRef]
- Yitgin, Y.; Altınkaya, N.; Turaliev, N.; Guven, S.; Ergul, R.B.; Boyuk, A.; Verep, S.; Tefik, T.; Karagoz, M.A.; Ibis, M.A.; others. Evaluation of the optimal duration for retrograde intrarenal stone surgery to prevent postoperative complications. Scottish Medical Journal 2022, 67, 121–125. [Google Scholar] [CrossRef]
- Kubi, B.; Nudotor, R.; Fackche, N.; Nizam, W.; Cloyd, J.M.; Grotz, T.E.; Fournier, K.F.; Dineen, S.P.; Powers, B.D.; Veerapong, J.; others. Impact of perioperative blood transfusions on outcomes after hyperthermic intraperitoneal chemotherapy: A propensity-matched analysis. Annals of surgical oncology 2021, 28, 4499–4507. [Google Scholar] [CrossRef]
- Prescott, L.S.; Taylor, J.S.; Lopez-Olivo, M.A.; Munsell, M.F.; VonVille, H.M.; Lairson, D.R.; Bodurka, D.C. How low should we go: a systematic review and meta-analysis of the impact of restrictive red blood cell transfusion strategies in oncology. Cancer treatment reviews 2016, 46, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kietpeerakool, C.; Supoken, A.; Laopaiboon, M.; Lumbiganon, P. Effectiveness of tranexamic acid in reducing blood loss during cytoreductive surgery for advanced ovarian cancer. Cochrane Database of Systematic Reviews 2016. [Google Scholar] [CrossRef]
- Prescott, L.S.; Vergote, I.; Sun, C.C.; Bodurka, D.C.; Coleman, R.L. Transfusion use and effect on progression-free, overall survival, and quality of life in upfront treatment of advanced epithelial ovarian cancer: evaluation of the European Organization for Research and Treatment EORTC-55971 Cohort. International Journal of Gynecologic Cancer 2023, 33. [Google Scholar] [CrossRef] [PubMed]
- Hunsicker, O.; Fotopoulou, C.; Pietzner, K.; Koch, M.; Krannich, A.; Sehouli, J.; Spies, C.; Feldheiser, A. Hemodynamic consequences of malignant ascites in epithelial ovarian cancer surgery: a prospective substudy of a randomized controlled trial. Medicine 2015, 94. [Google Scholar] [CrossRef] [PubMed]
- Tse, A.; Chow, O.; Matar, A.; Alzahrani, N.; Morris, D. Strategies for ‘bloodless’ surgery: the experience of cytoreductive surgery for peritoneal carcinomatosis in Jehovah’s Witnesses. ANZ Journal of Surgery 2020, 90, 1953–1957. [Google Scholar] [CrossRef] [PubMed]
- Miralpeix, E.; Sole-Sedeno, J.M.; Rodriguez-Cosmen, C.; Taus, A.; Muns, M.D.; Fabregó, B.; Mancebo, G. Impact of prehabilitation during neoadjuvant chemotherapy and interval cytoreductive surgery on ovarian cancer patients: a pilot study. World Journal of Surgical Oncology 2022, 20, 46. [Google Scholar] [CrossRef] [PubMed]
- Tanner, E.J.; Filippova, O.T.; Gardner, G.J.; Roche, K.C.L.; Sonoda, Y.; Zivanovic, O.; Fischer, M.; Chi, D.S. A prospective trial of acute normovolemic hemodilution in patients undergoing primary cytoreductive surgery for advanced ovarian cancer. Gynecologic oncology 2018, 151, 433–437. [Google Scholar] [CrossRef]
- Prescott, L.S.; Vergote, I.; Sun, C.C.; Bodurka, D.C.; Coleman, R.L. Transfusion use and effect on progression-free, overall survival, and quality of life in upfront treatment of advanced epithelial ovarian cancer: evaluation of the European Organization for Research and Treatment EORTC-55971 Cohort. International Journal of Gynecologic Cancer 2023, 33. [Google Scholar] [CrossRef]
- Castro, B.G.R.; Dos Reis, R.; Cintra, G.F.; de Assunção Sousa, M.M.; de Andrade Vieira, M.; da Cunha Andrade, C.E.M. Predictive factors for surgical morbidities and adjuvant chemotherapy delay for advanced ovarian cancer patients treated by primary debulking surgery or interval debulking surgery. International Journal of Gynecologic Cancer 2018, 28. [Google Scholar] [CrossRef]
- Sheehy, J.; Rutledge, H.; Acharya, U.R.; Loh, H.W.; Gururajan, R.; Tao, X.; Zhou, X.; Li, Y.; Gurney, T.; Kondalsamy-Chennakesavan, S. Gynecological cancer prognosis using machine learning techniques: A systematic review of last three decades (1990–2022). Artificial Intelligence in Medicine, 2023; p. 102536. [Google Scholar]
Figure 1.
Prediction performance of the XGBoost model for the prediction of the risk of blood transfusion at cytoreductive surgery (A) Receiver Operator Characteristic (ROC) curve (B) Precision-Recall (PR) curve.
Figure 1.
Prediction performance of the XGBoost model for the prediction of the risk of blood transfusion at cytoreductive surgery (A) Receiver Operator Characteristic (ROC) curve (B) Precision-Recall (PR) curve.
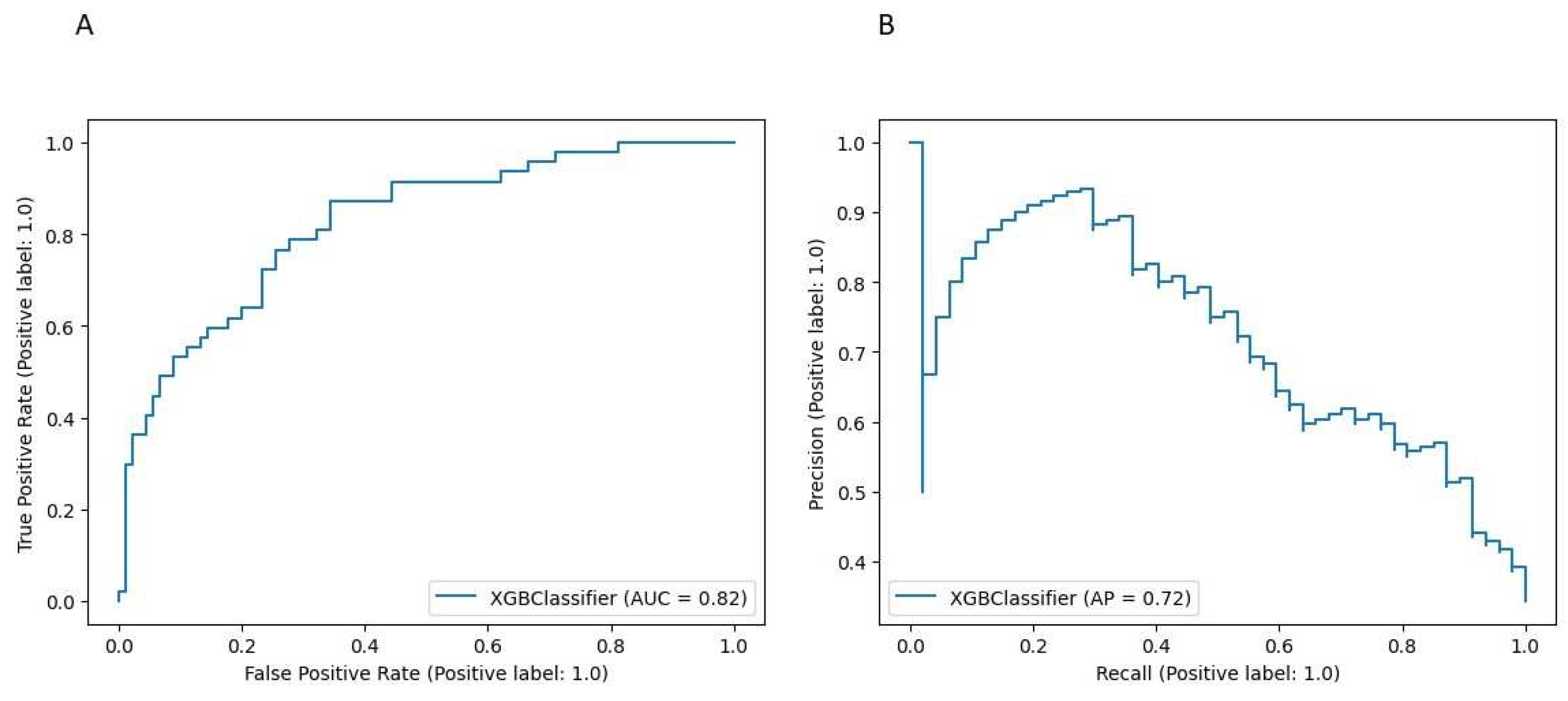
Figure 2.
(A) Summary plot showing a set of feature distribution beeswarm plots for global(threshold) explainability of 10%EBV threshold prediction (B) Feature importance bar plot of their SHAP values. PCI, Peritoneal Carcinomatosis Index;RD, Residual Disease; PDS, Primary Debulking surgery; IDS, Interval Debulking Surgery; PS, Performance Status.
Figure 2.
(A) Summary plot showing a set of feature distribution beeswarm plots for global(threshold) explainability of 10%EBV threshold prediction (B) Feature importance bar plot of their SHAP values. PCI, Peritoneal Carcinomatosis Index;RD, Residual Disease; PDS, Primary Debulking surgery; IDS, Interval Debulking Surgery; PS, Performance Status.
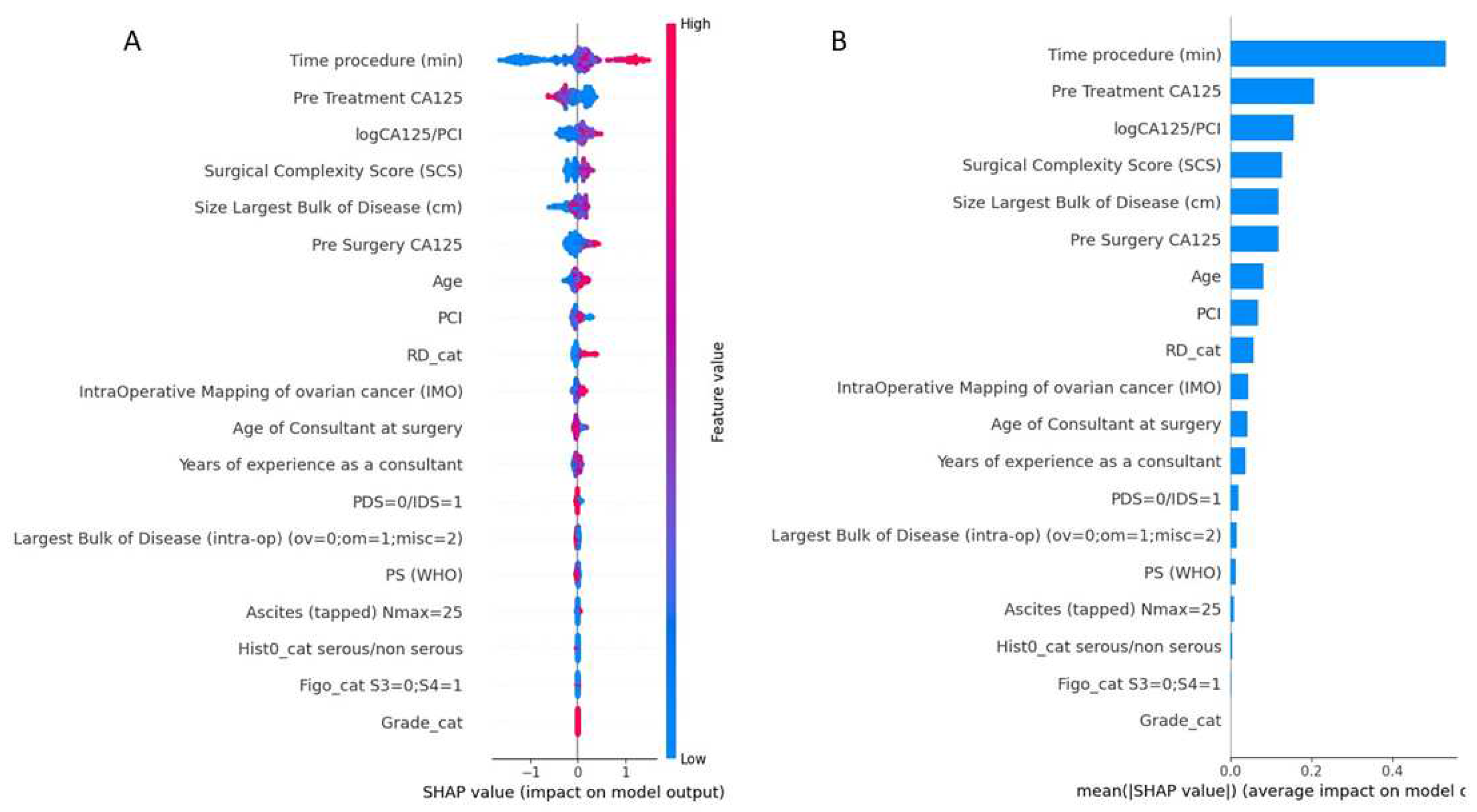
Figure 3.
Examples of SHAP value Dependence plots for global explainability features showing the impact of each feature value in the risk prediction of blood transfusion at cytoreductive surgery. (A) Pre-treatment (B) Grade (C) PS (D) Serous vs non-serous pathology. PS, Performance Status
Figure 3.
Examples of SHAP value Dependence plots for global explainability features showing the impact of each feature value in the risk prediction of blood transfusion at cytoreductive surgery. (A) Pre-treatment (B) Grade (C) PS (D) Serous vs non-serous pathology. PS, Performance Status
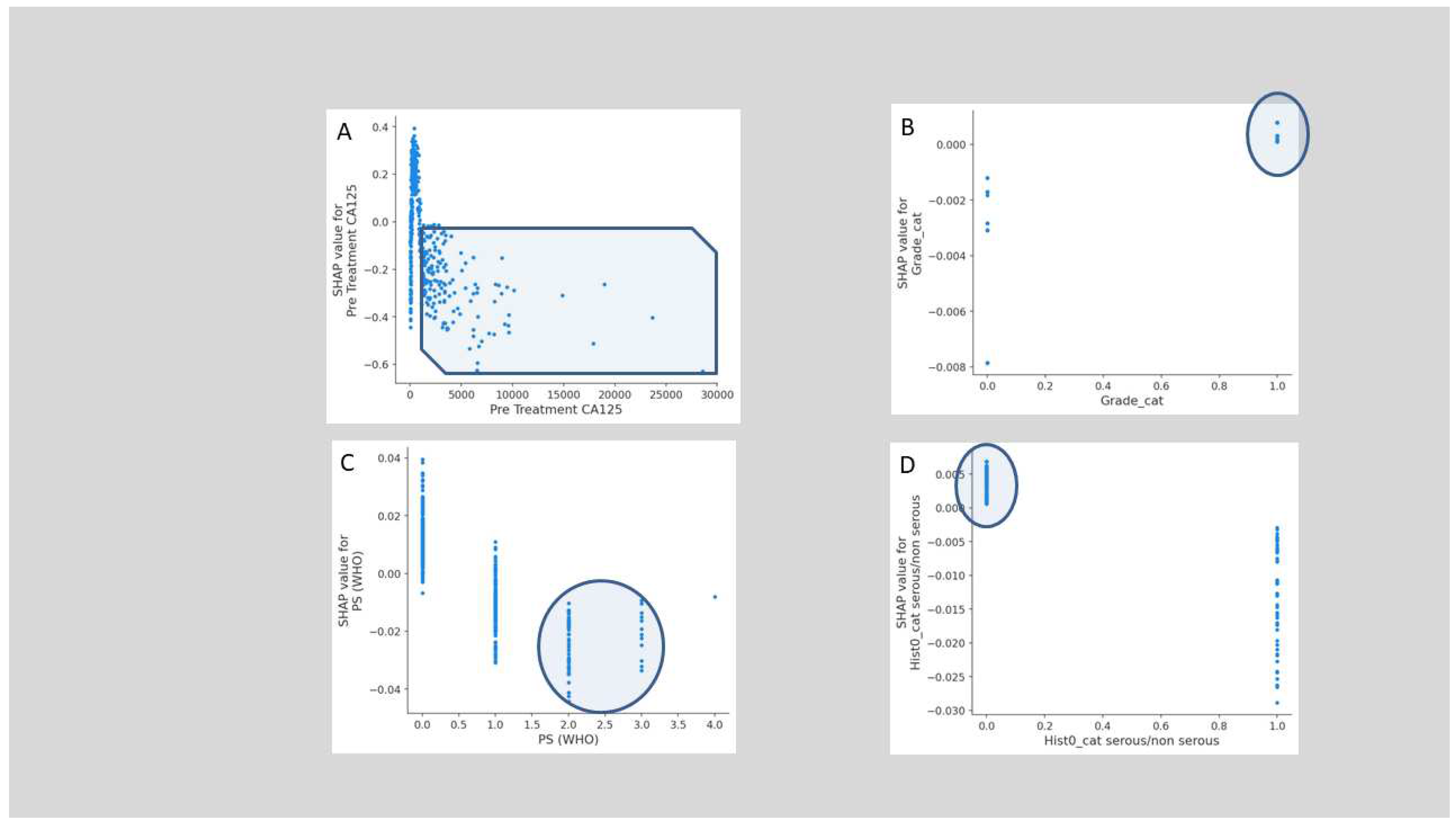
Figure 4.
Examples of SHAP value Dependence plots for global explainability features showing the impact of each feature value in the risk prediction of blood transfusion at cytoreductive surgery. (A) Operative time (B) timing of cytoreduction (C) Intra-operative mapping of ovarian cancer score (D) Peritoneal Carcinomatosis Index (E) Surgical Complexity Score (F) Residual disease.
Figure 4.
Examples of SHAP value Dependence plots for global explainability features showing the impact of each feature value in the risk prediction of blood transfusion at cytoreductive surgery. (A) Operative time (B) timing of cytoreduction (C) Intra-operative mapping of ovarian cancer score (D) Peritoneal Carcinomatosis Index (E) Surgical Complexity Score (F) Residual disease.
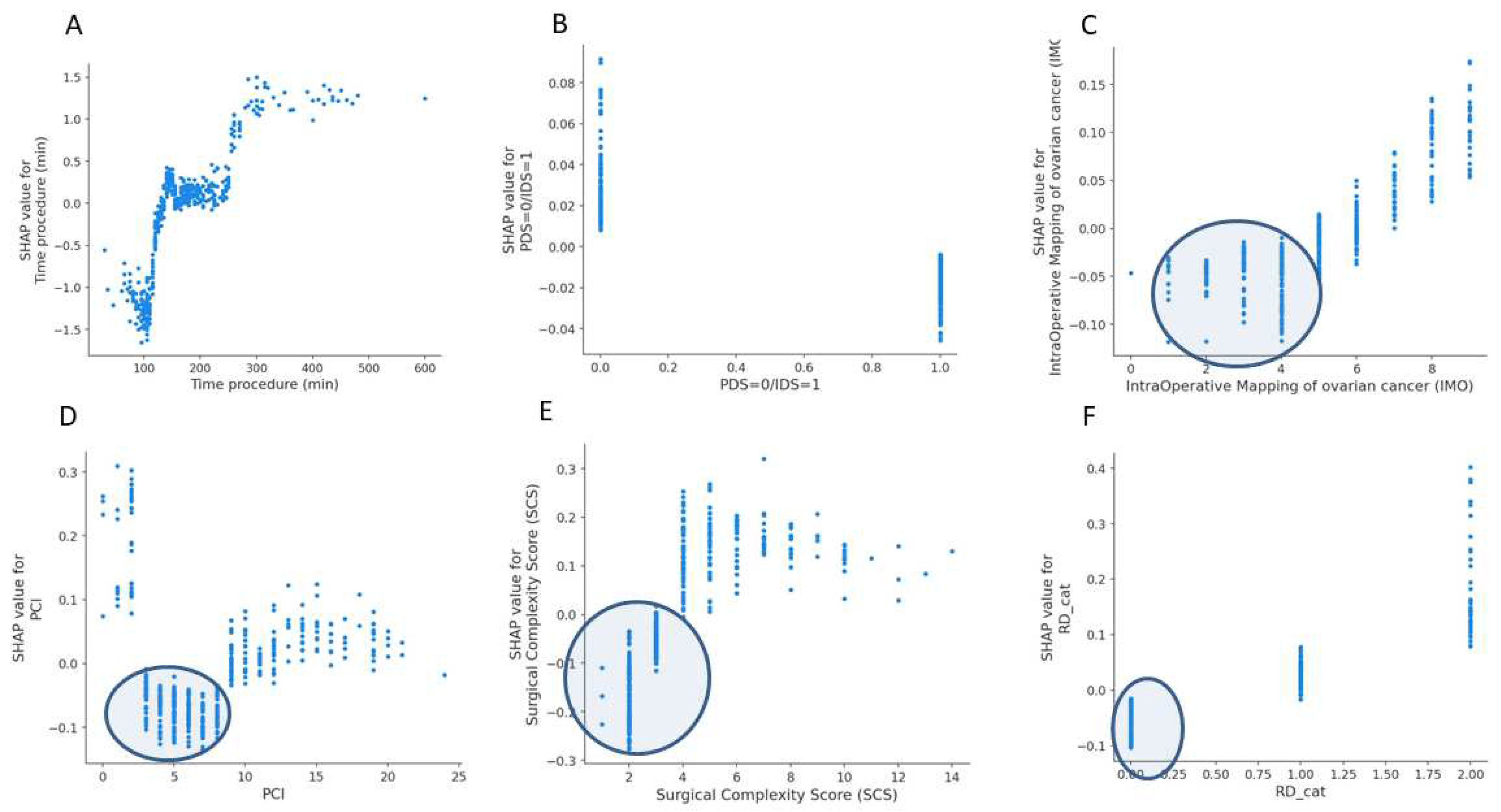
Figure 5.
Examples of SHAP value Dependence plots for global explainability features showing the impact of surgical sub-procedures in the risk prediction of blood transfusion at cytoreductive surgery. The important features include (A) stoma formation (B) Bladder peritonectomy (C) Para-aortic lymphadenectomy (D) Ileo-caecal resection/right hemicolectomy (E) Mesenteric resection (F) Upper abdominal peritonectomy (G) Large bowel resection (H) Pelvic lymph node dissection. LND,lymph node dissection.
Figure 5.
Examples of SHAP value Dependence plots for global explainability features showing the impact of surgical sub-procedures in the risk prediction of blood transfusion at cytoreductive surgery. The important features include (A) stoma formation (B) Bladder peritonectomy (C) Para-aortic lymphadenectomy (D) Ileo-caecal resection/right hemicolectomy (E) Mesenteric resection (F) Upper abdominal peritonectomy (G) Large bowel resection (H) Pelvic lymph node dissection. LND,lymph node dissection.
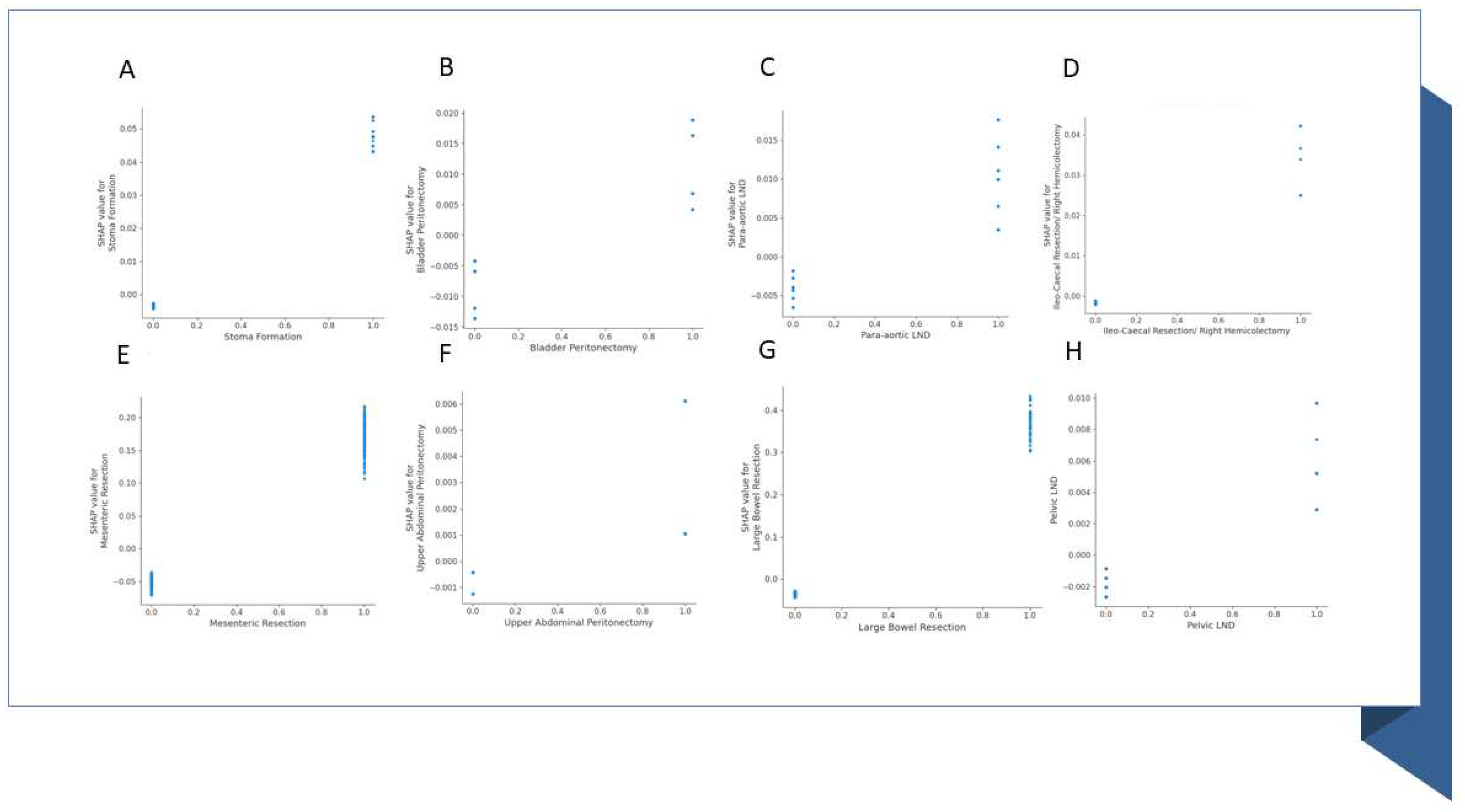
Figure 6.
Kaplan Meier (KM) curve showing overall survivals between the <10%EBV and >10%EBV threshold cohorts of women undergoing cytoreduction for advanced epithelial ovarian cancer. No statistical significance was demonstrated.
Figure 6.
Kaplan Meier (KM) curve showing overall survivals between the <10%EBV and >10%EBV threshold cohorts of women undergoing cytoreduction for advanced epithelial ovarian cancer. No statistical significance was demonstrated.
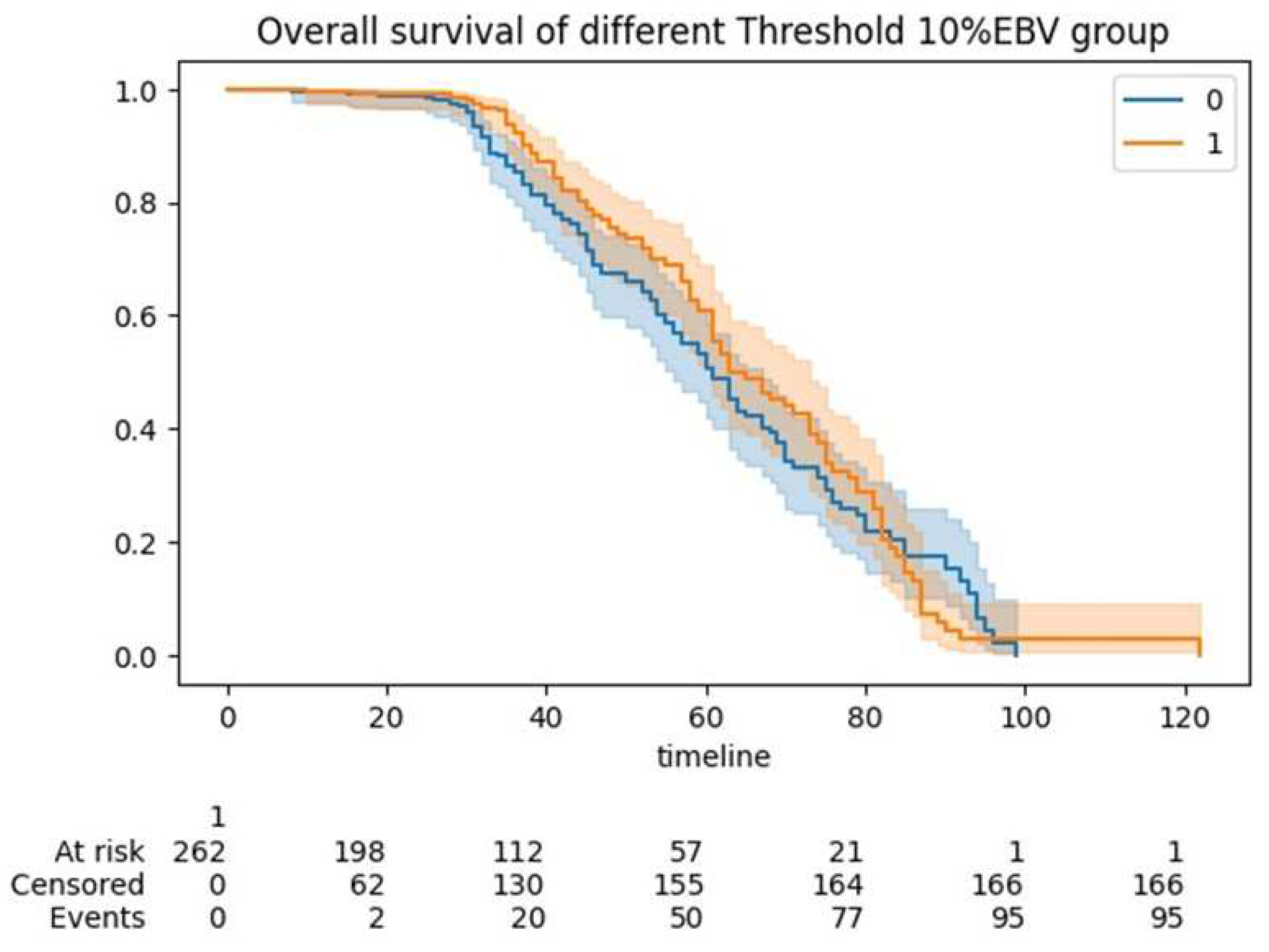
Figure 7.
Schematic representation of our study. According to our concept, ML-based feature selection identified operative time out of an exhaustive list of patient, disease and operation- specific features as the top feature for the risk prediction of blood transfusion at cytoreductive surgery.
Figure 7.
Schematic representation of our study. According to our concept, ML-based feature selection identified operative time out of an exhaustive list of patient, disease and operation- specific features as the top feature for the risk prediction of blood transfusion at cytoreductive surgery.
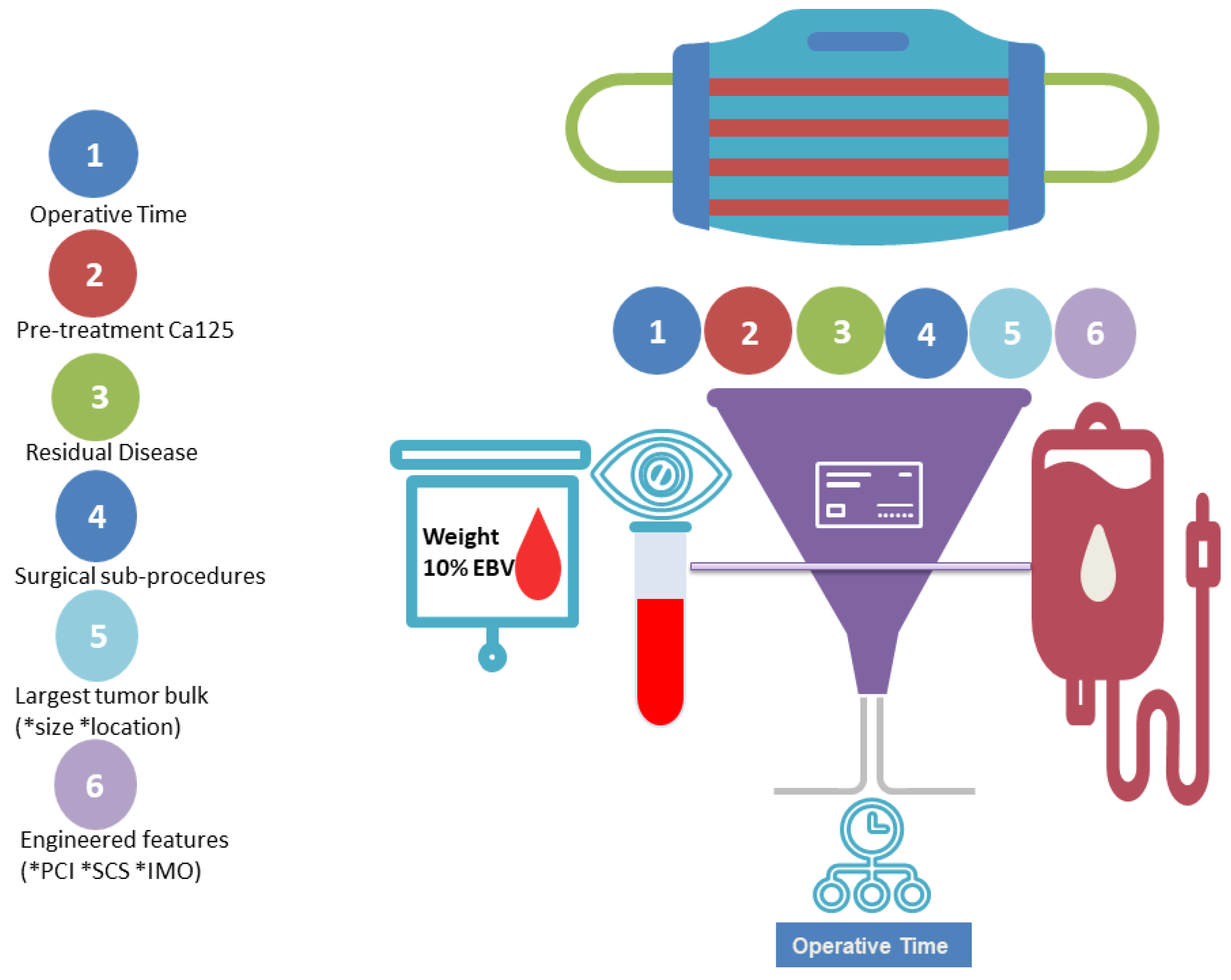

Table 1.
Cohort statistics
| Overall | Training Set | Testing Set | pvalue (training) | Group <10%EBV | Group >10%EBV) | pvalue (Threshold 10%EBV) | ||
|---|---|---|---|---|---|---|---|---|
| Histo_cat1 | 0 | 489 (87.32) | 394 (87.95) | 95 (84.82) | 0.465 | 264 (88.59) | 137 (87.82) | 0.929 |
| 1 | 71 (12.68) | 54 (12.05) | 17 (15.18) | 0.465 | 34 (11.41) | 19 (12.18) | 0.929 | |
| Grade_cat | 0 | 56 (10.0) | 46 (10.27) | 10 (8.93) | 0.805 | 20 (6.71) | 22 (14.1) | 0.016 |
| 1 | 504 (90.0) | 402 (89.73) | 102 (91.07) | 0.805 | 278 (93.29) | 134 (85.9) | 0.016 | |
| Figo_cat2 | 0 | 406 (72.5) | 322 (71.88) | 84 (75.0) | 0.586 | 216 (72.48) | 113 (72.44) | 1 |
| 1 | 154 (27.5) | 126 (28.12) | 28 (25.0) | 0.586 | 82 (27.52) | 43 (27.56) | 1 | |
| PS (WHO) | 0 | 266 (47.5) | 205 (45.76) | 61 (54.46) | 0.099 | 137 (45.97) | 76 (48.72) | 0.048 |
| 1 | 208 (37.14) | 175 (39.06) | 33 (29.46) | 0.099 | 111 (37.25) | 65 (41.67) | 0.048 | |
| 2 | 67 (11.96) | 56 (12.5) | 11 (9.82) | 0.099 | 43 (14.43) | 9 (5.77) | 0.048 | |
| 3 | 17 (3.04) | 11 (2.46) | 6 (5.36) | 0.099 | 7 (2.35) | 5 (3.21) | 0.048 | |
| 4 | 2 (0.36) | 1 (0.22) | 1 (0.89) | 0.099 | 0 (0.0) | 1 (0.64) | 0.048 | |
| PDS=0/ IDS=1 | 0 | 172 (30.71) | 132 (29.46) | 40 (35.71) | 0.243 | 72 (24.16) | 61 (39.1) | 0.001 |
| 1 | 388 (69.29) | 316 (70.54) | 72 (64.29) | 0.243 | 226 (75.84) | 95 (60.9) | 0.001 | |
| RD_cat | 0 | 369 (65.89) | 294 (65.62) | 75 (66.96) | 0.168 | 209 (70.13) | 93 (59.62) | 0.051 |
| 1 | 130 (23.21) | 100 (22.32) | 30 (26.79) | 0.168 | 64 (21.48) | 41 (26.28) | 0.051 | |
| 2 | 61 (10.89) | 54 (12.05) | 7 (6.25) | 0.168 | 25 (8.39) | 22 (14.1) | 0.051 | |
| Ascites3 | 0 | 414 (73.93) | 335 (74.78) | 79 (70.54) | 0.427 | 234 (78.52) | 103 (66.03) | 0.005 |
| 1 | 146 (26.07) | 113 (25.22) | 33 (29.46) | 0.427 | 64 (21.48) | 53 (33.97) | 0.005 | |
| Largest Bulk of Disease Location 4 | PA node | 1 (0.18) | 1 (0.22) | 0 (0.0) | 0.023 | 1 (0.34) | 0 (0.0) | 0.446 |
| POD | 1 (0.18) | 0 (0.0) | 1 (0.89) | 0.023 | 1 (0.34) | 0 (0.0) | 0.446 | |
| caecum | 1 (0.18) | 0 (0.0) | 1 (0.89) | 0.023 | 1 (0.34) | 0 (0.0) | 0.446 | |
| mesentery | 2 (0.36) | 2 (0.45) | 0 (0.0) | 0.023 | 0 (0.0) | 2 (1.28) | 0.446 | |
| omentum | 249 (44.46) | 204 (45.54) | 45 (40.18) | 0.023 | 138 (46.31) | 71 (45.51) | 0.446 | |
| ovary | 300 (53.57) | 238 (53.12) | 62 (55.36) | 0.023 | 154 (51.68) | 82 (52.56) | 0.446 | |
| peritoneum | 1 (0.18) | 1 (0.22) | 0 (0.0) | 0.023 | 0 (0.0) | 1 (0.64) | 0.446 | |
| rectum | 1 (0.18) | 0 (0.0) | 1 (0.89) | 0.023 | 1 (0.34) | 0 (0.0) | 0.446 | |
| sigmoid | 1 (0.18) | 0 (0.0) | 1 (0.89) | 0.023 | 0.446 | |||
| umbilicus | 1 (0.18) | 0 (0.0) | 1 (0.89) | 0.023 | 1 (0.34) | 0 (0.0) | 0.446 | |
| Age | 63.51 ± 11.22 | 63.23 ± 11.06 | 64.64 ± 11.82 | 0.252 | 63.53 ± 11.24 | 62.78 ± 11.27 | 0.502 | |
| Consultant age5 | 49.13 ± 6.03 | 49.1 ± 6.07 | 49.25 ± 5.91 | 0.815 | 49.96 ± 6.09 | 48.43 ± 6.11 | 0.011 | |
| Years6 | 9.65 ± 5.33 | 9.65 ± 5.36 | 9.68 ± 5.22 | 0.952 | 10.03 ± 5.31 | 9.29 ± 5.47 | 0.165 | |
| SCS7 | 3.8 ± 2.11 | 3.82 ± 2.06 | 3.71 ± 2.31 | 0.648 | 3.34 ± 1.83 | 4.73 ± 2.51 | <0.001 | |
| Time procedure8 | 170.39 ± 77.55 | 172.98 ± 76.53 | 160.04 ± 81.03 | 0.129 | 147.84 ± 55.24 | 215.1 ± 97.06 | <0.001 | |
| Pre Treatment CA125 | 1516.14 ± 2711.14 | 1582.85 ± 2769.98 | 1249.29 ± 2455.18 | 0.212 | 1689.69 ± 3189.63 | 1420.7 ± 2071.05 | 0.279 | |
| Pre Surgery CA125 | 410.46 ± 1175.43 | 411.43 ± 944.52 | 406.56 ± 1833.3 | 0.978 | 360.46 ± 1280.81 | 614.46 ± 1298.66 | 0.048 | |
| logCA125/ PCI | 0.41 ± 0.36 | 0.4 ± 0.35 | 0.42 ± 0.4 | 0.756 | 0.41 ± 0.35 | 0.4 ± 0.41 | 0.657 | |
| IMO score9 | 4.92 ± 1.97 | 4.98 ± 1.99 | 4.7 ± 1.89 | 0.158 | 4.57 ± 1.86 | 5.6 ± 2.11 | <0.001 | |
| PCI | 7.37 ± 4.47 | 7.48 ± 4.51 | 6.92 ± 4.31 | 0.225 | 6.78 ± 4.08 | 8.79 ± 5.16 | <0.001 | |
| Largest Bulk (cm) | 8.89 ± 5.61 | 9.13 ± 5.69 | 7.96 ± 5.23 | 0.039 | 8.29 ± 5.64 | 9.98 ± 5.49 | 0.002 |
1serous/non serous, 2S3=0;S4=1, 3(tapped) Nmax=25, 4(intra-op) (ov=0;om=1;misc=2),5Age of Consultant at surgery,6Years of experience as a consultant,7Surgical Complexity Score,8 in minutes,9IntraOperative Mapping of ovarian cancer, S; Stage, PS; performance status, PDS; primary debulking surgery, IDS; interval debulking surgery, RD; residual disease, PA; para-aortic, POD; pouch of Douglas, SCS; surgical complexity score, IMO; intra-operative mapping of ovarian cancer, PCI; peritoneal carcinomatosis index
Table 2.
Surgical sub-procedures’ statistics for the whole dataset broken down by CC0/non-CC0 patients. Chi-Square Test of Independence was used. Statistical analysis was performed using Python’s SciPy library. Values are n (%).
Table 2.
Surgical sub-procedures’ statistics for the whole dataset broken down by CC0/non-CC0 patients. Chi-Square Test of Independence was used. Statistical analysis was performed using Python’s SciPy library. Values are n (%).
| Overall (n = 560) | CC0 (n = 368) | Non-CC0 (n = 192) | p-Value | ||
|---|---|---|---|---|---|
| Stoma Formation | 0 | 509 (90.89) | 334 (90.76) | 175 (91.15) | 1 |
| 1 | 51 (9.11) | 34 (9.24) | 17 (8.85) | 1 | |
| Bladder Peritonectomy | 0 | 358 (63.93) | 217 (58.97) | 141 (73.44) | 0.001 |
| 1 | 202 (36.07) | 151 (41.03) | 51 (26.56) | 0.001 | |
| Para-aortic node dissection | 0 | 381 (68.04) | 221 (60.05) | 160 (83.33) | <0.001 |
| 1 | 179 (31.96) | 147 (39.95) | 32 (16.67) | <0.001 | |
| Ileo-Caecal Resection/ Right Hemicolectomy | 0 | 539 (96.25) | 352 (95.65) | 187 (97.4) | 0.426 |
| 1 | 21 (3.75) | 16 (4.35) | 5 (2.6) | 0.426 | |
| Mesenteric Resection | 0 | 427 (76.25) | 269 (73.1) | 158 (82.29) | 0.02 |
| 1 | 133 (23.75) | 99 (26.9) | 34 (17.71) | 0.02 | |
| Upper Abdominal Peritonectomy | 0 | 481 (85.89) | 296 (80.43) | 185 (96.35) | <0.001 |
| 1 | 79 (14.11) | 72 (19.57) | 7 (3.65) | <0.001 | |
| Large Bowel Resection | 0 | 496 (88.57) | 323 (87.77) | 173 (90.1) | 0.494 |
| 1 | 64 (11.43) | 45 (12.23) | 19 (9.9) | 0.494 | |
| Pelvic node dissection | 0 | 414 (73.93) | 242 (65.76) | 172 (89.58) | <0.001 |
| 1 | 146 (26.07) | 126 (34.24) | 20 (10.42) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



