
Submitted:
29 October 2023
Posted:
30 October 2023
You are already at the latest version
Abstract
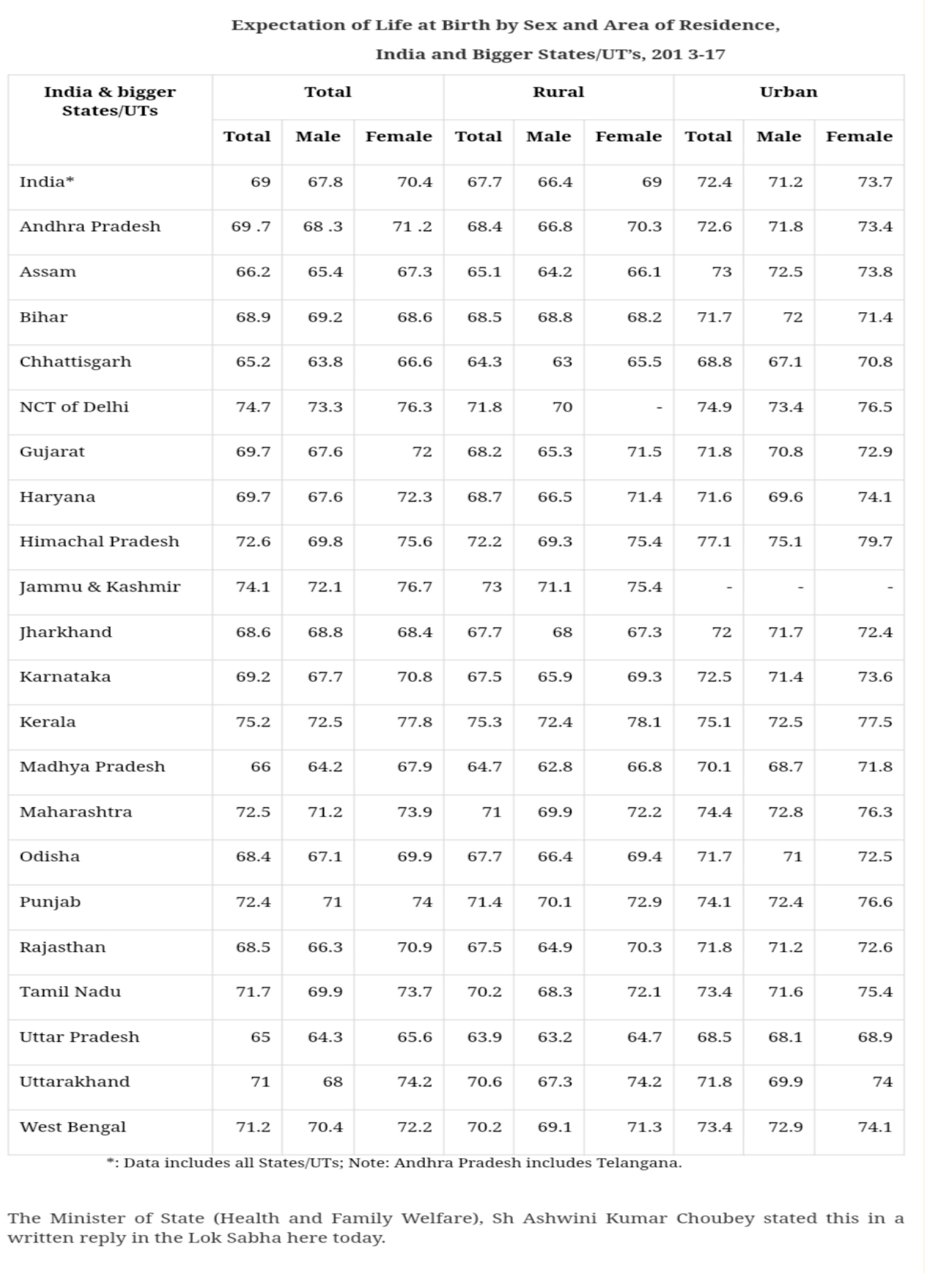
This research article provides a comprehensive analysis of the Expectation of Life at Birth in India and its larger states and union territories (UTs), with a specific focus on rural and urban disparities. The data, obtained from the Ministry of Health and Family Welfare of India, highlights the variations in life expectancy by sex and area of residence, shedding light on the health and socio-economic conditions in different regions. The article discusses the implications of these findings and their relevance for public health policy and interventions.
Keywords:
Birth
; expectation
; sex
; states
; India
Introduction
Expectation of Life at Birth (ELB) is a key demographic indicator that reflects the average number of years a newborn can expect to live, assuming the current mortality rates remain constant throughout their lifetime. ELB is influenced by a multitude of factors, including healthcare infrastructure, socio-economic status, education, and lifestyle, making it a vital metric for assessing overall population health and development.
Methodology
The data used in this study was sourced from the Ministry of Health and Family Welfare of India, encompassing a five-year period from 2013 to 2017. The data is organized by India as a whole and its larger states/UTs, as well as distinguishing between rural and urban areas. ELB is categorized by sex, including male and female.
Results
Findings
1. National Overview: The national overview of Expectation of Life at Birth (ELB) in India from 2013 to 2017 reveals a positive trend in life expectancy for both males and females. This period witnessed a noteworthy increase in ELB, indicating an overall improvement in the health and living conditions of the population.
For males, ELB increased from 67.8 years in 2013 to 71.2 years in 2017. Similarly, for females, ELB rose from 70.4 years in 2013 to 73.7 years in 2017. This upward trajectory is a promising sign of progress, reflecting advancements in healthcare, medical treatments, and lifestyle changes that have contributed to increased life expectancies. Furthermore, the data clearly illustrates a consistent urban-rural divide in ELB within India. Urban areas consistently report higher ELB figures when compared to their rural counterparts. This discrepancy can be attributed to several factors, including:
- Better Healthcare Access: Urban areas generally have more accessible healthcare facilities, hospitals, and specialized medical services. This ease of access to medical care is a significant factor contributing to higher life expectancies in urban settings.
- Sanitation and Hygiene: Urban areas typically have improved sanitation and hygiene standards, which reduce the prevalence of waterborne diseases and improve overall health. Clean water, proper sewage disposal, and sanitation practices contribute to better public health.
- Living Standards: Urban areas tend to have higher living standards, including better nutrition, housing, and overall quality of life. These factors contribute to the improved health and well-being of residents, further extending their life expectancy.
Despite these notable differences between urban and rural areas, it’s important to recognize that the overall increase in ELB for both segments of the population signifies that efforts have been made to enhance public health and well-being across the board.
2. State/UT Disparities: The data also highlights substantial disparities in ELB among India’s larger states and union territories (UTs). Notably, Kerala stands out with the highest ELB, both in urban and rural areas. This is a testament to Kerala’s robust healthcare system and its commitment to public health. Several factors contribute to Kerala’s high ELB, including a strong focus on healthcare infrastructure, education, and social development.
On the other end of the spectrum, states like Assam and Bihar exhibit lower ELB figures. This can be attributed to various socio-economic and healthcare challenges, such as:
- Limited Healthcare Infrastructure: Some states may lack sufficient healthcare infrastructure, leading to inadequate access to medical services and treatments.
- Low Socio-economic Development: Lower socio-economic development, coupled with higher poverty rates, can result in reduced access to nutrition, education, and healthcare, all of which impact life expectancy.
- Disease Burden: States with a higher burden of infectious diseases, malnutrition, and maternal and child health issues tend to have lower ELB figures. These issues can result from a lack of access to healthcare and education.
The disparities in ELB among Indian states and between urban and rural areas underscore the need for targeted interventions and policies to address the unique challenges each region faces. Recognizing these disparities is the first step in developing effective strategies to improve healthcare access, socio-economic development, and overall well-being for all citizens, regardless of their place of residence. The data provides a valuable foundation for policymakers to design region-specific public health initiatives aimed at narrowing the gaps in life expectancy and ensuring a healthier, more equitable future for all.
Discussions
The variations in Expectation of Life at Birth (ELB) between different states and between rural and urban areas in India signify the complex landscape of public health and socio-economic conditions in the country. These disparities emphasize the critical importance of targeted public health interventions and policies that are tailored to address the specific challenges faced by various regions.
1. Targeted Interventions for States with Lower ELB: States with lower ELB figures, such as Assam and Bihar, require focused efforts to improve healthcare infrastructure, access, and socio-economic development. These areas often grapple with a combination of challenges that impact life expectancy, making it essential to address these issues systematically:
- Healthcare Infrastructure: Insufficient healthcare infrastructure, including hospitals, clinics, and trained healthcare personnel, can result in limited access to medical care. Investment in building and upgrading healthcare facilities is crucial to ensure that residents have access to essential healthcare services.
- Access to Healthcare: In many low ELB states, a significant portion of the population faces barriers to accessing healthcare due to factors like distance, transportation, and cost. Initiatives that aim to improve healthcare access, especially in remote and underserved areas, are paramount.
- Socio-economic Development: Higher levels of poverty, lack of education, and unemployment are often associated with lower ELB. Therefore, socio-economic development programs, including skill development, poverty alleviation, and education initiatives, can contribute to improved overall well-being.
- Maternal and Child Health: High maternal and child mortality rates can significantly impact ELB. Focused programs that address maternal and child health, family planning, and nutrition can make a substantial difference in raising ELB in these regions.
- Infectious Disease Control: States with higher burdens of infectious diseases, such as malaria and tuberculosis, need targeted strategies for prevention, diagnosis, and treatment. These diseases can have a significant impact on life expectancy, and controlling their spread is essential.
2. Rural Healthcare Development: Recognizing the disparities between urban and rural areas in ELB underscores the need for rural healthcare development and policies to bridge this divide. Access to quality healthcare, sanitation, and education are key determinants in improving ELB in rural areas. Key considerations for addressing this challenge include:
- Rural Healthcare Infrastructure: Expanding and upgrading healthcare facilities in rural areas is crucial. This includes not only hospitals but also primary healthcare centers and telemedicine services to provide access to remote regions.
- Healthcare Workforce: Training and retaining healthcare professionals in rural areas is essential. Incentives and support for healthcare workers who choose to practice in underserved rural regions can help address the shortage of healthcare providers.
- Sanitation and Hygiene: Improving sanitation and hygiene standards in rural areas can reduce the burden of waterborne diseases and contribute to better public health. Initiatives promoting clean water sources and proper waste disposal are critical.
- Education and Awareness: Raising awareness about health and hygiene practices, as well as disease prevention, can empower rural communities to take charge of their well-being. Educational programs can also focus on lifestyle changes and preventive healthcare.
The disparities in ELB between states and between rural and urban areas are multifaceted, and addressing them requires a holistic approach. Public health interventions must be designed to account for the unique challenges and needs of each region. By focusing on healthcare infrastructure, access, socio-economic development, maternal and child health, infectious disease control, and rural healthcare development, policymakers can work toward bridging the gap in life expectancy and ensuring a healthier, more equitable future for all citizens. The data serves as a valuable guide for crafting region-specific public health initiatives that can lead to significant improvements in the overall health and well-being of the population.
Recommendations
Addressing the disparities in Expectation of Life at Birth (ELB) across India and its states/union territories (UTs) is an essential priority to ensure a healthier and more equitable future for all citizens. The following recommendations are designed to guide policymakers and stakeholders in taking targeted actions to improve ELB and overall public health:
1. Focused Investments in Healthcare Infrastructure and Services:
- To effectively raise ELB, states and UTs with lower ELB figures must receive targeted investments in healthcare infrastructure. This includes building and upgrading hospitals, clinics, and healthcare facilities in underserved areas.
- Strengthening healthcare services through the recruitment and training of healthcare professionals is crucial, as it ensures the availability of skilled personnel to provide quality care.
- Allocating adequate financial resources to healthcare is vital to maintain and expand healthcare infrastructure and services.
2. Targeted Efforts to Improve Maternal and Child Health, Nutrition, and Sanitation:
- Maternal and child health programs should be prioritized to reduce maternal and child mortality rates, as these have a significant impact on ELB.
- Nutrition initiatives, including supplementary feeding and nutrition education, can address malnutrition, one of the leading factors affecting ELB.
- Improving sanitation and hygiene standards through clean water sources, proper waste disposal, and community awareness programs can reduce the prevalence of waterborne diseases and enhance overall public health.
3. Strategies to Enhance Healthcare Access in Rural Areas:
- Access to quality healthcare in rural areas is critical to address disparities in ELB. Strategies include setting up telemedicine services, mobile clinics, and community health centers to ensure healthcare access in remote regions.
- Incentives and support for healthcare professionals willing to practice in rural areas can help address workforce shortages and improve healthcare availability.
- Expanding healthcare insurance and financial assistance programs can alleviate the financial burden of healthcare, especially in rural areas.
4. Promoting Education and Awareness for Lifestyle Changes and Preventive Healthcare:
- Educational campaigns should be launched to raise awareness about health and hygiene practices, disease prevention, and lifestyle changes.
- Providing access to quality education is essential for enhancing health literacy and promoting healthier lifestyles.
- Regular health check-up camps and screenings can identify health issues at an early stage, enabling timely interventions and preventive measures.
5. Data-Driven Decision-Making:
- Continuously monitor and analyze ELB data at the regional and national levels to assess the impact of interventions and identify areas that require further attention.
- Use data to guide resource allocation, policy adjustments, and the evaluation of healthcare and public health programs.
6. Collaboration and Partnerships: Foster collaborations between government agencies, non-governmental organizations (NGOs), and international partners to pool resources, share best practices, and collectively address public health challenges.
7. Holistic Approach: Ensure that policies and interventions adopt a holistic approach, addressing not only medical care but also social determinants of health, such as education, poverty, and nutrition.
8. Accountability and Transparency: Establish mechanisms for accountability and transparency in the allocation and utilization of healthcare resources. Regular reporting and audits can help ensure that investments are directed effectively.
Addressing disparities in ELB in India is a multifaceted endeavor that requires a combination of investments, targeted efforts, strategic planning, and a commitment to improving the overall health and well-being of the population. By focusing on these recommendations, policymakers and stakeholders can work towards achieving more equitable life expectancies, better healthcare access, and an improved quality of life for all citizens. These actions will contribute to a healthier and more prosperous India, promoting the well-being of its people and ensuring a brighter future for the nation as a whole.
Conclusions
In conclusion, the data on Expectation of Life at Birth (ELB) in India and its larger states and union territories from 2013 to 2017 reveals both positive trends and concerning disparities. While there has been an overall improvement in ELB, significant gaps persist between states, urban and rural areas, and genders. Addressing these disparities requires targeted efforts, including investments in healthcare infrastructure, improved maternal and child health, enhanced rural healthcare access, and education and awareness campaigns. Such actions are crucial to ensure a more equitable and healthier future for all citizens across the diverse regions of India.
Declarations
This study involving human subjects has received ethical approval from ERC: European Research Council. Approval from the ethics committee ensures that the study complies with ethical standards and safeguards the well-being of participants.
"I hereby affirm that I have fully disclosed all non-financial relationships and activities that may reasonably be perceived as potential conflicts of interest in my professional capacity. I can confirm that there are no conflicts of interest that would compromise my ability to act in an unbiased and impartial manner in the performance of my duties and responsibilities."
Author states that no funding was granted.
References
- Andrews, J. A., Hops, H., & Duncan, S. C. (1997). Adolescent modeling of parent substance use: The moderating effect of the relationship with the parent. Journal of Family Psychology, 11(3), 259–270. [CrossRef]
- Berndt, T. J., Hawkins, J. A., & Jiao, Z. (1999). Influences of friends and friendships on adjustment to junior high school. Merrill-Palmer Quarterly, 45(1), 13–41.
- Brechwald, W. A., & Prinstein, M. J. (2011). Beyond homophily: A decade of advances in understanding peer influence processes. Journal of Research on Adolescence, 21(1), 166–179. [CrossRef]
- Brown, B. B., Bakken, J. P., & Ameringer, S. W. (2009). A comprehensive conceptualization of the peer pressure process in adolescence. In G. R. Adams & M. D. Berzonsky (Eds.), Blackwell handbook of adolescence (pp. 361–393). Wiley-Blackwell.
- Chen, X., Chang, L., Liu, H., & He, Y. (2008). The peer group as a context: Mediating and moderating effects on relations between academic achievement and social functioning in Chinese children. Child Development, 79(6), 235–251. [CrossRef]
- Dumas, T. M., Ellis, W. E., & Wolfe, D. A. (2012). Identity development as a buffer of adolescent risk behaviors in the context of peer group pressure and control. Journal of Adolescence, 35(4), 917–927. [CrossRef]
- Eccles, J. S., Midgley, C., Wigfield, A., Buchanan, C. M., Reuman, D., Flanagan, C., & Iver, D. M. (1993). Development during adolescence: The impact of stage-environment fit on young adolescents’ experiences in schools and in families. American Psychologist, 48(2), 90–101. [CrossRef]
- Eccles, J. S., Midgley, C., Wigfield, A., Buchanan, C. M., Reuman, D., & Flanagan, C. (1993). Developmental transitions in school: Perceived performance as a context for motivation in middle school. Journal of Adolescent Research, 8(2), 187–204.
- Fletcher, A. C., Steinberg, L., & Williams-Wheeler, M. (2004). Parental influences on adolescent problem behavior: Revisiting Stattin and Kerr. Child Development, 75(3), 781–796. [CrossRef]
- Fredricks, J. A., Blumenfeld, P. C., & Paris, A. H. (2004). School engagement: Potential of the concept, state of the evidence. Review of Educational Research, 74(1), 59–109. [CrossRef]
- Guay, F., Marsh, H. W., & Boivin, M. (2003). Academic self-concept and academic achievement: Developmental perspectives on their causal ordering. Journal of Educational Psychology, 95(1), 124–136. [CrossRef]
- Hartup, W. W. (1989). Social relationships and their developmental significance. American Psychologist, 44(2), 120–126. [CrossRef]
- Helsen, M., Vollebergh, W., & Meeus, W. (2000). Social support from parents and friends and emotional problems in adolescence. Journal of Youth and Adolescence, 29(3), 319–335. [CrossRef]
- Juvonen, J., & Murdock, T. B. (1995). Grade-level differences in the social value of effort: Implications for self-presentation tactics of early adolescents. Child Development, 66(6), 1694–1705. [CrossRef]
- King, R. B., & McInerney, D. M. (2016). Culture’s consequences on student motivation: Capturing cross-cultural universality and variability through personal investment theory. Educational Psychologist, 51(3), 376–401.
- Lamborn, S. D., Mounts, N. S., Steinberg, L., & Dornbusch, S. M. (1991). Patterns of competence and adjustment among adolescents from authoritative, authoritarian, indulgent, and neglectful families. Child Development, 62(5), 1049–1065. [CrossRef]
- Pomerantz, E. M., Grolnick, W. S., & Price, C. E. (2005). The role of parents in how children approach achievement: A dynamic process perspective. In A. J. Elliot & C. S. Dweck (Eds.), Handbook of competence and motivation (pp. 259–278). Guilford Press.
- Prinstein, M. J., & Dodge, K. A. (2008). Understanding peer influence in children and adolescents. Guilford Press.
- Prinstein, M. J., & Wang, S. S. (2005). False consensus and adolescent peer contagion: Examining discrepancies between perceptions and actual reported levels of friends’ deviant and health risk behaviors. Journal of Abnormal Child Psychology, 33(3), 293–306. [CrossRef]
- Ryan, A. M., & Patrick, H. (2001). The classroom social environment and changes in adolescents’ motivation and engagement during middle school. American Educational Research Journal, 38(2), 437–460. [CrossRef]
- Ryan, A. M., & Shim, S. S. (2006). Social achievement goals: The nature and consequences of different orientations toward social competence. Personality and Social Psychology Bulletin, 32(9), 1246–1263. [CrossRef]
- Sebanc, A. M., & Pierce, W. D. (2001). Social comparison and dimensions of perceived academic competence among adolescents. Journal of Research on Adolescence, 11(3), 219–242. [CrossRef]
- Simpkins, S. D., Schaefer, D. R., Price, C. D., & Vest, A. E. (2013). Adolescent friendships, BMI, and physical activity: Untangling selection and influence through longitudinal social network analysis. Journal of Research on Adolescence, 23(3), 537–549. [CrossRef]
- Steinberg, L., & Monahan, K. C. (2007). Age differences in resistance to peer influence. Developmental Psychology, 43(6), 1531–1543. [CrossRef]
- Steinberg, L., Fletcher, A., & Darling, N. (1994). Parental monitoring and peer influences on adolescent substance use. Pediatrics, 93(6 Pt 2), 1060–1064. [CrossRef]
- Wentzel, K. R. (1998). Social relationships and motivation in middle school: The role of parents, teachers, and peers. Journal of Educational Psychology, 90(2), 202–209. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



