
Submitted:
27 October 2023
Posted:
01 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The persistence of geographic inequities in vaccination coverage often evidences the presence of zero-dose and missed communities and vulnerabilities to vaccine-preventable diseases. These inequities were exacerbated in many places during the COVID-19 pandemic, due to severe disruptions to vaccination services. Understanding changes in zero-dose prevalence and associated risk factors in the context of the COVID-19 pandemic is, therefore, critical to designing effective strategies to reach vulnerable populations. Using data from nationally representative household surveys conducted before the COVID-19 pandemic in 2018 and during the pandemic in 2021 in Nigeria, we fitted Bayesian geostatistical models to map the distribution of three vaccination coverage indicators: receipt of DTP1, MCV1 and any of the four basic vaccines (BCG, OPV0, DTP1 and MCV1), and corresponding zero-dose estimates independently at 1x1 km resolution and the district level during both time periods. We also explored changes in the factors associated with non-vaccination at the national and regional levels using multilevel logistic regression models. Our results revealed no increases in zero-dose prevalence due to the pandemic at the national level, although considerable increases were observed in a few districts. We found substantial subnational heterogeneities in vaccination coverage and zero-dose prevalence both before and during the pandemic, showing broadly similar patterns in both time periods. Areas with relatively higher zero-dose prevalence occurred mostly in the north and a few places in the south in both time periods. We also found consistent areas of low coverage and high zero-dose prevalence using all three zero-dose indicators, revealing areas in greatest need. At the national level, risk factors related to socioeconomic/ demographic status (e.g., maternal education), maternal access to and utilization of health services and remoteness were strongly associated with the odds of zero dose in both time periods, while those related to communication were mostly relevant before the pandemic. These associations were also supported at the regional level, but we additionally identified risk factors specific to zero dose in each region; for example, communication and cross-border migration in the northwest. Our findings can help guide tailored strategies to reduce zero-dose prevalence and boost coverage levels in Nigeria.
Keywords:
MCV1 coverage
; DTP1 coverage
; composite coverage
; zero-dose prevalence
; demographic and health surveys
; multiple indicator cluster survey
; Bayesian geostatistical modelling
; Bayesian multilevel modelling
1. Introduction
Vaccination is often regarded as one of the most successful and cost-effective public health interventions, saving millions of lives each year and guaranteeing global well-being and development [1]. Despite this, many children, especially those living in low- and middle-income countries, continue to miss out on life-saving vaccines even though there have been increased efforts globally to improve vaccination coverage and reduce zero-dose prevalence [2]. Before the pandemic in 2019, 18.4 million children did not receive all three recommended doses of the diphtheria-tetanus-pertussis containing vaccine (DTP), and of those, 70% (12.9 million) were zero-dose children who did not receive any doses of the DTP vaccine [2]. In 2020, these figures increased to 22 million children and 73% (16 million), respectively, due to the disruptions to immunization services caused by the coronavirus disease 2019 (COVID-19) pandemic [2,3,4]. These disruptions continued in 2021, resulting in 24 million being under-vaccinated and about 18 million being zero dose, with about 62% [5,6] of the estimated zero-dose children found to be living in 10 low- and middle-income countries (LMICs), including Nigeria. However, in 2022, a partial recovery in global DTP vaccination coverage was recorded, with the number of zero-dose children decreasing to 14.3 million, evidencing concerted efforts within countries to reach zero-dose children [2].
Zero-dose children often live in marginalized or underserved communities characterised by poverty, lack of access to basic health services, overcrowding, poor sanitation practices and conflict [7,8,9,10]. These characteristics, combined with other health-related, socioeconomic, demographic and gender-related factors, cause substantial disparities in the distribution of zero-dose children within countries [8]. Reaching these at-risk populations, therefore, requires timely and accurate evidence base regarding their sizes, geographic distribution, and other characteristics to support country-tailored strategies and interventions. Also, with recovery from the pandemic being uneven and much slower in LMICs [11], understanding any changes in vulnerabilities due to disruptions to both routine immunization and vaccination campaigns can help with planning effective mitigation strategies and strengthening immunization services to reach zero-dose children. Administrative data are regularly collected in many LMICs through platforms such as the District Health Information System version 2 (DHIS2) [12,13]. However, due to limitations such as numerator and denominator errors, these often have coverage values that cannot reliably inform spatially detailed heterogeneities in coverage and identification of zero-dose children. Household surveys, on the other hand, tend to produce more reliable estimates of coverage, but these are usually designed to be representative at coarse spatial scales, necessitating the use of geospatial modelling approaches to produce coverage estimates at fine spatial scales and for operationally relevant areas, e.g., districts, which are then integrated with population data to assess zero-dose prevalence [14,15,16]. Moreover, survey questionnaires include several modules that assess different characteristics of participants, making the data ideal for evaluating correlates of non-vaccination. Addressing zero-dose prevalence is critical to achieving the WHO’s Immunisation Agenda 2030 target of a 50% reduction in zero-dose children by 2030 and promises to “leave no one behind”, as well as targets within the Sustainable Development Goals [7,17] and Gavi, the Vaccine Alliance’s 2021–2025 Strategy [7,18].
Nigeria has one of the largest cohorts of un- and under-vaccinated children globally, with 2.3 million and 3 million children estimated to not have received any dose of the DTP and MCV vaccines, respectively, in 2022 [2]. Before the pandemic in 2019, routine coverage of essential vaccines such as DTP1 and MCV1 were estimated to be 72% and 58%, respectively. In 2022, although global coverage levels showed some recovery following the pandemic, routine coverage remained suboptimal in Nigeria standing at 70% and 60%, respectively, for both basic vaccines [2]. As a result, Nigeria has continued to experience measles outbreaks, with a resurgence of diphtheria outbreaks in 2023 [19,20]. Utazi et al. [21] found that despite repeated measles vaccination campaigns, measles incidence was related to RI coverage. Over the years, there has been a persistent north-south divide in vaccination coverage in Nigeria, with the northern regions having poorer coverage levels and often higher rates of disease incidence [21,22]. Many studies have also identified several demand- and supply-side factors such as maternal education, religion, maternal access to and utilization of health services, poor attitude of health workers, staff shortages, poor conditions at health facilities and vaccine stockouts [23,24,25,26], as being responsible for poor vaccine uptake and heterogeneities in the distribution of vaccination coverage within the country. The first case of the SARS-CoV-2 virus was recorded on 27 February 2020 [27] in Lagos state, Nigeria, following which the government launched a response to the pandemic, including a lockdown from March 30 to May 15, 2020 [28]. COVID-19 vaccination began on March 5, 2021, which saw significant shifts of priorities and resources from vaccination services to COVID-19 response [29]. These and other interventions are also thought to have further impacted immunization services negatively in the form of reduced access to vaccination, decreases in vaccine demand and uptake, cessation of outreach services and postponement of vaccination campaigns [3,21,30,31,32]. These challenges call for innovative approaches and intensified efforts to identify and reach zero-dose children in Nigeria.
Against this backdrop, our study aimed to estimate changes in the spatial distribution of zero-dose children and associated risk factors before and during the COVID-19 pandemic in Nigeria, with a view to assessing the impact of the pandemic on immunization service delivery in the country, which can help consolidate mitigation and other strategies required to boost coverage beyond pre-pandemic levels. We analyzed three outcomes/indicators using data from two household surveys implemented before and during the COVID-19 pandemic in Nigeria. We defined a zero-dose child for each outcome as a child aged 12-23 months who had not received the first dose of the diphtheria–tetanus–pertussis-containing vaccine (i.e., DTP or PENTA zero dose) or the first dose of the measles-containing vaccine (MCV zero dose) or any dose of the four basic vaccines—bacilli Calmette-Guerin (BCG) vaccine, oral polio vaccine (OPV), DTP and MCV—(Composite zero dose indicator). Due to data availability, our study considered only demand-side factors or reasons for non-vaccination.
2. Materials and Methods
Data and sources
We utilized data from two recent household surveys conducted in Nigeria, namely the 2018 Demographic and Health Survey (DHS) [33] and the 2021 Multiple Indicator Cluster Survey—National Immunization Coverage Survey (MICS-NICS) [34]. We also assembled geospatial covariate data obtained from various sources and relevant geospatial population data. To ensure respondents confidentiality, the cluster-level geographical coordinates were displaced up to 2km in urban areas and up to 5km is rural areas. We present detailed descriptions of these data sources in this section.
2018. Nigeria Demographic and Health Survey (DHS)
The 2018 Nigeria DHS was conducted between August and December 2018. The survey was designed to be representative at the national, zonal and state levels (including the Federal Capital Territory) and for urban and rural areas. It employed a two-stage stratified sampling design with stratification achieved by separating each of the 36 states and the Federal Capital Territory (FCT) into urban and rural areas. The first and second stages of the sampling design involved the selection of enumeration areas (EAs) or survey clusters with probability proportional to size from each stratum using a national sampling frame and the selection of households at random from household lists within the selected clusters. Detailed information on the methods employed in the survey is published elsewhere [33].
The survey was implemented in a total of 1389 clusters, with 11 of the 1400 clusters selected initially dropped due to security reasons. Also, in Borno state, only 11 of the 27 local government areas were considered in the survey due to high insecurity. Data on children between age 12-23 months were extracted for this study. Information on routine vaccination coverage obtained from both home-based records (or vaccination cards) and through maternal/caregiver recall were included in our study, as in previous studies [7,24].
2021. Nigeria Multiple Indicator Cluster Survey-National Immunization Coverage Survey (MICS-NICS)
The UNICEF implements MICS surveys to collect globally comparable data on several indicators relating to the situation of women and children within countries. On the other hand, the NICS surveys are implemented by the Nigerian government to provide reliable estimates of indicators of vaccination coverage used to evaluate the performance of the vaccination program. The MICS survey was integrated with NICS for the first time in Nigeria during its 5th round in 2016-17, paving the way for the joint implementation of both surveys in the current round in 2021.
Field work for the 2021 MICS-NICS took place between September and December 2021. Similar to the 2018 NDHS, the survey had a two-stage stratified sampling design and was also representative at the national, zonal and state levels and for urban and rural areas. Details of the sampling methodology are provided in the survey report [34]. The MICS had a target sample size of 1,850 clusters. A supplemental sample of 337 clusters was selected for NICS to increase the combined sample of children and the precision of vaccination coverage indicators, resulting in a total of 2187 clusters for the MICS-NICS. About 128 of the combined sampled clusters were inaccessible and could not be visited during the survey. Also, in Borno State, sampling took place in only 7 (out of 27) accessible local government areas, in which 29% of the total population of the state resided. As with the 2018 DHS, we extracted all relevant information on routine vaccination coverage for our study for children aged 12-23 months.
As we show in Supplementary Figure S1, children aged 12-23 months in the MICS-NICS survey were born between September 2019 and September 2020. Among these, those born after January 2020 became eligible to receive BCG, OPV0 and DTP1 vaccinations during the pandemic, whereas the entire birth cohort became eligible to receive MCV1 within the pandemic period. Also, the first and second waves of the pandemic which peaked in July 2020 and February 2021, respectively, overlapped considerably with the time intervals during which the MICS-NICS birth cohort became eligible for all four vaccines included in our study. This demonstrates that the analysis carried out using the 2021 MICS-NICS are ideal for assessing the impact of the COVID-19 pandemic on immunization service delivery within the country. Also, since data collection for the 2018 DHS took place before the pandemic, the survey is suitable for assessing the performance of the vaccination program before the pandemic. However, because both surveys were implemented independently and not as rolling/repeated surveys, there could be sampling and other methodological differences that could impact the comparisons between both surveys, which is a potential limitation of our study.
Outcome indicators of zero dose included in the study
To assess changes in zero-dose prevalence and associated risk factors before and during the pandemic in Nigeria, our study considered binary indicators of receipt of DTP1 (PENTA1) (yes=1, no=0), receipt of MCV1 (yes=1, no=0), and receipt of any of the four basic vaccines—BCG, OPV0, DTP1 and MCV1—as a composite coverage indicator (yes=1, no=0) among children aged 12-23 months. We note that both BCG and OPV0 are birth doses, while DTP1 and MCV1 are administered at age 6 weeks and from age 9 months, respectively, according to Nigeria’s immunization schedule [35]. For all the 3 indicators, we extracted data on 5,459 children and 6,393 children aged 12-23 months from the 2021 MICS and the 2018 DHS, respectively, for our analysis.
At the cluster level, we aggregated the individual level data to produce numbers of children surveyed, numbers vaccinated, and empirical proportions of children vaccinated. In each case, we obtained the (displaced) geographical (i.e., longitude and latitude) coordinates of the survey clusters. These cluster level data are displayed in Figure 1 for both surveys.
Independent variables and geospatial covariate data
Following previous studies [7,24], we included individual child, mother, household, and community characteristics as risk factors for zero dose [7,24]. These are: sex of child, skilled birth attendance, mother’s receipt of tetanus toxoid vaccination, mother’s antenatal care visits, maternal age and mother’s marital status, maternal education, religion, access to media, and phone/internet, land ownership, health insurance, ethnicity, sex of household head and household wealth. Other covariates considered are maternal access to a bank account, household size and length of stay, place (urban/rural) and region of residence. These variables were considered due to data availability in both the 2018 DHS and 2021 MICS-NICS surveys. Detailed definitions of the variables are provided in Supplementary Table S1.
The geospatial covariates considered include travel time to the nearest health facility, distance to conflict areas, poverty index, number of wet days, daytime land surface temperature, livestock density index, slope, enhanced vegetation index (EVI), distance to coastline, distance to the edge of cultivated areas, proximity to national borders and proximity to protected areas. Consideration of these covariates was informed by their use in previous studies [15,21,36] to model and predict various indicators of vaccination coverage. These covariates were processed as detailed in previous work [15,21,36,37] to produce 1x1 km raster layers and cluster level data using the geographical coordinates from each of the surveys. Some of these covariate layers are displayed in Supplementary Figure S2 and detailed descriptions are provided in Supplementary Table S2. The classifications of the cluster-level values of some of the covariates for use in the multilevel analyses are also shown in Supplementary Figure S3.
Furthermore, for our multilevel analyses (see model (1)) using each survey, we calculated the tertiles of the distribution of the extracted cluster level data and used these to group the (continuous) values of the covariates into three classes, namely lower, medium, and higher, which were used in the analyses (see Supplementary Table S1 and Figure S3) together with the survey-derived covariates discussed previously. However, for the geospatial models, the included covariates were on their original continuous scale (except where these were log-transformed prior to model-fitting). As in previous studies [16,36,37], for each survey and indicator, we implemented a detailed covariate selection process to determine the best combination of the geospatial covariates to be included in the geospatial analyses using model (2). The covariate selection process involved various steps to check the relationships between the geospatial covariates and the coverage indicators, resolve the problem of multicollinearity and then choosing the best set of covariates using stepwise regression (backward elimination based on Akaike Information Criterion (AIC)) in a non-spatial framework. The final step of the covariate selection process involved creating a uniform set of covariates for modelling all the indicators for both time periods to enhance comparability.
Population data
We obtained 1x1 km estimates of numbers of children aged under 1 year old in 2017 and 2020 (corresponding to the birth cohorts included in our analyses) from WorldPop [38], adjusted to United Nations Population Division (UNPD) estimates at the national level for both time periods [39]. These data were used in our work to calculate zero-dose estimates through integration with the coverage maps, and as weighting layers when aggregating grid-level coverage estimates to the administrative level.
Statistical analysis
Descriptive and bivariate analysis
Descriptive analyses were performed using individual level data for each survey to estimate frequencies and corresponding proportions for each indicator at the national level, as a precursor to the multi-level analyses.
Multilevel model
We fitted Bayesian multi-level random intercept logistic regression models, accounting for individual, household, community, and stratum level variation, to estimate the relationships between each outcome variable (i.e., odds of DTP1, MCV1 and composite coverage) and the covariates/risk factors for zero dose.
Let i index a child aged 12-23 months residing in household j community/cluster k and stratum (there were 37 strata in MICS-NICS and 74 in DHS). Also, let be a vector of associated covariates. The multi-level model is given by:
where denotes a binary response (or vaccination status; coded as 1—vaccinated and 0 unvaccinated) for child , represents the corresponding odds of DTP1, MCV1 or zero-dose vaccination, is the overall intercept, is a vector of associated regression coefficients for the covariates , is the residual random effect for stratum l, is the residual random effect for community (or survey cluster) k located in stratum l, is the random effect of household j within community k located in stratum l. The quantities , , and are assumed to be identically and independently normally distributed with the zero means and variances , , and respectively [40]. We note that the individual level (level 1) residual is assumed to follow the standard logistic distribution with variance expressed as 3.29 [41].
We applied model (1) to both surveys to identify significant associated risk factors for zero dose using all three indicators at the national level. In addition, we applied the model to examine regional variation in the risk factors associated with zero dose by subsetting the data to the North Central, North East, North West and Southern regions of the country. The three geopolitical zones in the southern part of the country (i.e., the Southeast, South-south, and Southwest regions) were combined in the regional analysis due to insufficient sample sizes. Also, a reduced set of risk factors were considered in the regional analyses to increase the samples sizes within the categories of the risk factors in each region.
The Bayesian models were fitted using the integrated nested Laplace approximation (INLA) approach implemented in the R-INLA package. The default priors in R-INLA were assigned to both the fixed and random effect parameters in the models [42]. Following model-fitting, we calculated the adjusted odds ratios and their associated 95% credible intervals to evaluate the significance of the associations between the risk factors and the odds of zero dose.
Geostatistical model
To predict each of the outcome indicators on a 1x1 km grid, we applied a Bayesian geostatistical model to the aggregated cluster level data from each survey. Let denote the number of children who received DTP1, MCV1 or any of the four basic vaccines (BCG, OPV0, DTP1 and MCV1) out of a total of children drawn from each sampled cluster location , and the corresponding unknown true vaccination coverage. Also, let denote a vector of geospatial covariate information for location . The geostatistical model assumes that follows the binomial probability distribution given by
where is an intercept parameter, is a vector of regression coefficients corresponding to , and is a spatially structured random effect and follows a zero-mean Gaussian process with variance and covariance function, . There are various parametric families for [43]. In the current analysis, we assumed the Matérn class of covariance functions[44] given by
where the notation |||| denotes the Euclidean distance between locations and , is the variance of the spatial field as noted earlier, is a smoothness parameter, is a scaling parameter related to the range —the distance at which spatial correlation is negligible or approaches 0.1 and is the modified Bessel function of second kind and order . The smoothness parameter was set to for the purpose of identifiability as recommended [45]. Lastly, is an iid Gaussian random effect with mean 0 and variance, , capturing non-spatial residual variation.
The geostatistical model was fitted using the Integrated Nested Laplace Approximation—Stochastic Partial Differential Equations (INLA-SPDE) approach, implemented in the R-INLA package [45,46]. The predictive performance of all the fitted models were assessed using approaches discussed in previous work [16].
To aggregate the 1x1 km grid level estimates to the district and other administrative levels, we computed the areal estimates as population-weighted averages of the corresponding indicators (i.e., DTP1, MCV1 or Composite coverage) taken over all the grid cells falling within the administrative area, as in previous work [16]. We note that this is a common approach to handling point-to-area misalignment when mapping health and development indicators [16,47].
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1.1. Outcome indicators of vaccination coverage
The observed national-level coverage estimates for DTP1, MCV1 and the composite coverage indicator were 64.8% (95% CI: 63.6-66.0%), 53.4% (95% CI: 52.1-54.6%), and 73.8% (95% CI: 72.7-74.8%), respectively, for the 2018 DHS. For the 2021 MICS-NICS, the observed national-level coverage estimates were 71.0% (95% CI: 69.8-72.2%), 61.1% (95% CI: 59.8-62.4%) and 79.4% (95% CI: 78.3-80.4%) respectively, for DTP1, MCV1, and the composite coverage indicator. Generally, the observed coverage estimates appeared to be higher for the 2021 MICS-NICS relative to the 2018 DHS for all the three indicators (Supplementary Table S3).
3.1.2. 1 km x 1 km modelled estimates of coverage and associated uncertainties before and during the pandemic
Predicted coverage estimates and associated uncertainties for children aged 12-23 months in 2018 and 2021 are presented in Figure 2 and supplementary Figure S4 for DTP1, MCV1, and the composite coverage indicator. These maps show broadly similar patterns in coverage in both years, although coverage seemed relatively higher in some areas (e.g., parts of the northwest) in 2021. There are substantial geographical differences in coverage when examining DTP1 and MCV1 coverage, with a clear north-south divide for both vaccines and years. As expected, the coverage of the composite indicator is generally higher than DTP1 and MCV1 and areas of low coverage are also concentrated more in the northern areas for this indicator, as well as some southern coastal areas and some areas in Cross River state. Importantly, there are significant overlaps in low coverage areas across all three indicators in both time periods, suggesting persistent lack of access to vaccination services in these areas. These low coverage areas are more pronounced in Sokoto, Zamfara, Yobe and Kwara states, and parts of Bauchi, Gombe and Taraba states. In both Sokoto and Zamfara states, the poorest coverage levels were observed in areas such as Tangaza, Sangiwa, Naman Goma, Tureta, Anka, Ramfashi, Maru, Bungudu, Yar-Mahanga, and Maholo among others when examining the interactive web-based maps online (link1).
Table 0. for the predicted vaccination coverage estimates for 2018 DHS and less than 0.36 for the 2021 MICS-NICS, suggesting low uncertainties around the predicted coverage estimates in both years (Supplementary Figure S3).
3.1.2. District-level estimates of numbers of zero-dose children before and during the pandemic
Figure 3 presents district-level estimates of numbers of zero-dose children for the three coverage/zero dose indicators before and during the pandemic in 2018 and 2021, respectively. In general, the spatial distributions of the zero-dose estimates are identical across all three indicators in both time periods. The district level zero-dose estimates exhibit a clear north-south divide similar to the coverage estimates, with children residing in the northern districts being at higher risk of zero dose for all three indicators compared to their counterparts in the south. However, there are also clusters of districts with relatively higher numbers of zero-dose children in the south (in Lagos and Ogun states). As expected, there is a substantial overlap between the low coverage areas and areas with higher numbers of zero-dose children, although there are a few exceptions. For example, some districts in the southern coastal areas had lower coverage levels (supplementary Figure S5), but these were not densely populated areas, hence the zero-dose estimates were lower relative to some northern districts with similar coverage estimates.
In 2018, the national estimates of DTP, MCV and composite zero-dose children were 2 364 020, 3 121 156 and 1 703 296 respectively, while in 2021, these were 2 063 375, 2 784 980 and 1 457 068, respectively, indicating no increases in zero-dose prevalence due to the pandemic. The same pattern was generally observed at the district level (Figure 3), where we observed more decreases than increases in zero-dose prevalence (Figure 4). Additionally, we observed no (marked) increases in zero-dose prevalence in districts that had moderate to higher numbers of zero-dose children in 2018 (Figure 4d–f). However, there were a few districts, particularly those in Lagos (Alimosho), Bauchi (Ningi), Kano (Ugongo, Dala, Tarauni, Kumbotso, Dawakin Tofa, Minjibir, Gwale, etc) and Borno (Jere) states where considerable increases (>3000 unvaccinated children) were observed relative to the pre-pandemic period (Figure 4a–c). Also, we observed greater increases in zero-dose prevalence for MCV relative to DTP and the composite coverage indicator (Figure 3).
Districts with the highest numbers of composite zero-dose children (>10 000) were mostly located in Zamfara state (Bungudu, Gusau, Kaura Namoda, Zurmi, Maradun, Maru and Bukkuyum) in 2018, whereas in 2021, these (> 9 000 zero-dose children) were located in Bauchi (Ningi, Shira, Ganjuwa), Lagos (Alimosho), Kano (Ugongo) and Sokoto (Dange-Shuni) states, reflecting areas with lack of access to or poor utilization of vaccination services in both time periods. In supplementary Figures S6 and S7, we display the zero-dose estimates at the state and regional levels to facilitate comparisons at these administrative levels. These estimates show that the greatest numbers of unvaccinated children were located in the northwestern region in both time periods and across all three indicators, driven by highly populated states such as Kano and Katsina states.
The zero-dose estimates are also displayed using interactive web-based spatial maps online (link2) for better visualization.
3.1.3. Risk factors associated with zero dose at the national and regional levels before and during the pandemic
The associations between the risk factors (adjusted odds ratios (aORs) and corresponding 95% credible intervals (CIs)) and the odds of vaccination or zero dose are plotted in Figure 5 and Supplementary Figures S8 and S9 at the national level for both time periods. When considering the composite coverage indicator (Figure 5), we observed strong similarities as well as subtle/minor differences in both time periods with respect to the factors associated with zero dose. Factors associated with the odds of zero dose in both time periods include: skilled birth attendance, birth quarter, mother’s receipt of tetanus toxoid vaccination status, mother’s education, ethnicity, household wealth and access to bank account. The directions of the estimated relationships were generally the same between both time periods for these factors, except for birth quarter, suggesting different seasonal patterns in vaccination in both periods. These similarities mostly reflect lack of changes in the associations between risk factors characterising maternal access to and utilization of health services, socioeconomic/demographic status, and the odds of zero dose in both time periods. Factors associated with zero dose in the pre-pandemic period in 2018 only include: antenatal care attendance, access to media, use of phone/internet, rural/urban and travel time to the nearest health facility; while those associated with zero dose in the pandemic period only include: marital status, livestock density, distance to coastline and distance to conflicts. Considering that similar variables were also associated with vaccination in both time periods in most cases, these differences mostly reflect changes in the effect of communication which was only associated with zero dose before the pandemic, and different characterizations of the effect of remoteness on vaccination in both time periods. We also note that the unexpected direction in the effect of the urban/rural variable before the pandemic is likely due to undetected collinearity or the effect of suppressing variables [7,48]. Detailed results of the estimated odds ratios are provided in supplementary materials (see Figures S8–S13 and Tables S4 and S5).
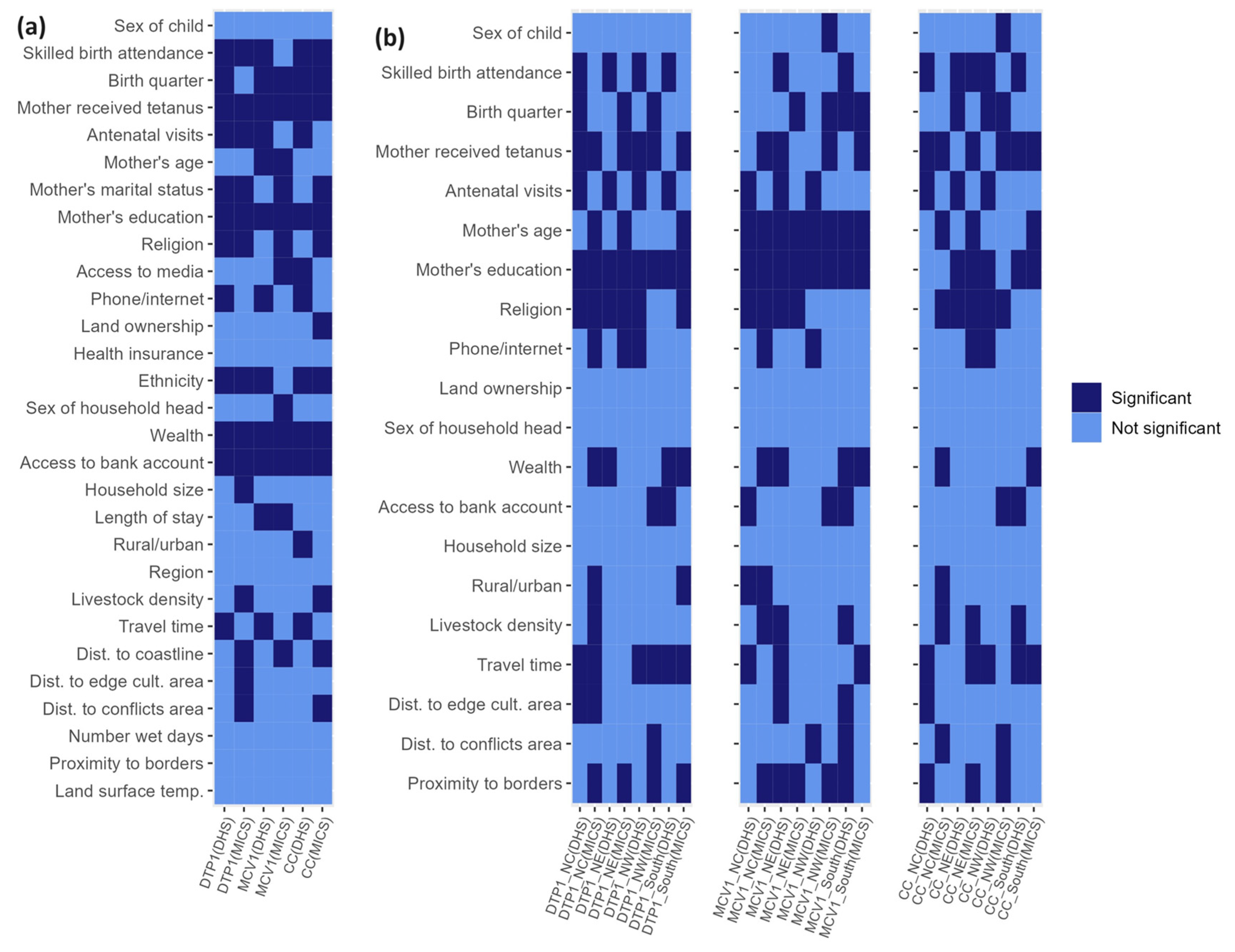
In Figure 5 and Figure 6, we provide summary plots of the (significant) risk factors that characterized the inequities in vaccination coverage at both the national and regional levels before and during the pandemic. At the national level, we found that mother’s receipt of tetanus toxoid vaccination, household wealth, access to bank account and mother’s education were associated with all three zero-dose indicators in both the pre-pandemic and pandemic periods. Also, mother’s ethnicity, religion, marital status, antenatal care attendance and skilled birth attendance were associated with receipt of DTP1 during both time periods whereas length of stay, mother’s age, and birth quarter were additionally associated with MCV1 in both periods. Additional factors associated with the composite coverage indicator in both periods were ethnicity, birth quarter and skilled birth attendance. When examining the differences in the risk factors associated with zero dose/vaccination between both time periods, we observed that travel time and phone/internet were associated with all three outcome indicators before the pandemic, while distance to coastline was associated with all three outcomes during the pandemic. There were also other factors associated with vaccination in one time period only when examining individual outcome indicators—e.g., additional remoteness variables such as distance to the edge of cultivated areas and distance to the conflicts—were associated with DTP1 during the pandemic only. Interestingly, mother’s age and length of stay (although with changing patterns for this risk factor) were only associated with MCV1 in both time periods and not associated with any other indicator in either or both time periods, highlighting the importance of both factors for MCV vaccination. Overall, these results agree with our initial conclusions using the composite coverage indicator.
At the regional level (Figure 6 and Supplementary Figures S10–S13), no risk factor was associated with all three indicators in both time periods in all the regions, evidencing greater variation in the associations between the risk factors and vaccination at the regional level or the effect of smaller sample sizes available at this level in the analysis (as highlighted previously, these analyses at the regional level were undertaken with a reduced set of risk factors due to sample size limitations). However, when examining individual indicators, we found that mother’s education was associated with DTP zero dose in all four regions in both time periods. Also, mother’s education and mother’s age were associated with MCV zero dose in all four regions in both time periods. No risk factor was associated with composite zero dose in all four regions and both time periods, although there were strong effects of religion in the northern regions, mother’s education in the northeast and southern regions, and mother’s receipt of tetanus toxoid vaccination in the north central and southern regions.
In the northwestern region, which had the highest estimates of numbers of zero-dose children among the six regions, no risk factor was associated with all three indicators in both time periods, although mother’s education was associated with DTP1 and MCV1 in both time periods. Additional factors associated with all three indicators in either of the two time periods were: antenatal care attendance (pre-pandemic), phone/internet (pre-pandemic), access to bank account (pandemic) and proximity to borders (pandemic). These results additionally evidence changes in the effect of communication between the two periods and the importance of maternal education, as in the national level results. In the northeast region, mother’s education and religion were associated with all three indicators both before and during the pandemic. Additionally, antenatal care attendance was associated with all three indicators in the pre-pandemic period in this region. No risk factor was consistently associated with all three indicators in one time period only. We note that the estimated associations in both periods for this region are also in agreement with the results obtained at the national level.
In the north central region, no risk factor was associated with all three indicators in both time periods. However, mother’s education and religion were associated with DTP and MCV zero dose in both time periods while mother’s receipt of tetanus toxoid vaccination was associated with DTP1 and composite coverage in both time periods. Other risk factors associated with all three indicators either before or during the pandemic were: antenatal care attendance (pre-pandemic), household wealth (pandemic), livestock density (pandemic) and proximity to borders (pandemic). These results obtained for this region are generally in agreement with the national level results, but additionally demonstrate the effect of wealth and potential cross-border migration on zero-dose. In the southern region, mother’s education was associated with all three indicators in both time periods. Additionally, travel time was associated with DTP and composite coverage zero dose in both time periods. Skilled birth attendance and access to bank account were also associated with all three indicators before the pandemic. No risk factor was associated with all three indicators in the pandemic period only. These results are also in agreement with the national results and additionally highlight the effect of maternal literacy, remoteness, maternal access to and utilization of health services and socioeconomic disparities on the odds of zero dose.
In general, these regional level results, though limited by smaller sample sizes, generally corroborate the findings at the national level and have additionally highlighted the risk factors most important for each region through consistent associations with all three indicators either in one or both of the time periods studied.
4. Discussion
By evaluating recent spatial and temporal trends in the distribution of zero-dose children in the context of the COVID-19 pandemic, our study further strengthens the scientific evidence base for improving childhood immunization in Nigeria.
Our study provided estimates of numbers of unvaccinated children for DTP, MCV and a composite coverage indicator at different spatial scales during the pre-pandemic and pandemic periods in Nigeria. Interestingly, our 2018 national level DTP and MCV zero-dose estimates of 2.4 million and 3.1 million are in very good agreement with (WHO and UNICEF estimates of national immunization coverage) WUENIC zero-dose estimates of 2.2 million and 3.1 million respectively. Also, our 2021 national level DTP and MCV zero-dose estimates of 2.1 million and 2.8 million in 2021 are very close to corresponding WUENIC zero-dose estimates of 2.2 million and 2.9 million children, respectively (WUENIC zero-dose estimates were calculated using 2022 WUENIC coverage estimates and UNPD estimates 2022 revision). Clearly, the pandemic did not result in any dramatic increases in zero-dose prevalence at the national level, but the persistence of large numbers of unvaccinated children in both time periods means that renewed efforts and novel strategies are needed to reach zero-dose and missed communities in the country. At the district level, no dramatic increases in zero-dose prevalence were found during the pandemic relative to the pre-pandemic era. However, there were some areas with elevated zero-dose estimates (> 3000 children) during the pandemic, as highlighted previously. Some of these districts were located in Kano and Lagos states where either relatively higher COVID-19 cases or deaths [49] were recorded during the study period, which could have also occurred as a result of the larger population sizes of both states [38]. Subnational variation in the effect of the pandemic on zero-dose prevalence in Nigeria has also been reported at the state level in a previous study [31] which focused on Kano and Kaduna states. We note that the lack of substantial increases in zero-dose prevalence at the national level and in many subnational areas in our study, contrary to expectations, might have been due to a quick recovery from the disruptions caused by the pandemic [50]. Additionally, our study revealed strong geographical disparities and a clear north-south divide in zero-dose prevalence in both time periods and across all three indicators, with districts with higher numbers of zero-dose children concentrated in the northern areas, as corroborated by previous studies [14,15,21,36,51]. However, there were also some districts in the south (e.g., in Lagos state) with higher numbers of zero-dose children. This recurring spatial pattern in the distribution of zero-dose children is a strong indication that targeted RI and campaign strategies, focusing on the most problematic areas, will be needed to achieve substantial reductions in zero-dose prevalence within the country. Previous studies [21,22] also revealed higher measles case counts in the north and high correlations between measles case counts and MCV zero-dose estimates, further strengthening the evidence for targeted interventions.
The underlying coverage levels also had similar patterns, revealing persistent areas of low coverage, mostly concentrated in the northeast and northwest regions across all three indicators and for both time periods. There were also persistent pockets of low coverage areas in the south, e.g., some areas in Cross River state and some areas near the coastline. However, we note that there were differences in the problematic areas when examining coverage and the zero-dose estimates at the district level. For example, there were some districts in Lagos and Ogun states with moderate coverage levels, but which had higher zero-dose estimates. Also, some of the low coverage districts in Cross River state did not have higher zero-dose estimates, likely due to these areas having lower population densities. Hence, efforts aimed at reducing zero-dose prevalence should target areas where higher zero-dose estimates were estimated, whereas strategies to improve equity in coverage should focus on the low coverage areas. When comparing maps of DTP1 and MCV1 coverage, we observed very similar patterns, with DTP1 coverage being higher in many places, due to the dropouts that often occur between both vaccine doses (and perhaps, the result of the suspension of MCV campaigns during the pandemic in 2021). This is a strong indication that frequent campaigns conducted in Nigeria for MCV, though an effective temporary measure, have not been successful in boosting coverage beyond RI levels. The targeted strategies advocated earlier should, therefore, focus more on strengthening the country’s RI program, as we have also argued elsewhere [21]. Furthermore, when examining maps of the composite coverage indicator, the low coverage areas occurring mostly in the northeast and northwest and overlapping considerably with low coverage areas for MCV1 and DTP1, are strongly indicative of non-availability of vaccination services and/or vaccine hesitancy. Different strategies would be required in these areas to unravel and address the barriers to vaccination.
When examining the risk factors associated with zero dose, we found that while there were strong similarities between the pre-pandemic and pandemic periods, there were also some minor differences which appeared more pronounced at the subnational/regional level. These similarities and differences are important for characterising the inequities that exist in vaccination coverage in both time periods. At the national level, our study revealed consistent associations between each of socioeconomic status (e.g., maternal literacy, household wealth and access to a bank account) and maternal access to and utilization of health services (e.g., skilled birth attendance) and the odds of zero dose in both time periods. We also found evidence of consistency in the effect of demographic factors (e.g., ethnicity, religion, and mother’s age) and seasonality of vaccination (e.g., birth quarter) on the odds of zero dose in both time periods. At the regional level (based on a reduced set of risk factors), we found additional evidence supporting the results obtained at the national level. Also, these regional level analyses revealed the risk factors most relevant to reaching zero-dose and missed communities in each region. These were: maternal access to and utilization of health services (all regions), communication (northwest), socioeconomic status (northwest, northcentral and south), religion (northeast and, to a great extent, north central), cross-border migration (northwest and northcentral) and remoteness (south). Furthermore, at the national level, we did not find any remarkable differences in the associations between the risk factors and the odds of zero dose between both time periods. However, we found that there were changes in the variables characterizing the effect of remoteness on zero dose in both time periods. For example, travel time to the nearest health facility was associated with all three zero-dose indicators before the pandemic, while distance to coastline was associated with all three zero-dose indicators during the pandemic. Also, there was a pronounced positive effect of communication on the odds of vaccination before the pandemic, suggesting reduced communication regarding vaccination services during the pandemic. We did not explore the differences between both time periods at the regional level further due to smaller sample sizes at this level.
To facilitate the operationalization of these findings, our study produced interactive web-based maps online (link1; link2) to further assist with the identification of towns, communities and, potentially, settlements in the problematic areas. Additional analyses can also be undertaken through triangulation with other data sets, e.g., data on public health facilities offering vaccination services, to better understand the costs and/or efforts needed to reach zero-dose children within each district. Furthermore, the multi-temporal analyses presented here are highly relevant to planning effective outbreak response strategies or catch-up vaccination activities. Nigeria is currently experiencing a diphtheria outbreak which, according to reports [20], has been more pronounced in Kano, Katsina, Yobe, Bauchi, Kaduna, Borno and Jigawa states as of the beginning of October 2023. Interestingly, these states were among the states where we had estimated the highest prevalence of DTP zero-dose children in both 2018 (mostly between 120 000 and 215 000 DTP zero-dose children per state—see Supplementary Figure S6) and 2021 (mostly between 80 000 and 240 000 DTP zero-dose children per state), further corroborating the findings from our study. Also, the occurrence of a considerable proportion (one-third) of the confirmed cases of the disease in children aged between 5 and 9 years (as of October 2023), which includes the birth cohort for which we produced zero-dose estimates in 2018 in our study, further evidences the programmatic and operational relevance of our analyses. Specifically, our maps of DTP zero-dose children for both years can be used to determine areas where interventions are needed to fill immunity gaps in both older birth and younger birth cohorts throughout the country. We also note that our district/LGA level zero-dose estimates can be further disaggregated to the ward level to enhance field operations if need be.
Through its Zero-dose Reduction Operational Plan (Z-DROP) programme, Nigeria is continuing to intensify efforts to reach its zero-dose and missed communities. Fundamentally, the Z-DROP programme is one of the strategies for achieving the country’s vision of integrated primary health care service delivery [52]. Through a rigorous prioritization exercise led by the National Primary Health Care Development Agency, Gavi, the Vaccine Alliance, and University of Southampton in August 2022, about 100 LGAs were identified as priority areas where (RI) interventions were urgently needed to reach zero-dose and under-immunized children. About 60 of these LGAs, spread across 8 states, are being targeted in the current phase of the Z-DROP programme. The programme employs a bottom-up approach to design and implement interventions in these areas through engagement with local health workers. These interventions include initial catch-up immunization activities planned as part of the 2023 measles campaigns, aiming to administer recommended routine vaccines to identified zero-dose children and then follow up RI activities to sustain the gains made and to ensure the completion of the immunization schedule. The process of identifying zero-dose children in these LGAs additionally involve the triangulation of coverage survey/zero-dose, surveillance and outreach services data at the ward and health facility levels to identify, geolocate and classify (unreached, far-to-reach, hard-to-reach and never reached) high-priority settlements. These additional analyses also include estimating the target populations and the cost of implementing the required interventions in the identified high-priority settlements to guide resource allocation. The programme also provides a mechanism to document all operational activities for effective supervision and timely tracking of progress.
Our study is subject to some limitations. Our vaccination coverage estimates were produced using information obtained from both home-based records and maternal/caregiver recall, with the latter being subject to recall bias. The sampling frames used in both the 2018 DHS and 2021 MICS-NICS may have missed important vulnerable populations such as those living in conflict areas in Borno state as highlighted previously. This may have led to an underestimation of the zero-dose prevalence in some areas. Our analyses included comparisons of vaccination coverage and zero-dose estimates between the 2018 NDHS and 2021 MICS-NICS to assess the impact of the COVID-19 pandemic on immunization services in Nigeria. Since these surveys were implemented independently and not as repeated or rolling surveys, differences in the survey instruments (e.g., questionnaires), sampling designs and implementation could have affected the differences seen in the comparisons. Our analyses utilized displaced cluster level geographical coordinates to predict coverage levels at 1x1 km resolution. While this may not matter for coverage and zero-dose estimation at the district level using the 2018 DHS data since the DHS program often retains the displaced clusters within their original districts [53], the displacement may have affected the district level estimates produced using the 2021 MICS-NICS as the initial displacement conducted by the MICS Team which was used in our work only preserved the state boundaries. Since completing our analyses, the displacement of the geographical coordinates from the 2021 MICS-NICS has been updated to preserve the district level boundaries. We carried out some sensitivity analyses (results not presented here) using the updated coordinates, which revealed very minor differences from the results (coverage maps) presented in this work. Furthermore, we did not quantify the uncertainties associated with the zero-dose estimates presented in our work. When uncertainty estimates are available for the population estimates [54,55], these can be combined with the uncertainties from vaccination coverage in a statistical framework to produce uncertainties for the zero-dose estimates. Our analysis of the risk factors associated with zero-dose included mainly demand-side factors due to data limitations. The inclusion of supply-side factors in future work will likely yield more programmable insights. Lastly, our exploration of the differences in the risk factors associated with zero dose at the regional level in the pre-pandemic and pandemic periods was limited by smaller sample sizes. This challenge can be overcome in future work through a pooled data analysis.
As immunization programs around the world continue to recover from the disruptions to immunization services caused by the COVID-19 pandemic and getting back on track to achieving the goals and targets set out in the Immunization Agenda 2030, our study has provided programmatically-important insights that can aid policy makers to plan and implement effective strategies to reach zero-dose and missed communities in Nigeria.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figures S1–S13. Tables S1–S5.
Author Contributions
Conceptualization, C.E.U., A.J.T. and J.M.K.A.; methodology, C.E.U. and J.M.K.A.; software, C.E.U. and J.M.K.A.; validation, C.E.U. and J.M.K.A.; formal analysis, C.E.U., J.M.K.A. and H.M.T.C.; investigation, C.E.U., J.M.K.A., H.M.T.C., and I.O.; resources, C.E.U.; data curation, C.E.U., J.M.K.A., H.M.T.C., and I.O; writing—original draft preparation, C.E.U. and J.M.K.A.; writing—review and editing, C.E.U., J.M.K.A., A.J.T., I.O., H.M.T.C., A.E., B.D., B.F., H.S., B.A., and J.C.; visualization, C.E.U., J.M.K.A., I.O., and H.M.T.C.; supervision, C.E.U. and A.J.T.; project administration, C.E.U.; funding acquisition, C.E.U.;. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by GAVI, the Vaccine Alliance.
Institutional Review Board Statement
Ethics approval for this study was provided by the University of Southampton, United Kingdom.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study during the primary data collection by the various survey programs. Only secondary data were analyzed in this study.
Data Availability Statement
The data used in this study are available from the DHS (https://dhsprogram.com/data/available-datasets.cfm) and MICS (https://mics.unicef.org/surveys) programs upon request. Other data (i.e., geospatial covariates) are publicly available via the sources referenced in the manuscript. The authors are not allowed to redistribute these datasets.
Conflicts of Interest
B.D., B.A. and J.C. work for GAVI, the Vaccine Alliance. The authors declare no other conflicts of interest.
References
- World Health Organization (WHO). Global Immunization Coverage 2021 [Internet]; WHO Estimates of National Immunization Coverage (data as of July 2022). Available from https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on March 20 2023). Geneva, Switzerland2021.
- World Health Organization (WHO), UNICEF. 2022 WHO/UNICEF Estimates of National Immunization Coverage (WUENIC). Available from: https://cdn.who.int/media/docs/default-source/immunization/wuenic-progress-and-challenges.pdf?sfvrsn=b5eb9141_12&download=true. [Accessed on 21 August 2023] WHO and UNICEF; 2023.
- Causey K, Fullman N, Sorensen RJD, Galles NC, Zheng P, Aravkin A, et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: a modelling study. Lancet. 2021;398:522-34. [CrossRef]
- Ho LL, Gurung S, Mirza I, Nicolas HD, Steulet C, Burman AL, et al. Impact of the SARS-CoV-2 pandemic on vaccine-preventable disease campaigns. International Journal of Infectious Diseases. 2022;119:201-9. [CrossRef]
- World Health Organization (WHO), UNICEF. 2021 WHO/UNICEF Estimates of National Immunization Coverage (WUENIC). Available from: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage. [Accessed on 20 February 2023]. 2022.
- Hogan D, Gupta A. Why Reaching Zero-Dose Children Holds the Key to Achieving the Sustainable Development Goals. Vaccines2023. [CrossRef]
- Utazi CE, Pannell O, Aheto JMK, Wigley A, Tejedor-Garavito N, Wunderlich J, et al. Assessing the characteristics of un- and under-vaccinated children in low- and middle-income countries: A multi-level cross-sectional study. PLOS Global Public Health. 2022;2:e0000244. [CrossRef]
- Wigley A, Lorin J, Hogan D, Utazi CE, Hagedorn B, Dansereau E, et al. Estimates of the number and distribution of zero-dose and under-immunised children across remote-rural, urban, and conflict-affected settings in low and middle-income countries. PLOS Global Public Health. 2022;2:e0001126. [CrossRef]
- Chopra M, Bhutta Z, Chang Blanc D, Checchi F, Gupta A, Lemango ET, et al. Addressing the persistent inequities in immunization coverage. Bull World Health Organ. 2020;98:146-8. [CrossRef]
- WHO. Immunization Agenda 2030: A Global Strategy To Leave No One Behind. [https://www.who.int/immunization/immunization_agenda_2030/en/. Accessed: June 25, 2021]. Geneva, Switzerland: World Health Organization; 2020.
- O’Brien KL, Lemango E. The big catch-up in immunisation coverage after the COVID-19 pandemic: progress and challenges to achieving equitable recovery. Lancet. 2023;402:510-2. [CrossRef]
- Shuaib F, Garba AB, Meribole E, Obasi S, Sule A, Nnadi C, et al. Implementing the routine immunisation data module and dashboard of DHIS2 in Nigeria, 2014–2019. BMJ Global Health. 2020;5:e002203. [CrossRef]
- District health information system, version 2, 2019. Available: https://www.dhis2.org/.
- Sbarra AN, Rolfe S, Nguyen JQ, Earl L, Galles NC, Marks A, et al. Mapping routine measles vaccination in low- and middle-income countries. Nature. 2021;589:415-9. [CrossRef]
- Utazi CE, Thorley J, Alegana VA, Ferrari MJ, Takahashi S, Metcalf CJE, et al. Mapping vaccination coverage to explore the effects of delivery mechanisms and inform vaccination strategies. Nature Communications. 2019;10:1633. [CrossRef]
- Utazi CE, Nilsen K, Pannell O, Dotse-Gborgbortsi W, Tatem AJ. District-level estimation of vaccination coverage: Discrete vs continuous spatial models. Statistics in Medicine. 2021;40:2197-211. [CrossRef]
- United Nations (UN). Transforming our world: The 2030 agenda for sustainable development; 2015. Available from: https://sustainabledevelopment.un.org/post2015/transformingourworld/publication. [Accessed on 20 August 2023]. UN; 2015.
- Gavi The Vaccine Alliance (GAVI). Gavi Strategy 5.0, 2021–2025; 2020. Available from: https://www.gavi.org/our-alliance/strategy/phase-5-2021-2025. [Accessed on 20 June 2023]. GAVI2020.
- Nigeria Centre for Disease Control and Prevention (NCDC). An Update of Measles Outbreak in Nigeria. Available at https://ncdc.gov.ng/diseases/sitreps (Accessed on 20th February 2023). 2023.
- Nigeria Centre for Disease Control and Prevention (NCDC). An Update of Diphtheria Outbreak in Nigeria. Available at https://ncdc.gov.ng/diseases/sitreps (Accessed on 20th February 2023). 2023.
- Utazi CE, Aheto JMK, Wigley A, Tejedor-Garavito N, Bonnie A, Nnanatu CC, et al. Mapping the distribution of zero-dose children to assess the performance of vaccine delivery strategies and their relationships with measles incidence in Nigeria. Vaccine. 2022. [CrossRef]
- Jean Baptiste AE, Masresha B, Wagai J, Luce R, Oteri J, Dieng B, et al. Trends in measles incidence and measles vaccination coverage in Nigeria, 2008–2018. Vaccine. 2021;39:C89-C95. [CrossRef]
- Akwataghibe NN, Ogunsola EA, Broerse JEW, Popoola OA, Agbo AI, Dieleman MA. Exploring Factors Influencing Immunization Utilization in Nigeria-A Mixed Methods Study. Front Public Health. 2019;7:392. [CrossRef]
- Aheto JMK, Pannell O, Dotse-Gborgbortsi W, Trimner MK, Tatem AJ, Rhoda DA, et al. Multilevel analysis of predictors of multiple indicators of childhood vaccination in Nigeria. PLoS ONE. 2022;17:e0269066. [CrossRef]
- Oku A, Oyo-Ita A, Glenton C, Fretheim A, Eteng G, Ames H, et al. Factors affecting the implementation of childhood vaccination communication strategies in Nigeria: a qualitative study. BMC Public Health. 2017;17:200. [CrossRef]
- International Vaccine Access Center (IVAC). Landscape Analysis of Routine Immunization in Nigeria. Available from https://www.jhsph.edu/ivac/wp-content/uploads/2018/05/IVAC-Landscape-Analysis-Routine-Immunization-Nigeria-Brief.pdf. IVAC; 2012.
- Nigeria Centre for Disease Control (NCDC). First Case of Corona Virus Disease Confirmed in Nigeria. Available from https://ncdc.gov.ng/news/227/first-case-of-corona-virus-disease-confirmed-in-nigeria (Accessed on 24th March 2023). 2020.
- Presidential Task Force on COVID-19—Nigeria. Presidential Task Force on COVID-19: Mid-Term Report. Available from https://statehouse.gov.ng/covid19/2020/10/02/presidential-task-force-on-covid-19-mid-term-report/ (Accessed on 30th April 2023). Nigeria2020.
- Mathieu E, Ritchie H, Rodés-Guirao L, Appel C, Giattino C, Hasell J, et al. Coronavirus pandemic (COVID-19), vaccinations by Country; Nigeria. Our World in Data. Available from https://ourworldindata.org/covid-vaccinations (Accessed on 21 February 2023). 2020.
- Essoh TA, Adeyanju GC, Adamu AA, Ahawo AK, Aka D, Tall H, et al. Early Impact of SARS-CoV-2 Pandemic on Immunization Services in Nigeria. Vaccines (Basel). 2022;10. [CrossRef]
- Ibrahim D, Alyssa S, Ismael H, Ricardo I. Analysis of the impact of COVID-19 pandemic and response on routine childhood vaccination coverage and equity in Northern Nigeria: a mixed methods study. BMJ Open. 2023;13:e076154. [CrossRef]
- Adelekan B, Goldson E, Abubakar Z, Mueller U, Alayande A, Ojogun T, et al. Effect of COVID-19 pandemic on provision of sexual and reproductive health services in primary health facilities in Nigeria: a cross-sectional study. Reproductive Health. 2021;18:166. [CrossRef]
- National Population Commission (NPC) [Nigeria], ICF. Nigeria Demographic and Health Survey 2018—Final Report. [https://dhsprogram.com/publications/publication-fr359-dhs-final-reports.cfm. Accessed: 16/03/2021]. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF; 2019.
- National Bureau of Statistics (NBS), United Nations Children’s Fund (UNICEF). Multiple Indicator Cluster Survey 2021—Survey Findings Report. Abuja, Nigeria: NBS and UNICEF; 2022.
- World Health Organization (WHO). Vaccination schedule for Nigeria. Available from https://immunizationdata.who.int/pages/schedule-by-country/nga.html?DISEASECODE=&TARGETPOP_GENERAL= (Accessed on 19 February 2023). WHO; 2023.
- Utazi CE, Wagai J, Pannell O, Cutts FT, Rhoda DA, Ferrari MJ, et al. Geospatial variation in measles vaccine coverage through routine and campaign strategies in Nigeria: Analysis of recent household surveys. Vaccine. 2020;38:3062-71. [CrossRef]
- Utazi CE, Thorley J, Alegana VA, Ferrari MJ, Takahashi S, Metcalf CJE, et al. High resolution age-structured mapping of childhood vaccination coverage in low and middle income countries. Vaccine. 2018;36:1583-91. [CrossRef]
- WorldPop. Open Spatial Demographic Data and Research. Available at https://www.worldpop.org/ (accessed on 20 February 2023). WorldPop; 2021.
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2022: Release note. Available at https://population.un.org/wpp/ (accessed on 19 October 2023). 2022.
- Leckie G, Charlton C. runmlwin—A Program to Run the MLwiN Multilevel Modelling Software from within Stata. Journal of Statistical Software. 2013;52:1-40.
- Hedeker D, Gibbons RD. MIXOR: a computer program for mixed-effects ordinal regression analysis. Comput Methods Programs Biomed. 1996;49:157-76. [CrossRef]
- Lindgren F, Rue H. Bayesian Spatial Modelling with R-INLA. Journal of Statistical Software; Vol 1, Issue 19 (2015). 2015. [CrossRef]
- Diggle P, Ribeiro PJ, MyiLibrary. Model-based geostatistics. Springer series in statistics. New York, NY: Springer; 2007.
- Matérn, B. Spatial Variation. 2nd ed. Berlin: Springer-Verlag; 1986.
- Lindgren F, Rue H, Lindström J. An explicit link between Gaussian fields and Gaussian Markov random fields: the stochastic partial differential equation approach. Journal of the Royal Statistical Society: Series B (Statistical Methodology). 2011;73:423-98. [CrossRef]
- Rue H, Martino S, Lindgren F, Simpson D, Riebler A. INLA: Functions which allow to perform full Bayesian analysis of latent Gaussian models using Integrated Nested2013.
- Mosser JF, Gagne-Maynard W, Rao PC, Osgood-Zimmerman A, Fullman N, Graetz N, et al. Mapping diphtheria-pertussis-tetanus vaccine coverage in Africa, 2000-2016: a spatial and temporal modelling study. Lancet. 2019;393:1843-55. [CrossRef]
- Ludlow L, Klein K. Suppressor Variables: The Difference Between ‘is’ Versus ‘Acting As’. Journal of Statistics Education. 2014;22:null-null.
- Nigeria Centre for Disease Control and Prevention (NCDC). COVID-19 NIGERIA. Available from https://covid19.ncdc.gov.ng/ (Accessed on 20th 23). Nigeria.
- Sato, R. Pattern of vaccination delivery around COVID-19 lockdown in Nigeria. Human Vaccines & Immunotherapeutics. 2021;17:2951-3. [CrossRef]
- Utazi CE, Aheto JMK, Chan HMT, Tatem AJ, Sahu SK. Conditional probability and ratio-based approaches for mapping the coverage of multi-dose vaccines. Stat Med. 2022;41:5662-78. [CrossRef]
- World Health Organization (WHO). States adopt integrated vaccination strategy to reach unimmunized children, Nigeria. Available from https://www.afro.who.int/countries/nigeria/news/states-adopt-integrated-vaccination-strategy-reach-unimmunized-children (Accessed on 19 February 2023). 2022.
- Burgert CR, Colston J, Roy T, Zachary B. Geographic displacement procedure and georeferenced data release policy for the Demographic and Health Surveys. DHS Spatial Analysis Reports No 7. Calverton, Maryland, USA: ICF International; 2013.
- Nilsen K, Tejedor-Garavito N, Leasure DR, Utazi CE, Ruktanonchai CW, Wigley AS, et al. A review of geospatial methods for population estimation and their use in constructing reproductive, maternal, newborn, child and adolescent health service indicators. BMC Health Services Research. 2021;21:370. [CrossRef]
- Leasure DR, Jochem WC, Weber EM, Tatem AJ. National population mapping from sparse survey data: A hierarchical Bayesian modeling framework to account for uncertainty. PNAS. 2020;117. [CrossRef]
Figure 1.
Survey cluster locations and observed vaccination coverage for children aged 12-23 months for both the 2018 DHS (top panel) and 2021 MICS-NICS (bottom panel).
Figure 1.
Survey cluster locations and observed vaccination coverage for children aged 12-23 months for both the 2018 DHS (top panel) and 2021 MICS-NICS (bottom panel).
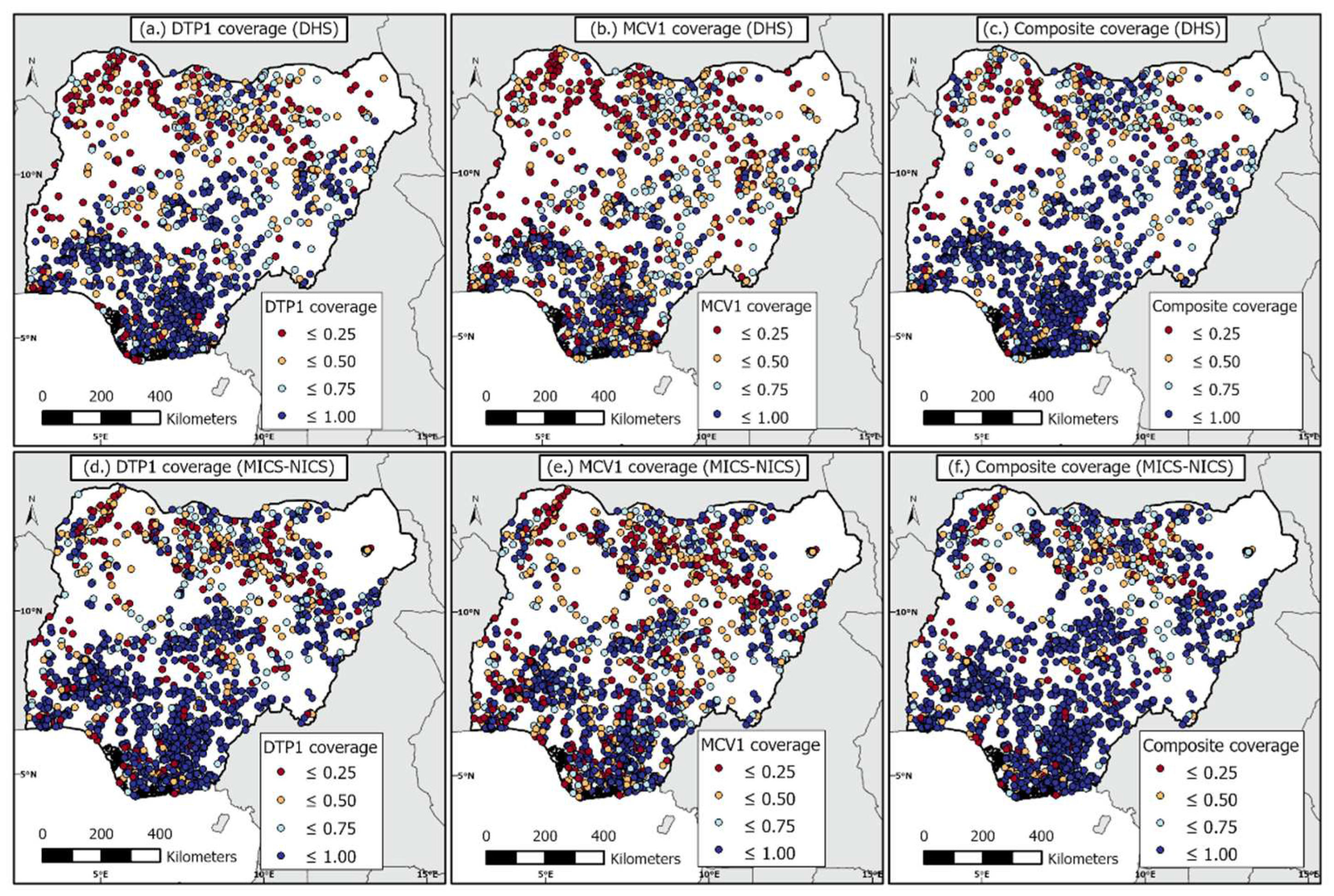
Figure 2.
1km x 1km modelled estimates of vaccination coverage for DTP1, MCV1, and composite coverage indicator before the pandemic, produced through using the 2018 DHS (top panel), and during the pandemic, produced through using the 2021 MICS-NICS (bottom panel). The associated uncertainty maps are shown in Supplementary Figure S4.
Figure 2.
1km x 1km modelled estimates of vaccination coverage for DTP1, MCV1, and composite coverage indicator before the pandemic, produced through using the 2018 DHS (top panel), and during the pandemic, produced through using the 2021 MICS-NICS (bottom panel). The associated uncertainty maps are shown in Supplementary Figure S4.
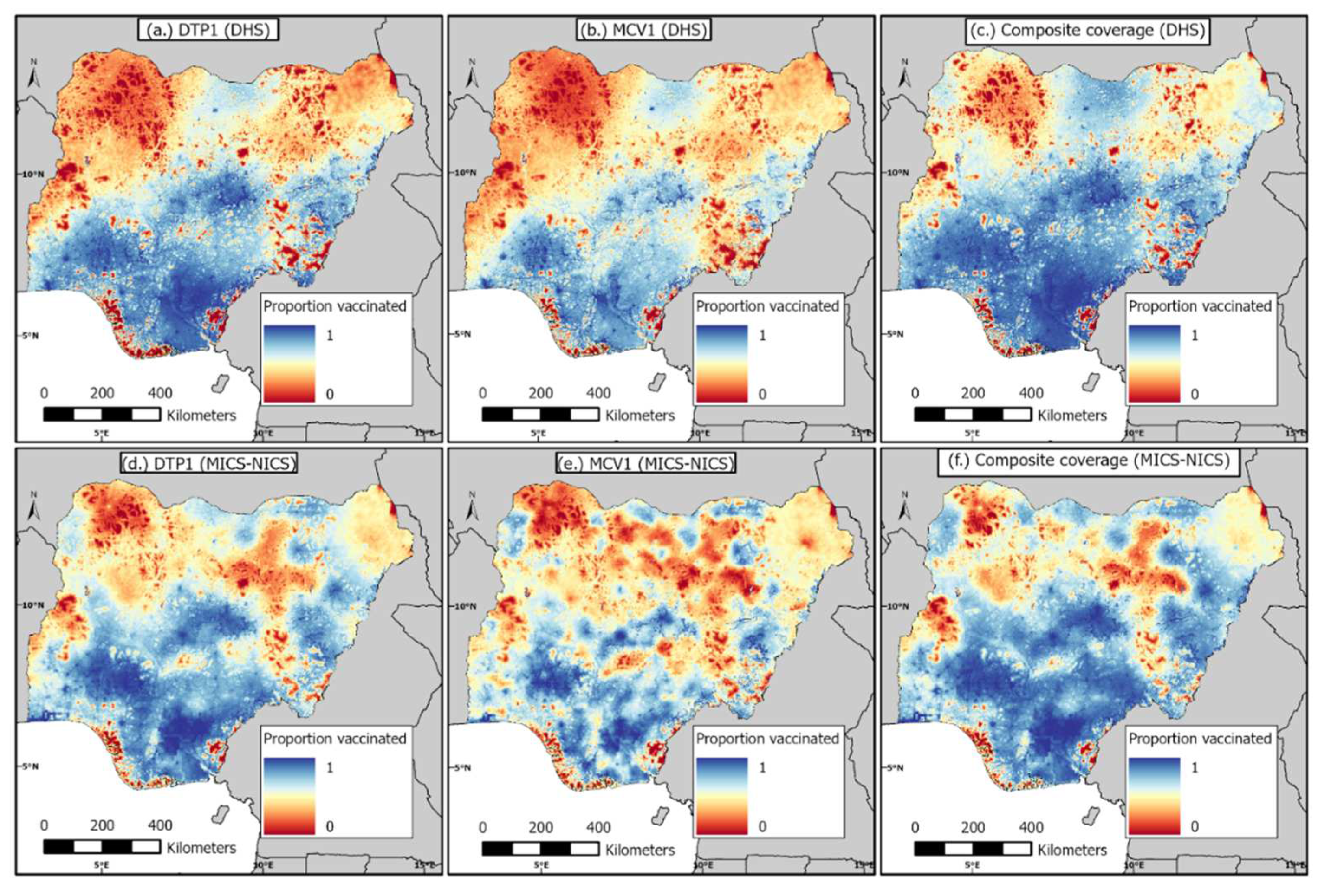
Figure 3.
District-level estimates of numbers of DTP, MCV and composite (i.e., BCG, OPV, DTP and MCV) zero-dose children during the pre-pandemic period in 2018 (top panel) and the pandemic period in 2021 (bottom panel). Corresponding coverage estimates are shown in supplementary Figure S5.
Figure 3.
District-level estimates of numbers of DTP, MCV and composite (i.e., BCG, OPV, DTP and MCV) zero-dose children during the pre-pandemic period in 2018 (top panel) and the pandemic period in 2021 (bottom panel). Corresponding coverage estimates are shown in supplementary Figure S5.
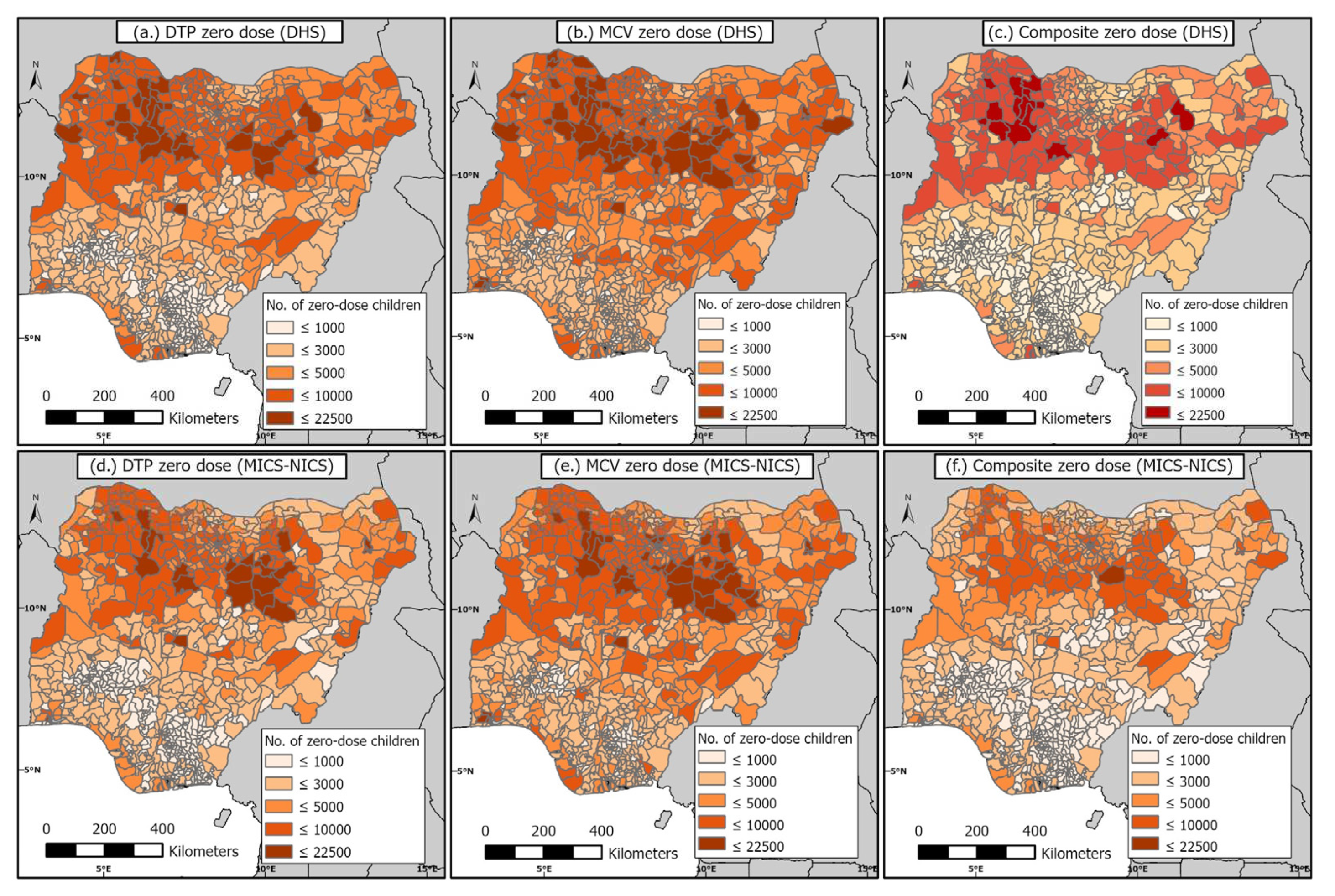
Figure 4.
(a–c) Absolute changes in estimates of numbers of zero-dose children between 2018 and 2021 (i.e., 2021 estimates minus 2018 estimates) and (d–f) 2018 zero-dose estimates versus the relative changes in zero-dose estimates between both time periods.
Figure 4.
(a–c) Absolute changes in estimates of numbers of zero-dose children between 2018 and 2021 (i.e., 2021 estimates minus 2018 estimates) and (d–f) 2018 zero-dose estimates versus the relative changes in zero-dose estimates between both time periods.
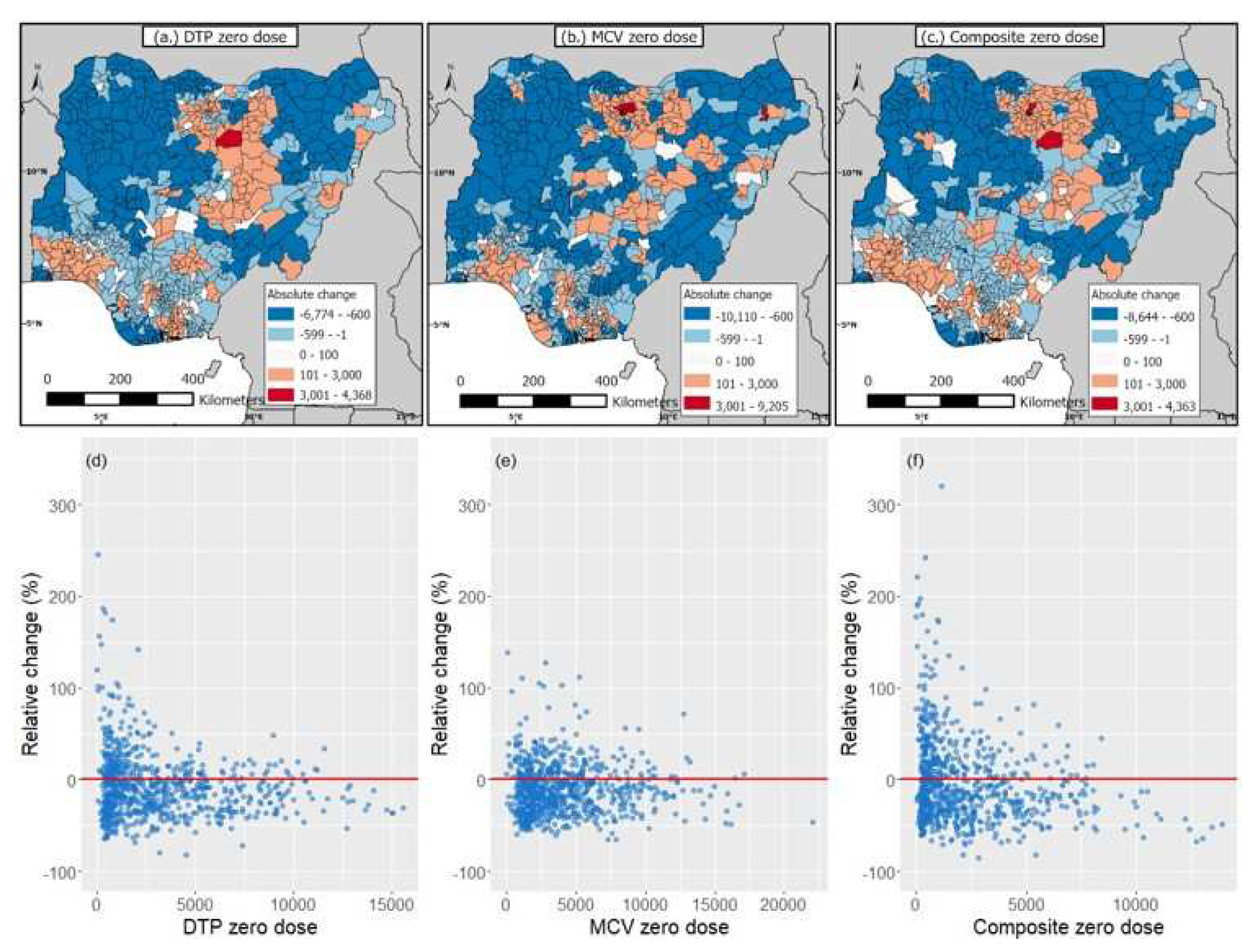
Figure 5.
Adjusted odds ratios (aORs) and corresponding 95% credible intervals (95% CI) showing associations between the risk factors and the composite coverage indicator in the pre-pandemic period in 2018 (DHS) and the pandemic period in 2021 (MICS-NICS) at the national level. The vertical dotted red lines mark the odds ratio of 1. Light blue dots and lines show the aORs and 95% CIs of variables that had significant associations with zero dose. Some upper CIs have been truncated at a value of 5. The definitions of the risk factors and their reference categories are provided in Supplementary Table S1.
Figure 5.
Adjusted odds ratios (aORs) and corresponding 95% credible intervals (95% CI) showing associations between the risk factors and the composite coverage indicator in the pre-pandemic period in 2018 (DHS) and the pandemic period in 2021 (MICS-NICS) at the national level. The vertical dotted red lines mark the odds ratio of 1. Light blue dots and lines show the aORs and 95% CIs of variables that had significant associations with zero dose. Some upper CIs have been truncated at a value of 5. The definitions of the risk factors and their reference categories are provided in Supplementary Table S1.
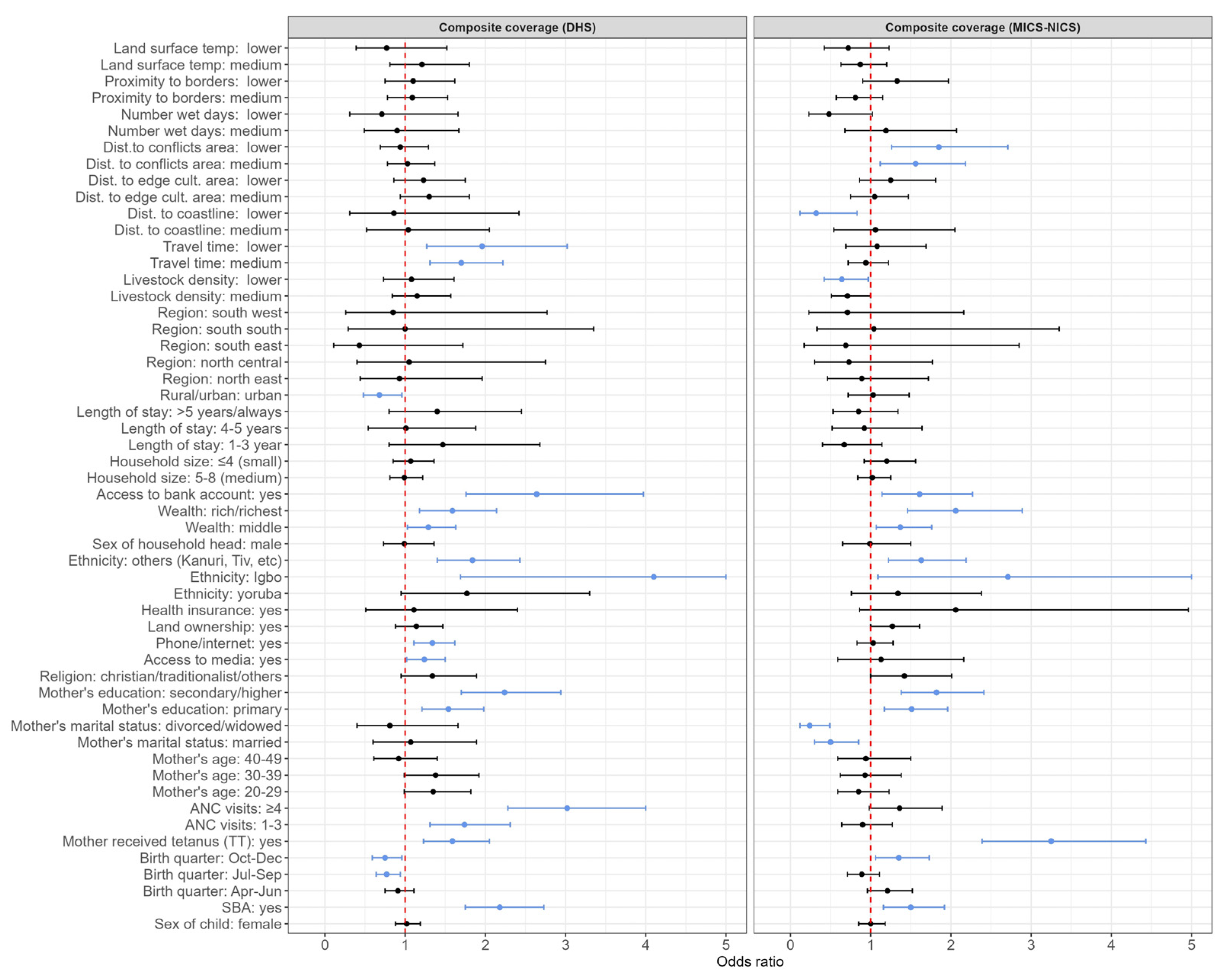
Figure 6.
Summary plots showing the risk factors associated with zero dose before the pandemic in 2018 (DHS) and during the pandemic in 2021 (MICS-NICS) at the (a) national and (b) regional levels, identified using three vaccination coverage indicators, namely DTP1, MCV1, and Composite coverage (CC).
Figure 6.
Summary plots showing the risk factors associated with zero dose before the pandemic in 2018 (DHS) and during the pandemic in 2021 (MICS-NICS) at the (a) national and (b) regional levels, identified using three vaccination coverage indicators, namely DTP1, MCV1, and Composite coverage (CC).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



