
Submitted:
31 October 2023
Posted:
31 October 2023
You are already at the latest version
Abstract
Radiotherapy for cancer has been known to affect the responses of immune cells, especially those of CD8+ T cells that play a pivotal role in anti-tumor immunity. Clinical success of immune checkpoint inhibitors led to an increasing interest into the ability of radiation to modulate CD8+ T cell responses. Recent studies that carefully analyzed the CD8+ T cell responses following radiotherapy suggest the beneficial roles of radiotherapy on anti-tumor immunity. In addition, numerous clinical trials that evaluate the efficacy of combining radiotherapy with immune checkpoint inhibitors are undergoing. In this review, we summarize the current status of knowledge regarding the changes of CD8+ T cells following radiotherapy from various preclinical and clinical studies. Furthermore, key biologic mechanisms that underlie such modulation, including both direct and indirect effects, are described. Lastly, we discuss the current evidence and essential considerations for harnessing radiotherapy as a combination partner for immune checkpoint inhibitors.
Keywords:
radiotherapy
; CD8+ T cells
; immune checkpoint inhibitors
1. Introduction
Radiotherapy (RT) is one of the major pillars of anti-cancer therapies and used for treatment of patients with various cancer types. Radiation brings about a cascade of molecular events within tumor cells, primarily by causing DNA double-strand breaks [1], that ultimately result in the mitotic death of the cells. Harnessing the mechanisms of direct tumor cell killing, approximately 60% of patients with cancer, including newly diagnosed and recurrent cancer, undergo RT with the aims of eradicating the tumor, preventing relapses, or relieving symptoms induced by tumors.
In addition to the ability of RT to achieve local control of the irradiated tumor, dozens of cases with response in unirradiated tumors, which is called an abscopal effect, have been reported to date [2]. First described in 1953 [3], the abscopal effect is now understood as an immune cell-mediated phenomenon; following the study that reported the difference in tumor susceptibility to RT between T-cell competent and T-cell depleted mice [4], a number of studies showed a direct linkage between the abscopal effect and mechanisms involving immune cells [5,6,7]. Although the abscopal effect after RT without any systemic treatment is rarely seen, the advent of immune checkpoint inhibitors (ICIs), which amplify anti-tumor immune responses by blocking negative immune regulators such as PD-1 and CTLA-4, has significantly heightened interest in the synergy between RT and ICIs, due to the capacity of RT to induce anti-tumor immune responses.
Among the myriad of immune cell populations that participate in anti-tumor or pro-tumor immune responses, CD8+ T cells are one of the most extensively investigated population in the context of cancer-related immunity. Furthermore, CD8+ T cells play pivotal roles in driving anti-tumor effects of ICIs, as evidenced by both preclinical and clinical studies [8,9]. Being part of adaptive immune system, CD8+ T cells are specialized in recognizing specific peptide epitopes loaded on the major histocompatibility complex (MHC) class I molecules. CD8+ T cells are heterogeneous population with diverse repertoire and recent analyses utilizing single-cell sequencing technologies have introduced deeper insights into the complexity of CD8+ T cells.
Given the importance of CD8+ T cells in anti-tumor immunity, growing number of preclinical and clinical studies are exploring the portraits of CD8+ T cell responses induced by RT. In this review, we first briefly address the key features and roles of CD8+ T cells in cancer. Then, we describe how CD8+ T cells respond to RT based on the evidence from animal studies and cancer patients. We also describe the mechanisms that underlies the responses of CD8+ T cells upon RT. Based on the evidence, we discuss how the alteration of CD8+ T cells induced by RT may be harnessed in the era of immunotherapy.
2. Features and Roles of CD8+ T Cells in Cancer
CD8+ T cells play crucial roles in anti-tumor immunity, owing to the cytoplasmic localization of a majority of neoantigens and tumor-associated antigens, collectively referred to as tumor antigens. Because of the universal expression pattern of MHC class I molecules, tumor-specific CD8+ T cells can recognize epitopes loaded on both tumor cells and antigen-presenting cells; meanwhile, some tumor cells lose MHC class I molecules on their surface, assisting tumor cells to evade from elimination by CD8+ T cells [10]. Type 1 conventional dendritic cells (cDC1s) are responsible for priming tumor-specific CD8+ T cells at tumor-draining lymph nodes (TDLNs) [11]. The stimulated tumor-specific CD8+ T cells get in to the circulation, infiltrate into the tumor microenvironment, and encounter tumor cells. Upon encounter with tumor cells, CD8+ T cells secrete proinflammatory cytokines, including interferon-γ, and cytolytic enzymes, such as granzymes and perforin, which induce apoptosis of the target cells.
Persistence of tumor cells leads to continuous T cell receptor (TCR) signaling within tumor-specific CD8+ T cells, ultimately rendering these cells dysfunctional through a process termed exhaustion. Exhausted CD8+ T cells are characterized by expression of multiple inhibitory immune checkpoint receptors, such as PD-1, Tim-3, Lag-3, and TIGIT, and significant impairment in their effector functions [12]. The exhaustion process cannot be reversed due to their epigenetically fixed status [13]. Despite their compromised function, the exhausted CD8+ T cells contribute to the anti-tumor activity within tumor [14]. Indeed, increase in the exhausted CD8+ T cells following ICIs is associated with better clinical response [15].
Recent advances in single-cell profiling technology have allowed to observe the detailed portraits of CD8+ tumor infiltrating lymphocytes (TIL). For example, CD8+ TILs with interferon-stimulated gene signature or stress response genes, and those with NK-like features including expression of killer cell immunoglobulin-like receptor have been identified [16,17]. Subset of CD8+ T cells produces IL-17 that promotes the exhaustion of CD8+ TILs and subsequent tumor progression [18]. Subpopulation among CD8+ T cell with immunosuppressive roles has been reported in autoimmune and infectious diseases [19], but their existence and functions in the context of cancer have not been investigated.
3. Changes of CD8+ T Cells Following RT
3.1. Evidence for CD8+ T Cell Responses by RT
CD8+ T cells are considered to be primarily responsible for the abscopal effect of RT. Activation of circulating CD8+ T cells and infiltration of CD8+ T cells in tumor microenvironment of tumor-bearing mice were increased by local RT [20,21,22,23,24,25,26,27]. Importantly, CD8+ T cell population specific tumor antigen were expanded by local RT in murine tumor models [25,28,29,30]. Moreover, local RT also increases the cytokine and cytolytic enzyme production of CD8+ TILs [23,29,30]. Accordingly, in vivo depletion of CD8+ T cells was found to hamper the anti-tumor effects of RT and preclude the occurrence of the abscopal effect [28,31,32,33].
Studies using clinical samples also support the activation of CD8+ T cells, possibly including tumor-specific cells, by RT. Chow et al. convincingly described the activation of anti-tumor CD8+ T cells by RT [34]. They harnessed blood and tissue samples of patients with renal cell carcinoma undergoing preoperative SBRT with 15 Gy in a single fraction. Using TCR-sequencing of CD8+ T cells from tumor and peripheral blood, the authors showed the increase of tumor-enriched clonotypes among circulating CD8+ T cell pool after irradiation, suggesting that systemic anti-tumor responses are induced by local RT in the immunologically hot tumor.
Responses of circulating CD8+ T cells following stereotactic body radiotherapy (SBRT) in early-stage non-small cell lung cancer (NSCLC) were evaluated in two studies. Zhang et al. analyzed 6 patients with stage I NSCLC undergoing SBRT with daily dose of 6 Gy or 8 Gy, and showed that the proportion of CD8+ T cells among immune cells and production of proinflammatory cytokines by CD8+ T cells after in vitro stimulation was significantly increased by SBRT [35]. Similarly, a study by Gkika et al. that examined 50 early-stage NSCLC patients treated with ablative dose of SBRT demonstrated that expression levels of Ki-67 and IFN-γ in CD8+ T cells were significantly increased following SBRT, although the absolute count of CD8+ T cells was diminished [36]. Notably, these changes were observed only in patients who were treated with SBRT with a daily dose of 10 Gy or lower. Kim et al. analyzed the circulating CD8+ T cells from patients with locally advanced NSCLC and found that proliferation of circulating CD8+ T cells and relative frequency of CD39+ tumor-specific cells among circulating CD8+ T cells were increased by concurrent chemoradiotherapy (CCRT) [37]. Analyses on tumor samples of NSCLC also showed that CD8+ TILs were also increased following CCRT [38,39,40].
Activation of CD8+ T cells by RT was also observed in patients with localized or metastatic prostate cancer. In a study by Evans et al., SBRT to oligometastatic lesions of prostate cancer with various dose-fractionation schedules with daily dose of 10 Gy or higher increased tumor-reactive CD8+ T cells, defined by the expression of CD11a, in the peripheral blood [41]. Similarly, another study showed that circulating CD8+ T cells reactive to tumor-associated antigens were increased in two prostate cancer patients at 1 month after RT [42]. Palermo et al. compared the effects of varying RT schemes, including SBRT, hypofractionated RT, and conventionally fractionated RT, and revealed that proportion of CD8+ T cells among circulating T cells was increased after RT regardless of the RT scheme [43]. Notably, effector memory CD8+ T cells and VISTA-expressing CD8+ T cells were increased only in patients undergoing SBRT. Interestingly, Hoffmann et al. demonstrated that the decrease of circulating CD45RA+CD28- effector CD8+ T cells after conventionally fractionated RT was correlated with higher dose to pelvic bone marrow or blood vessels [44], indicating that both daily dose and irradiated site may be associated with the responses of CD8+ T cells following RT. In contrast, the infiltration of CD8+ T cells in prostatic tumors was decreased 2 weeks after SBRT to the prostate in a study of 6 patients [45].
Explorations in cervical cancer also provide insights into how CD8+ T cells respond to RT. Studies have shown that CCRT induces increased clonality [46] and proportion of HPV-specific clonotypes [47] among circulating T cells. A study by Li et al. showed that PD-1+ CD8+ T cells, which are known to be enriched for tumor-specific cells, are expanded in circulation following CCRT [48], while another study demonstrated a decrease in the PD-1+ CD8+ T cell population [46]. On the other hand, infiltration of CD8+ T cells within cervical cancer was significantly decreased after CCRT [46,49,50]. Additionally, expressions of negative immune checkpoint receptors on CD8+ TILs were decreased [51], while those of activation markers were significantly increased following CCRT [49]. Chen et al. dissected the heterogeneity of CD8+ T cell infiltration by CCRT and showed that the CCRT-mediated increase of CD8+ TILs is associated with intratumoral induction of interferons [52]. Interestingly, naive CD8+ T cells in TDLNs were diminished by CCRT, and CCR5+ CXCR3+ CD8+ T cells in TDLNs were increased after lower total dose (39.6 Gy) but not after higher dose (50 Gy) [53].
In rectal cancer, where neoadjuvant CCRT is provided as a standard-of-care treatment, density of CD8+ TILs was increased after CCRT [54,55,56,57,58,59,60,61,62,63]. Interestingly, the clonal composition of TILs became significantly diverse after CCRT [64]. Similarly, infiltration of CD8+ T cells into tumor was increased following CCRT in esophageal cancer [65,66,67], and responses of circulating T cells to tumor-associated antigens were enhanced following CCRT to esophageal cancer [68]. Increased infiltration of CD8+ T cells following RT was also noted in patients with sarcoma [69,70]. Analysis on peripheral blood from metastatic breast cancer undergoing SBRT to bone metastasis showed that circulating PD-1+ CD8+ T cells were activated following SBRT [71]. In contrast, the amount of stromal CD8+ TILs was decreased following RT in squamous cell carcinoma of oral cavity [72]. Moreover, neoadjuvant CCRT reduced the infiltration of CD8+ T cells in clinical T4 gastric cancer [73].
In summary, majority of the reported data suggest that local RT induces both systemic activation and local expansion of anti-tumor CD8+ T cells. However, some reports examining tumor tissues imply the negative impact of RT on CD8+ T cell responses in local tumor microenvironment. The studies on CD8+ T cell responses using peripheral blood samples and tumor tissues from cancer patients are listed on Table 1 and Table 2, respectively.
3.2. Factors that Influence RT-Induced CD8+ T Cell-Responses
Multiple tumor- or treatment-related factors are considered to be associated with the T-cell responses. First of all, total dose or fraction size may be a crucial factor, as shown by the study of the murine breast cancer model demonstrating decreased immunostimulatory effects in a dose above 12 Gy [74]. Consistent with this concept, a study on early-stage NSCLC patients demonstrated that proliferation of circulating CD8+ T cells was increased by SBRT with daily dose of 10 Gy or less, but not with higher doses [36]. Nonetheless, an analysis on prostate cancer patients and metastatic breast cancer patients did not observe any difference among varying daily doses [43,71], suggesting that the relationship between CD8+ T cell responses and daily dose should be investigated in detail.
Furthermore, various chemotherapeutic agents also have capacity to modulate immune cells. The majority of aforementioned studies, especially those quantified density of CD8+ TILs, investigated the changes of CD8+ T cells by CCRT. Various cytotoxic chemotherapeutic drugs and targeted agents are capable of not only inducing anti-tumor CD8+ T cell responses, but also depleting CD8+ T cells through their direct effects [75]. Since it is impossible to dissect the changes of CD8+ T cells into those resulted from RT and systemic therapies, the studies that analyzed the patients receiving CCRT should be interpreted with extreme caution.
Treatment field is also considered to have an impact on the T-cell responses. Anti-PD-1 blockade is known to provide limited efficacy for metastatic cancer to liver [76,77] or bone [78] owing to the distinct microenvironment. Hence, the irradiated organ or site may also contribute to the T-cell responses following RT. McGee et al. reported that activated memory CD8+ T cells in peripheral blood were expanded by SBRT to parenchymal metastases, but not to brain or bone metastases [79]. Moreover, multiple lines of preclinical evidence suggest that irradiating TDLN has detrimental effects in terms of systemic T cells responses and abscopal effects [29,30,80,81], possibly owing to the lymphodepleting effects of RT. Hence, intentional or unintentional irradiation to regional lymphatics in cancer patients may also affect the responses of CD8+ T cells.
Type of irradiation might also affect the responses of CD8+ T cells. While most of the studies used X-rays for irradiation, few studies have explored the effects of particle beams, such as protons and carbon ions, on the activity of CD8+ T cells. Proton therapy has shown to elicit CD8+ T cell responses and its effect was similar to X-ray irradiation [82,83]. Abscopal response in a sarcoma patient undergoing proton therapy also has been reported [84]. Interestingly, carbon ion irradiation has shown enhanced ability to upregulate calreticulin and increase CD8+ TILs compared to X-ray [85,86]. Despite the lack of comprehensive analyses on the differential effects on CD8+ T cell responses according to type of irradiation, several clinical trials involving particle beam therapy and ICIs are ongoing [87], and their results are strongly awaited.
Last but not least, tumor types and their characteristics are involved in the efficacy of RT to elicit anti-tumor CD8+ T cell responses. For instance, amount of CD8+ TILs was decreased in cervical cancer, but increased in rectal cancer following CCRT in most studies as described above. Moreover, studies using clinical samples are mostly skewed to cancer types that include RT as a definitive or neoadjuvant setting, although some scrutinized the changes of T cells during palliative RT. Therefore, the results of individual studies should be interpreted cautiously and not be generalized into other disease or treatment settings.
4. Mechanisms of RT-Induced T-Cell Responses
4.1. Activation of Innate Immune Cells
Innate immune cells play crucial roles in orchestrating the anti-tumor functions of CD8+ T cells. In the tumor microenvironment, local RT triggers a cascade of responses to modulate innate immune cells. RT induces DNA-sensing pathways, such as cGAS-STING pathway, in host or tumor cells to upregulate the production of type I interferon [74,88,89], which in turn activates tumor-infiltrating dendritic cells (DC) to augment their activity to cross-prime tumor-specific CD8+ T cells [89]. Consequently, infiltration of functional CD8+ T cells into tumor microenvironment is increased after local RT [21]. These findings from animal models are also supported by the increase in plasma level of type I interferons in patients after combination of local RT and ICIs [90]. Vanpouille-Box et al. showed that a single ablative dose (>12 Gy) induces Trex1 that degrades cytosolic DNA molecules, preventing the activation of cGAS-STING pathway, release of type I interferons, and even abscopal effects [74]; these results indicates that the activation of DCs play important roles in promoting CD8+ T cell responses after RT.
Release of soluble factors that stimulate innate immune cells also contributes to the responses of CD8+ T cells. Danger-associated molecular patterns, such as high-mobility group protein B1 (HMGB1), calreticulin and ATP are released following a process called immunogenic cell death [91]. These molecules induce the maturation of DCs, leading to their recruitment and activation. For instance, HMGB1 interacts with TLR4 expressed on the surface of DCs, which subsequently activates NF-κB signaling pathway to promote the activation of DCs [92]. TLR4-deficient mice exhibited remarkable decrease in the infiltration of tumor-specific CD8+ T cells [93]. Additionally, calreticulin exposed to the cell surface promotes phagocytosis of the dying cells [94], rendering innate immune cells to activate CD8+ T cells more proficiently.
RT also generates reactive oxygen species and reactive nitrogen species that are capable of recruiting neutrophils and NK cells [95], which interact with anti-tumor CD8+ T cells [96]. Moreover, RT-induced pyroptosis improve the antigen-presenting function of DCs and infiltration of CD8+ T cells, although the exact mechanisms remain to be clarified [97]. Further studies are needed to gain further insights into various mechanisms underpinning responses of anti-tumor CD8+ T cells mediated by innate immune cells.
4.2. Generation and Release of Tumor Antigens
Tumor antigens include neoantigens that are generated by somatic nonsynonymous mutation, and tumor-associated antigen that are overexpressed in tumor cells compared to normal cells. Expression and immunogenicity of tumor antigens are essential for responses of CD8+ T cells, as evidenced by the increased response rate to ICIs in tumors with high mutational burden [98]. Changes of TCR repertoire of tumor-infiltrating T cells following local RT indicate that antigenicity of tumor cells can be modulated by RT [99,100,101].
Irradiation elevated the intracellular protein levels and, subsequently, activity of the transporter associated with antigen processing, which is involved in the cross-presentation for CD8+ T cells [102]. Of note, irradiation generated a novel set of MHC class I-binding peptides. Upregulation of immunoproteasome subunits, which are involved in the production of peptides with higher binding capacity to MHC class I molecules than standard proteasome, may partly explain the increased neoepitopes following RT [103]. Lhuillier et al. reported a direct evidence that expression of immunogenic neoantigens on murine breast cancer cells is increased by RT [104]. Interestingly, Lussier et al. showed that irradiation induces novel mutations that generate immunogenic epitope for CD8+ T cells in murine sarcoma model [105]. Upregulation of tumor antigens following irradiation in vitro or in vivo has been also reported in other preclinical studies [82,90]. Importantly, expression of tumor-associated antigens, including NY-ESO-1 and CT7, was increased after local RT in patients with sarcoma [69]. Although multiple layers of evidence suggests that tumor antigens are upregulated by RT, the underlying mechanisms remain to be revealed.
4.3. Increased Susceptibility of Tumor Cells to CD8+ T Cell-Mediated Death
Expression of MHC class I molecules on tumor cells is required for CD8+ T cells to kill the tumor cells. Although MHC class I molecules are expressed on all normal nucleated cells, some of cancer cells do not express MHC class I molecules to evade anti-tumor immune reaction [10]. Notably, studies using animal tumor models demonstrated that RT upregulates MHC class I molecules on tumor cells [20,103,106], as a result of increased degradation of cytosolic proteins [102]. Similarly, RT with or without concurrent chemotherapy to cancer patients significantly increased the expression of MHC class I molecules in cancer patients [69]. The mTOR-signaling pathway and NF-κB signaling pathway are responsible for the RT-induced upregulation of MHC class I molecules [103].
Irradiation also enhances the expression of Fas (CD95) on tumor cells [95,104]. When Fas binds to the FasL, which is typically expressed on CD8+ T cells, it activates a cascade of reactions involving caspase that ultimately leads to the apoptosis. The cytolytic activity of tumor-specific CD8+ T cells was decreased when Fas:FasL interaction was blocked [107].
4.4. Recruitment and Retention of CD8+ T Cells
Tumor cells and various tumor-infiltrating immune cells secrete a series of chemokines to recruit immune cells that shape the tumor microenvironment. CD8+ T cells also harness various chemokine receptors expressed on their cell surface to navigate to and remain at the tumor site [108]. Several studies proposed that local RT upregulates the production of chemokines to increase the infiltration of CD8+ T cells. Matsumura et al. showed that irradiation upregulates the expression of CXCL16 that recruits CXCR6+ CD8+ T cells in murine breast cancer model [109]. Importantly, infiltration of CD8+ T cells was decreased in CXCR6-deficient mice with impaired efficacy of local RT. Another study showed that RT-induced production of CXCL10 by lung cancer cells activated CXCR3+ CD8+ T cells [110]. Additionally, expression of CCL22 in nasopharyngeal cancer xenograft models was upregulated by RT, which was associated with the increased infiltration of CD8+ T cells [111]. Enhanced production of other chemokines, including CCL2 [112,113,114], CCL5 [32], CXCL1 [112], and CXCL9 [115], by tumor or normal cells has been reported, yet their roles in regulation of CD8+ T cell trafficking are unknown.
4.5. Direct Induction of Apoptosis
Hematopoietic cells, including CD8+ T cells, are susceptible to radiation-induced cell death. Indeed, the number of CD8+ TILs shortly after RT is reduced, probably by direct effects of radiation, and then restored afterward [116]. Interestingly, sensitivity of CD8+ T cells to radiation differs according to their differentiation status. Tabi et al. showed that naïve and early memory T cells are more sensitive to irradiation-induced apoptosis compared to CD45RA– T cells [42]. Moreover, CD8+ TILs are more radioresistant than CD8+ T cells at circulation or lymphoid tissues and survive following RT to exert anti-tumor activity in a murine tumor model [117]. Since the discrimination between pre-existing and newly infiltrated CD8+ T cells is difficult in human samples, whether tumor-specific CD8+ TILs resist to RT and maintain their anti-tumor functions remains unanswered.5. Combination of RT and ICIs
ICIs exert anti-tumor effects mainly by reinvigorating the functions of exhausted CD8+ T cells and recruiting novel tumor-specific CD8+ T cells from the periphery [118,119]. Based on the aforementioned evidence demonstrating the ability of local RT to provoke responses of CD8+ T cells, local RT has been regarded as a reasonable partner for combination with ICIs [120]. The co-administration of local RT and ICIs is considered tolerable, as reported by numerous clinical works [121,122,123]. Genetic deletion of PD-1 in mice significantly improved the systemic anti-tumor efficacy of RT [124]. Accordingly, multiple preclinical studies using mouse models revealed that RT synergistically augment the efficacy of anti-PD-1/PD-L1 blockade [20,23,125,126,127,128] or anti-CTLA-4 blockade [33,99,129]. Anti-tumor effects of the combination strategies were abolished after in vivo depletion of CD8+ [125,126,130], supporting the CD8+ T cell–mediated mechanisms underpinning the synergism.
Unsurprisingly, CD8+ T cells play a crucial role in the combination strategies of RT and ICIs in cancer patients. Activation of circulating CD8+ T cells was observed in patients with metastatic melanoma showing abscopal response by the combination therapy [131,132]. In a study dissecting the clonal composition of CD8+ T cells in a metastatic melanoma patient undergoing pembrolizumab and brain RT, a proportion of tumor-enriched clonotypes were expanded in peripheral blood after RT [133]. In the clinical trial of RT and anti-CTLA-4 blockade in NSCLC patients, clonal expansion of circulating T cells were more prominent in responders compared to non-responders [90]. Additionally, the expansion of neoantigen-specific CD8+ T cells among circulating CD8+ T cells was observed. Of note, pembrolizumab plus SBRT increased the infiltration of CD8+ T cells, as well as those expressing CD103, more prominently than pembrolizumab alone in patients with metastatic NSCLC [134], suggesting that effects of RT on tumor-specific CD8+ T cells may enhance the anti-tumor activity of ICIs.
Recently, results of the clinical trials assessing the efficacy of adding RT to ICIs have been reported; however, the role of local RT is conflicting across the studies. A pooled analysis of two randomized trials showed that combination of RT and pembrolizumab showed significantly improved survival outcomes compared to pembrolizumab alone in metastatic NSCLC patients [135]. In contrast, addition of SBRT to anti-PD-1 blockade did not provide any benefit for metastatic head and neck squamous cell carcinoma [136] and adenoid cystic carcinoma [137]. Additionally, local RT did not improve the treatment outcomes when added to co-administration of anti-PD-1/PD-L1 and anti-CTLA-4 antibodies in patients with NSCLC [138] and Merkel cell carcinoma [139]. These findings suggest that the incorporation of local RT alongside ICIs does not consistently provide beneficial outcomes.
The impact of local RT on the anti-tumor effects of ICIs may vary across cancer types, regimen of ICIs, and timing and dose-fractionation scheme of RT, which were mostly discussed in the previous section (see section 3.2). Indeed, the responses of tumor-specific CD8+ T cells upon ICIs are different according to the features of tumor microenvironment, especially exhaustion status of tumor-specific CD8+ T cells [15,140]. Moreover, anti-PD-1/PD-L1 and anti-CTLA-4 blocking antibodies elicit distinct cellular responses, not just in CD8+ T cells but also in CD4+ T cells, particularly regulatory CD4+ T cells (TREG cells) [8], which directly regulate the functions of CD8+ TILs. Additionally, Wei et al. recently showed that administration of the first dose of anti-PD-1 antibodies prior to irradiation hampered the abscopal effects of local RT using a mouse tumor model [130]. This phenomenon was owing to the sensitization of CD8+ TILs to RT-induced DNA damage after anti-PD-1 blockade. Hence, optimizing the treatment setting for meaningful benefit of local RT is necessary.
Modulation of other immune cells is also an important factor that determines the combined efficacy of ICIs and RT. A series of reports revealed that blocking PD-1:PD-L1 pathway in TREG cells enhances their suppressive capacity [141,142,143]. Besides, RT has been shown to increase the infiltration of TREG cells into tumor microenvironment and enhance their suppressive functions [144,145,146]. Thus, anti-tumor activity of the combination strategy also depends on how TREG cells are modulated by the therapies, although evidence regarding the association between treatment- or tumor-related factors and responses of TREG cells is scarce. Moreover, phenotypes and functions of various immune cells, including tumor-associated macrophages, NK cells, and dendritic cells, are altered by local RT as well as ICIs [147]. However, impacts of the combination therapy on these immune cells have not been studied in depth. Therefore, further studies as to how the therapies reshape the tumor microenvironment and systemic immunity would provide profound insight regarding the optimal strategy to combine the local RT and ICIs.
6. Conclusions and Future Directions
Current evidence from preclinical and clinical research supports the modulation of local and systemic CD8+ T cell responses by local RT. The changes in anti-tumor CD8+ T cells and their mechanisms are summarized in Figure 1. How clinically relevant factors, such as dose-fractionation schedule, irradiation site, and characteristics of irradiated tumor, impact the CD8+ T cell responses is largely unknown and remains to be elucidated. Moreover, the mechanisms behind the RT-induced CD8+ T cell responses are not fully understood. Recent techniques including single-cell profiling may facilitate the detailed characterization of CD8+ T cell responses and their relationship with key features of tumor or RT. Future works aiming to study the unraveled issues in this field will suggest the optimal RT strategies for evoking anti-tumor CD8+ T cell responses in the era of immunotherapy.
Author Contributions
Conceptualization, S.H.J., I.A.K. and J.S.K.; Data curation, S.H.J., C.S., and K.Y.E.; Writing – original draft preparation, S.H.J.; Writing – review and editing, J.S.K.; Supervision, J.S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The figure was created with BioRender.com.
Conflicts of Interest
We declare that we have no conflict of interest nor any commercial or associative interest that represents a conflict of interest in connection with the work submitted.
References
- Pastink, A.; Eeken, J.C.J.; Lohman, P.H.M. Genomic Integrity and the Repair of Double-Strand DNA Breaks. Mutat. Res. - Fundam. Mol. Mech. Mutagen. 2001, 480–481, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Abuodeh, Y.; Venkat, P.; Kim, S. Systematic Review of Case Reports on the Abscopal Effect. Curr. Probl. Cancer 2016, 40, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Mole, R.H. Whole Body Irradiation; Radiobiology or Medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Slone, H.B.; Peters, L.J.; Milas, L. Effect of Host Immune Capability on Radiocurability and Subsequent Transplantability of a Murine Fibrosarcoma. J. Natl. Cancer Inst. 1979, 63, 1229–1235. [Google Scholar] [CrossRef]
- Chakravarty, P.K.; Alfieri, A.; Thomas, E.K.; Beri, V.; Tanaka, K.E.; Vikram, B.; Guha, C. Flt3-Ligand Administration after Radiation Therapy Prolongs Survival in a Murine Model of Metastatic Lung Cancer. Cancer Res. 1999, 59, 6028–6032. [Google Scholar] [PubMed]
- Camphausen, K.; Moses, M.A.; Ménard, C.; Sproull, M.; Beecken, W.D.; Folkman, J.; O’Reilly, M.S. Radiation Abscopal Antitumor Effect Is Mediated through P53. Cancer Res. 2003, 63, 1990–1993. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Ng, B.; Devitt, M.L.; Babb, J.S.; Kawashima, N.; Liebes, L.; Formenti, S.C. Ionizing Radiation Inhibition of Distant Untreated Tumors (Abscopal Effect) Is Immune Mediated. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.C.; Levine, J.H.; Cogdill, A.P.; Zhao, Y.; Anang, N.A.A.S.; Andrews, M.C.; Sharma, P.; Wang, J.; Wargo, J.A.; Pe’er, D.; et al. Distinct Cellular Mechanisms Underlie Anti-CTLA-4 and Anti-PD-1 Checkpoint Blockade. Cell 2017, 170, 1120–1133.e17. [Google Scholar] [CrossRef]
- Xu, W.; Schenkel, J.M.; Pauken, K.E.; Staupe, R.P.; McGettigan, S.; George, S.M.; Giles, J.R.; Adamow, M.; Wubbenhorst, B.; Kothari, S.; et al. T-Cell Invigoration to Tumour Burden Ratio Associated with Anti-PD-1 Response. Nature 2017, 545, 60–65. [Google Scholar] [CrossRef]
- Sadagopan, A.; Michelakos, T.; Boyiadzis, G.; Ferrone, C.; Ferrone, S. Human Leukocyte Antigen Class I Antigen-Processing Machinery Upregulation by Anticancer Therapies in the Era of Checkpoint Inhibitors A Review. JAMA Oncol. 2022, 8, 462–473. [Google Scholar] [CrossRef]
- Kvedaraite, E.; Ginhoux, F. Human Dendritic Cells in Cancer. Sci. Immunol. 2022, 7, 9409. [Google Scholar] [CrossRef]
- McLane, L.M.; Abdel-Hakeem, M.S.; Wherry, E.J. CD8 T Cell Exhaustion During Chronic Viral Infection and Cancer. Annu. Rev. Immunol. 2019, 37, 457–495. [Google Scholar] [CrossRef]
- Philip, M.; Fairchild, L.; Sun, L.; Horste, E.L.; Camara, S.; Shakiba, M.; Scott, A.C.; Viale, A.; Lauer, P.; Merghoub, T.; et al. Chromatin States Define Tumour-Specific T Cell Dysfunction and Reprogramming. Nature 2017, 545, 452–456. [Google Scholar] [CrossRef]
- LaFleur, M.W.; Nguyen, T.H.; Coxe, M.A.; Miller, B.C.; Yates, K.B.; Gillis, J.E.; Sen, D.R.; Gaudiano, E.F.; Al Abosy, R.; Freeman, G.J.; et al. PTPN2 Regulates the Generation of Exhausted CD8+ T Cell Subpopulations and Restrains Tumor Immunity. Nat. Immunol. 2019, 20, 1335–1347. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Zhang, Y.; Wang, D.; Hu, X.; Zhang, Z. Single-Cell Meta-Analyses Reveal Responses of Tumor-Reactive CXCL13+ T Cells to Immune-Checkpoint Blockade. Nat. cancer 2022, 3, 1123–1136. [Google Scholar] [CrossRef]
- Zheng, L.; Qin, S.; Si, W.; Wang, A.; Xing, B.; Gao, R.; Ren, X.; Wang, L.; Wu, X.; Zhang, J.; et al. Pan-Cancer Single-Cell Landscape of Tumor-Infiltrating T Cells. Science 2021, 374. [Google Scholar] [CrossRef]
- Chu, Y.; Dai, E.; Li, Y.; Han, G.; Pei, G.; Ingram, D.R.; Thakkar, K.; Qin, J.J.; Dang, M.; Le, X.; et al. Pan-Cancer T Cell Atlas Links a Cellular Stress Response State to Immunotherapy Resistance. Nat. Med. 2023, 29, 1550–1562. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Kuen, D.S.; Koh, C.H.; Kim, H.D.; Chang, S.H.; Kim, S.; Jeon, Y.K.; Park, Y.J.; Choi, G.; Kim, J.; et al. Type 17 Immunity Promotes the Exhaustion of CD8 + T Cells in Cancer. J. Immunother. Cancer 2021, 9, e002603. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zaslavsky, M.; Su, Y.; Guo, J.; Sikora, M.J.; van Unen, V.; Christophersen, A.; Chiou, S.-H.; Chen, L.; Li, J.; et al. KIR + CD8 + T Cells Suppress Pathogenic T Cells and Are Active in Autoimmune Diseases and COVID-19. Science 2022. [Google Scholar] [CrossRef]
- Zeng, J.; See, A.P.; Phallen, J.; Jackson, C.M.; Belcaid, Z.; Ruzevick, J.; Durham, N.; Meyer, C.; Harris, T.J.; Albesiano, E.; et al. Anti-PD-1 Blockade and Stereotactic Radiation Produce Long-Term Survival in Mice with Intracranial Gliomas. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 343–349. [Google Scholar] [CrossRef]
- Lim, J.Y.H.; Gerber, S.A.; Murphy, S.P.; Lord, E.M. Type i Interferons Induced by Radiation Therapy Mediate Recruitment and Effector Function of CD8+ T Cells. Cancer Immunol. Immunother. 2014, 63, 259–271. [Google Scholar] [CrossRef]
- Herrera, F.G.; Ronet, C.; de Olza, M.O.; Barras, D.; Crespo, I.; Andreatta, M.; Corria-Osorio, J.; Spill, A.; Benedetti, F.; Genolet, R.; et al. Low-Dose Radiotherapy Reverses Tumor Immune Desertification and Resistance to Immunotherapy. Cancer Discov. 2022, 12, 108–133. [Google Scholar] [CrossRef]
- Ban, Y.; Markowitz, G.J.; Zou, Y.; Ramchandani, D.; Kraynak, J.; Sheng, J.; Lee, S.B.; Wong, S.T.C.; Altorki, N.K.; Gao, D.; et al. Radiation-Activated Secretory Proteins of Scgb1a1 + Club Cells Increase the Efficacy of Immune Checkpoint Blockade in Lung Cancer. Nat. Cancer 2021, 2, 919–931. [Google Scholar] [CrossRef] [PubMed]
- Blair, T.; Baird, J.; Bambina, S.; Kramer, G.; Gostissa, M.; Harvey, C.J.; Gough, M.J.; Crittenden, M.R. ICOS Is Upregulated on T Cells Following Radiation and Agonism Combined with Radiation Results in Enhanced Tumor Control. Sci. Rep. 2022, 12, 1–13. [Google Scholar] [CrossRef]
- Lugade, A.A.; Moran, J.P.; Gerber, S.A.; Rose, R.C.; Frelinger, J.G.; Lord, E.M. Local Radiation Therapy of B16 Melanoma Tumors Increases the Generation of Tumor Antigen-Specific Effector Cells That Traffic to the Tumor. J. Immunol. 2005, 174, 7516–7523. [Google Scholar] [CrossRef]
- Schmidt, D.R.; Monique, I.; Gramatikov, T.; Sheen, A.; Williams, C.L.; Hurwitz, M.; Dodge, L.E.; Holupka, E.; Kiger Iii, W.S.; Cornwall-Brady, M.R.; et al. Ablative Radiotherapy Improves Survival but Does Not Cure Autochthonous Mouse Models of Prostate and Colorectal Cancer. Commun. Med. 2023, 3, 1–20. [Google Scholar] [CrossRef]
- Han, M.G.; Jang, B.S.; Kang, M.H.; Na, D.; Kim, I.A. PI3Kγδ Inhibitor plus Radiation Enhances the Antitumour Immune Effect of PD-1 Blockade in Syngenic Murine Breast Cancer and Humanised Patient-Derived Xenograft Model. Eur. J. Cancer 2021, 157, 450–463. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Probst, H.C.; Vuong, V.; Landshammer, A.; Muth, S.; Yagita, H.; Schwendener, R.; Pruschy, M.; Knuth, A.; van den Broek, M. Radiotherapy Promotes Tumor-Specific Effector CD8+ T Cells via Dendritic Cell Activation. J. Immunol. 2012, 189, 558–566. [Google Scholar] [CrossRef]
- Marciscano, A.E.; Ghasemzadeh, A.; Nirschl, T.R.; Theodros, D.; Kochel, C.M.; Francica, B.J.; Muroyama, Y.; Anders, R.A.; Sharabi, A.B.; Velarde, E.; et al. Elective Nodal Irradiation Attenuates the Combinatorial Efficacy of Stereotactic Radiation Therapy and Immunotherapy. Clin. Cancer Res. 2018, 24, 5058–5071. [Google Scholar] [CrossRef]
- Buchwald, Z.S.; Nasti, T.H.; Lee, J.; Eberhardt, C.S.; Wieland, A.; Im, S.J.; Lawson, D.; Curran, W.; Ahmed, R.; Khan, M.K. Tumor-Draining Lymph Node Is Important for a Robust Abscopal Effect Stimulated by Radiotherapy. J. Immunother. Cancer 2020, 8, e000867. [Google Scholar] [CrossRef]
- Lee, Y.; Auh, S.L.; Wang, Y.; Burnette, B.; Wang, Y.; Meng, Y.; Beckett, M.; Sharma, R.; Chin, R.; Tu, T.; et al. Therapeutic Effects of Ablative Radiation on Local Tumor Require CD8 + T Cells: Changing Strategies for Cancer Treatment. Blood 2009, 114, 589–595. [Google Scholar] [CrossRef]
- Chen, H.Y.; Xu, L.; Li, L.F.; Liu, X.X.; Gao, J.X.; Bai, Y.R. Inhibiting the CD8+ T Cell Infiltration in the Tumor Microenvironment after Radiotherapy Is an Important Mechanism of Radioresistance. Sci. Rep. 2018, 8, 11934. [Google Scholar] [CrossRef] [PubMed]
- Yoshimoto, Y.; Suzuki, Y.; Mimura, K.; Ando, K.; Oike, T.; Sato, H.; Okonogi, N.; Maruyama, T.; Izawa, S.; Noda, S.E.; et al. Radiotherapy-Induced Anti-Tumor Immunity Contributes to the Therapeutic Efficacy of Irradiation and Can Be Augmented by CTLA-4 Blockade in a Mouse Model. PLoS One 2014, 9, e92572. [Google Scholar] [CrossRef]
- Chow, J.; Hoffend, N.C.; Abrams, S.I.; Schwaab, T.; Singh, A.K.; Muhitch, J.B. Radiation Induces Dynamic Changes to the T Cell Repertoire in Renal Cell Carcinoma Patients. Proc. Natl. Acad. Sci. U. S. A. 2020, 117, 23721–23729. [Google Scholar] [CrossRef]
- Zhang, T.; Yu, H.; Ni, C.; Zhang, T.; Liu, L.; Lv, Q.; Zhang, Z.; Wang, Z.; Wu, D.; Wu, P.; et al. Hypofractionated Stereotactic Radiation Therapy Activates the Peripheral Immune Response in Operable Stage i Non-Small-Cell Lung Cancer. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef]
- Gkika, E.; Firat, E.; Adebahr, S.; Graf, E.; Popp, I.; Radicioni, G.; Lo, S.S.; Nestle, U.; Nicolay, N.H.; Niedermann, G.; et al. Systemic Immune Modulation by Stereotactic Radiotherapy in Early-Stage Lung Cancer. npj Precis. Oncol. 2023, 7, 1–6. [Google Scholar] [CrossRef]
- Kim, K.H.; Pyo, H.; Lee, H.; Oh, D.; Noh, J.M.; Ahn, Y.C.; Yoon, H.I.; Moon, H.; Lee, J.; Park, S.; et al. Dynamics of Circulating Immune Cells During Chemoradiotherapy in Patients with Non-Small Cell Lung Cancer Support Earlier Administration of Anti-PD-1/PD-L1 Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2022, 113, 415–425. [Google Scholar] [CrossRef]
- Yoneda, K.; Kuwata, T.; Kanayama, M.; Mori, M.; Kawanami, T.; Yatera, K.; Ohguri, T.; Hisaoka, M.; Nakayama, T.; Tanaka, F. Alteration in Tumoural PD-L1 Expression and Stromal CD8-Positive Tumour-Infiltrating Lymphocytes after Concurrent Chemo-Radiotherapy for Non-Small Cell Lung Cancer. Br. J. Cancer 2019, 121, 490–496. [Google Scholar] [CrossRef]
- Choe, E.A.; Cha, Y.J.; Kim, J.H.; Pyo, K.H.; Hong, M.H.; Park, S.Y.; Shim, H.S.; Jung, I.; Lee, C.Y.; Cho, B.C.; et al. Dynamic Changes in PD-L1 Expression and CD8+ T Cell Infiltration in Non-Small Cell Lung Cancer Following Chemoradiation Therapy. Lung Cancer 2019, 136, 30–36. [Google Scholar] [CrossRef]
- Shirasawa, M.; Yoshida, T.; Matsumoto, Y.; Shinno, Y.; Okuma, Y.; Goto, Y.; Horinouchi, H.; Yamamoto, N.; Watanabe, S. ichi; Ohe, Y.; et al. Impact of Chemoradiotherapy on the Immune-Related Tumour Microenvironment and Efficacy of Anti-PD-(L)1 Therapy for Recurrences after Chemoradiotherapy in Patients with Unresectable Locally Advanced Non-Small Cell Lung Cancer. Eur. J. Cancer 2020, 140, 28–36. [Google Scholar] [CrossRef]
- Evans, J.D.; Morris, L.K.; Zhang, H.; Cao, S.; Liu, X.; Mara, K.C.; Stish, B.J.; Davis, B.J.; Mansfield, A.S.; Dronca, R.S.; et al. Prospective Immunophenotyping of CD8+ T Cells and Associated Clinical Outcomes of Patients With Oligometastatic Prostate Cancer Treated With Metastasis-Directed SBRT. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 229–240. [Google Scholar] [CrossRef]
- Tabi, Z.; Spary, L.K.; Coleman, S.; Clayton, A.; Mason, M.D.; Staffurth, J. Resistance of CD45RA− T Cells to Apoptosis and Functional Impairment, and Activation of Tumor-Antigen Specific T Cells during Radiation Therapy of Prostate Cancer. J. Immunol. 2010, 185, 1330–1339. [Google Scholar] [CrossRef]
- Palermo, B.; Bottero, M.; Panetta, M.; Faiella, A.; Sperduti, I.; Masi, S.; Frisullo, G.; Foddai, M.L.; Cordone, I.; Nisticò, P.; et al. Stereotactic Ablative Radiation Therapy in 3 Fractions Induces a Favorable Systemic Immune Cell Profiling in Prostate Cancer Patients. Oncoimmunology 2023, 12, 2174721. [Google Scholar] [CrossRef]
- Hoffmann, E.; Paulsen, F.; Schaedle, P.; Zips, D.; Gani, C.; Rammensee, H.G.; Gouttefangeas, C.; Eckert, F. Radiotherapy Planning Parameters Correlate with Changes in the Peripheral Immune Status of Patients Undergoing Curative Radiotherapy for Localized Prostate Cancer. Cancer Immunol. Immunother. 2022, 71, 541–552. [Google Scholar] [CrossRef]
- Kane, N.; Romero, T.; Diaz-Perez, S.; Rettig, M.B.; Steinberg, M.L.; Kishan, A.U.; Schaue, D.; Reiter, R.E.; Knudsen, B.S.; Nickols, N.G. Significant Changes in Macrophage and CD8 T Cell Densities in Primary Prostate Tumors 2 Weeks after SBRT. Prostate Cancer Prostatic Dis. 2023, 26, 207–209. [Google Scholar] [CrossRef]
- Li, R.; Liu, Y.; Yin, R.; Yin, L.; Li, K.; Sun, C.; Zhou, Z.; Li, P.; Tong, R.; Xue, J.; et al. The Dynamic Alternation of Local and Systemic Tumor Immune Microenvironment During Concurrent Chemoradiotherapy of Cervical Cancer: A Prospective Clinical Trial. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 1432–1441. [Google Scholar] [CrossRef]
- Colbert, L.E.; El Alam, M.B.; Lynn, E.J.; Bronk, J.; Karpinets, T. V.; Wu, X.; Chapman, B. V.; Sims, T.T.; Lin, D.; Kouzy, R.; et al. Expansion of Candidate HPV-Specific T Cells in the Tumor Microenvironment during Chemoradiotherapy Is Prognostic in HPV16 Cancers. Cancer Immunol. Res. 2022, 10, 259–271. [Google Scholar] [CrossRef]
- Li, D.; Guan, Y.; Dong, Y.; Wu, J.; Zhang, Y.; Chen, R.; Lin, Y.T.; Fornace, A.J.; Li, H.H.; Yuan, Z. Radiochemotherapy Upregulates Expression of Checkpoint Receptors on Circulating T Cells. Int. J. Radiat. Biol. 2021, 97, 1563–1568. [Google Scholar] [CrossRef]
- Dorta-Estremera, S.; Colbert, L.E.; Nookala, S.S.; Yanamandra, A. V.; Yang, G.; Delgado, A.; Mikkelson, M.; Eifel, P.; Jhingran, A.; Lilie, L.L.; et al. Kinetics of Intratumoral Immune Cell Activation During Chemoradiation for Cervical Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 593–600. [Google Scholar] [CrossRef]
- Mori, Y.; Sato, H.; Kumazawa, T.; Mayang Permata, T.B.; Yoshimoto, Y.; Murata, K.; Noda, S.E.; Kaminuma, T.; Ando, K.; Oike, T.; et al. Analysis of Radiotherapy-Induced Alteration of CD8+ T Cells and PD-L1 Expression in Patients with Uterine Cervical Squamous Cell Carcinoma. Oncol. Lett. 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Herter, J.M.; Kiljan, M.; Kunze, S.; Reinscheid, M.; Ibruli, O.; Cai, J.; Niu, L.; Heßelmann, I.; Trommer, M.; Herter-Sprie, G.S.; et al. Influence of Chemoradiation on the Immune Microenvironment of Cervical Cancer Patients. Strahlentherapie und Onkol. 2023, 199, 121–130. [Google Scholar] [CrossRef]
- Chen, J.; Chen, C.; Zhan, Y.; Zhou, L.; Chen, J.; Cai, Q.; Wu, Y.; Sui, Z.; Zeng, C.; Wei, X.; et al. Heterogeneity of IFN-Mediated Responses and Tumor Immunogenicity in Patients with Cervical Cancer Receiving Concurrent Chemoradiotherapy. Clin. Cancer Res. 2021, 27, 3990–4002. [Google Scholar] [CrossRef]
- Battaglia, A.; Buzzonetti, A.; Martinelli, E.; Fanelli, M.; Petrillo, M.; Ferrandina, G.; Scambia, G.; Fattorossi, A. Selective Changes in the Immune Profile of Tumor-Draining Lymph Nodes After Different Neoadjuvant Chemoradiation Regimens for Locally Advanced Cervical Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 1546–1553. [Google Scholar] [CrossRef]
- Baeten, C.I.M.; Castermans, K.; Lammering, G.; Hillen, F.; Wouters, B.G.; Hillen, H.F.P.; Griffioen, A.W.; Baeten, C.G.M.I. Effects of Radiotherapy and Chemotherapy on Angiogenesis and Leukocyte Infiltration in Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 1219–1227. [Google Scholar] [CrossRef]
- Teng, F.; Mu, D.; Meng, X.; Kong, L.; Zhu, H.; Liu, S.; Zhang, J.; Yu, J. Tumor Infiltrating Lymphocytes (TILs) before and after Neoadjuvant Chemoradiotherapy and Its Clinical Utility for Rectal Cancer. Am. J. Cancer Res. 2015, 5, 2064–2074. [Google Scholar]
- Teng, F.; Meng, X.; Kong, L.; Mu, D.; Zhu, H.; Liu, S.; Zhang, J.; Yu, J. Tumor-Infiltrating Lymphocytes, Forkhead Box P3, Programmed Death Ligand-1, and Cytotoxic T Lymphocyte-Associated Antigen-4 Expressions before and after Neoadjuvant Chemoradiation in Rectal Cancer. Transl. Res. 2015, 166, 721–732.e1. [Google Scholar] [CrossRef]
- Lim, S.H.S.; Chua, W.; Cheng, C.; Descallar, J.; Ng, W.; Solomon, M.; Bokey, L.; Wong, K.; Lee, M.T.; De Souza, P.; et al. Effect of Neoadjuvant Chemoradiation on Tumor-Infiltrating/Associated Lymphocytes in Locally Advanced Rectal Cancers. Anticancer Res. 2014, 34, 6505–6513. [Google Scholar]
- Shinto, E.; Hase, K.; Hashiguchi, Y.; Sekizawa, A.; Ueno, H.; Shikina, A.; Kajiwara, Y.; Kobayashi, H.; Ishiguro, M.; Yamamoto, J. CD8+ and FOXP3+ Tumor-Infiltrating T Cells before and after Chemoradiotherapy for Rectal Cancer. Ann. Surg. Oncol. 2014, 21, 414–421. [Google Scholar] [CrossRef]
- Lim, Y.J.; Koh, J.; Kim, S.; Jeon, S.R.; Chie, E.K.; Kim, K.; Kang, G.H.; Han, S.W.; Kim, T.Y.; Jeong, S.Y.; et al. Chemoradiation-Induced Alteration of Programmed Death-Ligand 1 and CD8+ Tumor-Infiltrating Lymphocytes Identified Patients With Poor Prognosis in Rectal Cancer: A Matched Comparison Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 1216–1224. [Google Scholar] [CrossRef]
- Cho, H.; Kim, J.E.; Hong, Y.S.; Kim, S.Y.; Kim, J.; Ryu, Y.M.; Kim, S.Y.; Kim, T.W. Comprehensive Evaluation of the Tumor Immune Microenvironment and Its Dynamic Changes in Patients with Locally Advanced Rectal Cancer Treated with Preoperative Chemoradiotherapy: From the Phase II ADORE Study. Oncoimmunology 2022, 11. [Google Scholar] [CrossRef]
- Mirjolet, C.; Charon-Barra, C.; Ladoire, S.; Arbez-Gindre, F.; Bertaut, A.; Ghiringhelli, F.; Leroux, A.; Peiffert, D.; Borg, C.; Bosset, J.F.; et al. Tumor Lymphocyte Immune Response to Preoperative Radiotherapy in Locally Advanced Rectal Cancer: The LYMPHOREC Study. Oncoimmunology 2018, 7. [Google Scholar] [CrossRef]
- Ogura, A.; Akiyoshi, T.; Yamamoto, N.; Kawachi, H.; Ishikawa, Y.; Mori, S.; Oba, K.; Nagino, M.; Fukunaga, Y.; Ueno, M. Pattern of Programmed Cell Death-Ligand 1 Expression and CD8-Positive T-Cell Infiltration before and after Chemoradiotherapy in Rectal Cancer. Eur. J. Cancer 2018, 91, 11–20. [Google Scholar] [CrossRef]
- Matsutani, S.; Shibutani, M.; Maeda, K.; Nagahara, H.; Fukuoka, T.; Nakao, S.; Hirakawa, K.; Ohira, M. Significance of Tumor-Infiltrating Lymphocytes before and after Neoadjuvant Therapy for Rectal Cancer. Cancer Sci. 2018, 109, 966–979. [Google Scholar] [CrossRef]
- Akiyoshi, T.; Gotoh, O.; Tanaka, N.; Kiyotani, K.; Yamamoto, N.; Ueno, M.; Fukunaga, Y.; Mori, S. T-Cell Complexity and Density Are Associated with Sensitivity to Neoadjuvant Chemoradiotherapy in Patients with Rectal Cancer. Cancer Immunol. Immunother. 2021, 70, 509–518. [Google Scholar] [CrossRef]
- Kelly, R.J.; Zaidi, A.H.; Smith, M.A.; Omstead, A.N.; Kosovec, J.E.; Matsui, D.; Martin, S.A.; DiCarlo, C.; Day Werts, E.; Silverman, J.F.; et al. The Dynamic and Transient Immune Microenvironment in Locally Advanced Esophageal Adenocarcinoma Post Chemoradiation. Ann. Surg. 2018, 268, 992–999. [Google Scholar] [CrossRef]
- Zhou, S.; Yang, H.; Zhang, J.; Wang, J.; Liang, Z.; Liu, S.; Li, Y.; Pan, Y.; Zhao, L.; Xi, M. Changes in Indoleamine 2,3-Dioxygenase 1 Expression and CD8+ Tumor-Infiltrating Lymphocytes after Neoadjuvant Chemoradiation Therapy and Prognostic Significance in Esophageal Squamous Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 286–294. [Google Scholar] [CrossRef]
- Chen, W.C.; Wu, C.C.; Chen, Y.H.; Lee, J.Y.; Wang, Y.K.; Wu, N.S.; Wu, M.T.; Wu, I.C. Change in PD-L1 and CD8 Expression after Chemoradiotherapy for Esophageal Squamous Cell Carcinoma. Biomedicines 2022, 10, 1888. [Google Scholar] [CrossRef]
- Suzuki, Y.; Mimura, K.; Yoshimoto, Y.; Watanabe, M.; Ohkubo, Y.; Izawa, S.; Murata, K.; Fujii, H.; Nakano, T.; Kono, K. Immunogenic Tumor Cell Death Induced by Chemoradiotherapy in Patients with Esophageal Squamous Cell Carcinoma. Cancer Res. 2012, 72, 3967–3976. [Google Scholar] [CrossRef]
- Sharma, A.; Bode, B.; Studer, G.; Moch, H.; Okoniewski, M.; Knuth, A.; Von Boehmer, L.; Van Den Broek, M. Radiotherapy of Human Sarcoma Promotes an Intratumoral Immune Effector Signature. Clin. Cancer Res. 2013, 19, 4843–4853. [Google Scholar] [CrossRef]
- Keung, E.Z.; Tsai, J.W.; Ali, A.M.; Cormier, J.N.; Bishop, A.J.; Guadagnolo, B.A.; Torres, K.E.; Somaiah, N.; Hunt, K.K.; Wargo, J.A.; et al. Analysis of the Immune Infiltrate in Undifferentiated Pleomorphic Sarcoma of the Extremity and Trunk in Response to Radiotherapy: Rationale for Combination Neoadjuvant Immune Checkpoint Inhibition and Radiotherapy. Oncoimmunology 2018, 7. [Google Scholar] [CrossRef]
- Jeon, S.H.; Jang, B.-S.; Kim, D.-Y.; Kim, J.H.; Shin, E.-C.; Kim, I.A. Dynamic Responses of Circulating T Cells Following Stereotactic Body Radiotherapy for Bone Metastasis in Patients with Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2023, 0. [Google Scholar] [CrossRef]
- Tabachnyk, M.; Distel, L.V.R.; Büttner, M.; Grabenbauer, G.G.; Nkenke, E.; Fietkau, R.; Lubgan, D. Radiochemotherapy Induces a Favourable Tumour Infiltrating Inflammatory Cell Profile in Head and Neck Cancer. Oral Oncol. 2012, 48, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Yang, Y.; Zhang, S.; Su, Z.; Peng, T.; Wang, X.; Zhao, Y.; Li, S. Regulatory T-Cell Density and Cytotoxic T Lymphocyte Density Are Associated with Complete Response to Neoadjuvant Paclitaxel and Carboplatin Chemoradiotherapy in Gastric Cancer. Exp. Ther. Med. 2018, 16, 3813–3820. [Google Scholar] [CrossRef]
- Vanpouille-Box, C.; Alard, A.; Aryankalayil, M.J.; Sarfraz, Y.; Diamond, J.M.; Schneider, R.J.; Inghirami, G.; Coleman, C.N.; Formenti, S.C.; Demaria, S. DNA Exonuclease Trex1 Regulates Radiotherapy-Induced Tumour Immunogenicity. Nat. Commun. 2017, 8, 15618. [Google Scholar] [CrossRef] [PubMed]
- van den Ende, T.; van den Boorn, H.G.; Hoonhout, N.M.; van Etten-Jamaludin, F.S.; Meijer, S.L.; Derks, S.; de Gruijl, T.D.; Bijlsma, M.F.; van Oijen, M.G.H.; van Laarhoven, H.W.M. Priming the Tumor Immune Microenvironment with Chemo(Radio)Therapy: A Systematic Review across Tumor Types. Biochim. Biophys. Acta - Rev. Cancer 2020, 1874, 188386. [Google Scholar] [CrossRef]
- Lee, J.C.; Mehdizadeh, S.; Smith, J.; Young, A.; Mufazalov, I.A.; Mowery, C.T.; Daud, A.; Bluestone, J.A. Regulatory T Cell Control of Systemic Immunity and Immunotherapy Response in Liver Metastasis. Sci. Immunol. 2020, 5, 759. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Green, M.D.; Li, S.; Sun, Y.; Journey, S.N.; Choi, J.E.; Rizvi, S.M.; Qin, A.; Waninger, J.J.; Lang, X.; et al. Liver Metastasis Restrains Immunotherapy Efficacy via Macrophage-Mediated T Cell Elimination. Nat. Med. 2021, 27, 152–164. [Google Scholar] [CrossRef]
- Jiao, S.; Subudhi, S.K.; Aparicio, A.; Ge, Z.; Guan, B.; Miura, Y.; Sharma, P. Differences in Tumor Microenvironment Dictate T Helper Lineage Polarization and Response to Immune Checkpoint Therapy. Cell 2019, 179, 1177–1190. [Google Scholar] [CrossRef]
- McGee, H.M.; Daly, M.E.; Azghadi, S.; Stewart, S.L.; Oesterich, L.; Schlom, J.; Donahue, R.; Schoenfeld, J.D.; Chen, Q.; Rao, S.; et al. Stereotactic Ablative Radiation Therapy Induces Systemic Differences in Peripheral Blood Immunophenotype Dependent on Irradiated Site. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1259–1270. [Google Scholar] [CrossRef]
- Kim, Y.B.; Byun, H.K.; Kim, D.Y.; Ahn, S.J.; Lee, H.S.; Park, W.; Kim, S.S.; Kim, J.H.; Lee, K.C.; Lee, I.J.; et al. Effect of Elective Internal Mammary Node Irradiation on Disease-Free Survival in Women With Node-Positive Breast Cancer: A Randomized Phase 3 Clinical Trial. JAMA Oncol. 2022, 8, 96–105. [Google Scholar] [CrossRef]
- Saddawi-Konefka, R.; O’Farrell, A.; Faraji, F.; Clubb, L.; Allevato, M.M.; Jensen, S.M.; Yung, B.S.; Wang, Z.; Wu, V.H.; Anang, N.A.; et al. Lymphatic-Preserving Treatment Sequencing with Immune Checkpoint Inhibition Unleashes CDC1-Dependent Antitumor Immunity in HNSCC. Nat. Commun. 2022, 13, 1–19. [Google Scholar] [CrossRef]
- Gameiro, S.R.; Malamas, A.S.; Bernstein, M.B.; Tsang, K.Y.; Vassantachart, A.; Sahoo, N.; Tailor, R.; Pidikiti, R.; Guha, C.P.; Hahn, S.M.; et al. Tumor Cells Surviving Exposure to Proton or Photon Radiation Share a Common Immunogenic Modulation Signature, Rendering Them More Sensitive to T Cell-Mediated Killing. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Mirjolet, C.; Nicol, A.; Limagne, E.; Mura, C.; Richard, C.; Morgand, V.; Rousseau, M.; Boidot, R.; Ghiringhelli, F.; Noel, G.; et al. Impact of Proton Therapy on Antitumor Immune Response. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Brenneman, R.J.; Sharifai, N.; Fischer-Valuck, B.; Hassanzadeh, C.; Guzelian, J.; Chrisinger, J.S.A.; Michalski, J.M.; Oppelt, P.; Baumann, B.C. Abscopal Effect Following Proton Beam Radiotherapy in a Patient with Inoperable Metastatic Retroperitoneal Sarcoma. Front. Oncol. 2019, 9, 483523. [Google Scholar] [CrossRef]
- Huang, Y.; Dong, Y.; Zhao, J.; Zhang, L.; Kong, L.; Lu, J.J. Comparison of the Effects of Photon, Proton and Carbon-Ion Radiation on the Ecto-Calreticulin Exposure in Various Tumor Cell Lines. Ann. Transl. Med. 2019, 7, 542–542. [Google Scholar] [CrossRef]
- Zhou, H.; Tu, C.; Yang, P.; Li, J.; Kepp, O.; Li, H.; Zhang, L.; Zhang, L.; Zhao, Y.; Zhang, T.; et al. Carbon Ion Radiotherapy Triggers Immunogenic Cell Death and Sensitizes Melanoma to Anti-PD-1 Therapy in Mice. Oncoimmunology 2022, 11. [Google Scholar] [CrossRef]
- Marcus, D.; Lieverse, R.I.Y.; Klein, C.; Abdollahi, A.; Lambin, P.; Dubois, L.J.; Yaromina, A. Charged Particle and Conventional Radiotherapy: Current Implications as Partner for Immunotherapy. Cancers (Basel). 2021, 13, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Liang, H.; Xu, M.; Yang, X.; Burnette, B.; Arina, A.; Li, X.D.; Mauceri, H.; Beckett, M.; Darga, T.; et al. STING-Dependent Cytosolic DNA Sensing Promotes Radiation-Induced Type I Interferon-Dependent Antitumor Immunity in Immunogenic Tumors. Immunity 2014, 41, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Burnette, B.C.; Liang, H.; Lee, Y.; Chlewicki, L.; Khodarev, N.N.; Weichselbaum, R.R.; Fu, Y.X.; Auh, S.L. The Efficacy of Radiotherapy Relies upon Induction of Type I Interferon-Dependent Innate and Adaptive Immunity. Cancer Res. 2011, 71, 2488–2496. [Google Scholar] [CrossRef]
- Formenti, S.C.; Rudqvist, N.P.; Golden, E.; Cooper, B.; Wennerberg, E.; Lhuillier, C.; Vanpouille-Box, C.; Friedman, K.; Ferrari de Andrade, L.; Wucherpfennig, K.W.; et al. Radiotherapy Induces Responses of Lung Cancer to CTLA-4 Blockade. Nat. Med. 2018, 24, 1845–1851. [Google Scholar] [CrossRef]
- Galluzzi, L.; Vitale, I.; Warren, S.; Adjemian, S.; Agostinis, P.; Martinez, A.B.; Chan, T.A.; Coukos, G.; Demaria, S.; Deutsch, E.; et al. Consensus Guidelines for the Definition, Detection and Interpretation of Immunogenic Cell Death. J. Immunother. Cancer 2020, 8, e000337. [Google Scholar] [CrossRef] [PubMed]
- Ashrafizadeh, M.; Farhood, B.; Eleojo Musa, A.; Taeb, S.; Najafi, M. Damage-Associated Molecular Patterns in Tumor Radiotherapy. Int. Immunopharmacol. 2020, 86, 106761. [Google Scholar] [CrossRef] [PubMed]
- Apetoh, L.; Ghiringhelli, F.; Tesniere, A.; Obeid, M.; Ortiz, C.; Criollo, A.; Mignot, G.; Maiuri, M.C.; Ullrich, E.; Saulnier, P.; et al. Toll-like Receptor 4-Dependent Contribution of the Immune System to Anticancer Chemotherapy and Radiotherapy. Nat. Med. 2007, 13, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Panaretakis, T.; Kepp, O.; Brockmeier, U.; Tesniere, A.; Bjorklund, A.C.; Chapman, D.C.; Durchschlag, M.; Joza, N.; Pierron, G.; Van Endert, P.; et al. Mechanisms of Pre-Apoptotic Calreticulin Exposure in Immunogenic Cell Death. EMBO J. 2009, 28, 578–590. [Google Scholar] [CrossRef] [PubMed]
- Cytlak, U.M.; Dyer, D.P.; Honeychurch, J.; Williams, K.J.; Travis, M.A.; Illidge, T.M. Immunomodulation by Radiotherapy in Tumour Control and Normal Tissue Toxicity. Nat. Rev. Immunol. 2022, 22, 124–138. [Google Scholar] [CrossRef] [PubMed]
- Governa, V.; Trella, E.; Mele, V.; Tornillo, L.; Amicarella, F.; Cremonesi, E.; Muraro, M.G.; Xu, H.; Droeser, R.; Däster, S.R.; et al. The Interplay between Neutrophils and CD8+ T Cells Improves Survival in Human Colorectal Cancer. Clin. Cancer Res. 2017, 23, 3847–3858. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Chen, G.; Wu, L.; Yu, K.N.; Sun, M.; Yang, M.; Jiang, Y.; Jiang, Y.; Xu, Y.; Peng, S.; et al. Ionizing Radiation Triggers the Antitumor Immunity by Inducing Gasdermin E-Mediated Pyroptosis in Tumor Cells. Int. J. Radiat. Oncol. Biol. Phys. 2023, 115, 440–452. [Google Scholar] [CrossRef] [PubMed]
- Havel, J.J.; Chowell, D.; Chan, T.A. The Evolving Landscape of Biomarkers for Checkpoint Inhibitor Immunotherapy. Nat. Rev. Cancer 2019, 19, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Twyman-Saint Victor, C.; Rech, A.J.; Maity, A.; Rengan, R.; Pauken, K.E.; Stelekati, E.; Benci, J.L.; Xu, B.; Dada, H.; Odorizzi, P.M.; et al. Radiation and Dual Checkpoint Blockade Activate Non-Redundant Immune Mechanisms in Cancer. Nature 2015, 520, 373–377. [Google Scholar] [CrossRef]
- Rudqvist, N.P.; Pilones, K.A.; Lhuillier, C.; Wennerberg, E.; Sidhom, J.W.; Emerson, R.O.; Robins, H.S.; Schneck, J.; Formenti, S.C.; Demaria, S. Radiotherapy and CTLA-4 Blockade Shape the TCR Repertoire of Tumor-Infiltrating T Cells. Cancer Immunol. Res. 2018, 6, 139–150. [Google Scholar] [CrossRef]
- Morrow, M.; Vignali, M.; Illidge, T.M.; Robins, H.S.; Dovedi, S.J.; Cheadle, E.J.; Yusko, E.C.; Popple, A.L.; Wilkinson, R.W.; Poon, E.; et al. Fractionated Radiation Therapy Stimulates Antitumor Immunity Mediated by Both Resident and Infiltrating Polyclonal T-Cell Populations When Combined with PD-1 Blockade. Clin. Cancer Res. 2017, 23, 5514–5526. [Google Scholar] [CrossRef]
- Reits, E.A.; Hodge, J.W.; Herberts, C.A.; Groothuis, T.A.; Chakraborty, M.; Wansley, E.K.; Camphausen, K.; Luiten, R.M.; De Ru, A.H.; Neijssen, J.; et al. Radiation Modulates the Peptide Repertoire, Enhances MHC Class I Expression, and Induces Successful Antitumor Immunotherapy. J. Exp. Med. 2006, 203, 1259–1271. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-H.; Ratanachan, D.; Wang, Z.; Hack, J.; Adbulrahman, L.; Shamlin, N.P.; Kalayjian, M.; Nesseler, J.P.; Ganapathy, E.; Nguyen, C.; et al. Adaptation of the Tumor Antigen Presentation Machinery to Ionizing Radiation. J. Immunol. 2023, 211, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Lhuillier, C.; Rudqvist, N.P.; Yamazaki, T.; Zhang, T.; Charpentier, M.; Galluzzi, L.; Dephoure, N.; Clement, C.C.; Santambrogio, L.; Zhou, X.K.; et al. Radiotherapy-Exposed CD8+ and CD4+ Neoantigens Enhance Tumor Control. J. Clin. Invest. 2021, 131. [Google Scholar] [CrossRef] [PubMed]
- Lussier, D.M.; Alspach, E.; Ward, J.P.; Miceli, A.P.; Runci, D.; White, J.M.; Mpoy, C.; Arthur, C.D.; Kohlmiller, H.N.; Jacks, T.; et al. Radiation-Induced Neoantigens Broaden the Immunotherapeutic Window of Cancers with Low Mutational Loads. Proc. Natl. Acad. Sci. U. S. A. 2021, 118. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Schoenhals, J.E.; Li, A.; Valdecanas, D.R.; Ye, H.; Zang, F.; Tang, C.; Tang, M.; Liu, C.G.; Liu, X.; et al. Suppression of Type I IFN Signaling in Tumors Mediates Resistance to Anti-PD-1 Treatment That Can Be Overcome by Radiotherapy. Cancer Res. 2017, 77, 839–850. [Google Scholar] [CrossRef]
- Chakraborty, M.; Abrams, S.I.; Camphausen, K.; Liu, K.; Scott, T.; Coleman, C.N.; Hodge, J.W. Irradiation of Tumor Cells Up-Regulates Fas and Enhances CTL Lytic Activity and CTL Adoptive Immunotherapy. J. Immunol. 2003, 170, 6338–6347. [Google Scholar] [CrossRef] [PubMed]
- Hoch, T.; Schulz, D.; Eling, N.; Gómez, J.M.; Levesque, M.P.; Bodenmiller, B. Multiplexed Imaging Mass Cytometry of the Chemokine Milieus in Melanoma Characterizes Features of the Response to Immunotherapy. Sci. Immunol. 2022, 7, 1692. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, S.; Wang, B.; Kawashima, N.; Braunstein, S.; Badura, M.; Cameron, T.O.; Babb, J.S.; Schneider, R.J.; Formenti, S.C.; Dustin, M.L.; et al. Radiation-Induced CXCL16 Release by Breast Cancer Cells Attracts Effector T Cells. J. Immunol. 2008, 181, 3099–3107. [Google Scholar] [CrossRef]
- Wang, C.L.; Ho, A.S.; Chang, C.C.; Sie, Z.L.; Peng, C.L.; Chang, J.; Cheng, C.C. Radiotherapy Enhances CXCR3highCD8+ T Cell Activation through Inducing IFNγ-Mediated CXCL10 and ICAM-1 Expression in Lung Cancer Cells. Cancer Immunol. Immunother. 2023, 72, 1865–1880. [Google Scholar] [CrossRef]
- Li, H.; Chen, X.; Zeng, W.; Zhou, W.; Zhou, Q.; Wang, Z.; Jiang, W.; Xie, B.; Sun, L.Q. Radiation-Enhanced Expression of CCL22 in Nasopharyngeal Carcinoma Is Associated With CCR4+ CD8 T Cell Recruitment. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 126–139. [Google Scholar] [CrossRef]
- Kalbasi, A.; Komar, C.; Tooker, G.M.; Liu, M.; Lee, J.W.; Gladney, W.L.; Ben-Josef, E.; Beatty, G.L. Tumor-Derived CCL2 Mediates Resistance to Radiotherapy in Pancreatic Ductal Adenocarcinoma. Clin. Cancer Res. 2017, 23, 137–148. [Google Scholar] [CrossRef]
- Mondini, M.; Loyher, P.L.; Hamon, P.; de Thore, M.G.; Laviron, M.; Berthelot, K.; Clemenson, C.; Salomon, B.L.; Combadiere, C.; Deutsch, E.; et al. CCR2-Dependent Recruitment of Tregs and Monocytes Following Radiotherapy Is Associated with TNFa-Mediated Resistance. Cancer Immunol. Res. 2019, 7, 376–387. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Yu, P.; Lin, W.J.; Chen, S.; Hu, X.; Chen, S.; Cheng, J.; Liu, Q.; Yang, Y.; Li, S.; et al. Microglia Drive Transient Insult-Induced Brain Injury by Chemotactic Recruitment of CD8+ T Lymphocytes. Neuron 2023, 111, 696–710. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.C.; Chang, Y.F.; Ho, A.S.; Sie, Z.L.; Chang, J.S.; Peng, C.L.; Chang, C.C. Irradiation Mediates IFNa and CXCl9 Expression in Non-Small Cell Lung Cancer to Stimulate CD8+ t Cells Activity and Migration toward Tumors. Biomedicines 2021, 9, 1349. [Google Scholar] [CrossRef] [PubMed]
- Herter-Sprie, G.S.; Koyama, S.; Korideck, H.; Hai, J.; Deng, J.; Li, Y.Y.; Buczkowski, K.A.; Grant, A.K.; Ullas, S.; Rhee, K.; et al. Synergy of Radiotherapy and PD-1 Blockade in Kras-Mutant Lung Cancer. JCI Insight 2016, 1, 87415. [Google Scholar] [CrossRef]
- Arina, A.; Beckett, M.; Fernandez, C.; Zheng, W.; Pitroda, S.; Chmura, S.J.; Luke, J.J.; Forde, M.; Hou, Y.; Burnette, B.; et al. Tumor-Reprogrammed Resident T Cells Resist Radiation to Control Tumors. Nat. Commun. 2019, 10, 1–13. [Google Scholar] [CrossRef]
- Yost, K.E.; Satpathy, A.T.; Wells, D.K.; Qi, Y.; Wang, C.; Kageyama, R.; McNamara, K.L.; Granja, J.M.; Sarin, K.Y.; Brown, R.A.; et al. Clonal Replacement of Tumor-Specific T Cells Following PD-1 Blockade. Nat. Med. 2019, 25, 1251–1259. [Google Scholar] [CrossRef]
- Callahan, M.K.; Wolchok, J.D. Recruit or Reboot? How Does Anti-PD-1 Therapy Change Tumor-Infiltrating Lymphocytes? Cancer Cell 2019, 36, 215–217. [Google Scholar] [CrossRef]
- Jagodinsky, J.C.; Harari, P.M.; Morris, Z.S. The Promise of Combining Radiation Therapy With Immunotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 6–16. [Google Scholar] [CrossRef]
- Luke, J.J.; Onderdonk, B.E.; Bhave, S.R.; Karrison, T.; Lemons, J.M.; Chang, P.; Zha, Y.; Carll, T.; Krausz, T.; Huang, L.; et al. Improved Survival Associated with Local Tumor Response Following Multisite Radiotherapy and Pembrolizumab: Secondary Analysis of a Phase I Trial. Clin. Cancer Res. 2020, 26, 6437–6444. [Google Scholar] [CrossRef] [PubMed]
- Parikh, A.R.; Szabolcs, A.; Allen, J.N.; Clark, J.W.; Wo, J.Y.; Raabe, M.; Thel, H.; Hoyos, D.; Mehta, A.; Arshad, S.; et al. Radiation Therapy Enhances Immunotherapy Response in Microsatellite Stable Colorectal and Pancreatic Adenocarcinoma in a Phase II Trial. Nat. Cancer 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Voorwerk, L.; Slagter, M.; Horlings, H.M.; Sikorska, K.; van de Vijver, K.K.; de Maaker, M.; Nederlof, I.; Kluin, R.J.C.; Warren, S.; Ong, S.F.; et al. Immune Induction Strategies in Metastatic Triple-Negative Breast Cancer to Enhance the Sensitivity to PD-1 Blockade: The TONIC Trial. Nat. Med. 2019, 25, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Park, S.S.; Dong, H.; Liu, X.; Harrington, S.M.; Krco, C.J.; Grams, M.P.; Mansfield, A.S.; Furutani, K.M.; Olivier, K.R.; Kwon, E.D. PD-1 Restrains Radiotherapy-Induced Abscopal Effect. Cancer Immunol. Res. 2015, 3, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired Resistance to Fractionated Radiotherapy Can Be Overcome by Concurrent PD-L1 Blockade. Cancer Res. 2014, 74, 5458–5468. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Liang, H.; Burnette, B.; Beckett, M.; Darga, T.; Weichselbaum, R.R.; Fu, Y.X. Irradiation and Anti-PD-L1 Treatment Synergistically Promote Antitumor Immunity in Mice. J. Clin. Invest. 2014, 124, 687–695. [Google Scholar] [CrossRef]
- Gong, X.; Li, X.; Jiang, T.; Xie, H.; Zhu, Z.; Zhou, F.; Zhou, C. Combined Radiotherapy and Anti–PD-L1 Antibody Synergistically Enhances Antitumor Effect in Non–Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 1085–1097. [Google Scholar] [CrossRef]
- Azad, A.; Yin Lim, S.; D’Costa, Z.; Jones, K.; Diana, A.; Sansom, O.J.; Kruger, P.; Liu, S.; McKenna, W.G.; Dushek, O.; et al. PD -L1 Blockade Enhances Response of Pancreatic Ductal Adenocarcinoma to Radiotherapy. EMBO Mol. Med. 2017, 9, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Dewan, M.Z.; Galloway, A.E.; Kawashima, N.; Dewyngaert, J.K.; Babb, J.S.; Formenti, S.C.; Demaria, S. Fractionated but Not Single-Dose Radiotherapy Induces an Immune-Mediated Abscopal Effect When Combined with Anti-CTLA-4 Antibody. Clin. Cancer Res. 2009, 15, 5379–5388. [Google Scholar] [CrossRef]
- Wei, J.; Montalvo-Ortiz, W.; Yu, L.; Krasco, A.; Ebstein, S.; Cortez, C.; Lowy, I.; Murphy, A.J.; Sleeman, M.A.; Skokos, D. Sequence of APD-1 Relative to Local Tumor Irradiation Determines the Induction of Abscopal Antitumor Immune Responses. Sci. Immunol. 2021, 6, 117. [Google Scholar] [CrossRef]
- Postow, M.A.; Callahan, M.K.; Barker, C.A.; Yamada, Y.; Yuan, J.; Kitano, S.; Mu, Z.; Rasalan, T.; Adamow, M.; Ritter, E.; et al. Immunologic Correlates of the Abscopal Effect in a Patient with Melanoma. N. Engl. J. Med. 2012, 366, 925–931. [Google Scholar] [CrossRef]
- Watanabe, T.; Firat, E.; Scholber, J.; Gaedicke, S.; Heinrich, C.; Luo, R.; Ehrat, N.; Multhoff, G.; Schmitt-Graeff, A.; Grosu, A.L.; et al. Deep Abscopal Response to Radiotherapy and Anti-PD-1 in an Oligometastatic Melanoma Patient with Unfavorable Pretreatment Immune Signature. Cancer Immunol. Immunother. 2020, 69, 1823–1832. [Google Scholar] [CrossRef]
- Wieland, A.; Kamphorst, A.O.; Adsay, N.V.; Masor, J.J.; Sarmiento, J.; Nasti, T.H.; Darko, S.; Douek, D.C.; Xue, Y.; Curran, W.J.; et al. T Cell Receptor Sequencing of Activated CD8 T Cells in the Blood Identifies Tumor-Infiltrating Clones That Expand after PD-1 Therapy and Radiation in a Melanoma Patient. Cancer Immunol. Immunother. 2018, 67, 1767–1776. [Google Scholar] [CrossRef] [PubMed]
- Van Der Woude, L.L.; Gorris, M.A.J.; Wortel, I.M.N.; Creemers, J.H.A.; Verrijp, K.; Monkhorst, K.; Grünberg, K.; Van Den Heuvel, M.M.; Textor, J.; Figdor, C.G.; et al. Tumor Microenvironment Shows an Immunological Abscopal Effect in Patients with NSCLC Treated with Pembrolizumab-Radiotherapy Combination. J. Immunother. Cancer 2022, 10, e005248. [Google Scholar] [CrossRef]
- Theelen, W.S.M.E.; Chen, D.; Verma, V.; Hobbs, B.P.; Peulen, H.M.U.; Aerts, J.G.J.V.; Bahce, I.; Niemeijer, A.L.N.; Chang, J.Y.; de Groot, P.M.; et al. Pembrolizumab with or without Radiotherapy for Metastatic Non-Small-Cell Lung Cancer: A Pooled Analysis of Two Randomised Trials. Lancet Respir. Med. 2021, 9, 467–475. [Google Scholar] [CrossRef]
- McBride, S.; Sherman, E.; Jillian Tsai, C.; Baxi, S.; Aghalar, J.; Eng, J.; Zhi, W.I.; McFarland, D.; Michel, L.S.; Young, R.; et al. Randomized Phase II Trial of Nivolumab with Stereotactic Body Radiotherapy versus Nivolumab Alone in Metastatic Head and Neck Squamous Cell Carcinoma. J. Clin. Oncol. 2021, 39, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, U.; Bang, A.; Chen, Y.H.; Mak, R.H.; Lorch, J.H.; Hanna, G.J.; Nishino, M.; Manuszak, C.; Thrash, E.M.; Severgnini, M.; et al. A Randomized Phase 2 Study of Pembrolizumab With or Without Radiation in Patients With Recurrent or Metastatic Adenoid Cystic Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 134–144. [Google Scholar] [CrossRef]
- Schoenfeld, J.D.; Giobbie-Hurder, A.; Ranasinghe, S.; Kao, K.Z.; Lako, A.; Tsuji, J.; Liu, Y.; Brennick, R.C.; Gentzler, R.D.; Lee, C.; et al. Durvalumab plus Tremelimumab Alone or in Combination with Low-Dose or Hypofractionated Radiotherapy in Metastatic Non-Small-Cell Lung Cancer Refractory to Previous PD(L)-1 Therapy: An Open-Label, Multicentre, Randomised, Phase 2 Trial. Lancet Oncol. 2022, 23, 279–291. [Google Scholar] [CrossRef]
- Kim, S.; Wuthrick, E.; Blakaj, D.; Eroglu, Z.; Verschraegen, C.; Thapa, R.; Mills, M.; Dibs, K.; Liveringhouse, C.; Russell, J.; et al. Combined Nivolumab and Ipilimumab with or without Stereotactic Body Radiation Therapy for Advanced Merkel Cell Carcinoma: A Randomised, Open Label, Phase 2 Trial. Lancet 2022, 400, 1008–1019. [Google Scholar] [CrossRef]
- Liu, B.; Hu, X.; Feng, K.; Gao, R.; Xue, Z.; Zhang, S.; Zhang, Y.; Corse, E.; Hu, Y.; Han, W.; et al. Temporal Single-Cell Tracing Reveals Clonal Revival and Expansion of Precursor Exhausted T Cells during Anti-PD-1 Therapy in Lung Cancer. Nat. Cancer 2021, 1–14. [Google Scholar] [CrossRef]
- Kamada, T.; Togashi, Y.; Tay, C.; Ha, D.; Sasaki, A.; Nakamura, Y.; Sato, E.; Fukuoka, S.; Tada, Y.; Tanaka, A.; et al. PD-1+ Regulatory T Cells Amplified by PD-1 Blockade Promote Hyperprogression of Cancer. Proc. Natl. Acad. Sci. U. S. A. 2019, 116, 9999–10008. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.L.; Kuchroo, J.R.; Sage, P.T.; Liang, D.; Francisco, L.M.; Buck, J.; Thaker, Y.R.; Zhang, Q.; McArdel, S.L.; Juneja, V.R.; et al. PD-1 Restraint of Regulatory T Cell Suppressive Activity Is Critical for Immune Tolerance. J. Exp. Med. 2021, 218. [Google Scholar] [CrossRef]
- Kumagai, S.; Togashi, Y.; Kamada, T.; Sugiyama, E.; Nishinakamura, H.; Takeuchi, Y.; Vitaly, K.; Itahashi, K.; Maeda, Y.; Matsui, S.; et al. The PD-1 Expression Balance between Effector and Regulatory T Cells Predicts the Clinical Efficacy of PD-1 Blockade Therapies. Nat. Immunol. 2020, 21, 1346–1358. [Google Scholar] [CrossRef] [PubMed]
- Muroyama, Y.; Nirschl, T.R.; Kochel, C.M.; Lopez-Bujanda, Z.; Theodros, D.; Mao, W.; Carrera-Haro, M.A.; Ghasemzadeh, A.; Marciscano, A.E.; Velarde, E.; et al. Stereotactic Radiotherapy Increases Functionally Suppressive Regulatory T Cells in the Tumor Microenvironment. Cancer Immunol. Res. 2017, 5, 992–1004. [Google Scholar] [CrossRef] [PubMed]
- Son, C.H.; Bae, J.H.; Shin, D.Y.; Lee, H.R.; Jo, W.S.; Yang, K.; Park, Y.S. Combination Effect of Regulatory T-Cell Depletion and Ionizing Radiation in Mouse Models of Lung and Colon Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Han, M.G.; Wee, C.W.; Kang, M.H.; Kim, M.J.; Jeon, S.H.; Kim, I.A. Combination of OX40 Co-Stimulation, Radiotherapy, and PD-1 Inhibition in a Syngeneic Murine Triple-Negative Breast Cancer Model. Cancers (Basel). 2022, 14, 2692. [Google Scholar] [CrossRef]
- Weichselbaum, R.R.; Liang, H.; Deng, L.; Fu, Y.X. Radiotherapy and Immunotherapy: A Beneficial Liaison? Nat. Rev. Clin. Oncol. 2017, 14, 365–379. [Google Scholar] [CrossRef]
Figure 1.
Summary for key features of radiotherapy-induced changes of anti-tumor CD8+ T cells and their underlying mechanisms.
Figure 1.
Summary for key features of radiotherapy-induced changes of anti-tumor CD8+ T cells and their underlying mechanisms.
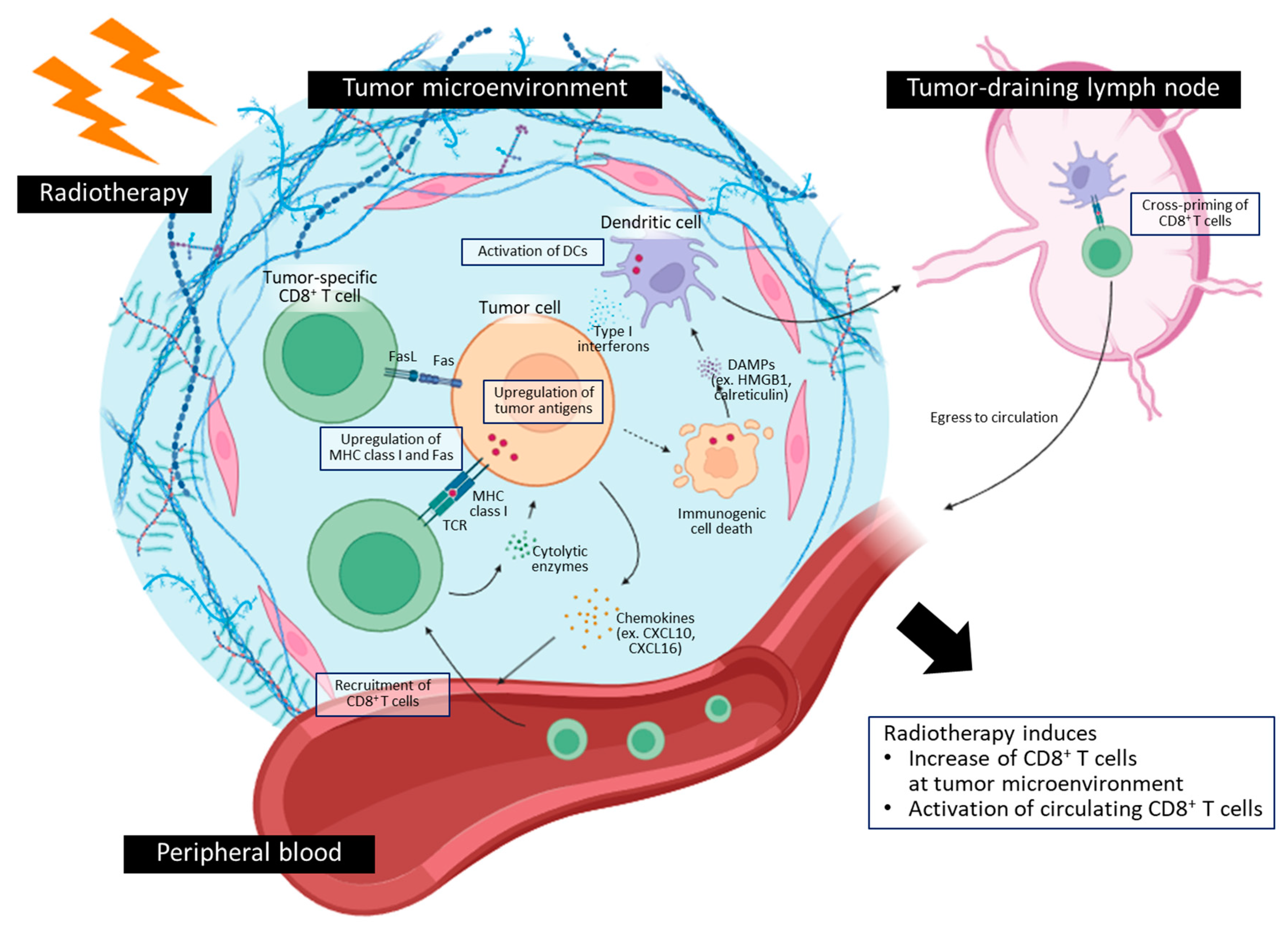

Table 1.
Studies regarding responses of circulating CD8+ T cells following radiotherapy in cancer patients.
Table 1.
Studies regarding responses of circulating CD8+ T cells following radiotherapy in cancer patients.
| Study | Cancer | RT | Systemic therapy | Patients | Findings | Ref |
|---|---|---|---|---|---|---|
| Chow et al. (2020) |
RCC | 15Gy/1fx | No | 11 | - Increase in tumor-enriched clonotypes at 2 weeks after RT | [34] |
| Zhang et al. (2017) |
NSCLC (early stage) |
48Gy/6fx, 48Gy/8fx |
No | 6 | - Increase in inflammatory cytokine production potency at 3 weeks after RT | [35] |
| Gkika et al. (2023) |
NSCLC (early stage) |
45Gy/3fx, 50Gy/5fx, 60Gy/8fx, 66Gy/12fx | No | 50 | - Increase in Ki-67 expression after RT (≤10 Gy/fx) - Increase in IFN-γ production potency during and after RT |
[36] |
| Kim et al. (2022) |
NSCLC (locally advanced) |
66Gy/30fx | Paclitaxel/cisplatin or Paclitaxel/carboplatin |
24 | - Increase in Ki-67 expression at the end of CCRT - Increase in PD-1+CD39+ tumor-specific CD8+ T cells at the end of CCRT |
[37] |
| Evans et al. (2019) |
Prostate ca (oligometastatic) |
16-24Gy/1fx, 30Gy/3fx | Androgen deprivation therapy | 37 | - Decrease in CCR7-CD45RA+ effector CD8+ T cells after RT | [41] |
| Tabi et al. (2010) |
Prostate ca (locally advanced) |
55Gy/20fx | Androgen deprivation therapy | 12 | - Increase in TAA-specific CD8+ T cell responses after RT | [42] |
| Palermo et al. (2023) |
Prostate ca | 40Gy/3fx, 62Gy/20fx, 66-69Gy/30fx |
Androgen deprivation therapy | 18 | - Increase in CCR7+CD45RA- central memory CD8+ T cells during RT - Increase in CCR7-CD45RA- effector memory CD8+ T cells after RT (40Gy/3fx) |
[43] |
| Hoffmann et al. (2022) |
Prostate ca (locally advanced) |
70-78Gy/ 35-39fx |
Androgen deprivation therapy | 18 | - Increase of Ki-67 expression during and after RT | [44] |
| Li et al. (2021) |
Cervical ca (locally advanced) |
50Gy/25fx + 25-36Gy/5-6fx |
Cisplatin | 55 | - Decrease of PD-1+ CD8+ T cells during and after CCRT - Increase in clonality of T cells |
[46] |
| Colbert et al. (2022) |
HPV-positive ca (mostly cervical ca) |
≥45Gy/25fx | Cisplatin | 86 | - Increase in HPV-specific T cells during CCRT | [47] |
| Li et al. (2021) |
Cervical ca or Esophageal ca |
50.4Gy/28fx + 30Gy/5fx (cervical ca) 60Gy/30fx (esophageal ca) |
Cisplatin (cervical ca) Cisplatin/Docetaxel (esophageal ca) |
57 | - Increase in PD-1hi CD8+ T cell during CCRT | [48] |
| Suzuki et al. (2012) |
Esophageal ca | 60-66Gy/ 30-33fx |
Cisplatin-based | 16 | - Increase in TAA-specific CD8+ T cell responses | [68] |
| Jeon et al. (2023) |
Breast ca (metastatic) |
12-20Gy/1fx or 24-27Gy/3fx |
Various (90%) | 30 | - Increase in Ki-67 expression on PD-1+ CD8+ T cells | [71] |
Table 2.
Table 2. Studies regarding responses of tumor-infiltrating CD8+ T cells following radiotherapy in cancer patients.
Table 2.
Table 2. Studies regarding responses of tumor-infiltrating CD8+ T cells following radiotherapy in cancer patients.
| Study | Cancer | RT | Systemic therapy | Patients | Findings | Ref |
|---|---|---|---|---|---|---|
| Yoneda et al. (2019) |
NSCLC (locally advanced) |
Median 60Gy | Platinum doublet | 23 | - Increase in stromal CD8+ TIL density after CCRT | [38] |
| Choe et al. (2019) |
NSCLC (locally advanced) |
40-50Gy | Docetaxel/carboplatin | 43 | - Increase in CD8+ TIL density after CCRT | [39] |
| Shirasawa et al. (2020) |
NSCLC (locally advanced) |
Mostly ≤66 Gy | Platinum doublet, Carboplatin |
14 | - Increase in tumoral CD8+ TIL density after CCRT | [40] |
| Kane et al. (2023) |
Prostate cancer (high-risk) |
24Gy/3fx | No | 6 | - Decrease in CD8+ TIL density after RT | [45] |
| Li et al. (2021) |
Cervical ca (locally advanced) |
50Gy/25fx + 25-36Gy/5-6fx |
Cisplatin | 55 | - Decrease in CD8+ TIL density during and after CCRT | [46] |
| Dorta-Estremera et al. (2018) |
Cervical ca (locally advanced) |
40-45Gy + brachytherapy |
Cisplatin | 20 | - Decrease in CD8+ TIL proportion during CCRT - Increase in Ki-67 expression on CD8+ TIL during CCRT |
[49] |
| Mori et al. (2021) |
Cervical ca (locally advanced) |
50Gy/25fx + 24Gy/4fx (m/c) |
Cisplatin (64%) | 75 | - Decrease in stromal CD8+ TIL density during CCRT (no change in RT alone) | [50] |
| Herter et al. (2023) |
Cervical ca (locally advanced) |
Not documented | Cisplatin, Carboplatin |
22 | - Decrease in expressions of PD-1 and TIGIT on CD8+ TIL after CCRT | [51] |
| Chen et al. (2021) |
Cervical ca (locally advanced) |
46Gy/23fx + 24-32Gy/4-5fx |
Cisplatin, Cisplatin/5-FU |
30 | - No change in CD8+ TIL density during CCRT - Increase in CD8+ TIL density correlated with nuclear IRF1 in tumor cells |
[52] |
| Baeten et al. (2006) |
Rectal ca (locally advanced) |
50.4Gy/28fx, 25Gy/5fx |
Capecitabine, 5-FU (for 50.4Gy/28fx) |
32 | - Increase in CD8+ TIL density after CCRT (25Gy/5fx) | [54] |
| Teng et al. (2015) |
Rectal ca (locally advanced) |
40-45Gy/25-28fx + 5.4Gy boost |
Fluoropyrimidine-based | 103 | - Increase in CD8+ TIL density after CCRT and RT alone | [55] |
| Teng et al. (2015) |
Rectal ca (locally advanced) |
40-45Gy/25-28fx + 5.4Gy boost |
Fluoropyrimidine-based | 62 | - Increase in CD8+ TIL density after CCRT | [56] |
| Lim et al. (2014) |
Rectal ca (locally advanced) |
45-50.4Gy/25-28fx, 25Gy/5fx |
5-FU (long-course) | 52 | - Increase in CD8+ TIL density after CCRT (long-course) | [57] |
| Shinto et al. (2014) |
Rectal ca (locally advanced) |
20Gy/5fx | UFT | 93 | - Increase in stromal CD8+ TIL density after CCRT | [58] |
| Lim et al. (2017) |
Rectal ca (locally advanced) |
Median 50.4Gy/28fx | Capecitabine, 5-FU | 123 | - Increase in CD8+ TIL density after CCRT | [59] |
| Cho et al. (2022) |
Rectal ca (locally advanced) |
Median 50Gy/25fx | Capecitabine, 5-FU | 101 | - Increase in CD8+ TIL density after CCRT | [60] |
| Mirjolet et al. (2018) |
Rectal ca (locally advanced) |
N/D | Fluoropyrimidine-based | 132 | - Increase in CD8+ TIL/Treg ratio after CCRT | [61] |
| Ogura et al. (2018) |
Rectal ca (locally advanced) |
45Gy/25fx, 50.4Gy/28fx |
Capecitabine | 281 | - Increase in stromal CD8+ TIL density after CCRT | [62] |
| Matsutani et al. (2018) |
Rectal ca (locally advanced) |
50.4Gy/28fx | Fluoropyrimidine-based | 31 | - Increase in CD8+ TIL density after CCRT | [63] |
| Akiyoshi et al. (2021) |
Rectal ca (locally advanced) |
45Gy/25fx, 50.4Gy/28fx |
Capecitabine | 65 | - Increase in clonal diversity of TIL after CCRT (poor responders) | [64] |
| Kelly et al. (2018) |
Esophageal ca (locally advanced) |
41.4-54Gy | N/D | 31 | - Increase in CD8+ TIL density after CCRT | [65] |
| Zhou et al. (2020) |
Esophageal ca (locally advanced) |
Median 40Gy (36-46Gy) |
Cisplatin-based | 82 | - Increase in CD8+ TIL density after CCRT | [66] |
| Chen et al. (2022) |
Esophageal ca (locally advanced) |
N/D | N/D | 23 | - Increase in expression of CD8 in tumor after CCRT | [67] |
| Sharma et al. (2013) |
Sarcoma | 50Gy (m/c) | No | 38 | - Increase in CD8+ TIL density after RT | [69] |
| Keung et al. (2018) |
Undifferentiated pleomorphic sarcoma | 50Gy/25fx | Yes (59%; m/c=adrimycin/ifosfamide) |
17 | - Increase in CD8+ TIL density after (CC)RT | [70] |
| Tabachnyk et al. (2012) |
Oral cavity SqCC (locally advanced) |
50.4Gy/28fx | Cisplatin/5-FU | 22 | - Decrease in stromal CD8+ TIL density after CCRT | [72] |
| Huang et al. (2018) |
Gastric ca (locally advanced) |
N/D | Paclitaxel/carboplatin | 68 | - Increase in CD8+ TIL density after CCRT (T2) - Decrease in CD8+ TIL density after CCRT (T4) |
[73] |
Abbreviation: TIL, tumor-infiltrating lymphocyte; N/D, not documented; m/c, most common.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



