
Submitted:
31 October 2023
Posted:
01 November 2023
You are already at the latest version
Abstract
Exudative-pleural-effusion (ePE) is a common presentation in pulmonology clinics. Pleural biopsy is indicated for identifying the aetiology in undiagnosed ePE especially the ones with low adenosine-deaminase levels. The access to rigid and semi-rigid medical thoracoscopy is scarce and heterogeneous in a resource limited country like India. In such circumstances, using flexible bronchoscope via intercostal-chest-tube for visualization of parietal pleura and pleural biopsy offers a way out. Here, in this retrospective study, we have presented our experience of such practice on 25 cases. Mean age was 52.4±1 years. Adhesions were present in 40% of the subjects. Most common finding was presence of nodules. On an average 6.8 passes were taken with maximum of 10. In 32% cases only tiny tissue was obtained, hence requiring multiple passes. Large tissue could be obtained in 44% of the subjects. Mean duration of the procedure was 35.6±9.0 minutes. Tissue diagnosis was established in 80% with most common being malignancy (48%) followed by tuberculosis (20%). In 3 cases, the final diagnosis was made by exclusion. No major complications were recorded. In conclusion, medical thoracoscopy using flexible video bronchoscope via intercostal-chest-tube was a feasible alternative for the diagnosis of ePE effusion in resource limited settings.
Keywords:
Bronchoscope
; Medical Thoracoscopy
; Tuberculosis
; Exudative Pleural Effusion
; Malignant Pleural Effusion
Highlights:
Main Findings:
Medical diagnostic thoracoscopy using flexible bronchoscope via intercostal chest tube has similar diagnostic accuracy and procedure duration as that to semi-rigid thoracoscopy.
No significant complications were observed with the new technique and the overall diagnosis was established in 92% cases.
Implications:
Flexible bronchoscope can be used to perform medical thoracoscopy in a safe and effective manner.
It can be an acceptable alternative for undiagnosed pleural effusions especially in resource limited settings.
Introduction:
Pleural effusion, a common disease in pulmonary medicine, results from a diverse range of causes, including localized pleural or lung diseases, systemic diseases, and drug treatments. Generally pleural effusion related to localized causes are exudative whereas systemic causes lead to transudative nature effusion. Swift identification of the underlying aetiology and initiation of early treatment are key factors determining morbidity and mortality in pleural effusion patients. In India the two most common causes of exudative pleural effusion are tuberculosis and malignant pleural effusion [1]. The commonly employed algorithm for the diagnosis of pleural effusion is to do a diagnostic pleural tap. Bare minimum investigation include total count with differentials, protein & sugar, LDH, ADA (adenosine deaminase) and cytological assessment [2]. However, despite employing appropriate investigations, delineating the aetiology remains a challenge in 20-25% of pleural fluid patients [3]. In such instances, pleural biopsy is considered the gold standard investigative method for establishing a diagnosis. Historically, a blind percutaneous biopsy of the parietal pleura was conducted, which has now been largely supplanted by imaging (USG/CT) guided biopsies or biopsies through diagnostic medical thoracoscopy [4].
In 1910, Swedish internist Hans Christian Jacobeus introduced the concept of thoracoscopy for pulmonary tuberculosis patients to achieve lung expansion via lysis of pleural adhesions [5]. Over last century thoracoscopy has seen remarkable progress in the form of being done under general anaesthesia to a day care procedure in the current era. This minimally invasive outpatient procedure done under conscious sedation and local anaesthesia, generally performed by a pulmonologist, enables exploration of both parietal and visceral pleural surfaces. Furthermore, it allows for biopsy samples to be obtained from the affected site under direct visualization, accounting for its higher diagnostic yield compared to percutaneous/closed or blind pleural biopsy [6].
While historically thoracoscopy was performed using a rigid thoracoscope, the evolution in (diagnostic) medical thoracoscopy led to the advent of semi-rigid thoracoscopes. These devices offer added advantages such as easy manoeuvrability, smaller incision sites, reduced anaesthetic requirements and decreased post-operative pain/discomfort. Despite the invention of medical thoracoscopy a decade back, its accessibility and implementation remain limited in developing nations such as India. This is primarily due to the cost, unavailability of equipment (thoracoscopes) in several tertiary care facilities and a lack of trained physicians [7].
In such circumstances, to obtain pleural biopsy under vision we developed an unconventional technique to perform diagnostic medical thoracoscopy. The department has a functional bronchoscopy suite where flexible video bronchoscopies are routinely conducted, but the equipment for either rigid or semi-rigid bronchoscopy was not available. The study site is a tertiary care hospital where patients in need of pleural biopsy are commonly referred. Closed/blinded or ultrasound guided pleural biopsies were routinely performed, however the yield remained poor. In order to conduct pleural biopsies under vision a new makeshift arrangement was made with the use of intercostal chest tube and flexible bronchoscope. We performed 25 such procedures over a period of approximately one and half year on consenting eligible subjects, following which the department got its first semi-rigid thoracoscope. Here we are reporting our experience with this novel practice.
Material and methods
We conducted a retrospective study in the Department of Pulmonary and Critical Care Medicine at a tertiary care university teaching hospital in northern India. Medical records of all subjects who had undergone diagnostic medical thoracoscopy using a flexible video bronchoscope from January 2018 to August 2019, was retrieved and analysed. Being a retrospective analysis, permission to access the records was sought from the head of the institute (medical superintendent) and consent was waivered off by the biomedical research and ethics committee vide letter number BREC/22/2603 dated 15 December 2022.
Data of all adult patients aged 18 years and above, who had undiagnosed exudative pleural effusion and underwent medical thoracoscopy via a flexible video bronchoscope inserted via an intercostal chest tube, was retrieved and recorded. Prior to the thoracoscopy, each patient underwent a chest ultrasound to identify any pleural adhesion or thickening, and flexible bronchoscopy was performed to identify any intrabronchial growth or obstruction as per the standard protocol. Subjects having extensive adhesions, trapped lung due to pleural thickening were excluded from medical thoracoscopy.
To describe the technique in brief, after obtaining informed consent for the procedure, patients were positioned in the lateral decubitus position. A chest ultrasound was performed to identify the site with maximum pleural fluid thickness, and the skin was sterilized using chlorhexidine. Further after sterilization with povidone iodine, local anaesthesia was administered with 2% lidocaine at and around the marked point. Subsequently a 32 Fr chest tube was inserted through an approximately 1.5 cm chest incision (and blunt dissection). Patients were then sedated with initial boluses of midazolam and fentanyl. A flexible video bronchoscope (Olympus BF-1T180 bronchoscope with CV-180 video processor and CLV-180 light source) was introduced into the pleural space through the intercostal chest tube (ICT) (Figure 1).
After insertion and visualization of pleural cavity the parietal pleura was inspected. Careful handling of the bronchoscope was required in order to avoid excessive bending of the scope outside of the thoracic cavity. Another difficulty faced during the procedure was the holding of the scope near the thoracic cavity, as it was covered by the ICT. Still the navigation of the scope inside the pleural cavity was largely smooth and most of the pleural surfaces could be examined with ease. Following inspection of the parietal pleura, biopsy samples were obtained using Olympus reusable endojaw biopsy forceps FB-20C-1/202C-1. Site of sampling was selected based on the findings of observation. Most biopsies were taken from abnormal looking pleura or the nodules but in few cases with normal pleura random biopsies were also taken. Throughout the procedure, blood pressure, pulse rate, electrocardiogram, and continuous pulse-oximetry were closely monitored. Intermittent boluses of midazolam or fentanyl were also given for conscious sedation at the discretion of the operator. After completion of the procedure, the same chest tube was secured in the pleural cavity through the same port and was attached to a water seal (in a drainage bag). Following the procedure selective cases required parental analgesics in the form of diclofenac or tramadol injections. ICT was kept in situ till the output decreased to less than 100 ml per day. In the case of malignant pleural effusion, pleurodesis was subsequently done using povidone iodine. No antibiotics were administered either during or after thoracoscopy unless indicated and, all manipulations were performed aseptically.
The diagnostic yield and complications were evaluated. We could not evaluate the pain and discomfort related outcome as those were not routinely recorded in the procedure notes. Clinical, demographic, pleural fluid characteristics, radiological findings, hospital stay and thoracoscopic findings were recorded. As we were comparing a modification of diagnostic technique, we specifically focussed on the diagnostic yield of the procedure. Diagnostic yield was measured in the terms of final tissue diagnosis with adequacy of the tissue for molecular analysis (in case of non-squamous non-small cell lung cancer) and sizes of the tissue obtained with the biopsy forceps. As the data with regards to operator ease is not routinely recorded, we used the duration of the procedure as a crude representative. Hospital stay and development of empyema were also analysed to assess the safety of the procedure. Data was collected in paper format initially and later entered in Microsoft Office® excel sheet. After coding in the excel sheet, data was transferred for analysis in SPSS version 26.0 by IBM®. Data was presented in a descriptive fashion as means (and standard deviation) or numbers (percentage with 95% confidence intervals) or medians, depending upon type of variables. We compared the baseline characteristics and other finding among various groups stratified according to either sex, diagnosis, diagnostic yield, or size of tissue obtained. Size of tissue obtained is routinely recorded in following manner- tissue smaller than the cup of the forceps is tiny, just filling the cup completely is moderate and tissue bigger than the size of the cup is labelled as large. Categorical data was compared between the two groups using Pearson Chi-square test, whereas the difference between continuous variables was analysed using independent Student’s t-test. For all outcomes, a two-sided p-value of less than 0.05 was considered to indicate statistical significance.
Results:
Over a period of 18 months, 28 thoracoscopies via flexible bronchoscopes were conducted in the interventional pulmonology suite of the institute, data of 25 of which has been presented here (Figure 2). Most of the subjects were males (56%) and belonged to rural background (64%). Mean age was 52.4±14 years. Majority of the females were housewives (81.8%) and most of the males were farmers (57.1%). 48% subjects had fever at the time of presentation followed by cough and dyspnea (both 28%). Constitutional symptoms were present in majority of cases (loss of appetite in 58% and loss of weight in 40%). Radiological evaluation revealed that left side was most commonly involved (60%) but lung parenchyma was normal in 48%. Lung mass was reported in 16% whereas nodules were present in 24% cases. Mediastinal lymphadenopathy was reported in 36%. 16% had mild effusion (defined as occupying less than one third of hemithorax). 3 subjects had chest tube in situ at the time of the procedure. Pleural fluid analysis data showed that 56% had straw coloured and only one had chylous effusion based on appearance. Atypical cells were reported in 24% in the cytology but none of them had a conclusive diagnosis on cell block analysis. Mean total cell count was 418±288.3 per µl. 84% had mononuclear cell predominant differential count. All pleural fluid samples were exudative and mean LDH was 375.2±266.7 IU/l whereas mean pleural fluid proteins were 5.1±1.2 gm/dl. High ADA (greater than 70IU/l) was reported in only two cases, and both had lung mass in the CECT thorax. Mean ADA in the study population was 29.1±18.6IU/l. Baseline characteristics are provided in Table 1.
During medical thoracoscopy, all surfaces of pleural were inspected. Adhesions were present in 40% of the subjects. Most common finding was presence of nodules. 40% of the subjects had crops of fine nodules present whereas 60% of the subjects had discrete nodules of variable sizes. 5 subjects had normal shiny pleural at all surfaces. On an average 6.8 passes were taken with maximum of 10. In 32% cases only tiny tissue was obtained, hence requiring multiple passes. Large tissue could be obtained in 44% of the subjects. Mean duration of the procedure was 35.6±9.0 minutes requiring dual sedation with midazolam (mean 3.7±1.3 mg) and fentanyl (mean 108.0±24.7 µg). None of the patients complained of any severe pain or met with any major complication. Tissue diagnosis was established in 80% with most common being malignancy (48%) followed by tuberculosis (20%). All subjects of malignancy had sufficient tissue for immunohistochemistry. 9 subjects had lung as a primary tumor (all adenocarcinoma). In 3 cases, the final diagnosis was made by exclusion, one in each- uremic pleuritis, effusion secondary to pulmonary embolism and congestive heart failure. Hospital stay was prolonged in 3 subjects who had developed empyema after the procedure. All these subjects had insertion of chest tube in the emergency department where they had presented with dyspnea at rest and massive pleural effusion. Overall average hospital stay was 3.44±2 days.
We further compared the clinical and other characteristics of subjects with final diagnosis of pleural tuberculosis and malignancy. None of the categorical variable were significantly different in the two groups except for the lung mass lesions in radiology, which were presently exclusively in cases with malignancy. Whereas, on comparing the continuous variables, duration of symptoms was significantly longer in the malignancy group (35 versus 21.2 days, p=0.03). Also, the pleural fluid total cell count was higher in malignancy subjects (483.3 versus 340, p=0.034). None of the other variable were statistically different in the two groups.
Subsequently we compared the characteristics of the subjects grouped according to the diagnostic tissue yield of the procedure. Using the chi-square test, it was found that Loss of appetite was more common in patients without a definite tissue diagnosis (p=0.032) and subjects with crop of nodules were at higher risk of not getting a conclusive tissue diagnosis (p=0.02). Also, as anticipated, tiny tissue samples were associated with high probability of not getting a tissue diagnosis (p=0.006). None of the other variables were significantly different among the two groups. Using the independent sample t test, we also compared the means of the continuous variables among the two groups but none of them were found to be significantly different except age, which was higher in subject without a diagnosis (61.8 versus 48 years, p=0.01). Finally, we tried to analyse the factors associated with size of tissue. Both, the moderate and large tissues were clubbed together as sufficient samples. Only the diagnosis of tuberculosis was found to be an independent risk factor of getting tiny tissue samples (p=0.01), and none of the other variable were found to be significantly different among the two groups.
Discussion:
In the current retrospective study assessing the feasibility of doing diagnostic medical thoracoscopy using a flexible video bronchoscope through intercostal chest tube, including 25 subjects, we found that diagnostic yield was 80% with Large sized tissue biopsy in 44%. None of the patients had any significant complications during the procedure and 3 (12%) patient developed empyema.
Medical thoracoscopy is a vital modality for any interventional pulmonology suite but the availability of equipment in India is grossly heterogeneous (geographically) and limited to major cities only. Whereas the need of such diagnostic procedure is very high. Pleural effusion is one of the common presenting manifestations for tuberculosis as well as malignancy. Extrapulmonary tuberculosis (EPTB) comprises of nearly 40% of all TB cases and pleural TB is the most common type of EPTB [8]. Majority of such cases are diagnosed on the basis of ADA levels in pleural fluid as the microbiological evidence in the form of CBNAAT (cartridge based nucleic acid amplification test) or AFB stain/culture have low sensitivity [9]. Despite the sensitivity of ADA levels, a significant proportion of pleural tuberculosis cases are left without diagnosis and in the need of diagnostic pleural biopsy [10]. Malignant pleural effusion, similarly, represent a common problem in clinics. Exudative pleural effusion with low ADA with or without haemorrhagic pleural effusion are frequently attributed to an underlying malignancy. Pleural fluid cytology and cell block assessment can help in identifying the underlying cause but sensitivity remains low [11]. In such scenarios, pleural biopsy offers an additional advantage for the diagnosis as well as molecular profiling of the tumors using methods like Next Generation Sequencing and Fluorescent in Situ Hybridization. Following the recent revolution in the management of non-small cell lung cancer (which is the most common cause of malignant pleural effusion), tissue has become a vital source of information, affecting management at all levels. The list of recommended molecular tests (to be conducted on tissue samples) after histology and immunohistochemistry, is growing day by day. As per NCCN recommendations, EGFR (done by RTPCR), ALK (done by IHC), ROS1 (done by FISH) are the bare minimum investigations which require adequate quantities of tissue samples [12]. Thoracoscopy guided pleural biopsy offers the exact same advantage over cytology and cell block. Big chunk of tissue samples provides an opportunity to comprehensively investigate for targetable genetic alteration in one single attempt. This makes malignant pleural effusion an important indication for diagnostic medical thoracoscopy.
In addition to this the availability of the equipment and the expertise is grossly limited in India. In a recent survey by Madan et al., nearly half of the respondents (physicians performing medical thoracoscopies routinely) had an experience of 3 years or less. Though the survey did not include place of practice, nearly half of the participants were from multi-specialty hospitals with majority using standard equipment. Commonly such facilities are only limited to tier 1 cities in India [13]. Using flexible bronchoscope for the visualization of parietal pleural and pleural biopsy is not a novel technique and had been tested previously in anecdotal reports, more so by the surgeons [14,15]. In a Japanese study the technique of using intercostal chest tube as a trocar/port and bronchoscope for pleuroscopy was tested on seven cases and it was found to be safely tolerated [16].
Similar to our results, we found that thoracoscopy with a flexible bronchoscope was well tolerated and had no major complications. Additionally looking at the efficacy of such technique in the diagnosis, it was revealed that the final diagnosis could be established in 92% (23/25) of the subjects which was similar to previous studies on semi rigid thoracoscope [17,18]. When compared to the results of MINT trial the tissue diagnostic yield in our study was 80% compared to 81.1% in the semi-rigid arm of the trial [19]. MINT trial also compared the size of the tissue obtained and the size was measured in millimetres. This is not a routine practice in our institute, and we assess the tissue size based on the gross visualization and comparing with the cup of the forceps.
Another important observation in our study was that duration of the procedure was lesser to that compared with the study conducted by Dhooria et al. (53.4±10.8 minutes in semirigid arm versus 35.6±9.0 minutes in our study) [20]. This could have been due to choice of countdown time. We started the timing the procedure once the chest tube has been inserted. It is also reflected from the results of MINT trial where the duration of the procedure was similar to our study in semi-rigid arm (28.03 ± 9.9 minutes) [19]. Assessing the safety of the procedure with regards to the development of empyema, the results of our study were similar to the previous studies [21]. However, as all these cases had intercostal chest tube in situ before the procedure was planned (in emergency department), the development of empyema might not have been related to the procedure. We did not face any case of significant subcutaneous emphysema in our study, which is one of the commonly reported complications of the pleuroscopy procedure (12.5%) using semirigid scope [22]. This could have been probably due to retrospective nature of the study and mild subcutaneous emphysema are not recorded in hospital records.
Procedure related pain is one of the factor which gives semi-rigid thoracoscopy an advantage over rigid one and hence has been an important secondary end point in such clinical studies. Procedure related pain has been commonly measured using visual analogue scales but as ours was a retrospective study and VAS was not routinely employed, we had to use other surrogate variables. One of such variables was the use of sedative/analgesic agent during the procedure, which is routinely recorded and can be found in hospital records. However, the previously published literature has widely different reported values for these agents (1.8±0.7 for midazolam in MINT trial versus 3.9±1.3 mg for midazolam by Dhooria et al.) [19,20]. This suggests that pain management has largely been dependent upon the operator perceptions and preferences. In support of our results, the values of fentanyl and midazolam used in our studies have been similar to what was reported from study by Tousheed et al. which is one of the largest data sets in the world in the field of medical thoracoscopy [23].
Another important variable which needs to be analysed while assessing a new technique for an established procedure is the physician comfort. There was no way for us to analyse this factor in a retrospective fashion. The use of bronchoscope in place of a thoracoscope has several limitations as far as operator comfort is concerned. The greater length of the scope hinders the manoeuvrability and limits the ease of approach. Additionally, the inability to pincer hold the scope near the chest wall due to intercostal chest tube is an additional factor working against the practical utility of the new technique. The proposal of using a standard trocar in place of chest tube for insertion of bronchoscope was considered in initial stage but due to the flexible and delicate nature of the scope, and its length, it was very likely that scope may get damaged due to the hard ring of the trocar. Hence the chest tube was selected as the port of entry. Another difficulty faced by the operator during the procedure was the frequent need of manipulating the depth of insertion of the chest tube so as to provide space to the distal tip of the bronchoscope to make movements inside the cavity.
Our study offers the largest experience of using bronchoscope for pleuroscopy and confirms its applicability in terms of efficacy as well as safety, however, there are several limitations to our findings. Bring a retrospective study limits our findings to only those variables which are recorded. Also, the experience is collected from only one centres, and centre specific practices may influence the final outcomes. One of such practice is the routine admission of thoracoscopy subjects which not commonly done in other centres. We admit all cases of thoracoscopy till the chest tube is out in order to reduce the risk of complications. Other limitations have been our inability to record pain and operator ease outcomes, which are otherwise important factor while choosing the modality of access. Comparison of our findings with semi-rigid thoracoscopy (now available at out centre) would have added value to our findings but a case control study increases the risk of selection bias and hence, we planned to limit out results to a descriptive study.
In conclusion, we found that, when needed, the innovative use of flexible bronchoscope through chest tube for performing medical diagnostic thoracoscopy is feasible, safe, and probably as successful in obtaining tissue as semi-rigid thoracoscopy. Such technique can help navigate the limitation of availability of equipment in resource limited conditions. However, the real impact on patient comfort and operator ease needs to be evaluated in larger head-to-head comparative studies.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author Contributions (CReDiT Statement):
RK: Conceptualization, investigation (lead), methodology, writing original draft. RD: Data curation, formal analysis (lead), validation. AC: Resources (lead), visualization, writing original draft. PKS: Investigation, visualization, writing review & editing. DC: Supervision (lead), writing review & editing (lead). AA: Writing original draft, resources. GA: Formal analysis, proof reading. All authors have contributed substantially to the current research work, drafting the manuscript, final approval, and are accountable for all aspects of this study.
Data Sharing Statement
The anonymized individual patient data can be shared upon request to the corresponding author.
Acknowledgments
We would like to thank the study participants for their faith and support for the operators using new technique.
Conflicts of Interest
None to declare.
References
- Biswas, B.; Sharma, S.K.; Negi, R.S.; Gupta, N.; Jaswal, V.M.; Niranjan, N. Pleural effusion: Role of pleural fluid cytology, adenosine deaminase level, and pleural biopsy in diagnosis. Journal of cytology 2016, 33, 159–62. [Google Scholar] [CrossRef] [PubMed]
- Chinchkar, N.J.; Talwar, D.; Jain, S.K. A stepwise approach to the etiologic diagnosis of pleural effusion in respiratory intensive care unit and short-term evaluation of treatment. Lung India : official organ of Indian Chest Society 2015, 32, 107–15. [Google Scholar] [CrossRef] [PubMed]
- Maji, A.; Maikap, M.K.; Jash, D.; Saha, K.; Kundu, A.; Saha, D.; et al. Role of common investigations in aetiological evaluation of exudative pleural effusions. Journal of clinical and diagnostic research : JCDR 2013, 7, 2223–6. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Gupta, R.; Christopher, D.J.; Balamugesh, T. Evaluation of the diagnostic yield and safety of closed pleural biopsy in the diagnosis of pleural effusion. The Indian journal of tuberculosis 2010, 57, 19–24. [Google Scholar] [PubMed]
- Vecchio, R.; MacFayden, B.V.; Palazzo, F. History of laparoscopic surgery. Panminerva medica 2000, 42, 87–90. [Google Scholar]
- Casal, R.F.; Eapen, G.A.; Morice, R.C.; Jimenez, C.A. Medical thoracoscopy. Current opinion in pulmonary medicine 2009, 15, 313–20. [Google Scholar] [CrossRef]
- Chawla, R.K.; Christopher, D.J.; Dhar, R.; Yuvarajan, S.; Chopra, K.; Samaria, J.K.; et al. Thoracoscopic practices in India-a survey by Indian chest society. The Indian journal of tuberculosis 2021, 68, 485–90. [Google Scholar] [CrossRef] [PubMed]
- Prakasha, S.R.; Suresh, G.; D'Sa, I.P.; Shetty, S.S.; Kumar, S.G. Mapping the pattern and trends of extrapulmonary tuberculosis. Journal of global infectious diseases 2013, 5, 54–9. [Google Scholar] [CrossRef]
- Lokhande, L.; Malhotra, A.G.; Vishwakarma, S.P.; Shankar, P.; Singh, J.; Khurana, A.K.; et al. Diagnosis of tuberculous pleural effusion in a tertiary care hospital of central India: The role of xpert Mycobacterium tuberculosis/rifampicin. International journal of mycobacteriology 2023, 12, 162–7. [Google Scholar] [CrossRef]
- Casalini, A.G.; Mori, P.A.; Majori, M.; Anghinolfi, M.; Silini, E.M.; Gnetti, L.; et al. Pleural tuberculosis: medical thoracoscopy greatly increases the diagnostic accuracy. ERJ open research 2018, 4. [Google Scholar] [CrossRef]
- Ghosh, I.; Dey, S.K.; Das, A.; Bhattacharjee, D.; Gangopadhyay, S. Cell block cytology in pleural effusion. Journal of the Indian Medical Association 2012, 110, 390–2. [Google Scholar] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Ettinger, J.R.; Bharat, A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network : JNCCN 2022, 20, 497–530. [Google Scholar] [CrossRef] [PubMed]
- Madan, K.; Tiwari, P.; Thankgakunam, B.; Mittal, S.; Hadda, V.; Mohan, A.; et al. A survey of medical thoracoscopy practices in India. Lung India : official organ of Indian Chest Society 2021, 38, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Senno, A.; Moallem, S.; Quijano, E.R.; Adeyemo, A.; Clauss, R.H. Thoracoscopy with the fiberoptic bronchoscope. A simple method in diagnosing pleuropulmonary diseases. The Journal of thoracic and cardiovascular surgery 1974, 67, 606–11. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.C.; George, R.J.; Sheldon, C.D.; Sinha, G.; Corrin, B.; Geddes, D.M. Thoracoscopy: assessment of a physician service and comparison of a flexible bronchoscope used as a thoracoscope with a rigid thoracoscope. Thorax 1988, 43, 327–32. [Google Scholar] [CrossRef]
- Yokoyama, T.; Toda, R.; Tomioka, R.; Aizawa, H. Medical Thoracoscopy Performed Using a Flexible Bronchoscope Inserted through a Chest Tube under Local Anesthesia. Diagnostic and therapeutic endoscopy 2009, 2009, 394817. [Google Scholar] [CrossRef]
- Tousheed, S.Z.; Ranganatha, R.; Hemanth Kumar, M.; Manjunath, P.H.; Philip, D.S.; Punitha, M.; et al. Role of medical thoracoscopy in the diagnosis of pleural effusions. The Indian journal of tuberculosis 2022, 69, 584–9. [Google Scholar] [CrossRef] [PubMed]
- Patil, C.B.; Dixit, R.; Gupta, R.; Gupta, N.; Indushekar, V. Thoracoscopic evaluation of 129 cases having undiagnosed exudative pleural effusions. Lung India : official organ of Indian Chest Society 2016, 33, 502–6. [Google Scholar] [CrossRef]
- Bansal, S.; Mittal, S.; Tiwari, P.; Jain, D.; Arava, S.; Hadda, V.; et al. Rigid Mini-Thoracoscopy Versus Semirigid Thoracoscopy in Undiagnosed Exudative Pleural Effusion: The MINT Randomized Controlled Trial. Journal of bronchology & interventional pulmonology 2020, 27, 163–71. [Google Scholar] [CrossRef]
- Dhooria, S.; Singh, N.; Aggarwal, A.N.; Gupta, D.; Agarwal, R. A randomized trial comparing the diagnostic yield of rigid and semirigid thoracoscopy in undiagnosed pleural effusions. Respiratory care 2014, 59, 756–64. [Google Scholar] [CrossRef]
- Mootha, V.K.; Agarwal, R.; Singh, N.; Aggarwal, A.N.; Gupta, D.; Jindal, S.K. Medical thoracoscopy for undiagnosed pleural effusions: experience from a tertiary care hospital in north India. The Indian journal of chest diseases & allied sciences 2011, 53, 21–4. [Google Scholar]
- Kapadia, V.; Jindal, S.; Patel, P.; Tripathi, S. A Study of Role of Medical Thoracoscopy in Undiagnosed Pleural Effusion. The Journal of the Association of Physicians of India 2023, 71, 11–2. [Google Scholar] [CrossRef] [PubMed]
- Tousheed, S.Z.; Ranganatha, R.; Hemanth Kumar, M.; Manjunath, P.H.; Philip, D.S.; Punitha, M.; et al. Role of medical thoracoscopy in the diagnosis of pleural effusions. Indian Journal of Tuberculosis 2022, 69, 584–9. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Representative image of the procedure showing the flexible bronchoscope (red arrow) transversing through the intercostal chest tube (yellow arrow), which is acting as port.
Figure 1.
Representative image of the procedure showing the flexible bronchoscope (red arrow) transversing through the intercostal chest tube (yellow arrow), which is acting as port.
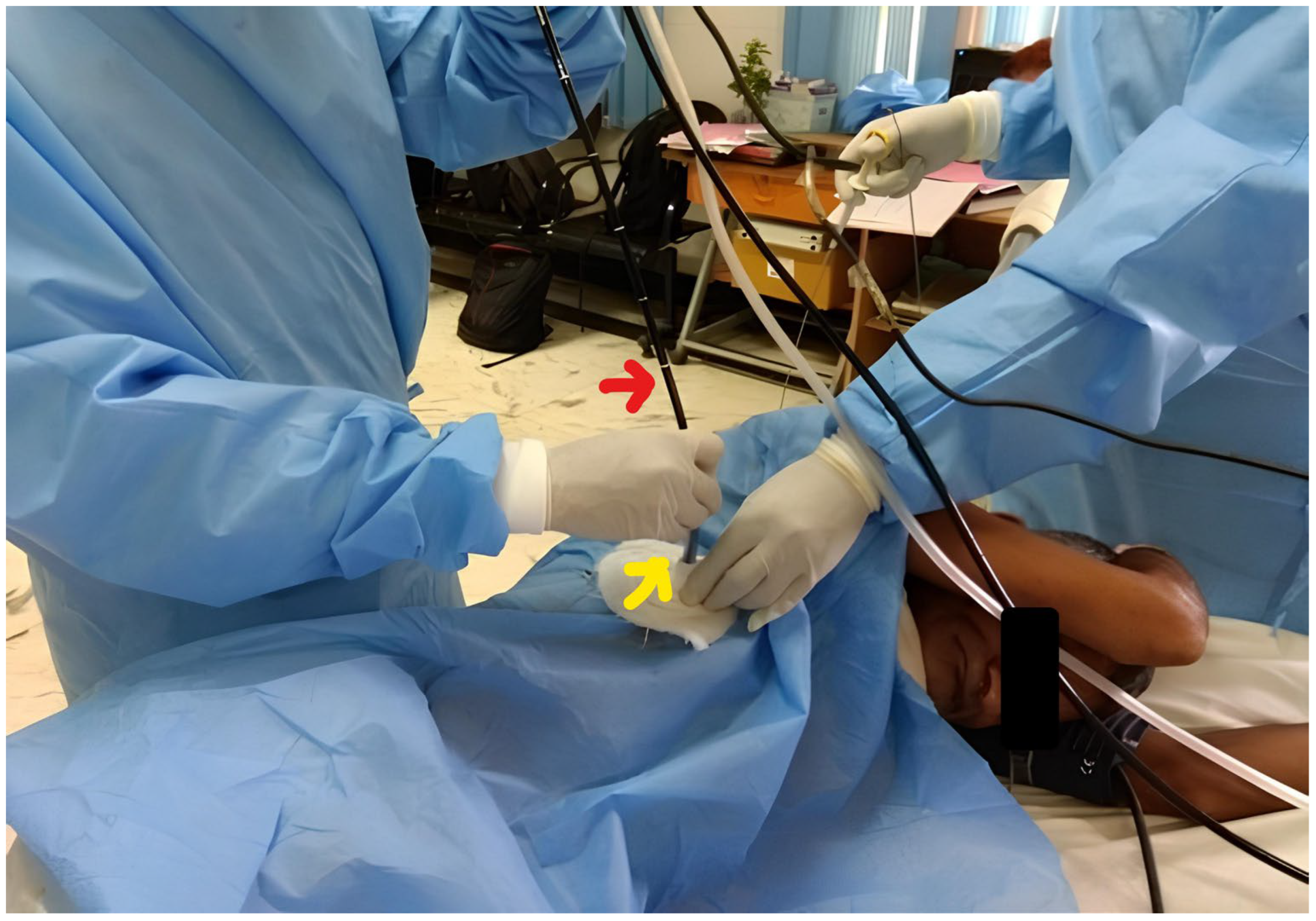
Figure 2.
Flow diagram showing the case selection for the study analysis.
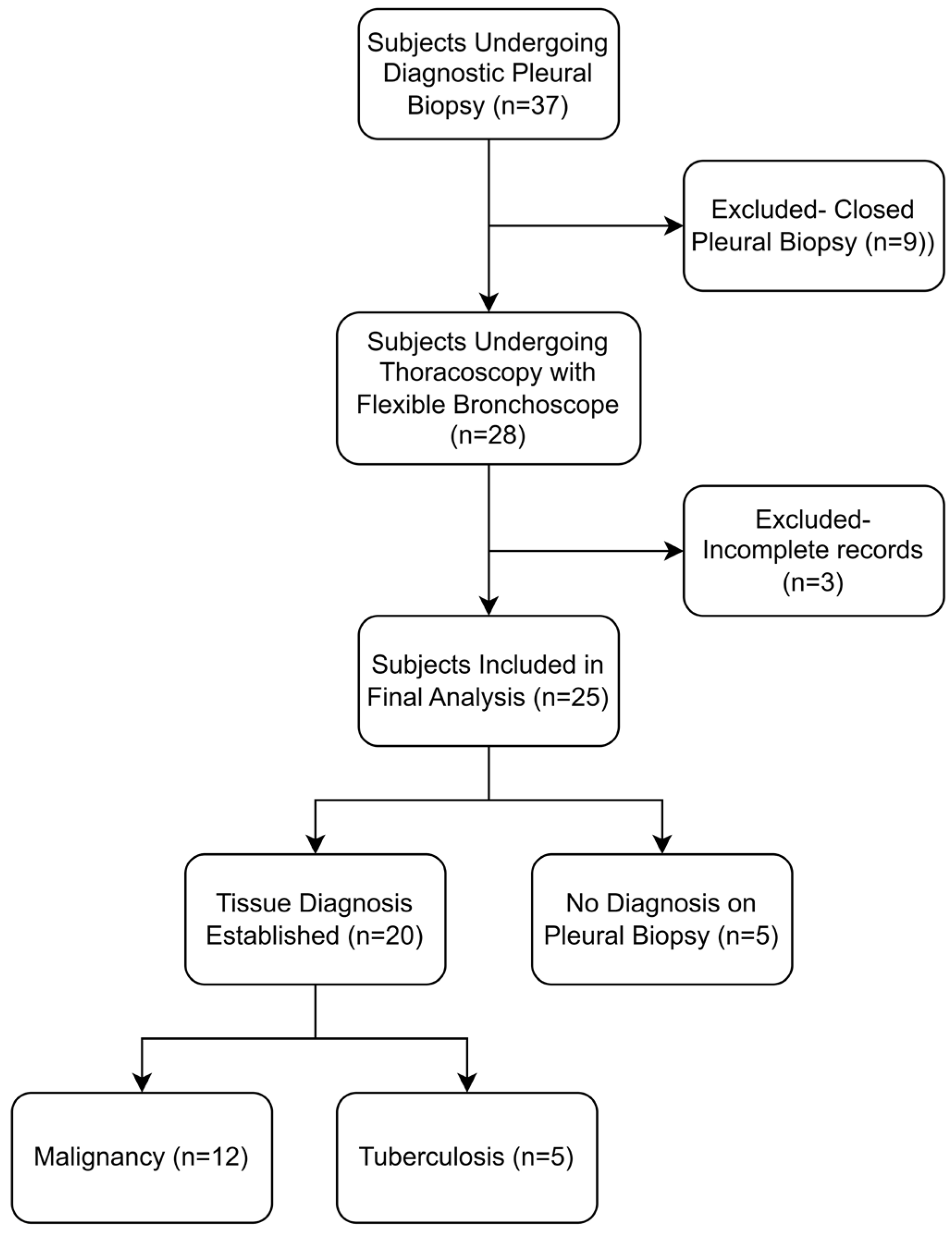

Table 1.
Baseline characteristics of the study population. SD: Standard Deviation; LAP: Lymphadenopathy; LDH: Lactate Dehydrogenase; ADA: Adenosine Deaminase.
Table 1.
Baseline characteristics of the study population. SD: Standard Deviation; LAP: Lymphadenopathy; LDH: Lactate Dehydrogenase; ADA: Adenosine Deaminase.
| Variable | n(%) | |
|---|---|---|
| Age in years (mean±SD), Range | 52.4±14.0, 22 to 74 | |
| Sex | Male | 14(56) |
| Females | 11(44) | |
| Residence | Urban | 9(36) |
| Rural | 16(64) | |
| Occupation | Farmer | 8(32) |
| Homemaker | 9(36) | |
| Skilled Job | 4(16) | |
| Desk Job | 4(16) | |
| Duration of symptoms in days (mean±SD) | 24.7±18.0 | |
| Symptoms | Fever | 12(48) |
| Cough | 7(28) | |
| Dyspnea | 8(32) | |
| Constitutional Symptoms* | 24(96) | |
| Radiological Features | Normal | 12(48) |
| Lung Nodules | 6(24) | |
| Mass | 4(16) | |
| Consolidation | 3(12) | |
| Mediastinal LAP | 9(36) | |
| Pleural Fluid work up | Appearance (Straw, Haemorrhagic, Chylous) | 14(56), 10(40), 1(4) |
| Total Cell (mean±SD) | 418±288.3 | |
| Protein in gm/dl (mean±SD) | 5.1±1.2 | |
| Sugar in mg/dl (mean±SD) | 70.6±36.3 | |
| LDH in IU/L (mean±SD) | 375.2±266.7 | |
| ADA in U/L (mean±SD) | 29.1±18.6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



