
Submitted:
01 November 2023
Posted:
02 November 2023
You are already at the latest version
Abstract
Introduction: Crohn's disease (CD) is a chronic inflammatory granulomatous disease that can affect the entire gastrointestinal tract. It is characterized by various extraintestinal manifestations (EIM), of which oral manifestations (OM) are often possible. One of the possible OM is periodontal disease (PD) a chronic inflammatory condition of the supporting tissues of the teeth. This study aimed to show the existence of a mutual relationship between the clinical activity of PD and the clinical and endoscopic activity of CD.
Materials and methods: Using one clinical and two endoscopic indexes for the assessment of CD activity and clinical attachment loss (CAL), bleeding on probing (BOP), pocket probing depth (PPD) and radiographic bone loss (RDL) on dental panoramic tomogram to assess PD in CD patients.
Results: A total of 38 patients underwent the entire study process, of which 20 patients with CD and 18 patients with CD and PD. Considering all CD activity scores, there were 26 patients with active disease, and half of them had PD, and 85.7% of operated patients had active CD. Values of CAL, PPD, BOP and RBL were higher in active CD than remission, except BOP when compared to CDAI score which was higher in remission of CD.
Discussion and conclusion: The results of this study indicate that there is a connection between the activity of CD and the worse condition of the supporting tissues of the gums in the oral cavity which is important to keep in mind the necessity of referring patients with CD to a dentist for timely and adequate therapeutic measures.
Keywords:
Crohn’s disease
; periodontal disease
; Crohn’s disease activity indexes
; periodontal indexes
Introduction
Inflammatory bowel diseases (IBD) comprise two entities, Crohn's disease (CD) and ulcerative colitis (UC). They represent chronic inflammation of the gastrointestinal tract, which can affect the entire GIT in the case of Crohn's disease. CD and UC are idiopathic IBD characterized by periods of relapse and remission. Inflammation is dominantly present in the lining of the colon (sometimes also in the small intestine) in patients with UC. In patients with CD, inflammation, which is mainly segmental and transmural, can be registered in all parts of the digestive tract (from the oral cavity to the anus), especially in the small and large intestine (1,2). Numerous extraintestinal manifestations of these diseases can also occur. IBD is clinically characterized by recurrent inflammation of gastrointestinal tract segments and diverse clinical manifestations, often very unpredictable and sometimes fatal (3,4).
Until now, it is known that the intestinal microbiota plays an important role in the development and maintenance of IBD, although the specific effect of all microorganisms that can affect it has been insufficiently investigated. (5) Several genes are associated with an increased risk of developing CD. So far, the most studied are NOD2 and IL23R, whose mutations are found in about 20% and 10% of people with CD. Also, mutations in the genes ATG16L1, IRGM, and CARD15 predispose to the manifestation of CD. Although the mechanism of all the genes that can be affected has not been sufficiently elucidated so far, their identification enables a better understanding of the disease and helps develop new diagnostic and treatment strategies (6–8).
Research indicates that the prevalence of IBD worldwide is increasing, but the necessity of hospital treatment is statistically significantly higher in patients with CD (5,9). The frequency of CD is higher in developed countries and urban areas than in rural areas and developing countries. The first symptoms of CD usually appear in the second to fourth decade of life. Previous research has shown that there is no significant difference in the occurrence of CD by gender (1). There is an increased incidence of CD in the first or second generation among populations migrating from low-incidence regions to high-incidence regions. This information points to the importance of environmental and early exposure to factors influencing the development of CD (1,5,9).
Periodontal disease (PD) is a chronic inflammatory condition of the supporting tissues of the teeth. It is caused by bacteria that form a sticky biofilm on the teeth. In the earlier stage, it is characterized by gingivitis, and clinically, redness and swelling of the gums, which bleed easily when irritated, are observed. If left untreated, it can progress to periodontitis, when the periodontal ligament and alveolar bone are affected. It is a more severe form of PD characterized by the appearance of periodontal pockets and causes receding gums terminal loosening and loss of teeth (10).
Factors that are important for the development of periodontitis are diet (mainly carbohydrates), bad habits, diabetes, family history, certain medications, and immunodeficiency. Diagnosis is made by visual and tactile examination of the gingival tissue, probing, and radiographic evaluation to determine the presence and assess the depth of periodontal pockets (11).
There is evidence that the risk of CD is increased in people with a history of PD, suggesting that systemic inflammation in people with PD may trigger or exacerbate current IBD (12). Intestinal bacterial flora, immune-mediated inflammatory processes, and certain risk factors are thought to play a common role in both PD and CD. The pathogenesis and whether the interaction between these diseases is one-way or two-way is still not fully explained (12,13).
This study aimed to show the existence of a mutual relationship between the clinical activity of PD and the clinical and endoscopic activity of CD using indexes for the assessment of disease activity and to assess the prevalence of PD in patients with CD.
Patients and Methods
The study was approved by the Ethics Committee of the Faculty of Medical Sciences in Kragujevac, University of Kragujevac, and the Ethics Committee of the University Clinical Center Kragujevac.
Patients
This study included patients diagnosed with Crohn's disease based on an endoscopic examination of the colon and pathohistological findings of a biopsy taken during the endoscopic examination. Patients were excluded if they were under the age of 18, pregnant or nursing, had limited legal responsibility or reduced cognitive abilities, had chronic diseases, or had used therapy or procedures that may affect the examination of parameters in the two weeks before or at the time of the research or were edentulous.
Assessment of Crohn’s disease activity
Clinical activity of Crohn's disease was determined using the Crohn's Disease Activity Index (CDAI) (14), the Harvey Bradshaw index (15), and the Van Hess index (16). These indices include data on the number of daily stools, the presence of abdominal pain, the subjective condition of patients, the existence of extraintestinal manifestations, the use of probiotics and opioids, the body mass index of patients, and the values of blood parameters.
The clinical activity of a disease is the assessment of the disease at a given point in time. It is important to select induction therapy and evaluate the need for hospitalization, or the efficacy of a drug. The clinical classification categorizes the disease as mild, moderate, or severe depending on the following factors: response to therapy, presence of malnutrition, dehydration, or systemic toxicity, presence of abdominal tenderness, mass, or obstruction, degree of weight loss, and anemia. Symptoms do not necessarily correlate with objective assessments of disease activity, such as endoscopy, cross-sectional imaging (cecum), or biomarkers (C reactive protein (CRP) or fecal calprotectin), leucocytes and hemoglobin.
Endoscopic activity was assessed using the Crohn's Disease Endoscopic Severity Index (CDEIS) (17) and the Simple Endoscopic Score for Crohn's Disease (SES-CD) (18). Endoscopic activity is determined based on the existence, characteristics, and extent of inflammation and ulceration in the digestive tract by segment.
Also, assessment of localization of CD depending on age and predominant type of CD was assessed using The Viena and Montreal classification.
Assessment of periodontal disease
The presence of periodontitis was assessed using the periodontological indexes Clinical attachment level (CAL) (19), Bleeding on probing (BOP) (20), and Periodontal pocket depth (PPD) (19,21). CAL represents the distance from the enamel-cementum border to the bottom of the gingival sulcus or periodontal pocket, BOP informs us if there is inflammation and bleeding, and PPD represents the distance from gingival margins to the bottom of the gingival sulcus/periodontal pocket. All of these classifications are presented in Table 1.
Periodontal disease was also confirmed by measuring radiographic bone loss (RBL) on dental panoramic tomograms (DPTs). All DPTs were taken on Orthophos XG 3D device (Sirona Dental Systems GmbH, Bensheim, Germany) in the Department of Dentistry at the Faculty of Medical Sciences, University of Kragujevac. To clarify alveolar bone levels and root apices of the entire dentition, all radiographic images were enhanced in the picture editing software GIMP (GNU Image Manipulation Program, Software version 2.10) and were subsequently printed and used for measuring the distance (22) (Figure 1). Periodontal disease staging was assessed from the classification of 2018 (19,23) with extracted referent values by stages (Table 1).
Statistics
The Statistical Package for Social Sciences software (SPSS, version 27, Chicago, IL, USA) was used for statistical processing and data analysis. Variables were described using frequency distribution for categorical variables and mean and standard deviation for continuous variables as well as medians and interquartile range depending on the normality test. After the normality test, the Mann Witney U Test and Independent Samples T-test were used accordingly for scale variables. Chi-square was used for categorical variables and statistical significance Fisher’s Exact Test, Continuity Correction, and Pearson Chi-Square were used where needed. Sensitivity and specificity are shown using Receiver Operating Characteristic (ROC) curve and Area Under the ROC Curve (AUC).
Results
This study aimed to examine the correlation between activity indexes of CD and PD and to assess the prevalence of PD in patients with CD. A total of 38 patients underwent the entire study process, of which 20 patients with CD and 18 patients with CD and PD. Clinical and demographic characteristics are shown in Table 2.
The mean value of age of all 38 patients was 39.45±13.29 years. Duration of Crohn’s disease varies from one month to 25 years depending on the patient. The mean value was 7.05±6.4 years, and there was no statistical significance comparing groups with PD and without PD. Clinical score CDAI and endoscopic scores CDEIS and SES-CD mean values for all patients were 115.11±71.86, 4.18±5.2, and 6.92±8.67, respectively. Of all patients, 12 (31.58%) had clinically active CD considering CDAI score, six with PD and six without PD. Using CDEIS and SES-CD scores there were 26 (68.4%) and 19 (50%) patients with active CD, respectively. There was no statistically significant difference between the groups. Considering all CD activity scores, there were 26 patients with active disease, and half of them had PD. The BMI mean values difference was statistically significant between CD patients with and without PD (Table 2).
All patients that underwent surgery (36.84%) belonged to either group i0 (57%) or group i1 (43%) of Rutgeerts score that represents there were no lesions or less than five aphthous lesions after surgery, respectively. It is important to emphasize that the difference in the mean values of the disease duration in patients with PD who underwent surgery compared to those who did not was clinically significant and the values were 9.43±7.73 and 5.67±5.16, respectively. Also, 85.7% of operated patients had active CD.
The results of our study, using the Vienna and Montreal classifications, showed that in more than half (60%) of the patients with Crohn's disease, the disease was localized in the ileocolon (group L3). In most patients, 44.7% had inflammatory and 34.2% had structuring type of CD. The penetrating type was represented in 21.1% of cases of which all had perianal complications. In the CD+PD group, 22% of patients had perianal complications and in the CD group, that percentage was 15%. Also, the ileum and colon were mostly affected in both groups, 66% and 50% in CD+PD and CD respectively.
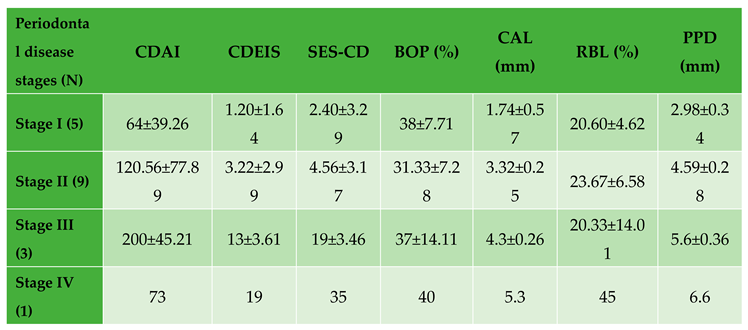
Periodontal disease indexes mean values were calculated for BOP - 25.24±11.44 (%), CAL - 2.61±0.96 (mm), and PPD - 3.71±1.09 (mm). All these measurements and CD activity scores are presented in Table 3 by stage of periodontal disease. The mean value of RBL in all patients was 11.66±12.87 (%) with significantly higher values in the CD + PD group (23%). Average values of CAL, PPD, BOP, and RBL according to CD activity scores are presented in Figure 2.
By using the ROC curve to assess the predictive ability for the presence of OM in CD patients, we used CAL, PPD and BOP values, and it was shown that BOP values can be an indicator of the occurrence of OM in CD patients (AUC=0.976, P<0.001) with a sensitivity of 94.4% while the specificity is 85%, and the limit value is 23.00. Also values of CAL (AUC=0.814, P=0.001) and PPD (AUC=0.840, P<0.001) can be indicators as well with similar sensitivity of 72.2%, and 77.8% and specificity of 100% and 75% respectively. Threshold values of CAL was 2.90 and for PPD 3.30. Statistically significant sensitivity and specificity are shown using ROC curve in Figure 3. There was no significant differences of values of CRP, fecal calprotectin, leucocytes and hemoglobin between CD patients with and without PD.
Discussion
It is known that in the active state of CD, there are significantly more inflammatory processes in the body, and the same is the case with PD and intestinal flora imbalance (1,24,25). To point out the importance of the correlation between the activity of CD and PD, using the mentioned methods for determining both the activity and the severity of the disease, the importance and need for further research in this area was pointed out. The results of this study indicate that there is a connection between the activity of CD and the worse condition of the supporting tissues of the gums in the oral cavity. The prevalence of CD patients with PD in our study was 47.4%. The study by Lauritano et al. shows that the prevalence of any oral manifestation (OM) in patients with CD varies from 0.7% to 37% (26), and Lankarani et al. reported in their study that the prevalence rate of extraintestinal manifestations ranges from 6%-47% (27) In a study by Alvarado Julio et al. the presence of OM was reported in as many as 63% of patients with IBD, the most common of which is gingivitis in as many as 55% of cases (3).
Large differences in the frequency of the disease reported in different studies may be due to different study designs, study objectives, the number of subjects in each study, as well as the inexperience of the researchers or doctors in diagnosing or conducting the research. It is important to keep in mind the lack of a universal classification of OM or their severity in people with Crohn's disease, and the difficulty in comparing the parameters used in different studies.
Oral manifestations that can occur in patients with CD are divided into specific ones in the form of cobblestone mucosa, granulomatous cheilitis and seals on the mucosa, and non-specific ones in the form of aphthae, fissures, other types of cheilitis, Lichen planus, periodontal disease, dental caries, and others. They are in most cases asymptomatic and the prevalence of these OM is 0.5% and 37% (28), while according to some earlier studies it was from 12.7–21% (26). The most common OM generally in IBD is aphthous ulcerations which are clinically hard to distinguish from aphthous ulcerations in healthy people so a biopsy and/or Anti-Saccharomyces cerevisiae antibody (ASCA) test is necessary (29).
Our results are in agreement with a cohort study that evaluated the association between IBD and periodontitis. The authors concluded that patients with IBD in whom the disease is active have a more severe clinical picture and the extent of periodontitis compared to those in remission (30). In our study, although there were the same number of patients with active disease in both the CD+PD and CD groups, the CD activity clinical score values were higher in the CD+PD group, which represents a third of the group. Also, a study by Zhang et al. showed a higher risk of PD in patients with IBD (31).
Following the Vienna and Montreal classification, the results indicate that the CD+PD group has more patients with perianal complications than the CD group, which may be clinically significant, although no statistically significant difference is obtained. The reason for this may be the greater spread of the disease since the disease in the CD+PD group involved more patients with perianal complications than in more parts of the gastrointestinal tract.
Using the new classification from 2018, it is difficult to compare the results obtained in studies carried out before the establishment of this classification (32).
Our results showed BOP values were statistically significant in the group of patients with CD with OM compared to the CD group. The mean value of BOP we found was 25.24% which is similar to some other studies (33–36), but higher values are also reported (37,38). In a study by Vavricka et al., the results of BOP were shown, which are more pronounced in patients with CD (39), which is also shown in the study of Imai et al. (40). That does not correlate with the study which the results indicate that the presence of dental plaque was associated with a lower risk of CD (41), and values of BOP were similar in IBD and control group. Patients with CD had higher PPD and CAL values in the study (36) compared to the control group, which is contrary to the study where they found higher PPD values in the control group compared to the IBD patients (35). Although PPD values were higher in the control group, higher CAL values were observed in more places in the oral cavity in patients with IBD in both mentioned studies, which may be the reason for the immediate remission of PD and previously greater loss of periodontal tissue. It is important to note that in several studies the clinically significant information is that the measured values of CAL >6mm, even up to 32% of cases, although no statistically significant differences between groups were obtained, both for CAL and for BOP and PPD (33). Our results show significantly higher CAL values in 47% of patients with a mean value greater than 3mm, while in some studies where periodontitis was present, the CAL value was less than 3mm (mean 0.9mm) (36). In most studies, there is information about a significantly greater number of missing teeth in IBD patients compared to control groups (30,33,38,42). The study by Baima et al. found a significantly higher prevalence of PD in IBD patients compared to the control group. It has been shown that stage III and stage IV are significantly more common in IBD patients. The difference in PPD (≥5mm) and CAL values is also significantly higher in IBD patients. What is important is that this study showed the same significance using the 2018 classification used in our study (32,43). Statistical significance was shown by comparing the presence of periodontal disease and the age of the subjects, where subjects with PD had a higher mean age. We can see such data in other studies, where it has been shown that patients with CD aged 51-65 years have significantly more severe forms of PD as well as higher values of CAL and PPD (43).
The duration of IBD is a clinically significant factor both for determining the quality of life in patients and for prognostic therapeutic planning. It may also be significant for explaining certain results obtained in studies comparing clinical and endoscopic IBD scores with other parameters, as in this study. Our results show that the duration of CD (7.05±6.4 years) is shorter than those values in another study (43), where the importance of disease duration and surgery related to IBD is also indicated, which in that study are negatively associated with periodontitis. Based on this, it can be concluded that timely and regular control of IBD can play a protective role, both for the underlying disease and for the onset and progression of oral manifestations. Our results indicate a significant difference in the number of operated patients and it is higher in the CD group without OM, with statistically significantly more cases by type i1 Rutgeerts score (Table 2). It is important to state that in our study, illness duration was significantly higher in patients who underwent surgery.
Conclusion
In conclusion, our data show that active CD causes increased bone loss visible on the orthopantomogram and causes more inflammatory processes in the oral cavity, which is most often manifested in the form of gingivitis.
So far, we know that there is an association of pathogenesis between IBD and PD and that both diseases may depend on genetic, environmental, microbial, and immunological factors. In the study by Tanwar et al., patients with IBD showed a significantly higher number of OM compared to the control group, which is explained by difficult oral hygiene and a changed diet due to stomach problems, which causes a more suitable environment in the oral cavity for the development of microorganisms and the progression of periodontitis (44). In addition to studies indicating more frequent OM of CD, there is also a study in which no statistical or clinical significance of the frequency or severity of the clinical picture of PD was shown (35).
The shortcoming of this study is possibly the number of patients with a wider demographic coverage as well as a larger number of measured variables, which is certainly planned in the continuation of the research. The strength of this study is reflected in the fact that several parameters of CD and PD activity were compared both with the Vienna and Montreal classifications, the Rutgeerts classification, and with some values from serum, which can be significant in the objectivity of determining the scores and finding the correlation of all variables with PD stages using new classification.
Collaboration between dentists, gastroenterologists, immunologists, and infectious disease specialists, along with other healthcare professionals, is necessary to provide holistic oral-systemic healthcare. Optimal dental care should reduce the intestinal supply of pathogenic oral bacteria, offering innovative methods to reduce the risk and severity of IBD. It is important to keep in mind the necessity of referring patients with CD to a dentist for timely and adequate therapeutic measures to stabilize the disease, and thus significantly reduce inflammatory processes in the body.
Author Contributions
The following statements should be used "Conceptualization, N.Z. and M.Ž.; Methodology, N.Z, M.Ž.; Software, M.Ž.; Validation, B.S., B.M. and Ž.T.; Formal Analysis, M.Ž, Ž.T.; Investigation, M.Ž and N.Z.; Resources, N.Z, B.S, B.M., M.Ž; Data Curation, N.Z.; Writing – Original Draft Preparation, M.Ž.; Writing – Review & Editing, N.Z. and M.Ž; Visualization, M.Ž.; Supervision, N.Z.; Project Administration, N.Z.; Funding Acquisition, M.A and S.M.” All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Faculty of Medical Sciences, University of Kragujevac, and the Ethics Committee of the University Clinical Center Kragujevac. Informed consent was obtained from all subjects involved in the study.
Funding
This research was funded by Faculty of Medical Sciences, University of Kragujevac grant number JP 17-19.
Acknowledgments
None.
Declaration of Interest
The authors declare that they have no conflict of interest.
Consent to Publish
The authors consent to the publication of this study, including their data.
References
- Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s disease. The Lancet. 2017;389(10080):1741–55.
- Baumgart DC, Sandborn WJ. Crohn’s disease. The Lancet. 2012;380(9853):1590–605.
- Alvarado-Julio A, Chumacero-Palma K, Buenahora MR, Parra-Izquierdo V, Monsalve M, Torres AM, et al. Oral manifestations associated with inflammatory bowel disease and early endoscopic findings in patients with spondyloarthritis. BMC Oral Health. 2022;22(1):477.
- Matkowskyj KA, Chen ZE, Rao MS, Yang GY. Dysplastic Lesions in Inflammatory Bowel Disease: Molecular Pathogenesis to Morphology. Arch Pathol Lab Med. 2013;137(3):338–50.
- Borowitz, SM. The epidemiology of inflammatory bowel disease: Clues to pathogenesis? Front Pediatr. 2023;10:1103713.
- Festen EAM, Weersma RK. How will insights from genetics translate to clinical practice in inflammatory bowel disease? Best Pract Res Clin Gastroenterol. 2014;28(3):387–97.
- Annese, V. Genetics and epigenetics of IBD. Pharmacol Res. 2020;159:104892.
- Brand, S. Moving the genetics of inflammatory bowel diseases from bench to bedside: first steps towards personalised medicine. Gut. 2013;62(11):1531–3.
- Buie MJ, Quan J, Windsor JW, Coward S, Hansen TM, King JA, et al. Global Hospitalization Trends for Crohn’s Disease and Ulcerative Colitis in the 21st Century: A Systematic Review With Temporal Analyses. Clin Gastroenterol Hepatol. 2023;21(9):2211–21.
- Meurman J, Bascones-Martinez A. Oral Infections and Systemic Health – More than Just Links to Cardiovascular Diseases. Oral Health Prev Dent. 2021;19(1):441–8.
- Kinane DF, Stathopoulou PG, Papapanou PN. Periodontal diseases. Nat Rev Dis Primer. 2017;3(1):17038.
- Papageorgiou SN, Hagner M, Nogueira AVB, Franke A, Jäger A, Deschner J. Inflammatory bowel disease and oral health: systematic review and a meta-analysis. J Clin Periodontol. 2017;44(4):382–93.
- She Y yang, Kong X bo, Ge Y ping, Liu Z yong, Chen J yu, Jiang J wei, et al. Periodontitis and inflammatory bowel disease: a meta-analysis. BMC Oral Health. 2020;20(1):67.
- Best WR, Becktel JM, Singleton JW, Kern F. Development of a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study. Gastroenterology. 1976;70(3):439–44.
- Harvey RF, Bradshaw JM. A SIMPLE INDEX OF CROHN’S-DISEASE ACTIVITY. The Lancet. 1980;315(8167):514.
- Van Hees PA, Van Elteren PH, Van Lier HJ, Van Tongeren JH. An index of inflammatory activity in patients with Crohn’s disease. Gut. 1980;21(4):279–86.
- Mary JY, Modigliani R. Development and validation of an endoscopic index of the severity for Crohn’s disease: a prospective multicentre study. Groupe d’Etudes Therapeutiques des Affections Inflammatoires du Tube Digestif (GETAID). Gut. 1989;30(7):983–9.
- Daperno M, D’Haens G, Van Assche G, Baert F, Bulois P, Maunoury V, et al. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: the SES-CD. Gastrointest Endosc. 2004;60(4):505–12.
- Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol. 2018;89:S159–72.
- Trombelli L, Farina R, Silva CO, Tatakis DN. Plaque-induced gingivitis: Case definition and diagnostic considerations. J Periodontol. 2018;89:S46–73.
- Chapple ILC, Mealey BL, Van Dyke TE, Bartold PM, Dommisch H, Eickholz P, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89:S74–84.
- Shaker ZMH, Parsa A, Moharamzadeh K. Development of a Radiographic Index for Periodontitis. Dent J. 2021;9(2):19.
- Ertaş K, Pence I, Cesmeli MS, Ay ZY. Determination of the stage and grade of periodontitis according to the current classification of periodontal and peri-implant diseases and conditions (2018) using machine learning algorithms. J Periodontal Implant Sci. 2023;53(1):38.
- Baumgart DC, Sandborn WJ. Crohn’s disease. The Lancet. 2012;380(9853):1590–605.
- Sedghi LM, Bacino M, Kapila YL. Periodontal Disease: The Good, The Bad, and The Unknown. Front Cell Infect Microbiol. 2021;11:766944.
- Lauritano, Boccalari, Stasio, Vella, Carinci, Lucchese, et al. Prevalence of Oral Lesions and Correlation with Intestinal Symptoms of Inflammatory Bowel Disease: A Systematic Review. Diagnostics. 2019;9(3):77.
- Lankarani, KB. Oral manifestation in inflammatory bowel disease: A review. World J Gastroenterol. 2013;19(46):8571.
- Tan CXW. Oral manifestations of Crohn’s disease. Ned Tijdschr Tandheelkd. 2018;125(01):15–20.
- Villanacci V, Reggiani-Bonetti L, Salviato T, Leoncini G, Cadei M, Albarello L, et al. Histopathology of IBD Colitis. A practical approach from the pathologists of the Italian Group for the study of the gastrointestinal tract (GIPAD). Pathologica. 2021;113(1):39–53.
- Habashneh RA, Khader YS, Alhumouz MK, Jadallah K, Ajlouni Y. The association between inflammatory bowel disease and periodontitis among Jordanians: a case-control study: Inflammatory bowel disease and periodontitis. J Periodontal Res. 2012;47(3):293–8.
- Zhang Y, Qiao D, Chen R, Zhu F, Gong J, Yan F. The Association between Periodontitis and Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. Khazaei S, editor. BioMed Res Int. 2021;2021:1–8.
- Caton JG, Armitage G, Berglundh T, Chapple ILC, Jepsen S, Kornman KS, et al. A new classification scheme for periodontal and peri-implant diseases and conditions – Introduction and key changes from the 1999 classification. J Clin Periodontol. 2018;45(S20).
- Stein JM, Lammert F, Zimmer V, Granzow M, Reichert S, Schulz S, et al. Clinical Periodontal and Microbiologic Parameters in Patients With Crohn’s Disease With Consideration of the CARD15 Genotype. J Periodontol. 2010;81(4):535–45.
- Zhang L, Gao X, Zhou J, Chen S, Zhang J, Zhang Y, et al. Increased risks of dental caries and periodontal disease in Chinese patients with inflammatory bowel disease. Int Dent J. 2020;70(3):227–36.
- Grossner-Schreiber B, Fetter T, Hedderich J, Kocher T, Schreiber S, Jepsen S. Prevalence of dental caries and periodontal disease in patients with inflammatory bowel disease: a case-control study. J Clin Periodontol. 2006;33(7):478–84.
- Brito F, Barros FCD, Zaltman C, Pugas Carvalho AT, De Vasconcellos Carneiro AJ, Fischer RG, et al. Prevalence of periodontitis and DMFT index in patients with Crohn’s disease and ulcerative colitis. J Clin Periodontol. 2008;35(6):555–60.
- Menegat JSB, Lira-Junior R, Siqueira MA, Brito F, Carvalho AT, Fischer RG, et al. Cytokine expression in gingival and intestinal tissues of patients with periodontitis and inflammatory bowel disease: An exploratory study. Arch Oral Biol. 2016;66:141–6.
- Koutsochristou V, Zellos A, Dimakou K, Panayotou I, Siahanidou S, Roma-Giannikou E, et al. Dental Caries and Periodontal Disease in Children and Adolescents with Inflammatory Bowel Disease: A Case–Control Study. Inflamm Bowel Dis. 2015;21(8):1839–46.
- Vavricka SR, Manser CN, Hediger S, Vögelin M, Scharl M, Biedermann L, et al. Periodontitis and Gingivitis in Inflammatory Bowel Disease: A Case–Control Study. Inflamm Bowel Dis. 2013;19(13):2768–77.
- Imai J, Ichikawa H, Kitamoto S, Golob JL, Kaneko M, Nagata J, et al. A potential pathogenic association between periodontal disease and Crohn’s disease. JCI Insight. 2021;6(23):e148543.
- Yin W, Ludvigsson JF, Liu Z, Roosaar A, Axéll T, Ye W. Inverse Association Between Poor Oral Health and Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol. 2017;15(4):525–31.
- Piras V, Usai P, Mezzena S, Susnik M, Ideo F, Schirru E, et al. Prevalence of Apical Periodontitis in Patients with Inflammatory Bowel Diseases: A Retrospective Clinical Study. J Endod. 2017;43(3):389–94.
- Baima G, Muwalla M, Testa G, Mazza F, Bebars A, Perotto S, et al. Periodontitis prevalence and severity in inflammatory bowel disease: A case–control study. J Periodontol. 2023;94(3):313–22.
- Tanwar H, Gnanasekaran JM, Allison D, Chuang LS, He X, Aimetti M, Baima G, Costalonga M, Cross RK, Sears C, Mehandru S, Cho J, Colombel JF, Raufman JP, Thumbigere-Math V. Unraveling the Link between Periodontitis and Inflammatory Bowel Disease: Challenges and Outlook. ArXiv. 2023; arXiv:2308.10907v1.
Figure 1.
An example of measuring radiographic bone loss using a Schei ruler where the red arrow indicates the line tangent to the cementoenamel junction, the yellow arrow indicates the line tangent to the highest point of the crown, and the blue line represents approximately 1.5 fields between the cementoenamel junction and the alveolar bone level.
Figure 1.
An example of measuring radiographic bone loss using a Schei ruler where the red arrow indicates the line tangent to the cementoenamel junction, the yellow arrow indicates the line tangent to the highest point of the crown, and the blue line represents approximately 1.5 fields between the cementoenamel junction and the alveolar bone level.
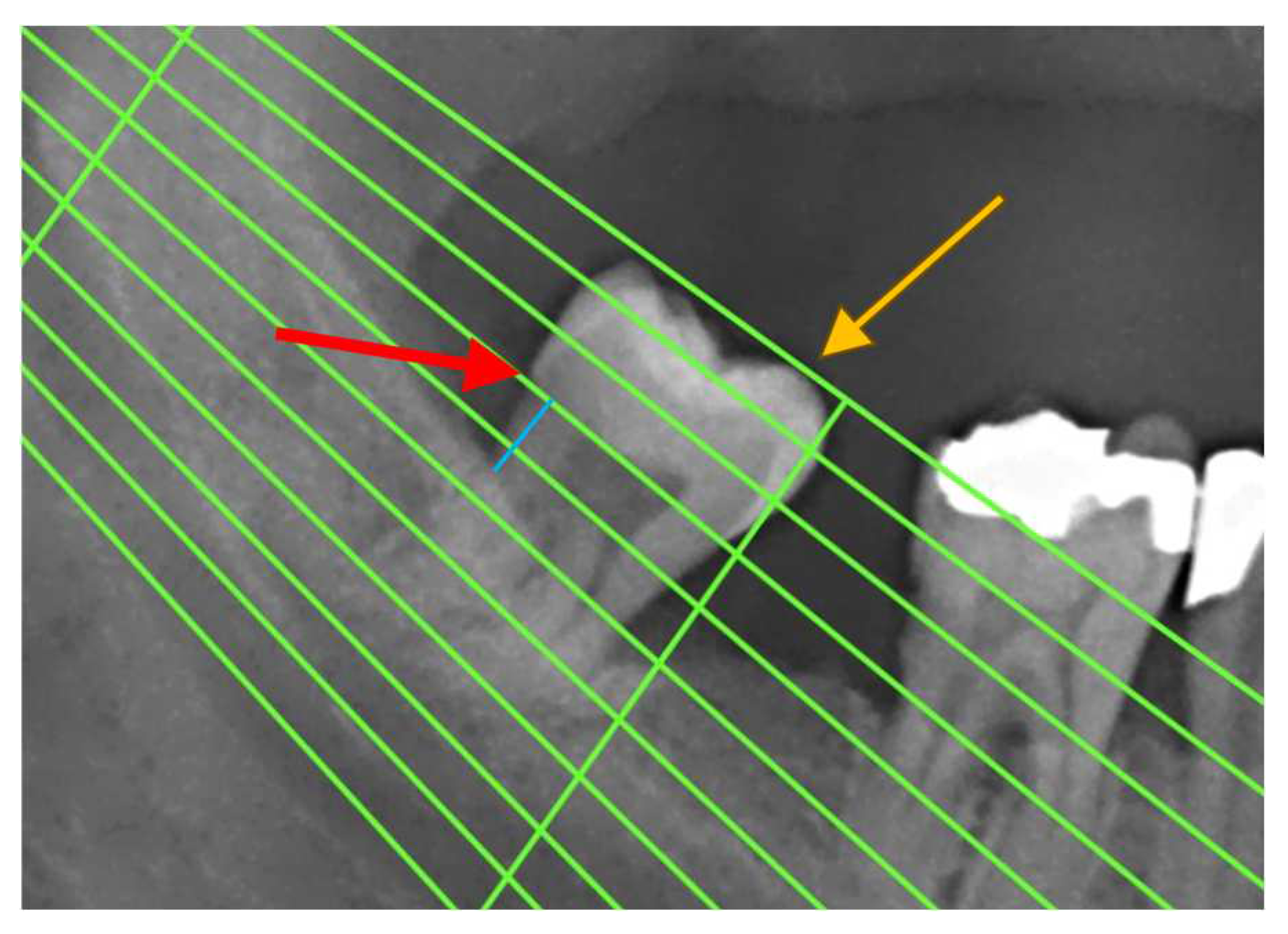
Figure 2.
Average values of CAL, PPD, BOP, and RBL according to CD activity scores (red – active disease; blue – remission).
Figure 2.
Average values of CAL, PPD, BOP, and RBL according to CD activity scores (red – active disease; blue – remission).
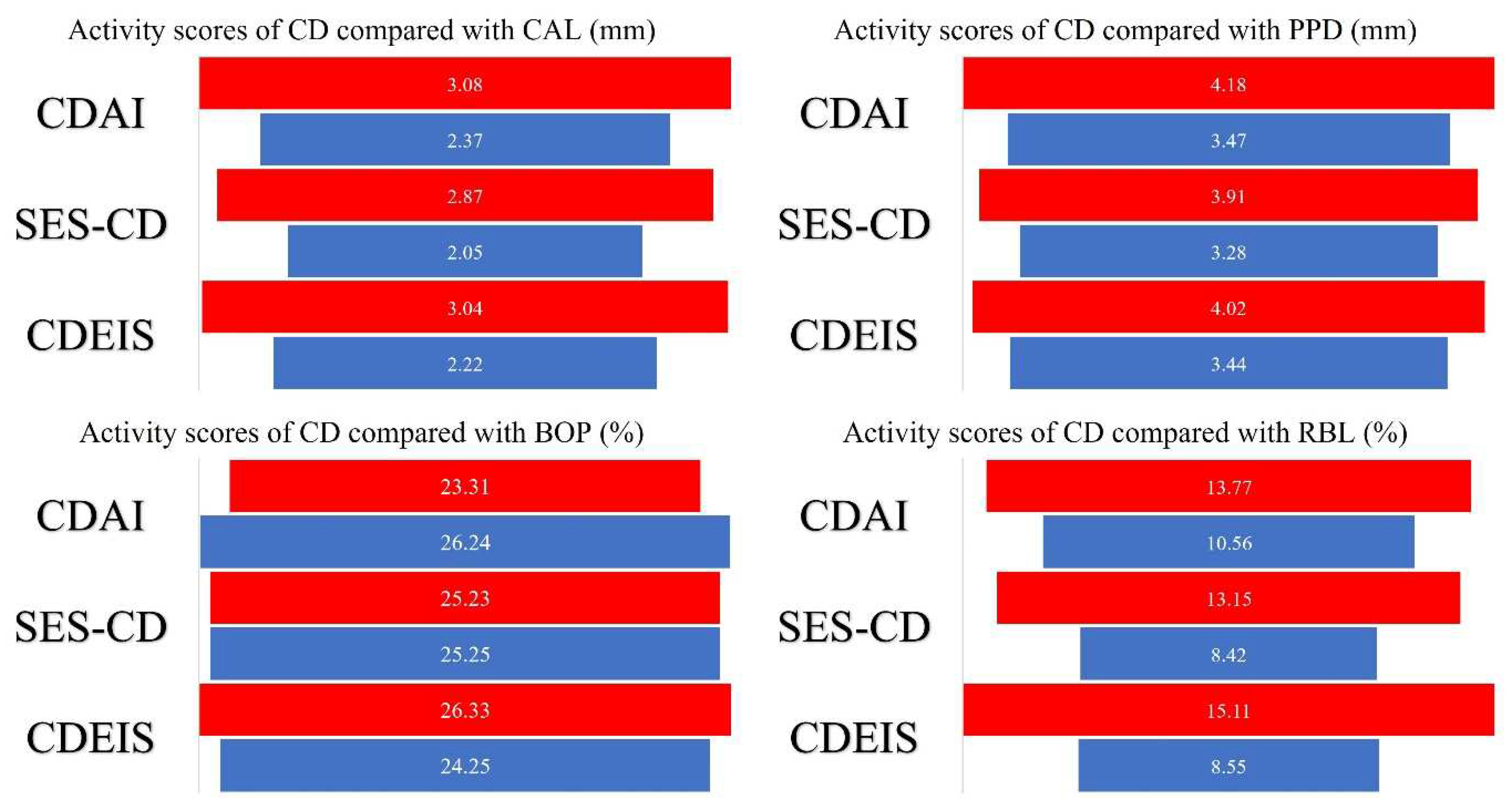
Figure 3.
ROC curves showing the sensitivity and the specificity of BOP, CAL and PPD in prediction of oral manifestations. These ROC curves show that all three are good predictors of belonging to the group that developed oral manifestations.
Figure 3.
ROC curves showing the sensitivity and the specificity of BOP, CAL and PPD in prediction of oral manifestations. These ROC curves show that all three are good predictors of belonging to the group that developed oral manifestations.
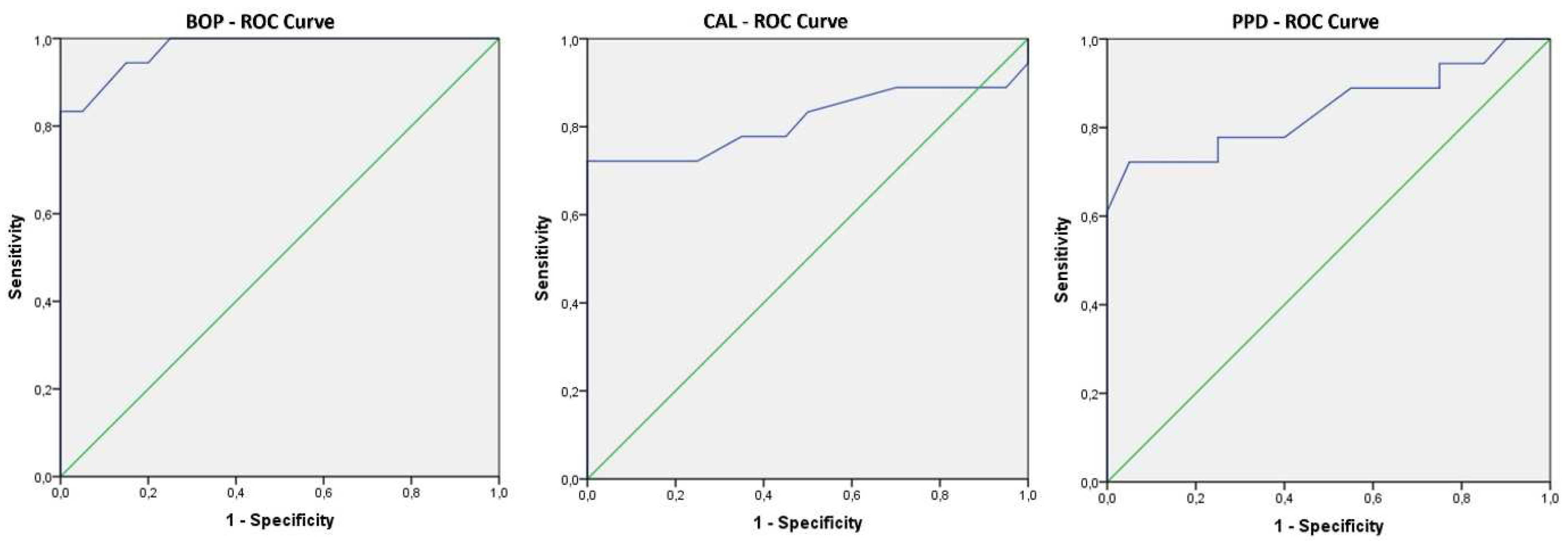

Table 1.
Referent values by stages of periodontal disease (classification of 2018).
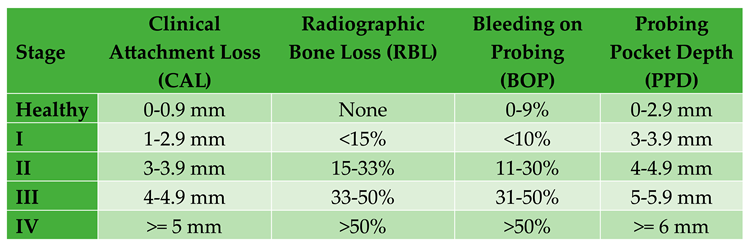 |
Table 2.
Clinical and demographic characteristics of the subjects presented as “mean value±standard deviation” or “median (The Interquartile Range - IQR)” depending on the normality test.
Table 2.
Clinical and demographic characteristics of the subjects presented as “mean value±standard deviation” or “median (The Interquartile Range - IQR)” depending on the normality test.
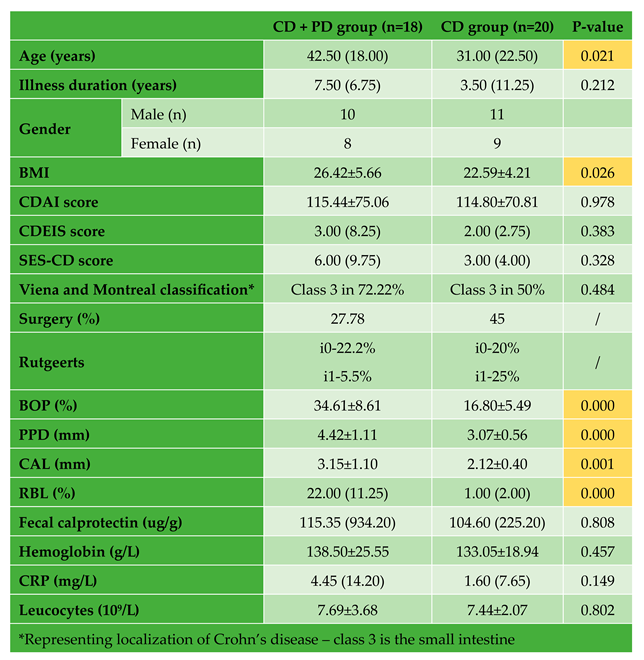 |
Table 3.
Mean and standard deviation of activity scores of CD and PD compared to stages of periodontal disease.
Table 3.
Mean and standard deviation of activity scores of CD and PD compared to stages of periodontal disease.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



