
Submitted:
30 November 2023
Posted:
01 December 2023
You are already at the latest version
Abstract
Background and Objectives: Obesity-related elevated body mass index (BMI) across life is associated with chronic low-grade inflammation and increased levels of C-reactive protein (CRP) in blood. CRP is a marker and promoter of inflammation. The objectives of this study were to examine the effect of obesity on the relationship between peripheral and gingival CRP levels and examine the effects of gingival CRP levels on gingival fluid inflammatory cytokines in periodontitis resistant obese individuals. Materials and Methods: Thirty-nine, periodontally healthy subjects were enrolled. Based on BMI scores, 20 subjects were categorized as lean and 19 as obese. A comprehensive periodontal examination was performed. Gingival crevicular fluid (GCF) and blood samples were collected. Both GCF and blood samples were assessed for interleukin-1β (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), tumor necrosis factor-α (TNF-α), interleukin-10 (IL-10), interleukin-17A (IL-17A) and CRP. Results: GCF CRP levels were significantly higher in obese than lean individuals. No statistically significant differences were noted between the two groups in both GCF and blood on any of the inflammatory cytokine levels. IL-17A was not detected in GCF of most subjects in both groups. GCF CRP levels were positively associated with blood CRP levels, the association tended to be stronger in obese individuals. GCF CRP showed no associations with GCF IL-10 in both groups. Although GCF CRP levels positively associated with multiple GCF inflammatory cytokines (e.g., IL-1β, IL-6, IL-8 and TNF-α) in all subjects, the associations tended to be weaker in obese individuals (e.g., IL-1β, IL-6, TNF-α). Furthermore, the levels of GCF inflammatory cytokines IL-6 and TNF-α were depressed in obese individuals. Conclusions: Obesity unfavorably influences the relationship between blood and GCF CRP levels and promotes increased CRP levels in GCF. Collectively, the findings suggest a dysregulated inflammatory cytokine response in the gingival tissues of obese individuals.
Keywords:
inflammatory cytokines
; C-reactive protein
; gingival fluid
; obesity
1. Introduction
Obesity is a chronic inflammatory disorder in which excessive fat accumulation presents a risk to health. In obesity, white fat tissue does not operate normally and does not expand to store excess energy. Enlarged visceral adipose tissue is infiltrated with proinflammatory immune cells (e.g., M1 macrophages and cytotoxic T cells), and it secretes excessive amounts of proinflammatory adipokines (e.g., adiponectin, leptin, visfatin, resistin, and chemerin) and cytokines (e.g., TNF-α, IL-1β, and IL-6) [1]. These adverse inflammatory signals induce a state of chronic systemic inflammation and increased levels of C-reactive protein (CRP) in blood [2].
CRP is an acute inflammatory protein and an important marker of systemic inflammation [3]. CRP is primarily synthesized in liver hepatocytes. Hepatocytes are the primary cells that exhibit the transcriptional activation of the CRP gene in response to elevated levels of inflammatory cytokines, specifically IL-6. Other cells, including macrophages, lymphocytes, endothelial cells, and adipocytes, can also synthesize CRP [3]. CRP is generated as a homopentameric protein known as native CRP (nCRP), which, at sites of inflammation, permanently splits into five distinct monomers known as monomeric CRP (mCRP) [3]. CRP was named for its response to the capsular (C)-polysaccharide of Pneumococcus [4]. CRP is not only a marker of infection and inflammation but also plays a protective role against bacterial infections through the activation of complement, the opsonization of pathogens, and the induction of inflammatory cytokines [3]. CRP is elevated in many inflammatory conditions, including obesity [2].
Periodontitis is a chronic inflammatory oral disease distinguished by gingival inflammation and the destruction of alveolar bone. Disproportionate host responses and bacterial dysbiosis are the two main etiological factors [5]. Failure in the resolution of gingival inflammation leads to destructive periodontal disease. In the pathogenesis of periodontitis, monocytes/macrophages play important roles in tissue destruction and repair. Their cytokine secretions contribute significantly to the inflammatory burden in the gingival tissues, they bridge innate immunity with adaptive immunity, and, finally, they promote the resolution of inflammation [6]. The major inflammatory cytokines involved in periodontitis include IL-1β [7,8], TNFα [9,10], IL-6 [11,12], IL-8 [13,14], IL-17A [5], and anti-inflammatory IL-10 [15,16].
Periodontal disease is prevalent among obese individuals [17,18], and the response to periodontal therapy is compromised [19]. Inflammation may provide a common link between periodontal disease and obesity [20,21]. Previously, it was shown that CRP levels are elevated in the gingival fluid of obese individuals [22]. Since CRP is a proinflammatory protein, we hypothesized that increased levels of CRP in the gingival tissues of obese individuals would promote gingival inflammation and may explain the increased susceptibility to periodontitis in obesity. Previous studies mainly focused on periodontally diseased individuals [22]. The effect of obesity on the periodontium without the confounding effect of periodontitis is not well understood. Obesity-related increased levels of CRP in gingival tissues may provide insightful information about how obesity affects periodontal health.
The aims of this study were to examine the effect of obesity on the relationship between peripheral and gingival CRP levels and to examine the association of gingival CRP levels with clinical periodontal measures and gingival fluid inflammatory cytokines in periodontally healthy obese individuals.
2. Materials and Methods
Recently, we described a distinct population of elderly individuals (>60 yrs.) who are resistant to periodontitis [23,24]. The recruitment and enrollment process for subjects has already been reported [23,24].
The Recruitment, Screening, and Enrollment of Subjects: A total of 136 individuals were interviewed over the phone to determine their eligibility. In total, 54 individuals agreed to participate, 39 of whom met the criteria for periodontal health (pocket depth ≤ 3 mm and bleeding on probing (BOP) < 10%) [25]. All subjects provided written informed consent. A history of diabetes, fewer than 15 teeth, pocket depth > 3 mm and BOP ≥ 10%, antibiotic treatment within the previous three months, dental cleaning within the previous three months, current tobacco use, non-English speaking, and limitations interfering with dental examinations were among the exclusion criteria.
A thorough medical history interview was conducted. The measures of height, weight, and BMI were recorded. Waist circumference was measured with a measuring tape placed around the abdomen at the top of the hip and at the level of the navel. A questionnaire about dietary preferences, educational background, income, dental care, and history of cigarette smoking was completed by all participants [23,24].
2.1. Clinical Assessments and Sample Collection
All dental exams were conducted by a single, experienced dental examiner (LL). The examiner was familiar with and trained in the use of the clinical assessments used in this study [23,24]. The plaque index (PI) and gingival index (GI) were recoded around all existing teeth [26]. Teeth with crowns, extensive restorations, partially erupted teeth, and third molars were not examined. Missing teeth and dental caries were also noted.
A standard periodontal probe (Michigan-O Probe Williams-labeled, Hu-Friedy, Chicago, IL, USA) was used for probing measurements. Probing depth (PD) was recorded at six sites per tooth: the mesiobuccal, buccal, distobuccal, mesiolingual, lingual, and distolingual sites. The position of the gingival margin (GM) in relation to the cementoenamel junction was recorded at the same six sites per tooth. The periodontal attachment level (AL) was calculated using the formula AL = PD + GM. BOP was also recorded.
Blood Samples: A blood sample was collected via a single vein puncture into serum-separating (red/black-topped) Vacutainer tubes at the scheduled clinic visit. Blood was allowed to clot at room temperature for 30 min; the clot was removed by centrifuging at 1000–2000 x g for 15 min [27]. Serum was collected and aliquoted into 8 × 0.6 mL microcentrifuge tubes. Serum samples were frozen at −80 °C until analyzed.
GCF was collected with filter paper strips (Oraflow Inc., Smithtown, NY, USA). Three interproximal sites (PD ≤ 3 mm, no BOP, and no loss of attachment) were selected at random. Before collecting GCF samples, the chosen sites were isolated, supragingival plaque was removed, and the tooth surface was air-dried. After gently inserting the strip 1 to 2 mm into the gingival crevice, it was left in place for 30 s. Blood-contaminated strips were discarded. Sample volume was estimated using a Periotron 8000 (Oraflow Inc., Smithtown, NY, USA). The 3 GCF strips collected from each subject were placed in a single microcentrifuge tube. The tube was sealed, put on ice, and then frozen at −80 °C until the laboratory analysis was performed. All clinical evaluations and sample collections were performed on the same day.
2.2. Laboratory Analyses
The GCF and serum samples were thawed and processed for analysis prior to running cytokine assays as per the standard protocol. The GCF and serum samples were analyzed for IL-1β, IL-6, IL-8, IL-10, IL-17A, TNF-α, and CRP.
The Elution of GCF: the three strips from each vial were immersed in 1 mL of elution buffer consisting of PBS containing 0.1% Triton X-100 and 0.1% bovine serum albumin (BSA) [28]. The elution process was performed overnight in a refrigerator [28]. To determine the percentage of recovery, a set of controls for each biomarker (in which a known concentration of each biomarker was added to the filter papers) was utilized to simulate the elution of the biological components under investigation from the filter paper strips. Every biomarker had a recovery rate of at least 98%. Standard curves were generated in the same elution buffer, thus preserving the integrity of the matrix.
CRP concentrations were determined using enzyme-linked immunosorbent assay (ELISA) kits from AssayPro (St. Charles, MO, USA). Each sample was assayed in duplicate in accordance with the manufacturers’ instructions [27], and the data are expressed as ng/mL. The minimal detectable concentration was 100 pg/mL. IL-1β, IL-6, IL-8, IL-10, IL-17A, and TNF-α levels were determined simultaneously using a human cytokine/chemokine Milliplex Luminex magnetic bead multiplexed panel (EMD Millipore, Billerica, MA, USA) coated with specific antibodies (Milliplex MAP Kit), and they are expressed as pg/mL. The samples were run in duplicate as directed by the manufacturer. Fluorescence was read using a Luminex 200 (Millipore). Analytes were normalized to the total protein concentration determined using a Bradford assay (using the elution buffer as the baseline), and the data are expressed as pg/mL.
2.3. Statistical Analysis
This is a convenience sample of a previously described periodontitis-resistant cohort [23,24]. A total of 20 subjects were lean (BMI <25), 11 subjects were overweight (BMI 25–<30), and 8 subjects were obese (BMI ≥ 30). Overweight and obese subjects were combined into one group for data analysis. CRP, cytokine levels, and clinical periodontal measures were all positively skewed. For statistical analyses, non-parametric tests were employed. The Wilcoxon rank-sum test for continuous measurements and the Pearson chi-square test for categorical variables were used to identify significant differences between groups.
Zero-order correlations between blood CRP, GCF CRP, periodontal measures, and GCF inflammatory cytokines were determined with Pearson correlation analyses. We used rank regression analyses adjusted for age, gender, and race to examine the associations of the measures of obesity (BMI and waist size) with peripheral CRP levels, peripheral CRP levels with GCF CRP levels, GCF CRP with clinical measures of gingival health, and GCF inflammatory cytokines. A type 1 error rate of 5% was used.
3. Results
The demographics and clinical data of this cohort were previously reported and are summarized in Table 1 [24].
Nineteen subjects were classified as overweight/obese, while twenty subjects were classified as lean (BMI of ≥25). All subjects were medically healthy and non-smokers. The two groups were statistically comparable on age, sex, race, blood pressure readings, the number of missing teeth, PI, GI, BOP, PD, and AL. As predicted, the obese group had considerably greater weight, waist size, and BMI scores. The subjects in both groups satisfied the criterion for periodontal health. PI tended to be higher in the obese subjects, even though it was statistically comparable between the two groups. All subjects reported that they practiced oral hygiene at least once a day and received preventive dental care on average twice a year. The subjects’ blood pressure readings fell within the normal ranges for their age. Systolic blood pressure was somewhat higher in the obese individuals.
In Table 2, we compare blood and GCF CRP and inflammatory cytokine levels between the lean and obese individuals. For GCF measures (Table 2a), the univariate analyses showed that the two groups were statistically comparable on all measures, except for GCF CRP, with levels being significantly higher in the obese individuals than in the lean individuals. Despite the lack of statistical significance, IL-6 and TNF-α levels tended to be higher in the lean than in the obese individuals; IL-8 tended to be higher in the obese than in the lean individuals. GCF IL-17A was detected at low levels in only two subjects (one lean subject and one obese subject) and was excluded from analysis. The lack of detectible GCF IL-17A in most subjects suggests that IL-17A activity is absent in healthy gingival tissues. For blood measures (Table 2b), both CRP and inflammatory cytokine levels were statistically comparable between the obese and lean subjects.
The differences in GCF and blood CRP levels between the lean and obese individuals are illustrated in Figure 1. Although blood CRP levels tended to be higher in the obese than in the lean individuals, the differences were not statistically significant. Blood CRP levels showed a high variance among the obese individuals, which may explain the lack of statistical significance between the two groups. By contrast, GCF levels were significantly higher in the obese than in the lean individuals.
We then examined the association between blood and gingival CRP levels. The Pearson correlation analysis indicated a significant correlation between blood and GCF CRP levels in all subjects combined (r = 0.52, p = 0.001). Figure 2 presents the regression line slopes of the association of blood with GCF CRP according to obesity status. Although the line slop of the obese group was steeper than that of the lean group, the difference was not statistically significant.
Blood cytokine measures showed no statistically significant associations with obesity measures (BMI and waist size), blood pressure measures, or GCF cytokine measures (data not presented).
Next, we investigated the association of GCF CRP levels and oral hygiene (PI scores) with measures of gingival health and GCF inflammatory cytokines. Zero-order correlation analyses showed significant positive associations between GCF CRP levels with multiple measures of gingival health and GCF inflammatory cytokines in both the lean and obese individuals (Table 3a). The correlation coefficients for IL-1β, IL-6, and TNF-α tended to be stronger in the lean individuals; by contrast, the correlation coefficient for IL-8 tended to be stronger in the obese individuals (Table 3a). These data suggest that GCF CRP levels may be involved in the promotion of inflammation in gingival tissues. IL-10 showed no association with GCF CRP in both subject groups, and the GCF IL-1β association with GCF CRP in the obese subjects lacked statistical significance (Table 3a). In Table 3b, we compare the association of PI scores with measures of gingival health and GCF inflammatory cytokines between the lean and obese individuals. In both groups, PI was significantly associated with BOP, but the association was weaker in the obese individuals. No statistically significant correlations were noted between PI and inflammatory cytokines. The Pearson correlation coefficients between PI and inflammatory cytokines were poor in both groups and tended to be even weaker in the obese than in the lean individuals.
Finally, in a series of rank regression models adjusted for age, race, and gender, we further examined the association of measures of obesity (BMI and waist size) with peripheral CRP levels, peripheral CRP levels with GCF CRP levels, GCF CRP with clinical measures of gingival health, and GCF inflammatory cytokines. Figure 3 outlines the noted associations between the various factors assessed in the multivariate analyses. As expected, both waist size and BMI measures were positively associated with serum CRP levels. Waist size measures showed a stronger association with serum CRP levels than BMI measures.
In the adjusted models, the association between blood and GCF CRP levels remained significant. Again, the strength of the association was statistically comparable between the lean and the obese individuals. The multivariate analyses also confirmed the positive associations of GCF CRP with clinical measures of gingival health (BOP and PD) and the inflammatory cytokines IL-6, IL-8, and TNF-α; the strengths of the associations for these measures were statistically comparable between the two groups. The association of GCF CRP with IL-1β showed a group interaction, and the association was significant only in the lean individuals. The non-significant association between GCF CRP and IL-1β in the obese individuals confirms the univariate findings.
Additional multivariate analyses adjusting for oral hygiene (PI scores) did not alter the previously noted associations between GCF CRP with clinical measures of gingival health and the inflammatory cytokines IL-1β, IL-6, IL-8, and TNF-α (data not presented). PI showed an association with BOP (standardized beta = 0.52, p = 0.0006) independent from GCF CRP levels. In addition, the multivariate analyses also showed that IL-6 and TNF-α levels were significantly lower in the obese than in the lean individuals (Figure 4).
4. Discussion
The aims of this study were to examine the effect of obesity on the association between peripheral blood and GCF CRP levels and to examine the association between GCF CRP and GCF inflammatory cytokines in periodontally healthy obese individuals without the confounding effect of periodontal disease. The data showed that blood CRP levels positively correlated with GCF CRP levels in all subjects, and the association tended to be stronger in the obese individuals. GCF CRP levels were significantly higher in the obese than in the lean individuals. Although GCF CRP levels were positively associated with multiple GCF inflammatory cytokines (e.g., IL-1β, IL-6, and TNF-α) in all subjects, the associations tended to be weaker in the obese individuals. Furthermore, the levels of the GCF inflammatory cytokines IL-6 and TNF-α were decreased in the obese individuals. Collectively, these findings suggest a weakened inflammatory cytokine response to increased levels of CRP in the gingival tissues of obese individuals.
The Adventist Health Study-2 (AHS-2) cohort, which consists of over 96,000 Seventh-Day Adventists in the US and Canada, was used to recruit study participants [29,30]. Health-conscious Seventh-Day Adventists build on good health practices by avoiding meat and emphasizing a plant-based diet rich in whole grains, legumes, and nuts. To increase power and supplement the limited number of individuals available, overweight and obese subjects were combined into a single group. The average BMI of the obese participants in this study was 32, indicating low-level obesity. The clinical measures, CRP levels, and cytokine levels of the obese and overweight participants were statistically similar. The health-conscious behavior and good systemic health of this cohort may explain the lack of differences in systemic inflammatory biomarker levels between the lean and obese individuals.
The primary site of CRP production is the liver [3]. The CRP levels in blood reflect the presence of inflammation [3]. Our data showed a significant correlation between blood and GCF CRP levels in all subjects, suggesting that blood CRP contributes to GCF CRP levels. Contrary to our findings, a previous study reported a lack of correlation between blood and the GCF levels of CRP in periodontitis subjects [31]. It is possible that gingival inflammation in periodontitis may mask the association between blood and GCF CRP levels. Our data also showed that obesity has an unfavorable influence on the association between blood and GCF CRP levels; the association was more pronounced in the obese individuals. Despite the variability in blood CRP levels in this cohort, the obese individuals tended to have higher blood CRP levels. This may explain the stronger association between blood and CRP levels in the obese individuals. However, the difference in the strength of the association was not statistically significant. Again, the variance in blood CRP levels may also explain the lack of statistical significance.
In the current study, GCF CRP levels were significantly elevated in the obese individuals. These data support those of previous studies showing elevated GCF CRP in obese individuals [32] and expand on previous reports by including periodontitis-resistant elderly individuals. GCF is a transudate of serum and thus includes both serum constituents and locally produced molecules. Blood is the primary contributor of CRP in GCF [33]. In this cohort, there was variance in blood CRP levels among the obese subjects. Yet, despite the blood CRP variance, gingival fluid demonstrated significantly elevated levels of CRP in the obese individuals. These findings suggest the possibility of local CRP production in the gingival tissues of obese individuals. Although a previous study did not show CRP mRNA in the gingival tissues [33], gingival CRP production was not examined in obesity. Possible local cells that may contribute to gingival CRP production may include lymphocytes [34], macrophages [35], and epithelial cells [36].
CRP is not only a marker of inflammation but also plays an active role in the inflammatory process [3]. Our data showed significant associations between GCF CRP levels and IL-1β, IL-6, IL-8, and TNF-α cytokine measures.
IL-1β is a proinflammatory cytokine with angiogenic activity that promotes blood vessel formation in inflamed tissues [37]. IL-1β levels are elevated in inflamed gingival tissues [38]. Gingival epithelial cells produce IL-1β in response to microbial pathogens [39]. Activated macrophages and other inflammatory cells release TNF-α, a significant cytokine that promotes inflammation [10]. TNFα is elevated in the GCF of individuals with gingival inflammation [38,40] and helps the inflammatory front advance further into gingival connective tissue. IL-6 is a multifunctional proinflammatory cytokine primarily produced by T cells. Its main role is the final differentiation of B lymphocytes into plasma cells, which is associated with periodontal tissue damage [12].
Previous research showed that elevated CRP levels in atheroma induce the production of IL-1β, IL-6, and TNF-α by macrophages [41]. A similar effect may occur in gingival tissues, where increased levels of CRP may promote inflammatory cytokine production from local immune cells. Conversely, an increased production of inflammatory cytokines in the gingival tissues may induce the local transcription of CRP [42,43,44].
Our data showed that the association of GCF CRP with IL-1β was statistically nonsignificant in the obese individuals. Furthermore, the multivariate analyses showed that GCF IL-6 and TNF-α levels were decreased in the obese individuals. These data suggest a dysregulated inflammatory cytokine response to increased levels of CRP in the gingival tissues of obese individuals. The main contributors of inflammatory cytokines in the gingiva are macrophages [45]. In an animal model, the infiltration of macrophages was significantly decreased in the gingival tissues of obese mice [46]. Furthermore, obese mice with periodontitis showed a weakened macrophage inflammatory response with a reduced expression of the NLRP3 signal pathway [46]. These obesity-related alterations in macrophage number and function in the gingival tissues may lead to innate immune dysfunction and adversely affect cytokine production. Human studies examining gingival macrophage activity in obesity are lacking.
The chemokine IL-8 is mostly secreted by macrophages and monocytes. The recruitment and activation of neutrophils are its primary roles [13]. The neutrophils and monocytes recruited by IL-8 release copious inflammatory cytokines, such as IL-1β and TNF-α. CRP plays a role in atherosclerosis via enhanced IL-8 production and an increased expression of IL-8 mRNA [47]. CRP promotes IL-8 production via the activation of the ERK, p38 MAPK, and JNK pathways [47]. In our study, IL-8 was the only cytokine that tended to show a strong association with GCF CRP in the obese subjects, suggesting that IL-8 production in gingival tissues is not weakened by obesity. Unlike IL-1β, IL-6, and TNF-α, which are primarily produced by cells of the immune system, such as monocytes, macrophages, and T-helper cells, IL-8 is produced by numerous other cell types, including inflammatory cells, as well as keratinocytes, fibroblasts, and endothelial cells. Although the infiltration and function of immune cells in the gingival tissues of obese individuals may be compromised, other cells may compensate for immune cell deficiency and produce IL-8 in the gingival tissues of obese individuals.
The anti-inflammatory cytokine IL-10 inhibits the activation of immune cells. IL-10 levels tend to be inversely associated with pocket depth [13]. Our data showed no association between GCF IL-10 and GCF CRP. CRP decreases IL-10 production in immune cells via the inhibition of cyclic AMP production [48]. The combination of obesity-related monocyte dysfunction and the suppressing effect of CRP on IL-10 secretion may explain the noted lack of association between GCF CRP and IL-10 in our results.
Despite this study’s limitations, which include the limited sample size and participants’ low-grade obesity, relevant associations were noted between the obesity-related increase in GCF CRP levels and measures of periodontal health and GCF inflammatory cytokines, which further our understanding of how obesity may impact periodontal health. Future studies examining local cytokine production in relation to immune cell infiltration in the gingival tissues of obese individuals could further enhance our understanding of how obesity impacts gingival immune/inflammatory responses and identify common inflammatory pathways that can be pharmacologically targeted to improve the response to therapy.
5. Conclusions
Obesity unfavorably influences the relationship between blood and GCF CRP levels and promotes increased CRP levels in GCF. Our findings were contrary to our hypothesis. Despite the obesity-related increase in GCF CRP levels, the clinical measures of gingival inflammation and GCF inflammatory cytokine levels were not significantly increased. The association between GCF CRP and GCF IL-1β levels in the obese individuals lacked statistical significance. Furthermore, the levels of the GCF inflammatory cytokines IL-6 and TNF-α were decreased in the obese individuals. Collectively, these findings suggest a weakened inflammatory cytokine response in the gingival tissues of obese individuals.
Author Contributions
Conceptualization, A.K. and G.F.; methodology, A.K. and D.B.; formal analysis, A.K.; investigation, A.K., L.L., and C.I.; writing—original draft preparation, A.K.; writing—review and editing, A.K., D.B., and G.F; supervision, A.K.; project administration, A.K.; funding acquisition, A.K. and G.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the LLU-GRASP small project grant #5130413, Loma Linda University, awarded to Dr. Khocht and NIH grant # U01CA152939 awarded to Dr. Fraser (NIH support for parent cohort Adventist Health Study-2).
Institutional Review Board Statement
The study protocol and consent forms were approved by Loma Linda University Institutional Review Board, approval #5160077, March 23, 2017.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data published in this study are available upon reasonable request from the first author.
Conflicts of Interest
The authors declare that they have no conflicts of interest or financial affiliations to disclose.
References
- Jung, U.J.; Choi, M.S. Obesity and its metabolic complications: The role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int. J. Mol. Sci. 2014, 15, 6184–6223. [CrossRef]
- Park, H.S.; Park, J.Y.; Yu, R. Relationship of obesity and visceral adiposity with serum concentrations of CRP, TNF-alpha and IL-6. Diabetes Res. Clin. Pract. 2005, 69, 29–35. [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [CrossRef]
- Tillett, W.S.; Francis, T. Serological Reactions in Pneumonia with a Non-Protein Somatic Fraction of Pneumococcus. J. Exp. Med. 1930, 52, 561–571. [CrossRef]
- Zhang, S.; Yu, N.; Arce, R.M. Periodontal inflammation: Integrating genes and dysbiosis. Periodontol. 2000 2020, 82, 129–142. [CrossRef]
- Kornman, K.S. Mapping the pathogenesis of periodontitis: A new look. J. Periodontol. 2008, 79, 1560–1568. [CrossRef]
- Prince, L.R.; Allen, L.; Jones, E.C.; Hellewell, P.G.; Dower, S.K.; Whyte, M.K.; Sabroe, I. The role of interleukin-1beta in direct and toll-like receptor 4-mediated neutrophil activation and survival. Am. J. Pathol. 2004, 165, 1819–1826. [CrossRef]
- Tamura, M.; Sebastian, S.; Yang, S.; Gurates, B.; Fang, Z.; Bulun, S.E. Interleukin-1beta elevates cyclooxygenase-2 protein level and enzyme activity via increasing its mRNA stability in human endometrial stromal cells: An effect mediated by extracellularly regulated kinases 1 and 2. J. Clin. Endocrinol. Metab. 2002, 87, 3263–3273. [CrossRef]
- Sainson, R.C.; Johnston, D.A.; Chu, H.C.; Holderfield, M.T.; Nakatsu, M.N.; Crampton, S.P.; Davis, J.; Conn, E.; Hughes, C.C. TNF primes endothelial cells for angiogenic sprouting by inducing a tip cell phenotype. Blood 2008, 111, 4997–5007. [CrossRef]
- Zhang, Y.H.; Heulsmann, A.; Tondravi, M.M.; Mukherjee, A.; Abu-Amer, Y. Tumor necrosis factor-alpha (TNF) stimulates RANKL-induced osteoclastogenesis via coupling of TNF type 1 receptor and RANK signaling pathways. J Biol Chem. 2001, 276, 563–568. [CrossRef]
- Barnes, T.C.; Anderson, M.E.; Moots, R.J. The many faces of interleukin-6: The role of IL-6 in inflammation, vasculopathy, and fibrosis in systemic sclerosis. Int. J. Rheumatol. 2011, 2011, 721608. [CrossRef]
- Giannopoulou, C.; Kamma, J.J.; Mombelli, A. Effect of inflammation, smoking and stress on gingival crevicular fluid cytokine level. J. Clin. Periodontol. 2003, 30, 145–153. [CrossRef]
- Gamonal, J.; Acevedo, A.; Bascones, A.; Jorge, O.; Silva, A. Levels of interleukin-1 beta, -8, and -10 and RANTES in gingival crevicular fluid and cell populations in adult periodontitis patients and the effect of periodontal treatment. J. Periodontol. 2000, 71, 1535–1545. [CrossRef]
- Senturk, T.; Kozaci, L.D.; Kok, F.; Kadikoylu, G.; Bolaman, Z. Proinflammatory cytokine levels in hyperthyroidism. Clin Invest Med. 2003, 26, 58–63.
- Couper, K.N.; Blount, D.G.; Riley, E.M. IL-10: The master regulator of immunity to infection. J. Immunol. 2008, 180, 5771–5777. [CrossRef]
- Moore, K.W.; de Waal Malefyt, R.; Coffman, R.L.; O’Garra, A. Interleukin-10 and the interleukin-10 receptor. Annu. Rev. Immunol. 2001, 19, 683–765. [CrossRef]
- Arboleda, S.; Vargas, M.; Losada, S.; Pinto, A. Review of obesity and periodontitis: An epidemiological view. Br. Dent. J. 2019, 227, 235–239. [CrossRef]
- Martinez-Herrera, M.; Silvestre-Rangil, J.; Silvestre, F.J. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e708–e715. [CrossRef]
- Akram, Z.; Safii, S.H.; Vaithilingam, R.D.; Baharuddin, N.A.; Javed, F.; Vohra, F. Efficacy of non-surgical periodontal therapy in the management of chronic periodontitis among obese and non-obese patients: A systematic review and meta-analysis. Clin. Oral Investig. 2016, 20, 903–914. [CrossRef]
- Iwashita, M.; Hayashi, M.; Nishimura, Y.; Yamashita, A. The Link Between Periodontal Inflammation and Obesity. Curr. Oral Health Rep. 2021, 8, 76–83. [CrossRef]
- Pamuk, F.; Kantarci, A. Inflammation as a link between periodontal disease and obesity. Periodontol. 2000 2022, 90, 186–196. [CrossRef]
- Akram, Z.; Abduljabbar, T.; Abu Hassan, M.I.; Javed, F.; Vohra, F. Cytokine Profile in Chronic Periodontitis Patients with and without Obesity: A Systematic Review and Meta-Analysis. Dis. Markers. 2016, 2016, 4801418. [CrossRef]
- Khocht, A.; Orlich, M.; Paster, B.; Bellinger, D.; Lenoir, L.; Irani, C.; Fraser, G. Cross-sectional comparisons of subgingival microbiome and gingival fluid inflammatory cytokines in periodontally healthy vegetarians versus non-vegetarians. J. Periodontal Res. 2021, 56, 1079–1090. [CrossRef]
- Khocht, A.; Paster, B.; Lenoir, L.; Irani, C.; Fraser, G. Metabolomic profiles of obesity and subgingival microbiome in periodontally healthy individuals: A cross-sectional study. J. Clin. Periodontol. 2023, 50, 1455–1466. [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89 (Suppl 1), S1–S8. [CrossRef]
- Loe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [CrossRef]
- Dos Santos, H.; Raphael, J.C.; Reis, W.P.; Gaio, J.; Berk, L.S.; Bellinger, D.L.; Lee, J.W. The Association between Affect and Biomarkers of Stress and Inflammation in Healthy Seventh-Day Adventists. Adv. Mind Body Med. 2019, 33, 12–20.
- Aboyoussef, H.; Carter, C.; Jandinski, J.J.; Panagakos, F.S. Detection of prostaglandin E2 and matrix metalloproteinases in implant crevicular fluid. Int. J. Oral Maxillofac. Implants. 1998, 13, 689–696.
- Fraser, G.; Katuli, S.; Anousheh, R.; Knutsen, S.; Herring, P.; Fan, J. Vegetarian diets and cardiovascular risk factors in black members of the Adventist Health Study-2. Public Health Nutr. 2015, 18, 537–545. [CrossRef]
- Fraser, G.E.; Jaceldo-Siegl, K.; Henning, S.M.; Fan, J.; Knutsen, S.F.; Haddad, E.H.; Sabaté, J.; Beeson, W.L.; Bennett, H. Biomarkers of Dietary Intake Are Correlated with Corresponding Measures from Repeated Dietary Recalls and Food-Frequency Questionnaires in the Adventist Health Study-2. J. Nutr. 2016, 146, 586–594. [CrossRef]
- Baser, U.; Oztekin, G.; Ademoglu, E.; Isik, G.; Yalcin, F. Is the severity of periodontitis related to gingival crevicular fluid and serum high-sensitivity C-reactive protein concentrations? Clin. Lab. 2014, 60, 1653–1658. [CrossRef]
- Pradeep, A.R.; Priyanka, N.; Prasad, M.V.; Kalra, N.; Kumari, M. Association of progranulin and high sensitivity CRP concentrations in gingival crevicular fluid and serum in chronic periodontitis subjects with and without obesity. Dis. Markers. 2012, 33, 207–213. [CrossRef]
- Megson, E.; Fitzsimmons, T.; Dharmapatni, K.; Bartold, P.M. C-reactive protein in gingival crevicular fluid may be indicative of systemic inflammation. J. Clin. Periodontol. 2010, 37, 797–804. [CrossRef]
- Kuta, A.E.; Baum, L.L. C-reactive protein is produced by a small number of normal human peripheral blood lymphocytes. J. Exp. Med. 1986, 164, 321–326. [CrossRef]
- Yasojima, K.; Schwab, C.; McGeer, E.G.; McGeer, P.L. Generation of C-reactive protein and complement components in atherosclerotic plaques. Am. J. Pathol. 2001, 158, 1039–1051. [CrossRef]
- Gould, J.M.; Weiser, J.N. Expression of C-reactive protein in the human respiratory tract. Infect Immun. 2001, 69, 1747–1754. [CrossRef]
- Carmi, Y.; Dotan, S.; Rider, P.; Kaplanov, I.; White, M.R.; Baron, R.; Abutbul, S.; Huszar, M.; Dinarello, C.A.; Apte, R.N.; et al. The role of IL-1beta in the early tumor cell-induced angiogenic response. J. Immunol. 2013, 190, 3500–3509. [CrossRef]
- Baser, U.; Cekici, A.; Tanrikulu-Kucuk, S.; Kantarci, A.; Ademoglu, E.; Yalcin, F. Gingival inflammation and interleukin-1 beta and tumor necrosis factor-alpha levels in gingival crevicular fluid during the menstrual cycle. J Periodontol. 2009, 80, 1983–1990. [CrossRef]
- Uchida, Y.; Shiba, H.; Komatsuzawa, H.; Takemoto, T.; Sakata, M.; Fujita, T.; Kawaguchi, H.; Sugai, M.; Kurihara, H. Expression of IL-1 beta and IL-8 by human gingival epithelial cells in response to Actinobacillus actinomycetemcomitans. Cytokine. 2001, 14, 152–161. [CrossRef]
- Ertugrul, A.S.; Sahin, H.; Dikilitas, A.; Alpaslan, N.; Bozoglan, A. Comparison of CCL28, interleukin-8, interleukin-1beta and tumor necrosis factor-alpha in subjects with gingivitis, chronic periodontitis and generalized aggressive periodontitis. J. Periodontal. Res. 2013, 48, 44–51. [CrossRef]
- Han, K.H.; Hong, K.H.; Park, J.H.; Ko, J.; Kang, D.H.; Choi, K.J.; Hong, M.-K.; Park, S.-W.; Park, S.-J. C-reactive protein promotes monocyte chemoattractant protein-1--mediated chemotaxis through upregulating CC chemokine receptor 2 expression in human monocytes. Circulation 2004, 109, 2566–2571. [CrossRef]
- Szalai, A.J.; van Ginkel, F.W.; Dalrymple, S.A.; Murray, R.; McGhee, J.R.; Volanakis, J.E. Testosterone and IL-6 requirements for human C-reactive protein gene expression in transgenic mice. J. Immunol. 1998, 160, 5294–5299. [CrossRef]
- Weinhold, B.; Bader, A.; Poli, V.; Ruther, U. Interleukin-6 is necessary, but not sufficient, for induction of the humanC-reactive protein gene in vivo. Biochem. J. 1997, 325 (Pt 3), 617–621. [CrossRef]
- Zhang, D.; Sun, M.; Samols, D.; Kushner, I. STAT3 participates in transcriptional activation of the C-reactive protein gene by interleukin-6. J. Biol. Chem. 1996, 271, 9503–9509. [CrossRef]
- Fageeh, H.I.; Fageeh, H.N.; Patil, S. Monocyte Differentiation into Destructive Macrophages on In Vitro Administration of Gingival Crevicular Fluid from Periodontitis Patients. J. Pers Med. 2021, 11, 555. [CrossRef]
- Huang, X.; Yu, T.; Ma, C.; Wang, Y.; Xie, B.; Xuan, D.; Zhang, J. Macrophages Play a Key Role in the Obesity-Induced Periodontal Innate Immune Dysfunction via Nucleotide-Binding Oligomerization Domain-Like Receptor Protein 3 Pathway. J. Periodontol. 2016, 87, 1195–1205. [CrossRef]
- Kibayashi, E.; Urakaze, M.; Kobashi, C.; Kishida, M.; Takata, M.; Sato, A.; Yamazaki, K.; Kobayashi, M. Inhibitory effect of pitavastatin (NK-104) on the C-reactive-protein-induced interleukin-8 production in human aortic endothelial cells. Clin. Sci. 2005, 108, 515–521. [CrossRef]
- Singh, U.; Devaraj, S.; Dasu, M.R.; Ciobanu, D.; Reusch, J.; Jialal, I. C-reactive protein decreases interleukin-10 secretion in activated human monocyte-derived macrophages via inhibition of cyclic AMP production. Arter. Thromb Vasc. Biol. 2006, 26, 2469–2475. [CrossRef]
Figure 1.
Blood and gingival fluid CRP levels according to obesity status. Box plots of rank-transformed CRP levels according to obesity status. The bottom and top sides of each box represent the lower and upper quartiles, respectively. The line inside the box represents the median. The bottom and top whiskers represent the minimum and maximum values, respectively. (a) Blood CRP: Wilcoxon rank-sum test (untransformed actual data) showed no statistically significant difference between the two groups (Z = 1.18, p < 0.23). ANCOVA (rank-transformed data) adjusting for age, gender, and race confirmed the univariate analysis (F(4,32) = 2.06, p = 0.16). (b) GCF CRP: Wilcoxon rank-sum test (untransformed actual data) showed that GCF CRP levels were significantly higher in obese than in lean individuals (Z = −2.02, p < 0.04). ANCOVA (rank-transformed data) adjusting for age, gender, and race confirmed the univariate analysis (F(4,37) = 4.77, p = 0.03.
Figure 1.
Blood and gingival fluid CRP levels according to obesity status. Box plots of rank-transformed CRP levels according to obesity status. The bottom and top sides of each box represent the lower and upper quartiles, respectively. The line inside the box represents the median. The bottom and top whiskers represent the minimum and maximum values, respectively. (a) Blood CRP: Wilcoxon rank-sum test (untransformed actual data) showed no statistically significant difference between the two groups (Z = 1.18, p < 0.23). ANCOVA (rank-transformed data) adjusting for age, gender, and race confirmed the univariate analysis (F(4,32) = 2.06, p = 0.16). (b) GCF CRP: Wilcoxon rank-sum test (untransformed actual data) showed that GCF CRP levels were significantly higher in obese than in lean individuals (Z = −2.02, p < 0.04). ANCOVA (rank-transformed data) adjusting for age, gender, and race confirmed the univariate analysis (F(4,37) = 4.77, p = 0.03.
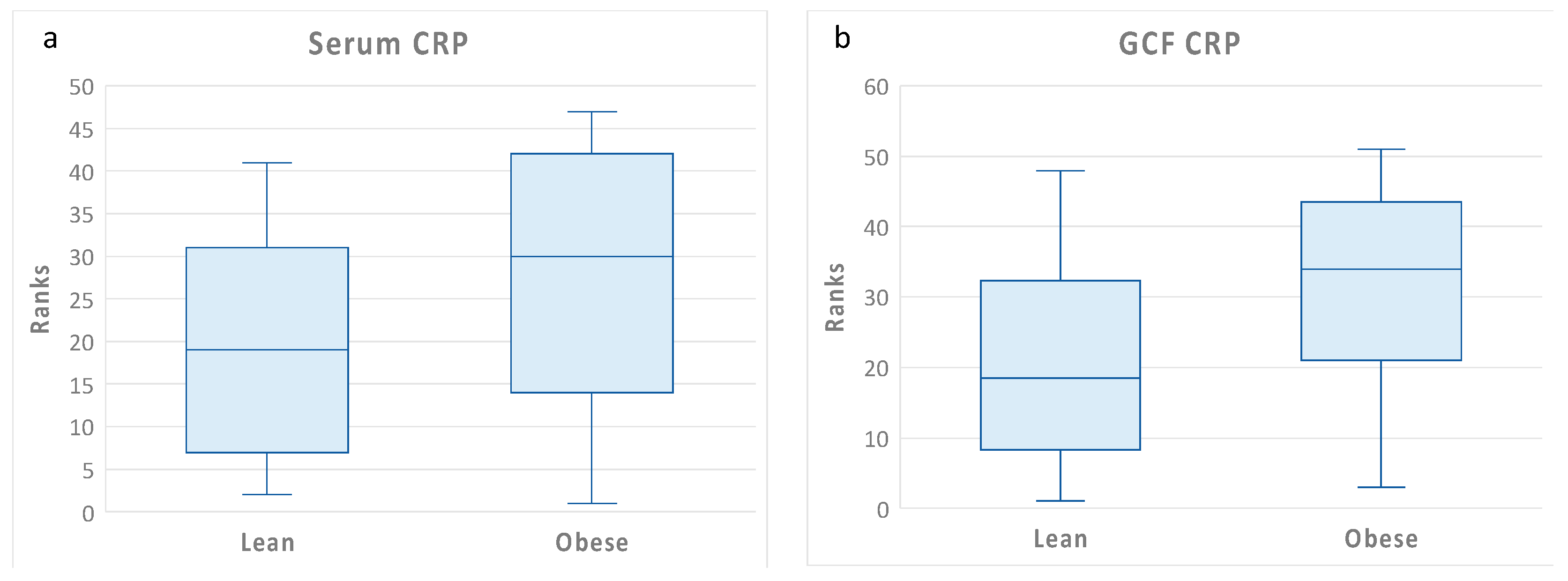
Figure 2.
Scatter plots and regression lines of serum CRP (independent variable) versus GCF CRP (dependent variable) according to group, with unadjusted rank transformed data. Slope equations are indicated. Pairwise slope difference test: Difference (obese – lean) = 0.37, p = 0.27. Pearson correlation coefficients for obese individuals: r = 0.63, p = 0.008, and for lean individuals: r = 0.40, p = 0.12.
Figure 2.
Scatter plots and regression lines of serum CRP (independent variable) versus GCF CRP (dependent variable) according to group, with unadjusted rank transformed data. Slope equations are indicated. Pairwise slope difference test: Difference (obese – lean) = 0.37, p = 0.27. Pearson correlation coefficients for obese individuals: r = 0.63, p = 0.008, and for lean individuals: r = 0.40, p = 0.12.
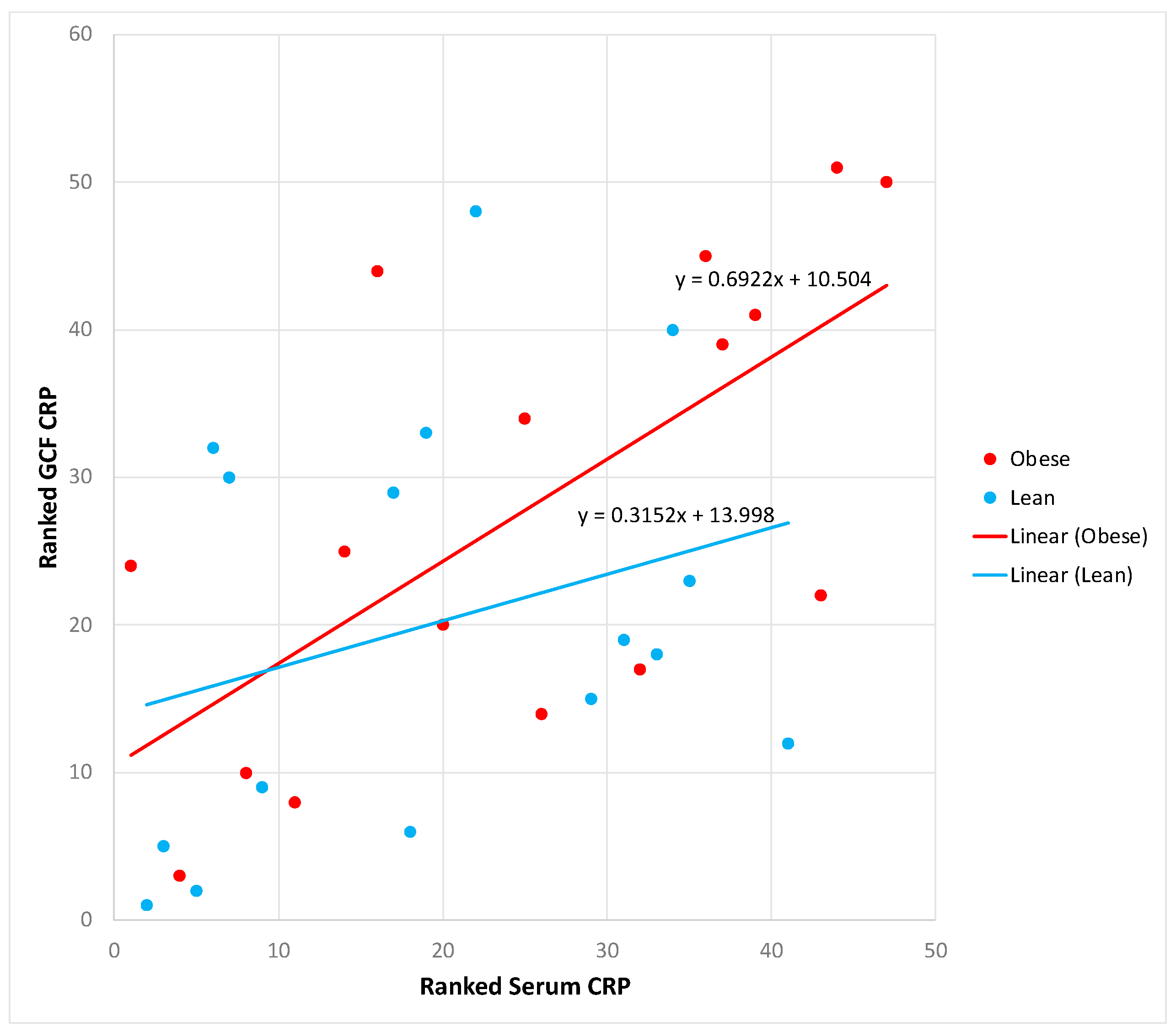
Figure 3.
Flow diagram outlining the hypothesized association sequence of measures of obesity (BMI and waist size) with peripheral CRP levels, peripheral CRP levels with GCF CRP levels, GCF CRP with clinical measures of gingival health, and GCF inflammatory cytokines. Rank regression models adjusted for age, race, and gender were used for prediction of dependent variables. Data are presented as standardized beta weight. When the strength of association was comparable between the two groups, a light arrow with a single value is presented. When the strength of association differed between the two groups, a heavy arrow with two values is presented; values of obese individuals are bolded. p < 0.05 *, p < 0.01 **.
Figure 3.
Flow diagram outlining the hypothesized association sequence of measures of obesity (BMI and waist size) with peripheral CRP levels, peripheral CRP levels with GCF CRP levels, GCF CRP with clinical measures of gingival health, and GCF inflammatory cytokines. Rank regression models adjusted for age, race, and gender were used for prediction of dependent variables. Data are presented as standardized beta weight. When the strength of association was comparable between the two groups, a light arrow with a single value is presented. When the strength of association differed between the two groups, a heavy arrow with two values is presented; values of obese individuals are bolded. p < 0.05 *, p < 0.01 **.
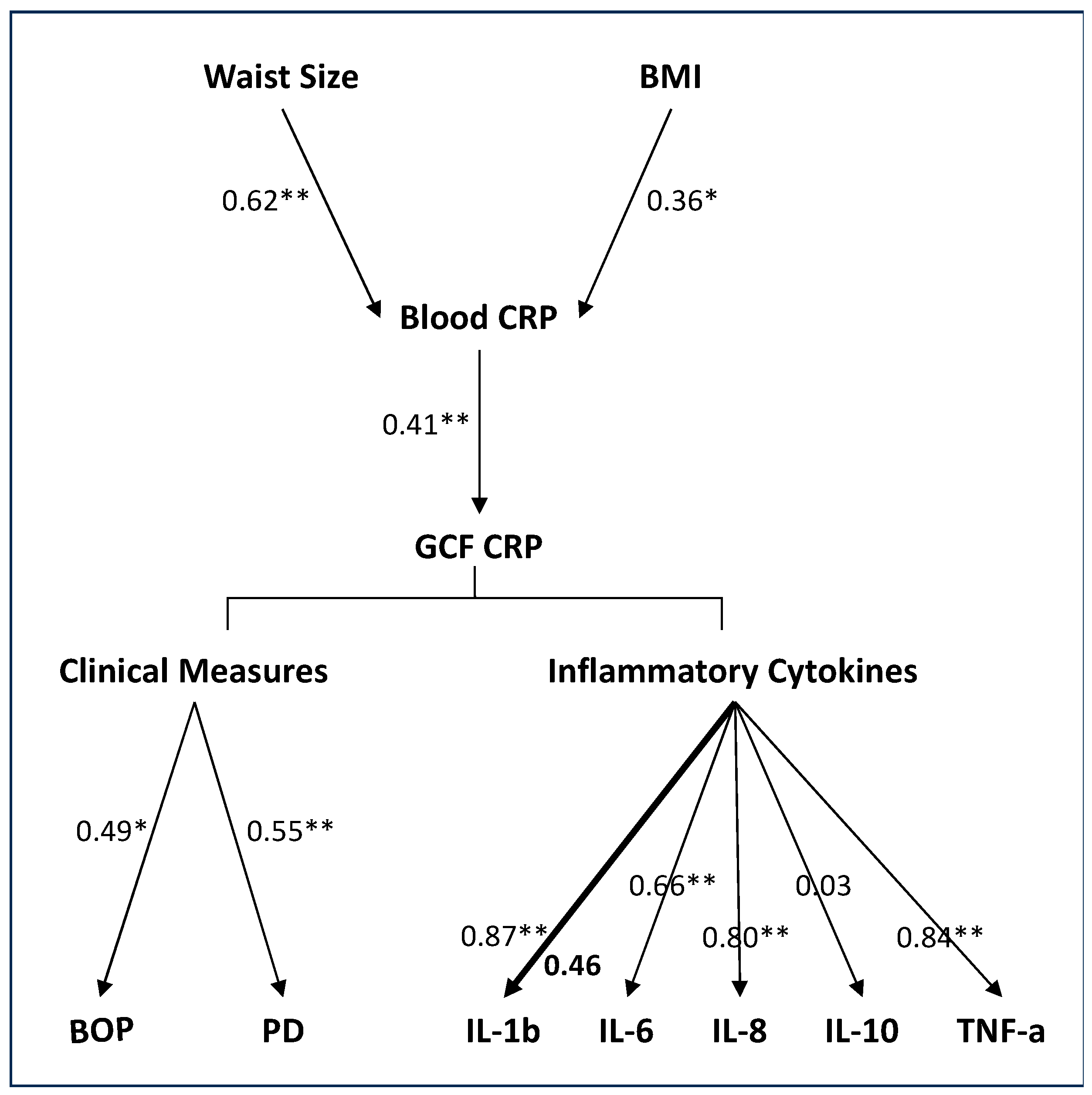
Figure 4.
GCF IL-6 and TNF-α levels according to obesity status. Box plots of rank-transformed cytokine levels according to obesity status. The bottom and top sides of each box represent the lower and upper quartiles, respectively. The line inside the box represents the median. The bottom and top whiskers represent the minimum and maximum values, respectively. IL-6: (a) Wilcoxon rank-sum test (untransformed actual data) showed no statistically significant difference between the two groups (Z = −0.93, p < 0.35). (b) ANCOVA of rank transformed data adjusting for PI and GCF CRP levels indicated that GCF IL-6 levels in lean individuals were significantly higher than in obese individuals (F(3,34) = 10.68, p = 0.002). TNF-α: (c) Wilcoxon rank-sum test (untransformed actual data) showed no statistically significant difference between the two groups (Z = −0.16, p < 0.86). (d) ANCOVA of rank-transformed data adjusting for PI and GCF CRP levels indicated that GCF TNF-α levels in lean individuals were significantly higher than in obese individuals (F(3,34) = 8.45, p = 0.006).
Figure 4.
GCF IL-6 and TNF-α levels according to obesity status. Box plots of rank-transformed cytokine levels according to obesity status. The bottom and top sides of each box represent the lower and upper quartiles, respectively. The line inside the box represents the median. The bottom and top whiskers represent the minimum and maximum values, respectively. IL-6: (a) Wilcoxon rank-sum test (untransformed actual data) showed no statistically significant difference between the two groups (Z = −0.93, p < 0.35). (b) ANCOVA of rank transformed data adjusting for PI and GCF CRP levels indicated that GCF IL-6 levels in lean individuals were significantly higher than in obese individuals (F(3,34) = 10.68, p = 0.002). TNF-α: (c) Wilcoxon rank-sum test (untransformed actual data) showed no statistically significant difference between the two groups (Z = −0.16, p < 0.86). (d) ANCOVA of rank-transformed data adjusting for PI and GCF CRP levels indicated that GCF TNF-α levels in lean individuals were significantly higher than in obese individuals (F(3,34) = 8.45, p = 0.006).
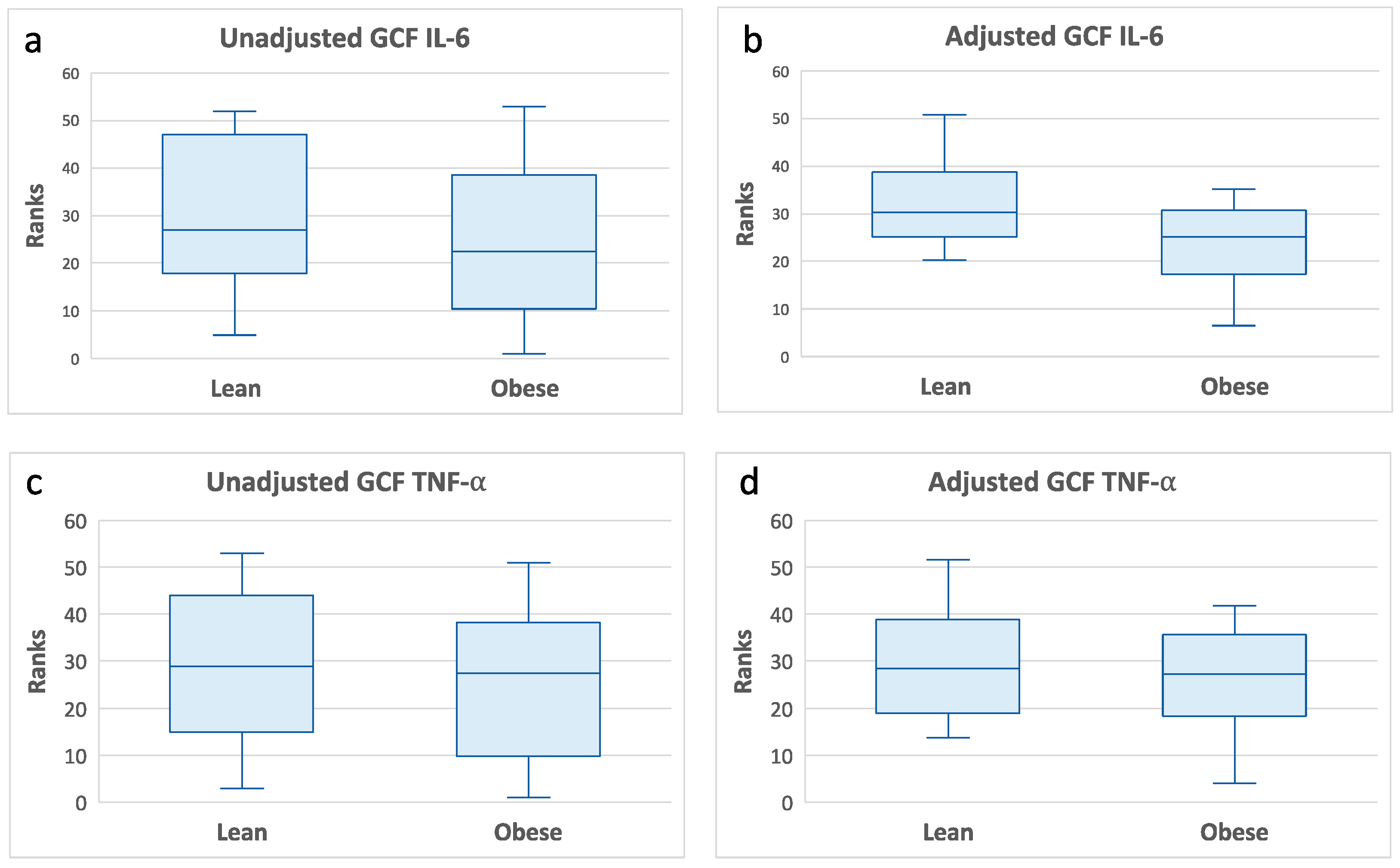

Table 1.
Demographics and clinical measures according to obesity status.
| Variable | Lean (BMI < 25) | Obese (BMI ≥ 25) | p-Value |
|---|---|---|---|
| a. Demographics | |||
| Age (years) | 69.1 (2.18) | 71.42 (1.71) | 0.55 |
| % Male | 45 | 47 | 0.77 |
| % Black | 30 | 37 | 0.65 |
| b. Clinical Measures | |||
| Weight (lbs.) | 153.2 (5.49) | 183.3 (8.18) | 0.009 |
| Waist (cm) | 87.91 (83.54) | 102.5 (96.94) | 0.0003 |
| BMI | 22.26 (0.35) | 29.65 (0.73) | 0.0001 |
| Missing teeth | 1.95 (0.58) | 2.52 (0.60) | 0.51 |
| PI | 0.44 (0.06) | 0.63 (0.08) | 0.06 |
| GI | 0.58 (0.06) | 0.58 (0.06) | 0.83 |
| GCF volume | 2.06 (0.23) | 1.93 (0.26) | 0.59 |
| BOP% | 4.28 (1.14) | 5.84 (1.30) | 0.32 |
| PD mm | 1.85 (0.06) | 1.98 (0.04) | 0.16 |
| AL mm | 1.32 (0.21) | 1.34 (0.19) | 0.63 |
Data are presented as mean (SE) or percentage. p value gives the probability that the groups differ in either Wilcoxon test using ranks or chi-square test for proportions. AL, attachment level; BMI, body mass index; BOP, bleeding on probing; GI, gingival index; PD, probing depth.
Table 2.
CRP and cytokine measures according to obesity status.
| Variable | Lean (BMI < 25) | Obese (BMI ≥ 25) | p-Value |
|---|---|---|---|
| (a) Gingival Fluid | |||
| GCF CRP (ng/mL) | 0.03 (0–0.08) | 0.07 (0.03–0.54) | 0.04 |
| IL-1β (pg/mL) | 1.41 (0.27–9.99) | 2.58 (1.54–5.7) | 0.17 |
| IL-6 (pg/mL) | 0 (0–1.91) | 0 (0–0.57) | 0.34 |
| IL-8 (pg/mL) | 57.59 (22.24–307.80) | 103.68 (58.78–282.08) | 0.16 |
| IL-10 (pg/mL) | 5 (0–5) | 0 (0–5) | 0.21 |
| TNF-α (pg/mL) | 0 (0–1.49) | 0 (0–0.68) | 0.85 |
| (b) Blood (Serum) | |||
| CRP (µg/mL) | 7.6 (2.4–18.2) | 9.8 (4.42–29.5) | 0.22 |
| IL-1β (pg/mL) | 1.84 (1.26–2.14) | 1.2 (0.78–3.64) | 0.52 |
| IL-6 (pg/mL) | 5 (2.86–8.67) | 5.06 (2.92–11.9) | 1 |
| IL-8 (pg/mL) | 10.56 (5.9–21.62) | 10.6 (6.52–13.54) | 0.93 |
| IL-10 (pg/mL) | 16.2 (5.12–23.36) | 11.98 (5.38–37.14) | 0.89 |
| IL-17A (pg/mL) | 12.47 (9.07–25.84) | 11.96 (8.8–27.52) | 1 |
| TNF-α (pg/mL) | 9.7 (7.98–11.29) | 10.38 (8.2–14.02) | 0.27 |
Data reported as median (25th percentile to 75th percentile). p value gives the probability that the groups differ in Wilcoxon test using ranks. GCF IL-17A was not detected in most subjects (data not presented).
Table 3.
Pearson correlation analyses examining the associations of GCF CRP and PI with clinical measures of gingival health and GCF inflammatory cytokines according to obesity status.
Table 3.
Pearson correlation analyses examining the associations of GCF CRP and PI with clinical measures of gingival health and GCF inflammatory cytokines according to obesity status.
| Lean | Obese | |||
|---|---|---|---|---|
| Variable | r | p-Value | r | p-Value |
| (a) GCF CRP Correlations | ||||
| BOP% | 0.45 | 0.06 | 0.56 | 0.01 |
| PD (average) | 0.57 | 0.01 | 0.32 | 0.2 |
| IL-1β (pg/mL) | 0.64 | 0.003 | 0.36 | 0.1 |
| IL-6 (pg/mL) | 0.80 | 0.0001 | 0.52 | 0.02 |
| IL-8 (pg/mL) | 0.48 | 0.03 | 0.82 | 0.0001 |
| IL-10 (pg/mL) | 0.09 | 0.7 | 0.09 | 0.7 |
| TNF-α (pg/mL) | 0.83 | 0.0001 | 0.73 | 0.0004 |
| (b) PI Correlations | ||||
| BOP% | 0.59 | 0.005 | 0.48 | 0.03 |
| PD-ave | 0.17 | 0.45 | 0.20 | 0.40 |
| IL-1β (pg/mL) | 0.28 | 0.23 | 0.06 | 0.79 |
| IL-6 (pg/mL) | 0.15 | 0.51 | −0.01 | 0.94 |
| IL-8 (pg/mL) | 0.15 | 0.50 | −0.16 | 0.49 |
| IL-10 (pg/mL) | 0.12 | 0.60 | 0.01 | 0.95 |
| TNFα (pg/mL) | 0.18 | 0.43 | −0.12 | 0.61 |
Data presented as Pearson correlation coefficients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



