
Submitted:
03 November 2023
Posted:
03 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background
The coronavirus pandemic has led to the creation of clinical guidelines by a large number of professional medical communities. However, the quality and methodology of development of Russian clinical guidelines has been little studied. The continued relevance of studying the use of DOACs in patients with COVID-19 was the basis for conducting this study.
Aim
The objective of this study was to assess DOACs consumption and expenditures in Russian Federation during COVID-19 pandemic and to analyse domestic evidence base for the use of DOACs in COVID-19 patients through identifying all publicly available Russian-produced CPGs for the treatment of COVID-19 and assessing their quality as the source of recommendations for the use of oral anticoagulants for the prevention of thrombotic complications in COVID-19 patients.
Methods
We searched Russian databases for CPGs, published between 2020 and 2023. We identified 7 relevant documents that met our inclusion criteria.
Three authors analyzed Russian clinical guidelines using a AGREE II questionnaire.
We calculated DOACs DDD consumption according to Russian clinical guidelines and DDD consumption in patients with COVID-19 for the period 2020-2022.
Results
7 clinical CPGs were analyzed with the AGREE II tool, it was revealed that experts gave the highest scores for the sections scope and purpose (from 62.98% to 100%), clarity of presentation (from 96.30% to 100%). The lowest scores were given for the sections stakenholder involment (33.33% to 64.81%), rigour of development (from 0% to 49.31%), applicability (from 23.61% to 50%), editory independence ( from 0% to 50%). When comparing the total score, it was found that two clinical guidelines received the highest scores - ROPNIZ (Livzan), ROPNIZ (Drapkina). The minimum score is registered with the NIIOZMM (Khripun) clinical guideline. No guideline received a total score of more than 70%.
According to clinical recommendations, the consumption of apixaban and rivaroxaban is 15 DDD (30-day course of therapy), 22.5 DDD (45-day course of therapy).
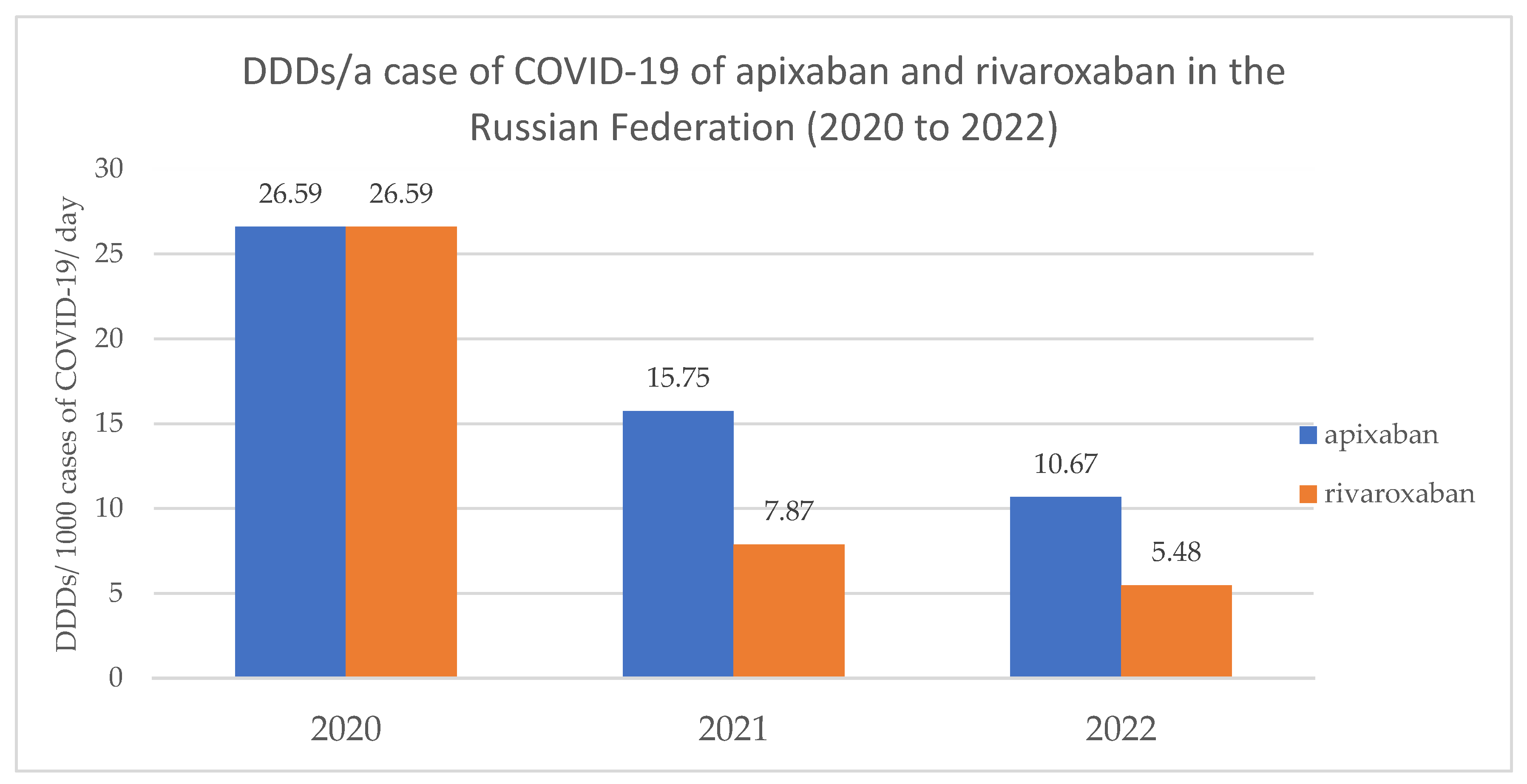
Consumption of apixaban in the Russian Federation in 2020 and 2021 corresponds to the indicators presented in clinical recommendations (in 2020 – 26.59 DDD per patient with COVID-19; in 2021 – 15.75 DDD per patient with COVID-19), and in 2022 – 10.67 DDD, which is below the recommended values. In 2020, consumption of rivaroxaban in the Russian Federation was 26.59 which corresponds to data from clinical recommendations; in 2021, consumption decreased to 7.87 DDD; in 2022 – 5.48 DDD, which is 2.74 times less than recommended.
Keywords:
COVID-19
; DOACs
; pharmacoepidemiology
; pharmacoeconomics
; clinical practice guidelines
; clinical trials
; AGREE II
; CONSORT
1. Introduction
The global COVID-19 epidemic, officially recognized by WHO on March 11, 2020, has become a serious test for global health. The most common manifestation of COVID-19 is damage to the respiratory system. However, this disease is characterized by high inflammatory activity and thrombotic complications leading to multiple organ damage. Management of a patient with COVID-19 involves not only the treatment of pneumonia and respiratory failure, but also the timely recognition and treatment of damage to other body systems. The risk of thrombosis in hospitalized patients with COVID-19 is an emerging issue that requires investigation. The incidence of thrombosis in hospitalized patients with severe COVID-19 may be over 35% with mortality rate of 45% [1,2].
To prevent thrombotic complications in patients with COVID-19, low molecular weight heparin (LMWH) preparations, and in some cases, unfractionated heparin (UFH) preparations, were used empirically. Direct oral anticoagulants (DOACs) are currently recognized as the standard of care for treatment of venous thrombosis and atrial fibrillation, however, the balance of benefits and risks of their use in hospitalized patients with COVID-19 is not clearly understood and hence the use of DOACs is not recommended. However, in patients with confirmed COVID-19 at outpatient basis, DOAC therapy may be recommended [3]. Direct oral anticoagulants are used to improve prognosis in patients with COVID-19, likely to reduce venous thrombosis and pulmonary embolism regardless of their dose compared with untreated patients and placebo patients. There is also no significant difference in the development of such outcomes as hospitalization, adverse events, death and major bleeding in patients receiving different doses of the same direct anticoagulant. The results of other systematic review of seven studies involving 16.185 people from Brazil, Iran, Italy, the USA and a number of other countries hospitalized with severe COVID-19, requiring intensive care and emergency care conducted, clearly demonstrated the benefits of using rivaroxaban. The authors found that there was little or no difference between using higher-dose or lower-dose anticoagulants- rivaroxaban for 15 to 90 days in patients aged 55 to 68 years in all-cause mortality and increase minor bleeding. However, the data of direct anticoagulants reduced all-cause mortality in treated patients compared with untreated patients come from non-randomized studies and is very uncertain, that requires the continuation of new randomized trials and confirmation of these results. When used in the outpatient setting, anticoagulants (blood thinners) probably reduce venous thromboembolism (VTE) and pulmonary embolism (PE) when compared with placebo or no treatment in people with COVID-19. However, these drugs seem to have little or no effect in reducing death, major bleeding, need for hospitalisation, or adverse events [4,5].
One of the limiting factors for prescribing DOACs is the high risk of drug-drug interactions, including those at the level of CYP450 and P-glycoprotein. Bleeding is a serious complication of DOAC therapy, with major bleeding occurring in approximately 2-4% of patients receiving oral anticoagulants (OACs) during the year, and the mortality rate can be 8 -15% [6]. It was shown that the incidence of major bleeding increased with the severity of COVID-19: 0.5%, 2.3% and 12.3% in patients with mild, moderate and severe forms of COVID-19, respectively. Anticoagulants are independently associated with the risk of bleeding. The gastrointestinal tract is the most vulnerable to bleeding, with a bleeding rate of 44% [7]. It was shown that 17.35% of patients with upper gastrointestinal bleeding used anticoagulant therapy. During the pandemic, this number nearly doubled (up to 24.39% than before the pandemic) with mortality rate of 12.21% [8]. Taking into account the fact that DOACs are recommended at the outpatient stage of treatment of COVID-19 by various clinical practice guidelines (CPGs), including clinical recommendations of the Ministry of Health of the Russian Federation, the drugs of choice are the following: rivaroxaban (10 mg once daily), apixaban (2.5 mg twice daily) 30 – 45 days [9]. Currently, rivaroxaban is the most commonly used DOAC for coronavirus infection, followed by dabigatran and apixaban. The authors of a systematic review with meta-analysis showed that the use of DOACs for the prevention of thromboembolic complications in hospitalized patients led to fewer deaths due to bleeding: 5 for dabigatran, 7 for apixaban, 7 for rivaroxaban, 9 for LMWH and 15 for warfarin per 10 000 patients [10]. In addition, according to one study [11], it the use of DOACs helped reducing the risk of hospitalization to the ICU by 50%, as well as reducing COVID-associated mortality by 31%, which was noted in the population of patients taking DOACs on an outpatient basis before COVID infection -19. Undoubtedly, during the COVID-19 pandemic and owing to clinical recommendations, DOAC drugs have become one of the most sought-after groups of the pharmaceutical segment. For example, in the Russian Federation in 2021 the sales of DOACs increased by 6.6%, and the market share for apixaban and rivaroxaban increased by 0.5% compared to 2020 [12]. The probability of prescribing rivaroxaban or apixaban was on average 33% per patient, and treatment with the above drugs costed 911.08 and 840.80 rubles. for a course of treatment [13].
Since CPGs are universally recognized to be an algorithm for clinical decision-making and advancing rational use of medicines aimed at achieving higher probability of favorable outcomes, we conducted a comparative analysis of the domestic evidence base for the use of DOACs in COVID-19 patients in order to identify potential strengths and weaknesses. We used the AGREE II and CONSORT instruments. Competent development of CRs, which take into account the latest research evidence and their adequate implementation by medical specialists (health care providers), ensures improved quality of care, optimization of treatment costs, as well as reduced risk of adverse events and potential medication errors [14].
There are multiple organisations in Russia that publish clinical practice guidelines (CPGs). The demand for CPGs and appreciation of their role in healthcare provision has been steadily growing. However, quality and methodology of development of CPGs have not been systematically addressed.
Aim
The objective of this study was to assess DOACs consumption and expenditures in Russian Federation during COVID-19 pandemic and to analyse domestic evidence base for the use of DOACs in COVID-19 patients through identifying all publicly available Russian-produced CPGs for the treatment of COVID-19 and assessing their quality as the source of recommendations for the use of oral anticoagulants for the prevention of thrombotic complications in COVID-19 patients.
Materials and methods
Design
It is a descriptive study. We used qualitative and quantitative methods. The study consisted of two parts: 1) analysis of DOAC consumption and expenditures at the All-Russia (National) level and 2) analysis of Russian CPGs, recommending DOAC use in COVID-19 patients.
DOAC consumption and expenditure (Pharmacoepidemiology of DOAC in Russia in COVID-19 pandemic)
We studied official data from open sources on medicine use and expenditure. We used data for the ATC class B01A, antithrombotic medicines. We used DDD values and guidelines of their use [15] to calculate National DOAC consumption. Aggregated data for calculation of pharmacoepidemiological parameters and indicators of NOAC consumption in the Russian Federation 2020-2023 were obtained from the following information sources: annual reports by DSM Group and Pharmaceutical sales in Russia by AlphaRM [16,17].
Consumption of apixaban (Eliquis) in the Russian Federation, National consumption: Example
(See appendix 1).
We used sales data from these annual reports and calculated parameters of our interest. For example, the market share of rivaroxaban in 2021 was 0.1% in the pharmacy market in physical terms. Knowing the overall sales volume for Russia for 2021 (National), we calculated the sales volume of rivaroxaban (million packages) in 2021 using the published percentage of its market share:
5 512 000 000 packages * 0.001=5 512 000 packages of rivaroxaban sold in 2021.
We calculated the total drug consumption per year in mg, as well as the amount of DDD consumed. Total (National) drug consumption in mg = Dose per release form (package form in mg) * number of release forms per year.
The resulting value was used to calculate the number of DDD consumed by patients: Number of DDD consumed = Total drug consumption in mg / DDD in mg.
CPG recommended consumption:
The recommended consumption of DOACs per one patient per one course of prophylactic treatment in patients with COVID was carried out in accordance with the data found in the Russian CPGs as follows:
1.Recommended doses of rivaroxaban, apixaban and dabigatran etexilate and the duration of the course of treatment were extracted from the text of each CPG;
2. These doses were multiplied by the duration of treatment;
3. Resultant dose was divided by DDD value.
Apixaban: 2.5 mg 2 times a day of 30 days = 150 mg; 150 mg: 10 (DDD) = 15 DDD – for one course of prophylactic treatment. Apixaban administration during 45 days leads to consumption of 22.5 DDD preparation: 2.5 mg 2 times a day of 450 days =225 mg; 225 mg: 10 (DDD) = 22.5 DDD – for one course prophylactic treatment
Based on the results of these two series of calculations, the number of patients who completed at least 1 course of DOACs was determined by dividing the resulting national consumption in DDDs by the DDD equivalent of the CPG-recommended course of treatment / prophylaxis.
Consumption of apixaban (Eliquis) in the Russian Federation for 2022 (January-August). Example
(See appendix 1).
2. 1 package of apixaban 2.5 mg contains 60 tablets; Accordingly, 1 package contains 150 mg of apixaban.
3. Total amount of apixaban consumption in 2022 (in mg) = total number of packages consumed in 2022 in the Russian Federation × amount of apixaban in 1 package = 7 600 000 packages of apixaban × 150 mg = 1 140 000 000 mg
4. The number of DDDs of apixaban consumed in the Russian Federation in 2022 = 1 140 000 000 mg/ DDD (apixaban, mg) = 1 140 000 000/ 10 = 114 000 000 DDD of apixaban consumed in the Russian Federation in 2022.
Knowing the incidence of coronavirus infection in the period from 2020 to 2022, you can calculate the consumption of DOACs per person. Data on the incidence of COVID-19 in the Russian Federation from 2020 to 2022 [18,19,20] are presented in the Table 1.
5. We analyzed DDDs/а case of COVID-19 of apixaban and rivaroxaban in the Russian Federation (2020 to 2022). (See appendix 2)
6. We analyzed estimated number of people taking a CPG recommended course of apixaban and rivaroxaban in the Russian Federation in 2020-2022 based on the assumption that only COVID-19 patients were responsible for gross national consumption. (See appendix 2)
Eligibility criteria for inclusion of CPGs and Clinical trials
We included Russian clinical practice guidelines (CPGs, the guidelines) for the treatment of new coronavirus infection COVID-19 and Non-Infectious Diseases during the pandemic period which recommended use of new DOACs and Russian randomized clinical trials of Covid-19 patients with the use of DOACs. The guidelines and clinical trial reports had to be published between 2020 and 2023. The CPGs had to be written in Russian language and to be intended for health care professionals and be freely available online.
Search methods for identification of CPGs and clinical trials
We searched for all guidelines, that would meet our eligibility criteria regardless of their official standing (endorsement by either the Ministry of Health, or professional associations, or alternative health bodies or organisations. The guidelines could be endorsed, approved or accepted for practical implementation, published as draft consultations or documents in development). We searched for all randomised clinical trials of Covid-19 patients with the use of new oral anticoagulants.
We searched the following databases (See appendix 3):
- Official collection of clinical guidelines of the Ministry of Health (https://cr.minzdrav.gov.ru/; last searched 01 September 2023;
- Russian Databases: eLIBRARY.RU (www.elibrary.ru; from 2020 to 2023; last searched 01 September 2023;
- National Library of Medicine (National Centre for Biotechnology Information, NCBI, https://pubmed.ncbi.nlm.nih.gov; from 2020 to 2023; last searched 01 September 2023;
- Google scholar (https://scholar.google.ru; from 2020 to 2023; last searched 01 September 2023;
- US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; from 2020 to 2023; last searched 01 September 2023; Appendix 5);
- the Cochrane Library (https://www.cochranelibrary.com; from 2020 to 2023; last searched 01 September 2023;
Description of the databases and websites used for searched, selection and analysis of clinical practice guidelines and clinical trials
- 1.
- The official collection of clinical practice guidelines of the Ministry of Health (MoH), named Rubricator
The Rubricator contains a searchable collection of guidelines, grouped according to the International Classification of Diseases 10 (ICD-10). With its first launch in October—November 2017 it established the system of National Clinical Guidelines. Rubricator operates in Russian language only, it allows simple search by a term, by a number of a CPG, by a year of publication, by the ICD position, and by official status (endorsed for implementation or approved, draft in development or outdated) with filters for adults and children.
- 2.
- eLIBRARY.RU
It is the open-access searchable Russian electronic database of scientific publications integrated with the Russian Scientific Citation Index (RSCI). It is the largest available database. The RSCI presents a tool for measuring publication activity both of individual researchers and of organizations, it is commissioned by the Ministry of Education and Science of the Russian Federation, it is freely publicly available. The eLIBRARY.RU and RSCI were developed and are being supported by the Scientific Electronic Library Company. The detailed description of the eLIBRARY.RU platform is available elsewhere [21].
eLIBRARY.RU operates in Russian only, it contains publications in other languages, including English.
- 3.
- National Library of Medicine (National Centre for Biotechnology Information, NCBI, https://pubmed.ncbi.nlm.nih.gov);
- 4.
- Google scholar (https://scholar.google.ru);
- 5.
- US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov);
- 6.
- The Cochrane Library (https://www.cochranelibrary.com
We searched by the search terms of our research interest, (COVID-19) and direct oral anticoagulants (DOAC) in above listed databases.
The official collection of clinical practice guidelines of the Ministry of Health (MoH), named Rubricator
The search strategies are presented in (appendix 3)
Three review authors (EAB, EAK and MSC) independently examined titles and abstracts of records from the electronic searches and excluded those studies that were obviously irrelevant. Additionally we used Microsoft word auto-search and sorting program, EndNote's duplicate program, which allowed for duplicate removal. We analysed the fulltexts of the remaining papers, and the same three review authors independently selected studies for inclusion based on the inclusion criteria. Disagreements were resolved by discussion within the author team. We excluded articles that did not meet the inclusion criteria, providing reasons for their exclusion in the appendix 3.
We used a PRISMA flow checklist to create the PRISMA diagrams for our literature searches (Checklist). We conducted the searches in September 2023 (See appendix 4,5).
Results of the searches
The initial searches yielded 2 082 records from PubMed.gov, Google scholar, Clinicaltrials.gov, Cochrane library and 2 384 – from the Russian database eLibrary.ru and 1 record from the Minzdrav.gov collection of CPGs. Totally we retrieved 4 468 records.
After title / abstract screening 330 (77 - foreign and 253- Russian) records were excluded as irrelevant unrelated to the use of new anticoagulants in COVID 19.
After the title/abstract analysis of 2240 remaining records-1725 removed as non-Russian and 497 records did not report our outcome of interest and were excluded as illegible by inclusion criteria. The 5 foreign and 13 Russian remaining records were then screened for eligibility to be included in this review. Eighteen articles were included for data of our interest. After quantitative evaluation of these articles in foreign and Russian databases, 4 common duplicates have excluded.
We searched 14 Full-text articles included in review by abstracts. 6 records were removed after the qualitative assessment of these articles in foreign and Russian databases. Reasons of removing: 2 articles from Russian database had the same information, so 1 of them was removed; 5 was as illegible by inclusion criteria: Tarlovskaya-2021, Kalinin-2023, Vorobyev-2020, Ruzhentsova-2021, Krivoshchekov-2022.
8 full-text articles were evaluated as meeting the inclusion criteria and were taken for further qualitative analysis. Articles included: one international clinical randomized trials conducted in Russia (Eikelboom J.W., Drapkina O.M.) and seven Russian clinical guidelines for the management of COVID-19 patients with the use of direct oral anticoagulants (DOAC). The data is presented in appendix 5.
We report here on seven Russian clinical guidelines for the management of COVID-19 patients with the use of direct oral anticoagulants and one Russian clinical randomized trial founded from 01. 01.2020 to 01.09.2023, which met inclusion criteria, and how we identified these trials. In eLibrary we ran a series of searches by condition of interest (COVID-19) and direct oral anticoagulants (DOAC), which yielded finally 6 potential records of CPG. In the Rubricator of the Ministry of Health of the Russian Federation we found one CPG which met our inclusion criteria. (Table 2).
Searches in PubMed.gov, Google scholar, Clinicaltrials.gov, Cochrane library databases after removal of duplicates, irrelevant records and ineligable studies through title / abstract screening and full text screening we identified only one Russian clinical randomized trial, which was eligible to be included: Eikelboom 2022 . It appeared to be an open-label, factorial, randomised, multi-center [22] an open-label, factorial, randomised, controlled trial, with one centre in Russia led by Russian researcher Drapkina. We coded the study for the use in this project Drapkina-Eikelboom 2022.
The identified CPGs are presented in Table 2 with the coding for them, which we use throughout the text.
CPG assessment with AGREE II instrument
The three experts of the author team independently performed the assessment with the AGREE II instrument.
The AGREE II is a questionnaire designed to assess the quality of health care guidelines and to be used as a tool to develop clinical practice guidelines.
AGREE II includes 23 questions in 6 different domains that address different aspects of guidelines. Those domains are Scope and Purpose (3 questions), Stakeholder Involvement (3 questions), Rigour of Development (8 questions), Clarity of Presentation (3 questions), Applicability (4 questions), and Editorial Independence (4 questions. For each question, the expert is asked to provide a numerical score between 1 and 7, 1 being the minimum score and 7 being the maximum score. Each question is presented as a statement and the experts should answer the questions based on how much they agree with the statement (1 –strongly disagree, 7 –strongly agree). Each CPG receives a raw score between 23 and 161 points from a single expert. It is recommended that at least two experts analyse the same guidelines using the AGREE II tool. Additionally, experts may leave comments for each question and state whether they would recommend the use of the guideline at the end of the questionnaire.
Next, derived data was calculated by compiling the scores of all experts for each domain and scaling them as a percentage of a maximum possible score for that specific domain. That is done by using the formula (Eq 1):
Table 3 below provides a sample set of data for Scope and Purpose domain for COVID-19 CPG by the Ministry of Health of the Russian Federation, in which we show sample calculations to illustrate how the AGREE II scoring was used in our study.
The total obtained score is calculated by summing the individual scores of all experts (Eq 2):
16+21+21=58
The minimum possible score is calculated by attributing 1 to each question, as the minimum possible score is 1 for each question and multiplying it by the number of experts (Eq 3):
(1+1+1)×3=9
The maximum possible score is calculated by attributing 7 to each question, as the maximum possible score is 7 for each question and multiplying it by the number of experts (Eq 4):
(7+7+7)×3=63
The original formula is used to calculate the domain score (Eq 5):
We performed this calculation in Microsoft Excel. We created a separate data sheet for each CPG and another sheet—for the comparison of all guidelines. First, we created a table for each CPG with all 23 questions organized in the 6 domains. Each table included the data from three experts.
We added the scores for each question from the three experts. Next, we calculated minimum and maximum scores for each domain. Then, we calculated the difference between the maximum and the minimum score for each domain. We used the above formula to calculate a domain score for each domain and the total sum of assessment for each CPG.
Finally, we created a comparison table for all seven CPGs and made a bar graph to visualize the difference in total sum of assessment between all the CPGs studied.
Results
DOAC pharmacoepidemiology
See Appendix 1, 6
The defined daily doses (DDDs) of direct oral anticoagulants established by WHO are the following: for apixaban – 10 mg (5 mg 2 times a day); rivaroxaban - 20 mg; dabigatran etexilate - 300 mg.
We calculated hypothetical dosing load for a COVID-19 patient in DDDs as recommended by the CPGs DOAC. As a result of detailed analysis of the available data in the Russian guidelines for the management of patients with COVID-19 which recommended DOAC use, we obtained the following recommended consumed doses of each DOAC to patient for a course of prophylactic treatment:
The CPG of the Ministry of Health recommended preventive use of direct oral anticoagulants in patients with COVID-19 with the following dosage regime: rivaroxaban -10 mg once daily, apixaban - 2.5 mg twice daily, dabigatran etexilate - 110 mg twice daily for prevention of deep vein thrombosis of the lower extremities and pulmonary embolism. The duration of anticoagulants use in COVID-19 out-patients was not described, however, it was recommended for up to 30-45 days depending on the patient's clinical condition and timing of recovery of motor activity. In accordance with this we calculated the recommended consumed doses of drugs in DDDs as shown in the appendix 7.
All studied CPGs were in agreement on recommending rivaroxaban, apixaban and dabigatran etexilate equally without preference for prophylaxis of deep vein thrombosis and pulmonary embolism in COVID-19 patients after discharge from hospitals in cases of concern of potential embolic complications. Out-patients with COVID-19 with persistent risk factors for deep vein thrombosis or pulmonary embolism (DVT/PE): for elderly patients, patients undergoing treatment in the intensive care unit, with active cancer, history of DVT/PE, patients with ongoing severe mobility limitation, with a D-dimer concentration in the blood 2 times the upper limit of normal and a low risk of bleeding are recommended to be treated with prophylactic doses of anticoagulants for 30 days, which can be extended to 45 days. The dabigatran dosage and mode of administration was not described in ROPNIZ -2021 (Drapkina) recommendation. In the recommendations of MGNOT-2020, NIIOZMM 2021, FAR 2020 there is information about the equal doses of rivaroxaban, apixaban and dabigatran etexilate, but there is no description of the mode of their use in patients with Covid-19. RSC- 2020 guideline does not contain information about drugs doses, indications, the dosage regimen of direct oral anticoagulants, which makes it impossible to determine the consumer dose of drugs, however, there are warnings of combination therapy with a protease, P-glycoprotein inhibitors.
The CGS of NIIOZMM-2021, MGNOT-2020, ROPNIZ-2021 and MoH-2022 contain the same information about combined prescribing anticoagulants and protease inhibitors. The use of apixaban should be avoided, or the dose (5 or 10 mg) should be reduced by 50% with simultaneous systemic therapy with P-glycoprotein and CYP450 3A4 inhibitors. Simultaneous use of dabigatran with ritonavir is not recommended in patients with impaired renal function and correction of it’s dose is necessary, monitoring of the patient for the development of bleeding. Simultaneous use of rivaroxaban with inhibitors of P-glycoprotein is contraindicated.
The lack of necessary information in the CGS of FAR-2020, NIIOZMM-2021, MGNOT-2020 does not allow us to calculate the recommended consumption of drugs from the group of DOACs.
In the recommended regimens of DOAC use in COVID-19 patients in the Russian guidelines MoH 2022; ROPNIZ 2021 (Drapkina); ROPNIZ 2021 (Livzan), we obtained equally comparable consumption rates of rivaroxaban, apixaban and dabigatran for the treatment and prevention of deep vein thrombosis and pulmonary thromboembolism in patients at high risk.
Recommended doses and calculated hypothetical DOAC dosing load are presented in Table 4.
Gross national apixaban consumption varied through the years of 2020, 2021, and 2022 with the maximum consumption in 2021, which was nearly 2 times higher than in 2020. In 2022 national apixaban consumption decreased, but did not reach the level of 2020.
Gross national consumption of rivaroxaban demonstrated steady downward trend through 2020, 2021 and 2022. Interestingly, in 2020 rivaroxaban consumption was equal to that of apixaban. In 2022, consumption of rivaroxaban in the Russian Federation decreased by 29.25% compared to 2021 and by 30.35% compared to 2020.

Table 6.
DDDs/а case of COVID-19 of apixaban and rivaroxaban in the Russian Federation (2020 to 2022).
Table 6.
DDDs/а case of COVID-19 of apixaban and rivaroxaban in the Russian Federation (2020 to 2022).
| Name of the drug | DDD (WHO), mg | 2020 | 2021 | 2022 |
|---|---|---|---|---|
| Apixaban | 10 | 26.59 | 15.75 | 10.67 |
| Rivaroxaban | 20 | 26.59 | 7.87 | 5.48 |
When studying the consumption of apixaban and rivaroxaban per patient with COVID-19, it was revealed that the maximum consumption of apixaban was in 2020, the minimum in 2022. When analyzing the results of rivaroxaban consumption, similar results were obtained: the maximum consumption was in 2020, the minimum in 2022.
In 2021, apixaban consumption decreased by 40.77% compared to 2020; in 2022, the downward trend in consumption continued: DDD decreased by another 32.25% compared to 2021.
The highest consumption of rivaroxaban was observed in 2020 - 26.59 DDD per case of COVID-19. In 2021, we found a decrease in consumption by 70.40% compared to 2020. In 2022, this trend continued and the DDD per patient of rivaroxaban decreased by 30.37% compared to 2021.
Table 7.
Estimated number of people taking a CPG recommended course of apixaban and rivaroxaban in the Russian Federation in 2020-2022 based on the assumption that only COVID-19 patients were responsible for gross national consumption.
Table 7.
Estimated number of people taking a CPG recommended course of apixaban and rivaroxaban in the Russian Federation in 2020-2022 based on the assumption that only COVID-19 patients were responsible for gross national consumption.
| Name of the drug | DDD (according to Russian clinical guidelines) | 2020 | 2021 | 2022 |
|---|---|---|---|---|
| Apixaban | 15 DDD (30 days) | 5 600 000 | 11 024 000 | 7 600 000 |
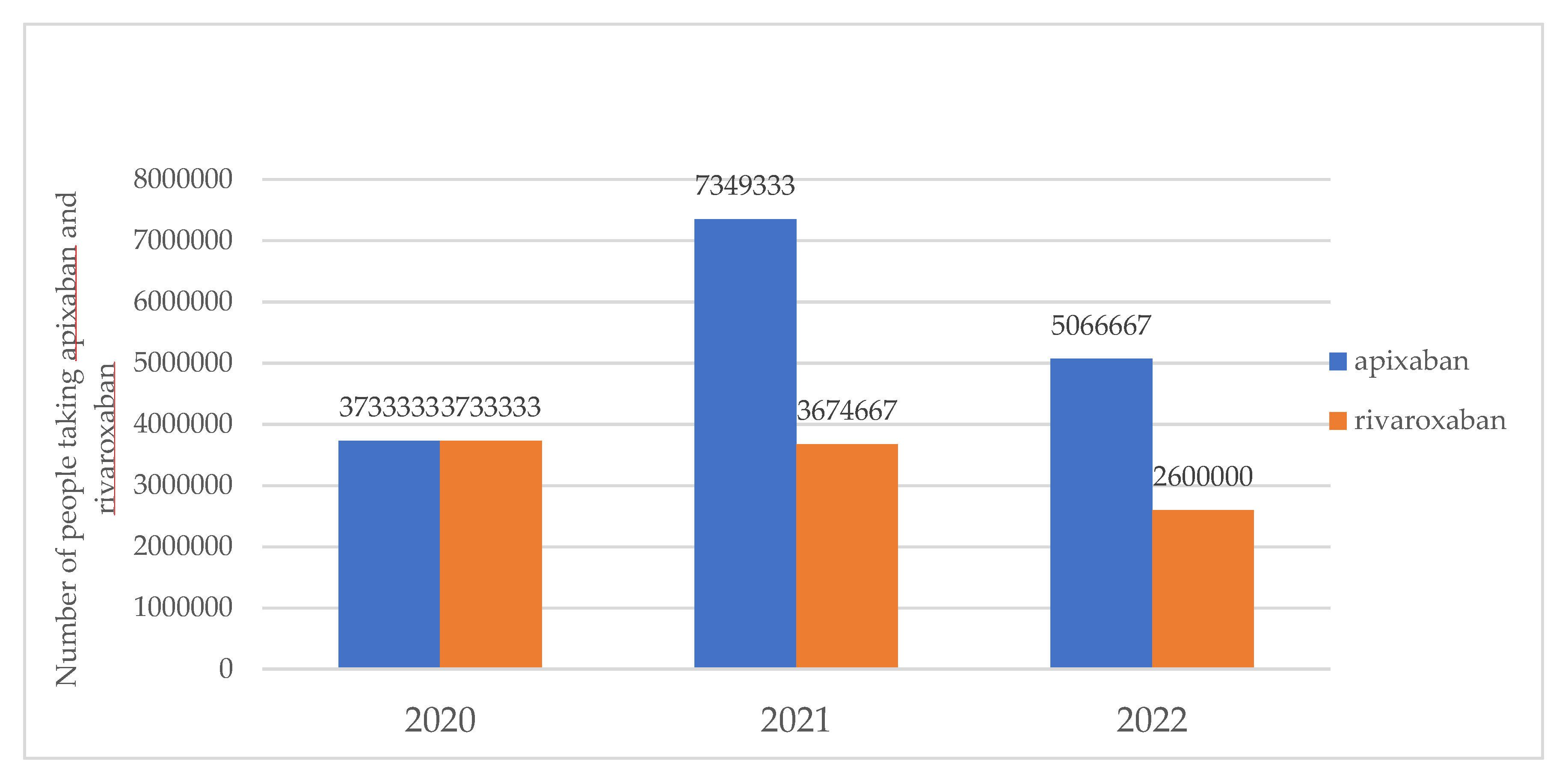
| 22,5DDD (45 days) | 3 733 333 | 7 349 333 | 5 066 667 | |
| Rivaroxaban | 15 DDD (30 days) | 5 600 000 | 5 512 000 | 3 900 000 |
| 22,5 DDD (45 days) | 3 733 333 | 3 674 667 | 2 600 000 |
The hypothetical number of people taking the CPG-recommended course of apixaban in 2020 (if we consider a 30-day course of therapy) exceeds the number of officially registered Covid patients by 1.77 times. If we consider a 45-day course of therapy, the results practically coincide with the estimated number of Covid cases in 2020 of 3 733 333 patients.
In 2021, the hypothetical number of people taking the CPG-recommended course of apixaban was 11 024 000, which was by 4.75% more than the number of COVID-19 patients (if we consider a 30-day course of therapy). If we consider a 45-day course of therapy, the hypothetical number of people taking the CPG-recommended course of apixaban in 2021 was by 30.0% less than the number of officially registered 10 499 982 cases.
In 2022, 71.13% of patients with coronavirus infection received at least one 30-day course of apixaban therapy; If we consider a 45-day course, then 47.42% of patients received at least one course of apixaban.
The hypothetical number of people taking the CPG-recommended course of rivaroxaban in 2020 (if we consider a 30-day course of therapy) exceeds the number of COVID-19 patients by 43.58%; If we consider a 45-day course of therapy, the results obtained practically coincide with the number of COVID-19 cases in 2020 and amount to 3 733 333.
In 2021, the hypothetical number of people taking the CPG-recommended course of rivaroxaban was 5 512 000, which is 47.50% less than the number of COVID-19 patients (if we consider a 30-day course of therapy). If we consider a 45-day course of therapy, then the hypothetical number of people taking the CPG-recommended course of rivaroxaban in 2021 was 65.00% less than the number of cases.
In 2022, there was a decrease in rivaroxaban consumption compared to 2021: 36.5% of COVID-19 patients received rivaroxaban in 2022 (30-day course) or 24.3% if we consider a 45-day course of therapy.
The largest number of COVID-19 patients was registered in 2021-2022. The smallest number of patients was registered in 2020. At the same time, the highest consumption of apixaban was in 2021, the lowest - in 2020, and the largest amount of rivaroxaban was consumed in the Russian Federation in 2020, subsequently its consumption decreased and the lowest consumption was noted in 2022.
The above presented calculations mean that in 2020, each patient with covid received more than 1 course of therapy with apixaban (1.77 course of apixaban therapy (30-day)) and rivaroxaban (1.77 course of rivaroxaban therapy (30-day)), which indicates serious overuse of DOACs at the beginning of the pandemic.
In 2021, almost every patient with COVID-19 received apixaban, and every second patient was prescribed rivaroxaban.
In 2022, DOAC consumption decreased, every third patient took rivaroxaban, and about ¾ of all patients took apixaban (30-day course).
This shows a more rational and targeted use of doacs in patients with covid in the 3rd year of the pandemic, which may be the result of both, the accumulated experience and the emergence of clear algorithms for the management of patients with coronavirus infection (the CPGs).
Table 8.
Number of people taking apixaban and rivaroxaban in the Russian Federation in 2020-2022 (15 DDD, 30 days) and (22,5 DDD, 45 days).
Table 8.
Number of people taking apixaban and rivaroxaban in the Russian Federation in 2020-2022 (15 DDD, 30 days) and (22,5 DDD, 45 days).
| 2020 | 2021 | 2022 | |
|---|---|---|---|
| COVID-19 patients | 3 159 297 | 10 499 982 | 10 684 204 |
| 30 days | |||
| Total consumption of Rivaroxaban and Apixaban (patients) | 11 200 000 | 16 536 000 | 11 500 000 |
| 45 days | |||
| Total consumption of Rivaroxaban and Apixaban (patients) | 7 466 666 | 11 023 999 | 7 666 667 |
Results of CPGs assessment domain scores
The domain scores differed between CPGs. The domains Scope and Purpose, and Clarity of Presentation consistently received high scores across all seven CPGs. The domains Applicability, Editorial Independence and Rigour of Development received lower scores.
The domain Scope and Purpose deals with the main objective of CPGs, the health question and the population to whom the guideline is meant to apply. This domain includes 3 items (items 1–3). The range of scores for Scope and Purpose was 67%–100% (See Appendix 8 - Section assessment results SCOPE AND PURPOSE)
Most CPGs received high scores for this domain (89%–100%), while one CPG received lower score – 67 %. The CPG by the FAR (Zabolotskikh I.B., et al) obtained the lowest score for this domain. We attributed it to the guidelines having a vague and not clearly defined objective. The CPGs by ROPNIZ (Livzan M.A. et al), MGNOT (Vorobyev P.A., et al) score for Scope and Purposes. The population was clearly described and the purpose was well defined and worded here.
The domain Stakeholder Involvement is focused on assessing whether all relevant clinical professionals participated in the development of the CPG and whether the target audience who would use the CPG is specified. This domain includes three items (items 3–6). The range of scores was 31%–67% (See Appendix 8 - Section assessment results STAKEHOLDER INVOLVEMENT). The CPG by NIIOZMM (Khripun A.I., et al) received the lowest score (31%) and the CPG by ROPNIZ (Livzan M.A., et al) received the highest score – 67%.
We assigned relatively low score (31%) to the NIIOZMM (Khripun A.I., et al) for the domain Stakeholder Involvement as it did not include any specifications about the target audience. The experts pointed out that epidemiologists and medical statisticians should have been included in the development of CPG of NIIOZMM (Khripun A.I., et al)
The ROPNIZ CPG (Livzan M.A., et al) received the highest score (67%) for the domain Stakeholder Involvement (See Appendix 8 - Section assessment results STAKEHOLDER INVOLVEMENT). The variety of specialists were involved in the development of these guidelines, which was better than in all other identified CPGs. A similar score (65%) for this domain received in the ROPNIZ CPGs (Drapkina O.M., et al) and MGNOT (Vorobyev P.A., et al) (See Appendix 8 - Section assessment results STAKEHOLDER INVOLVEMENT). These three CPGs received similar comments.
The domain Rigour of Development deals with the actual methods used to compose the CPGs. It is the largest domain in the AGREE II and consists of eight items (items 7–14). The range of scores for this domain was 0%–49% (See Appendix 8 - Section assessment results RIGOUR OF DEVELOPMENT). Rigour and Development had the largest variation between the highest and the lowest scores, as it is the biggest and arguably the most important domain in the AGREE II. The scores for all CPGs varied.
The lowest score for the domain Rigour and Development we attributed to the ROPNIZ (Livzan M.A., et al) CPG by (See Appendix 8 - Section assessment results RIGOUR OF DEVELOPMENT).
This CPG lacked a procedure of evidence search, strengths and limitations of this evidence and most other items of this domain. The only item in the Rigour and Development that received a score above 1 from all three author-experts was the item 14, which deals with a procedure for updating the guideline, which is described in the guideline.
The highest score (49%) for the domain Rigour and Development was attributed to the ROPNIZ (Drapkina O.M., et al) CPG (Table_. Section assessment results RIGOUR OF DEVELOPMENT). Even though this CPG had a high score, there were comments for this domain: the ROPNIZ (Drapkina O.M., et al) CPG did not include the methods for formulating the recommendations and aren’nt clearly described, opinion of external experts and the update procedure is not described. It did not include a method for reviewing the strengths and limitations of the evidence (such as GRADE), or a Delphi method for formulating the recommendations.
The fourth domain Clarity of Presentation consists of three items (items 15–17). Clarity of presentation is focused on the way the CPG is written, specifically its language, format, and structure. This domain consistently received a high score in each of the CPGs (96%–100%) (See Appendix 8 - Section assessment results CLARITY OF PRESENTATION). All CPGs scored high (96-100%). The comments stated that the recommendations are clear and unambiguous (See Appendix 8 - Section assessment results CLARITY OF PRESENTATION).
The domain Applicability includes four items (items 18–21). Applicability mostly assesses the way that the CPG can be used in the society, including crucial factors such as assessment of cost, barriers and facilitators of implementation, as well as possible tactics for uptake of the recommendations. Overall, Applicability received a low score from the experts throughout all studied CPGs (24%–50%) (See Appendix 8 - Section assessment results APPLICABILITY).
The lowest score (24%) for the Applicability domain we attributed to the MGNOT (Vorobyev P.A., et al). Еhere was not enough information about the implementation factors in the CPG. On the other hand, the ROPNIZ (Drapkina O.M., et al) and its assumption received the highest score for the domain Applicability (See Appendix 8 -Section assessment results APPLICABILITY).
The last domain in the AGREE II is called Editorial Independence and it consists of two items (items 22–23). This domain score reflects whether the authors of a CPG could have had any conflict of interest in the matter of creating the CPG. This domain received the lowest ratings from all experts. The range of the scores was 0%–50%.
The lowest score of 0% was obtained for the ROPNIZ (Drapkina O.M., et al) CPG (See Appendix 8 - Section assessment results EDITORIAL INDEPENDENCE). because no information about the potential conflict of interest of the CPG authors was provided.
The highest score was received in the CPG for the diagnosis and treatment of circulatory diseases in the context of the COVID-19 pandemic (both received 50%; See Appendix 8 -Section assessment results EDITORIAL INDEPENDENCE).
Total sum of assessment scores
The total sum of scores, or the overall calculation was performed for each of the CPGs. Their comparison can be viewed in (See Appendix 8 - TOTAL SUM OF ASSESSMENT). It was used to assess the overall quality of the CPGs. Overall, the highest score (65%) was received in the CPG for the outpatient medical care in patients with chronic diseases under dispensary supervision in the conditions of the COVID-19 pandemic. Temporary guidelines. Version 2 (Table) and Guidelines for the diagnosis and treatment of circulatory diseases in the context of the COVID-19 pandemic. Only the domains Stakeholder involvement and Editorial Independence received low scores.
The lowest total sum score was given to the CPG by NIIOZMM (Khripun A.I., et al) (43%; (See Appendix 8 - TOTAL SUM OF ASSESSMENT). In four domains the score was less than 50%.
The peculiarity of the analyzed clinical recommendations were as follows that they were all written during the pandemic of the new coronavirus infection, which certainly affected the quality of the work. All clinical recommendations were issued as soon as possible, despite the lack of any evidence base. Their main goal was to develop an algorithm for the doctors actions and improve the quality of care provided to patients with the new coronavirus infection.
Comparison with U.S. data in consumption and sales of DOACs
We examined the available publicly data on the costs of sold rivaroxaban and apixaban in 2020, 2021 in the USA and noted the following dynamics [30,31].
The result was performed in (Appendix 9 - U.S.A. and Russia sales of DOACs 2020 -2021)
Discussion
The high level of consumption of NOACs and the growing cost of drugs in this group is a significant burden on the country’s economy, given the fact that the effectiveness and safety of the use of NOACs in patients with COVID-19 still requires more careful study.
In Russia and the USA, there is a tendency for the cost of consumption of apixaban and rivaroxaban to increase in 2021 compared to 2022.
In the USA, the consumption costs in 2021 compared to 2020 year of Rivaroxaban increased by 8%, apixaban by 23 % accordingly [30,31].
In Russia, the consumption costs for rivaroxaban in 2021 compared to 2020 increased by 90%, for apixaban- by 186% accordingly. The consumption costs for rivaroxaban in 2020 year was 89 millions USD, in 2021-171 millions USD and for apixaban- 28/ 81millions USD in 2020/2021 accordingly.
Thus, the cost of consumption of rivaroxaban in Russia compared to the USA exceeds by more than 12 times, and apixaban-by more than 2 times in 2020, and in 2021: rivaroxaban - by 23 times, apixaban - by 5 times.
It should be noted that the dynamics of changes in costs by country differs. Despite the higher cost of rivaroxaban and apixaban consumption in Russia compared to the USA, the share of gross consumption of apixaban in both countries is comparably higher than rivaroxaban.
Figure 1.
Gross national consumption of apixaban and rivaroxaban in the Russian Federation in 2020-2022 (number of DDDs per year).
Figure 1.
Gross national consumption of apixaban and rivaroxaban in the Russian Federation in 2020-2022 (number of DDDs per year).
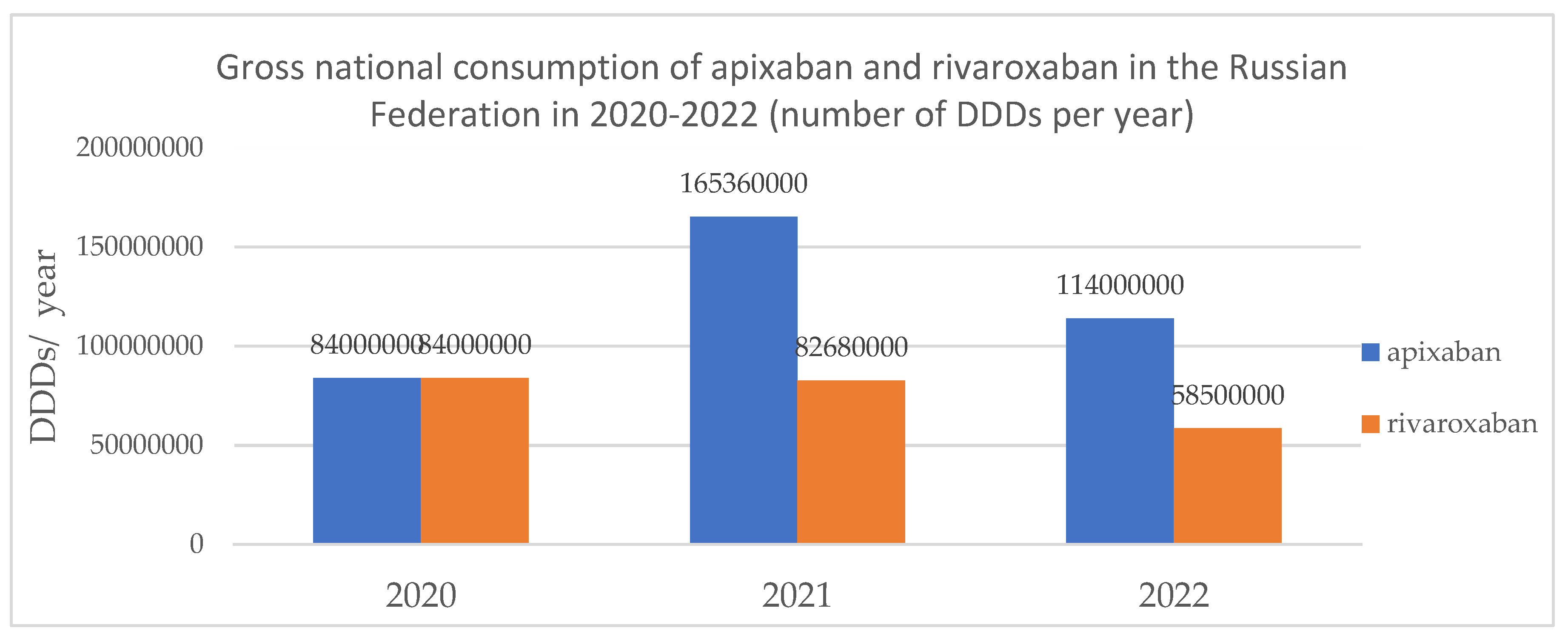
The highest DDD consumption of DOACs was in 2020, which exceeded the DOACs recommended DDD by Russian clinical guidelines, which is probably due to polypragmasia.
Figure 2.
DDDs/а case of COVID-19 of apixaban and rivaroxaban in the Russian Federation (2020 to 2022).
Figure 2.
DDDs/а case of COVID-19 of apixaban and rivaroxaban in the Russian Federation (2020 to 2022).
The above presented results mean that in 2020, each patient with covid received more than 1 course of therapy with apixaban (1.77 course of apixaban therapy (30-day)) and rivaroxaban (1.77 course of rivaroxaban therapy (30-day)), which indicates serious overdose of DOACs at the beginning of the pandemic. Excessive prescribing and consumption of DOAC may have been dictated by the available data from a number of studies that established the benefits of treating patients with COVID by DOACs for the prevention of deep vein thrombosis and pulmonary embolism compared to patients untreated with DOACs or receiving placebo. At the same time, there was no significant difference in the effect of small and large doses of drugs on the risk of bleeding [4,5].
Figure 3.
Number of people taking apixaban and rivaroxaban in the Russian Federation in 2020-2022 (15 DDD, 30 days).
Figure 3.
Number of people taking apixaban and rivaroxaban in the Russian Federation in 2020-2022 (15 DDD, 30 days).
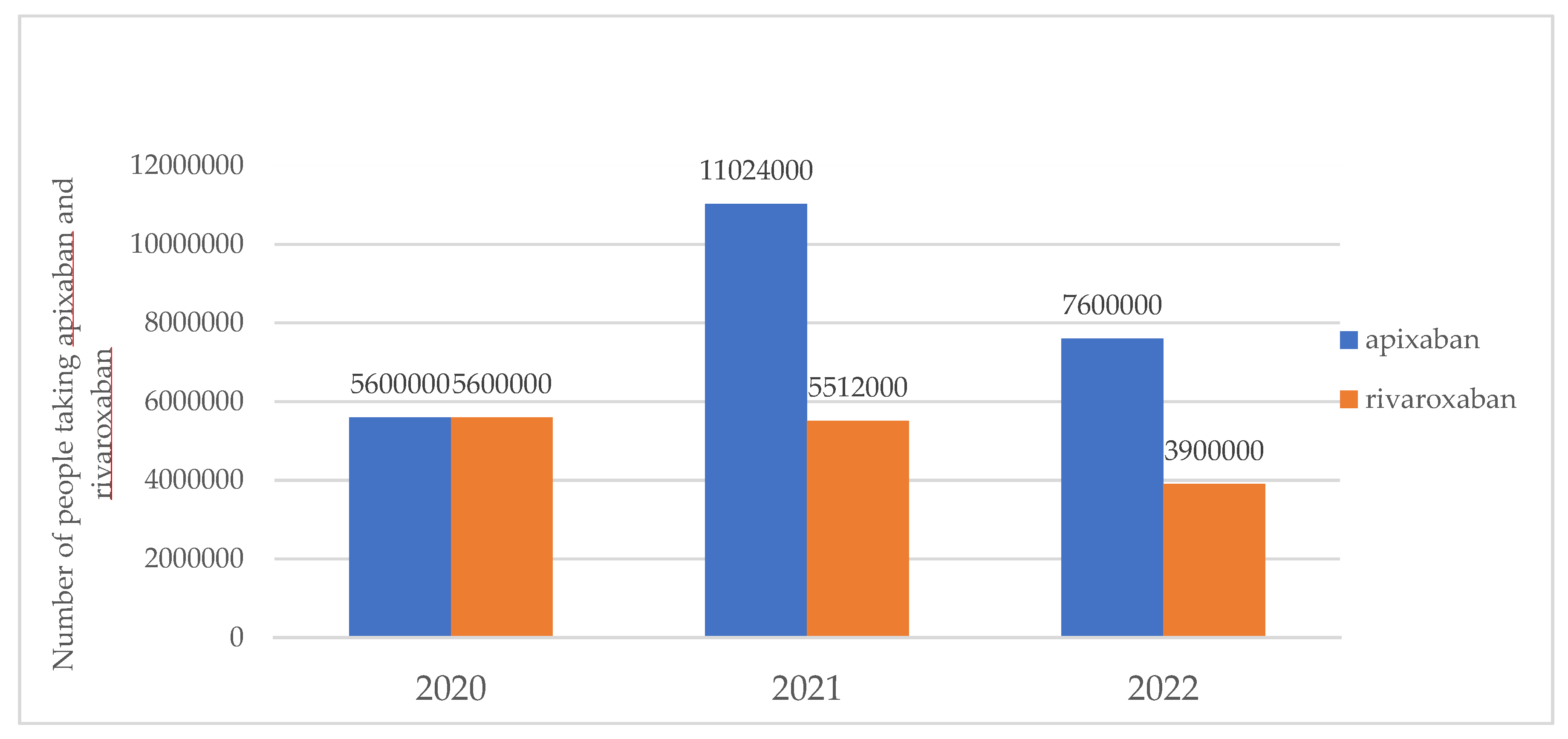
Figure 4.
Number of people taking apixaban and rivaroxaban in the Russian Federation in 2020-2022 (22,5 DDD, 45 days).
Figure 4.
Number of people taking apixaban and rivaroxaban in the Russian Federation in 2020-2022 (22,5 DDD, 45 days).
In 2020, there was a significant increase in demand for DOACs and apixaban consumption in our study was at the leading position what is comparable to the results of another study [32]. In 2021, the highest gross national consumption of apixaban was noted, almost every patient with COVID-19 received apixaban, and every second patient was prescribed rivaroxaban, which is probably due to the growth of the disease and the advantage of the drug compared to rivaroxaban: higher efficiency in reducing the risk of secondary episodes of venous thrombosis and pulmonary embolism, better tolerability-lower risk of minor bleeding and a favorable price [33].
DOACs consumption has decreased by 2022 but every third patient took rivaroxaban, and about ¾ of all patients took apixaban (30-day course). Тhe decrease in DOACs consumption occurred while maintaining a higher proportion of apixaban consumption during the coronavirus pandemic.
The dynamics of the decline in consumption of apixaban and rivaroxaban by 2022 may be a consequence of a more rational and targeted use of DOACs in patients with covid in the 3rd year of the pandemic, which may be the result of both, the accumulated experience and the emergence of clear algorithms for the management of patients with coronavirus infection (the CPGs).
Clinical practice guidelines (guidelines or clinical practice guidelines) are systematically developed statements to assist existing regimens, practitioners and patients on appropriate medical care in specific cases. The AGREE tool is a means of assessing the methodological rigor and transparency used in developing the guidelines.
We analyzed national guidelines using the AGREE II tool and obtained the following results.
7 clinical guidelines were assessed. The quality of some CPGs really has to be questioned due to the complete lack of in-text citations. Only two of the seven guidelines (FAR 2020 (Zabolotskikh I.B). and MGNOT 2021 (Vorobyev P.A.)) references are constantly cited throughout the text.
Each author reviewed the clinical guidelines using the AGREE II tool separately and independently. We did not compare each other's assessments. After each author rated the clinical guidelines and provided comments, we followed the same protocol described in the Methods section to calculate item scores and total scores for each clinical guideline. We also created a summary table (See appendix 8) to easily visualize the differences in scores between clinical guidelines. We tried to analyze only the methodological quality of the guidelines and the possibility of their practical implementation in the Russian Federation, as provided for by the AGREE II tool.
When reviewing clinical guidelines, we found significant variability in the CPGs assessed. Each CPG differs in its structure, organization of content, use of evidence, etc. Two clinical guidelines (ROPNIZ -Drapkina O.M., et al) and ROPNIZ (Livzan M.A., et al) were developed by a coalition of organizations, while all other guidelines were created individual organizations and ministries. Interestingly, ROPNIZ (Drapkina O.M., et al) and RSC 2020 (Shlyakhto E.V.) received the highest total score among the clinical guidelines studied (65%), and ROPNIZ 2021 (Livzan) took 5th place in overall rating of clinical recommendations, although the clinical recommendations ROPNIZ (Drapkina O.M., et al) and ROPNIZ 2021 (Livzan) were created by one group of organizations consisting of: ROPNIZ, NIIOZMM (Khripun A.I., et al).
One clinical guideline (Research Institute for Healthcare Organization and Medical Management of Moscow Healthcare Department 2021) has a low overall evaluation score.
We gave 0% points to three clinical guidelines (MoH 2022, ROPNIZ 2021(Drapkina), NIIOZMM 2021 for the last domain “EDITORIAL INDEPENDENCE”, as they did not indicate any funding or competing interests in the guideline text. Detailed scores for each domain can be found in table (See appendix 8)
In general, the authors' assessments differed slightly from each other. One of the reasons why the authors' answers were similar was that all the authors are specialists in the same field - pharmacology, so we may have the same points of view. The authors gave a low overall rating to certain clinical recommendations, but at the same time rated them 7 for overall quality (the last question of the AGREE II questionnaire, not used in calculating the total score). This may be explained by the fact that the authors took into account that the recommendations were created during a pandemic and were limited in information and time.
We do not know whether any of the developers of the clinical guidelines assessed in this study used AGREE II to develop their guidelines.
The low total scores we received when assessing Russian clinical guidelines can be explained by the fact that they were created during the COVID-19 pandemic, when there was still no clinical trial data and the time frame for creating guidelines was limited, since there was an urgent need to create algorithms for providing medical care to COVID-19 patients in order to simplify decision making by doctors.
Study limitations
There were no data on adverse reactions associated with using DOACs in patients with COVID-19 in the Russian Federation. There was a limitation on pharmacoepidemiological and pharmacoeconomic indicators in patients with COVID-19 for the period 2020-2022. Only CPGs available online were analysed. Institutional or any other CPGs were not analysed.
Conclusions:
1. Analysis of 7 clinical recommendations revealed that such sections of clinical recommendations as scope, purpose, clarity of presentation had the highest degree of assessment in accordance with AGREE II. The lowest scores were given for the sections stakehholder involment rigour of development, applicability, editorial independence. When comparing the total score, it was found that two clinical guidelines received the highest scores - Russian Society for the Prevention of Non-communicable Diseases (Livzan), Russian Society for the Prevention of Non-communicable Diseases (Drapkina). The minimum score was registered with the Research Institute for Healthcare Organization and Medical Management of Moscow Healthcare Department clinical guideline. No guideline received a total score of more than 70%.
2. During the pandemic, the highest DDD consumption of DOACs was in 2020, which exceeded the DOACs recommended DDD by Russian clinical guidelines. DOACs consumption has decreased by 2022. There was a decrease in the consumption of rivaroxaban, with an increase of apixaban share in the structure of DOACs consumption during the coronavirus pandemic.
3. Obtained data indicate that in 2021 the apixaban consumption in the Russian Federation corresponded to the recommended DDD in the national guidelines, which indicates the most correct use of apixaban according to Russian GPGs.
These findings and the limitations of this research are important to the Russian health community.
Russian clinical guidelines do not have a high rating due to the lack of clinical trial results and time restrictions during their creation during the pandemic.
List of abbreviation
| AGREE II | Appraisal of Guidelines for REsearch & Evaluation |
| ATC | Anatomical Therapeutic Chemical code |
| CDSR | Cochrane Database of Systematic Reviews |
| CONSORT | Consolidated Standards of Reporting Trials |
| COVID-19 | COronaVIrus Disease 2019 |
| CPG | clinical practice guidelines |
| DDD | Defined Daily Dose |
| DOAC | direct oral anticoagulants |
| DVT/ PE | deep vein thrombosis/ pulmonary embolism |
| FAR | The All-Russia Public Organization «Federation of Anaesthesiologists and Reanimatologists» |
| ICD-10 | International Classification of Diseases 10 |
| LMWH | Low molecular weight heparin |
| MGNOT (in Russ) | Moscow City Scientific Society of Physicians |
| MoH | Ministry of Health of the Russian Federation |
| NIIOZMM (in Russ) | Research Institute for Healthcare Organization and Medical Management of Moscow Healthcare Department |
| PE | pulmonary embolism |
| PMC | Pubmed Central |
| ROPNIZ (in Russ) | Russian Society for the Prevention of Non-communicable Diseases |
| RSC | Russian Society of Cardiology |
| RSCI | Russian Scientific Citation Index |
| VTE | venous thromboembolism |
| WHO | World health organization |
Author Contributions
Conceptualization, L.E.Z., S.K.Z., and E.A.B.; resources, L.E.Z. and S.K.Z.; data curation, L.E.Z. and E.A.B.; search of data sources—E.A.B., E.A.K and M.S.C.; writing—original draft preparation, E.A.B., E.A.K., M.S.C.; writing—review and editing, L.E.Z. and E.A.B.; supervision, S.K.Z and L.E.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Sources of information used in this review are listed in the References.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Schutgens RE. DOAC in COVID-19: Yes or No? Hemasphere. 2020 Dec 29;5(1):e526. PMID: 33403357; PMCID: PMC7773328. [CrossRef]
- Liao, SC., Shao, SC., Chen, YT. et al. Incidence and mortality of pulmonary embolism in COVID-19: a systematic review and meta-analysis. Crit Care 24, 464 (2020). [CrossRef]
- Roguljić H, Arambašić J, Ninčević V, Kuna L, Šesto I, Tabll A, Smolić R, Včev A, Primorac D, Wu GY, Smolić M. The role of direct oral anticoagulants in the era of COVID-19: are antiviral therapy and pharmacogenetics limiting factors? Croat Med J. 2022 Jun 22;63(3):287-294. PMID: 35722697; PMCID: PMC9284020. [CrossRef]
- Santos BC, Flumignan RL, Civile VT, Atallah ÁN, Nakano LC. Prophylactic anticoagulants for non-hospitalised people with COVID-19. Cochrane Database Syst Rev. 2023 Aug 16;8(8):CD015102. PMID: 37591523; PMCID: PMC10428666. [CrossRef]
- Flumignan RL, Civile VT, Tinôco JDS, Pascoal PI, Areias LL, Matar CF, Tendal B, Trevisani VF, Atallah ÁN, Nakano LC. Anticoagulants for people hospitalised with COVID-19. Cochrane Database Syst Rev. 2022 Mar 4;3(3):CD013739. PMID: 35244208; PMCID: PMC8895460. [CrossRef]
- Siegal DM. What we have learned about direct oral anticoagulant reversal. Hematology Am Soc Hematol Educ Program. 2019 Dec 6;2019(1):198-203. PMID: 31808835; PMCID: PMC6913453. [CrossRef]
- Nakamura J, Tsujino I, Yachi S, Takeyama M, Nishimoto Y, Konno S, Yamamoto N, Nakata H, Ikeda S, Umetsu M, Aikawa S, Hayashi H, Satokawa H, Okuno Y, Iwata E, Ogihara Y, Ikeda N, Kondo A, Iwai T, Yamada N, Ogawa T, Kobayashi T, Mo M, Yamashita Y; CLOT-COVID Study Investigators. Incidence, risk factors, and clinical impact of major bleeding in hospitalized patients with COVID-19: a sub-analysis of the CLOT-COVID Study. Thromb J. 2022 Sep 20;20(1):53. PMID: 36127738; PMCID: PMC9485792. [CrossRef]
- Popa P, Iordache S, Florescu DN, Iovanescu VF, Vieru A, Barbu V, Bezna MC, Alexandru DO, Ungureanu BS, Cazacu SM. Mortality Rate in Upper Gastrointestinal Bleeding Associated with Anti-Thrombotic Therapy Before and During Covid-19 Pandemic. J Multidiscip Healthc. 2022 Nov 18;15:2679-2692. PMID: 36425876; PMCID: PMC9680964. [CrossRef]
- Davtyan P.A., Gumerov R.M., Zagidullin S.Z., Samorodov A.V., Cai B., Zagidullin N.S. Is anticoagulant therapy necessary after hospitalization with COVID-19 pneumonia? Russian Journal of Cardiology. 2021;26(4S):4652. (In Russ.). [CrossRef]
- Tian Y, Pan T, Wen X, Ao G, Ma Y, Liu X, Liu R, Ran H. Efficacy and Safety of Direct Oral Anticoagulants Compared With Heparin for Preventing Thromboembolism in Hospitalized Patients With COVID-19: A Systematic Review and Meta-Analysis. Clin Appl Thromb Hemost. 2023 Jan-Dec;29:10760296231164355. PMID: 37131319; PMCID: PMC10170187. [CrossRef]
- Toubasi AA. Effect on Morbidity and Mortality of Direct Oral Anticoagulants in Patients With COVID-19. Am J Cardiol. 2022 May 15;171:174-177. Epub 2022 Mar 12. PMID: 35292148; PMCID: PMC8917387. [CrossRef]
- https://delprof.ru/press-center/open-analytics/farmatsevticheskiy-rynok-rossii-itogi-2021-goda-i-sobytiya-2022-goda/.
- Zhuravleva M.V., Chulanov V.P., Gagarina Yu.V., Shabalina E.A. Pharmacoeconomic analysis of tixagevimab and cilgavimab combination for COVID-19 therapy. FARMAKOEKONOMIKA. Modern Pharmacoeconomics and Pharmacoepidemiology. 2023;16(2):149-161. (In Russ.). [CrossRef]
- Wang T, Tan JB, Liu XL, Zhao I. Barriers and enablers to implementing clinical practice guidelines in primary care: an overview of systematic reviews. BMJ Open. 2023 Jan 6;13(1):e062158. PMID: 36609329; PMCID: PMC9827241. [CrossRef]
- https://www.whocc.no/atc_ddd_index/.
- AlphaRM Pharmaceutical sales in Russia https://pharmvestnik.ru/content/news/Aptechnye-prodaji-lekarstv-ushedshego-goda-pobili-rekord-2020-goda.html.
- Annual report (2022) of DSM group https://dsm.ru/docs/analytics/Annual_report_2023_rus.pdf.
- Report on the current situation in the region with coronavirus. Communication Center for the Economy of the Russian Federation, 01/11/2022.
- https://who.maps.arcgis.com/apps/dashboards/a19d5d1f86ee4d99b013eed5f637232d.
- https://covid19.rosminzdrav.ru/.
- Lienhard DA, Kisser LV, Ziganshina LE. Assessing methodological quality of Russian clinical practice guidelines and introducing AGREE II instrument in Russia. PLoS One. 2018 Sep 11;13(9):e0203328. PMID: 30204760; PMCID: PMC6133363. [CrossRef]
- Eikelboom JW, Jolly SS, Belley-Cote EP, et al. Colchicine and the combination of rivaroxaban and aspirin in patients hospitalised with COVID-19 (ACT): an open-label, factorial, randomised, controlled trial. Lancet Respir Med. 2022 Dec;10(12):1169-1177. Epub 2022 Oct 10. PMID: 36228641; PMCID: PMC9635892. [CrossRef]
- Shlyakhto E.V., Konradi A.O., Arutyunov G.P., et al. Guidelines for the diagnosis and treatment of circulatory diseases in the context of the COVID-19 pandemic. Russian Journal of Cardiology. 2020;25(3):3801. (In Russ.). [CrossRef]
- Zabolotskikh I.B., Kirov M.Yu., Lebedinskii K.M., et al. Anesthesia and intensive care for patients with COVID-19. Russian Federation of anesthesiologists and reanimatologists guidelines. Annals of Critical Care. 2021; S1:9–143. (In Russ.). [CrossRef]
- Drapkina O. M., Drozdova L. Y., Avdeev S. N., et al. The outpatient medical care in patients with chronic diseases under dispensary supervision in the conditions of the COVID-19 pandemic. Temporary guidelines. Version 2. Cardiovascular Therapy and Prevention. 2021;20(8):3172. (In Russ.). [CrossRef]
- Livzan M. A., Drapkina O. M., Nikolaev N. A., et al. Algorithms for adult outpatient care of coronavirus disease 2019 (COVID-19) and its assumption. Cardiovascular Therapy and Prevention. 2021;20(4):2916. (In Russ.). [CrossRef]
- Clinical protocol for the treatment of patients with new coronavirus infection (COVID-19), undergoing inpatient treatment in medical organizations of the healthcare state system of Moscow / M. B. Antsiferov, L. S. Aronov, A. S. Belevsky, et al. Ed. by A. I. Khripun. – M.: GBU “NIIOZMM DZM”, 2020. – 28 p.: ill.
- Recommendations for the outpatient management of COVID-19 patients with the acute infection and POST-COVID syndrome (Issued by the Moscow City Scientific Society of Physicians). Ed. By prof. Vorobyev P.A. Problems of standardization in healthcare. 2021; 7-8: 3-96. [CrossRef]
- Temporary methodological recommendations for prevention, diagnostics and treatment of new coronavirus infections (COVID-19). version 17 (14.12.2022). Ministry of Health of the Russian Federation.
- Tichy EM, Hoffman JM, Suda KJ, Rim MH, Tadrous M, Cuellar S, Clark JS, Wiest MD, Matusiak LM, Schumock GT. National trends in prescription drug expenditures and projections for 2021. Am J Health Syst Pharm. 2021 Jul 9;78(14):1294-1308. PMID: 33880494; PMCID: PMC8365501. [CrossRef]
- Tichy EM, Hoffman JM, Suda KJ, Rim MH, Tadrous M, Cuellar S, Clark JS, Ward J, Schumock GT. National trends in prescription drug expenditures and projections for 2022. Am J Health Syst Pharm. 2022 Jul 8;79(14):1158-1172. PMID: 35385103; PMCID: PMC9383648. [CrossRef]
- Petrukhina I.K., Lebedev P.A., Ryazanova T.K., Blinkova P.R., Paranina E.V. Consumption of cardiovascular and antithrombotic drugs during the spread of coronavirus infection in retail sector of the Samara region pharmaceutical market. Cardiosomatics. 2021;12(4):219–226. [CrossRef]
- Dawwas GK, Leonard CE, Lewis JD, Cuker A. Risk for Recurrent Venous Thromboembolism and Bleeding With Apixaban Compared With Rivaroxaban: An Analysis of Real-World Data. Ann Intern Med. 2022 Jan;175(1):20-28. Epub 2021 Dec 7. Erratum in: Ann Intern Med. 2022 Nov;175(11):1627-1628. [CrossRef] [PubMed]
Table 1.
Population of the Russian Federation and the number of cases of COVID-19 in the period from 2020 to 2022.
Table 1.
Population of the Russian Federation and the number of cases of COVID-19 in the period from 2020 to 2022.
| Year | Population of the Russian Federation | Incidence of COVID-19 in the Russian Federation, people |
|---|---|---|
| 2020 | 144 100 000 people | 3 159 297 people |
| 2021 October- November | 143 400 000 people | 10 499 982 people |
| 2022 (01.01.2022) | 146 980 000 people | 10 684 204 people (10.01.22) |
| 2023 (01.01.2023) |
146 447 000 people | 4 718 854 people |
| Total | 23 078 812 people (confirmed cases) |
Table 2.
Identified clinical practice guidelines to be assessed with AGREE II instrument.
| Condition | Organization | Year | Organization abbreviation with expansion |
|---|---|---|---|
| COVID-19 | Russian Society of Cardiology | 2020 | RSC 2020 (Shlyakhto E.V.) [23] |
| COVID-19 | The All-Russia Public Organization «Federation of Anaesthesiologists and Reanimatologists» | 2020 | FAR 2020 (Zabolotskikh I.B.) [24] |
| COVID-19 | Russian Society for the Prevention of Non-communicable Diseases | 2021 | ROPNIZ 2021(Drapkina O.M.) [25] |
| COVID-19 | Russian Society for the Prevention of Non-communicable Diseases | 2021 | ROPNIZ 2021 (Livzan M.A.) [26] |
| COVID-19 | Research Institute for Healthcare Organization and Medical Management of Moscow Healthcare Department | 2021 | NIIOZMM 2021 (Khripun A.I.) [27] |
| COVID-19 | Moscow City Scientific Society of Physicians | 2021 | MGNOT 2021 (Vorobyev P.A.) [28] |
| COVID-19 | Ministry of Health of the Russian Federation | 2022 | MoH 2022 [29] |
Table 3.
Sample data set for the domain Scope and Purpose.
| SCOPE AND PURPOSE | Е1 | Е2 | Е3 | Total (n) | Total (%) |
|---|---|---|---|---|---|
| 16 | 21 | 21 | 58 | 90.7% | |
| The overall objective(s) of the guideline is (are) specifically described. | 6 | 7 | 7 | 20 | |
| The health question(s) covered by the guideline is (are) specifically described. | 5 | 7 | 7 | 19 | |
| The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. |
5 | 7 | 7 | 19 |
Table 4.
Recommended NOAC consumption per patient with Covid-19 by Clinical Practice Guidelines.
| № | DOAC | DDD/ course of treatment or prophylaxis /patient | CPG |
|---|---|---|---|
| 1. | Rivaroxaban | 15 DDDs (30 days of course); 22,5 DDDs (45 days of course) |
MoH 2022; ROPNIZ 2021 (Drapkina); ROPNIZ 2021 (Livzan) |
| 2. | Apixaban | 15 (30 days of course); 22,5 (45 days of course) |
MoH 2022; ROPNIZ 2021 (Drapkina); ROPNIZ 2021 (Livzan) |
| 3. | Dabigatran etexilate | 22 (30 days of course); 15 (with creatinine clearance 30-49 ml/min) |
MoH 2022; ROPNIZ 2021 (Livzan) |
| 4. | Rivaroxaban | n/a | NIIOZMM 2021, MGNOT 2020, FAR 2020 |
| 5. | Apixaban | n/a | |
| 6. | Dabigatran etexilate | n/a |
Table 5.
Gross national consumption of apixaban and rivaroxaban in the Russian Federation in 2020-2022 (number of DDDs per year).
Table 5.
Gross national consumption of apixaban and rivaroxaban in the Russian Federation in 2020-2022 (number of DDDs per year).
| Name of the drug | 2020 (DDDs / year) | 2021 (DDDs / year) | 2022 (DDDs / year) |
|---|---|---|---|
| Apixaban | 84 000 000 DDD | 165 360 000 DDD | 114 000 000 DDD |
| Rivaroxaban | 84 000 000 DDD | 82 680 000 DDD | 58 500 000 DDD |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



