
Submitted:
04 November 2023
Posted:
06 November 2023
You are already at the latest version
Abstract
Background: This study delves into the examination of racial and ethnic disparities in the distribution of the Monkeypox (MPOX) virus vaccine within the United States, offering a critical healthcare perspective on an emerging public health concern. It particularly focuses on the demographic patterns associated with MPOX transmission and the allocation of vaccines. Methods: A comprehensive analysis was conducted, drawing on a wide array of data sources to understand the vaccine distribution and demographic trends in the United States. The study scrutinized three main aspects: MPOX cases by race and ethnicity, vaccine administration across different racial and gender categories, and the potential disparities therein. Results: The findings reveal significant disparities in the distribution of vaccine doses, with males, particularly gay, bisexual, and other Men who have sex with men (MSM), receiving the majority of doses. Moreover, substantial variations in MPOX cases are observed among different racial and ethnic groups, emphasizing the need for culturally sensitive public health strategies. Conclusions: The study underscores the urgent need for targeted public health interventions to address disparities and safeguard the well-being of those at higher risk, particularly MSM. It highlights the importance of equity in vaccine distribution and culturally sensitive approaches, and serves as a foundation for shaping effective public health policies and strategies to mitigate the spread of MPOX. This research advances our understanding of healthcare disparities in the context of an emerging viral infection, providing valuable insights for future public health initiatives.
Keywords:
MPOX
; health care intervention
; Men who have sex with men
; public health strategies
; vaccine
1. Introduction
MPOX (or monkeypox) is an illness caused by the monkeypox virus [1]. It is a viral infection which can spread between people and occasionally from the environment to people via things and surfaces that have been touched by a person with MPOX [2,3]. In settings where the monkeypox virus is present among some wild animals, it can also be transmitted from infected animals to people who have contact with them. The emergence of novel infectious diseases, such as MPOX viruses, has underscored the critical importance of equitable vaccine distribution and the impact of demographic factors on public health outcomes [4]. MPOX viruses, a family of rapidly evolving pathogens, have posed significant challenges to global health systems. As the United States, like other nations, grapples with containing the spread of MPOX viruses, it has become apparent that there are significant disparities in vaccine distribution and demographic trends affecting the effectiveness of vaccination efforts [5,6].
The COVID-19 pandemic, which emerged in the early 2020s, exposed the stark disparities in health outcomes, particularly among racial and ethnic minority populations. These disparities were attributed to a complex web of factors, including socioeconomic status, access to healthcare, structural racism, and healthcare disparities. It served as a poignant reminder of the need to address these issues comprehensively and in a timely manner [7,8,9,10]. As a result, the distribution of vaccines for emerging infectious diseases, such as MPOX viruses, has taken center stage in discussions surrounding public health, with the aim of rectifying past inequalities [11,12,13,14].
In the United States, the MPOX virus outbreak has had a significant impact on public health [15]. As of the latest available data, the country has reported a total of 30,861 confirmed cases of MPOX virus infection. Tragically, the virus has also led to the loss of 54 lives in the United States. These numbers provide a snapshot of the domestic situation and the challenges the country is facing in containing the spread of this emerging infectious disease. On a global scale, the MPOX virus has affected numerous nations, with a total of 90,656 confirmed cases reported worldwide [16,17]. While the United States is one of the countries grappling with this public health crisis, the global reach of the virus underscores the urgency of finding effective solutions to control its spread and minimize its impact. The correlation between MPOX and healthcare is multifaceted, playing a pivotal role in addressing the challenges posed by MPOX virus outbreaks [18]. The interplay between healthcare and MPOX encompasses several key aspects.
Within the sphere of healthcare, the response to MPOX outbreaks is a collective effort, requiring seamless coordination among healthcare systems, public health organizations, and various stakeholders [19,20,21]. This coordinated response includes early detection, effective case management, meticulous contact tracing, and the isolation of infected individuals. Such endeavors rely on adequate resources, personnel, and the joint commitment of healthcare agencies and public health organizations [22,23]. Furthermore, equitable vaccine distribution is an essential component of the healthcare response to MPOX. Healthcare systems are central to the distribution and administration of MPOX vaccines, ensuring their availability to all segments of the population [24]. Disparities in vaccine distribution can exacerbate existing health inequalities, emphasizing the significance of a healthcare-driven approach to vaccine dissemination.
In the event of an MPOX outbreak, the capacity of healthcare facilities is of paramount importance [25]. Adequate hospital capacity, which includes a sufficient number of intensive care units and ventilators, is vital in effectively managing patients, particularly those with severe MPOX cases. Ensuring this readiness is a shared responsibility that healthcare systems must fulfill [26]. The frontline healthcare workforce is directly involved in caring for MPOX patients. These dedicated professionals require specialized training, protective equipment, and support to ensure their safety and well-being while delivering optimal care. The collaboration between healthcare systems and healthcare workers is essential for maintaining an effective response during MPOX outbreaks. Additionally, healthcare organizations and professionals serve as a source of knowledge and guidance for the public [27,28]. They play a crucial role in educating communities about MPOX prevention, recognizing symptoms, and emphasizing the importance of vaccination. Public awareness and trust in the healthcare system are vital for building a cohesive and informed response. Moreover, healthcare systems are integral to the surveillance and data analysis of MPOX cases [29]. The data collected informs public health strategies and helps identify emerging trends in the spread of the virus, facilitating a more targeted and effective response. This underscores the interconnectedness of healthcare and data-driven decision-making in addressing MPOX outbreaks. The aim of this study is to provide a comprehensive investigation into racial and ethnic disparities in MPOX virus vaccine distribution and their interplay with demographic patterns within the United States, with a focus on the crucial role of the healthcare system.
This research seeks to illuminate how healthcare systems can address these disparities, encompassing vaccine distribution strategies and the effective management of hospital capacity during MPOX outbreaks. The objective is to identify key areas where healthcare systems can be pivotal in achieving equitable vaccine access and facilitating an efficient response to MPOX outbreaks. The ultimate goal is to offer evidence-based recommendations that empower healthcare stakeholders to strengthen healthcare-driven interventions for improved public health outcomes in the context of MPOX viruses.
2. Materials and Methods
Study design
Both datasets utilized in this study (N=29,162) were sourced from the U.S. Centers for Disease Control and Prevention (CDC), ensuring the reliability and credibility of the data [30].
Variables
- MPOX Cases Reported to CDC by Race and Ethnicity
The first dataset encompasses MPOX virus cases reported to the CDC and spans the period from May 2022 to September 2023. It provides comprehensive insights into the evolution of MPOX cases within various racial and ethnic groups. Demographic categories included American Indian or Alaska Native, Asian, Black or African American, Hispanic or Latino, Multiple Races, Native Hawaiian or Other Pacific Islander, Other Race, White, and cases with Missing Race and Ethnicity [31].
- MPOX Vaccine Administration and Effectiveness by Race/Ethnicity
The second dataset also originates from the CDC and focuses on MPOX vaccine administration and its effectiveness within distinct racial and ethnic segments of the population. It details the number of first and second doses administered, along with the percentage of the population that received the first and second doses [32].
- MPOX Vaccine Administration and Effectiveness by Sex
The third dataset offers insights into MPOX vaccine administration and its effectiveness classified by sex. It includes data on the number of first and second doses administered, as well as the percentage of the population that received the first and second doses. Sex categories analyzed encompass Male, Female, and cases with Unknown sex [32].
Data Analysis
The data analysis strategy employed a multifaceted approach to investigate patterns, disparities, and vaccine effectiveness in MPOX cases among diverse racial and ethnic groups. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to provide a comprehensive summary of the characteristics of MPOX cases and vaccine administration throughout the study period.
3. Results
Descriptive statistics analysis
Table 1 presents comprehensive descriptive statistics for MPOX cases, categorized by race and ethnicity, encompassing the total case count, the respective percentage within each category, and key statistical measures involving the mean and standard deviation. MPOX cases among Black or African American individuals total 9,461, comprising 32.45% of the overall cases.
Within this category, the mean number of cases stands at approximately 1,180.13, revealing a substantial level of variation in case numbers, accompanied by a standard deviation of approximately 2,375.49. Similarly, Hispanic or Latino individuals report 9,048 MPOX cases, constituting 31.03% of the total cases. In this group, the mean number of cases is approximately 1,131.00, and the standard deviation is roughly 2,208.59, indicating variations in case numbers. White individuals account for 8,600 MPOX cases, representing 29.49% of the total cases. Within this category, the mean number of cases is approximately 1,075.00, accompanied by a standard deviation of approximately 2,089.75, signifying variations in case numbers within this racial group. Additionally, Asian individuals contribute 808 MPOX cases, constituting 2.77% of the total cases, with a mean number of cases around 101.00 and a standard deviation of approximately 200.98. Furthermore, the "Other Race" category documents 606 MPOX cases, making up 2.08% of the total cases, with a mean case count of approximately 75.75 and a standard deviation of about 151.49. The Multiple Races category reports 441 MPOX cases, comprising 1.51% of the total cases, with a mean case count of around 55.13 and a standard deviation of approximately 111.58. American Indian or Alaska Native individuals experience 119 MPOX cases, representing 0.41% of the total cases. In this group, the mean case count is about 14.88, with a standard deviation of approximately 29.89. Additionally, individuals in the Native Hawaiian or Other Pacific Islander category report 77 MPOX cases, constituting 0.26% of the total cases, with a mean case count of approximately 9.63 and a standard deviation of about 19.34.
Table 2 presents descriptive statistics related to MPOX vaccine administration by race and ethnicity, showcasing the number of first and second doses administered, as well as the corresponding percentages. Additionally, it provides calculated values for the mean and standard deviation of first and second doses administered for each racial and ethnic category. White, non-Hispanic individuals received a total of 357,531 first doses and 242,890 second doses. This represents 51% of the total first doses administered and 54% of the second doses. Hispanic or Latino individuals received 162,461 first doses and 96,428 second doses, constituting 23% of the total first doses and 21% of the second doses. Black, non-Hispanic individuals received 88,134 first doses and 51,949 second doses, accounting for 12% of the total first doses and 11% of the second doses. Asian, non-Hispanic individuals received 52,288 first doses and 32,912 second doses, representing 7% of the total first doses and 7% of the second doses. Other, non-Hispanic individuals received 19,159 first doses and 10,542 second doses, constituting 3% of the total first doses and 2% of the second doses. American Indian/Alaska Native, non-Hispanic individuals received 3,021 first doses and 1,767 second doses. Multiple, non-Hispanic individuals received 20,173 first doses and 14,100 second doses. Native Hawaiian/Other Pacific Islander, non-Hispanic individuals received 1,830 first doses and 1,085 second doses.
Table 3 provides an overview of MPOX vaccine administration categorized by gender, encompassing the number of first and second doses administered, the respective percentages, and the calculated mean and standard deviation for both first and second doses.
Male individuals accounted for a substantial share of vaccine doses, with a total of 695,471 first doses and 449,205 second doses, making up 91% and 94% of the overall first and second doses, respectively. The mean number of first doses administered to males is estimated at approximately 347,735.50, displaying a significant degree of variability, as indicated by a standard deviation of around 411,838.50. Similarly, for second doses, males received an average of approximately 224,602.50, with a standard deviation of roughly 224,815.50, underscoring the variation in doses administered. In contrast, female individuals received 68,371 first doses and 31,046 second doses, representing 9% and 6% of the total first and second doses, respectively. The mean number of first doses administered to females is approximately 34,185.50, with a standard deviation of around 48,162.50, highlighting variations in the number of doses administered. For second doses, the mean number received by females is approximately 15,523.00, with a standard deviation of about 21,981.00, signifying fluctuations in dose administration within this group.
4. Discussion
Monkeypox is an illness resulting from infection with the human monkeypox virus, which belongs to the same virus family as smallpox [33,34]. Strikingly, its symptoms closely resemble those of smallpox, encompassing fever, headache, muscle aches, chills, and cold symptoms such as a cough or sore throat. These symptoms are often accompanied by a characteristic rash that forms blisters on various parts of the body, including the face, genitals, chest, back, hands, and feet (Figure 1; 34). In some cases, individuals may also experience painful sores in their mouth or other internal areas. For most individuals, the disease typically resolves within two to three weeks. Monkeypox is primarily transmitted through close physical contact with an infected person, predominantly via skin-to-skin contact, especially with the rashes and skin lesions characteristic of the disease. However, it can also spread through the release of large respiratory droplets, such as those generated by coughing and sneezing [35,36].
Regarding the hypothetical MPOX, a viral infection predominantly transmitted through close physical contact, including sexual activity, the implications are considerable in the realm of public health. This study unveils notable trends and disparities in MPOX cases, vaccine administration, and vaccination rates across different racial and gender categories. It’s essential to underscore those viral infections primarily transmitted through close physical contact, such as sexual activity, have the potential to affect individuals across diverse demographics [37]. The disparities elucidated in the data, particularly in vaccine administration and vaccination rates, emphasize the importance of targeted public health interventions. Importantly, these disparities aren’t uniform across racial and gender categories. Notably, males received the majority of vaccine doses, particularly second doses, raising questions about the effectiveness of vaccination campaigns among other demographic groups, including females and those categorized as "unknown." Furthermore, previous studies have highlighted that the majority of monkeypox infections are attributed to sexual contact, with a significant percentage involving rashes, mainly on the genitals, and a substantial portion presenting sores within the body, including the mouth or anus [38].
In a previous study, as evidenced by a report from the British Health Security Agency indicating that 97% of 699 monkeypox cases were observed in gay, bisexual, or other men who have sex with men (MSM). [39] Addressing the needs of vulnerable populations, notably sexually active gay, bisexual, and other Men who have sex with men (MSM), is critical in controlling the spread of MPOX. Such groups may necessitate tailored public health strategies ensuring accessible, affordable, and culturally sensitive vaccines [40,41]. This study underscores the urgency for discussions and actions within the public health sector to formulate strategies addressing the unique needs of these specific populations. Additionally, this study highlights significant variations in the number of MPOX cases across diverse racial and ethnic categories, emphasizing the necessity for culturally sensitive approaches in vaccination campaigns, particularly in communities with substantial numbers of cases, such as Black or African American and Hispanic or Latino populations.
This study underscores the importance of comprehending the demographics and disparities linked to MPOX cases and vaccine administration. This knowledge necessitates the development of comprehensive public health strategies to cater to the specific requirements of diverse communities and populations, particularly those at elevated risk. This approach should be rooted in principles of equity, ensuring equitable access and distribution of vaccines. These insights should serve as the foundation for policymaking and public health endeavors aimed at curbing the spread of MPOX while safeguarding the health of all individuals, irrespective of their demographic attributes.
5. Conclusions
The study related to vaccine administration raises questions about the effectiveness of vaccination campaigns. Notably, a skewed distribution of vaccine doses is observed, with males receiving the majority of doses, particularly in the case of second doses. This prompts further examination of vaccine coverage across different demographic groups, such as females and those categorized as "unknown," to ensure that vaccination efforts are inclusive and reach all segments of the population. These findings should serve as a catalyst for policy development and public health initiatives focused on controlling and mitigating the spread of MPOX while upholding health equity principles. Targeted strategies, cultural sensitivity, and equitable vaccine distribution should be at the forefront of our response to this emerging public health challenge. In summary, this study contributes valuable insights from a healthcare perspective, shedding light on the complex web of disparities and viral transmission patterns associated with MPOX. It underscores the pressing need for a multifaceted approach to address these issues and safeguard the well-being of all individuals affected by this emerging viral infection.
Funding
The preparation of this manuscript was partially supported by funding from the Department of Applied Social Sciences, The Hong Kong Polytechnic University.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
The data used in this study were sourced from the U.S. Centers for Disease Control and Prevention (CDC), guaranteeing the data’s reliability and credibility. Furthermore, this data is openly accessible to the public.
Acknowledgments
The preparation of this manuscript was partially supported by funding from the Department of Applied Social Sciences, The Hong Kong Polytechnic University, Hong Kong.
Conflicts of Interest
No potential conflict of interest was reported by the author.
References
- Petersen, Eskild et al. “Human Monkeypox: Epidemiologic and Clinical Characteristics, Diagnosis, and Prevention.” Infectious disease clinics of North America vol. 33,4 (2019): 1027-1043. [CrossRef]
- Berthet, Nicolas et al. “Genomic history of human monkey pox infections in the Central African Republic between 2001 and 2018.” Scientific reports vol. 11,1 13085. 22 Jun. 2021. [CrossRef]
- Thornhill, John P et al. “Monkeypox Virus Infection in Humans across 16 Countries - April-June 2022.” The New England journal of medicine vol. 387,8 (2022): 679-691. [CrossRef]
- Bunge, Eveline M et al. “The changing epidemiology of human monkeypox-A potential threat? A systematic review.” PLoS neglected tropical diseases vol. 16,2 e0010141. 11 Feb. 2022. [CrossRef]
- Adler, Hugh et al. “Clinical features and management of human monkeypox: a retrospective observational study in the UK.” The Lancet. Infectious diseases vol. 22,8 (2022): 1153-1162. [CrossRef]
- McCollum, Andrea M, and Inger K Damon. “Human monkeypox.” Clinical infectious diseases : an official publication of the Infectious Diseases Society of America vol. 58,2 (2014): 260-7. [CrossRef]
- Mitjà, Oriol et al. “Monkeypox.” Lancet (London, England) vol. 401,10370 (2023): 60-74. [CrossRef]
- Huang, Yong et al. “Monkeypox: epidemiology, pathogenesis, treatment and prevention.” Signal transduction and targeted therapy vol. 7,1 373. 2 Nov. 2022. [CrossRef]
- Gessain, Antoine et al. “Monkeypox.” The New England journal of medicine vol. 387,19 (2022): 1783-1793. [CrossRef]
- Kumar, Narendra et al. “The 2022 outbreak and the pathobiology of the monkeypox virus.” Journal of autoimmunity vol. 131 (2022): 102855. [CrossRef]
- Huang, Yong et al. “Monkeypox: epidemiology, pathogenesis, treatment and prevention.” Signal transduction and targeted therapy vol. 7,1 373. 2 Nov. 2022. [CrossRef]
- Poland, Gregory A et al. “Prevention of monkeypox with vaccines: a rapid review.” The Lancet. Infectious diseases vol. 22,12 (2022): e349-e358. [CrossRef]
- Harapan, Harapan et al. “Monkeypox: A Comprehensive Review.” Viruses vol. 14,10 2155. 29 Sep. 2022. [CrossRef]
- Kmiec, Dorota, and Frank Kirchhoff. “Monkeypox: A New Threat?.” International journal of molecular sciences vol. 23,14 7866. 17 Jul. 2022. [CrossRef]
- Centers for Disease Control and Prevention. (2023). 2022-2023 Outbreak Cases and Data. CDC. https://www.cdc.gov/poxvirus/mpox/response/2022/index.html.
- Centers for Disease Control and Prevention. (2023). 2022-2023 Outbreak Cases and Data. CDC. https://www.cdc.gov/poxvirus/mpox/response/2022/index.html.
- Centers for Disease Control and Prevention. (2023). 2022-2023 Mpox Outbreak Global Map. 2022 Mpox Outbreak Global Map | Mpox | Poxvirus | CDC.
- Minhaj, Faisal S et al. “Monkeypox Outbreak - Nine States, May 2022.” MMWR. Morbidity and mortality weekly report vol. 71,23 764-769. 10 Jun. 2022. [CrossRef]
- Rizk, John G et al. “Prevention and Treatment of Monkeypox.” Drugs vol. 82,9 (2022): 957-963. [CrossRef]
- Adler, Hugh et al. “Clinical features and management of human monkeypox: a retrospective observational study in the UK.” The Lancet. Infectious diseases vol. 22,8 (2022): 1153-1162. [CrossRef]
- Singhal, Tanu et al. “Monkeypox: A Review.” Indian journal of pediatrics vol. 89,10 (2022): 955-960. [CrossRef]
- Altindis, Mustafa et al. “Diagnosis of monkeypox virus - An overview.” Travel medicine and infectious disease vol. 50 (2022): 102459. [CrossRef]
- Farahat, Ramadan Abdelmoez et al. “Human monkeypox disease (MPX).” Le infezioni in medicina vol. 30,3 372-391. 1 Sep. 2022, doi:10.53854/liim-3003-6. [CrossRef]
- Velavan, Thirumalaisamy P, and Christian G Meyer. “Monkeypox 2022 outbreak: An update.” Tropical medicine & international health : TM & IH vol. 27,7 (2022): 604-605. [CrossRef]
- Petersen, Brett W et al. “Vaccinating against monkeypox in the Democratic Republic of the Congo.” Antiviral research vol. 162 (2019): 171-177. [CrossRef]
- Yinka-Ogunleye, Adesola et al. “Outbreak of human monkeypox in Nigeria in 2017-18: a clinical and epidemiological report.” The Lancet. Infectious diseases vol. 19,8 (2019): 872-879. [CrossRef]
- Patel, Aatish et al. “Clinical features and novel presentations of human monkeypox in a central London centre during the 2022 outbreak: descriptive case series.” BMJ (Clinical research ed.) vol. 378 e072410. 28 Jul. 2022. [CrossRef]
- Bryer, Josh et al. “Monkeypox emerges on a global scale: A historical review and dermatologic primer.” Journal of the American Academy of Dermatology vol. 87,5 (2022): 1069-1074. [CrossRef]
- Samaranayake, Lakshman, and Sukumaran Anil. “The Monkeypox Outbreak and Implications for Dental Practice.” International dental journal vol. 72,5 (2022): 589-596. [CrossRef]
- Centers for Disease Control and Prevention. (2023). Mpox Vaccination Basics. https://www.cdc.gov/poxvirus/mpox/response/2022/index.html.
- Centers for Disease Control and Prevention. (2023). Mpox Cases by Age and Gender and Race and Ethnicity. https://www.cdc.gov/poxvirus/mpox/response/2022/demographics.html.
- Centers for Disease Control and Prevention. (2023). Mpox Vaccine Administration in the U.S. https://www.cdc.gov/poxvirus/mpox/response/2022/vaccines_data.html.
- Alakunle, Emmanuel et al. “Monkeypox Virus in Nigeria: Infection Biology, Epidemiology, and Evolution.” Viruses vol. 12,11 1257. 5 Nov. 2020. [CrossRef]
- Petersen, Eskild et al. “Human Monkeypox: Epidemiologic and Clinical Characteristics, Diagnosis, and Prevention.” Infectious disease clinics of North America vol. 33,4 (2019): 1027-1043. [CrossRef]
- Kupferschmidt, Kai. “Why monkeypox is mostly hitting men who have sex with men.” Science (New York, N.Y.) vol. 376,6600 (2022): 1364-1365. [CrossRef]
- Martín-Delgado, M C et al. “Monkeypox in humans: a new outbreak.” Revista espanola de quimioterapia : publicacion oficial de la Sociedad Espanola de Quimioterapia vol. 35,6 (2022): 509-518. [CrossRef]
- Girometti, Nicolò et al. “Demographic and clinical characteristics of confirmed human monkeypox virus cases in individuals attending a sexual health centre in London, UK: an observational analysis.” The Lancet. Infectious diseases vol. 22,9 (2022): 1321-1328. [CrossRef]
- Minhaj, Faisal S et al. “Monkeypox Outbreak - Nine States, May 2022.” MMWR. Morbidity and mortality weekly report vol. 71,23 764-769. 10 Jun. 2022. [CrossRef]
- The UK Health Security Agency (UKHSA) (2023). Investigation into monkeypox outbreak in England: technical briefing 3. https://www.gov.uk/government/publications/monkeypox-outbreak-technical-briefings/investigation-into-monkeypox-outbreak-in-england-technical-briefing-3.
- Veeraraghavan, Vishnu Priya et al. “Improving the mental health of lesbian, gay, bisexual, transgender, queer, intersex and asexual (LGBTQIA+) community through counseling and rehabilitation measures during monkey pox disease outbreak.” Travel medicine and infectious disease vol. 52 (2023): 102558. doi:10.1016/j.tmaid.2023.102558. [CrossRef]
- Girometti, Nicolò et al. “Demographic and clinical characteristics of confirmed human monkeypox virus cases in individuals attending a sexual health centre in London, UK: an observational analysis.” The Lancet. Infectious diseases vol. 22,9 (2022): 1321-1328. doi:10.1016/S1473-3099(22)00411-X. [CrossRef]
Figure 1.
The Progression of MPOX Lesions: MPOX lesions initiate as flat bases, subsequently evolving into small, fluid-filled blisters.
Figure 1.
The Progression of MPOX Lesions: MPOX lesions initiate as flat bases, subsequently evolving into small, fluid-filled blisters.
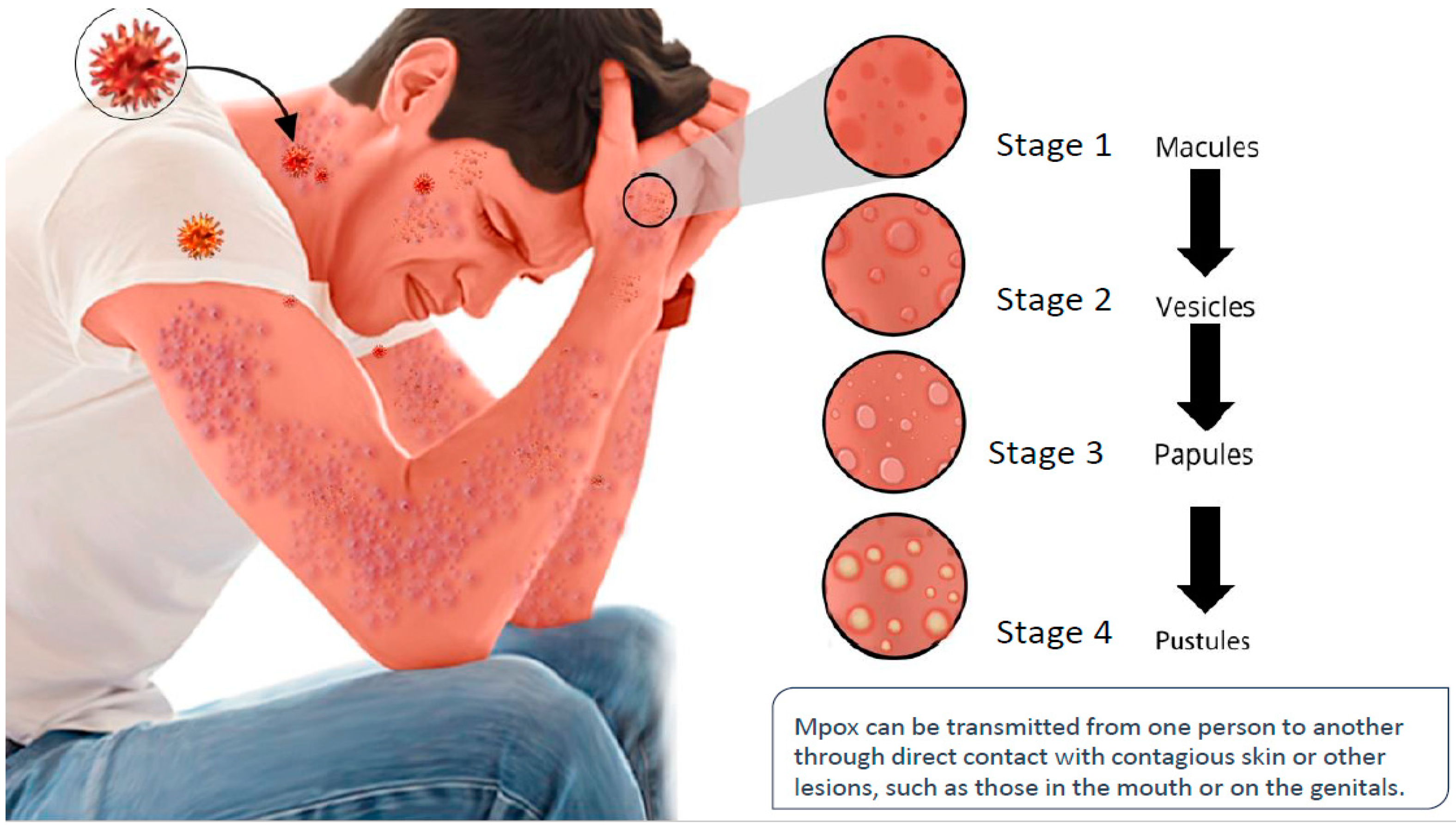

Table 1.
Descriptive Statistics for MPOX Cases by Race and Ethnicity
| Race/Ethnicity | Total Cases (N) | Percentage (%) | Mean Cases | Standard Deviation |
|---|---|---|---|---|
| Black or African American | 9,461 | 32.45% | 1,180.13 | 2,375.49 |
| Hispanic or Latino | 9,048 | 31.03% | 1,131.00 | 2,208.59 |
| White | 8,600 | 29.49% | 1,075.00 | 2,089.75 |
| Asian | 808 | 2.77% | 101.00 | 200.98 |
| Other Race | 606 | 2.08% | 75.75 | 151.49 |
| Multiple Races | 441 | 1.51% | 55.13 | 111.58 |
| American Indian or Alaska Native | 119 | 0.41% | 14.88 | 29.89 |
| Native Hawaiian or Other Pacific Islander | 77 | 0.26% | 9.63 | 19.34 |
| Missing | 1,701 | ... | ... | ... |
| Total | 29,162 | 100% | --- | --- |
Note:The percentages in the table represent the proportion of MPOX cases within each racial and ethnic category in relation to the total number of MPOX cases. The "Missing" category does not have specific numerical data available, which is why mean and standard deviation calculations were not applicable for this category.
Table 2.
Descriptive Statistics for MPOX Vaccine Administration by Race/Ethnicity
| Race/Ethnicity | First Doses (N) | Second Doses (N) | First Dose Percentage (%) | Second Dose Percentage (%) | Mean First Doses | Standard Deviation (First Doses) | Mean Second Doses | Standard Deviation (Second Doses) |
|---|---|---|---|---|---|---|---|---|
| White, non-Hispanic | 357,531 | 242,890 | 51% | 54% | 45,941 | 84,179 | 33,636 | 85,293 |
| Hispanic or Latino | 162,461 | 96,428 | 23% | 21% | 20,307 | 34,385 | 20,814 | 35,208 |
| Black, non-Hispanic | 88,134 | 51,949 | 12% | 11% | 11,017 | 13,190 | 8,656 | 12,933 |
| Asian, non-Hispanic | 52,288 | 32,912 | 7% | 7% | 6,536 | 6,416 | 4,738 | 6,440 |
| Other, non-Hispanic | 19,159 | 10,542 | 3% | 2% | 2,395 | 2,977 | 1,318 | 2,171 |
| American Indian/Alaska Native, non-Hispanic | 3,021 | 1,767 | 0% | 0% | 378 | 276 | 294 | 289 |
| Multiple, non-Hispanic | 20,173 | 14,100 | 3% | 3% | 2,521 | 2,511 | 1,758 | 2,476 |
| Native Hawaiian/Other Pacific Islander, non-Hispanic | 1,830 | 1,085 | 0% | 0% | 229 | 135 | 155 | 109 |
| Unknown | 70,506 | 32,970 | ... | ... | ... | ... | ... | ... |
Note: The percentages in the table represent the proportion of first and second doses administered within each racial and ethnic category in relation to the total first and second doses administered. The "Unknown" category contains data for which mean and standard deviation calculations were not applicable due to insufficient information.
Table 3.
Descriptive Statistics for MPOX Vaccine Administration by Gender
| Sex | First Doses (N) | Second Doses (N) | First Dose Percentage (%) | Second Dose Percentage (%) | Mean First Doses | Standard Deviation (First Doses) | Mean Second Doses | Standard Deviation (Second Doses) |
|---|---|---|---|---|---|---|---|---|
| Male | 695,471 | 449,205 | 91% | 94% | 347,735.50 | 411,838.50 | 224,602.50 | 224,815.50 |
| Female | 68,371 | 31,046 | 9% | 6% | 34,185.50 | 48,162.50 | 15,523.00 | 21,981.00 |
| Unknown | 13,170 | 5,855 | ... | ... | ... | ... | ... | ... |
| Total | 777,012 | 486,106 | 100% | 100% | ... | ... | ... | ... |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



