
Submitted:
07 November 2023
Posted:
07 November 2023
You are already at the latest version
Abstract
Ureteral stricture (US) following ureteroscopic lithotripsy (URSL) has emerged as a serious issue due to the widespread use of laser technology. The management of complex US is challenging. This prospective study evaluated the efficacy of robot-assisted uretero-ureterostomy (RAUU) in addressing US following URSL, and analyzed the pathology of transected ureteral tissues to identify the risk factors for US during URSL. Fourteen patients, with a mean age of 49.8 years, were included in this study. The mean stricture length on radiography was 22.66 ± 7.38 mm. Nine (64.2%) patients had experienced failure with previous interventions, including eight patients who underwent endoscopic incision plus balloon dilation. At an average follow-up of 12.8 months, the overall success rates were 92.9% both clinically and radiographically, without major complications. Pathological findings revealed microcalcifications in 57.1% patients and loss of ureteral mucosa in 28.6% patients. In conclusion, this technique of RAUU via end-to-end anastomosis exhibits promise as a viable option for US following URSL in appropriately selected patients, despite serious pathological changes of the ureter. Migration to the site of ureteral perforation may be the most serious factor contributing to the development of US.
Keywords:
robot-assisted uretero-ureterostomy
; ureteral stricture
; ureteroscopic lithotripsy
; microcalcification
1. Introduction
The utilization of ureteroscopic lithotripsy (URSL), a minimally invasive technique for the management of urinary calculi, has steadily increased over the past few decades [1,2]. Despite its efficacy in stone removal, the procedure may lead to severe postoperative complications, including sepsis, urinary injury, and ureteral stricture (US). Notably, with advances in laser technology, the incidence of US following URSL has gradually increased to approximately 3.0% [3,4]. The prompt treatment of these strictures is critical as they can lead to significant issues such as pain, hydronephrosis, recurrent urinary tract infections, and impaired renal function, if left untreated.
Nonetheless, managing US remains challenging. Endoscopic treatment, the least invasive option, may have reduced success rates when URSL is the cause of US [5]. Traditional surgical techniques, including open ureteral reimplantation and laparoscopic ureteral reconstruction, have been employed to manage complex or recurrent US [6,7]. However, these approaches have inherent limitations, including extended hospital stays, increased postoperative pain, and prolonged recovery periods [8,9]. Consequently, robot-assisted ureteral reconstruction has emerged as a viable option with good results because of the advantages of three-dimensional vision, magnified visibility, and adjunct near-infrared fluorescence (NIRF) imaging [8,9,10,11].
However, despite these promising outcomes, the specific utility of robot-assisted techniques for the management of US following URSL remains an underexplored area of investigation. Herein, we prospectively evaluated the efficacy of robot-assisted uretero-ureterostomy (RAUU) against US after URSL and analyzed the pathology of transected ureteral tissues to identify potential risk factors for US during URSL.
2. Patients and Methods
2.1. Patient Population
This prospective cohort study was approved by the Institutional Review Board of Nagoya City University Graduate School of Medical Sciences (46-21-0004). We included 14 patients who underwent RAUU for US following URSL at Nagoya City University Hospital from April 2021 to May 2023. This study adhered to the guidelines of the Declaration of Helsinki (revised in 2013) and informed consent was obtained from all participants.
Patients were selected for surgery based on the evidence of strictures on diagnostic imaging. The inclusion criteria were patients who had hydronephrosis (grade > 2 according to the Ellenborgen classification [12]) due to US following URSL. In this study, US was defined as at least one of the following: presence of long-segment US (2-4 cm) confirmed through radiographic evaluation after failed management, with deterioration of kidney function on the affected side (< 20 % diagnosed by renal scintigraphy).
Patients who were younger than 19 years old, undergoing treatment for malignant disease, had recent pyelonephritis, underwent dialysis treatment, were unable to undergo general anesthesia, or had suspected pregnancies were excluded from this study.
2.2. Data Collection
Clinical and imaging data were prospectively collected; patient demographics, including previous stone characteristics that were treated by URSL, and preoperative imaging including ultrasound, CT, retrograde ureterography, and renal scintigraphy. Stone volume was calculated using Tiselius’s formula (length × width × 3.14 × 0.25) [13]. US characteristics, including location, site, length, and previous management, were also evaluated. The US length was measured using antegrade or retrograde ureterographic imaging.
The primary goal of this study was to evaluate the success and complication rates of this procedure. The success status was determined as follows: absence of symptoms without ureteral stent and nephrostomy; relief of hydronephrosis on ultrasonography and CT 3 months postoperatively; and no recurrence of US at the latest follow-up. All patients were evaluated for perioperative complications according to the modified Clavien-Dindo classification [14]. Secondary outcomes were total surgical duration, console time, blood loss during surgery, and pathological characteristics of the stricture sites. Histopathological analysis was performed using hematoxylin and eosin staining and Masson’s trichrome staining to ascertain tissue levels of fibrosis, and Pizzolato staining and polarized light microscopy to observe calcification at the US site.
2.3. Surgical Technique
2.3.1. Patient and Robot Setup
All surgeries were performed transperitoneally using da Vinci Xi surgical system (Intuitive Surgical, Sunnyvale, Ca, USA) by two surgeons (SH, KT) who have performed > 200 robotic surgeries. Under general anesthesia, prior to RAUU, an open-end ureteral catheter or illumination catheter (infrared illumination system (IRIS); Stryker, Kalamazoo, MI, USA) was inserted transuretheally and positioned just below the stricture site under fluoroscopic guidance in the lithotomy position. The patient positioning and port placement were modified according to the US location. Patients undergoing proximal and middle US were positioned in the lateral flank position, with the affected site facing upwards. In contrast, patients who underwent distal US were positioned in the low-lithotomy position with a steep Trendelenburg. Generally, we employ four robotic trocars and one 12 mm trocar for assistance.
2.4. Stricture Identification
Following medial mobilization of the affected side of the colon, the retroperitoneal space was expanded to locate the ureter. In some cases, the US location was identified using intraureteral injection of indocyanine green (ICG) under NIRF, as previously described [10]. In other cases, illumination with an IRIS catheter was used to identify and secure the stricture (Figure 1A,B).
2.5. Dissection of the Ureteral Stricture, Anastomosis and Stenting
Following confirmation of the length of the US, the narrow segment was incised longitudinally on the ventral side using Potts scissors (Intuitive Surgical). Before the ureter was fully transected, two stitches were sutured between the proximal and distal ends of the healthy ureter to avoid misleading the anastomotic direction. Following the insertion of a 6Fr double-J ureteral catheter, the segmental lesion was completely resected, and anastomosis was performed using 4-0 Monocryl sutures. After the procedure, a suction drain was placed around the reconstruction site. Ureteral stents were removed 6 weeks postoperatively using retrograde pyelography to evaluate the status of the anastomosis site and resolution of obstruction.
2.6. Statistical Analysis
All data were analyzed using EZR software for R (The R Foundation for Statistical Computing, Vienna, Austria) [15]. The quantitative variables were expressed as mean ± SD or median (interquartile ranges (IQR)), depending on the distribution pattern. Categorical data were expressed as numbers (percentages).
3. Results
3.1. Clinical Characteristics
The demographic and clinical characteristics of the 14 patients with previous urinary calculi are summarized in Table 1. The cohort consisted of 10 males and four females, with a mean age of 49.8 years old. The urinary calculi that led to US were distributed in the UPJ (28.6%), proximal ureter (50.0%), middle ureter (14.3%), and distal ureter (7.1%). The median stone volume was 78.11 [IQR, 72.76–99.11] mm2. All patients underwent URSL, with a median of 2.00 [IQR 1.00–2.00] procedures performed.
Details of the US are presented in Table 2. US distribution sites encompassed the UPJ (21.4%), proximal ureter (50.0%), middle ureter (21.4%), and distal ureter (7.1%). Notably, four patients (28.6%) exhibited a mismatch between the location of urinary calculi and US. The mean stricture length on radiography was 22.66 ± 7.38 mm. Nine (64.2%) patients had undergone previously failed interventions, including eight patients who underwent endoscopic incision plus balloon dilation.
3.2. Surgical Outcomes
Perioperative and follow-up outcomes are shown in Table 3. All robotic procedures were completed successfully without intraoperative complications or the need for conversion. In eight patients (57.1%), intraureteral injection of ICG under NIRF was used for identifying the US, while illuminating IRIS catheter was used in six patients (42.9%). With regards to intraoperative variables, the mean console time was 164.36 ± 44.18 min and median blood loss was 10.00 [IQR 0.00—57.00] ml.
Postoperatively, two patients experienced complications: one patient had a port site infection requiring antibiotic treatment and one patient reported postoperative pain after discharge. However, no major complications occurred (more than grade III according to the Clavien-Dindo classification). All patients underwent successful removal of the ureteral stents, and in 13 patients, postoperative hydronephrosis improved or disappeared at 3 months after surgery. Preoperative hydronephrosis was observed in 13 patients; three (21.4%) had no hydronephrosis and 10 (71.4%) exhibited mild hydronephrosis without clinical significance. The overall success rate, both clinically and radiographically, was 92.9% at a mean follow-up of 12.8 months.
3.3. Pathological Analysis
The mean length of the transected ureter was 26.36 ± 39.34 mm. Hematoxylin and eosin staining (Figure 2A–C) revealed the loss of ureteral mucosa, inflammatory cell infiltration, and the presence of foreign body giant cells. Additionally, Masson’s trichrome staining revealed severe fibrosis in the periureteral tissues (Figure 2D). Pizzolato staining and polarized light microscopy revealed macrocalcifications (Figure 2E,F). Inflammatory cell infiltration and fibrosis were observed in 13 patients (92.9%), microcalcification in eight patients (57.1%), and loss of urothelium was observed in four patients (28.6%).
4. Discussion
This study demonstrated that RAUU is an effective and safe treatment for complex US following URSL. To our knowledge, this is the first study to reveal that most cases exhibited pathological changes, including fibrosis, calcification, and loss of the urothelium, potentially contributing to severe US.
The management of US is challenging because surgical options may be limited depending on the etiology, length, and site of US. US may have various etiologies including congenital ureteropelvic junction obstruction, traumatic or immunological diseases, compression from malignant disorders, retrocaval ureters, ureteral calculi, and previous endourological procedures. Care must be taken when treating US caused by endourological procedures, especially because it may be iatrogenic and the success rates of endoscopic management are low. We previously reported a significantly lower success rate of endoscopic management for the endoscopic management of US following URSL compared to other etiologies (30% vs. 100%, p=0.004) [5]. Ureteral damage caused by URSL has been reported to be associated with ischemic changes, which may result in the failure of endoscopic treatment [16,17]. In this study, 64.2% of patient had undergone prior failed endoscopic interventions. Redo procedures for complex US are often difficult owing to periureteral fibrosis, adhesions, and decreased vascularity. In such cases, open surgery, laparoscopic repair, and robot-assisted ureteral reconstruction may be good choices with excellent outcomes [18,19,20].
Recent advances in robot-assisted ureteral reconstruction for US has expanded the indications including ureterostomy, ureteral reimplantation, buccal mucosa graft ureteroplasty, and ileal replacement [21,22,23,24,25]. Robotic approaches have comparable efficacy to open techniques, with some perioperative advantages in terms of blood loss, surgical time, and hospitalization duration [9,26]. Moreover, robotic surgery has the advantage of a shorter learning curve for suturing than laparoscopic surgery. RAUU, a simple surgery yet effective technique, involves end-to-end anastomosis of the viable ureter after transection of the damaged ureter. Hemal et al. retrospectively reviewed 12 RAUU cases for proximal US or retrocaval ureters [27]. However, few studies have evaluated the efficacy of RAUU because it requires a watertight, tension-free, and well-vasculated anastomosis, and the indications for RAUU are relatively small. In particular, surgeons often opt against RAUU for distal US because of its low success rate owing to the tenuous plexiform vessels that supply the distal ureter. In a previous study, the success rate of RAUU in carefully selected patients was > 90% [23,28,29]. However, the success rate for managing complex US following URSL in this study was as high as 92.0%, including one distal US case, at a mean follow-up of 12.8 months. Furthermore, similar to previous reports, we found no major perioperative complications (> grade III) according to the Clavien-Dindo classification [23,29]. Our findings suggest that the RAUU may play a role in the management of US following URSL.
The versatility of the robotic platform in minimally invasive procedures does present specific challenges in identifying precise margins between the stricture and healthy ureteral tissue because the surgeon must rely on visual information due to the lack of tactile feedback. Several approaches have been reported for visually localizing US boundaries. Buffi et al. used a flexible ureteroscope to identify stricture in three of five cases during RAUU [21]. Lee et al. reported the efficacy of intraluminal ICG injection for rapid identification of US under NIRF using the Firefly system in a retrospective review of 26 robot-assisted ureteral reconstructions [10]. In this study, we successfully identified the US location using an illumination catheter in six cases. The IRIS is a new system that facilitates visualization of the ureter without a contrast agent, such as methylene blue or ICG, by inserting a thin translucent fiber connected to an NIRF source into a ureteral catheter. The brightness can be adjusted, making it useful for patients with ureteral walls thickened due to fibrosis. To the best of our knowledge, this is the first study to evaluate the efficacy of IRIS during RAUU. IRIS offers a promising avenue for enhanced visualization during RAUU procedures.
There have been some reports on the risk factors of postoperative US following URSL. Sunaryo et al. reported that, in a large population-based database of 329,776 patients, the US rate after URSL (2.9%) was higher than that after shock wave lithotripsy (1.5%), which may indicate a negative effect of the endoscopic device on stricture formation [3]. Ulvik et al. reported that the use of a ureteral access sheath (UAS), ureteral perforation, and long surgical time were risk factors for postoperative US formation. However, they only discussed the clinical results following URSL, and few reports have evaluated ureteral tissue that underwent US. To the best of our knowledge, this is the first study to examine the histopathology of the transected ureteral tissue leading to US. In this cohort, most patients exhibited inflammatory cell infiltration and fibrosis in the surrounding tissue. Important factors in US formation may be the wound-healing response to damage and subsequent remodeling of the ureteral wall; some inflammatory and wound-healing cytokines are involved in this process [30]. The inflammatory process subsequent to ureteral damage forms a fibrinous exudate at the site of tissue injury as part of the immune response, promoting adhesion and ultimately stricture formation. In addition, urine leakage from the ureter contributes to periureteral fibrosis, particularly in the presence of an infection [16]. Patients who underwent prior treatment tended to have severe fibrosis and inflammatory changes surrounding the ureter.
In this study, 57.1% patients had microcalcifications embedded in the ureteral mucosa. Dretler et al. [31] reported that migrated stone fragments into ureteral mucosa facilitate the formation of "stone granuloma" where macrophage and foreign body giant cells could be observed, resulting in the development of US. In short, migration to the site of ureteral perforation might be the most serious cause of US. The causes of ureteral perforation include a missed shot of the holmium-yttrium aluminum garnet (YAG) laser and USA insertion into a narrow ureter. Traxer et al. found that 46.5% of patients who underwent URSL with 12/14F UAS developed of ureteral wall injuries [32]. When stone dust migrates into areas of ureteral injury caused by UAS, the US may develop in a different area from the stone impaction site. In this study, 28.6% of patients exhibited US at a different site from where the previous stone localized.
In addition, thermal injuries may negatively affect US formation. Our study revealed that 28.6% patients had loss of ureteral mucosa due to damage from laser ablation. Holmium-YAG lasers are considered safe for use in endourological settings because they are completely absorbed by water within 0.4 mm. However, there is a risk of direct or indirect thermal injuries. Direct thermal injury occurs due to the attachment of laser bubbles, while indirect injuries occur when the fluid temperature around the laser increases excessively. In particular, temperature increases occurred with continuous laser irradiation without irrigation [33]. With the recent introduction of high-power lasers, some studies have reported their efficacy and safety during the procedure, particularly the clinical benefits of the dusting technique [34]. However, the potential risk of laser thermal injury from the improper use of high-power lasers must be considered.
This study has some methodological limitations. This descriptive study had a small sample size, which may limit the evaluation of RAUU efficacy. Subsequent larger cohort and comparative studies are warranted to further validate our findings. Nonetheless, this is the first study that focused on US following URSL and analyzed the pathological features of these changes. Our results highlight the importance of preventing ureteral damage during URSL.
5. Conclusion
We evaluated the safety and efficacy of RAUU for US following URSL. Despite the serious pathological changes observed in the ureter, this technique employing end-to-end anastomosis may be a viable option for US following URSL in appropriately selected patients.
Author Contributions
Conceptualization, Shuzo Hamamoto and Kazumi Taguchi; Data curation, Shuzo Hamamoto, Kengo Kawase and Toshiki Etani; Formal analysis, Kazumi Taguchi, Kengo Kawase and Rei Unno; Investigation, Shuzo Hamamoto, Koei Torii and Shoichiro Iwatsuki; Methodology, Masahiko Isogai; Project administration, Shuzo Hamamoto; Supervision, Atsushi Okada and Takahiro Yasui; Visualization, Toshiki Etani; Writing – original draft, Shuzo Hamamoto; Writing – review & editing, Shuzo Hamamoto, Kazumi Taguchi, Kengo Kawase, Taku Naiki and Atsushi Okada.
Funding
This study received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Nagoya City University Graduate School of Medical Sciences (46-21-0004).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgments
The authors would like to thank Editage for the English language review. We thank Ms. N. Kasuga for secretarial assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Chung, K.J.; Kim, J.H.; Min, G.E.; Park, H.K.; Li, S.; Del Giudice, F.; Han, D.H.; Chung, B.I. Changing trends in the treatment of nephrolithiasis in the real world. J Endourol 2019, 33, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, S.; Miyazawa, K.; Yasui, T.; Iguchi, T.; Fujita, M.; Nishimatsu, H.; Masaki, T.; Hasegawa, T.; Hibi, H.; Arakawa, T.; et al. Chronological changes in epidemiological characteristics of lower urinary tract urolithiasis in Japan. Int J Urol 2019, 26, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Sunaryo, P.L.; May, P.C.; Holt, S.K.; Sorensen, M.D.; Sweet, R.M.; Harper, J.D. Ureteral strictures following ureteroscopy for kidney stone disease: A population-based assessment. J Urol 2022, 208, 1268–1275. [Google Scholar] [CrossRef] [PubMed]
- Ulvik, Ø.; Harneshaug, J.R.; Gjengstø, P. Ureteral strictures following ureteroscopic stone treatment. J Endourol 2021, 35, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Sugino, T.; Taguchi, K.; Hamamoto, S.; Okada, T.; Isogai, M.; Tanaka, Y.; Unno, R.; Fujii, Y.; Hamakawa, T.; Ando, R.; et al. Risk factors for failure of endoscopic management of stone-related ureteral strictures. Urol J 2021, 19, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Carlton, C.E. Jr.; Guthrie, A.G.; Scott, R. Jr. Surgical correction of ureteral injury. J Trauma 1969, 9, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Simmons, M.N.; Gill, I.S.; Fergany, A.F.; Kaouk, J.H.; Desai, M.M. Laparoscopic ureteral reconstruction for benign stricture disease. Urology 2007, 69, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Kolontarev, K.; Kasyan, G.; Pushkar, D. Robot-assisted laparoscopic ureteral reconstruction: а systematic review of literature. Cent Eur J Urol 2018, 71, 221–227. [Google Scholar] [CrossRef]
- Elsamra, S.E.; Theckumparampil, N.; Garden, B.; Alom, M.; Waingankar, N.; Leavitt, D.A.; Kreshover, J.; Schwartz, M.; Kavoussi, L.R.; Richstone, L. Open, laparoscopic, and robotic ureteroneocystotomy for benign and malignant ureteral lesions: a comparison of over 100 minimally invasive cases. J Endourol 2014, 28, 1455–1459. [Google Scholar] [CrossRef]
- Lee, Z.; Moore, B.; Giusto, L.; Eun, D.D. Use of indocyanine green during robot-assisted ureteral reconstructions. Eur Urol 2015, 67, 291–298. [Google Scholar] [CrossRef]
- Elbers, J.R.; Rodríguez Socarrás, M.; Rivas, J.G.; Autran, A.M.; Esperto, F.; Tortolero, L.; Carrion, D.M.; Sancha, F.G. Robotic repair of ureteral strictures: techniques and review. Curr Urol Rep 2021, 22, 39. [Google Scholar] [CrossRef] [PubMed]
- Ellenbogen, P.H.; Scheible, F.W.; Talner, L.B.; Leopold, G.R. Sensitivity of gray scale ultrasound in detecting urinary tract obstruction. AJR Am J Roentgenol 1978, 130, 731–733. [Google Scholar] [CrossRef] [PubMed]
- Tiselius, H.G.; Andersson, A. Stone burden in an average Swedish population of stone formers requiring active stone removal: how can the stone size be estimated in the clinical routine? Eur Urol 2003, 43, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.W.; Cadeddu, J.A.; Micali, S.; Kavoussi, L.R.; Moore, R.G. Ureteral stricture formation after removal of impacted calculi. J Urol 1998, 159, 723–726. [Google Scholar] [CrossRef] [PubMed]
- Netto Júnior, N.R.; Ferreira, U.; Lemos, G.C.; Claro, J.F. Endourological management of ureteral strictures. J Urol 1990, 144, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Vannahme, M.; Mathur, S.; Davenport, K.; Timoney, A.G.; Keeley, F.X. Jr. The management of secondary pelvi-ureteric junction obstruction – a comparison of pyeloplasty and endopyelotomy. BJU Int 2014, 113, 108–112. [Google Scholar] [CrossRef]
- Moscardi, P.R.; Barbosa, J.A.; Andrade, H.S.; Mello, M.F.; Cezarino, B.N.; Oliveira, L.M.; Srougi, M.; Dénes, F.T.; Lopes, R.I. Reoperative laparoscopic ureteropelvic junction obstruction repair in children: safety and efficacy of the technique. J Urol 2017, 197, 798–804. [Google Scholar] [CrossRef]
- Lee, M.; Lee, Z.; Houston, N.; Strauss, D.; Lee, R.; Asghar, A.M.; Corse, T.; Zhao, L.C.; Stifelman, M.D.; Eun, D.D.; et al. Robotic ureteral reconstruction for recurrent strictures after prior failed management. BJUI Compass 2023, 4, 298–304. [Google Scholar] [CrossRef]
- Buffi, N.; Cestari, A.; Lughezzani, G.; Bellinzoni, P.; Sangalli, M.; Scapaticci, E.; Zanoni, M.; Annino, F.; Larcher, A.; Lazzeri, M.; et al. Robot-assisted uretero-ureterostomy for iatrogenic lumbar and iliac ureteral stricture: technical details and preliminary clinical results. Eur Urol 2011, 60, 1221–1225. [Google Scholar] [CrossRef]
- White, C.; Stifelman, M. Ureteral reimplantation, psoas hitch, and Boari flap. J Endourol 2020, 34, S25–S30. [Google Scholar] [CrossRef] [PubMed]
- Buffi, N.M.; Lughezzani, G.; Hurle, R.; Lazzeri, M.; Taverna, G.; Bozzini, G.; Bertolo, R.; Checcucci, E.; Porpiglia, F.; Fossati, N.; et al. Robot-assisted surgery for benign ureteral strictures: experience and outcomes from four tertiary care institutions. Eur Urol 2017, 71, 945–951. [Google Scholar] [CrossRef]
- Heijkoop, B.; Kahokehr, A.A. Buccal mucosal ureteroplasty for the management of ureteric strictures: A systematic review of the literature. Int J Urol 2021, 28, 189–195. [Google Scholar] [CrossRef]
- Yang, K.; Wang, X.; Xu, C.; Li, Z.; Han, G.; Fan, S.; Chen, S.; Li, X.; Zhu, H.; Zhou, L.; et al. Totally intracorporeal robot-assisted unilateral or bilateral ileal ureter replacement for the treatment of ureteral strictures: technique and outcomes from a Single Center. Eur Urol 2023. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Lu, Y.; Hu, H.; Zhang, J.; Qin, B.; Zhu, J.; Dirie, N.I.; Zhang, Z.; Wang, S. Management of recurrent ureteral stricture: a retrospectively comparative study with robot-assisted laparoscopic surgery versus open approach. PeerJ 2019, 7, e8166. [Google Scholar] [CrossRef] [PubMed]
- Hemal, A.K.; Nayyar, R.; Gupta, N.P.; Dorairajan, L.N. Experience with robot assisted laparoscopic surgery for upper and lower benign and malignant ureteral pathologies. Urology 2010, 76, 1387–1393. [Google Scholar] [CrossRef]
- Yang, K.K.; Asghar, A.M.; Lee, R.A.; Strauss, D.; Kuppa, S.; Lee, Z.; Metro, M.; Eun, D.D. Robot-assisted laparoscopic distal ureteroureterostomy for distal benign ureteral strictures with long-term follow-up. J Endourol 2022, 36, 203–208. [Google Scholar] [CrossRef]
- Lee, Z.; Llukani, E.; Reilly, C.E.; Mydlo, J.H.; Lee, D.I.; Eun, D.D. Single surgeon experience with robot-assisted ureteroureterostomy for pathologies at the proximal, middle, and distal ureter in adults. J Endourol 2013, 27, 994–999. [Google Scholar] [CrossRef]
- Ueshima, E.; Fujimori, M.; Kodama, H.; Felsen, D.; Chen, J.; Durack, J.C.; Solomon, S.B.; Coleman, J.A.; Srimathveeravalli, G. Macrophage-secreted TGF-β1 contributes to fibroblast activation and ureteral stricture after ablation injury. Am J Physiol Ren Physiol 2019, 317, F52–F64. [Google Scholar] [CrossRef]
- Dretler, S.P.; Young, R.H. Stone granuloma: a cause of ureteral stricture. J Urol 1993, 150, 1800–1802. [Google Scholar] [CrossRef] [PubMed]
- Traxer, O.; Thomas, A. Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol 2013, 189, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Wollin, D.A.; Carlos, E.C.; Tom, W.R.; Simmons, W.N.; Preminger, G.M.; Lipkin, M.E. Effect of laser settings and irrigation rates on ureteral temperature during holmium laser lithotripsy, an in vitro model. J Endourol 2018, 32, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Pietropaolo, A.; Massella, V.; Ripa, F.; Sinha, M.M.; Somani, B.K. Ureteroscopy and lasertripsy with pop dusting using high power holmium laser for large urinary stones > 15 mm: 6.5-year prospective outcomes from a high-volume stone center. World J Urol 2023, 41, 1935–1941. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Robot-assisted ureteroureterostomy in a patient with left ureteral stricture. Identification of ureteral stricture (A) in the absence of infrared illumination system (IRIS) and (B) under IRIS catheter. Red arrow heads indicate the top of the IRIS catheter. White arrows indicate the narrow segment of the ureter. (C) Excision of stricture segment (D) End-to-end anastomosis of the healthy ureters.
Figure 1.
Robot-assisted ureteroureterostomy in a patient with left ureteral stricture. Identification of ureteral stricture (A) in the absence of infrared illumination system (IRIS) and (B) under IRIS catheter. Red arrow heads indicate the top of the IRIS catheter. White arrows indicate the narrow segment of the ureter. (C) Excision of stricture segment (D) End-to-end anastomosis of the healthy ureters.
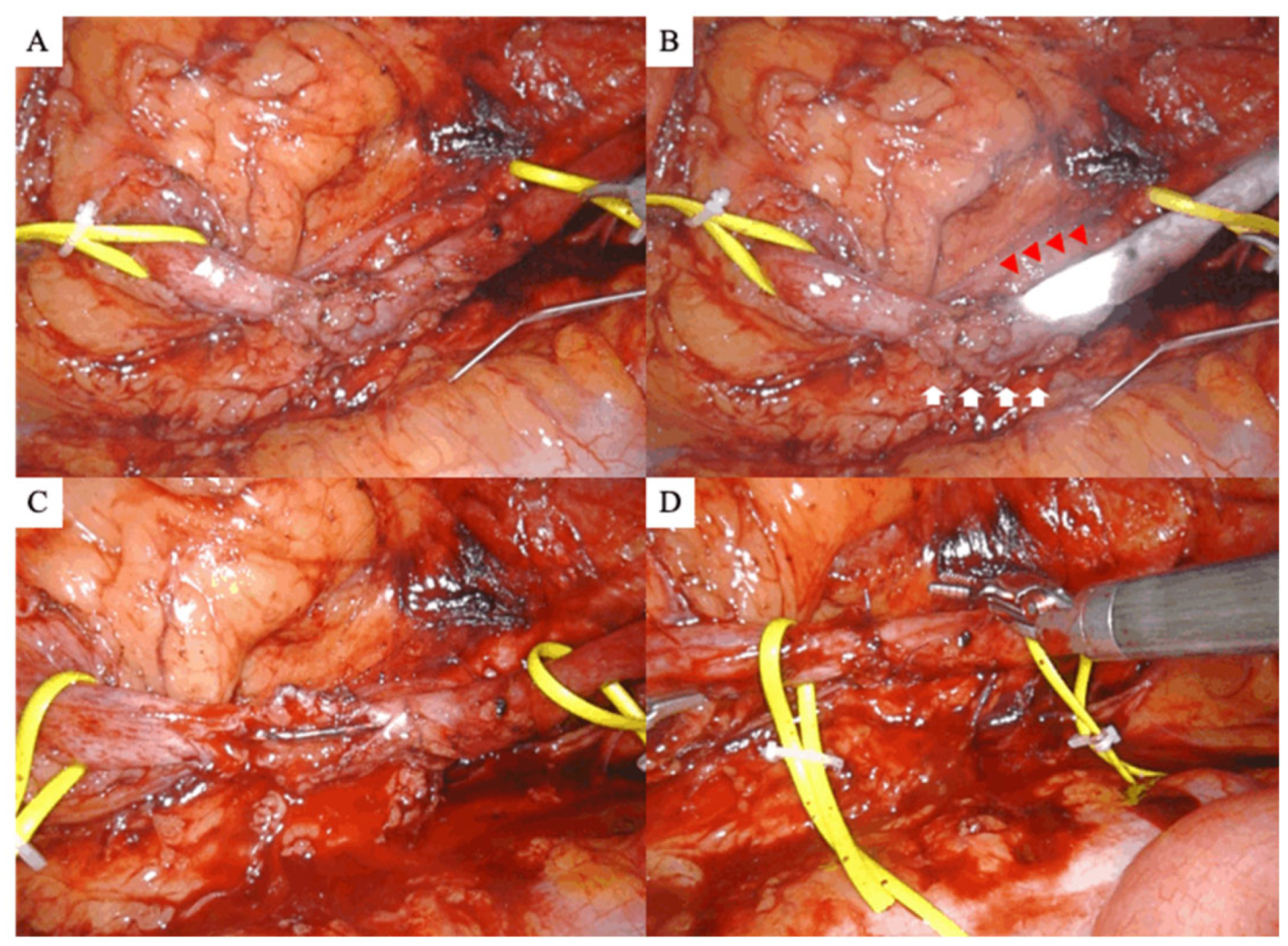
Figure 2.
Pathological findings of transected ureters. (A,B,C) Hematoxylin and eosin staining of these tissues. Loss of ureteral mucosa and inflammatory cell infiltration are observed in the tissue (A, B). (C) The high-power magnification of Fig (B) and foreign body giant cells can be observed in the ureteral submucosa. (D) Masson’s trichrome stain shows the fibrosis of periureteral tissues. (E) Pizzolato staining and (F) polarized light microscope indicate the existence of microcalcification. Scale bar, 500μm.
Figure 2.
Pathological findings of transected ureters. (A,B,C) Hematoxylin and eosin staining of these tissues. Loss of ureteral mucosa and inflammatory cell infiltration are observed in the tissue (A, B). (C) The high-power magnification of Fig (B) and foreign body giant cells can be observed in the ureteral submucosa. (D) Masson’s trichrome stain shows the fibrosis of periureteral tissues. (E) Pizzolato staining and (F) polarized light microscope indicate the existence of microcalcification. Scale bar, 500μm.
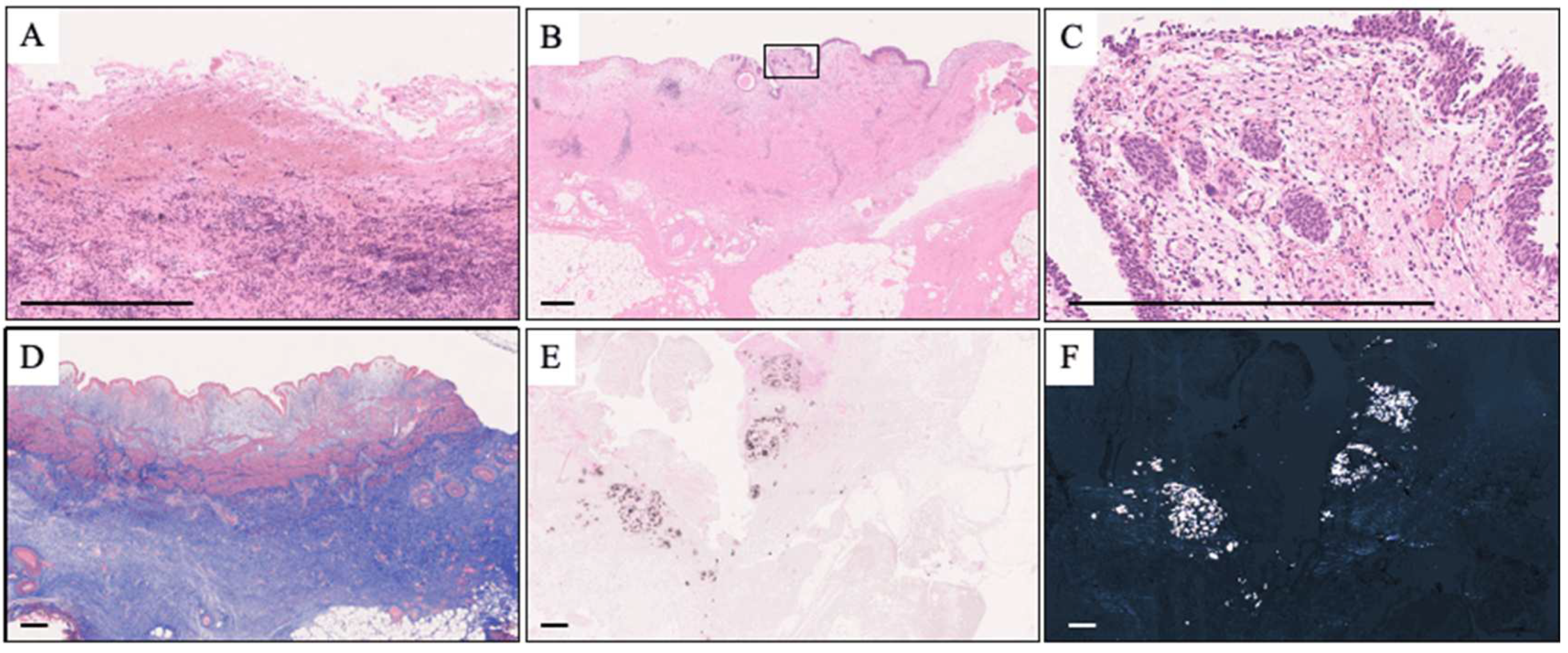

Table 1.
Patient and stone characteristics.
| Patient characteristics | |||
| age | y.o. | 49.8 | (10.2) |
| sex (%) | |||
| male | 10 | (71.4) | |
| female | 4 | (28.6) | |
| laterality (%) | |||
| right | 6 | (42.9) | |
| left | 8 | (57.1) | |
| BMI | kg/m2 | 23.07 | (2.11) |
| Characteristics of previous urinary calculi | |||
| location (%) | |||
| UPJ | 4 | (28.6) | |
| proximal ureter | 7 | (50.0) | |
| middle ureter | 2 | (14.3) | |
| distal ureter | 1 | (7.1) | |
| stone size | mm | 11.85 | [11.00, 14.75] |
| stone volume | mm2 | 78.11 | [72.76, 99.11] |
| number of previous stone treatment | |||
| SWL | 0.00 | [0.00, 0.00] | |
| URSL | 2.00 | [1.00, 2.00] | |
| PCNL | 0.00 | [0.00, 0.00] | |
| stone analysis (%) | |||
| calcium stone | 8 | (57.1) | |
| ammonium Acid Urate | 1 | (7.1) | |
| cystine | 1 | (7.1) | |
| unknown | 4 | (28.6) | |
Mean (SD), median [25% IQR, 75% IQR], number (%). BMI, body mass index; y.o, years old; UPJ, ureteropelvic junction; SWL, shock wave lithotripsy; URSL, ureteroscopic lithotripsy; PCNL, percutaneous nephrolithotomy.
Table 2.
Ureteral stricture characteristics.
| stricture location (%) | |||
|---|---|---|---|
| UPJ | 3 | (21.4) | |
| proximal ureter | 7 | (50.0) | |
| middle ureter | 3 | (21.4) | |
| distal ureter | 1 | (7.1) | |
| deviation from the previous stone site (%) | 4 | (28.6) | |
| stricture length on radiography | mm | 22.66 | (7.38) |
| prior treatment for stricture (%) | |||
| none | 5 | (35.7) | |
| balloon dilation | 1 | (7.1) | |
| endoscopic incision plus balloon dilation | 8 | (57.1) | |
| frequency of prior treatment for stricture | times | 1.00 | [0.00, 1.00] |
| perioperative hydronephrosis (%) | |||
| no obstruction | 0 | (0) | |
| mild | 0 | (0) | |
| moderate | 4 | (28.6) | |
| severe | 10 | (71.4) | |
| split renal function of the affected side | % | 29.28 | (15.31) |
Mean (SD), median [25% IQR, 75% IQR], number (%). UPJ, ureteropelvic junction.
Table 3.
Perioperative variables.
| stricture identification | |||
|---|---|---|---|
| ICG | 8 | (57.1) | |
| IRIS catheter | 6 | (42.9) | |
| transected ureter length | mm | 26.36 | (9.60) |
| surgery time | minutes | 205.53 | (46.51) |
| console time | minutes | 164.36 | (44.18) |
| blood loss | ml | 10.00 | [0.00, 57.00] |
| postoperative complication (Clavien-Dindo grade; %) | |||
| 0 | 12 | (85.7) | |
| I | 1 | (7.1) | |
| II | 1 | (7.1) | |
| >= III | 0 | (0) | |
| postoperative hydronephrosis 3 months after surgery (%) | |||
| none | 3 | (21.4) | |
| mild | 10 | (71.4) | |
| moderate | 1 | (7.1) | |
| severe | 0 | ||
| success rate (%) | 13 | (92.9) | |
| pathological features (%) | |||
| inflammatory cell infiltration | 13 | (92.9) | |
| fibrosis | 13 | (92.9) | |
| calcification | 8 | (57.1) | |
| loss of urothelium | 4 | (28.6) | |
Mean (SD), median [25% IQR, 75% IQR], number (%). ICG, indocyanine Green; IRIS, infrared illumination system.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



