
Submitted:
08 November 2023
Posted:
09 November 2023
You are already at the latest version
Abstract
Non-suicidal self-injurious behavior (NSSI), prevalent in patients with non-psychotic mental disorders (NPMD), is associated with numerous adverse outcomes. Despite active research into the clinical and psychological aspects of NSSI, the underlying biological mechanisms remain obscure. Early adverse experiences are believed to induce long-lasting changes in neuroendocrine mechanisms of stress control playing a key role in NSSI development. The aim of the study was to evaluate parameters potentially predicting development of NSSI in female patients with NPMD. Eighty female patients over 18 years with NPMD and suicidal ideation (40 with and 40 without NSSI) and 48 age matching women without evidence of mental illness (healthy controls) were enrolled. Diagnostic interviews and self-report measures were used to assess childhood maltreatment, presence, frequency, and characteristics of suicidal and self-injurious thoughts and behaviors, the Beck Depression Inventory scale to assess severity of depression. Hypothalamic-pituitary-adrenal axis markers, hormones, and neurotrophic factors were measured in blood serum. The likelihood of developing NSSI in patients with NPMD was associated with early adverse family history and elevated adrenocorticotropic hormone levels. Dysregulation of hypothalamic-pituitary-adrenal axis as a result of early chronic stress experiences may represent critical biological mechanism promoting the development of NSSI behaviors in patients with NPMD.
Keywords:
non-suicidal self-injury (NSSI)
; non-psychotic mental disorder
; suicidal ideation
; stress
; hypothalamic-pituitary-adrenal (HPA) axis
; cortisol
; adrenocorticotropic hormone (ACTH)
; brain-derived neurotrophic factor (BDNF)
; early adverse experience
1. Introduction
Non-suicidal self-injury (NSSI) is characterized by the intentional destruction of one’s own body tissue without suicidal intent and for purposes not socially sanctioned. NSSI typically begins in adolescence and the most common motives for self-harm are to reduce negative emotions, resolve interpersonal difficulties or induce positive feelings [1]. NSSI is believed to be a complex behavior that emerges through the intersecting effects of social, psychological and biological mechanisms. Recent studies have demonstrated the advantages of conceptualizing NSSI as a transnosological construct. For example, Wang and Eaton [2] found that transdiagnostic dimensions were superior to common DSM-IV and DSM-5 diagnoses in predicting NSSI, accounting for 33.6-38.7% of the variance in NSSI across the sample. These recent findings on NSSI are consistent with data on suicidal behavior, which may also exist across diagnostic boundaries, since suicide-related variables are more strongly associated with the shared variance of multiple mental disorders than with their unique disorder-specific variances [3,4].
Although the purpose of NSSI at the time of harm is, by definition, other than suicide, a history of NSSI has been shown to be an important risk factor for both future suicide attempts and completed suicides. These risks increase dramatically when NSSI is co-occurring with mental disorders. Notably, there is a bidirectional relationship between NSSI and mental disorders: the risk of developing non-psychotic mental disorders (NPMD) (personality disorders, bipolar disorder, eating disorders, etc.) is higher among those who have engaged in self-harm, and vice versa [5,6]. Some studies suggest that the comorbidity between depression and NSSI is very high and that depression is one of the most important clinical risk factors for the development of NSSI [7]. Depression and NSSI have been shown to have an interactive effect on suicide risk that is higher than either depression or NSSI alone [8]. Among several possible explanations for these data, it should be noted that patients with NSSI comorbid with depression tend to have poorer interpersonal and family relationships, more negative and stressful life events, a more frequent family history of mental illness, and a more severe clinical course [9,10].
Unfortunately, the lack of extensive knowledge about the biological mechanisms underlying NSSI hampers the prevention of suicide remaining one of the leading causes of death among adolescents and young adults worldwide [11,12,13,14,15]. A strong relationship was revealed between a corresponding pattern of the hypothalamic-pituitary-adrenal (HPA) axis dysregulation and chronic stress experiences [16], particularly those experiences that are regarded as an important risk factor for the development of NSSI [17].Long-lasting activation of HPA axis and the associated release of its executive hormone, cortisol, may be particularly critical during the sensitive period of adolescent development, when glucocorticoids can interfere with the development of brain structures critical for emotional control [18].Changes in the functioning of the hypothalamic-pituitary-adrenal (HPA) axis may be one of the biological mechanisms contributing to the development and maintenance of NSSI behavior [19,20].
Although a large number of previous studies have focused on different aspects of NSSI, the results are often controversial and it is difficult to draw definite conclusions concerning the biological mechanisms of NSSI. This could be explained by the heterogeneity of the study cohorts due to the use of different screening instruments for NSSI and the reliance on the categorical approach to mental disorders as presented in ICD-10 and the main sections of DSM-5. Given the high comorbidity of NSSI with different mental disorders, which in turn are comorbid with each other, we decided to include in our study patients with different NPMDs. Considering data from previous studies showing that most NPMDs, suicide attempts, and NSSI are more common in women than in men [21,22,23,24], we used data from women only in the current study. We focused on patients with NPMD and suicidal ideation because of the increased risk of suicide in this population, particularly among those who also engage in NSSI. Therefore, identifying variables, in particular associated with HPA axis, associated with NSSI in this high-risk population seems particularly important, since this could be a step forward in developing early diagnosis and personalized treatment approaches for this cohort.
The aim of the study was to assess the relationship between HPA axis indices and NSSI in female patients with NPMD and suicidal ideation.
2. Materials and Methods
2.1. Setting and Subjects
The study was conducted from September 2019 to October 2020. in the Moscow Research and Clinical Center for Neuropsychiatry, the largest clinic in Moscow specializing in the treatment of patients with non-psychotic mental disorders providing free services to permanent residents of Moscow, both by self-referral and by referral from a general practitioner.
All procedures in studies involving human subjects have been conducted in accordance with a set of ethical principles presented in the Seventh Revision of Declaration of WorldMedicalAssociation [25].The studies were conducted in accordance with local legislation and institutional requirements; protocol of the the study was approved by the Research Ethics Committee of the Moscow Research and Clinical Center for Neuropsychiatry (approval № 42, 19.08.2019).
Inclusion criteria were: diagnosis of a NPMD according to ICD-10 criteria, suicidal ideation, age 18 years or older, ability to give informed consent and comply with the study protocol. Exclusion criteria were: cognitive impairment (score less than or equal to 24 on the Mini-Mental State Examination (MMSE) [26], current psychotic disorder or lifetime diagnosis of primary psychotic disorder, alcohol and substance use disorders, severe comorbid somatic (e.g., diabetes mellitus, autoimmune or oncologic diseases) and neurologic disorders (e.g., Alzheimer’s and Parkinson’s diseases).
Patients received appropriate medication (treatment as usual) prescribed by a psychiatrist.
2.2. Procedure and instruments
According to the criteria described above, 40 female patients aged 18 years and older with NPMD, suicidal ideation, and NSSI were enrolled (cases—NSSI group). After the enrolment of cases was completed, we also enrolled controls (case-control ratio 1:1)—40 female patients of the same age as the case group participants with NPMD and suicidal ideation but without NSSI (controls—non-NSSI group).
All patients were seen by an experienced psychiatrist to confirm the diagnosis of NPMD and completed the MMSE. In addition, on the day of admission, all patients were interviewed about NSSI and suicidal behavior using relevant sections of the Russian version of Self-Injurious Thoughts and Behaviors Interview (SITBI) [23,27]. Socio-demographic and clinical data were collected using an ad hoc case report form. On the first three days, all participants completed the Russian versions of the following self-report instruments: the Beck Depression Inventory (BDI) [25], the State and Trait Anxiety Inventory (STAI) [29], the Brief Reasons for Living Inventory (bRFL) [30,31], and the brief form of the Personality Inventory for DSM-5 (PID-5-BF) [32] and the Child Abuse and Trauma Scale (CATS) [33].
In addition, 48 generally healthy women of similar age with no current or past history of mental disorders were enrolled as healthy controls (HC) for comparative assessment of average normal levels of biochemical parameters.
Informed consent was obtained from all participants enrolled in the study. Participants provided written informed consent prior to any procedure included in the study protocol.
2.3. Samples
Biochemical and hormonal parameters were measured in blood serum obtained from fasting morning venous blood. Samples were collected in Gel/Clotting activator S-Monovette tubes and centrifuged at 2000× g for 10 min at 8 ◦C on an Allegra X-30R Centrifuge (Beckman Coulter, Brea, CA, USA).
2.4. Assessment of Biochemical Indices and Hormones
Cortisol, thyroid stimulating hormone (TSH), prolactin, and testosterone levels were measured in blood serum by competitive enzyme immunoassay using appropriate kits (Beckman Coulter, USA) and an ACCESS® 2 immunoassay system (Beckman Coulter, USA). Adrenocorticotropic hormone (ACTH) was measured using enzyme immunoassay kits from Biomerica (Irvine, CA, USA). Brain-derived neurotrophic factor (BDNF) levels were determined by enzyme-linked immunosorbent assay (ELISA) in blood serum using appropriate Quantikine ELISA test systems (R&D Systems, Minneapolis, MN, USA). BDNF and ACTH levels were measured on an automated enzyme immunoassay analyzer (ChemWell 2910, Awareness Technologies Inc., Palm City, FL, USA). Routine biochemical parameters were determined in blood serum on an automated biochemical analyzer Beckman Coulter AU 680 (Beckman Coulter, Brea, CA, USA) using appropriate kits (Beckman Coulter, USA). Complete blood count with differential white blood cell count (CBC with diff) and hemogram were performed on an automated analyzer LH-500 (Beckman Coulter, USA).
2.5. Statistical analysis
Statistical analyses were performed using STATISTICA 10.0 (StatSoft Inc., Tulsa, OK, USA), GraphPad Prism version 9.4.1 (GraphPad Software, Inc., San Diego, CA, USA) and the R programming environment on the RStudio version 2023.06 platform. 2 (2009-2023, Posit Software, PBC) with the following libraries: ggplot2, ROCR, dplyr, tidyr, MASS, caret, margins. Normality of distributions was assessed using Shapiro-Wilk and Kolmogorov-Smirnov tests. Fisher’s exact test was used to compare qualitative data. To compare quantitative data between multiple unrelated groups, either the ANOVA test with post hoc analysis using Tukey’s test or the Kruskal-Wallis test with post hoc analysis using Dunn’s test was used, depending on the distribution. The Mann-Whitney test was used to compare two independent samples. Data in tables are presented as mean with SD, median with interquartile range or percentage. Differences were considered significant at p < 0.05. The backward logistic regression model was used with the significance level for each variable included set at 0.05. A logistic regression model included several independent (predictor) variables (nominal or continuous) that can be used to predict a dependent (outcome) binominal variable.
3. Results
3.1. Clinical characteristics of the patients
The cohort consisted of patients with the following current diagnoses: personality disorders (34%), depressive disorders (30%), bipolar affective disorders (15%), neurotic and stress-related disorders (13%), mental disorders caused by brain damage and dysfunction (7%). Almost 36% of patients had two or more co-occurring diagnoses, the most common being eating disorders (32%).
The patients in the two groups compared did not differ in age or socio-demographic characteristics. All patients had suicidal ideation and 38% of patients in each group had attempted suicide in their lifetime. In the NSSI group, almost a quarter of patients had a family history of self-harm (p<0.05). Both groups were similar in terms of psychiatric diagnoses, with the exception of a significantly lower proportion of patients with neurotic and stress-related disorders in the NSSI group as compared to participants without NSSI experience. Depression (BDI) and trait anxiety (STAI-t) scores were significantly higher in patients with NSSI (Table 1).
3.2. Biochemical characteristics of the patient and control groups
Hormone levels (cortisol, ACTH, prolactin, testosterone) in patients ofNSSI- and NSSI+ groups were significantly increased, whereas BDNF concentration, neutrophil/lymphocyte ratio and Hb levels were significantly decreased as compared to respective indices in healthy subjects (Table 2). As compared to patients without NSSI, those with NSSI had significantly higher ACTH levels and significantly lower BDNF levels (Table 2).
3.3. Distribution of clinical and biochemical parameters according to the importance of their influence on the development of NSSI in patients with NPMD
The regression model assessing the factors influencing the development of NSSI was constructed using the Russian version of the CATS subscales such as ‘physical and emotional abuse’, ‘sexual abuse’, ‘neglect and loneliness’, ‘negative home environment’ and ‘punishment’ as variables. The varImp function in the R programming environment was used to assess the importance of the variables in the regression model. The graph (Figure 1 a)shows that the factors ‘negative home environment’ and ‘physical and emotional abuse’ have the greatest impact on the accuracy of the regression model. Building a similar model using biochemical parameters, in particular ACTH, prolactin, TSH, testosterone, cortisol and BDNF selected as variables, demonstrated that levels of anterior pituitary hormones (ACTH, prolactin, TSH) were most important factors influencing NSSI (Figure 1b).
3.4. Model for predicting the probability of developing NSSI in patients with NPMD
The model was constructed using logistic regression. The BDI and STAI scale scores, each of the CATS subscale scores (physical and emotional abuse, sexual abuse, neglect and loneliness, negative home environment, punishment), hormone levels (ACTH, pg/ml; cortisol, nmol/L; TSH, Ulu/ml; prolactin, ng/ml; testosterone, nmol/L), BDNF, ng/ml concentration) as predictors (independent variables) were used to build the model.
The coefficient values in the summary table of the model showed that only variables such as ACTH level and CATS subscale ‘negative home environment’ had a statistically significant effect on the occurrence of NSSI development in patients with NPMD and suicidal ideation. The McFadden’s pseudo-R-square used for this model was 0.55. This indicates that the model fits the data well and has a good predictive power. The dependence of the probability of developing NSSI on the levels of the predictors is shown in Figure 2 (ACTH level, a; CATS “‘negative home environment” subscale scores, b).
According to this model, an increase in ACTH of 10 pg/ml augments the odds of NSSI in patients by a factor of 11, and an increase in the CATS “‘negative home environment” subscale by 1 unit raises the odds of NSSI in patients by a factor of 6.4 (Table 3).
In accordance with the classification table, using tested data from 25 patients (31% of the total cohort), the sensitivity of the model was 94% and the specificity was 100%. The accuracy of the selected model with a cut-off of 0.5 for binary classification was 96%, the area under the curve was 0.9. These data indicate a good performance of the model selected.
4. Discussion
The aim of the current study was to assess HPA axis parameters associated with NSSI in female patients with NPMD. The cohort consisted of 34% patients with personality disorders, 30% with depressive disorders, 15% with bipolar disorder, and 15% with other neurotic and stress-related disorders. Patients with NSSI had significantly higher levels of trait anxiety and higher scores on the Beck Depression Scale. In this group of patients, the percentage of women with a family history of NSSI was five times higher than in patients without NSSI, which may indicate a predisposition to NSSI [34,35].
The biochemical results obtained suggest that the levels of stress hormones (ACTH, cortisol) were significantly elevated in patients of both NPMD groups, while the concentration of BDNF and the neutrophil/lymphocyte ratio were significantly reduced as compared to the corresponding parameters of healthy individuals. These data are consistent with most of the available literature and generally confirm that the HPA axis, the neurotrophic factor system, and cell-mediated inflammation are involved in the pathophysiology of patients with NPMD.The HPA axis is a major neuroendocrine system that controls responses to stress and several other major bodily processes, including digestion, immunity, mood and emotion, sexuality, and energy storage and expenditure. It is well known that HPA axis with cortisol as its main output, orchestrate the development of psychopathologies [36]. Previous studies examining associations between NSSI and the HPA axis in patients with major depressive disorder (MDD) have found an altered pattern of HPA axis regulation [37,38]. Most importantly, the data showed that depressed individuals with NSSI had the lowest levels of salivary cortisol in response to the Trier Social Stress Test accompanied by the highest ratings of observed stress as compared to patients with depression and healthy persons [39]. In the current study, no significant difference in cortisol levels was found between the group of patients with NSSI and those without NSSI, possibly due to increased cortisol production in both groups. Notably, cortisol levels were slightly higher in patients with NSSI, but did not reach the level of significance though showing a statistical trend (p=0.06).
An important result of this study is revealing significantly higher ACTH levels and significantly lower BDNF levels in patients with NSSI as compared to those without NSSI. This may indicate a more pronounced HPA axis dysregulation potentially leading to subsequent damage to sensitive brain structures, including the hippocampus, and more prominent disturbances in neuroplasticity in patients with NSSI. Previously, HPA axis disturbances have been shown to affect memory function in patients with MDD, post-traumatic stress disorder, and borderline personality disorder [40]. In addition, mental health disorders, including NSSI, depression, anxiety, and post-traumatic stress disorder, are known to be associated with HPA axis and prefrontal cortex dysfunction, suggesting a functional link between aberrant prefrontal corticosteroid signaling, stress adaptation, emotional control, mood regulation, and pathways mediating stress -induced psychopathology [41]. The difference in both ACTH and BDNF levels found in our study between patients with and without NSSI seems to be important and may be the basis for further research on the mechanisms underlying comorbidity of mental disorders and NSSI.
The distribution of biochemical parameters of the patients according to their importance for NSSI suggests that the anterior pituitary hormones (ACTH, prolactin, TSH) may be tightly involved in its development (Figure 1b), with ACTH playing the leading role. Previously, it was shown that the level of prolactin, vulnerable to the influence of different stressors, has a regulatory effect on the adrenal glands, acting as a synergist of ACTH, and, accordingly, modifying the stress response [42]. These findings suggest that the development of NSSI in patients with NPMD may be associated with HPA axis dysregulation at the pituitary level. The pituitary gland is known to play an integral role in mediating stress response through its involvement in HPA axis function. The pituitary gland is under the influence of hypothalamic corticotropin-releasing hormone and secretes ACTH acting in a feedback loop to propagate the stress response; thus pituitary may be a region critically affected by failure in stress control. Some studies suggest that pituitary gland volume (PGV) is altered in individuals with stress-related psychopathology which may be associated with age-related changes in PGV during adolescence [43,44]. A recent study examining pituitary PGV by magnetic resonance imaging in adolescents with NSSI as compared to age-matched healthy controls provided preliminary evidence of alterations in pituitary maturation in adolescents engaged in NSSI [45].
All patients enrolled in our study had suicidal ideation. It was found that the age of onset of suicidal ideation in the group of patients without NSSI was 18.0 (13.8; 22.0) years, while in patients with NSSI it was 14.0 (13.0; 16.3) years, and the age of onset of NSSI was 14.5 (13.0;18.0) years; this means that the onset of the disease in patients with NSSI occurred during adolescence. The association between NSSI, adolescence and female gender is consistent with the importance of the role played by biological hormonal components, particularly pituitary hormones. Adolescence is a transitional period, defined as the period between the onset of puberty and the beginning of independence, and is characterized by continued structural maturation of the brain and hormonal changes that begin at puberty. [46]. This period coincides with the onset of HPA axis reactivity to psychological stress, sex differences and the behavioral expression of negative emotions in response to stressful situations [47].Stress-responsive regions of the brain, such as the fronto-cortical and limbic areas, are still maturing during adolescence [48]. Stress responses emerging during this period of life are accompanied by close interactions between stress hormones, the increase in HPA axis responsiveness and the gonadal hormonal axes [49]. Brain structures mediating emotions and cognitive functions, particularly the hippocampus, are known to be most vulnerable to changes in HPA axis activity associated with early stress experiences [50,51].
In the current study, we examined the effects of a number of different types of early life stressors (i.e., childhood and adolescence), including physical and emotional abuse, sexual abuse, neglect and loneliness, negative home environment, and punishment, on the development of NSSI in female patients with NPMD. It was found that the factors ‘negative home environment’ and ‘physical and emotional abuse’ had the greater impact on the development of NSSI (Figure 1a). The most important factor increasing the likelihood of developing NSSI in such patients was an adverse family environment, according to data from the CATS subscale ‘negative home environment’ (Figure 2b). This subscale includes statements about family relationships: abuse, violence, feelings of unhappiness, alcoholism/drug addiction in the family, feelings of security in the family, the ability to freely invite someone to home, and a question about the general feeling of having had a difficult childhood. It can be assumed that people whose mental disorder was exacerbated by NSSI had previously experienced prolonged exposure to stress. Simultaneously, most of them had a family history of NSSI. A number of studies suggest that during sensitive periods in genetically predisposed individuals, prolonged exposure to stress may have a greater impact on the developmental trajectory of brain structures as compared with potentially stronger but shorter-term stressors [19].
The results obtained in the current study using the logistic regression method indicate that the likelihood of developing NSSI in patients with NPMD is associated with early adverse family experiences and elevated ACTH levels (Figure 2, Table 3). More than half of the studies mentioned that child maltreatment, especially emotional abuse and emotional neglect, may contribute to the development of NSSI in patients with mental disorders [51,52,53,54,55]. It has been suggested that exposure to psycho-emotional trauma in childhood and adolescence may trigger psychiatric disorders by altering the function of the HPA axis [56,57]. Previous research has also found links between early life stress and changes in PGV growth during adolescence [58,59].
Developmental plasticity is usually maximal during immature stages of development, and the neuroendocrine stress system might be expected to be most vulnerable to chronic stress [60].The negative effects of chronic stress are likely to be mostly due to its prolonged duration, overriding the highly dynamic regulation critical for optimal HPA axis function. Some studies have also shown that chronic stress is associated with hyperactivation of HPA axis [61]. Glucocorticoids, executive hormones of HPA axis ensure the coordinated functioning of key components and mechanisms of brain plasticity at different levels, including neurogenesis, glutamatergic neurotransmission, microglia and astrocytes, systems of neurotrophic factors, neuroinflammation, etc. [62]. Adaptation to chronic hyperactivation of the HPA axis may lead to loss of the system sensitivity through chronic activation of negative feedback and feed-forward regulators. The results of some studies have shown a reciprocal relationship between chronic emotional stress and engagement in NSSI [63]. It has been suggested that chronic stress in adolescence promotes the development of atypical regulation of the HPA axis, leading to increased emotional vulnerability in adulthood.
Our study showed that the likelihood of developing NSSI in female patients with NPMD was increased by elevated levels of ACTH, one of the main players in HPA axis activity, and by early adverse family environment, which may indirectly indicate the presence of chronic stress during immature stages of development. The results suggest that chronic stress during adolescence in some people with NPMD may alter the neuro-architecture in brain regions that regulate the HPA axis, affecting the trajectory of brain development and exacerbating patterns of emotional and cognitive behavior.
5. Limitations
The main limitations of this study are the rather small cohort of patients enrolled and the lack of comparison with male patients.
Author Contributions
Conceptualization, M.S.Z. and N.V.G.; methodology M.S.Z. and T.A.D.; software, M.Y.Z.; validation, T.A.D.; formal analysis, M.Y.Z.; S.B.P. and T.A.D.; investigation, S.B.P. and T.A.D.; resources, A.B.G.; data curation, T.A.D.; writing—original draft preparation, M.S.Z. and T.A.D.; writing—review and editing, N.V.G.; visualization, M.Y.Z.; supervision, A.B.G. and N.V.G.; project administration, M.S.Z. and T.A.D.; funding acquisition, M.S.Z. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by grant from the Moscow Center for Healthcare Innovations [Grant No. 2412-36/22].
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Moscow Research and Clinical Centre for Neuropsychiatry (protocol #42, 19.08.2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data generated in the present study are available upon a reasonable request.
Acknowledgments
The open access publication costs were covered by the Moscow Center for Healthcare Innovations.
Conflicts of Interest
The authors declare no conflict of interest.
Abbrevations
ACTH, adrenocorticotropic hormone; BDI, the Beck Depression Inventory; BDNF, brain-derived neurotrophic factor; bRFL, Brief Reasons for Living Inventory; CATS, the Child Abuse and Trauma Scale; DSM, The Diagnostic and Statistical Manual of Mental Disorders; HC, healthy controls; HPA axis, hypothalamic-pituitary-adrenal axis;ICD-10,International Classification of Diseases 10th Revision; NPMD, non-psychotic mental disorders; NSSI, nonsuicidal self-injury; PID-5-BF, the brief form of the Personality Inventory for DSM-5; PGV, pituitary gland volume; SITBI, Self-Injurious Thoughts and Behaviors Interview; STAI, the State and Trait Anxiety Inventory; TSH, thyroid stimulating hormone.
References
- Diagnostic And Statistical Manual Of Mental Disorders, Fifth Edition. American Psychiatric Association Publishing. [CrossRef]
- Wang, M.; Eaton, N.R. Linking non-suicidal self-injury to psychopathology: The utility of transdiagnostic and DSM-based models. J. Affect. Disord. 2023, 332, 55-63. [CrossRef]
- Eaton, N.R.; Krueger, R.F.; Markon, K.E.; Keyes, K.M.; Skodol, A.E.; Wall, M.; Hasin, D.S.; Grant, B.F. The structure and predictive validity of the internalizing disorders. J. Abnorm. Psychol. 2013, 122, 86-92. [CrossRef]
- Karnick, A.T.; Fergerson, A.K.; Caulfield, N.M.; Buerke, M.; Albanese, B.J.; Schmidt, N.B.; Capron, D.W. Toward an integrative model of transdiagnostic risk factors and suicide: A network comparison of psychiatric outpatients. J. Psychiatr. Res. 2022, 154,252-260. [CrossRef]
- Nitkowski, D.; Petermann, F. Selbstverletzendes Verhalten und komorbide psychische Störungen: ein Überblick [Non-suicidal self-injury and comorbid mental disorders: a review]. Fortschr. Neurol. Psychiatr.2011,79, 9-20. [CrossRef]
- Kiekens, G.; Claes, L.; Hasking, P.; Mortier, P.; Bootsma, E.; Boyes, M.; Myin-Germeys, I.; Demyttenaere, K.; Cuijpers, P.; Kessler, R.C.; Nock, M.K.; Bruffaerts, R. A longitudinal investigation of non-suicidal self-injury persistence patterns, risk factors, and clinical outcomes during the college period. Psychol. Med.2023,53, 6011-6026. [CrossRef]
- Kang, L.; Li, R.; Liu, H.; Ma, S.; Sun, S.; Zhang, N.; Yao, L.; Wang, Y.; Zong, X.; Ai, C.; Zou, Z.; Yang, B.X.; Bai, H.; Liu, Z. Nonsuicidal self-injury in undergraduate students with major depressive disorder: The role of psychosocial factors. J. Affect. Disord. 2021, 290, 102-108. [CrossRef]
- Groschwitz, R.C.; Kaess, M.; Fischer, G.; Ameis, N.; Schulze, U.M.; Brunner, R.; Koelch, M.; Plener, P.L. The association of non-suicidal self-injury and suicidal behavior according to DSM-5 in adolescent psychiatric inpatients. Psychiatry Res. 2015, 228, 454-461. [CrossRef]
- Shao, C.; Wang, X.; Ma, Q.; Zhao, Y.; Yun, X. Analysis of risk factors of non-suicidal self-harm behavior in adolescents with depression. Ann. Palliat. Med. 2021, 10, 9607-9613. [CrossRef]
- Taş Torun, Y., Gul, H.; Yaylali, F.H.; Gul, A. Intra/interpersonal Functions of Non-suicidal Self-injury in Adolescents with Major Depressive Disorder: The Role of Emotion Regulation, Alexithymia, and Childhood Traumas. Psychiatry2022, 85, 86-99. [CrossRef]
- Kiekens, G.; Hasking, P.; Boyes, M.; Claes, L.; Mortier, P.; Auerbach, R.P.; Cuijpers, P.; Demyttenaere, K.; Green, J.G.; Kessler, R.C.; Myin-Germeys, I.; Nock, M.K.; Bruffaerts, R. The associations between non-suicidal self-injury and first onset suicidal thoughts and behaviors. J. Affect. Disord. 2018, 239, 171-179. [CrossRef]
- Koenig, J., Brunner, R., Fischer-Waldschmidt, G., Parzer, P., Plener, P.L., Park, J., Wasserman, C., Carli, V., Hoven, C.W., Sarchiapone, M., Wasserman, D., Resch, F., Kaess, M. Prospective risk for suicidal thoughts and behaviour in adolescents with onset, maintenance or cessation of direct self-injurious behaviour. Eur. Child. Adolesc. Psychiatry2017, 26, 345-354. [CrossRef]
- Hamza, C.A.; Stewart, S.L.; Willoughby, T. Examining the link between nonsuicidal self-injury and suicidal behavior: a review of the literature and an integrated model. Clin. Psychol. Rev. 2012, 32, 482-495. [CrossRef]
- Ribeiro, J.D., Franklin, J.C., Fox, K.R., Bentley, K.H., Kleiman, E.M., Chang, B.P., Nock, M.K. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: a meta-analysis of longitudinal studies. Psychol. Med.2016, 46, 225-236. [CrossRef]
- Bryan, C.J., Rudd, M.D., Wertenberger, E., Young-McCaughon, S., Peterson, A. Nonsuicidal self-injury as a prospective predictor of suicide attempts in a clinical sample of military personnel. Compr. Psychiatry2015, 59:1-7. [CrossRef]
- Miller, G.E., Chen, E., Zhou, E.S. If it goes up, must it come down? Chronic stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychol. Bull.2007, 133, 25-45. [CrossRef]
- Reichl, C., Heyer, A., Brunner, R., Parzer, P., Völker, J.M., Resch, F., Kaess, M. Hypothalamic-pituitary-adrenal axis, childhood adversity and adolescent nonsuicidal self-injury. Psychoneuroendocrinology2016, 74, 203-211. [CrossRef]
- Lupien, S.J., McEwen, B.S., Gunnar, M.R., Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci.2009, 10, 434-445. [CrossRef]
- Kaess, M., Hooley, J.M., Klimes-Dougan, B., Koenig, J., Plener, P.L., Reichl, C., Robinson, K., Schmahl, C., Sicorello, M., Westlund Schreiner, M., Cullen, K.R. Advancing a temporal framework for understanding the biology of nonsuicidal self- injury: An expert review. Neurosci. Biobehav. Rev.2021, 130, 228-239. [CrossRef]
- Klimes-Dougan, B.; Begnel, E.; Almy, B.; Thai, M.; Schreiner, M.W.; Cullen, K.R. Hypothalamic-pituitary-adrenal axis dysregulation in depressed adolescents with non-suicidal self-injury. Psychoneuroendocrinology2019, 102, 216-224. [CrossRef]
- Bresin, K.; Schoenleber, M. Gender differences in the prevalence of nonsuicidal self-injury: A meta-analysis. Clin. Psychol. Rev.2015, 38, 55-64. [CrossRef]
- Gutiérrez-Rojas L.; Porras-Segovia A.; Dunne H.; Andrade-González N.; Cervilla J.A. Prevalence and correlates of major depressive disorder: a systematic review. Braz. J. Psychiatry2020, 42, 657-672. [CrossRef]
- Zinchuk, M.; Beghi, M.; Beghi, E.; Bianchi, E.; Avedisova, A.; Yakovlev, A.; Guekht, A. Non-Suicidal Self-Injury in Russian Patients with Suicidal Ideation. Arch. Suicide Res.2022, 26, 776-800. [CrossRef]
- The global health observatory. Suicide rates. https://www.who.int/data/gho/data/themes/mental-health/suicide-rates.
- World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J.A.M.A. 2013, 310, 2191-2194. [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res.1975, 12, 189-198. [CrossRef]
- Nock, M.K.; Holmberg, E.B.; Photos, V.I.; Michel, B.D. Self-Injurious Thoughts and Behaviors Interview: development, reliability, and validity in an adolescent sample. Psychol. Assess.2007, 19, 309-317. [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory, 2nd ed.; (BDI-II); Psychological Corporation: San Antonio, TX, USA, 1996.
- Spielberger, C. D.; Gorsuch, R. L.; Lushene, R.; Vagg, P. R.; Jacobs, G. A. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press.1983.
- Ivanoff, A.; Jang, S.J.; Smyth, N.J.;Linehan,M. M. Fewer reasons for staying alive when you are thinking of killing yourself: The brief reasons for living inventory. J. Psychopathol. Behav. Assess.1994, 16, 1–13. [CrossRef]
- Kustov, G.V.; Zinchuk, M.S.; Gersamija, A.G.; Voinova, N.I.; Yakovlev, A.A.; Avedisova, A.S.; Guekht, A.B. Psychometric properties of the Russian version of the brief «Reasons for Living Inventory». Zh. Nevrol. Psikhiatr. Im. S. S. Korsakova2021, 121, 87-94. [CrossRef]
- The Personality Inventory for DSM-5—Brief Form (PID-5-BF)—Adult https://www.psychiatry.org/getmedia/f65c4386-b2bc-44a5-9ace-d6fea2211506/APA-DSM5TR-ThePersonalityInventoryForDSM5BriefFormAdult.pdf.
- Sanders, B.; Becker-Lausen, E. The measurement of psychological maltreatment: early data on the Child Abuse and Trauma Scale. Child Abuse Negl.1995, 19, 315-323. [CrossRef]
- Maciejewski, DF, Creemers, HE, Lynskey, MT, Madden, PA, Heath, AC, Statham, DJ, Martin, NG, Verweij, KJ. Overlapping genetic and environmental influences on nonsuicidal self-injury and suicidal ideation: different outcomes, same etiology? J.A.M.A. Psychiatry2014, 71, 699-705. [CrossRef]
- James, K. M.; Brandon, E. G. The Parent-Child Dyad and Other Family Factors Associated with Youth Nonsuicidal Self-Injury.The Oxford Handbook of Nonsuicidal Self-Injury, Lloyd-Richardson, E.E.; Baetens E.I; Whitlock J.L. (eds). 2023. [CrossRef]
- Nederhof, E.; van Oort, F.V.; Bouma, E.M.; Laceulle, O.M.; Oldehinkel, A.J.; Ormel, J. Predicting mental disorders from hypothalamic-pituitary-adrenal axis functioning: a 3-year follow-up in the TRAILS study. Psychol. Med. 2015, 45, 2403-2412. [CrossRef]
- Wu, B.; Zhang, H.; Chen, G.; Chen, G.; Liu, Z.; Cheng, Y.; Yuan, N.; Peng, D. Potential mechanisms of non-suicidal self-injury (NSSI) in major depressive disorder: a systematic review. 2023, General Psychiatry 36, e100946. [CrossRef]
- Braquehais, M.D.; Picouto, M.D.; Casas, M.; Sher, L. Hypothalamic-pituitary-adrenal axis dysfunction as a neurobiological correlate of emotion dysregulation in adolescent suicide. World J. Pediatr. 2012, 8, 197-206. [CrossRef]
- Klimes-Dougan, B.; Begnel, E.; Almy, B.; Thai, M.; Schreiner, M.W.; Cullen, K.R. Hypothalamic-pituitary-adrenal axis dysregulation in depressed adolescents with non-suicidal self-injury. Psychoneuroendocrinology2019, 102, 216-224. [CrossRef]
- Wingenfeld, K.; Wolf, O.T. HPA axis alterations in mental disorders: impact on memory and its relevance for therapeutic interventions. C.N.S. Neurosci. Ther.2011, 17, 714-722. [CrossRef]
- McKlveen, J.M.; Myers, B.; Flak, J.N.; Bundzikova, J.; Solomon, M.B.; Seroogy, K.B.; Herman, J.P. Role of prefrontal cortex glucocorticoid receptors in stress and emotion. Biol. Psychiatry2013, 74, 672-679. [CrossRef]
- Lalli, E., Figueiredo, B.C. Prolactin as an adrenocorticotropic hormone: Prolactin signalling is a conserved key regulator of sexually dimorphic adrenal gland function in health and disease. Bioessays2022, 44, e2200109. [CrossRef]
- Garner, B., Pariante, C.M., Wood, S.J., Velakoulis, D., Phillips, L., Soulsby, B., Brewer, W.J., Smith, D.J., Dazzan, P., Berger, G.E., Yung, A.R., van den Buuse, M., Murray, R., McGorry, P.D., Pantelis, C. Pituitary volume predicts future transition to psychosis in individuals at ultra-high risk of developing psychosis. Biol. Psychiatry2005, 58, 417-423. [CrossRef]
- Ganella, D.E., Allen, N.B., Simmons, J.G., Schwartz, O., Kim, J.H., Sheeber, L., Whittle, S. Early life stress alters pituitary growth during adolescence-a longitudinal study. Psychoneuroendocrinology2015, 53, 185-194. [CrossRef]
- Schär, S., Mürner-Lavanchy, I., Slavova, N., Lerch, S., Reichl, C., Brunner, R., Koenig, J., Kaess, M. Pituitary volume in adolescents with non-suicidal self-injury: Preliminary evidence for alterations in pituitary maturation. Psychoneuroendocrinology2022, 138, 105662. [CrossRef]
- Dorn, L.D. Measuring puberty. J. Adolesc. Health2006, 39, 625-626. [CrossRef]
- Ordaz, S, Luna, B. Sex differences in physiological reactivity to acute psychosocial stress in adolescence. Psychoneuroendocrinology2012, 37, 1135-1157. [CrossRef]
- Morrison, K.E., Rodgers, A.B., Morgan, C.P., Bale, T.L. Epigenetic mechanisms in pubertal brain maturation. Neuroscience2014, 264, 17-24. [CrossRef]
- Handa, R.J., Weiser, M.J. Gonadal steroid hormones and the hypothalamo-pituitary- adrenal axis. Front. Neuroendocrinol.2014, 35, 197-220. [CrossRef]
- Teicher, M.H., Samson, J.A. Annual Research Review: Enduring neurobiologicaleffects of childhood abuse and neglect. J. Child. Psychol. Psychiatry2016, 57, 241-266. [CrossRef]
- Liu, R.T., Scopelliti, K.M., Pittman, S.K., Zamora, A.S. Childhood maltreatment and non-suicidal self-injury: a systematic review and meta-analysis. Lancet Psychiatry2018, 5, 51-64. [CrossRef]
- Brown, R.C., Heines, S., Witt, A., Braehler, E., Fegert, J.M., Harsch, D., Plener, P.L. The impact of child maltreatment on non-suicidal self-injury: data from a representative sample of the general population. BMC Psychiatry2018, 18, 181. [CrossRef]
- Franzke, I., Wabnitz, P., Catani, C. Dissociation as a mediator of the relationship between childhood trauma and nonsuicidal self-injury in females: a path analytic approach. J. Trauma Dissociation2015, 16, 286-302. [CrossRef]
- Chen, Y.; Zhao, X.; Liu, X.; Wu, D.; Zhan, S.; Liu, S.; Yin, H. Childhood maltreatment and non-suicidal self-injury among Chinese adolescents: a moderated mediation model of psychological suzhi and inferiority complex. Curr Psychol.2023. [CrossRef]
- Titelius, E.N.; Cook, E.; Spas J.; Orchowski, L.; Kivisto, K.; O’Brien, K.H.M.; Frazier, E.; Wolff, J.C.; Dickstein, D.P.; Kim, K.L., Seymour, K. Emotion Dysregulation Mediates the Relationship Between Child Maltreatment and Non-Suicidal Self-Injury. J. Aggress. Maltreat. Trauma2018, 27, 323-331. [CrossRef]
- Kuhlman, K.R.; Chiang, J.J.; Horn, S.; Bower, J.E. Developmental psychoneuroendocrine and psychoneuroimmune pathways from childhood adversity to disease. Neurosci. Biobehav. Rev. 2017, 80, 166-184. [CrossRef]
- Gu, W.; Zhao, Q.; Yuan, C.; Yi, Z.; Zhao, M.; Wang, Z. Impact of adverse childhood experiences on the symptom severity of different mental disorders: a cross- diagnostic study. Gen. Psychiatry2022, 35, e100741. [CrossRef]
- Carballedo, A., Lisiecka, D., Fagan, A., Saleh, K., Ferguson, Y., Connolly, G., Meaney, J., Frodl, T. Early life adversity is associated with brain changes in subjects at family risk for depression. World J. Biol. Psychiatry2012, 13, 569-578. [CrossRef]
- Farrow, P.; Simmons, J.G.; Pozzi, E.; Díaz-Arteche, C.; Richmond, S.; Bray, K.; Schwartz, O.; Whittle, S. Associations between early life stress and anterior pituitary gland volume development during late childhood. Psychoneuroendocrinology. 2020, 122. [CrossRef]
- Coffman, J. A. Chronic stress, physiological adaptation and developmental programming of the neuroendocrine stress system. Future Neurol. 2023, 15. [CrossRef]
- Stalder, T., Steudte-Schmiedgen, S., Alexander, N., Klucken, T., Vater, A., Wichmann, S., Kirschbaum, C., Miller, R. Stress-related and basic determinants of hair cortisol in humans: A meta-analysis. Psychoneuroendocrinology.2017, 77, 261-274. [CrossRef]
- Gulyaeva, N.V. Glucocorticoids Orchestrate Adult Hippocampal Plasticity: Growth Points and Translational Aspects. Biochemistry (Mosc).2023, 88, 565-589. [CrossRef]
- Miller, A.B.; Linthicum, K.P.; Helms, S.W.; Giletta, M.; Rudolph, K.D.; Hastings, P.D.; Nock, M.K.; Prinstein, M.J. Reciprocal Associations Between Adolescent Girls’ Chronic Interpersonal Stress and Nonsuicidal Self-Injury: A Multi-wave Prospective Investigation. J. Adolesc. Health. 2018, 63, 694-700. [CrossRef]
Figure 1.
Level of importance for factors influencing NSSI according to the CATS scale (a) and biochemical indices (b).
Figure 1.
Level of importance for factors influencing NSSI according to the CATS scale (a) and biochemical indices (b).
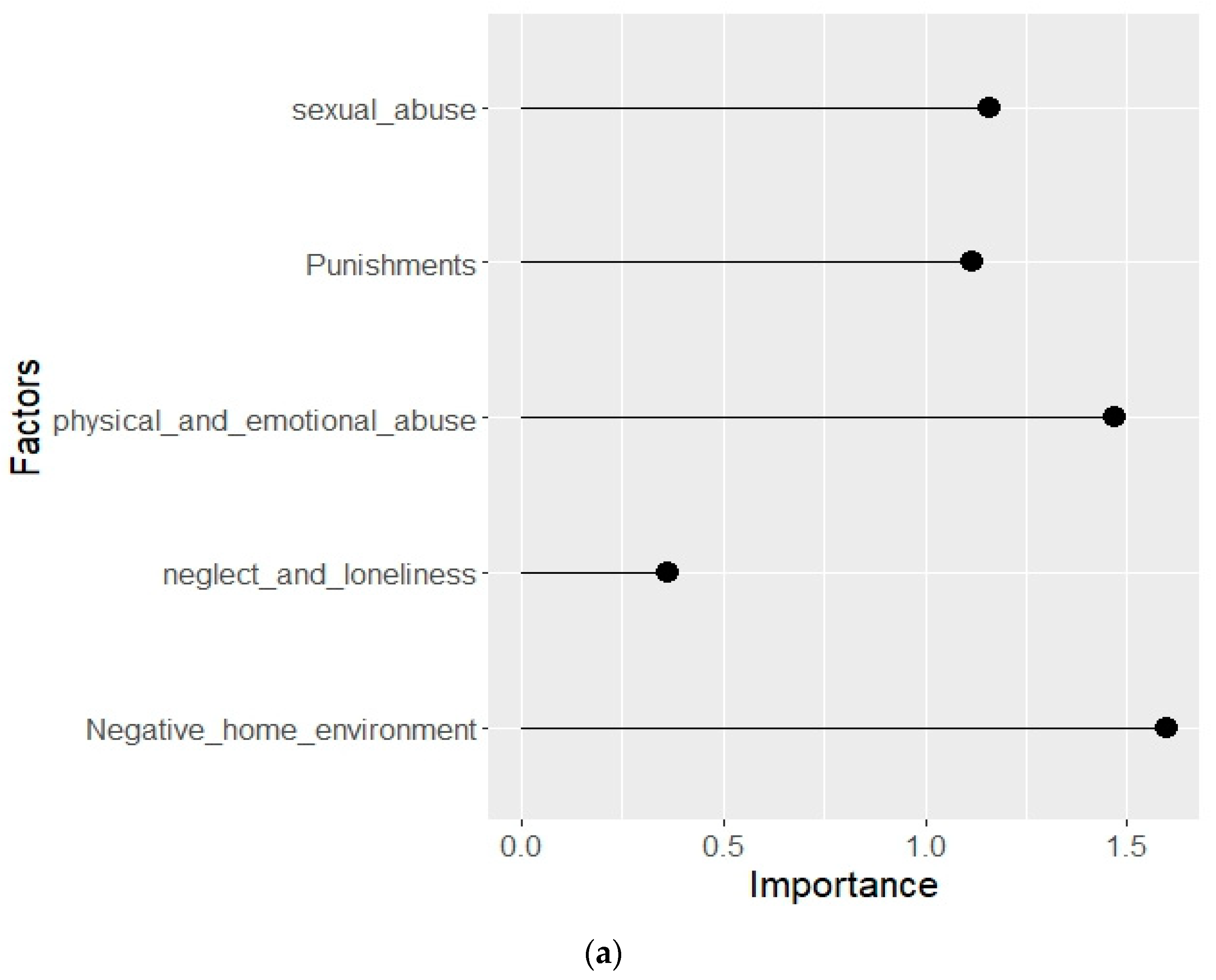
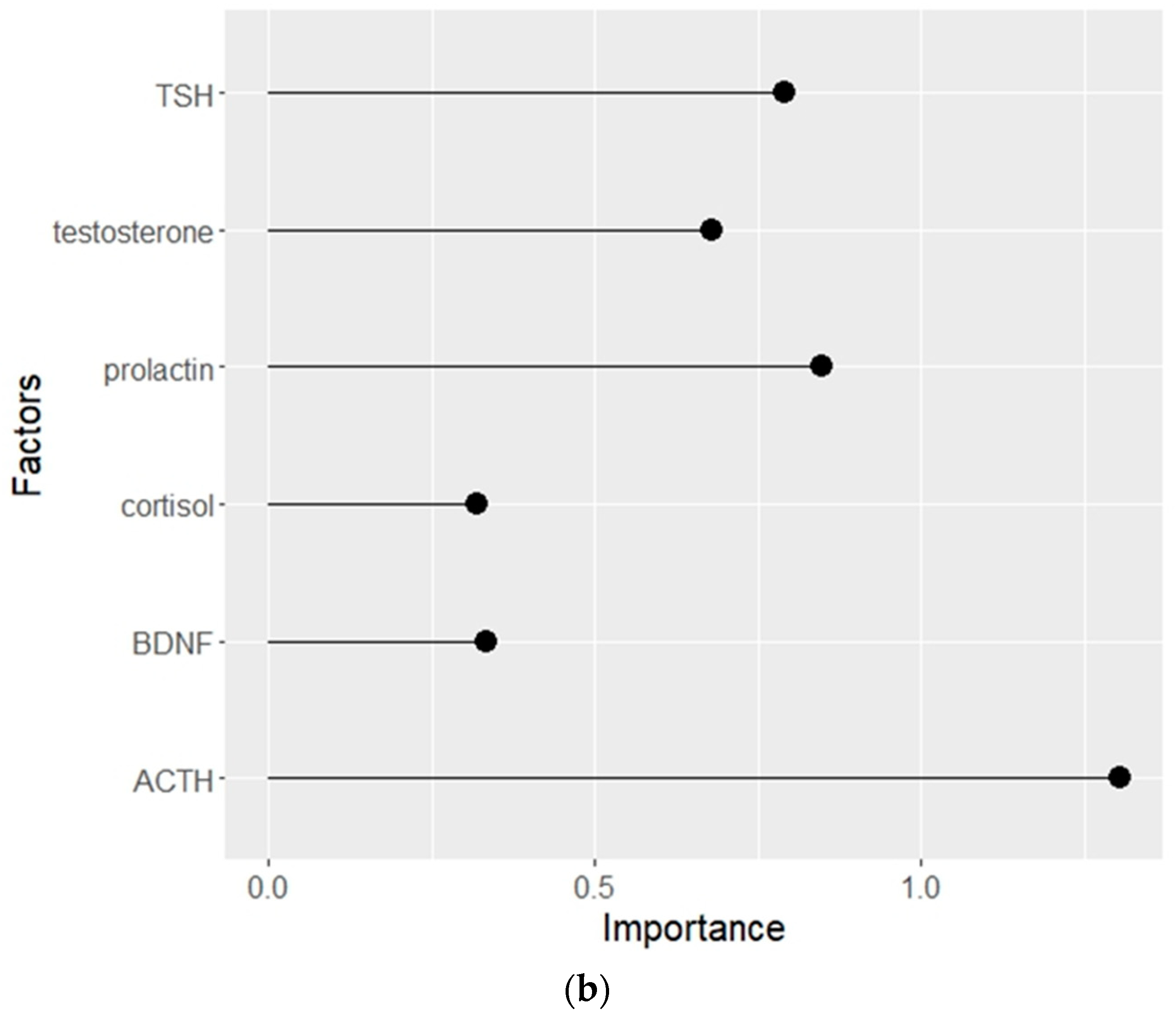
Figure 2.
Dependency of the probability of developing NSSI on ACTH level (a) and on CATS “negative home environment” subscale score (b).A grey area along the blue line indicates a 95% confidence interval.
Figure 2.
Dependency of the probability of developing NSSI on ACTH level (a) and on CATS “negative home environment” subscale score (b).A grey area along the blue line indicates a 95% confidence interval.
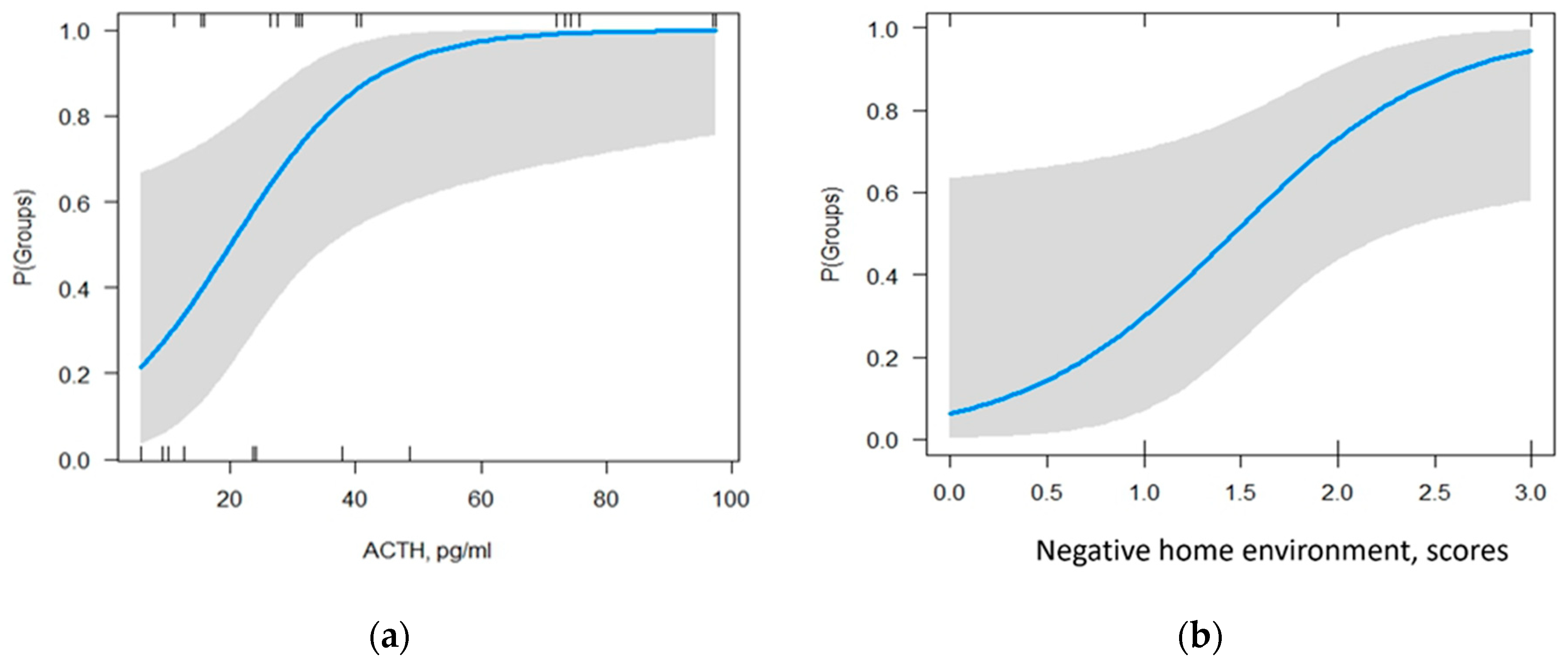

Table 1.
Sociodemographic and clinical characteristics of patients with and without NSSI.
| Parameter/Group | NSSI- | NSSI+ |
|---|---|---|
| Socio-demographic data | ||
| Age (years) | 27.5(22.0;32.0) | 27.5(22.0;31.8) |
| Education (secondary/incomplete higher; higher), % | 35/65 | 28/72 |
| Employed (-/+), % | 52/48 | 50/50 |
| Marital status (single/coupled), % | 55/45 | 50/50 |
| Parent’s family structure (incomplete/complete), % | 50/50 | 45/55 |
| Current diagnosis | ||
| Bipolar affective disorders (F31), % | 12 | 18 |
| Depressive disorders (F32/33), % | 30 | 30 |
| Neurotic and stress-related disorders (F40/41/43/44/45), % | 20 | 5∗ |
| Personality disorders(F60/61), % | 31 | 37 |
| Eating disorders, % | 23 | 40 |
| Mental disorders caused by brain damage and dysfunction (F06/07), % | 5 | 8 |
| Diagnosed with 2 or more mental disorders, % | 28 | 45 |
| Clinical characteristics | ||
| Family history of mental health disorders, % | 65 | 68 |
| Family history of suicidality, % | 20 | 38 |
| Family history of NSSI, % | 5 | 23* |
| History of physical abuse, % | 65 | 83 |
| History of bullying at school, % | 65 | 80 |
| Lifetime suicide attempts, % | 38 | 38 |
| Current smoking (nicotine products), %. | 56 | 55 |
| Age at first contact with mental health services, years | 22.5 (18.5;30) | 22.0 (18.0;28.0) |
| Age of onset of suicidal ideation, years old | 18.0 (13.8;22.0) | 14. 0 (13.0;16.3) |
| Age of onset of NSSI, years old | - | 14.5 (13.0;18.0) |
| Psychological scales data | ||
| BDI, scores | 27.8±9.4 | 31.1±9.1∗ |
| STAI (State Anxiety), scores | 60.2±9.9 | 63.8±9.6 |
| STAI (Trait anxiety), scores | 59.0±8.4 | 62.8±8.6∗ |
| bRFL (total), scores | 34.4±11.7 | 39.7±15.3 |
| PID-5-BF (total), scores | 34,8±9.2 | 32.4±11.4 |
| CATS (total), scores | 7.4±3.2 | 9.0±3.4 |
Data are presented as: mean with SD, median with interquartile range, percentages. Fisher’s exact test was used to compare qualitative data. To compare quantitative data between unrelated groups, either unpaired t-test or Mann-Whitney test was used, depending on the distribution. *p<0.05.
Table 2.
Laboratory data of patients and control group.
| Parameter/Group | HC n=48 |
NSSI- n=40 |
NSSI+ n=40 |
|---|---|---|---|
| age | 25.0 (23.0;27.0) | 27.5 (22.0;32.0) | 27.5 (22.0;31.8) |
| TSH3, ulU/mL | 1.7 (1.2;2.3) | 1.7 (1.3;2.1) | 1.9 (1.5;2.7) |
| ACTH, pg/mL | 15.8 (9.7;22.2) | 24.3 (16.0;57.0)*** | 37.4 (26.7;56.8)* |
| Testosterone, nmol/L | 1.4 (1.0;2.1) | 2.5 (1.6;2.9)* | 2.1 (1.5;2.7)* |
| Prolactin, ng/mL | 11.9 (8.2;15.9) | 20.9 (14.8;34.3)* | 19.7 (13.1;36.1)* |
| Cortisol, nmol/L | 265.9 (192.5; 378.8) | 447.6 (381.5;558.7)* | 533.7 (427.1; 600.9)* |
| BDNF, ng/ml | 25.5±5.5 | 22.1±6.0*** | 18.8±5.7* |
| While blood cell, WBC, 103µL | 6.3±1.6 | 6.5±1.5 | 6.0±1.5 |
| Neutrophils, NEI, %/ NEI, 103µL |
56.8±10.8/3.6±1.3 | 50.4±11.3/3.3±1.2∗ | 49.6±10.0/3.0±1.2∗ |
| Lymphocytes, LY, %/LY, 103µL | 32.2±9.6/2.0±0.7 | 37.2±10.0/2.4±0.8∗ | 38.9±9.0/2.3±0.7∗ |
| Monocytes, MO, %/MO, 103µL | 7.7±2.4 | 8.0±2.2 | 8.3±2.2 |
| Eosinophils, EO, % | 2.4±1.1 | 3.5±1.9*** | 2.4±1.3 |
| Basophils, BA, % | 0.8±0.4 | 0.9±0.4** | 0.7±0.3 |
| Erythrocytes, RBC, 106µL | 4.9±0.4 | 4.4±0.3 | 4.4±0.4 |
| Hemoglobin, Hb, g/L | 146.2±13.0 | 134.2±8.0∗ | 133.1±9.6∗ |
| Platelets, PLT, 103µL | 248.6±60.3 | 230.3±52.7 | 253.1±67.5 |
Data are presented as: mean with SD, median with interquartile range. To compare quantitative data between three unrelated groups, depending on the distribution, either the ANOVA test with post hoc analysis using Tukey’s test or the Kruskal-Wallis test with post hoc analysis using Dunn’s test was used. p<0.05: * compared to HC; ** compared to NSSI+.
Table 3.
Odds ratio of predictors for model-assessed probability of developing NSSI.
| Parameter | Estimate | Std Error | Statistic | p-Value |
|---|---|---|---|---|
| ACTH, pg/ml | 1.10 | 0.04 | 221 | 0.027 |
| CATS “negative home environment” subscale, scores | 6.37 | 0.9 | 2.06 | 0.039 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



