
Submitted:
08 November 2023
Posted:
09 November 2023
You are already at the latest version
Abstract
Background: Appendicitis is a common cause of emergency department visits and appendectomies in the US, with 250,000 appendectomies performed annually. Current diagnostic methods, such as clinical findings, lead to inaccuracies and missed diagnoses, increasing morbidity and mortality. The only solution is surgery, but current hematological tests are not reliable and may lead to unnecessary surgery if the underlying etiology is self-limiting or requires medical treatment. This study explores the role of MRI as a diagnostic modality that can replace US/CT and supplement traditional clinical diagnostic signs while avoiding ionizing radiation and intravenous contrast medium. The purpose of this meta-analysis is to determine the accuracy of MRI as a diagnostic modality in diagnosing appendicitis, addressing concerns about diagnostic modalities and their adverse effects, and addressing the necessity and success of relevant interventions. Methods: Medical literature was comprehensively searched and reviewed without restrictions to particular study designs, or publication dates using PubMed, Cochrane Library, and Google Scholar databases for all relevant literature formulated in English. The extraction of necessary data proceeded after specific inclusion and exclusion criteria were applied. Meta Analysis was performed for 5206 patients, with 35 RCTs being selected. Analysis was done using the QualSyst tool, wherein two writers independently assessed the caliber of each study as well as the use of the Cochrane tool for bias risk apprehension. The statistical software packages RevMan (Review Manager, version 5.3), SPSS (Statistical Package for the Social Sciences, version 20), and Excel in Stata 14 were used to perform the statistical analyses along with other analytical software. Results: MRI had an overall sensitivity of over 95%, an overall specificity of 94.2% with a PPV of 0.875 in comparison to CT scan in the diagnosis and intervention regarding appendicitis. Conclusion: These findings strongly suggest that MRI is a reasonable alternative to CT for the diagnosis of appendicitis in hospitals with appropriate access to this technology for reasons about accuracy, reliability, and reproducibility as well as addressing safety concerns.
Keywords:
MRI
; US
; CT
; Appendicitis
Introduction:
Millions of patients are seen in emergency departments (EDs) for abdominal pain. Appendicitis is a frequent cause of such visits, leading to 250,000 appendectomies performed annually in the United States.[1]
Diagnosing appendicitis based solely on clinical symptoms is often incorrect in approximately 30% of cases, potentially resulting in unnecessary surgical interventions [2]. Conversely, a missed diagnosis of appendicitis carries significant morbidity. And yet, appendicitis is diagnosed clinically with investigations that include blood tests and imaging studies, but no test exists that can reliably identify it with 100% accuracy.
The potential complications of a ruptured appendix are far too dangerous and carry a significant mortality and morbidity risk. To effectively manage patients suffering from appendicitis, once a diagnosis of appendicitis is made, the traditional treatment is surgical excision of the appendix (appendectomy) via open or laparoscopic approaches to the abdomen [3]
An incorrect diagnosis of appendicitis may lead to unnecessary surgery if the underlying etiology is self-limiting or requires medical treatment. Surgery will result in a negative appendectomy (NA), where the appendix is excised but tissue analysis reveals no inflammation (a negative appendectomy).
The risks of a missed diagnosis, as well as one associated with unnecessary surgery due to an incorrect diagnosis, both underline the necessity of an effective diagnostic algorithm based on imaging that offers accuracy as well as convenience. Diagnostic imaging with ultrasonography or computed tomography (CT) has been proven accurate to detect acute appendicitis [4]. However, these imaging modalities do not seem to be as effective in differentiating simple from perforated appendicitis. For ultrasonography, the reported sensitivities vary from 29% to 84% [5]. More recent studies evaluating the accuracy of CT in detecting perforated appendicitis have documented sensitivities between 28% and 62% and specificities between 81% and 91% [6] [7] [8]. While these numbers appear to be encouraging, they do not offer 100% accuracy for diagnosing appendicitis, which has been established to be a condition that would require prompt, accurate diagnosis followed by efficient interventions to be managed safely.
Magnetic resonance imaging (MRI) is a promising modality in the evaluation of suspected acute appendicitis owing to its high diagnostic accuracy [9] [10] and avoidance of ionizing radiation and intravenous contrast medium. In the past, MRI availability and affordability, especially in emergency department settings, have posed challenges. Nevertheless, the cost of MRI has gradually approached that of CT over time, and its accessibility has significantly improved in recent years. If MRI is confirmed to be an accurate, radiation-free imaging test, then it could be a valid alternative or even a first-line imaging modality for appendicitis. This would be particularly true in children and pregnant women, to whom avoidance of radiation is especially desirable.
The purpose of this meta-analysis was to ascertain the accuracy of MRI as a diagnostic modality in the context of diagnosing appendicitis, to pave the way for effective, efficient, and accurate management of the same, thereby addressing concerns about diagnostic modalities and their adverse effects, as well as the necessity and success of relevant interventions.
- METHODOLOGY:
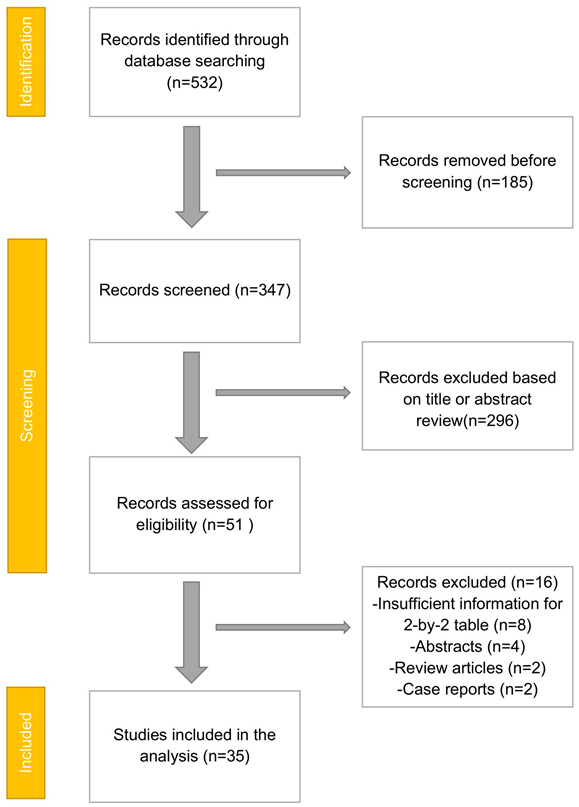
- PRISMA Flowchart (Figure 1)
- DATA COLLECTION
A comprehensive literature search was conducted using PubMed, Google Scholar, and the Cochrane Library databases to identify relevant articles. Only full-text articles in English were included in this analysis. Medical subject headings (MeSH) and keywords like 'CT scan,' 'MRI Scan,' 'MRI vs CT scan for Acute Appendicitis,' 'Diagnosis imaging for Acute Appendicitis,' and 'Acute Appendicitis' were employed. Additionally, we reviewed references, reviews, and meta-analyses for potential additional articles.
- INCLUSION AND EXCLUSION CRITERIA
Initial screening of titles and abstracts was performed to eliminate duplicate entries and citations. References of relevant papers were also reviewed to identify possible additional articles. Selection criteria included papers with detailed patient information and statistically supported results.
This study's primary objective was to assess the diagnostic accuracy of MRI in detecting appendicitis in diverse patient populations.
We included studies comparing MRI and CT scan outcomes for suspected appendicitis in the general population, encompassing children, pregnant patients, and adults. Hence, this study aimed to conduct a systematic review and meta-analysis of MRI's diagnostic efficacy for appendicitis in the broader population, not limited to specific subgroups like pregnant patients or children. Our primary outcomes of interest were MRI's sensitivity and specificity for this indication.
Inclusion criteria were: (1) studies reporting accurate diagnosis with MRI and CT scan, (2) studies published in English, and (3) studies comparing MRI with CT for Acute Appendicitis. Exclusion criteria included: (1) non-full-text articles, (2) unpublished articles, and (3) articles in languages other than English.
- DATA EXTRACTION
Each eligible paper was independently evaluated by two reviewers. They examined the number of patients, age, modality of procedures, and incidence of predetermined complications. Any conflicts were resolved through discussion with the author or a third party. We assessed the research quality using a modified Jadad score. According to the PRISMA guidelines, we selected a total of 35 randomized controlled trials (RCTs) involving 5206 patients.
- ASSESSMENT OF STUDY QUALITY
The quality of each included study was independently assessed by two reviewers using the QualSyst tool, consisting of ten questions with scores ranging from 0 to 2. The maximum possible total score is 20. Two authors evaluated each article based on the mentioned criteria. Interobserver agreement for study selection was determined using the weighted Cohen's kappa (K) coefficient. To assess the risk of bias in RCTs, we also employed the Cochrane tool. No assumptions were made about missing or unclear information, and no external funding was received for data collection or review.
- STATISTICAL ANALYSIS
Statistical analyses were conducted using software packages, including RevMan (Review Manager, version 5.3), SPSS (Statistical Package for the Social Sciences, version 20), and Stata 14 in Excel. Data were collected and entered into analytical software. We estimated sensitivity, specificity, positive predictive value (PPV), diagnostic odds ratios (DOR), and relative risk (RR) using fixed- or random-effects models, with 95 percent confidence intervals to evaluate critical clinical outcomes. We computed diagnosis accuracy and the Youden index for each outcome. Individual study sensitivity and specificity were depicted in Forest plots and receiver operating characteristic (ROC) curves. Additionally, we described the prior odds ratio, positive and negative likelihood ratios, and positive and negative post-test ratios in Fegan's analysis.
- BIAS STUDY
To assess the risk of bias, QUADAS-2 analysis was employed. This tool includes 4 domains Patient selection, Index test, Reference standard, Flow of the patients, and Timing of the Index tests.
- RESULT:

Table 1.
Table of the description of papers.
| First Author | Year | Location | Study type | Study dates | Index test | Reference standard | Total Patients | Females | Mean Age |
| Aggawala [12] |
2018 | Australia | Prospective | 2017-2018 | MRI | Histology or Follow-Up | 52 | 37 | Unclear (range 10-39 years) |
| Aguilera [13] | 2018 | U.S.A | Retrospective | 2014-2016 | MRI | Histology or Follow-Up | 52 | 52 | Median age 25 |
| Amitai [14] | 2016 | Isreal | Retrospective | 2007-2013 | MRI | Histology or Follow-Up | 49 | 49 | Unclear |
| Aspelund [15] | 2014 | U.S.A | Retrospective | 2008-2012 | MRI | Histology or Follow-Up | 397 | Unclear | Unclear |
| Avcu [16] | 2013 | Turkey | Prospective | 2009-2010 | MRI | Histology or Follow-Up | 55 | 26 | 35.6 |
| Batool [17] | 2016 | Canada | Prospective | Unclear | MRI | Histology or Follow-Up | 100 | 56 | Unclear |
| Bayraktutan [18] | 2014 | Turkey | Prospective | Unclear | MRI | Histology or Follow-Up | 45 | 19 | 7 |
| Burke [19] | 2015 | U.S.A,multicentre | Retrospective | 2009-2014 | MRI | Histology or Follow-Up | 709 | 709 | 27.5 |
| Burns [20] | 2018 | Canada | Retrospective | 2006-2012 | MRI | Histology or Follow-Up | 63 | 63 | 31 |
| Corkum [21] | 2018 | U.S.A | Retrospective | 2015-2016 | MRI | Histology or Follow-Up | 135 | Unclear | 11.5 |
| des Plantes [22] | 2016 | Netherlands | Prospective | Unclear | MRI | Histology or Follow-Up | 112 | 112 | 22 |
| Dibble [23] | 2017 | U.S.A | Retrospective | 2011-2012 | MRI | Histology or Follow-Up | 77 | Unclear | 11.5 |
| Didier [24] | 2017 | U.S.A | Retrospective | 2013-2015 | MRI | Histology or Follow-Up | 98 | 60 | 11 |
| Dillman [25] | 2016 | U.S.A | Retrospective | 2013-2014 | MRI | Histology or Follow-Up | 103 | 56 | 11.5 |
| Donlon [26] | 2015 | Ireland | Retrospective | 2008-2014 | MRI | Histology or Follow-Up | 29 | 29 | Unclear |
| Fonseca [27] | 2014 | U.S.A | Retrospective | 2000-2011 | MRI | Histology or Follow-Up | 31 | 31 | Unclear |
| Kearl [28] | 2016 | U.S.A | Retrospective | 2010-2013 | MRI | Histology or Follow-Up | 192 | Unclear | 14.8 |
| Kennedy [29] | 2018 | U.S.A | Retrospective | 2014-2017 | MRI | Histology or Follow-Up | 612 | 353 | 11.7 |
| Khalil [30] | 2018 | U.S.A | Retrospective | 2014-2017 | MRI | Histology or Follow-Up | 568 | Unclear | Unclear |
| Kinner [31] | 2017 | U.S.A | Prospective | 2012-2014 | MRI | Histology or Follow-Up | 230 | 28 | 17.1 |
| Koning [32] | 2014 | U.S.A | Retrospective | 2012-2013 | MRI | Histology or Follow-Up | 364 | 223 | 11.3 |
| Konrad [33] | 2015 | U.S.A | Retrospective | 2009-2011 | MRI | Histology or Follow-Up | 114 | 114 | Unclear |
| Kulaylat [34] | 2015 | U.S.A | Retrospective | 2011-2013 | MRI | Histology or Follow-Up | 510 | 23 | 11.3 |
| Shin [35] | 2017 | Korea | Retrospective | 2008-2015 | MRI | Histology or Follow-Up | 125 | 125 | 30.6 |
| Theilen [36] | 2015 | U.S.A | Retrospective | 2007-2012 | MRI | Histology or Follow-Up | 171 | 171 | Unclear |
| Thieme [37] | 2014 | Netherlands | Prospective | 2009 | MRI | Histology or Follow-Up | 104 | 57 | 12 |
| Tsai [38] | 2017 | U.S.A | Retrospective | 2003-2015 | MRI | Histology or Follow-Up | 233 | 233 | 28.4 |
| Nitta [39] | 2005 | Japan | Retrospective | Unclear | MRI | Histology or Follow-Up | 37 | 19 | 37.1 |
| Cobben [40] | 2009 | Netherlands | Prospective | 2005-2006 | MRI | Histology or Follow-Up | 138 | 80 | 29 |
| Singh [41] | 2009 | U.S.A | Retrospective | 2001-2007 | MRI | Histology or Follow-Up | 40 | unknown | 34 |
| Inci E [42] | 2011 | Turkey | Prospective | Unclear | MRI | Histology or Follow-Up | 119 | 36 | 27 |
| Chabanova [43] | 2011 | Denmark | Prospective | Unclear | MRI | Histology or Follow-Up | 48 | 29 | 37.1 |
| Heverhagen JT [44] | 2012 | Germany | Prospective | 2008 | MRI | Histology or Follow-Up | 52 | 21 | 44.7 |
| Zhu [45] | 2012 | China | Prospective | 2009-2011 | MRI | Histology | 41 | 23 | 41.5 |
| Leeuwenburgh [46] | 2014 | Netherlands | Prospective | 2010 | MRI | Histology or Follow-Up | 223 | 138 | 38 |
- MRI
- vs CT scan for Appendicitis
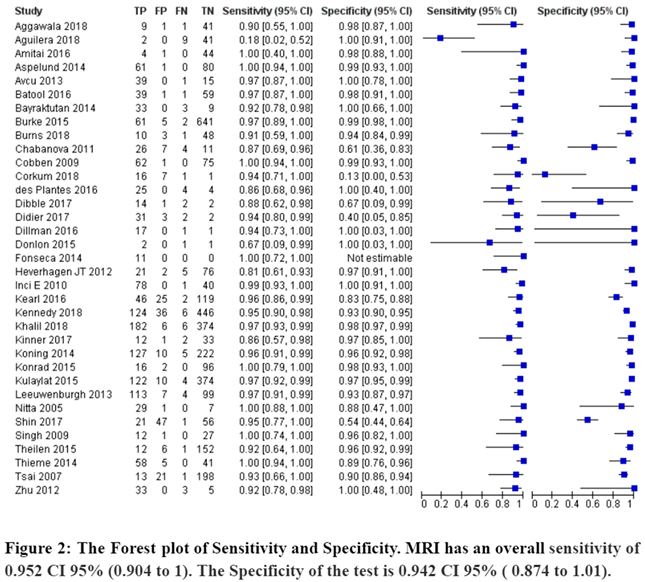
A total of 35 RCTs with 5206 patients were selected for the study(figure 2). Out of these tests, 19 tests showed a sensitivity of over 95%, and 22 tests provided a specificity of over 95%. And 12 tests showed both specificity and sensitivity over 95%. The value of True positive was 1481, True Negative was 3440, False negative was 74, and False Positive was 211. With a confidence interval of 95%, Sensitivity, specificity, and Positive Predictive values were calculated. A summary of these findings is depicted in Figure 2. The Sensitivity of the test is 0.952 with a CI of 95% in a range of (0.904 to 1) the mean being (0.048). The Specificity of the test is 0.942 with a CI of 95% in a range of ( 0.874 to 1.01) the mean being (0.068). The PPV is 0.875 with a CI of 95% in a range of (0.82 to 0.93) the mean being (0.055).
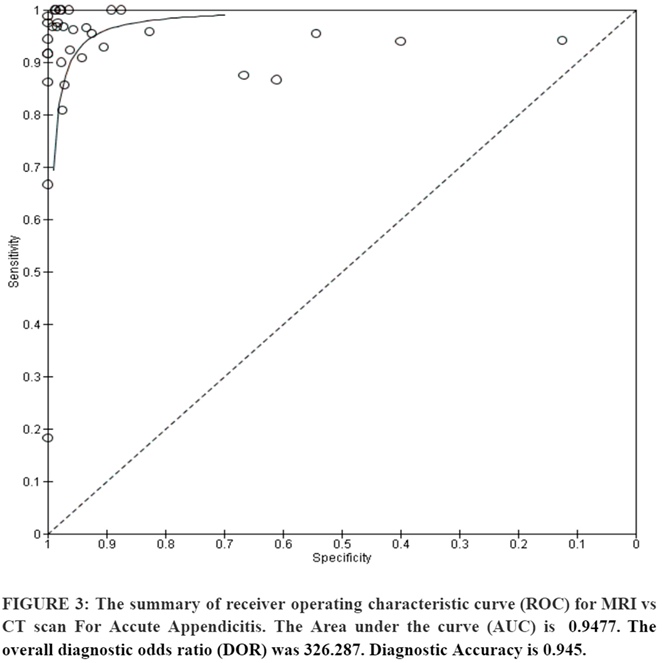
The summary of the ROC curve (Figure 3) shows that the area under the ROC (AUC) was 0.9477. The overall diagnostic odds ratio (DOR) was 326.287. Diagnostic Accuracy is 0.945 and The Younden Index is 0.895.
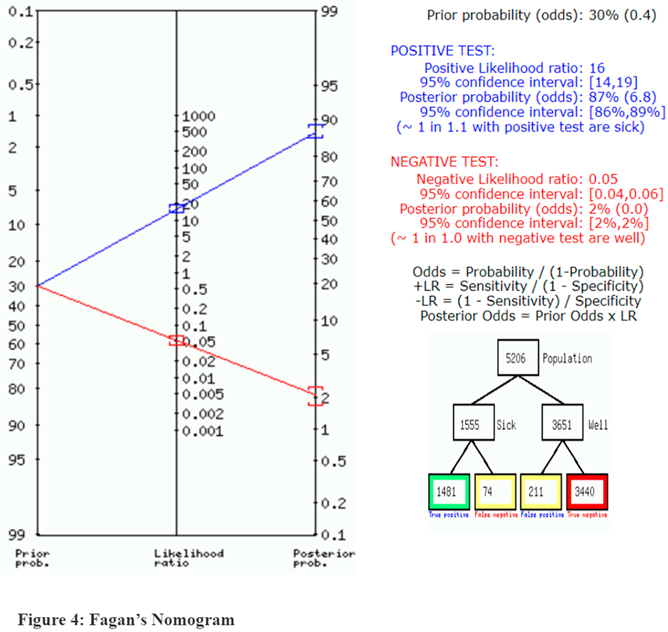
In Figure 4, a summary of Fagan’s analysis can be observed, in conclusion, the prior probability of the test was 30. The positive likelihood ratio was 16 and the post-test ratio was 87. The negative likelihood ratio was 0.05 and the post-test ratio was 2.
- Bias Study:
Table 2. Risk of bias and applicability concern
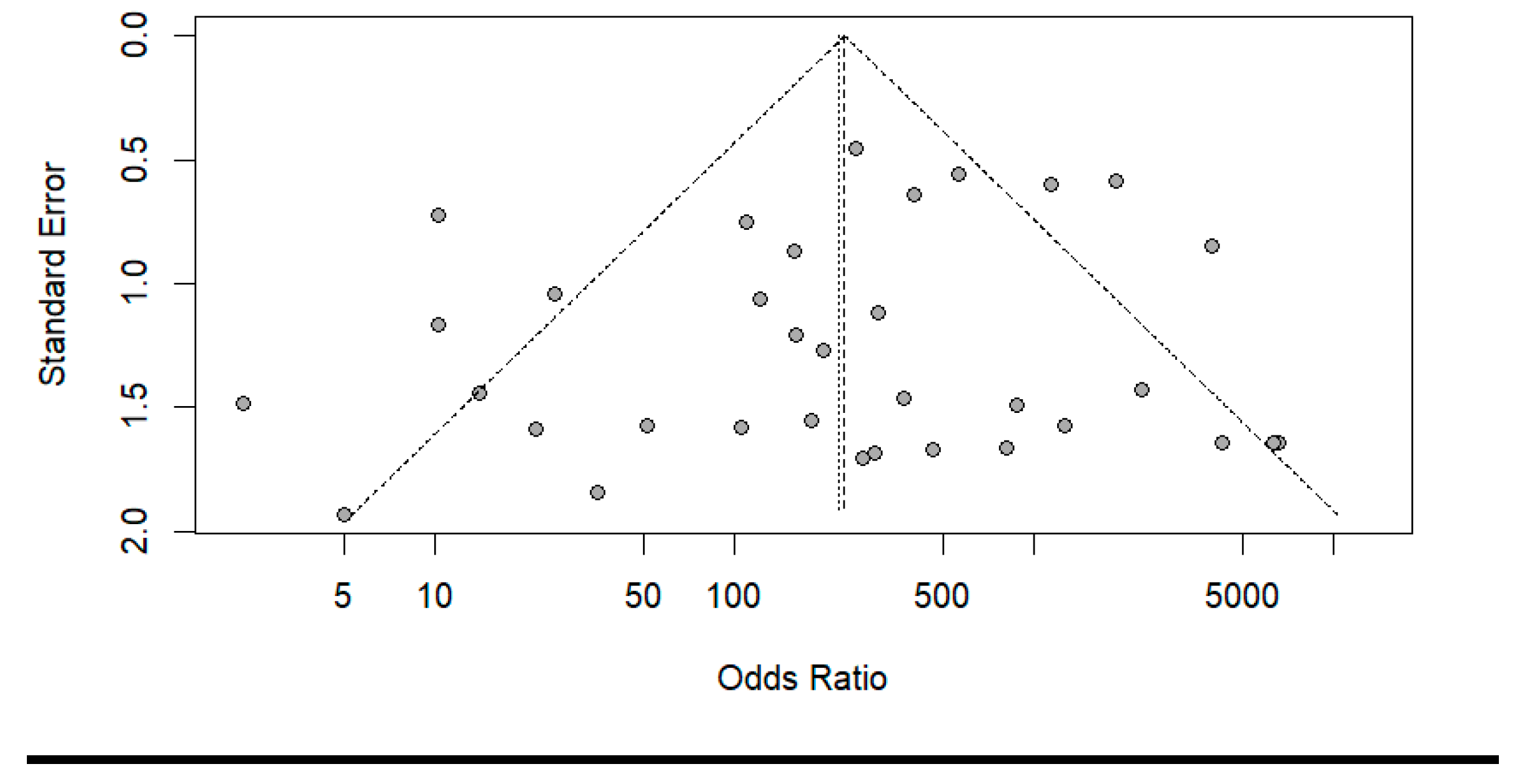
- Publication Bias:
The summary of publication bias is shown in (Table 2 and Figure 5). For the publication bias, Inpatient selection was low in 14 studies out of 35, unclear in 18, and high in 3. In the index test, it was low in 14 studies, unclear in 20, and high in 1. While the reference standard was low in 8, high in 13, and unclear in 14. The flow and timing were high in 23, low in 9, and unclear in 3. The applicability concerns in patient selection were low in 30 high in 4 and unclear in 1. The Reference standard was low in 32, and high in 3. The index test was high in 7 and low in 26, unclear in 2.
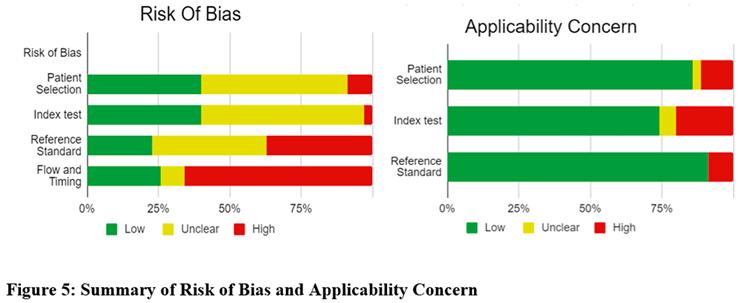
Figure 6.
Funnel plot for publication bias.
Discussion:
Acute appendicitis is one of the most commonly encountered emergency diseases that need urgent surgical intervention [47]. This demonstrates the need for urgent and precise diagnostic modalities. Commonly, ultrasound (US) and computed tomography (CT) are recognized as valuable imaging techniques for diagnosing acute appendicitis. The reported sensitivity of US in diagnosing acute appendicitis ranges from 75% to 90%, and the specificity and accuracy are greater than 90% [48] [49] [50] [51]. However, there are several disadvantages to using the US to diagnose acute appendicitis. Its diagnostic accuracy depends on the examiner's skill and experience. The graded compression technique, although effective, demands a high degree of technical skill and experience. The retro-cecal appendix is hard to visualize in US. Approximately 30% of cases missed on US examination are attributed to the appendix being in the retro-cecal position. In obese patients, visualizing the appendix using US can be challenging, and US may not accurately depict widespread inflammation. In addition, gaseous distension of the bowel loop in paralytic or obstructive conditions hinders the visualization of the appendix. These findings further establish the need to seek a more effective diagnostic tool.
CT is considered a highly accurate diagnostic modality for identifying acute appendicitis. According to previous reports, even when patients present with atypical symptoms, CT demonstrates sensitivity and specificity exceeding 80%. Reported accuracy typically ranges from 93% to 94%, with sensitivity values of 87% to 98% and specificity values of 83% to 97% [52] [53] [54] [55]. CT offers several advantages over ultrasound (US) in diagnosing appendicitis. It excels in correctly identifying periappendiceal inflammation by detecting increased fatty density, linear strands, or fluid collection.
Complicated appendicitis such as abscess formation or severe phlegmonous change around the cecal region is easily demonstrated, as is an extrapelvic extension of the inflammation. CT can also easily assess the remainder of the abdomen and pelvis, allowing non-appendiceal diseases with the same symptoms including cholecystitis, pancreatitis, gynecological disease, and urological disease to be diagnosed [56] [57].
In line with the findings of our study, there has been increasing awareness of the potential harms associated with the use of ionizing radiation from CT, despite its very high accuracy for imaging acute pathology in the abdomen. Certain reports have shown a strong trend of increasing use of CT for the evaluation of patients presenting to the ED with abdominal pain, without a corresponding increase in the number of cases of surgical emergencies identified [58]. This potentially led to the exploration of MRI as a safer and more accurate diagnostic modality for appendicitis.
MRI is an excellent technique for the diagnosis of acute appendicitis and the exclusion of diseases requiring surgical/ interventional treatment. By using MR imaging, the unnecessary appendectomy rate was decreased. MR imaging has reported a sensitivity of 95.2%, a specificity of 94.2% for the diagnosis of acute appendicitis, along with a diagnostic accuracy of 94.5% and Younden Index of 0.895. Cobben et al., showed the value of a shorter and simpler MRI protocol in patients with clinically suspected appendicitis. According to this study sensitivity and specificity were 100% and 98%, respectively [59]. It is also prudent to note the effect of an MRI scan of the appendix on the use of hospital resources, concluding that an abdominal MRI in the evaluation of patients suspected of having appendicitis is a reliable, safe, and potentially cost-effective technique, in line with the findings of Cobben et al.
However, a noteworthy drawback of MRI would be that when compared with CT, MRI is said to not be easily accessible for emergency studies. [60]
Conclusion:
These findings strongly suggest that MRI is a reasonable alternative to CT for the diagnosis of appendicitis in hospitals with appropriate access to this technology, as well as the financial ability to effectively make this technology available. In particular, the use of MRI instead of CT would avoid exposing patients to ionizing radiation, which may increase a patient’s lifetime risk of developing cancer, particularly in younger patients. MRI may not be appropriate for patients with specific contraindications such as metallic implants or claustrophobia. However, it could be a suitable imaging option for other patient groups, including those at risk for contrast-induced nephropathy due to iodinated contrast material, individuals with a history of iodinated contrast reactions, and those concerned about the potential for radiation-induced malignancies, particularly young patients.
Limitations:
The results of our meta-analysis should be interpreted with caution, given the limitations of conducting a meta-analysis. The assumption of 100% accuracy in a reference standard, US and CT in this study, does not hold in clinical practice, including the case of appendicitis. The accuracy of the results could have been improved by including a larger number of patients. However, in the absence of large studies, meta-analyses are an optimal method of synthesizing the data from available studies. Furthermore, studies that were not published in the English language were not included in this meta-analysis, thereby not excluding the possibility that relevant data has been missed. A meta-analysis involving more studies and a higher number of included patients would likely provide a more accurate estimate of the comparison of results. However, the results of this study are still robust, given the strict inclusion criteria to ensure the reasonable methodologic quality of the included studies as well as the appropriate methodology to compare the relevant modalities.
References
- Mason Rodney, J. , “Surgery for appendicitis: is it necessary?”.
- Bernard, A. Birnbaum and Stephanie R. Wilson, “Appendicitis at the Millennium”.
- Thomas Jaschinski, Mosch Christoph G, Eikermann Michaela, Edmund Am Neugebauer, and Stefan Sauerland, “Laparoscopic versus open surgery for suspected appendicitis”.
- Adrienne van Randen, Boermeester Marja A, Zwinderman Aeilko H, Ubbink Dirk T, Stoke Jaap, and Bipat Shandra, “Acute appendicitis: a meta-analysis of diagnostic performance of CT and graded compression US related to prevalence of disease”.
- K F Borushok, R R Townsend, F C Laing, and R B Jeffrey Jr, “Sonographic diagnosis of perforation in patients with acute appendicitis”.
- Jason D Fraser et al., “Accuracy of computed tomography in predicting appendiceal perforation”.
- Thomas A Foley, Frank Earnest 4th, David M Hough, Mark A Nathan, Henry J Schiller, and Tanya L Hoskin, “Differentiation of nonperforated from perforated appendicitis: accuracy of CT diagnosis and relationship of CT findings to length of hospital stay”.
- Suk Won Suh et al., “Clinical factors for distinguishing perforated from nonperforated appendicitis: a comparison using multidetector computed tomography in 528 laparoscopic appendectomies”.
- Marjolein M N Leeuwenburgh et al., “Comparison of imaging strategies with conditional contrast-enhanced CT and unenhanced MR imaging in patients suspected of having appendicitis: a multicenter diagnostic performance study”.
- Lodewijk Cobben, Emile Coerkamp, Ingrid Groot, Lucas Kingma, Julien Puylaert, and Johan Blickman, “A simple MRI protocol in patients with clinically suspected appendicitis: results in 138 patients and effect on the outcome of appendectomy”.
- Dr. Dev Desai, “Dev’s Formulae for Diagnostic Test Accuracy Meta-analysis”.
- S. Aggarwala et al., “The role of a rapid protocol abdominal MRI for patients with clinically suspected Appendicitis”.
- Fabiola Aguilera, Brian F Gilchrist, and Daniel T Farkas, “Accuracy of MRI in Diagnosing Appendicitis during Pregnancy”.
- Michal M Amitai et al., “Role of Emergency Magnetic Resonance Imaging for the Workup of Suspected Appendicitis in Pregnant Women”.
- Gudrun Aspelund et al., “Ultrasonography/MRI versus CT for diagnosing appendicitis”.
- Serhat Avcu, Halil Arslan, Feray Altun Çetin, Özgur Kemik, and Ahmet Cumhur Dülger, “The value of diffusion-weighted imaging and apparent diffusion coefficient quantification in the diagnosis of perforated and nonperforated appendicitis”.
- Batool S, Thomson G, Ortiz C, Bhandal S, and Gupta P, “Diagnostic accuracy of MR imaging for evaluation of acute appendicitis: a prime prospective study of Canadian pediatric population”.
- Ümmugulsum Bayraktutan et al., “Diagnostic performance of diffusion-weighted MR imaging in detecting acute appendicitis in children: comparison with conventional MRI and surgical findings”.
- Lauren M B Burke et al., “Magnetic resonance imaging of acute appendicitis in pregnancy: a 5-year multiinstitutional study”.
- Michael Burns, Patrick Vos, Cameron J Hague, Pari Tiwari, and Sam M Wiseman, “Utility of Magnetic Resonance Imaging for the Diagnosis of Appendicitis During Pregnancy: A Canadian Experience”.
- Kristine, S. Corkum, Julia E Grabowski, Tolulope A.Oyetunji, Cynthia K. Rigsby, and Timothy B. Lautz, “Absolute neutrophil count as a diagnostic guide for the use of MRI in the workup of suspected appendicitis in children ”.
- C M P Ziedses des Plantes, M J F van Veen, J van der Palen, J M Klaase, H A J Gielkens, and R H Geelkerken, “The Effect of Unenhanced MRI on the Surgeons’ Decision-Making Process in Females with Suspected Appendicitis”.
- Elizabeth H Dibble, Grayson L Baird, David W Swenson, Claudia Cartagena, and Thaddeus W Herliczek, “Effectiveness of a Staged US and Unenhanced MR Imaging Algorithm in the Diagnosis of Pediatric Appendicitis”.
- Ryne A Didier, Fergus V Coakley, Sanjay Krishnaswami, David M Spiro, Bryan R Foster, and Katharine L Hopkins, “Performance characteristics of magnetic resonance imaging without contrast agents or sedation in pediatric appendicitis”.
- Jonathan R Dillman et al., “Equivocal Pediatric Appendicitis: Unenhanced MR Imaging Protocol for Nonsedated Children-A Clinical Effectiveness Study”.
- Donlon N, Cormick P, Larkin J, and Mehigan B, “The use of MRI to diagnose appendicitis during pregnancy”.
- Annabelle L Fonseca, Adrian A Maung, Kevin M Schuster, Lewis J Kaplan, Felix Y Lui, and Kimberly A Davis, “The use of magnetic resonance imaging in the diagnosis of suspected appendicitis in pregnancy: shortened length of stay without an increase in hospital charges”.
- Y Liza Kearl et al., “Accuracy of Magnetic Resonance Imaging and Ultrasound for Appendicitis in Diagnostic and Nondiagnostic Studies”.
- Thomas M Kennedy, Amy D Thompson, Arabinda K Choudhary, Richard J Caplan, Kathleen E Schenker, and Andrew D DePiero, “Utility of applying white blood cell cutoffs to non-diagnostic MRI and ultrasound studies for suspected pediatric appendicitis”.
- Khalil S, Tripathee N, Skaug M, Shiralkar K, and Surabhi V, “Accuracy of unenhanced MR imaging in the detection of perforated acute appendicitis in pediatric patients”.
- Sonja Kinner et al., “Diagnostic Accuracy of MRI Versus CT for the Evaluation of Acute Appendicitis in Children and Young Adults”.
- Jeffrey L Koning, John H Naheedy, and Peter G Kruk, “Diagnostic performance of contrast-enhanced MR for acute appendicitis and alternative causes of abdominal pain in children”.
- Joseph Konrad, David Grand, and Ana Lourenco, “MRI: first-line imaging modality for pregnant patients with suspected appendicitis”.
- Afif N Kulaylat et al., “An implemented MRI program to eliminate radiation from the evaluation of pediatric appendicitis”.
- Ilah Shin, Joon Seok Lim, Chansik An, Myeong-Jin Kim, and Yong Eun Chung, “T1 bright appendix sign to exclude acute appendicitis in pregnant women”.
- Lauren H Theilen et al., “Utility of magnetic resonance imaging for suspected appendicitis in pregnant women”.
- Mai, E. Thieme et al., “Diagnostic accuracy and patient acceptance of MRI in children with suspected appendicitis”.
- 1, 1, 2, Richard Tsai 1, Kathryn J Fowler, Constantine Raptis, Joseph W Owen, and Vincent M Mellnick, “MRI of suspected appendicitis during pregnancy: interradiologist agreement, indeterminate interpretation and the meaning of non-visualization of the appendix”.
- Norihisa Nitta, Kiyoshi Murata, Masashi Takahashi, Akira Furukawa, Masayuki Mori, and Masanobu Fukushima, “MR imaging of the normal appendix and acute appendicitis”.
- Lodewijk Cobben, Emile Coerkamp, Ingrid Groot, Lucas Kingma, Julien Puylaert, and Johan Blickman, “A simple MRI protocol in patients with clinically suspected appendicitis: results in 138 patients and effect on the outcome of appendectomy”.
- Ajay K Singh, Hemali Desai, and Robert A Novelline, “Emergency MRI of acute pelvic pain: MR protocol with no oral contrast”.
- Ercan Inci, Elif Hocaoglu, Ozgur Kilickesmez, Sibel Aydin, Sibel Bayramoglu, and Tan Cimilli, “Utility of diffusion-weighted imaging in the diagnosis of acute appendicitis”.
- Elizaveta Chabanova et al., “Unenhanced MR Imaging in adults with clinically suspected acute appendicitis”.
- Johannes T Heverhagen, Klaus J Klose, Kathrin Pfestroff, Anna E Heverhagen, Katharina Kessler, and Helmut Sitter, “Diagnostic accuracy of magnetic resonance imaging: a prospective evaluation of patients with suspected appendicitis (diamond)”.
- Bin Zhu, Bing Zhang, Ming Li, Shifu Xi, Decai Yu, and Yitao Ding, “An evaluation of a superfast MRI sequence in the diagnosis of suspected acute appendicitis”.
- M M N Leeuwenburgh et al., “Accuracy of MRI compared with ultrasound imaging and selective use of CT to discriminate simply from perforated appendicitis”.
- D J Humes and J Simpson, “Acute appendicitis”.
- J B Puylaert, “Acute appendicitis: US evaluation using graded compression”.
- R B Jeffrey Jr, F C Laing, and R R Townsend, “Acute appendicitis: sonographic criteria based on 250 cases”.
- M M Abu-Yousef, J J Bleicher, J W Maher, L F Urdaneta, E A Franken Jr, and A M Metcalf, “High-resolution sonography of acute appendicitis”.
- M Rioux, “Sonographic detection of the normal and abnormal appendix”.
- E J Balthazar, B A Birnbaum, J Yee, A J Megibow, J Roshkow, and C Gray, “Acute appendicitis: CT and US correlation in 100 patients”.
- K R Curtin, S W Fitzgerald, A A Nemcek Jr, F L Hoff, and R L Vogelzang, “CT diagnosis of acute appendicitis: imaging findings”.
- E J Balthazar, A J Megibow, S E Siegel, and B A Birnbaum, “Appendicitis: prospective evaluation with high-resolution CT”.
- A J Malone Jr, C R Wolf, A S Malmed, and B F Melliere, “Diagnosis of acute appendicitis: the value of unenhanced CT”.
- E J Balthazar, J Roshkow, B A Birnbaum, J Yee, A J Megibow, and C Gray, “Acute appendicitis: CT and US correlation in 100 patients”.
- E J Balthazar, A J Megibow, S E Siegel, and B A Birnbaum, “Appendicitis: prospective evaluation with high-resolution CT”.
- Jesse M Pines, “Trends in the rates of radiography use and important diagnoses in emergency department patients with abdominal pain”.
- Lodewijk Cobben, Emile Coerkamp, Lucas Kingma, Julien Puylaert, Johan Blickman, and Ingrid Groot, “A simple MRI protocol in patients with clinically suspected appendicitis: results in 138 patients and effect on the outcome of appendectomy”.
- C. M. P. Ziedses des Plantes, M. J. F. van Veen, J. van der Palen, J. M. Klaase, H. A. J. Gielkens, and R. H. Geelkerken, “The Effect of Unenhanced MRI on the Surgeons’ Decision-Making Process in Females with Suspected Appendicitis”.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



