
Submitted:
09 November 2023
Posted:
10 November 2023
You are already at the latest version
Abstract
Background: Along with sarcopenia, delayed blood pressure (BP) recovery after standing and orthostatic hypotension (OH) are among key clinical challenges associated with ageing. Previous studies have reported an association between sarcopenia and delayed orthostatic BP recovery and OH. However, the haemodynamic mechanisms underlying this association remain unclear. Methods: 107 attendees to a falls and syncope clinic aged 50+ years underwent an active stand test with non-invasive beat-to-beat haemodynamic measurement. Hand grip strength and 5-chair stands time were measured. Muscle mass was estimated using bioelectrical impedance analysis, and participants were classified as non-sarcopenic and sarcopenic. Mixed effects models with linear splines were used to model the effect of sarcopenia status on Modelflow®-derived mean arterial pressure (MAP), cardiac output (CO), total peripheral resistance (TPR), stroke volume (SV) and heart rate (HR) after standing, while controlling for potential confounders. Results: Sarcopenia was associated with: attenuated recovery of MAP in the 10-20s period after standing (β -0.67, P<0.001); attenuated rise to peak (0-10s) and recovery from peak (10-20s) of CO (β -0.05, P<0.001; β 0.06, P<0.001); attenuated recovery (10-20s) of TPR from nadir (β -0.02, P<0.001) and attenuated recovery from peak (10-20s) of SV (β 0.54, P<0.001). HR was not significantly associated with sarcopenia status at any time interval after standing. Conclusion: The attenuated BP recovery after standing seen in sarcopenia appears to be driven by initial diminished peak of CO followed by attenuated recovery of CO from peak and TPR from nadir. The CO finding appears to be driven by SV rather than HR. Potential mechanisms for these findings include: cardio-sarcopenia, the effects of sarcopenia on the autonomic nervous system and/or the skeletal muscle pump.
Keywords:
sarcopenia
; delayed blood pressure recovery
; orthostatic hypotension
; orthostatic haemodynamics
; orthostasis
1. Introduction
Humans stand on average 60 times per day [1]. One of the key challenges associated with orthostasis is the maintenance of blood pressure (BP) in the upright position. Gravity leads to a pooling of blood in the lower limbs and below the level of the heart and therefore a reduction in intrathoracic blood volume [2]. As a consequence, this leads to a decrease in central venous pressure and therefore stroke volume (SV), resulting in a decline in cardiac output (CO) [3]. Without counter-regulatory measures a precipitous fall in mean arterial pressure (MAP) would occur [4].
A number of mechanisms are involved in the recovery of BP on standing. Carotid and cardiopulmonary baroreceptors detect a fall in BP triggering a reduction in cardiac vagal activity and increase in sympathetic activity leading to an increase in heart rate (HR) which limits the fall in CO (caused by the drop in SV) [5]. Total peripheral resistance (TPR) increases via sympathetic mediated vasoconstriction in splanchnic and peripheral blood vessels [6]. Finally, the rhythmic activity of the skeletal muscle pump of the lower limbs may also improve venous return and subsequent SV and CO, thus helping maintain MAP [7].
Impairment of these mechanisms with ageing or disease may result in a delayed recovery of BP or a failure of BP to recover – orthostatic hypotension (OH) [8]. In general, a ‘classic’ non-recovery OH pattern observed at three minutes post-standing, especially when accompanied by a reduced or absent HR increase, is more likely to be ‘neurogenic’, or largely caused by either primary or secondary autonomic failure [9]. However, the importance of causes such as heart failure, medications and hypovolaemia are increasingly recognised in non-neurogenic presentations [10].
A potential contributor to OH is sarcopenia, a clinical condition of low muscle mass and function [11] that is prevalent in older people [12] and has been associated with many adverse outcomes [13]. Previous research has demonstrated an association between classic OH, assessed with intermittent BP measurement, and sarcopenia [14,15]. We previously found an association between beat-to-beat orthostatic BP recovery and both probable sarcopenia in a population study [16] and sarcopenia in a clinical setting [17].
However, the potential mechanisms underlying these associations have not been investigated and remain unclear. Departing from the well-established physiology equations: and [18] the aim of this study was to explore how the relationship between orthostatic BP recovery and sarcopenia may be mediated in haemodynamic terms.
2. Materials and Methods
Participants were recruited from the Falls and Syncope Unit at the Mercer’s Institute for Successful Ageing in St James’s Hospital, Dublin, Ireland [19]. Criteria for inclusion in the study were: age 50 years or older, able to provide written informed consent, able to mobilise independently (with or without aid) and able to transfer independently or with minimal assistance of one person from lying to standing. Exclusion criteria were: history of confirmed or presumed neurogenic OH, or contraindication to bioelectrical impedance analysis (BIA) (e.g. presence of an indwelling electronic device such as a cardiac pacemaker). Ethical approval for the study was granted from the Tallaght University Hospital/St. James’s Hospital Joint Research Ethics Committee (Project ID: 0221; approval date: 4 May 2021) and approval was also granted by St James’s Hospital Research & Innovation Office (Reference: 6567, approval date: 26 July 2021). All participants in the study provided explicit, written, informed consent. The study adhered to the World Medical Association Declaration of Helsinki on ethical principles for medical research involving human subjects.
Participants’ medical history and use of medications were obtained from sources including self-report, electronic health record review and General Practitioner correspondence. Cardiovascular medication use was defined as regular use of one or more of the following medications (coded using the Anatomical Therapeutic Chemical Classification (ATC)): anti-arrhythmics (ATC C01), anti-hypertensives (ATC C02), diuretics (ATC C03), vasodilators (ATC C04), beta-blocking agents (ATC C07), calcium channel blockers (ATC C08), or agents acting on the renin–angiotensin system (ATC C09). Psychotropic medication use was defined as taking one or more of the following: anti-epileptics (ATC N03A), anti-psychotics, anxiolytics, hypnotics or sedatives (ATC N05), or anti-depressants (ATC N06A).
Hand grip strength (HGS) was assessed using a Jamar Hydraulic Hand Dynamometer (Performance Health, Wisconsin, USA). The maximum value of two seated, consecutive measurements taken on the left and right hands was used. Values were rounded to the nearest 2 kg, as per the precision of the device. The five-chair stands test time (5CST) was measured as the time to the nearest centi-second taken for a participant to stand up and sit back down five times from a standard chair (approximate height 43 cm), as fast as possible. Height was measured to the nearest 0.01 m with a Seca 222 Stadiometer (Seca Ltd, Birmingham, UK). BIA was performed with the TANITA® DC-430 MAP Body Composition Analyser (Tanita Europe, Amsterdam, The Netherlands). Participants stood barefoot on the scale, which also provided weight measurement to the nearest 0.01 kg. Participants were asked to remove their outerwear and empty their pockets, and 0.5 kg was entered as a standard tare value for clothing. Appendicular skeletal muscle mass was estimated using the Sergi equation [20]. The European Working Group on Sarcopenia in Older People (EWGSOP) revised criteria for sarcopenia (HGS of less than 27 kg in men and 16 kg in women and/or 5CST greater than 15 s, with muscle mass less than 20 kg in men and 15 kg in women) were used [21].
Participants underwent an active stand test with continuous non-invasive beat-to-beat BP measurement with the Finapres® Nova (Finapres Medical Systems, Amsterdam, The Netherlands). The active stand test consisted of a supine signal calibration and resting phase of 5–10 min, followed by standing as quickly as possible and remaining standing quietly for 3 min [22]. Signal calibration was performed using oscillometric brachial calibration and the Physiocal function on the Finapres® Nova with the height correction unit adjusting for differences in hydrostatic pressure. The Finapres® Nova automatically calculates MAP per beat as the integral of the arterial pressure waveform.
Beat-to-beat signals for the haemodynamic parameters: CO, TPR, HR and SV are derived by the Finapres® Nova using the built-in Modelflow® algorithm. The Modelflow® algorithm calculates the aortic flow waveform by simulating a non-linear three-element model of aortic input impedance [23]. This is integrated to compute the SV and from this the CO is calculated by multiplying by HR [24]. TPR is then derived from the MAP divided by CO.
Values were exported from the Finapres® Nova software and analysed using custom written software in MATLAB® version 9.14 (The MathWorks, Inc., Natick, MA, USA) in accordance with previously published recommendations [25]. The baseline signal was taken as the mean of 60 to 30 seconds before standing. For the period from 0 to 180 seconds after standing a ±5 second moving average filter was applied to the signals. The relative change in haemodynamic parameters, at 10-second time intervals from 0-180s, was then calculated by subtracting the baseline from the absolute values.
Statistical analysis was performed with Stata® version 15.1 (StataCorp LLC, College Station, TX, USA). To assess the relationship between sarcopenia and each of the haemodynamic parameters, we used multi-level mixed effects models, as previously employed by our group and others [16,17,26,27]. The fixed and random effects accounted for the repeated measures within participants. Piecewise linear splines were used to model five time-intervals: 0-10, 10-20, 20-30, 30-40 and 40-180 seconds after standing. Residual variance was modelled with a first order autoregressive process to account for the strong correlation between adjacent timepoints. The linear splines were entered into the model as independent parameters along with interaction of sarcopenia status (no sarcopenia = 0; sarcopenia = 1) and potential confounders as covariates. The potential confounders considered were: age, sex, diabetes, hypertension, cardiovascular medications, and psychotropic medications.
3. Results
Of the 123 participants recruited to the study, 5 had a contraindication to or declined BIA, 7 had probable or confirmed neurogenic OH, 1 had no active stand test and in 3 the beat-to-beat haemodynamic signals were of poor quality. This left a final analytical sample size of 107 with a mean age of 69.7 years (standard deviation 10.4 years), with 61 (57%) being women. Further characteristics of this sample, grouped by sarcopenia status, are presented in Table 1.
The beta coefficients with confidence intervals and p-values, at each of the 5 time segments, from the adjusted mixed effects models for the relationship between sarcopenia status and each of the haemodynamic parameters is shown in Table 2. Plots of the marginal effects of the means for the two groups is shown in Figure 1 for each of the haemodynamic parameters.
The recovery in MAP in the 10-20s post-stand period was significantly attenuated in the sarcopenia group compared to the no sarcopenia group as evidenced by the highly statistically significant negative beta coefficient, at a time when the overall MAP trend was upwards.
CO for the sarcopenia group had an attenuated initial rise to peak in the 0-10s period, shown by the significant negative coefficients when overall CO was rising. This was followed by an attenuated recovery of CO from peak, for the sarcopenia group, in the 10-20s period, demonstrated by the significant positive beta coefficient at a time when CO was returning to baseline.
TPR showed a significantly attenuated recovery in the 10-20s period after standing for the sarcopenia group compared with no sarcopenia, again as indicated by a significant negative coefficient at a time when overall TPR was recovering.
For SV, the sarcopenia group had an attenuated recovery in the 10-20s period, demonstrated by a significant positive coefficient. For HR, no significant differences were seen between the two groups at any of the time intervals.
4. Discussion
In this study, we explored the relationship between sarcopenia status (present vs. absent) and the haemodynamic response to standing. We found that sarcopenia was associated with an attenuated recovery of MAP during the 10-20s period after standing, in keeping with our previous findings regarding systolic and diastolic BP [17]. We expanded upon our previous findings by examining the components of MAP, namely CO and TPR, demonstrating early post-standing changes in both factors that may drive the alterations observed in MAP. Furthermore, CO is determined by SV and HR and we observed significant changes in SV in the 10-20s period after standing, but no significant difference in HR between sarcopenia and non-sarcopenia groups. These results are important as they provide insights into the possible underlying pathophysiology of delayed BP recovery in older adults with sarcopenia and this may have implications for the clinical management of this condition. Our findings are strengthened by a well-characterised participant cohort, enabling adjustments for potential confounders. Additionally, the use of continuous beat-to-beat hemodynamic measurements allows for a non-invasive and precise characterisation of the hemodynamic response to orthostasis.
The finding of an attenuated rate of recovery of MAP in the 10 to 20s period after standing is in keeping with our previous study, which also found an attenuated rate of systolic and diastolic BP recovery in both probable and confirmed cases of sarcopenia during the same timeframe [17]. To our knowledge, apart from our previous study, no previous studies had examined the relationship between sarcopenia and the early BP response to standing. However, one study [28] found an association between 5CST time (a component of the EWGSOP criteria for probable sarcopenia) and diastolic BP recovery, 30 to 60s after standing, with a longer 5CST time being associated with worse diastolic BP recovery. Another study [29] found that those in the slowest category for 5CST had significantly higher odds of initial orthostatic hypotension in the first 15s after standing. Together with our study, they add weight to the hypothesis that muscle function and mass may be linked to BP recovery early after standing.
CO showed a significantly attenuated initial increase in the sarcopenic group when compared to the non-sarcopenic. The sarcopenic group also showed an attenuated recovery from peak CO in the 10 to 20s period. Thus, we can surmise that the changes in MAP were related to the attenuated CO response in the initial 10 seconds contributing to subsequent slower MAP recovery in the 10 to 20s period. The initial increase in CO on standing followed by prompt recovery seen in the non-sarcopenic group has been previously established in healthy participants [30,31]. Whilst no previous data had been reported in subjects with sarcopenia, Wieling et al. [32] found that older participants had a less pronounced rise in CO to peak after standing when compared to younger participants, similar to our finding in CO in the same period. The effects of ageing on skeletal muscle may have played a role in these findings. On the other hand, Van Wijnen and colleagues [33] found that in a group with delayed BP recovery there was no significant difference on average in CO compared to a normal BP recovery group but there was a large interparticipant variation in the delayed BP recovery group; yet, muscle mass or strength was not assessed in this study, and since the participants were 18 years and older, the likelihood of sarcopenia within this cohort is low.
Examining the TPR response, it is known that in healthy adults TPR falls initially due to a number of mechanisms related to the muscular effort of standing, before recovering from nadir [34]. The attenuated recovery of TPR in the sarcopenia group in the 10-20s period is similar to that of MAP, suggesting that the attenuated MAP recovery is driven at least partially by TPR [6]. Indeed, Van Wijnen et al. [33] found that TPR recovery was impaired in those with delayed BP recovery compared to normal BP recovery while changes in CO were not different, suggesting that TPR was the primary driver of delayed BP recovery in that group. Decreased TPR leading to OH has been reported previously in diabetics [35] and Pérez-Denia et al. [36] found impaired TPR recovery in those with multimorbidity and suggested that this might drive impairments in BP recovery. Again in these two studies muscle parameters were not examined but we know that both multimorbidity [37] and diabetes [38] are related to sarcopenia and so it may be one of the factors involved.
When breaking down CO into its constituents, SV and HR, we observed that SV showed an attenuated recovery in the 10-20s period while there were no significant differences in HR. This suggests that CO changes were driven by SV rather than HR. This finding is somewhat unexpected, as one might anticipate an increase in HR in individuals with sarcopenia to compensate for the potential reduction in venous return due to impaired skeletal muscle pump function, which could result in decreased SV. The association between sarcopenia and SV/HR after standing has not previously been investigated but the response of SV to standing has been show previously to differ between younger and older subjects. Wieling et al. [32] demonstrated a stable SV with large increase in HR in the initial 7s after standing in the younger group while in the older group there was less of a HR increase with initial fall in SV followed by transient recovery and subsequent further fall. As before, although muscle factors were not included, it is possible that they played a role in the differential response seen in older people.
There are several potential mechanisms underlying our findings. Specifically, in this sample, the effects on CO seemed primarily driven by SV rather than HR. It is established that SV is determined by preload, contractility and afterload [39]. Afterload is largely determined by MAP itself, thereby acting as a negative feedback mechanism [40]. Contractility is determined in part through preload via the Frank-Starling mechanism, as well as intrinsic factors [41]. It is here that the influences of sarcopenia on the heart muscle might act. Cardio-sarcopenia is a relatively novel concept [42], especially as traditionally hypertrophy rather than wasting of the heart is seen with ageing. However, a small number of studies have shown reductions in left ventricular mass in sarcopenia [43,44]. If correct, one might hypothesise that cardio-sarcopenia could lead to decreased contractility, leading to decreased SV, in turn impacting CO and subsequently leading to delayed recovery of MAP as seen in our study. When examining preload, it is influenced by end-diastolic volume, which is influenced by venous return [40]. It is in this aspect that the skeletal muscle pump may play a role [7], potentially contributing to the effects of sarcopenia. This impairment in preload might subsequently affect SV, consequently leading to impaired MAP recovery as described in the pathway above. With regards TPR, this may be an effect of sarcopenia on the autonomic nervous system. It has been shown that general muscle sympathetic nerve activity (MSNA) is proportional to the muscle mass involved [45]. Therefore, those with sarcopenia might have reduced MSNA leading to impaired recovery of TPR and resultant delayed recovery of MAP.
Of course, there may be other mechanisms at play. Other syndromes such as frailty may be involved although the underlying pathophysiology between sarcopenia and physical frailty are increasingly recognised as likely being common [46]. Impairment of the exercise pressor reflex [47] may be involved although this is less likely as no significant differences in HR were found in our study. In a cross-sectional analysis, we cannot assert causality. However, it is more plausible that the pathway from sarcopenia to impaired BP recovery is the causal direction rather than the reverse pathway from impaired BP recovery to sarcopenia. There is the possibility of a positive feedback loop in that those with impaired BP recovery leading to falls may restrict activity due to fear of falling, which could lead to sarcopenia. We were unable to adjust for this pathway in our analysis and so acknowledge it as a limitation. Other limitations include the inherent limitations of BIA in the estimation of muscle mass [48], the relatively small sample size, and the lack of information on timing of medications in respect to the active stand test. Furthermore, the use of Modelflow® derived haemodynamics has inherent limitations [49]. Whilst the gold standard would be invasive measurement [50], conducting this procedures would be neither practical nor ethical in this population. Doppler echocardiography could be used, however Modelflow® has been shown to be an acceptable alternative [51] especially when relative haemodynamic changes are required rather than absolute [52], as in our design.
Our results are important for a number of reasons. Firstly, from a pure pathophysiological and scientific point of view, they are novel. To the best of our knowledge, no previous study has utilised our methodology to address the question as to how sarcopenia could contribute to delayed BP recovery in older individuals. Secondly, results are of clinical importance. Through the use of beat-to-beat BP monitoring, impaired BP recovery has become increasingly recognised [53,54] and been shown to independently predict falls, fractures and mortality [55,56,57]. Our results link sarcopenia with impaired BP recovery and this, in turn, could potentially be implicated in subsequent falls and fractures. Importantly, sarcopenia is potentially reversible and multicomponent interventions that improve sarcopenia [58] could also be used to ameliorate delayed BP recovery. This of course underlines the importance of identifying sarcopenia in the falls and syncope unit in the first place [59]. Pressor agents such as fludrocortisone and midodrine are routinely prescribed for OH and delayed BP recovery [60] despite their off-label use and potential side effects [61]. Perhaps increasing use of multicomponent intervention as well as training in physical counterpressure manoeuvres [62] would lessen the use of these medications and also benefit cases of combined supine hypertension and OH [63], where physical interventions could help both.
5. Conclusions
We observed sarcopenia to be associated with an attenuated rate of recovery of MAP early after standing. This appeared to be driven by initial blunted peak of CO followed by attenuated recovery of CO from peak and TPR from nadir. The CO finding appeared to be driven by SV rather than HR. There are a number of potential mechanisms implicated including: cardio-sarcopenia, the effects of sarcopenia on the autonomic nervous system and the skeletal muscle pump and further research is needed to clarify the mechanisms involved and their relative contributions.
Author Contributions
Conceptualization, E.D. & R.RO.; methodology, E.D., S.K. & R.RO; software, E.D & S.K.; validation, E.D. & S.K..; formal analysis, E.D.; data curation, E.D..; writing—original draft preparation, E.D..; writing—review and editing, E.D., S.K., F.X.& R.RO.; visualization, E.D..; supervision, R.RO.; project administration, R.RO.; funding acquisition, R.RO. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Science Foundation Ireland (SFI), grant number 18/FRL/6188.
Institutional Review Board Statement
Ethics approval for the study was granted from the Tallaght University Hospital/St. James’s Hospital Joint Research Ethics Committee (Project ID: 0221; approval date: 4 May 2021). Approval was also granted by St James’s Hospital Research & Innovation Office (Reference: 6567, approval date: 26 July 2021). The study adhered to the World Medical Association Declaration of Helsinki on ethical principles for medical research involving human subjects.
Informed Consent Statement
Written, explicit, informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Contingent on compliance with data protection legislation and ethical approval data may be available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to acknowledge the patients who gave their time to participate in this study and to thank the staff of the Falls and Syncope Unit, St. James’s Hospital, Dublin for their help and support.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Dall, P.M.; Kerr, A. Frequency of the Sit to Stand Task: An Observational Study of Free-Living Adults. Appl. Ergon. 2010, 41, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Blomqvist, C.; Stone, H. Cadiovascular Adjustments to Gravitational Stress. In Handbook of Physiology: The Cardiovascular System: Peripheral Circulation and Organ Blood Flow; Shepherd, J., Abboud, F., Geiger, S., Eds.; American Physiological Society: Bethesda, Md, 1983. [Google Scholar]
- Smith, J.J.; Porth, C.M.; Erickson, M. Hemodynamic Response to the Upright Posture. J. Clin. Pharmacol. 1994, 34, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Low, P.A.; Benarroch, E.E. Clinical Autonomic Disorders, 3rd ed.; Lippincott Williams & Wilkins: Wilkins: Philadelphia, 2009; ISBN 978-0-7817-7381-2. [Google Scholar]
- Borst, C.; Van Brederode, J.F.M.; Wieling, W.; Van Montfrans, G.A.; Dunning, A.J. Mechanisms of Initial Blood Pressure Response to Postural Change. Clin. Sci. 1984, 67, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Sprangers, R.L.; Wesseling, K.H.; Imholz, A.L.; Imholz, B.P.; Wieling, W. Initial Blood Pressure Fall on Stand up and Exercise Explained by Changes in Total Peripheral Resistance. J. Appl. Physiol. 1991, 70, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Rowell, L.B. Human Cardiovascular Control; Oxford University Press: New York, 1993; ISBN 978-0-19-507362-1. [Google Scholar]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Panagopolous, D.; Torocastro, M.; Sutton, R.; Lim, P.B. Orthostatic Hypotension in Older People: Considerations, Diagnosis and Management. Clin. Med. 2021, 21, e275–e282. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R. Neurogenic Orthostatic Hypotension. N. Engl. J. Med. 2008, 358, 615–624. [Google Scholar] [CrossRef]
- Fedorowski, A.; Ricci, F.; Hamrefors, V.; Sandau, K.E.; Hwan Chung, T.; Muldowney, J.A.S.; Gopinathannair, R.; Olshansky, B. Orthostatic Hypotension: Management of a Complex, But Common, Medical Problem. Circ. Arrhythm. Electrophysiol. 2022, 15. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Gonzalez, M.C.; Prado, C.M. Sarcopenia ≠ Low Muscle Mass. Eur. Geriatr. Med. 2023. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global Prevalence of Sarcopenia and Severe Sarcopenia: A Systematic Review and Meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLOS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Kocyigit, S.E.; Dokuzlar, O.; Bulut, E.A.; Smith, L.; Isik, A.T. Relationship between Sarcopenia and Orthostatic Hypotension. Age Ageing 2020, 49, 959–965. [Google Scholar] [CrossRef]
- Keskin, K.; Çiftçi, S.; Öncö, J.; Dogan, G.M.; Çetinkal, G.; Yildiz, S.S.; Sigirci, S.; Kiliçkesmez, K.O. Orthostatic Hypotension and Age-Related Sarcopenia. Turk. J. Phys. Med. Rehabil. 2021, 67, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Duggan, E.; Murphy, C.H.; Knight, S.P.; Davis, J.R.C.; O’Halloran, A.M.; Kenny, R.A.; Romero-Ortuno, R. Differential Associations Between Two Markers of Probable Sarcopenia and Continuous Orthostatic Hemodynamics in The Irish Longitudinal Study on Ageing. J. Gerontol. Ser. A 2022, glac243. [Google Scholar] [CrossRef]
- Duggan, E.; Knight, S.P.; Romero-Ortuno, R. Relationship between Sarcopenia and Orthostatic Blood Pressure Recovery in Older Falls Clinic Attendees. Eur. Geriatr. Med. 2023. [CrossRef] [PubMed]
- Herring, N.; Paterson, D.J.; Levick, J.R. Levick’s Introduction to Cardiovascular Physiology; Sixth edition.; CRC Press: Boca Raton London New York, 2018; ISBN 978-0-8153-6361-3. [Google Scholar]
- O’Donoghue, P.J.; Claffey, P.; Rice, C.; Byrne, L.; Cunningham, C.; Kenny, R.A.; Romero-Ortuno, R. Association between Gait Speed and the SHARE Frailty Instrument in a Falls and Syncope Clinic. Eur. Geriatr. Med. 2021, 12, 1101–1105. [Google Scholar] [CrossRef] [PubMed]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing Appendicular Skeletal Muscle Mass with Bioelectrical Impedance Analysis in Free-Living Caucasian Older Adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 601–601. [Google Scholar] [CrossRef] [PubMed]
- Finucane, C.; van Wijnen, V.K.; Fan, C.W.; Soraghan, C.; Byrne, L.; Westerhof, B.E.; Freeman, R.; Fedorowski, A.; Harms, M.P.M.; Wieling, W.; et al. A Practical Guide to Active Stand Testing and Analysis Using Continuous Beat-to-Beat Non-Invasive Blood Pressure Monitoring. Clin. Auton. Res. 2019, 29, 427–441. [Google Scholar] [CrossRef]
- Wesseling, K.H.; Jansen, J.R.; Settels, J.J.; Schreuder, J.J. Computation of Aortic Flow from Pressure in Humans Using a Nonlinear, Three-Element Model. J. Appl. Physiol. 1993, 74, 2566–2573. [Google Scholar] [CrossRef]
- Harms, M.P.M.; Wesseling, K.H.; Pott, F.; Jenstrup, M.; Van Goudoever, J.; Secher, N.H.; Van Lieshout, J.J. Continuous Stroke Volume Monitoring by Modelling Flow from Non-Invasive Measurement of Arterial Pressure in Humans under Orthostatic Stress. Clin. Sci. 1999, 97, 291–301. [Google Scholar] [CrossRef]
- Soraghan, C.J.; Fan, C.W.; Hayakawa, T.; Cronin, H.; Foran, T.; Boyle, G.; Kenny, R.-A.; Finucane, C. TILDA Signal Processing Framework (SPF) for the Analysis of BP Responses to Standing in Epidemiological and Clinical Studies. In Proceedings of the IEEE-EMBS International Conference on Biomedical and Health Informatics (BHI); IEEE: Valencia, Spain, June, 2014; pp. 793–796. [Google Scholar]
- Newman, L.; O’Connor, J.D.; Romero-Ortuno, R.; Reilly, R.B.; Kenny, R.A. Supine Hypertension Is Associated With an Impaired Cerebral Oxygenation Response to Orthostasis: Finding From The Irish Longitudinal Study on Ageing. Hypertension 2021, 78, 210–219. [Google Scholar] [CrossRef]
- O’Connor, J.D.; O’Connell, M.D.L.; Knight, S.P.; Newman, L.; Donoghue, O.A.; Kenny, R.A. Impaired Stabilisation of Orthostatic Cerebral Oxygenation Is Associated with Slower Gait Speed: Evidence from The Irish Longitudinal Study on Ageing. J. Gerontol. Ser. A 2022, 77, 1216–1221. [Google Scholar] [CrossRef] [PubMed]
- Mol, A.; Slangen, L.R.N.; van Wezel, R.J.A.; Maier, A.B.; Meskers, C.G.M. Orthostatic Blood Pressure Recovery Associates with Physical Performance, Frailty and Number of Falls in Geriatric Outpatients. J. Hypertens. 2021, 39, 101–106. [Google Scholar] [CrossRef] [PubMed]
- de Bruïne, E.S.; Reijnierse, E.M.; Trappenburg, M.C.; Pasma, J.H.; de Vries, O.J.; Meskers, C.G.M.; Maier, A.B. Diminished Dynamic Physical Performance Is Associated With Orthostatic Hypotension in Geriatric Outpatients. J. Geriatr. Phys. Ther. 2019, 42, E28–E34. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Sjöberg, B.J.; Thulesius, O. Cardiac Output and Blood Pressure during Active and Passive Standing. Clin. Physiol. 1996, 16, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Marshall, R.J.; Shepherd, J.T. THE EFFECT OF CHANGES IN POSTURE AND OF GRADED EXERCISE ON STROKE VOLUME IN MAN *. J. Clin. Invest. 1960, 39, 1051–1061. [Google Scholar] [CrossRef]
- Wieling, W.; Veerman, D.P.; Dambrink, J.H.A.; Imholz, B.P.M. Disparities in Circulatory Adjustment to Standing between Young and Elderly Subjects Explained by Pulse Contour Analysis. Clin. Sci. 1992, 83, 149–155. [Google Scholar] [CrossRef] [PubMed]
- van Wijnen, V.K.; Hove, D.T.; Finucane, C.; Wieling, W.; van Roon, A.M.; Ter Maaten, J.C.; Harms, M.P.M. Hemodynamic Mechanisms Underlying Initial Orthostatic Hypotension, Delayed Recovery and Orthostatic Hypotension. J. Am. Med. Dir. Assoc. 2018, 19, 786–792. [Google Scholar] [CrossRef]
- van Twist, D.J.L.; Harms, M.P.M.; van Wijnen, V.K.; Claydon, V.E.; Freeman, R.; Cheshire, W.P.; Wieling, W. Diagnostic Criteria for Initial Orthostatic Hypotension: A Narrative Review. Clin. Auton. Res. 2021, 31, 685–698. [Google Scholar] [CrossRef]
- Hilsted, J.; Parving, H.H.; Christensen, N.J.; Benn, J.; Galbo, H. Hemodynamics in Diabetic Orthostatic Hypotension. J. Clin. Invest. 1981, 68, 1427–1434. [Google Scholar] [CrossRef]
- Pérez-Denia, L.; Claffey, P.; Byrne, L.; Rice, C.; Kenny, R.A.; Finucane, C. Increased Multimorbidity Is Associated with Impaired Cerebral and Peripheral Hemodynamic Stabilization during Active Standing. J. Am. Geriatr. Soc. 1781; .0. [Google Scholar] [CrossRef]
- Veronese, N.; Smith, L.; Cereda, E.; Maggi, S.; Barbagallo, M.; Dominguez, L.J.; Koyanagi, A. Multimorbidity Increases the Risk for Sarcopenia Onset: Longitudinal Analyses from the English Longitudinal Study of Ageing. Exp. Gerontol. 2021, 156, 111624. [Google Scholar] [CrossRef]
- Mesinovic, J.; Zengin, A.; De Courten, B.; Ebeling, P.R.; Scott, D. Sarcopenia and Type 2 Diabetes Mellitus: A Bidirectional Relationship. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, Volume 12, 1057–1072. [Google Scholar] [CrossRef]
- Bugge-Asperheim, B.; Kiil, F. Preload, Contractility, and Afterload as Determinants of Stroke Volume during Elevation of Aortic Blood Pressure in Dogs. Cardiovasc. Res. 1973, 7, 528–541. [Google Scholar] [CrossRef]
- Norton, J.M. TOWARD CONSISTENT DEFINITIONS FOR PRELOAD AND AFTERLOAD. Adv. Physiol. Educ. 2001, 25, 53–61. [Google Scholar] [CrossRef]
- Solaro, R.J. Regulation of Cardiac Contractility; Integrated Systems Physiology: From Molecule to Function to Disease; Morgan & Claypool Life Sciences: San Rafael, CA, 2011; Vol. 3. [Google Scholar]
- Loh, D.R.; Tan, R.-S.; Lim, W.S.; Koh, A.S. Cardio-Sarcopenia: A Syndrome of Concern in Aging. Front. Med. 2022, 9, 1027466. [Google Scholar] [CrossRef] [PubMed]
- Keng, B.M.H.; Gao, F.; Teo, L.L.Y.; Lim, W.S.; Tan, R.S.; Ruan, W.; Ewe, S.H.; Koh, W.; Koh, A.S. Associations between Skeletal Muscle and Myocardium in Aging: A Syndrome of “Cardio-Sarcopenia”? J. Am. Geriatr. Soc. 2019, 67, 2568–2573. [Google Scholar] [CrossRef]
- Pelà, G.; Tagliaferri, S.; Perrino, F.; Bussolati, G.; Longobucco, Y.; Zerbinati, L.; Adorni, E.; Calvani, R.; Cesari, M.; Cherubini, A.; et al. Interaction of Skeletal and Left Ventricular Mass in Older Adults with Low Muscle Performance. J. Am. Geriatr. Soc. 2021, 69, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Seals, D.R. Influence of Muscle Mass on Sympathetic Neural Activation during Isometric Exercise. J. Appl. Physiol. 1989, 67, 1801–1806. [Google Scholar] [CrossRef]
- Cesari, M.; Landi, F.; Vellas, B.; Bernabei, R.; Marzetti, E. Sarcopenia and Physical Frailty: Two Sides of the Same Coin. Front. Aging Neurosci. 2014, 6. [Google Scholar] [CrossRef]
- Mitchell, J.H.; Kaufman, M.P.; Iwamoto, G.A. The Exercise Pressor Reflex: Its Cardiovascular Effects, Afferent Mechanisms, and Central Pathways. Annu. Rev. Physiol. 1983, 45, 229–242. [Google Scholar] [CrossRef]
- Sergi, G.; De Rui, M.; Stubbs, B.; Veronese, N.; Manzato, E. Measurement of Lean Body Mass Using Bioelectrical Impedance Analysis: A Consideration of the Pros and Cons. Aging Clin. Exp. Res. 2017, 29, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Remmen, J.J.; Aengevaeren, W.R.M.; Verheugt, F.W.A.; Van Der Werf, T.; Luijten, H.E.; Bos, A.; Jansen, R.W.M.M. Finapres Arterial Pulse Wave Analysis with Modelflow® Is Not a Reliable Non-Invasive Method for Assessment of Cardiac Output. Clin. Sci. 2002, 103, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Jhanji, S.; Dawson, J.; Pearse, R.M. Cardiac Output Monitoring: Basic Science and Clinical Application. Anaesthesia 2008, 63, 172–181. [Google Scholar] [CrossRef]
- Matsukawa, K.; Kobayashi, T.; Nakamoto, T.; Murata, J.; Komine, H.; Noso, M. Noninvasive Evaluation of Cardiac Output during Postural Change and Exercise in Humans: Comparison between the Modelflow and Pulse Dye-Densitometry. Jpn. J. Physiol. 2004, 54, 153–160. [Google Scholar] [CrossRef]
- Sugawara, J.; Tanabe, T.; Miyachi, M.; Yamamoto, K.; Takahashi, K.; Iemitsu, M.; Otsuki, T.; Homma, S.; Maeda, S.; Ajisaka, R.; et al. Non-invasive Assessment of Cardiac Output during Exercise in Healthy Young Humans: Comparison between Modelflow Method and Doppler Echocardiography Method. Acta Physiol. Scand. 2003, 179, 361–366. [Google Scholar] [CrossRef]
- Briggs, R.; Carey, D.; Kennelly, S.P.; Kenny, R.A. Longitudinal Association Between Orthostatic Hypotension at 30 Seconds Post-Standing and Late-Life Depression. Hypertension 2018, 71, 946–954. [Google Scholar] [CrossRef] [PubMed]
- Finucane, C.; O’Connell, M.D.L.; Fan, C.W.; Savva, G.M.; Soraghan, C.J.; Nolan, H.; Cronin, H.; Kenny, R.A. Age-Related Normative Changes in Phasic Orthostatic Blood Pressure in a Large Population Study: Findings From The Irish Longitudinal Study on Ageing (TILDA). Circulation 2014, 130, 1780–1789. [Google Scholar] [CrossRef]
- Doyle, K.; Lavan, A.; Kenny, R.-A.; Briggs, R. Delayed Blood Pressure Recovery After Standing Independently Predicts Fracture in Community-Dwelling Older People. J. Am. Med. Dir. Assoc. 2021, 22, 1235–1241e1. [Google Scholar] [CrossRef]
- Finucane, C.; O’Connell, M.D.L.; Donoghue, O.; Richardson, K.; Savva, G.M.; Kenny, R.A. Impaired Orthostatic Blood Pressure Recovery Is Associated with Unexplained and Injurious Falls. J. Am. Geriatr. Soc. 2017, 65, 474–482. [Google Scholar] [CrossRef]
- Lagro, J.; Schoon, Y.; Heerts, I.; Meel-van den Abeelen, A.S.S.; Schalk, B.; Wieling, W.; Olde Rikkert, M.G.M.; Claassen, J.A.H.R. Impaired Systolic Blood Pressure Recovery Directly After Standing Predicts Mortality in Older Falls Clinic Patients. J. Gerontol. A. Biol. Sci. Med. Sci. 2014, 69, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Bernabei, R.; Landi, F.; Calvani, R.; Cesari, M.; Del Signore, S.; Anker, S.D.; Bejuit, R.; Bordes, P.; Cherubini, A.; Cruz-Jentoft, A.J.; et al. Multicomponent Intervention to Prevent Mobility Disability in Frail Older Adults: Randomised Controlled Trial (SPRINTT Project). BMJ 2022, e068788. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and Its Association with Falls and Fractures in Older Adults: A Systematic Review and Meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.-C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martín, A.; et al. 2018 ESC Guidelines for the Diagnosis and Management of Syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef] [PubMed]
- Wieling, W.; Kaufmann, H.; Claydon, V.E.; van Wijnen, V.K.; Harms, M.P.M.; Juraschek, S.P.; Thijs, R.D. Diagnosis and Treatment of Orthostatic Hypotension. Lancet Neurol. 2022, 21, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.L.; Khan, F.M.; Claydon, V.E. Counter Pressure Maneuvers for Syncope Prevention: A Semi-Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 1016420. [Google Scholar] [CrossRef]
- Gibbons, C.H.; Schmidt, P.; Biaggioni, I.; Frazier-Mills, C.; Freeman, R.; Isaacson, S.; Karabin, B.; Kuritzky, L.; Lew, M.; Low, P.; et al. The Recommendations of a Consensus Panel for the Screening, Diagnosis, and Treatment of Neurogenic Orthostatic Hypotension and Associated Supine Hypertension. J. Neurol. 2017, 264, 1567–1582. [Google Scholar] [CrossRef]
Figure 1.
Predicted means and standard error of the mean from mixed-effects models for change in mean arterial pressure (MAP; mmHg), cardiac output (CO; l/min), total peripheral resistance (TPR; mmHg*s/ml), stroke volume (SV; ml) and heart rate (HR; beats per minute) from baseline after standing grouped by sarcopenia status. Models were adjusted for age, sex, diabetes, hypertension, cardiovascular and psychotropic medications..
Figure 1.
Predicted means and standard error of the mean from mixed-effects models for change in mean arterial pressure (MAP; mmHg), cardiac output (CO; l/min), total peripheral resistance (TPR; mmHg*s/ml), stroke volume (SV; ml) and heart rate (HR; beats per minute) from baseline after standing grouped by sarcopenia status. Models were adjusted for age, sex, diabetes, hypertension, cardiovascular and psychotropic medications..
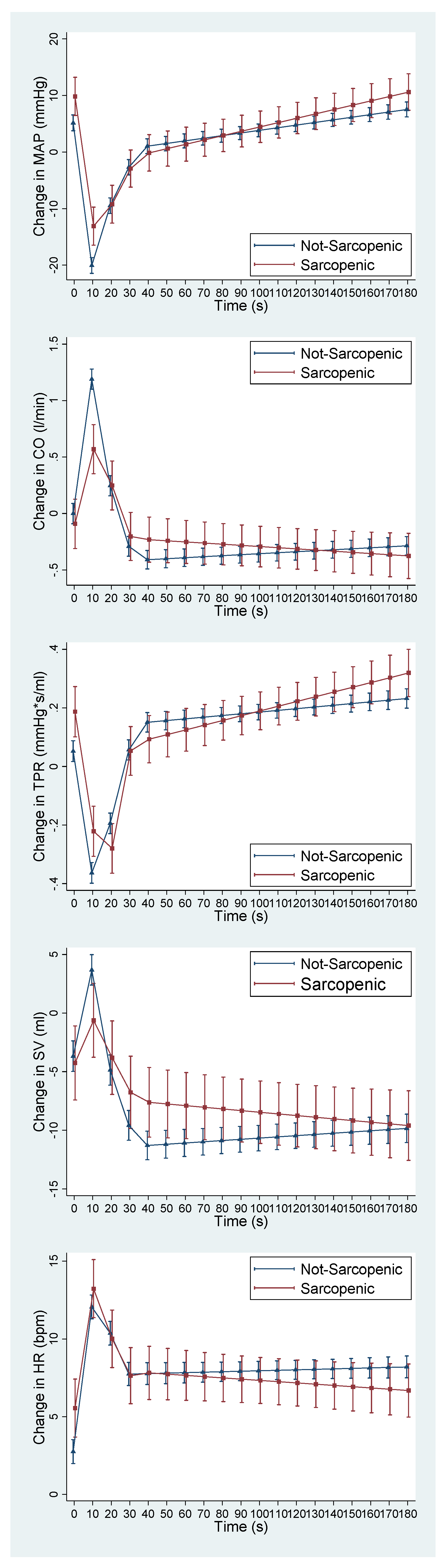

Table 1.
Characteristics of the sample grouped by sarcopenia status. Meds – medications; SD – standard deviation.
Table 1.
Characteristics of the sample grouped by sarcopenia status. Meds – medications; SD – standard deviation.
| No Sarcopenia (91/85%) | Sarcopenia (16/15%) | |
|---|---|---|
| Age (years) (mean/SD) | 68.6 (9.9) | 76.0 (11.24) |
| Female (n/%) | 52 (57.1) | 9 (56.3) |
| Hypertension (n/%) | 42 (46.2) | 9 (56.3) |
| Diabetes (n/%) | 15 (16.5) | 1 (6.3) |
| Cardiovascular Meds (n/%) | 44 (48.4) | 10 (62.5) |
| Psychotropic Meds (n/%) | 27 (29.7) | 7 (43.8) |
Table 2.
Beta-coefficients (β) and 95% confidence intervals (CI) for the effect of sarcopenia status on the change in mean arterial pressure (MAP; mmHg), cardiac output (CO; l/min), total peripheral resistance (TPR; mmHg*s/ml), stroke volume (SV; ml) and heart rate (HR; beats per minute) from baseline at time intervals 0–10 s, 10–20 s, 20–30 s, 30–40 s and 40–180 s after standing. Models were adjusted for age, sex, diabetes, hypertension, cardiovascular and psychotropic medications. *P < 0.05, **P < 0.01, ***P < 0.001
Table 2.
Beta-coefficients (β) and 95% confidence intervals (CI) for the effect of sarcopenia status on the change in mean arterial pressure (MAP; mmHg), cardiac output (CO; l/min), total peripheral resistance (TPR; mmHg*s/ml), stroke volume (SV; ml) and heart rate (HR; beats per minute) from baseline at time intervals 0–10 s, 10–20 s, 20–30 s, 30–40 s and 40–180 s after standing. Models were adjusted for age, sex, diabetes, hypertension, cardiovascular and psychotropic medications. *P < 0.05, **P < 0.01, ***P < 0.001
| 0-10s β (95% CI) |
10-20s β (95% CI) |
20-30s β (95% CI) |
30-40s β (95% CI) |
40-180s β (95% CI) |
|
|---|---|---|---|---|---|
| MAP | 0.23 (-0.13,0.59) |
-0.67 (-1.03,-0.31)*** |
-0.05 (-0.41,0.31) |
-0.10 (-0.45,0.31) |
0.03 (-0.02,0.08) |
| CO | -0.05 (-0.08,-0.03)*** |
0.06 (0.03,0.09)*** |
0.01 (-0.02,0.04) |
0.01 (-0.02,0.04) |
<-0.01 (<-0.01,<0.01) |
| TPR | <0.01 (-0.01,0.01) |
-0.02 (-0.03,-0.01)*** |
0.01 (<-0.01,0.02) |
-0.01 (-0.02,<0.01) |
<0.01 (<-0.01,<0.01) |
| SV | -0.37 (-0.72,-0.02) |
0.54 (0.19,0.88)*** |
0.18 (-0.17,0.52) |
0.09 (-0.25,0.43) |
-0.02 (-0.06,0.02) |
| HR | -0.16 (-0.40,0.08) |
-0.15 (-0.39,0.09) |
0.03 (-0.21,0.26) |
0.02 (-0.22,0.25) |
-0.01 (-0.04,0.01) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



