
Submitted:
09 November 2023
Posted:
13 November 2023
You are already at the latest version
Abstract
Background: Malnutrition was associated with worse survival outcomes, impaired quality of life, and deteriorated performance status across various cancer types. We aimed to identify risk factors for malnutrition in patients with epithelial ovarian(EOC) and impact on survival.
Methods: In our prospective study, we included the patients with primary and recurrent EOC, tubal or peritoneal cancer conducted. We assessed serum laboratory parameters, body mass index, nutritional risk index, nutritional risk screening score(NRS-2002), and bio-electrical impedance analysis.
Results: We recruited a total of 152. Patients >65 years-old, with ascites of >500 ml, or with platinum-resistant EOC showed statistically significant increased risk of malnutrition when evaluated by NRS-2002(p-values = 0.014, 0.001, and 0.007, respectively). An NRS-2002<3 was an independent predictive factor for complete tumor resectability (p=0.009). The patients with NRS-2002≥3 had a median overall survival(OS) of seven months (95% CI=0-24 months), as compared to the patients with NRS-2002<3 where median OS was 46 months(p=0,001). Phase angle(PhAα)≤ 4.5 was the strongest predictor of OS.
Conclusion: Malnutrition is an independent predictor of incomplete cytoreduction in study population. It is an independent prognostic factor for poor OS. Preoperative nutritional assessment is an effective tool in identification of high-risk groups within EOC characterized by poor clinical outcome.
Keywords:
malnutrition
; ovarian cancer
; overall survival
; nutritional risk screening score
; nutrition
; phase angle
; progression-free survival
Introduction
Malnutrition has been associated with worse survival outcome, impaired quality of life, and deteriorated performance status in patients across various cancer types [1,2,3]. Although modern interventions are continuously being developed within cancer therapies, advances in assessing, preventing, and treating malnutrition still remained limited. Approximately 30-80% of all patients with cancer are malnourished or cachectic [4,5,6,7]. This is influenced by tumor type, location, stage and current therapy [6,8,9]. Malnutrition can even be a direct cause of death in patients with advanced cancer stages [10]. Currently, the validated tools for nutritional screening include Nutritional Risk Screening 2002 (NRS-2002), Malnutrition Universal Screening Tool (MUST), Malnutrition Screening Tool (MST), and Mini Nutritional Assessment (MNA) in the literature [11]. Moreover, Nutritional Risk Index (NRI) has been developed to assess malnutrition in surgical patients [12].
The global cancer statistics 2020, including data from 185 countries, revealed that the estimated global incidence and mortality in ovarian cancer as 313,959 and 207,252, respectively [13]. The same report also showed that ovarian cancer mortality was the second highest among all the gynecologic cancers [13]. Patients with ovarian cancer are at higher risk of malnutrition compared to any other gynecological cancers [14]. Protein-energy malnutrition and cachexia are diagnosed in up to 81.4% of all the patients with ovarian cancer [14,15,16,17,18,19]. Moreover, patients with ovarian cancer were found to be 19 times more likely to present with malnutrition compared to the patients with benign conditions [14]. at the time of diagnosis, 66.7% of patients with OC have been found to be malnourished [14] and showed higher complication rates and longer hospital stays [20]. Additionally, malnutrition has been associated with shorter overall survival in patients with ovarian cancer [15,21,22]. Consequently, these high-risk patients require a complex combination of nutritional assessment strategies and individualized treatment plans.
In this prospective study, we aim to identify risk factors for malnutrition in patients with ovarian cancer, determine the diagnostic relevance of the commonest methods used to assess nutritional status in these patients, and evaluate the predictive and prognostic values of malnutrition in patients with primary and relapsed ovarian cancer.
Materials and methods
Study Design
This is a prospective single center study of the patients with primary and recurrent epithelial ovarian cancer (EOC), tubal or peritoneal cancer conducted at a tertiary care comprehensive cancer center. Approval from the Ethics Committee was obtained under the following reference number: EA2/142/07. We recruited patients between February 2007 and October 2008. Inclusion and registration in the study occurred upon admission. All the data was collected until discharge with a follow-up period of up to 3 years after diagnosis or until death. All patients over 18 years of age with histologically confirmed EOC, tubal or peritoneal cancer in the primary or relapse setting, who were admitted for cytoreductive surgery were included in the study. We obtained written consent from all the patients for their participation and inclusion in the tumor bank ovarian cancer (TOC) database. We excluded the patients with pre-existing cardiac conditions as well as pregnant or breast-feeding patients from our study.
Assessment of Nutritional Status
All the parameters described in our study have been validated in the previous clinical studies. We assessed patients’ nutritional status preoperatively on admission to classify patients as “malnourished” or “non-malnourished”. Our study focused on the objective methods for nutritional-status assessment. Venipuncture was always performed on the first day of admission prior to any intravenous infusions or supplements. Patient baseline characteristics were collected including past medical history and general clinical examination.
We determined the following nutritional-status indicators for each patient:
- 1)
- Serum laboratory parameters: hemoglobin (g/dl), lymphocytes(/nl), albumin(g/dl), pre-albumin (mg/l), transferrin (mg/dl), and C-reactive protein (CRP) (mg/dl).
- 2)
- Body mass index (BMI) and nutritional risk index (NRI) calculations were based on the following formulas: BMI= weight(kg)/(height(m))2 and NRI= (1.489 x Serum Albumin g/l) + 41.7 x (current weight/ usual weight) [12].
- 3)
- Nutritional Risk Screening Score (NRS-2002), a validated score, was determined in each patient to classify the risk for malnutrition [23]. We classified the patients with a score of ≥3 as high-risk for malnutrition.
- 4)
- Bio-electrical Impedance Analysis (BIA) is a relatively simple, inexpensive and non-invasive technique to measure body composition [24]. Each patient underwent BIA to measure body composition.
We used the following equipment to perform the analysis: B.I.A 2000-M (Series No. 0706) measurement apparatus from Darmstadt GmbH, BIA Phasertabs Ag/AgCl electrodes from MEDI CAL Healthcare GmbH Karlsruhe, and the software Nutri Plus Version 5.1, Data Input GmbH Darmstadt. We followed the standard company instructions to obtain all the measurements. During the measurements, each patient was asked to lie supine at approximately 45 degrees. The electrodes were applied to the right hand and foot and then connected to the measurement-device via color-coded wires, in accordance with the instruction manual. All measurements were made by the same investigator to eliminate the risk of inter-observer variability. Two main BIA-parameters were recorded Extra Cellular Mass (ECM)/Body Cell Mass (BCM) index and the Phase angle (PhAα).
In a healthy well-nourished adult, the BCM is always greater than ECM with an ECM/BCM index <1. BCM loss is mainly due to loss of muscle-mass secondary to increased catabolism, while a rise in ECM can be due to the third space fluid losses from edema, renal or cardiac failure. Changes in the ECM/BCM index can occur before weight loss (WL) is detected and is a sensitive index of malnutrition [24].
The PhAα is the relation of the two impedance components at 50 KHz, reactance (Xc) and resistance (R), expressed as PhAα = (Xc × 180°)/(R × π). In female patients a value of ≥ 5 degrees is considered adequate.
The Cut-off values for each nutritional status indicator, at which patients were classified as “malnourished”, were defined as follows based on corresponding receiver operating characteristic (ROC)-curve analyses: NRS-2002 ≥ 3, NRI < 100, albumin ≤ 4 g/dl, pre-albumin < 20 mg/l, transferrin < 200 mg/dl, BMI<18.5 kg/m2, ECM/BCM index > 1.2, PhAα ≤ 4.5°, and weight loss (WL) > 5% in the last 3 months.
Intra- and Post-operative Data Collection
Intra-operative tumor dissemination was documented using the validated intraoperative mapping of ovarian (IMO)-Script at time of cytoreductive-surgery [25]. This also included presence of ascites, peritoneal carcinosis, and residual tumor. No visible residual tumor was defined as complete cytoreduction. Tumor dissemination pattern was determined through the IMO-Script by quadrants and levels. The final histology, grading, and FIGO staging were also evaluated.
All complications occurring within 30 post-operative days were recorded. All patients were then followed up for a period of three years following the primary surgery to determine relapse, response, and survival rates.
The predictive value of malnutrition in patients with EOC was assessed using three main factors postoperative residual tumor, postoperative complications and response to platinum-based chemotherapy [26].
Moreover, we evaluated predictive and prognostic values of malnutrition via overall survival (OS) and progression-free survival (PFS) analysis.
Statistical Analysis
The results of the descriptive statistical nominal data were indicated as absolute values and percentages. For continuous and non-normally distributed variables, the median value with interquartile range (25%-75%) was presented. Ninety-five percent confidence interval (CI) were presented, where applicable. ROC curves were used to calculate the diagnostic accuracy of the methods used for nutritional-status assessment, with the NRS-2002 as a reference standard. For all other indicators of nutritional status that were used (NRI, PhA, ECM/BCM index, albumin, prealbumin, transferrin, and 5% weight loss in the last 3 months) a specific cut-off value was defined, which was subsequently used to classify patients’ nutritional status. A Phi-Factor 0,8 was used to classify a test as redundant. We performed univariate and multivariate survival analyses using the Kaplan–Meier method (log-rank testing) and Cox regression models. In this study, we accepted p-value<0.005 as statistically significant. We used Statistical Package for the Social Sciences (SPSS) Software, Version 19.0 for Windows (SPSS Inc. Chicago IL, USA) for the data analysis.
Results
A total of 152 patients were recruited based on our inclusion and exclusion criteria. Among these patients, 52% (n=79) had primary, and 48% (n=73) had recurrent EOC. The median age was 56 (19 – 84) years. Table 1 represents the patients’ baseline characteristics.
The validity of each nutritional-status indicator was evaluated in comparison with the NRS-2002. All nutritional-status indicators correlated significantly with the NRS-2002 (p<0.001) apart from BMI (p=0.786). The respective sensitivity and specificity values of each method were shown in Table 2. According to the NRS-2002 a total of 18.4% (n=28) of patients were classified as malnourished. Of those, 18 (64.3%) patients had primary EOC and 10 (35.7%) had recurrent EOC. Consequently, 22.8% of patients with primary EOC and 13.7% of patients with recurrent EOC were classified as malnourished. Moreover, depending on the nutritional-status indicator used, between 2% to 78.1% of patients with EOC were classified as malnourished (Table 2).
Risk Factors for Malnutrition
Patient and tumor characteristics were evaluated according to NRS-2002. Patients >65 years-old, with ascites of >500 ml, or with platinum-resistant EOC showed statistically significant increased risk of malnutrition when evaluated by NRS-2002 (p-values = 0.014, 0.001, and 0.007, respectively) (Table3). There were no other tumor or patient characteristics that correlated significantly with NRS-2002 ≥ 3 (Table 3).
The tumor characteristics were then correlated with the other nutritional-status indicators and with the NRS-2002 as demonstrated in Table 4. Non-serous and high grade EOC, bowel-infiltration, peritoneal carcinomatosis, and advanced FIGO-stage were associated with increased risk of malnutrition. The NRI showed similar correlation with the NRS-2002 but was not compatible with regards to tumor type, bowel involvement, and peritoneal carcinomatosis. Pre-albumin correlated with NRS-2002 with regards to ascites and platinum-sensitivity but did not show correlation with age. Transferrin correlated with NRS-2002 with regards to age, ascites and response to platinum-based chemotherapy. Moreover, transferrin correlated with bowel-involvement, peritoneal carcinosis and advanced FIGO-stage. WL over 5% in the last 3 months correlated with age but not with ascites and platinum-sensitivity. The ECM/BCM index corresponded to the NRS-2002, tumor stage, grading and FIGO-stage also influence the ECM/BCM index. The PhAα correlated with age and platinum-sensitivity similarly to the NRS-2002, but not with regards to ascites. Albumin was compatible with the NRS-2002 with regards to ascites, platinum-sensitivity and age. In addition, low albumin levels also correlated with bowel-involvement.
On average, all patients had tumor in at least three quadrants. Patients with NRS-2002 ≥3 had a significantly higher tumor burden than patients with NRS-2002 <3 (p=0.044) (Table 5). All nutritional-status indicators correlated significantly with tumor dissemination, except for WL> 5% in 3 months (Table 5).
Moreover, nutritional-status indicators and levels of tumor spread were examined. NRS-2002 showed no significance in tumor dissemination at particular levels in malnourished patients versus non-malnourished. Pre-albumin < 20mg/l was the only indicator that correlated significantly with a more frequent tumor dissemination on all three levels (level 1,2, 3; p-values: 0.001, 0.006, and 0.018, respectively). Transferrin <200 mg/dl correlated with more frequent tumor dissemination at level 2 and 3 (p-values: 0.001 and <0.001, respectively). Furthermore, albumin ≤ 4,0 g/dl, NRI < 100, and ECM/BCM > 1,2 were correlated significantly with malnutrition at level 3 (p-values: 0.008, 0.004, and 0.045, respectively).
Predictive Value of Malnutrition
Complete cytoreduction was achieved in 61.8% (n=94) of cases. Only 32.1% (n=9) of patients classified as malnourished had complete cytoreduction. The majority of patients (69.1%, n=85) who had complete cytoreduction had an NRS-2002 <3. An NRS-2002 <3 was an independent predictive factor for complete tumor resectability (p=0.009). Patients with NRS-2002 ≥3 had a 4.6-fold higher risk of postoperative residual tumor compared to patients with NRS-2002 <3 (OR=0.22, 95% CI=0,07-0,69). The PhAα, NRS-2002, ECM/BCM index, NRI, albumin, and prealbumin showed a significant correlation with postoperative residual tumor. This correlation was mostly significant for the PhAα. When compared to PhAα > 4.5, a PhAα ≤ 4.5 indicated a 5.4-fold higher risk of postoperative residual tumor. WL and transferrin did not correlate significantly with postoperative residual tumor.
More than three-fourth of the patients (75.7%) received at least one unit packed red blood cells (RBC) during the admission, with a median of two units RBC per patient. Majority of the patients (80.3%) received a blood product (RBCs, fresh frozen plasma, or platelets) with a median of eight units per patient. Malnourished patients received on average more RBC-transfusions than non-malnourished patients (p=0.019). On average malnourished patients received five units RBC (range 0-18) whilst non-malnourished patients receiving only two units (0-19) (p=0.002).
More than forty-two percent of the patients had at least one postoperative complication, including fistula, ileus, bowel perforation, anastomotic leaks, wound dehiscence, pneumothorax, embolism, infections, sepsis, organ failure, cardiac problems, and postoperative ascites or pleural effusions. The most frequent complication was infection, which occurred in 7.9% patients (n=12). Malnourished patients were significantly more likely to have a postoperative complication compared to non-malnourished patients (p=0.010). However, in the multivariate regression analysis, outcome for NRS-2002 was not statistically significant. Instead, only two nutritional-status indicators were independent predictors for postoperative complications: transferrin < 225 mg/dl (p =0.003, OR=3.49, 95%-CI=1.53-7.96) and PhAα ≤ 4.5 (p=0.034, OR=2.98, 95%CI=1.09-8.14). Patients with transferrin < 225 mg/dl have a 3.5-fold higher risk of postoperative complications. Patients with PhAα ≤ 4.5 have a 3-fold higher risk of postoperative complications. The other indicators did not show any statistically significant correlation with frequency of postoperative complications.
In total, three patients died within 30 days after cytoreductive surgery where mortality rate was 2.0%. All of them had an NRS-2002 score ≥ 3 and were also classified as malnourished according to pre-albumin, transferrin, ECM/BCM index and PhAα.
The median hospital stay was 15 days following surgery (2-68 days). There was no significant difference in hospital stay between patients with NRS-2002 ≥3 compared to NRS-2002 <3. However, ECM/BCM index, NRI, albumin, and pre-albumin correlated significantly with increased duration of hospital stay (p-values= 0.007, 0.005, 0.004, and 0.007, respectively). In fact, patients classified as malnourished according to those indicators stayed on average 2-4 days longer compared to non-malnourished patients.
According to NRS-2002, 18 patients (22.8%) were classified as malnourished. Four of them (22.2%), developed platinum resistance on follow-up. From the non-malnourished patients whereas only 7 patients (11.5%) were platinum-refractory at follow-up. In the univariate analysis, NRS-2002 showed no significant correlation with worse response to chemotherapy. WL of 5% over last 3 months was the only indicator that did show a significant correlation with platinum-based chemotherapy response. This was also confirmed in the multivariate regression analysis (p=0.041, OR=6.99, 95%-CI=1.08-45.45). Consequently, all other indicators were not independent prognostic factors for response to platinum-based chemotherapy.
Prognostic Value of Malnutrition
The follow-up period consisted of 37 months (0-59 months). Estimated median OS was 41 months (95% CI=33-48 months). After three years, 37 patients (24.3%) had no recurrence. The estimated PFS was 15 months (95% CI= 12-18 months).
The patients with NRS-2002 ≥3 had a median OS of seven months (95% CI=0-24 months), as compared to the patients with NRS-2002 <3 where median OS was 46 months (p=0,001). However, in the multivariate regression analysis, NRS-2002 score was not a significant independent prognostic factor (p=0,051). PhAα and ECM/BCM index correlated with shorter OS while PhAα ≤ 4.5 was the strongest predictor (Figure 1 A-B). No other indicators showed significant correlation with OS.
The malnourished patients according to NRS-2002 had a PFS of seven months (95% CI= 2-12 months), compared to non-malnourished patients with PFS of 16 months (95% CI=12-20 months). This was statistically significant (p=0.006) (Figure 2). Although PhAα, ECM/BCM index, and transferrin correlated with PFS, they were not statistically significant.
In patients without ascites, we detected a statistically significant difference in OS between malnourished and non-malnourished patients (p=0.001) (Figure 3). However, this difference was not statistically significant in patients with ascites <500ml and ascites >500ml. Hence, as ascites volume increases, the difference in OS between malnourished and non-malnourished patients decreases.
Discussion
In this prospective single cancer study, we included 152 patients with EOC and tubal or peritoneal cancer. In our study, 28 patients (18.4%) were classified as malnourished according to the NRS-2002 (Table 2). This might be due to the variation in nutritional aspects that can be identified by each parameter. When evaluated by NRS-2002, patients >65 years-old, with ascites of >500 ml, or with platinum-resistant EOC had statistically significant increased risk of malnutrition (Table 3). We found transferrin’s correlations with various tumor characteristics, except histology, grading, and primary vs recurrent cancer (Table 4). Majority of nutritional-status indicators correlated significantly with tumor dissemination (Table 5). The only indicator that correlated significantly with a more frequent tumor dissemination on all three levels was pre-albumin < 20mg/l. Compared to patients with NRS-2002 <3 or PhAα > 4.5, patients with NRS-2002 ≥3 or PhAα > 4.5 had around 5-fold higher risk of postoperative residual tumor. Transferrin < 225 mg/dl and PhAα ≤ 4.5 were found as independent predictors for postoperative complications. Only WL of 5% over last 3 months showed a significant correlation with platinum-based chemotherapy response. While both PhAα and ECM/BCM index correlated with shorter OS, PhAα ≤ 4.5 was the strongest predictor. sBased on NRS-2002, the malnourished patients had shorter PFS of compared to non-malnourished patients (p=0.006) (Figure 2). Among patients without ascites, the malnourished group had longer OS than non-malnourished patients (p=0.001) (Figure 3).
Many studies evaluating malnutrition in patients with gynecological cancers often analyze EOC patients as a separate “high risk” subgroup. To evaluate and identify malnutrition, several diagnostic methods are listed in current literature, including dual-energy X-Ray absorptiometry (DEXA) scan and densitometry. These methods are precise, but time-consuming, invasive, and expensive, and as such are not widely used in clinical practice. Various nutritional assessment tools are used, but no accepted gold standard exists. Nonetheless, evaluating and identifying malnutrition within clinical practice remains difficult, due to lack of diagnostic criteria and consistent documentation. A systematic review evaluating 5 frequently used nutrition screening tools warranted a need for gold standard for use in the elderly [27].
The nutritional parameters used in our study were cost-effective, non-invasive, and simple to use. Other nutritional parameters such as the patient-generated subjective global assessment (PG-SGA) and the subjective global assessment (SGA) have been used in studies, to classify between 0-81.4% of EOC patients as malnourished [14,15,16,18,19]. Moreover, we did not use SGA and PG-SGA in our study. This could indicate that our patient cohort was less malnourished compared to the literature, or more likely that the use of the NRS-2002 was more specific for our cohort.
Similar to our findings, increasing age has been previously identified as a risk factor for malnutrition [28]. However, the correlations shown in our study between malnutrition and ascites volume, and malnutrition and platinum-resistance in patients with ovarian cancer have not been described before. Possible explanations could include that ascites predisposes to higher protein-loss, change in bowel-motility and malabsorption, and increase in resting energy expenditure (REE) [29].
It is unclear why platinum-resistant patients are at higher risk of malnutrition than platinum-sensitive patients. Perhaps the platinum-resistant tumor biology, due to its worse prognosis and more aggressive natural course, causes metabolic changes leading to malnutrition [30,31]. A study, involving 237 patients with newly diagnosed stage 3 ovarian cancer, revealed that association with decreased prognostic nutritional index and platinum resistance, poor OS, and poor PFS (p-values: < 0.001, < 0.001, and < 0.001, respectively) [32].
Lieffers et al reported a direct correlation between tumor mass and REE in patients with advanced colorectal cancer [33]. Similarly, Cao et al. described a higher REE in oncological patients with malnutrition [34]. It appears, there is a correlation between tumor mass, tumor dissemination, and malnutrition. However, this correlation has, until now, not been described in EOC patients. In our study, tumor dissemination was documented according to the validated IMO-Script. We showed that patients who had widely disseminated tumor had a higher risk of malnutrition compared to patients with localized tumor spread. However, the IMO-Script does not differentiate between tumor dissemination and tumor burden as a cause for malnutrition.
It is well-established that complete macroscopic cytoreduction is the single most important prognostic factor in EOC patients [35,36,37]. Few studies have been published that examine the correlation between malnutrition and complete cytoreduction. In a retrospective study of EOC patients over 75 years, an albumin level ≤3.7 g/dl was associated with a 2.4 times higher risk of residual tumor at cytoreductive surgery [18]. Our study also shows a similar significant correlation. In our cohort, malnourished patients as classified by NRS-2002 had a higher risk of residual tumor at cytoreductive surgery (OR=4.6, 95%CI=1.5-14.5). This is perhaps not surprising, as malnutrition is associated with other factors known to be linked to complete cytoreduction, such as tumor dissemination (especially level 3) [38,39], platinum-resistance, and ascites [40,41].
In our cohort, malnourished EOC patients received on average twice as much blood-products than non-malnourished patients. Intraoperative blood transfusion increases the likelihood of postoperative complications including mortality and increased hospital-stay [42]. This could be due to immunosuppression caused after allogenic blood transfusion increasing the risk for infection, as described in patients with colorectal cancer [43]. Another study reported that the surgical patients receiving blood transfusions were at higher risk for anastomotic leaks and postoperative sepsis and have a shorter OS [44]. Consequently, blood transfusions in surgical patients have a negative predictive and prognostic influence.
In addition, it is well reported that postoperative complications are more frequent in malnourished patients [19,45,46]. In our study, malnourished patients had a higher rate of postoperative complications. All EOC patients that died within 30 postoperative days, had been classified as malnourished according to the NRS-2002 and other parameters. Moreover, malnutrition significantly correlated with increased hospital stay as classified by NRI, albumin, prealbumin, and ECM/BCM index. Similar results have been reported in other studies [7,47].
Malnourished patients have higher complication rates under chemotherapy treatment and worse response rates compared to non-malnourished patients [48]. In our study, patients with NRS-2002 ≥ 3 were more likely to develop platinum-resistance. Although, on multivariate regression analysis, this was not statistically significant, interestingly, WL >5% in the last 3 months significantly correlated with platinum-resistance (p=0.041, OR=6.99, 95%-CI=1.08-45.45). It can be described as a parameter to predict response to chemotherapy.
Our analysis did not show independent correlation between preoperative malnutrition and PFS. However, we report that malnutrition as assessed by PhAα ≤ 4.5 is an independent prognostic factor for OS in EOC patients. This correlates with previous retrospective studies [21,22] and also a prospective study [49]. In our cohort, EOC patients with ascites had a higher risk of malnutrition. Based on our analysis, ascites was found to increase the risk of malnutrition and indirectly influence the prognosis. Malnutrition seems to be a stronger prognostic factor than ascites for OS in EOC patients. This requires further prospective analyses and was outside the scope of our study.
Conclusions
According to the results of our prospective study, malnutrition is an independent predictor of incomplete cytoreduction in patients with ovarian and peritoneal cancer. Moreover, defined by PhAα it is also an independent prognostic factor for poor overall survival. The preoperative nutritional assessment is an effective tool in identification of high-risk groups within patients with ovarian or peritoneal cancer characterized by poor clinical outcome.
In patients with EOC, malnutrition is a common and serious problem that is often underestimated and misdiagnosed. Our study shows that nutritional status parameters can be used in daily clinical practice to objectively assess for malnutrition. Malnutrition has a significant predictive and prognostic role in the peri-operative care of patients. Hence, nutritional status assessment should be standardized and included in pre-operative screening to provide nutritional support, improve prognosis, and reduce the consequences of cancer-associated nutritional decline.
Author Contributions
Conceptualization: N.S., R.R., and J.S.; Methodology: N.S. and J.S.; Formal Analysis: Bi.E, N.S, G.J and D.X., Resources: N.S, Bi.E, G.J, K.H, B.E, R.C and J.S. Data Curation: B.E, K.H, D.X and R.R.; Writing – Original Draft Preparation: N.S., G.J and Bi.E. Writing – Review & Editing: N.S., Bi.E., R.R., R.C, A.P., and J.S.; Visualization: N.S. and Bi.E.; Supervision: J.S and B.E. Nasser S: N.S, Bilir E: Bi.E, Derin X: D.X, Richter R: R.R, Grabowski J: G.J, Ali P: A.P, Kulbe H: K.H, Chekerov R: C.R, Braicu E: B.E, Sehouli J: S.J.
Funding
None.
Institutional Review Board Statement
Charite Comprehensive Cancer Center, Berlin, Germany (Reference Number: EA2/142/07).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank the study participants.
Conflicts of Interest
None.
References
- Polanski: J., et al., Relationship between Nutritional Status and Clinical Outcome in Patients Treated for Lung Cancer. Nutrients, 2021. 13(10). [CrossRef]
- Brinksma, A., et al., Malnutrition is associated with worse health-related quality of life in children with cancer. Support Care Cancer, 2015. 23(10): p. 3043-52. [CrossRef]
- Zhang, Q., et al., Prevalence and Prognostic Value of Malnutrition Among Elderly Cancer Patients Using Three Scoring Systems. Front Nutr, 2021. 8: p. 738550. [CrossRef]
- Albrecht, J.T. and T.W. Canada, Cachexia and anorexia in malignancy. Hematol Oncol Clin North Am, 1996. 10(4): p. 791-800. [CrossRef]
- Dewys, W.D., et al., Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am J Med, 1980. 69(4): p. 491-7.
- Nitenberg, G. and B. Raynard, Nutritional support of the cancer patient: issues and dilemmas. Crit Rev Oncol Hematol, 2000. 34(3): p. 137-68. [CrossRef]
- Santoso, J.T., et al., Prognostic nutritional index in relation to hospital stay in women with gynecologic cancer. Obstet Gynecol, 2000. 95(6 Pt 1): p. 844-6.
- Ravasco, P., et al., Nutritional deterioration in cancer: the role of disease and diet. Clin Oncol (R Coll Radiol), 2003. 15(8): p. 443-50. [CrossRef]
- Shike, M., Nutrition therapy for the cancer patient. Hematol Oncol Clin North Am, 1996. 10(1): p. 221-34. [CrossRef]
- Pressoir, M., et al., Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. Br J Cancer, 2010. 102(6): p. 966-71. [CrossRef]
- Caccialanza, R., et al., Nutritional Support in Cancer Patients: A Position Paper from the Italian Society of Medical Oncology (AIOM) and the Italian Society of Artificial Nutrition and Metabolism (SINPE). J Cancer, 2016. 7(2): p. 131-5. [CrossRef]
- Buzby, G.P., et al., Study protocol: a randomized clinical trial of total parenteral nutrition in malnourished surgical patients. Am J Clin Nutr, 1988. 47(2 Suppl): p. 366-81. [CrossRef]
- Sung, H., et al., Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin, 2021. 71(3): p. 209-249. [CrossRef]
- Laky, B., et al., Malnutrition among gynaecological cancer patients. Eur J Clin Nutr, 2007. 61(5): p. 642-6. [CrossRef]
- Gupta, D., et al., Impact of improved nutritional status on survival in ovarian cancer. Support Care Cancer, 2010. 18(3): p. 373-81. [CrossRef]
- Kathiresan, A.S., et al., Malnutrition as a predictor of poor postoperative outcomes in gynecologic cancer patients. Arch Gynecol Obstet, 2011. 284(2): p. 445-51. [CrossRef]
- Tunca, J.C., Nutritional evaluation of gynecologic cancer patients during initial diagnosis of their disease. Am J Obstet Gynecol, 1983. 147(8): p. 893-6. [CrossRef]
- Alphs, H.H., et al., Predictors of surgical outcome and survival among elderly women diagnosed with ovarian and primary peritoneal cancer. Gynecol Oncol, 2006. 103(3): p. 1048-53. [CrossRef]
- Ottery, F.D., Cancer cachexia: prevention, early diagnosis, and management. Cancer Pract, 1994. 2(2): p. 123-31.
- Phippen, N.T., et al., Evaluation of the Patient-Generated Subjective Global Assessment (PG-SGA) as a predictor of febrile neutropenia in gynecologic cancer patients receiving combination chemotherapy: a pilot study. Gynecol Oncol, 2011. 123(2): p. 360-4. [CrossRef]
- Asher, V., J. Lee, and A. Bali, Preoperative serum albumin is an independent prognostic predictor of survival in ovarian cancer. Med Oncol, 2012. 29(3): p. 2005-9. [CrossRef]
- Gupta, D., et al., Can subjective global assessment of nutritional status predict survival in ovarian cancer? J Ovarian Res, 2008. 1(1): p. 5. [CrossRef]
- Kondrup, J., et al., Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr, 2003. 22(3): p. 321-36. [CrossRef]
- Jackson, A.A., et al., Body composition assessment in nutrition research: value of BIA technology. Eur J Clin Nutr, 2013. 67 Suppl 1: p. S71-8. [CrossRef]
- Sehouli, J., et al., ["IMO"--intraoperative mapping of ovarian cancer]. Zentralbl Gynakol, 2003. 125(3-4): p. 129-35.
- Sehouli J, Mustea A, Konsgen D, Lichtenegger W. [Conventional and experimental prognostic factors in ovarian cancer] Zentralbl.Gynakol. 2004;126:315-22.
- Cascio, B.L. and J.V. Logomarsino, Evaluating the effectiveness of five screening tools used to identify malnutrition risk in hospitalized elderly: A systematic review. Geriatr Nurs, 2018. 39(1): p. 95-102. [CrossRef]
- Pirlich, M., et al., The German hospital malnutrition study. Clin Nutr, 2006. 25(4): p. 563-72. [CrossRef]
- Dolz, C., et al., Ascites increases the resting energy expenditure in liver cirrhosis. Gastroenterology, 1991. 100(3): p. 738-44. [CrossRef]
- Kuhn, W.C., Therapy for recurrent ovarian cancer. Curr Womens Health Rep, 2003. 3(1): p. 33-8.
- Eisenkop, S.M. and N.M. Spirtos, The clinical significance of occult macroscopically positive retroperitoneal nodes in patients with epithelial ovarian cancer. Gynecol Oncol, 2001. 82(1): p. 143-9. [CrossRef]
- Zhang, W., et al., Preoperative prognostic nutritional index is a powerful predictor of prognosis in patients with stage III ovarian cancer. Sci Rep, 2017. 7(1): p. 9548. [CrossRef]
- Lieffers, J.R., et al., A viscerally driven cachexia syndrome in patients with advanced colorectal cancer: contributions of organ and tumor mass to whole-body energy demands. Am J Clin Nutr, 2009. 89(4): p. 1173-9. [CrossRef]
- Cao, D.X., et al., Resting energy expenditure and body composition in patients with newly detected cancer. Clin Nutr, 2010. 29(1): p. 72-7. [CrossRef]
- Elattar, A., et al., Optimal primary surgical treatment for advanced epithelial ovarian cancer. Cochrane Database Syst Rev, 2011(8): p. CD007565. [CrossRef]
- Fotopoulou, C., et al., Primary radical surgery in elderly patients with epithelial ovarian cancer: analysis of surgical outcome and long-term survival. Int J Gynecol Cancer, 2010. 20(1): p. 34-40. [CrossRef]
- Fotopoulou, C., et al., Surgical outcome and survival analysis of young patients with primary epithelial ovarian cancer. Anticancer Res, 2009. 29(7): p. 2809-15.
- Fotopoulou, C., et al., Can complete tumor resection be predicted in advanced primary epithelial ovarian cancer? A systematic evaluation of 360 consecutive patients. Eur J Surg Oncol, 2010. 36(12): p. 1202-10. [CrossRef]
- Sehouli, J., et al., Intra-abdominal tumor dissemination pattern and surgical outcome in 214 patients with primary ovarian cancer. J Surg Oncol, 2009. 99(7): p. 424-7. [CrossRef]
- Gil-Ibanez, B., et al., Predictive factors in relapsed ovarian cancer for complete tumor resection. Anticancer Res, 2011. 31(8): p. 2583-7.
- Tian, W.J., et al., A risk model for secondary cytoreductive surgery in recurrent ovarian cancer: an evidence-based proposal for patient selection. Ann Surg Oncol, 2012. 19(2): p. 597-604. [CrossRef]
- Al-Refaie, W.B., et al., Blood transfusion and cancer surgery outcomes: a continued reason for concern. Surgery, 2012. 152(3): p. 344-54. [CrossRef]
- Nielsen, H.J., Detrimental effects of perioperative blood transfusion. Br J Surg, 1995. 82(5): p. 582-7. [CrossRef]
- Golub, R., et al., A multivariate analysis of factors contributing to leakage of intestinal anastomoses. J Am Coll Surg, 1997. 184(4): p. 364-72. [PubMed]
- Barbosa-Silva, M.C. and A.J. Barros, Bioelectric impedance and individual characteristics as prognostic factors for post-operative complications. Clin Nutr, 2005. 24(5): p. 830-8. [CrossRef]
- Makela, J.T., et al., Morbidity and mortality after abdominal operations for cancer. Hepatogastroenterology, 1992. 39(5): p. 420-3. [PubMed]
- Laky, B., et al., Pretreatment malnutrition and quality of life - association with prolonged length of hospital stay among patients with gynecological cancer: a cohort study. BMC Cancer, 2010. 10: p. 232. [CrossRef]
- Van Cutsem, E. and J. Arends, The causes and consequences of cancer-associated malnutrition. Eur J Oncol Nurs, 2005. 9 Suppl 2: p. S51-63. [CrossRef]
- Sehouli, J., et al., Effects of sarcopenia and malnutrition on morbidity and mortality in gynecologic cancer surgery: results of a prospective study. J Cachexia Sarcopenia Muscle, 2021. 12(2): p. 393-402. [CrossRef]
Figure 1.
A) Median overall survival of patients with Nutritional Risk Screening (NRS)-2002 ≥3 vs NRS-2002 <3 (p=0.001), B) Median overall survival of patients with Phase-angle α ≤ 4.5 º vs. Phase-angle α > 4.5 º (p=0.001).
Figure 1.
A) Median overall survival of patients with Nutritional Risk Screening (NRS)-2002 ≥3 vs NRS-2002 <3 (p=0.001), B) Median overall survival of patients with Phase-angle α ≤ 4.5 º vs. Phase-angle α > 4.5 º (p=0.001).
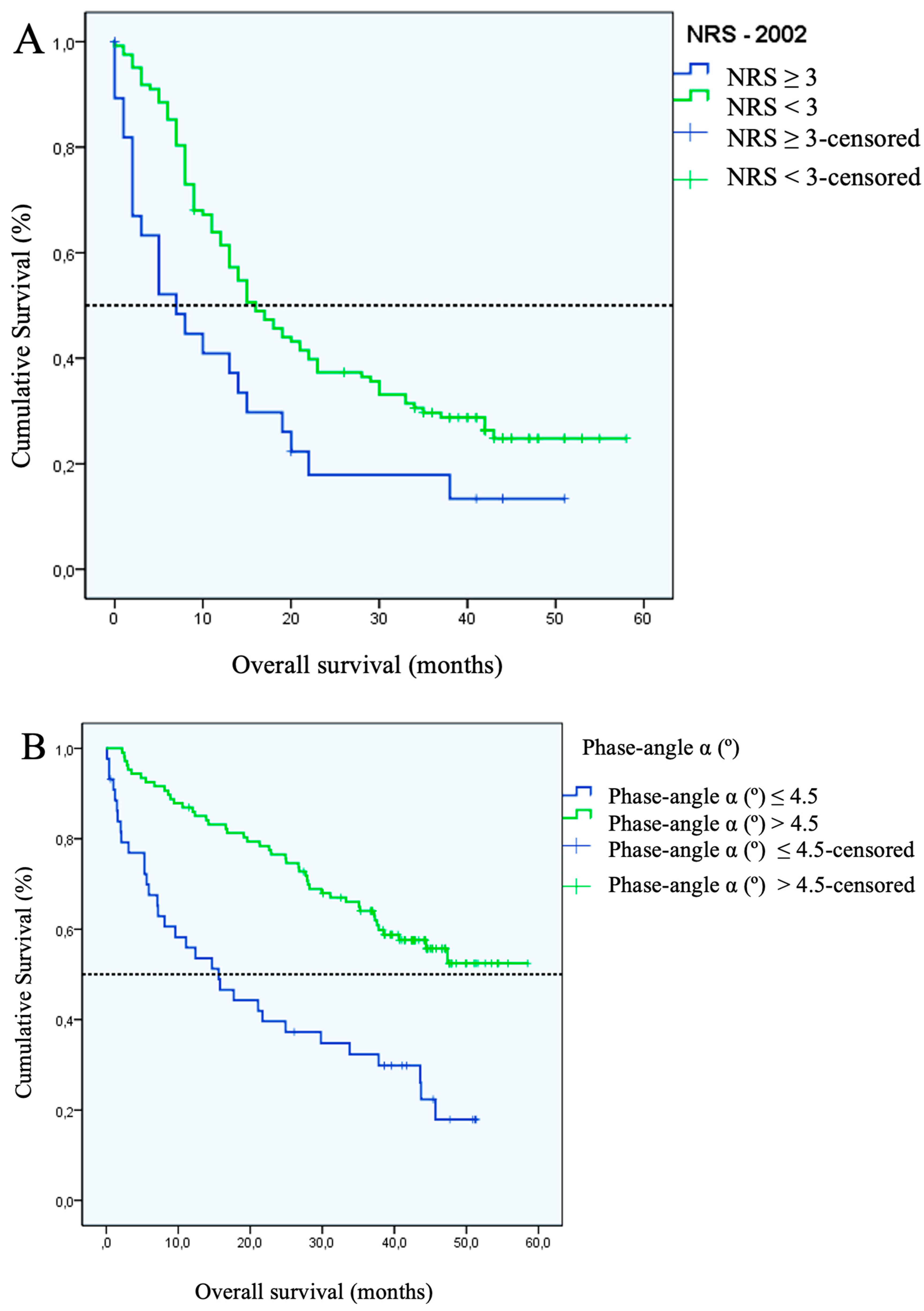
Figure 2.
Median progression-free survival in patients with Nutritional Risk Screening (NRS)-2002 ≥3 vs. NRS-2002 <3 (p=0.006).
Figure 2.
Median progression-free survival in patients with Nutritional Risk Screening (NRS)-2002 ≥3 vs. NRS-2002 <3 (p=0.006).
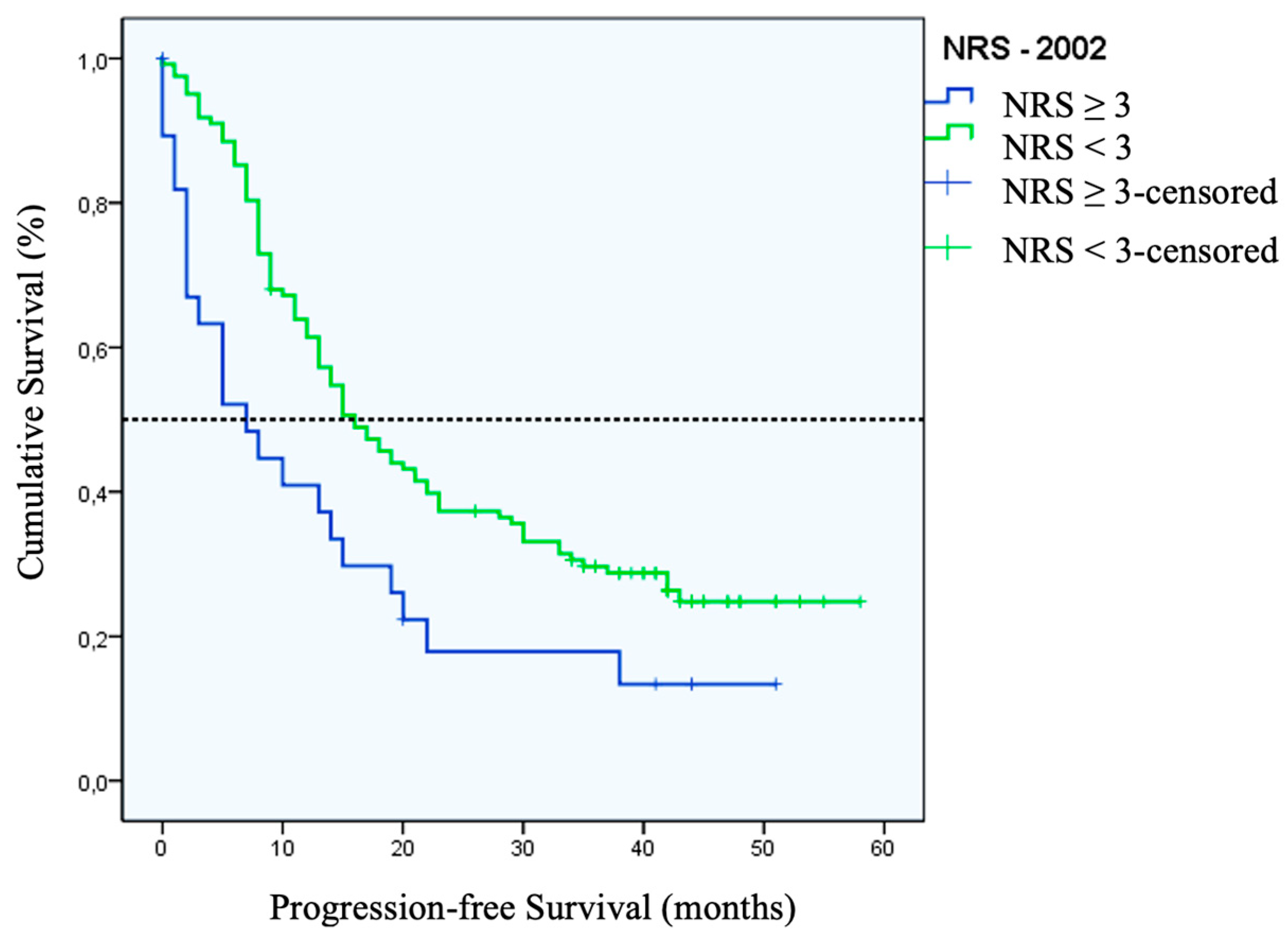

Table 1.
Patient Baseline Characteristics (n=152).
| Characteristic | Number (%) |
|---|---|
| Age (years) | 56 (19 – 84)* |
| Weight (kg) | 65 (45 – 141)* |
| BMI (kg/m²) | 24,4 (17,8 – 48,8)* |
| Primary OC | 79 (52.0) |
| FIGO Staging (Primary OC only) | |
| I | 8 (10.3) |
| II | 8 (10.3) |
| III | 39 (50) |
| IV | 22 (28.2) |
| Unknown | 2 (2.5) |
| Recurrent OC | 73 (48.0) |
| Platin Response (Recurrent OC only) | |
| Platin sensitive | 48 (65.8) |
| Platin resistant | 25 (34.2) |
| Grading | |
| I | 4 (2.6) |
| II | 40 (26.3) |
| III | 82 (53.9) |
| Unknown | 26 (17.1) |
| Histology | |
| Serous | 119 (78.3) |
| Endometrioid | 7 (4.6) |
| Mucinous | 6 (3.9) |
| Clear cell | 7 (4.6) |
| Other | 3 (2.0) |
| Unknown | 10 (6.6) |
| Ascites | |
| ≥ 500 ml | 26 (17.1) |
| < 500 ml | 49 (32.2) |
| No ascites | 75 (49.3) |
| Unknown | 2 (1.3) |
| Tumor Spread | |
| Small bowel involvement | 56 (36.8) |
| Large bowel involvement | 83 (54.6) |
| Peritoneal carcinomatosis | 120 (78.9) |
| Residual Tumor | |
| None | 94 (61.8) |
| ≤ 1 cm | 30 (19.8) |
| > 1 cm | 28 (17.7) |
*Median (Interquartile Range). BMI: body mass index, FIGO: International Federation of Gynaecology and Obstetrics, OC: Ovarian Cancer
Table 2.
Prevalence of malnutrition according to various nutritional status indicators and their respective sensitivity and specificity when correlated with NRS-2002.
Table 2.
Prevalence of malnutrition according to various nutritional status indicators and their respective sensitivity and specificity when correlated with NRS-2002.
| Nutritional Status Indicator* | Cut-off value for malnutrition | Number (%) | Area under the ROC curve | Sensitivity (%) |
Specificity (%) |
CI (95%) |
|---|---|---|---|---|---|---|
| NRS–2002 | ≥ 3 | 28 (18.4) | NA | NA | NA | NA |
| Prealbumin (mg/l) | < 20 | 51 (37.2) | 0,807 | 77.8 | 72.7 | 0.708-0.906 |
| NRI | < 100 | 47 (31.8) | 0,801 | 67.9 | 76.7 | 0.707-0.896 |
| Weight Loss in last 3 months (%) | > 5 | 29 (19.1) | 0,780 | 64.3 | 91.1 | 0.665-0.895 |
| Transferrin (mg/dl) | < 200 | 41 (28.1) | 0,785 | 65.4 | 80 | 0.680-0.890 |
| ECM/BCM Ratio | > 1,2 | 58 (38.4) | 0,762 | 77.8 | 70.2 | 0.653-0.871 |
| Phase-angle α (º) | ≤ 4,5 | 44 (29.1) | 0,760 | 66.7 | 79 | 0.651-0.869 |
| Albumin (g/dl) | ≤ 4,0 | 53 (35.3) | 0,769 | 75 | 73.8 | 0.665-0.872 |
BCM: Body Cell Mass, BMI: body mass index, CI: Confidence Interval, ECM: Extra Cellular Mass, NA: not applicable, NRI: Nutritional Risk Index, NRS-2002: Nutritional Risk Screening-2002. *BMI did not correlate with NRS-2002 and was therefore excluded from further evaluations
Table 3.
Prevalence of malnutrition as evaluated by the Nutritional Risk Screening (NRS)-2002 according to patient and tumor characteristics.
Table 3.
Prevalence of malnutrition as evaluated by the Nutritional Risk Screening (NRS)-2002 according to patient and tumor characteristics.
| Characteristic | Label | Total (n=152) (%) |
Patients with NRS ≥ 3 (n=28) (%) |
p-Value |
|---|---|---|---|---|
| Age | > 65 years | 42 (27,6) | 13 (46,4) | p = 0.014 |
| ≤ 65 years | 110 (72,3) | 15 (53,6) | ||
| Diagnosis | Primary | 79 (51,9) | 18 (64,3) | NS |
| Recurrent | 73 (48,0) | 10 (35,7) | ||
| Ascites | > 500 ml | 28 (18,4) | 11 (39,3) | p = 0.001 |
| < 500 ml | 124 (81,6) | 17 (60,7) | ||
| Histology | Serous | 123 (80,9) | 22 (78,6) | NS |
| Non-serous | 29 (19,1) | 6 (21,4) | ||
| Grading | I + II | 50 (32,9) | 9 (32,1) | NS |
| III | 87 (57,3) | 18 (64,3) | ||
| Bowel involvement | Yes | 93 (61,2) | 17 (60,7) | NS |
| No | 59 (38,8) | 11 (39,3) | ||
| Peritoneal carcinomatosis | Yes | 120 (78,9) | 24 (85,7) | NS |
| No | 30 (19,7) | 4 (14,2) | ||
| FIGO Stage | I + II | 16 (10,5) | 3 (10,7) | NS |
| III + IV | 63 (41,4) | 15 (53,6) | ||
| Platinum sensitivity | Platinum sensitive | 49 (32,2) | 3 (10,7) | p = 0.007 |
| Platinum resistant | 24 (15,8) | 7 (25,0) |
FIGO: International Federation of Gynaecology and Obstetrics, NS= not significant.
Table 4.
Correlation of Nutritional Status Indicators and tumor characteristics where plus sign (+) indicated correlation.
Table 4.
Correlation of Nutritional Status Indicators and tumor characteristics where plus sign (+) indicated correlation.
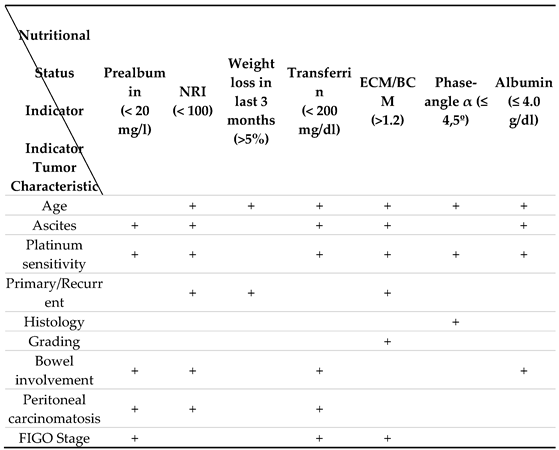
BCM: Body Cell Mass, ECM: Extra Cellular Mass, FIGO: International Federation of Gynaecology and Obstetrics. + is defined as positive correlation between the variables.
Table 5.
Malnutrition and tumor spread according to Nutritional Status Indicators.
| Nutritional Status Indicators | Number of fields with tumor load – IMO-Script (median) | p-value | |
| Malnourished | Non-malnourished | ||
| NRS–2002 (≥ 3) | 5 | 3 | 0,044 |
| NRI (< 100) | 6 | 3 | < 0,001 |
| Prealbumin (< 20 mg/l) | 6 | 3 | < 0,001 |
| Transferrin (< 200 mg/dl) | 6 | 3 | < 0,001 |
| Albumin (≤ 4.0 g/dl) | 5 | 3 | 0,001 |
| ECM/BCM (>1.2) | 4 | 3 | 0,024 |
| Phase-angle α (≤ 4,5º) | 4 | 3 | 0,041 |
| Weight loss in last 3 months (>5%) | 4 | 3 | NS |
BCM: Body Cell Mass, BMI: body mass index, ECM: Extra Cellular Mass, IMO: intraoperative mapping of ovarian, NRI: Nutritional Risk Index, NRS-2002: Nutritional Risk Screening 2002, NS= not significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



